Reading performance after implantation of a small-aperture corneal inlay for the surgical correction of presbyopia: Two-year follow-up Alois K. Dexl, MD, MSc, Orang Seyeddain, MD, Wolfgang Riha, MD, Melchior Hohensinn, MD, Wolfgang Hitzl, PhD, MSc, G€ unther Grabner, MD PURPOSE: To evaluate the change in reading-performance parameters after implantation of the Kamra small-aperture intracorneal inlay over a 2-year follow-up. SETTING: University Eye Clinic, Paracelsus Medical University, Salzburg, Austria. DESIGN: Cohort study. METHODS: This study comprised naturally emmetropic presbyopic patients. Bilateral reading acuity, reading distance, reading speed, and the smallest log-scaled sentence were evaluated in a standardized testing procedure using the Salzburg Reading Desk. The minimum postoperative follow-up was 24 months. RESULTS: The study enrolled 32 patients. The reading desk results showed a significant improvement in each parameter tested. After a mean follow-up of 24.2 months G 0.8 (SD), the mean reading distance changed from the preoperative value of 48.1 G 5.5 cm to 38.9 G 6.3 cm (P < .0001), the mean reading acuity at best distance improved from 0.3 G 0.14 logRAD to 0.24 G 0.11 logRAD (P < .000001), and the mean reading speed increased from 142 G 13 words per minute (wpm) to 149 G 17 wpm (PZ.029). One patient lost 1 line, and 1 patient had no change. The improvement was up to 6 log-scaled lines (mean improvement 2.7 G 1.6 lines) in the other 30 patients. CONCLUSIONS: After implantation of the small-aperture intracorneal inlay, there was an improvement in all tested reading performance parameters in emmetropic presbyopic patients; the improvement was the result of an increased depth of field. These 2-year results indicate that the inlay is an effective treatment for presbyopia. Financial Disclosure: Drs. Seyeddain, Riha, Hohensinn, and Hitzl have no financial or proprietary interest in any material or method mentioned. Additional disclosures are found in the footnotes. J Cataract Refract Surg 2011; 37:525–531 Q 2011 ASCRS and ESCRS In recent years, the focus of interest in refractive surgery has clearly shifted toward the correction of presbyopia. The increasing interest is stimulated by the sheer num- ber of potential patients who might seek permanent spectacle-free correction of this condition. This number is projected to increase in the coming decades. Although most presbyopic people use spectacles and contact lenses with a near addition for reading, many extraocu- lar and intraocular surgical procedures have been intro- duced in clinical studies and clinical practice. However, none has emerged as the solution for the perfect correc- tion of presbyopia. The idea of inserting intrastromal corneal implants to correct ametropia was first proposed by J.I. Barraquer in the middle of the 20th century. 1 Other researchers followed his idea by implanting corneal inlays to modify the shape and overall refractