Periodontology 2000, Vol. 6, 1994, 88-1 00 Printed in Denmark . All rights resewed Copyright 0 Munksgaard 1994 PERIODONTOLOGY 2000 ISSN 0906-6713 Papillon-Leewe syndrome THOMAS C. HART & LIOR SHAPIRA Most forms of inflammatory periodontal disease can be successfully treated and managed in the majority of patients. As a result, the ultimate goal of periodontal therapy has changed from that of simply arresting disease progression to one aimed at regenerating the supporting tissues. Unfortu- nately, not all forms of periodontal disease respond to treatment. Severe periodontitis that is resistant to conventional periodontal treatment has been recognized in a number of monogenic conditions (81). Certainly one of the most intriguing and den- tally challenging of these conditions is Papillon- Lefevre syndrome. In 1924, Papillon & Lefevre (58) described two siblings, the products of a first-cousin mating, with a condition characterized by diffuse transgradient palmoplantar keratosis and the premature loss of both the deciduous and permanent dentitions. This condition came to be known as Papillon-Lefkvre syndrome, and subsequently over 200 cases have been described. The hallmarks of Papillon-Lefkvre syndrome are palmoplantar keratosis and rapid periodontal destruction of both dentitions. An in- creased susceptibility to infection has been re- ported in approximately 20% of Papillon-Lefkvre patients (3, 32, 33, 361, and additional reported findings include intracranial calcifications (9, 13, 32, 40, 98), retardation of the somatic development (711, follicular hyperkeratosis (71) and onycho- gryphosis (71, 98). Comprehensive reviews of the Papillon-Lefevre syndrome literature have been conducted by Gorlin et al. in 1964 (32) and most recently by Haneke in 1979 (35). Clinical findings reported in Papillon-Lefevre patients suggest that the clinical expression of the condition is highly variable. Unfortunately, to date, no pathognomonic disease marker exists allowing definitive diagnosis of Papillon-Lefevre syndrome. Therefore, it is not clear if all reported cases are actually Papillon- Lefkvre syndrome or rather represent an etiolog- ically diverse group of conditions sharing similar clinical disease manifestations. Differential diagnosis The two cardinal diagnostic features of the Papillon- Lefevre syndrome are palmoplantar keratosis and an early-onset form of rapidly progressive periodontitis (35). The differential diagnosis of Papillon-Lefevre syndrome should include all congenital forms of dif- fuse palmoplantar hyperkeratosis summarized in Table 1. The association with severe early-onset peri- odontitis is unique to Papillon-Lefkvre syndrome and Haim-Munk syndrome. The Haim-Munk syn- drome is an unusual condition of palmoplantar keratosis (Fig. 1, 21, early-onset periodontitis (Fig. 3), arachnodactyly (a peculiar deformity of the terminal phalanges of the hands and feet) and recurrent ab- scess formation (31-33, 80). Historically, the diagnostic distinction between the palmoplantar hyperkeratosis syndromes and Pa- pillon-Lefkvre syndrome has been the occurrence of severe early-onset periodontal destruction (35). Re- cently this assumption has been challenged (64) by reports of families affected by Papillon-Lefevre syn- drome and Haim-Munk syndrome in which some family members manifest the typical skin and peri- odontal lesions, whereas other siblings manifest only the palmoplantar keratosis with no periodontal in- volvement of either the primary or permanent den- titions (10, personal communications from Jorge Meyle and Aubrey Soskolne). Bullon et al. (10) re- ported variable clinical expression of palmoplantar hyperkeratotic skin lesions in a Papillon-Lefkvre syn- drome family with 6 children, including 2 unaffected individuals and 4 individuals with skin lesions. Only 2 of those with skin lesions had severe periodontitis. Bullon et al. noted a wide range in the clinical ex- pression of skin lesions in the 4 affected children. The skin manifestations varied from the presence of hyperkeratotic areas on the dorsum of the feet, hands, elbows and knees in one sibling to only trans- gradient plantar hyperkeratosis and slight palmar keratosis in an older sibling. A number of individuals 88
Transcript
Periodontology 2000, Vol. 6, 1994, 88-1 00 Printed in Denmark . All rights resewed
Copyright 0 Munksgaard 1994
PERIODONTOLOGY 2000 ISSN 0906-6713
Papillon-Leewe syndrome THOMAS C. HART & LIOR SHAPIRA
Most forms of inflammatory periodontal disease can be successfully treated and managed in the majority of patients. As a result, the ultimate goal of periodontal therapy has changed from that of simply arresting disease progression to one aimed at regenerating the supporting tissues. Unfortu- nately, not all forms of periodontal disease respond to treatment. Severe periodontitis that is resistant to conventional periodontal treatment has been recognized in a number of monogenic conditions (81). Certainly one of the most intriguing and den- tally challenging of these conditions is Papillon- Lefevre syndrome.
In 1924, Papillon & Lefevre (58) described two siblings, the products of a first-cousin mating, with a condition characterized by diffuse transgradient palmoplantar keratosis and the premature loss of both the deciduous and permanent dentitions. This condition came to be known as Papillon-Lefkvre syndrome, and subsequently over 200 cases have been described. The hallmarks of Papillon-Lefkvre syndrome are palmoplantar keratosis and rapid periodontal destruction of both dentitions. An in- creased susceptibility to infection has been re- ported in approximately 20% of Papillon-Lefkvre patients (3, 32, 33, 361, and additional reported findings include intracranial calcifications (9, 13, 32, 40, 98), retardation of the somatic development (711, follicular hyperkeratosis (71) and onycho- gryphosis (71, 98). Comprehensive reviews of the Papillon-Lefevre syndrome literature have been conducted by Gorlin et al. in 1964 (32) and most recently by Haneke in 1979 (35). Clinical findings reported in Papillon-Lefevre patients suggest that the clinical expression of the condition is highly variable. Unfortunately, to date, no pathognomonic disease marker exists allowing definitive diagnosis of Papillon-Lefevre syndrome. Therefore, it is not clear if all reported cases are actually Papillon- Lefkvre syndrome or rather represent an etiolog- ically diverse group of conditions sharing similar clinical disease manifestations.
Differential diagnosis
The two cardinal diagnostic features of the Papillon- Lefevre syndrome are palmoplantar keratosis and an early-onset form of rapidly progressive periodontitis (35). The differential diagnosis of Papillon-Lefevre syndrome should include all congenital forms of dif- fuse palmoplantar hyperkeratosis summarized in Table 1. The association with severe early-onset peri- odontitis is unique to Papillon-Lefkvre syndrome and Haim-Munk syndrome. The Haim-Munk syn- drome is an unusual condition of palmoplantar keratosis (Fig. 1, 21, early-onset periodontitis (Fig. 3), arachnodactyly (a peculiar deformity of the terminal phalanges of the hands and feet) and recurrent ab- scess formation (31-33, 80).
Historically, the diagnostic distinction between the palmoplantar hyperkeratosis syndromes and Pa- pillon-Lefkvre syndrome has been the occurrence of severe early-onset periodontal destruction (35). Re- cently this assumption has been challenged (64) by reports of families affected by Papillon-Lefevre syn- drome and Haim-Munk syndrome in which some family members manifest the typical skin and peri- odontal lesions, whereas other siblings manifest only the palmoplantar keratosis with no periodontal in- volvement of either the primary or permanent den- titions (10, personal communications from Jorge Meyle and Aubrey Soskolne). Bullon et al. (10) re- ported variable clinical expression of palmoplantar hyperkeratotic skin lesions in a Papillon-Lefkvre syn- drome family with 6 children, including 2 unaffected individuals and 4 individuals with skin lesions. Only 2 of those with skin lesions had severe periodontitis. Bullon et al. noted a wide range in the clinical ex- pression of skin lesions in the 4 affected children. The skin manifestations varied from the presence of hyperkeratotic areas on the dorsum of the feet, hands, elbows and knees in one sibling to only trans- gradient plantar hyperkeratosis and slight palmar keratosis in an older sibling. A number of individuals
88
Papillon-Lef&vre syndrome
Table 1. Skin diseases with palmoplantar keratoderma Disease Inheritance Onset Appearance Associated features Palmoplantar hyper- dominant first year diffuse, uniform rarely ainhum
keratosis (Unna-Thost syndrome)
Howel-Evans’ syndrome dominant ages 5-15 diffuse years
esophageal carcinoma within patient’s lifetime in most cases
Palmoplantar hyper- dominant second or third punctate often in creases; striate form also exists; ar- keratosis-punctate disease sometimes very painful senic exposure produces
a phenocopy of this dis- ease; may have focal gingival hyperkeratosis
Vohwinkel’s svndrome dominant childhood diffuse with stellate pattern ainhum frequent Ma1 deMeleda recessive infancy lesions also on dorsa of -
feet, elbows, knees; very fissured; malodorous
Papillon-Lefevre recessive ages 1-5 psoriasis-like lesions on periodontal disease and
fication of falx cerebri common
syndrome elbows and knees and teeth loss common; calci- over Achilles tendon
Gamborg-Nielsen recessive childhood diffuse with very thick -
syndrome ages 3-8 horny layer; distinct de- marcation to normal skin by a bluish-red zone
swdrome Haim-Munk syndrome recessive infancy similar to Papillon-Lefkvre arachnodact
with Papillon-Lefkvre have been reported to have palmoplantar keratosis but no periodontal destruc- tion of the primary dentition, although the perma- nent dentition was affected (35, 54, 70).
Clinical description of Papillon-Lefevre syndrome
Skin
Hyperkeratosis of the palms and soles is the primary skin lesion found in Papillon-Lefevre syndrome. Hy- perkeratosis refers to hypertrophy of the horny layer of the epidermis. The involved palmar and plantar surfaces are initially affected between the first and fourth years (2, 12, 32, 38, 44, 51), although skin lesions may occur shortly after birth (13, 55, 69, 96). Initially, the palms and soles present a dry, red and scaly appearance. The dermal involvement may ex- hibit a parchment-like quality, with a diffuse distri- bution similar to a glove effect, or may present as a well demarcated hyperkeratotic involvement of the
palms. The most common presentation is the well demarcated form (12). Occasionally, the external malleoli, tibia1 tuberosities and dorsum of finger and toe joints are involved with hyperkeratotic plaques (32). The soles of the feet are usually more severely affected than the hands, and the lesions may extend to the Achilles tendon (Fig. 4). Thickening and crack- ing of the plantar skin may be so severe that walking is difficult. The degree of hyperkeratosis varies sig- nificantly from patient to patient, even within the same family, and a seasonal variation in the severity of symptoms has been reported (23, 32, 34, 39, 44, 52, 62,63). Krebs (44) noted that cutaneous flare-ups were most severe during episodes of feverish disease. In some children palmoplantar keratosis appears simultaneously with the periodontal involvement of the primary teeth and regress once the periodontally involved teeth are lost (32). Recurrence of hyperkera- totic lesions has been observed coincident with peri- odontal involvement of the permanent teeth. Several reports suggest that the degree of hyperkeratosis is greatest at the time the periodontal involvement is the most severe (32, 43, 94). Skin lesions are often
89
Hart & ShaDira
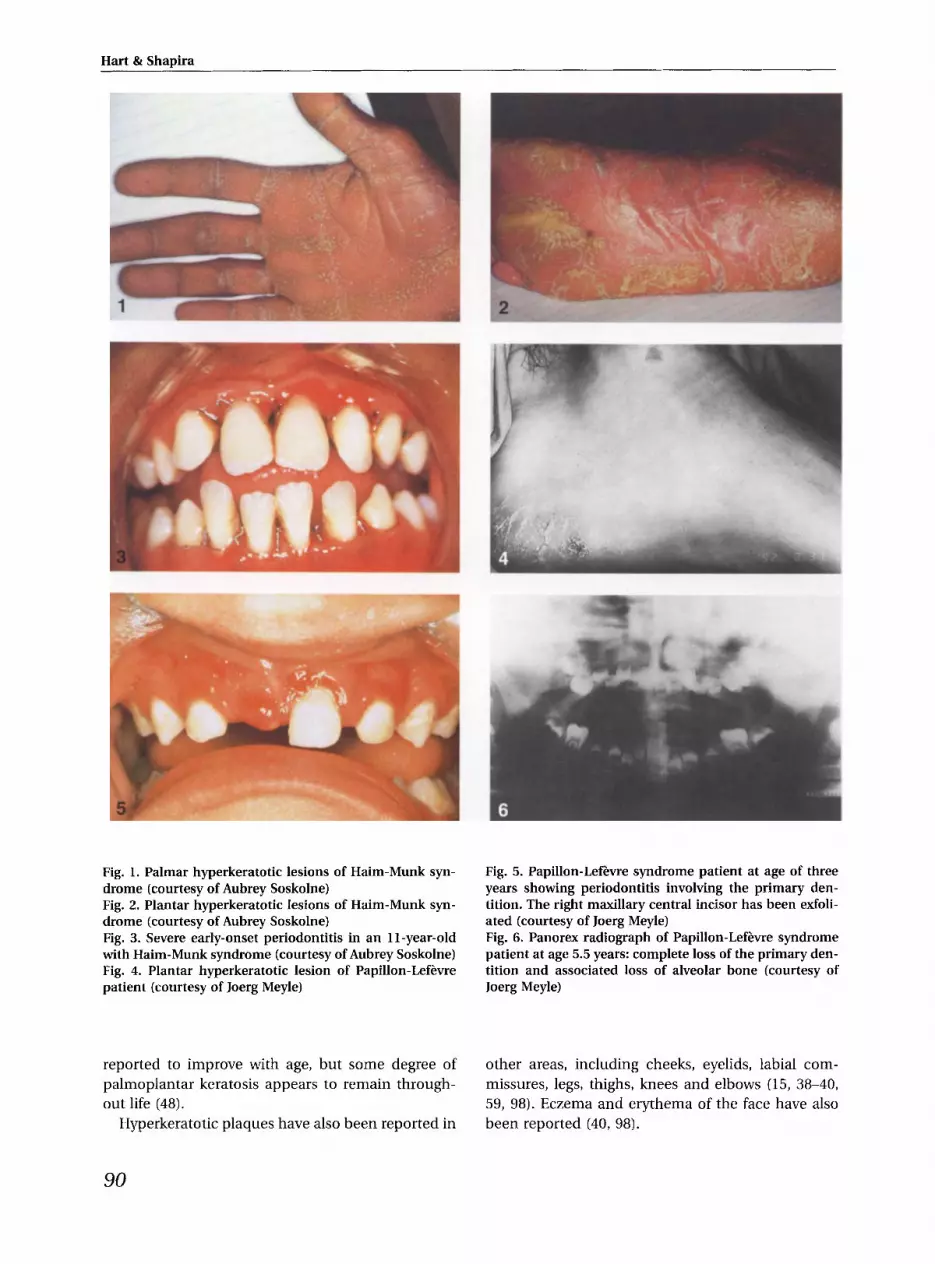
Fig. 1. Palmar hyperkeratotic lesions of Haim-Munk syn- drome (courtesy of Aubrey Soskolne) Fig. 2. Plantar hyperkeratotic lesions of Haim-Munk syn- drome (courtesy of Aubrey Soskolne) Fig. 3. Severe early-onset periodontitis in an 11-year-old with Haim-Munk syndrome (courtesy of Aubrey Soskolne) Fig. 4. Plantar hyperkeratotic lesion of Papillon-Lefhre patient (courtesy of Joerg Meyle)
Fig. 5. Papillon-Lefkvre syndrome patient at age of three years showing periodontitis involving the primary den- tition. The right maxillary central incisor has been exfoli- ated (courtesy of Joerg Meyle) Fig. 6. Panorex radiograph of Papillon-Lefkvre syndrome patient at age 5.5 years: complete loss of the primary den- tition and associated loss of alveolar bone (courtesy of Joerg Meyle)
reported to improve with age, but some degree of palmoplantar keratosis appears to remain through- out life (48).
Hyperkeratotic plaques have also been reported in
other areas, including cheeks, eyelids, labial com- missures, legs, thighs, knees and elbows (15, 38-40, 59, 98). Eczema and erythema of the face have also been reported (40, 98).
90
Papillon-LefZ-vre syndrome
Histology
Light microscopy. Histological examination of skin lesions show mild hyperkeratosis, focal hyperpara- keratosis, hypergranulosis, mild acanthosis and ir- regular elongation and widening of the rete ridges in the epidermis. In the upper dermis, a slight perivas- cular chronic inflammatory cell infiltrate composed mostly of mononuclear cells may be evident, similar to that seen with chronic dermatitis (46,521. The mi- totic index of cutaneous epidermal cells appears un- remarkable (46).
Electron microscopy. The dermoepidermal junction, basal cells and melanocytes are reportedly normal. The granular cells of the interfollicular epidermis are reported to contain numerous lipid-like vacuoles and frequently a reduced content of tonofilaments, with abnormal rectangular or globular keratohyaline granules (52).
Oral manifestations
Prior to tooth eruption, the gingival and mucosal surfaces appear normal. Primary tooth development and eruption is reported to be normal. However, concomitantly with the appearance of palmoplantar keratosis, the gingiva becomes inflamed, swells and bleeds. Rapid destruction of the periodontium sup- porting the primary dentition follows, with destruc- tion occurring in the general order of tooth eruption (44) (Fig. 5). Pathologically deepened periodontal pockets precedes exfoliation of the teeth. Typically, affected individuals have lost nearly all primary teeth by the age of 4 years (Fig. 6). Severe gingival in- flammation is a common finding (46), and in only a few instances is the loss of teeth not accompanied by severe gingival inflammation (24, 39, 68). Chew- ing may be difficult and painful due to hypermo- bility of the teeth, multiple abscesses and food im- paction (35, 46). Significant plaque and calculus de- posits may be present (721, and significant halitosis has also been reported (28, 92). Following exfoliation of the teeth, gingival inflammation subsides and the gingiva rapidly resumes a normal appearance. The gingival tissues appear normal until eruption of the permanent dentition, when the inflammatory pro- cess repeats itself. Aside from the periodontal de- struction, the teeth and gums are anatomically nor- mal. The roots of the periodontally involved perma- nent teeth show no significant signs of resorption at the time of exfoliation. By the age of 14 years, most of the permanent dentition is lost; however, the third
Fig. 7. Panorex radiograph of a Papillon-LeEvre patient at age 18 showing complete loss of the permanent dentition and gross atrophy of alveolar bone (courtesy of Joerg Meyle)
molars are often spared. Periodontal destruction is so severe that the alveolar bone resorption has been described as gross atrophy of alveolar bone (37, 52) (Fig. 7).
Genetics
Papillon-Lefevre syndrome displays familial aggre- gation, suggesting a genetic basis for its etiology. Gorlin et al. (32) noted 3 major features of genetic interest in this syndrome: 1) the parents are not affected, 2) affected siblings with similar pathology have been observed and 3) the observed rate of parental consanguinity is far greater than that for the general population. These observations support autosomal recessive transmission of Papillon- Lefevre syndrome, as proposed by Jansen & Dekker in 1956 (40). Cytogenetic karyotyping (GTG banding) has revealed normal karyotypes in two affected Papillon-Lefevre syndrome siblings, suggesting that the genetic mutation responsible for Papillon- Lefevre syndrome is unlikely to involve a large aber- ration or re-arrangement of chromosomal DNA (10). Approximately 2-4 of 1000 people are heterozygous for the Papillon-Lefevre syndrome gene and are therefore carriers (32). This carrier rate would result in a population prevalence of approximately 1 case of Papillon-Lefkvre syndrome in 1-4 million people. Although carriers do not express the clinical traits associated with Papillon-Lefkvre syndrome, when two such carriers mate, there is a 25% chance of producing an offspring with Papillon-Lefevre syn- drome. Parents who already have a child affected by Papillon-Lefevre syndrome seeking genetic counsel- ing should be advised that there is a 25% probability of Papillon-Lefkvre syndrome in each subsequent offspring.
91
Hart & Shapira
It has been suggested that the true incidence of Papillon-Lefevre syndrome is underreported (35). Most cases of Papillon-Lefevre syndrome in the literature are reports from dentists (57). If dermatol- ogists routinely conducted oral examinations for pa- tients with hyperkeratotic lesions, the reported inci- dence of Papillon-Lefevre syndrome could be greater. Both sexes appear to be affected at equal rates, and individuals of many racial groups have been reported to be affected including Caucasian (Europe, America, North Africa and the near East), Mongoloid (Japan), mestizo (Dominican Republic), Negroid (United States and Somalia) and Dravidian (India) (35).
Immunological findings
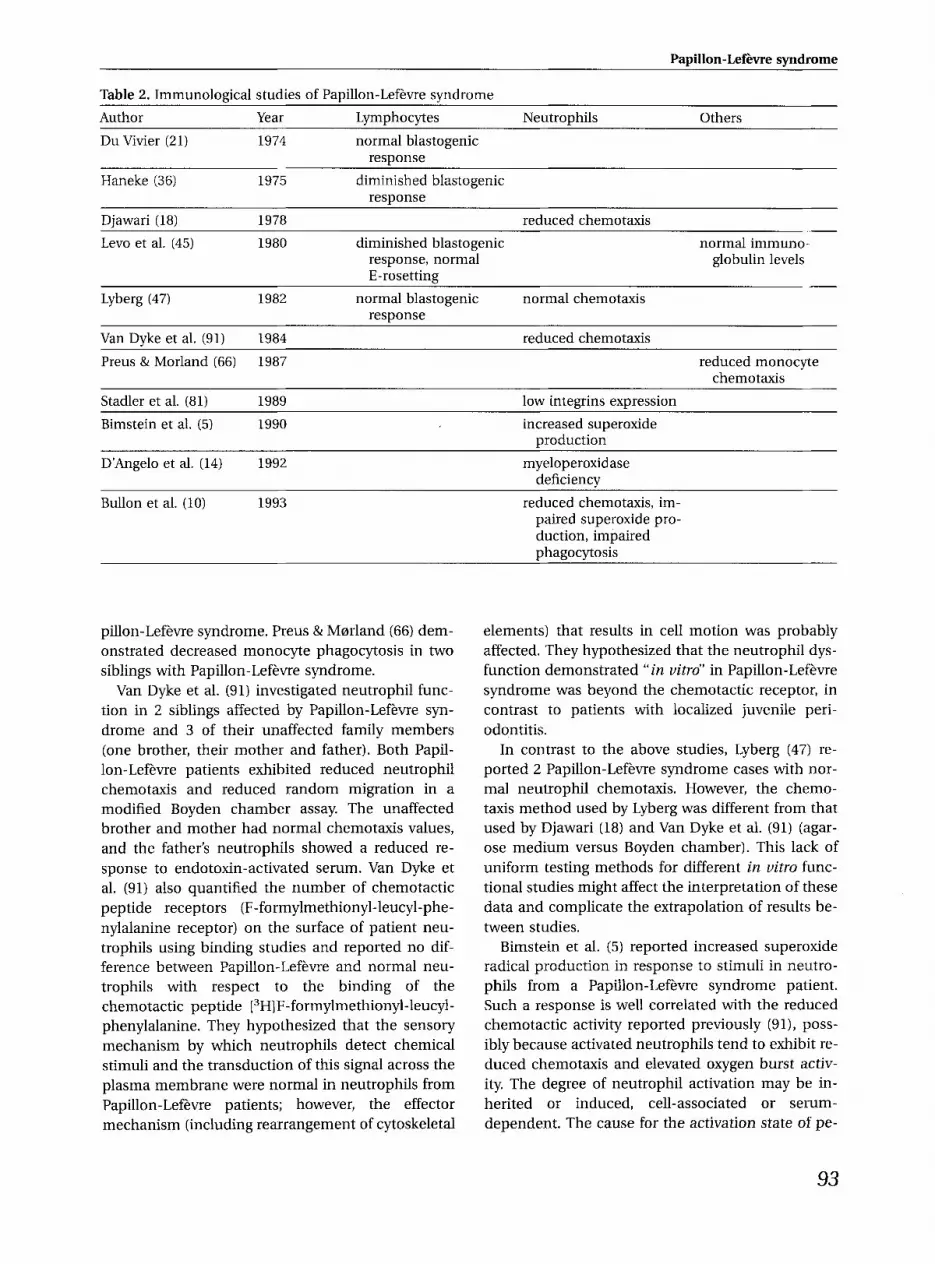
An increased susceptibility to generalized infections has been reported for both Papillon-Lefevre and Haim-Munk patients. Infections include furuncu- losis, pyoderma, liver abscesses, spastic bronchitis, phlyctenular conjunctivitis, tonsillitis, exudative ec- zema and pneumonia (14, 33, 35, 36). This increased incidence of infections led investigators to hypoth- esize that an underlying immune disorder is an im- portant primary or secondary etiological factor in predisposing Papillon-Lefevre patients to peri- odontitis. Unfortunately, because Papillon-Lefevre syndrome is uncommon, laboratory studies to date comprise assorted case reports. These are summar- ized in Table 2.
Laboratory evaluations of lymphocyte function
Du Vivier (21) reported normal lymphocyte blasto- genic activity in a 3-year-old patient with no history of increased susceptibility to infection. In contrast, Haneke et al. (36) and Vrahopoulos et al. (93) dem- onstrated a cellular immune defect with decreased phytohemagglutinin-induced mitogenic activity of lymphocytes in individuals with Papillon-Lefevre syndrome who exhibited multiple infections.
Levo et al. (45) investigated the possibility of an immune disorder associated with the Haim-Munk variant of Papillon-Lefevre syndrome. They studied 23 members of 4 related families, including 11 pa- tients and 12 healthy individuals. The E-rosetting ability of T-lymphocytes was normal in all except 2 of the 11 affected individuals and 1 of the 12 unaffected family members examined. However, lymphocyte proliferation data from these individuals suggested that the patients as well as their family members ex-
hibit diminished responsiveness to B and T cell mitogens. The lymphocyte response in patients affected by Haim-Munk was much lower than in their unaffected siblings and parents, and yet half of the latter also exhibited an abnormal mitogenic response. These results suggest that the observed al- tered lymphocyte functions are not secondary to the clinical manifestations of the disease. Excluding periodontitis, no evidence of in uiuo deficiency fol- lowed by recurrent infections could be demonstrated in these patients. Lyberg (47) did not find any devi- ation from the normal values of lymphocyte trans- formation in 2 Papillon-Lefevre patients. Differences in laboratory methods might account for the differ- ence in results. Lev0 et al. (45) reported that the mitogenic defect is demonstrated more clearly in ex- perimental conditions of suboptimal concentrations of mitogen for 3 days of incubation, which was dif- ferent from experimental conditions used in the Ly- berg study.
Recently, Celenligil et al. (11) studied lymphocyte subpopulations in periodontal lesions of a Papillon- Lefevre patient. Their findings were not different from other forms of early-onset periodontitis. The periodontal lesions they examined were dominated by plasma cells, and an increased number of natural killer cells were found in the circulation. These find- ings suggest that the etiology of the periodontal de- struction in Papillon-Lefevre syndrome may be simi- lar to that described for other periodontal diseases.
Neutrophil functions
Studies of host response in periodontal diseases have pointed clearly to the neutrophil as the key pro- tective cell that, under normal circumstances, limits the pathology caused by periodontal organisms (27). Neutrophil chemotaxis, phagocytosis and killing have been evaluated in Papillon-Lefevre patients. Djawari (18) assessed neutrophil function in a 5- year-old patient previously described by Haneke (36). His results demonstrated reduced in uitro chemotactic activity (about 50%) in a modified Boyden chamber assay compared with 50 healthy in- dividuals. This patients’ neutrophils also demon- strated decreased phagocytosis and intracellular kill- ing of Staphylococcus aureus. Although phagocytosis of Candida albicans was close to normal, the ability of neutrophils to kill this Candida was decreased. Djawari (18) hypothesized that a combination of de- fective neutrophil function and diminished lympho- cyte capacity to respond to stimulation may be the basis of increased susceptibility to infections in Pa-
92
Papillon-Lefhvre syndrome
Table 2. Immunological studies of Papillon-Lefkvre syndrome Author Year Lymphocytes Neutrophils Others Du Vivier (21) 1974 normal blastogenic
pillon-Lefkvre syndrome. Preus & Msrland (66) dem- onstrated decreased monocyte phagocytosis in two siblings with Papillon-Lefkvre syndrome.
Van Dyke et al. (91) investigated neutrophil func- tion in 2 siblings affected by Papillon-Lefkvre syn- drome and 3 of their unaffected family members (one brother, their mother and father). Both Papil- lon-Lefkvre patients exhibited reduced neutrophil chemotaxis and reduced random migration in a modified Boyden chamber assay. The unaffected brother and mother had normal chemotaxis values, and the father’s neutrophils showed a reduced re- sponse to endotoxin-activated serum. Van Dyke et al. (91) also quantified the number of chemotactic peptide receptors (F-formylmethionyl-leucyl-phe- nylalanine receptor) on the surface of patient neu- trophils using binding studies and reported no dif- ference between Papillon-Lefkvre and normal neu- trophils with respect to the binding of the chemotactic peptide [3H]F-formylmethionyl-leucyl- phenylalanine. They hypothesized that the sensory mechanism by which neutrophils detect chemical stimuli and the transduction of this signal across the plasma membrane were normal in neutrophils from Papillon-Lefcvre patients; however, the effector mechanism (including rearrangement of cytoskeletal
elements) that results in cell motion was probably affected. They hypothesized that the neutrophil dys- function demonstrated “in vitro” in Papillon-Lefkvre syndrome was beyond the chemotactic receptor, in contrast to patients with localized juvenile peri- odontitis.
In contrast to the above studies, Lyberg (47) re- ported 2 Papillon-Lefkvre syndrome cases with nor- mal neutrophil chemotaxis. However, the chemo- taxis method used by Lyberg was different from that used by Djawari (18) and Van Dyke et al. (91) (agar- ose medium versus Boyden chamber). This lack of uniform testing methods for different in vitro func- tional studies might affect the interpretation of these data and complicate the extrapolation of results be- tween studies.
Bimstein et al. (5) reported increased superoxide radical production in response to stimuli in neutro- phils from a Papillon-Lefkvre syndrome patient. Such a response is well correlated with the reduced chemotactic activity reported previously (91), poss- ibly because activated neutrophils tend to exhibit re- duced chemotaxis and elevated oxygen burst activ- ity. The degree of neutrophil activation may be in- herited or induced, cell-associated or serum- dependent. The cause for the activation state of pe-
93
Hart & Shapira
ripheral blood neutrophils in Papillon-Lefevre syn- drome patients needs to be investigated further. Bul- lon et al. (10) recently reported that neutrophil chemotaxis, superoxide radical production and phagocytosis were impaired in 2 sisters affected by Papillon-Lefevre syndrome. An orally asymptomatic but dermatologically affected brother showed no sig- nificant defect in phagocytic activity and superoxide radical production. After scaling and root planing, the periodontal lesions progressed; however, neutro- phi1 functions were reported to be normal in both sisters.
Stadler et al. (82, 83) studied 2 Papillon-Lefkvre syndrome patients with recurrent infections over a 10-year period. Initially, neutrophils from these pa- tients demonstrated reduced chemotactic activity. Seven years later, without treatment, the recurrent infections and hyperkeratosis spontaneously re- gressed and no neutrophil chemotactic defect could be demonstrated. Expression of molecules on the neutrophil membrane that function in cell-cell and cell-matrix adhesion (integrins) were also studied. The expression of integrins from the CD11 /CD18 family on patients’ neutrophils were normal, but after stimulation with the chemotactic peptide F-formylmethionyl-leucyl-phenylalanine, integrin expression did not increase as in control subjects. D’Angelo et al. (14) studied a Papillon- Lefevre syndrome patient with increased suscepti- bility to infection and found that her neutrophils show reduced chemotaxis and reduced myeloper- oxidase activity.
Immunoglobulin levels
Lev0 et al. (45) reported normal immunoglobulin G (IgG), IgA and IgM levels in Papillon-Lefevre syn- drome patients and in unaffected family members, with no evidence of autoantibodies. Van Dyke et al. (91) reported elevated serum IgG levels in 1 of 2 sib- lings with Papillon-Lefkvre syndrome. The other affected sibling and 3 unaffected family members had normal serum IgG levels. Although no definitive conclusion can be made based on these 2 case studies, total immunoglobulin levels do not appear to be important in the pathogenesis of Papillon- Lefevre syndrome.
Microbiological findings
Early studies that examined plaque samples from Papillon-Lefevre syndrome patients by scanning
electron microscopy and culture techniques found a bacterial flora consistent with adult periodontitis (41, 53). In the 1980s, more sophisticated culture systems and identification techniques became available for characterization of the periodontal flora. Van Dyke et al. (91) reported the cultivable flora and serum antibody levels for periodontal pathogens in a family with 2 Papillon-Lefevre sib- lings. Three unaffected family members did not demonstrate elevated antibody levels to any of the periodontal pathogens compared with controls. However, the 2 Papillon-Lefevre syndrome siblings showed increased antibody levels to Actinobacillus actinomycetemcomitans in several tests over a 3- year period. Salivary IgA levels gave a similar pat- tern of results. Microbial plaque samples from each of the two Papillon-Lefkvre patients harbored simi- lar species before therapy, and A. actinomycetem- comitans, Haemophilus aphrophilus and Prevotella intermedia comprised more than 50% of the iso- lates in each of the periodontitis sites. The dom- inance of A. actinomycetemcomitans in peri- odontitis-affected sites and high serum titer levels to A. actinomycetemcomitans in individuals affected by Papillon-Lefkvre syndrome were also described by several other laboratories (5, 65, 90). In contrast, D’Angelo et al. (14) did not find A. actinomycetem- comitans in a case of Papillon-Lefevre syndrome, but did find a dominance of black-pigmented an- aerobic rods and Fusobacterium, which are also putative periodontal pathogens found in early- onset periodontal diseases. Shtavholtz et al. (77) examined the levels of serum antibodies to the A. actinomycetemcomitans leukotoxin in Haim-Munk patients and unaffected family members (84, 89). Their results did not demonstrate any difference between anti-leukotoxin levels of affected and un- affected patients. This finding suggests no differ- ence in exposure to leukotoxin-bearing strains of A. actinomycetemcomitans between affected and unaf- fected family members.
Etiology
A specific defect in immune responsiveness has not been identified, yet there is evidence to suggest that both a specific pathogen, A. actinomycetemcomitans, and an underlying diathesis are important in the de- velopment of periodontal attachment loss in Papil- lon-Lefevre syndrome patients (73,971. Papillon- Lefevre syndrome patients may have an increased susceptibility to bacterial infection of the periodon-
94
PaDillon-Lefhe svndrome
tium. The susceptibility factor may involve defective immune cell function or a defective epithelial barrier or may affect both aspects due to a pleiotropic effect of a single mutant gene. Either type of defect could lead to an increased susceptibility to bacterial infec- tion in the gingival crevice.
Perhaps the most reasonable hypothesis sup- ported by clinical and laboratory studies is that pro- posed by Preus (641, who noted that, although there seems to be a heritable component inducing the de- fects in the host defense of Papillon-Lefkvre syn- drome patients, it appears that at least Preus’ pa- tients must have an infection with specific virulent bacteria like A. actinomycetemcomitans to develop the periodontal component of the syndrome. Preus speculated that the hereditary defect in Papillon- Lefhvre syndrome is located at the epithelial surface barrier. The junctional epithelium is development- ally unique (74), and thus an epithelial defect could manifest itself in a unique manner in this tissue. This may lead to a reduced defense against virulent peri- odontopathogens, resulting in severe periodontal destruction. If however, the patient is not infected by such bacteria, they may avoid periodontal destruc- tion, and their disease will be diagnosed as the more common Meleda’s disease (64).
Paghdiwala (57) felt that any attempt to identify an etiological factor for the Papillon-Lefkvre syn- drome should consider whether the main features of this disease result from different manifestations of the same causative factor or from manifestations of different causative factors acting concomitantly. He felt the skin and periodontal manifestations are manifestations of an adverse reaction to pressure, or a premature aging on the part of some structural component of the skin and periodontium. Several structural defects have been suggested, including defects of cementum (80, 93), gingival epithelium (32, 47, 75) and a functional imbalance of colla- genolytic activity in the periodontal ligament (76). There are also data to suggest that there may be an aberration in the epithelium. Aso et al. (1) demon- strated an absence of a 64-kDa keratin and a signifi- cant increase in a 56- to 58-kDa keratin in the plan- tar corneum of a Papillon-Lefkvre syndrome patient compared with healthy controls. Following retinoid therapy, the 64 kDa keratin appeared in the corne- um. These findings suggest that abnormal keratiniz- ation may underlie the Papillon-Lefhvre syndrome defect. These findings lend support to the hypothesis proposed by Preus (641, that the periodontal com- ponent hitherto described as an obligatory symptom of Papillon-Lefkvre syndrome may be a casual phen-
omenon. The normally protective epithelial barrier may be compromised in the Papillon-Lefevre pa- tient, permitting opportunistic infection by virulent bacteria such as A. actinomycetemcomitans, which may, by virtue of its virulence factors, locally over- whelm the immune response and cause severe peri- odontitis.
Traditional efforts to treat Papillon-Lefkvre syn- drome have been directed either to reducing the hyperkeratotic skin lesions or to halting the peri- odontal destruction. Typically, dermatologists have attempted the former and dentists the latter. Treat- ment for these two different clinical manifestations of Papillon-Lefevre syndrome was influenced and di- rected by the discipline of the health care provider. In general, prior to 1980, treatment of the skin and periodontal manifestations associated with Papillon- Lefhvre syndrome were ineffective (35).
Dermatological treatment
Treatment of disorders of palmoplantar keratiniz- ation remained unsatisfactory for decades. The use of lubricants, keratolytic agents, steroids and topical salicylic acid in different concentrations and in pro- pylene glycol with or without occlusion was the mainstay of treatment until the discovery of oral retinoids (22). The therapeutic effect of these former treatments was minimal. Synthetic retinoids are ana- logs of vitamin A that have proven effective in the treatment of a number of keratinizing disorders (16, 49, 56, 61, 85, 88) and were tried empirically in Papil- lon-Lefkvre patients. A beneficial effect has been re- ported following the administration of several syn- thetic retinoids, including etretinate (8, 19, 20, 42, 50, 95), isotretinoin (54) and acitretin (78).
Experimental protocols with the use of etretinate were found to successfully resolve the skin lesions of Papillon-Lefkvre patients (19, 22, 50, 54). Unfortu- nately, etretinate therapy is not without compli- cations. Adverse side effects may include dryness of lips, mild pruritis, transient hair loss, elevated serum triglycerides and liver enzymes, hypervitaminosis A, teratogenicity and liver toxicity (4). There have also been reports of osseous changes in patients treated with etretinate (17, 30, 79). Others have found no osseous changes (42). Tosti et al. (87) reported that a Papillon-Lefevre patient developed liver abscesses caused by pyogenic bacteria and a subphrenic ab- scess after beginning etretinate therapy, and another
95
Hart & Shapka
patient even died from uncontrolled infection (8). The life-threatening risk of etretinate therapy makes this approach of treating Papillon-Lefevre syndrome questionable. Etretinate is stored in adipose tissues and the elimination is very slow, with a half-life of 80 days (7, 60). Because of etretinate’s teratogenic potential and long-term retention in the body, pa- tients should not become pregnant for at least l year after taking the drug (4).
Acitretin is the free acid of etretinate and its main metabolite. Clinical studies of acitretin indicate that it is an effective therapy in disorders of keratiniz- ation. The results with acitretin have generally been better than with etretinate (6, 25, 49, 56, 61, 85). The superiority of acitretin over etretinate lies mainly in its low propensity for storage and its short elimin- ation time from the body. Acitretin is not stored in adipose tissue. Pharmacokinetic studies have indi- cated that the elimination half-life of acitretin in humans is 2 days compared with 80 days for etretin- ate. Due to the teratogenicity of retinoids, Nazzaro et al. (52) pointed out the advantage of acitretin for women who may become pregnant shortly after dis- continuing drug treatment. Acitretin increases the cellular retinoic acid-binding proteins in humans (78) and may exert its pharmacological effect by in- teracting with the natural retinoic acid-binding pro- tein. Side effects relating to long-term acitretin treat- ment may include hyperostoses (17) and severe skel- etal changes (79). However, no longitudinal study has been conducted, and knowledge has accumu- lated slowly from case reports.
Nazzaro et al. reported successful dermal and dental treatment using orally administered acitretin (52). They treated 4 siblings affected with Papillon- Lefevre syndrome who ranged in age from 2 to 11 years. Treatment was continued for 16 months, with patients seen monthly for clinical examination. After 16 months of treatment, the skin lesions were ab- sent, and new teeth that erupted during the course of treatment were reportedly free of periodontitis. The onIy reported side effect was moderate cheilitis. Light microscopy following 2 months of treatment revealed a marked reduction in hyperkeratosis. The parakeratosis disappeared completely, and a con- tinuous granular layer could be observed. Ultrastruc- turally, the most notable change was the marked re- duction in the number of lipid-like vacuoles ob- served before treatment in the horny and granular layers. An increased number of tonofilaments was also noted, and the keratohyaline formed normally shaped granules (52). Blanchet-Bardon et al. (6) also reported complete remission of skin lesions after 4
months of acitretin treatment in 3 unrelated Papil- lon-Lefevre patients.
Periodontal therapy
Conventional periodontal treatment of periodontitis associated with Papillon-Lefevre syndrome has been generally unsuccessful, and prior to 1980, tooth loss was believed to be an inevitable sequela of Papillon- Lefkvre syndrome (35, 44, 72). Therefore, treatment generally consisted of early tooth extraction for pre- vention of vertical alveolar bone loss followed by construction of dentures (29).
With the development of techniques for identify- ing periodontal pathogens and the ability to monitor patients before and after therapy, clinicians started to evaluate specific protocols for treating the peri- odontal component of Papillon-Lefkvre syndrome. Van Dyke et al. (91) reported the treatment of 2 pa- tients with periodontal surgery and administration of tetracycline for 3 weeks postoperatively. The anti- biotic course was repeated in the maintenance phase, but the periodontium continued to deterio- rate. Lu et al. (46) report a Papillon-Lefkvre patient who did not respond to conventional periodontal therapy that included extraction of hopeless teeth, pocket reduction surgery, chlorhexidine digluconate mouth rinse and systemic tetracycline therapy for 1 month. The periodontal condition continued to de- teriorate, and 6 months later hopeless teeth were ex- tracted. Vital root submersion procedures were per- formed on the 8 remaining teeth, with the goal of eliminating the dentogingival junction and main- taining the height of the alveolar ridges. Bullon et al. (10) were unsuccessful in treating a 12-year-old girl with biweekly scaling and root planing, oral tetracy- cline and subgingival irrigation with chlorhexidine digluconate. Due to a lack of response to treatment, the antibiotic was changed to amoxicillin with clavu- lanic acid. This treatment was repeated at regular in- tervals, but after 22 months without favorable re- sponse, the permanent teeth were extracted. This patient’s older sister also showed no response to similar treatment that included periodontal surgical flap procedures, and her teeth were also extracted.
Preus (65) reported the successful periodontal management of 2 cases following a rigorous regimen of oral hygiene, antibiotic coverage and extraction of periodontally involved teeth. Tetracycline treatment was continuous for 2.5 years. A meticulous oral hy- giene program included parental involvement, week- ly professional tooth cleaning and chlorhexidine di- gluconate mouth rinses twice a day. The remaining
Papillon-Lef&vre syndrome
periodontally involved teeth were extracted under supplemental antibiotic coverage. The presumed A. actinomycetemcomitans reservoir (family dog) re- ceived metronidazole and spiramycin treatment for 14 days (67). The maintenance phase consisted of weekly professional tooth cleaning and monthly monitoring for A. actinomycetemcomitans. The 2 pa- tients were free of periodontitis by clinical and radio- logical examination but still showed elevated serum antibody titers against A. actinomycetemcomitans. The peripheral blood monocytes of these Papillon- Lefevre patients had regained their normal phago- cytic capacity as compared with age-matched con- trols (64). Teeth with no periodontal involvement at the start of the continuous tetracycline therapy and teeth that erupted during the study period remained unaffected. Preus et al. suggested that the combi- nation of careful plaque control, periodontal surgery, antibiotic therapy and A. actinomycetemcomitans monitoring was important in successful therapy (64).
Umeda et al. (90) included microbial monitoring in the treatment of 2 Papillon-LefCvre cases. In one patient, extraction of the deciduous dentition was able to eliminate A. actinomycetemcomitans and the permanent teeth erupted uneventfully. In the second case, conventional periodontal therapy with admin- istration of minocycline and erythromycin was un- able to eliminate A. actinomycetemcomitans. Admin- istration of ofloxacin suppressed A. actinomycetem- comitans and resulted in a reduction of gingival inflammation and pocket depth.
A treatment protocol reported by D’Angelo et al. (14) included extraction of the primary dentition prior to the eruption of the permanent teeth, daily irrigation with chlorhexidine and weekly pro- fessional plaque control. A. actinomycetemcomitans could not be cultured, but black-pigmented anaer- obic rods and Fusobacterium were present. At age 6.5 years, the permanent dentition was reported to be clinically healthy, and radiographs revealed no evidence of periodontal pathology (14). Further fol- low-up of this patient would be helpful to evaluate this treatment. Tinanoff et al. (86) followed a Papil- lon-Lefevre case for 15 years and reported that suc- cessful therapy was possible with the use of systemic antibiotics. They suggested that an edentulous period between the periodontally diseased mixed dentition and the eruption of the remaining teeth along with systemic antimicrobial therapy appear to be the key elements of the treatment of the peri- odontal component of Papillon-Lefevre syndrome.
The literature contains few reports of traditional periodontal treatment modalities used in conjunc-
tion with dermal treatments such as oral retinoids. Unfortunately, most of the few reports available did not use standardized periodontal indices to evaluate treatment results. Driban & Jung (19) reported suc- cessful dermatological and periodontal maintenance of a 5-year-old girl with Papillon-Lefevre syndrome. A treatment regimen of a biweekly oral hygiene pro- gram, systemic antibiotics and etretinate improved the gingival status and stabilized the periodontal condition. Morishima et al. (50) treated an 8-year- old with etretinate for 14 months and reported no exfoliation of additional teeth. Long-term preser- vation of permanent teeth in a Papillon-LefGvre pa- tient treated with etretinate was also reported by Gelmetti et al. (26). Kellum (42) reported a 9-year evaluation of 4 Papillon-Lefevre siblings treated with etretinate. Two individuals did retain substantial numbers of teeth at the time of the report, when they were in their early twenties. Whether retention of teeth may be attributed to treatment with etretin- ate is unknown. No evidence of continuing gingival inflammation was reported in any of the siblings after discontinuation of the drug when the youngest sibling was 14 years old. Haneke postulated a re- duced expulsion of teeth after age 16-18 years (35), but it can only be speculated that, if the permanent dentition can be retained in reasonable periodontal health to this age, successful management of the dentition may be a realistic goal. It is interesting to note that the third molars are often reported to be spared periodontal destruction in Papillon-Lefcvre syndrome, possibly because they are not in direct contact with the oral environment during this criti- cal time period. Nazzaro et al. (52) reported success- ful dermatological and periodontal treatment in 4 siblings affected by Papillon-Lefbre syndrome using acitretin. During 16 months of treatment, these pa- tients were seen monthly for examination only. Gin- gival inflammation was gradually reduced and was almost completely resolved after 2 months. New teeth that erupted during the course of treatment were reportedly free of periodontitis, and radio- graphic evaluation revealed no new alveolar bone loss.
Recent data suggests that mechanical debride- ment in conjunction with antibacterial therapy may be successful in periodontal management of Papil- lon-Lefevre syndrome, particularly if administered early. Bacterial monitoring seems to be an important part of treatment follow-up. Most of the reported cases described A. actinomycetemcomitans as the major pathogen. Treatment should be aggressively directed against this specific pathogen when it is
97
Hart & ShaDira
identified. However, non-A. actinomyceterncomitans cases of Papillon-Lefkvre syndrome also appear to exist. Incorporation of periodontal indices into the evaluation of treatment protocols using synthetic retinoids is necessary to determine whether patients with Papillon-Lefkvre syndrome can have a healthy periodontium at the adult age, provided the treat- ment is started before the onset of permanent teeth eruption.
Conclusion
Successful periodontal management of Papillon- Lefevre syndrome patients remains challenging. However, as our understanding of the etiological fac- tors important in Papillon-Lefgvre syndrome in- creases, we can hope that successful treatment strat- egies will be developed. Dental management of Papillon-Lefevre syndrome is still under study. Two promising approaches have been documented, one aimed at eradication of A. actinomycetemcomitans and another using synthetic retinoids. In both cases, several investigators claim to have arrested the course of periodontal breakdown in a few cases, a result considered unobtainable until recently (73).
Acknowledgements
We would like to thank Pat Ragusa for the photo- graphs and Kimberly Ladley for preparing this manuscript. This work was supported in part by grant DE 10563.
References
1. Aso K, Shimoura T, Katagata Y. Abnormal 64 and 58-56 KD keratin in Papillon-Lefevre syndrome; its recovery following the normalization of lesions after retinoid therapy. Jpn Dermatol 1987: 97: 991-997.
2. Bach IN, Levan NE. Papillon-Lefkvre syndrome. Arch Dermatol 1968: 97: 154-158.
3. Bergman R, Friedman-Birnbaum R. Papillon-Lefevre syn- drome: a study of the long-term clinical course of recurrent pyogenic infections and the effects of etretinate treatment. Br J Dermatol 1988: 119: 731-736.
ant A. Acitretin in the treatment of severe disorders of kera- tinization. J Am Acad Dermatol 1991: 24: 982-986.
7. Bollag W. New retinoids with potential use in humans. In: Saurat JH, ed. Retinoids: new trends in research and ther- apy. New York Karger, 1985: 289-292.
8. Bravo-Piris J, Aparicio M, Moran M, Armijo M. Papillon- Lefivre syndrome: report of a case treated with oral retin- oid RO 10-9359. Dermatologica 1983: 166: 97-103.
9. Brownstein MM, Skolnik P. Papillon-Lefevre syndrome. Arch Dermatol 1972: 106: 533-534.
10. Bullon P, Pascual A, Fernandez-Novoa MC, Borobio MV, Muniain MA, Camacho F. Late onset Papillon-Lefkvre syn- drome? A chromosomic, neutrophil function and micro- biological study. J Clin Periodontol 1993: 20: 662-667.
11. Celenligil H, Kansu E, Ruacan S, Eratalay K. Papillon- Lefkvre syndrome. Characterization of peripheral blood and gingival lymphocytes with monoclonal antibodies. J Clin Periodontol 1992: 19: 392-397.
12. Coccia CT, McDonald RE, Mitchell DF. Papillon-Lefkvre syndrome: precocious periodontosis with palmar-plantar hyperkeratosis. J Periodontol 1966: 37: 408-414.
13. Corson EF. Keratosis palmaris et plantaris with dental alter- nation. Arch Dermatol Syphilis 1939: 40: 639.
14. D’Angelo M, Margiotti V, Ammatuna r: Sammartano E Treatment of prepubertal periodontitis. A case report and discussion. J Clin Periodontol 1992: 19: 214-219.
15. Dekker G, Jansen LH. Periodontosis in a child with hyper- keratosis palmo-plantares. J Periodontol 1958: 29: 266-271.
16. Dicken CH. Retinoids: a review. J Am Acad Dermatol 1984:
17. DiGiovanna JJ, Gerber LN, Helfgott G, Gantt GL. Ligamen- tous calcification and bony spurring after chronic etretin- ate therapy, abstract. J Invest Dermatol 1986: 86: 471.
18. Djawari D. Deficient phagocytic function in Papillon- Lefevre syndrome. Dermatologica 1978: 156: 189-192.
19. Driban NE, Jung JR. Papillon-Lefkvre syndrome. A clinical and therapeutical contribution. Dermatologica 1982: 165:
20. Driban NE, Jung JR. Treatment of Papillon-Lefevre syn- drome with etretinate. J Am Acad Dermatol 1988: 18: 583- 584.
21. Du Vivier A. Papillon-Lefkvre syndrome. Proc R SOC Med
22. El Darouti MA, Al Raubaie SM, Eiada MA. Papillon-Lefkvre syndrome. Successful treatment with oral retinoids in three patients. Int J Dermatol 1988: 27: 63-66.
23. Gauba ML. Periodontosis - a case report of an eight year- old suffering from advanced periodontosis. J All India Dent
24. Gedda L, Pignatelli A. Cheratosi palmo-plantare e allotopa associata a grave malattia dentaria in due fratelli mononati. Acta Genet Med Gemellol (Roma) 1954: 3: 133-142.
26. Gelmetti C, Nazzaro V, Cerri D, Fracasso L. Long-term pres- ervation of permanent teeth in a patient with Papillon- Lefgvre syndrome treated with etretinate. Pediatr Dermatol
27. Genco RJ, Van Dyke TE, Levine MJ, Nelson RD, Wilson ME. Molecular factors influencing neutrophil defects in peri- odontal disease. J Dent Res 1986: 65: 1379-1391.
28. Ghandour I. Hyperkeratosis palmoplantaris with prema-
11: 541-542.
653-659.
1974: 67: 440-441.
ASSOC 1960: 32: 131-133.
176: 182-190.
1989: 6: 222-225.
98
Papillon-Lefkvre syndrome
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
ture periodontal destruction (Papillon-Lefevre syndrome) - report of two cases. East Afr Med J 1989: 66: 615-619. Giansanti JS, Hrabak RP, Waldron CA. Palmar plantar hy- perkeratosis and concomitant periodontal destruction (Pa- pillon-Lefkvre syndrome). Oral Surg Oral Med Oral Pathol
Gluck S, Melnick B, Goerz G. Retrospective evaluation of skeletal radiographic changes after long-term etretinate therapy. J Invest Dermatol 1986: 86: 326 (abstr). Gorlin RJ, Cohen MM Jr., Levin LS. Syndromes of the head and neck. 3rd edn. New York Oxford University Press, 1990: 853-854 (Oxford Monographs on Medical Genetics, No. 19). Gorlin RJ, Sedano H, Anderson VE. The syndrome of pal- mar-plantar hyperkeratosis and premature periodontal de- struction of the teeth. J Pediatr 1964: 65: 895-908. Haim S, Munk J. Keratosis palmo-plantaris congenita, with periodontosis, arachnodactyly and a peculiar deformity of the terminal phalanges. Br J Dermatol 1965: 77: 42-54. Hall RK. Papillon-Lefevre syndrome. Aust Dent J 1963: 8:
Haneke E. The Papillon-Lefkvre syndrome: keratosis palmo- plantaris with periodontopathy: report of a case and review of the cases in the literature. Hum Genet 1979: 51: 1-35. Haneke E, Hornstein OP, Lex C. Increased susceptibility to infections in Papillon-Lefkvre syndrome. Dermatologica
Hathway R. Papillon-Lefevre syndrome. Br Dent J 1982:
Hawes RR. Report of three patients experiencing juvenile periodontosis and early loss of teeth. J Dent Child 1960: 26: 3 17-3 19. Ingle JI. Papillon-Lefkvre syndrome: precocious peri- odontitis with associated epidermal lesions. J Periodontol
Jansen LH, Dekker G. Hyperkeratosis palmo-plantaris with periodontosis (Papillon-Lefkvre). Dermatologica 1956: 113:
Jung J, Carranza FA, Newman MG. Scanning electron- microscopy of plaque in Papillon-Lefkvre syndrome. J Peri- odontol 1981: 52: 442-446. Kellum RE. Papillon-Lefkvre syndrome in four siblings treated with etretinate. A nine-year evaluation. Int J Dermatol 1989: 28: 605-608. Kohler JA. Parodontopathie jugendlicher und keratoma palmare und plantare. Forum Paradontol 1953: 3: 885-898. Krebs A. Papillon-Lefkvre syndrome. Dermatologica 1978:
Lev0 Y, Wollner S, Hacham-Zadeh S. Immunological study of patients with Papillon-Lefevre syndrome. Clin Exp Im- munol 1980: 40: 407-410. Lu Jackson H-K, Lin C-T, Kwan H-W. Treatment of a patient with Papillon-Lefivre syndrome. A case report. J Peri- odontol 1987: 58: 789-793. Lyberg T. Immunological and metabolical studies in two siblings with Papillon-Lefkvre syndrome. J Periodont Res
Manuzzi P, Costa AM. Sindrome di Papillon-Lefkvre evolu- zione spontanea e terapeuticamente indotta, in 2 casi clinici. G Ital Dermatol Venereol 1987: 123: 229-231. Marks R, Finlay AY, Holt PJ. Severe disorders of keratiniz- ation; effects of treatment with Tigason (etretinate). Br J Dermatol 1981: 104: 667-673. Morishima T, Higaki M, Maeda T. A case of an infant with
1973: 36: 40-48.
185-188.
1975: 150: 283-286.
153: 370-371.
1959: 30: 230-237.
207-219.
156: 59-63.
1982: 17: 563-568.
Papillon-Lefevre syndrome successfully treated with oral administration of etretinate: pharmacokinetics of etretinate (Ro 10-9359) and its main metabolite (Ro 10-1670). J Pedi- atr Dermatol 1983: 2: 255-260.
51. Moynahan EJ, Cross GW. Hyperkeratosis of palms and soles and “periodontosis” (Papillon-Lefgvre syndrome). Proc R SOC Med 1960: 53: 565.
52. Nazzaro V, Blanchet-Bardon C, Mimoz C, Revuz I, Puissant A. Papillon-Lefkvre syndrome. Ultrastructural study and successful treatment with acitretin. Arch Dermatol 1988:
53. Newman M, Angel I, Karge H, Weiner M, Grinenko V, Schusterman L. Bacterial studies of the Papillon-Lefkvre syndrome. J Dent Res 1977: 56: 545-546.
54. Nguyen TQ, Greer KE, Fisher GB Jr, Cooper PH. Papillon- Lefivre syndrome: report of two patients treated success- fully with isotretinoin. J Am Acad Dermatol 1986: 15: 46- 49.
55. Nouel AA, Jacobo M, Bogaert H. Sindrome de Papillon- Lefkvre. Hiperqueratosis palmo-plantar con periodontosis. Rev Dominicana Dermatol 1970: 4: 25-37.
56. Orfanos CE. Retinoids in clinical dermatology. An update. In: Saurat JH, ed. Retinoids: new trends in research and therapy. Basel: Karger, 1984: 314-334.
57. Paghdiwala AF. Papillon-Lefkvre syndrome. A case report. J Periodontol 1980: 51: 594-598.
58. Papillon MM, et Lefkvre €? Deux cas de keratodermie pal- maire et plantaire symktrique familiale (maladie de Mele- da) chez le frere et la soeur. Coexistence dans les deus cas d’altkrations dentaires grabes. Bull SOC Fr Dermatol Syph- ilis 1924: 31: 82-87.
59. Pareek SS, Al-Aska AK. Papillon-Lefkvre syndrome. A report of six cases in one family. Int J Dermatol 1986: 25: 638-641.
60. Parravicini U, Camenzind M, Gower M. Multiple dose phar- macokinetics of Ro 10-1670, the main metabolite of etretinate (Tigason). In: Saurat JH, ed. Retinoids: new trends in research and therapy. New York Karger, 1985:
61. Peck GL, DiGiovanna JJ. Retinoids. In: Fitzpatrick TB, Eisen Z, Wolff K, ed. Dermatology in general medicine. 3rd edn. New York: McGraw-Hill, 1987: 2582-2609.
62. Perry HO. Papillon-Lefkvre syndrome, Case presentation, Minnesota Dermatological Society Meeting, Mayo Clinic, Rochester, Minnesota, September 1963.
63. Pomposiello IM, Calandra R. Queratodermia palmoplantar con paradentosis (Papillon-Lefevre), Arch Argent Dermatol 1961: 11: 385-393.
64. Preus HR. Rapidly destructive periodontitis of Papillon- Lefkvre syndrome. Results of treatment based on labora- tory and clinical observations of two cases. J Clin Peri- odontol 1988: 15: 639-643.
65. Preus H, Gjermo E Clinical management of prepubertal periodontitis in two siblings with Papillon-Lefkvre syn- drome. J Clin Periodontol 1987: 14: 156-160.
66. Preus HR, Morland B. In vitro studies of monocyte function in two siblings with Papillon-Lefkvre syndrome. Scand J Dent Res 1987: 95: 59-64.
67. Preus HR, Olsen I. Possible transmittance of A. actinomyce- temcomituns from a dog to a child suffering from rapidly destructive periodontitis. J Periodont Res 1988: 23: 68-71.
68. Rainova I. Uber Insufficientia parodontalis (Parodontosis, Amphodontosis) bei Kindern. Dtsch Stomatol 1955: 5: 681- 685.
70. Rateitschak-Pliiss EM, Schroeder HE. History of peri- odontitis in a child with Papillon-Lefkvre syndrome. A case report. J Periodontol 1984: 55: 35-46.
72. Rosenthal SL. Case report. Periodontosis in a child result- ing in exfoliation of the teeth. J Periodontol 1951: 22: 101- 104.
73. Schnyder W. Inherited keratodermas of palms and soles. In: Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg IM, Austen FK, ed. Dermatology in general medicine. New York: McGraw-Hill, 1993: 557-564.
74. Schroeder HE. Marginal periodontium. In: Oral structure biology. New York Thieme Medical Publishers, 1991: 230- 264.
75. Schroeder HE, Seger RA, Keller HU, Rateitschak-Pluss EM. Behavior of neutrophilic granulocytes in a case of Papillon- Lefevre syndrome. J Clin Periodontol 1983: 10: 618-635.
76. Shoshan S, Finkelstein S, Rosenzweig KA. Disc electrophor- etic pattern of gingival collagen isolated from a patient with palmo plantar hyperkeratosis. J Periodontol Res 1970:
77. Shtavholtz A, Taichman N, Soskolne A. Occurrence of Actinobacillus actinornyceterncornitans and anti-leukotoxin antibodies in an extended family affected by Papillon- Lefevre syndrome. In preparation.
78. Siegenthaler G, Saurat JH. Therapy with a synthetic retin- oid - (Ro 10-1670) etretin - increases the cellular retinoic acid-binding protein in nonlesional psoriatic skin. J Invest Dermatol 1986: 87: 122-124.
79. Sillevis-Smith JH, DeMari E A serious side effect of etretin- ate (Tigason). Clin Exp Dermatol 1984: 9: 554-556.
80. Smith F: Rosenzeig KA. Seven cases of Papillon-Lefkvre syn- drome. Periodontics 1967: 5: 42-46.
81. Sofaer JA. Genetic approaches in the study of periodontal diseases. J Clin Periodontol 1990: 17: 401-408.
82. Stadler JE Gellard I! Vergracht A, Bignon JD, Dreno B, Li- toux I? Abnormalities in the expression of polymorpho- nuclear adhesion glycoproteins after stimulation in two pa- tients with Papillon-Lefkvre syndrome. Card Grenoble 1988 Proceedings. J Invest Dermatol 1989: 92: 146.
83. Stadler JE Torres M, Taraud D, Hakim J , Delaire J, Barriere H. Anomalies fonctionnelles des polynucleaires dans la maladie de Papillon Lefevre. Nouv Presse Med 1982: 11: 2135-2138.
195-197.
5: 255-258.
84. Taichman NS, Dean RT, Sanderson CJ. Biochemical and morphological characterization of the killing of human monocytes by a leukotoxin derived from Actinobacillus actinornyceterncornitans. Infect Immun 1980: 28: 258-268.
85. Tamayo L, Ruiz-Maldonado R. Long-term follow-up of 30 children under oral retinoid 10-9359. In: Orfanos CE, Braun-Falco 0, Farber EM, ed. Retinoids. New York: Springer-Verlag, 1981: 287-294.
86. Tinanoff N, Tempro PJ, Maderazo EG, Benitez C. Dental treatment of Papillon-Lefevre syndrome: 15 year follow-up. J Dent Res 1993: 72: 183, abstr 640.
87. Tosti A, Manuzzi P, Bardazzi F, Costa A. Is etretinate danger- ous in Papillon-Lefkvre syndrome? Dermatologica 1988:
88. Traupe H, Happle R. Etretinate therapy in children with se- vere keratinization defects. Eur J Pediatr 1985: 143: 166- 169.
89. Tsai CC, McArthur W, Baehni PC, Hammond BE Taichman NS. Extraction and partial characterization of a leukotoxin from a plaque-derived gram-negative microorganism. In- fect Immun 1979: 25: 427-439.
90. Umeda M, Zhang v, Koseki T, Ishikawa I. Clinical, bac- teriological, and immunological examination and treat- ment of two Papillon-Lefevre syndrome patients. J Oral Pathol 1990: 57: 430-440.
91. Van Dyke TE, Taubman MA, Ebersole JL et al. The Papillon- Lefevre syndrome: neutrophil dysfunction with severe peri- odontal disease. Clin Immunol Immunopathol 1984: 31:
92. Vassilopoulou A, Laskaris G. Papillon-Lefkvre syndrome: re- port of two brothers. J Dent Child 1989: 56: 388-391.
93. Vrahopoulos TF: Barber F: Liakoni H, Newman HN. Ultra- structure of the periodontal lesion in a case of Papillon- Lefkvre syndrome (PLS). J Clin Periodontol 1988: 15: 17-26.
94. Wannenmacher E. Umschau auf dem Gebiete der Parade- ntopathien. Zentralbl Gesamte Zahn Mund Kieferheilkd
95. Wehrmann W, Traupe H, Happle R. Papillon-Lefevre syn- drome (Keratosis palmoplantaris mit Periodontopathie): Behandlung mit Etretinat. Hautarzt 1985: 36: 173-175.
96. Woods EC, Wallace WRJ. A case of alveolar atrophy of un- known origin in a child. Am J Orthod Oral Surg 1941: 27:
97. Zambon JJ. Actinobacillus actinornyceterncornitans in hu- man periodontal disease. J Clin Periodontol 1985: 12: 1-20.
98. Ziprkowski L, Ramon Y, Brish M, Hashomer T. Hyperkera- tosis palmoplantaris with periodontosis (Papillon-Lefkvre). Arch Dermatol 1963: 88: 207-209.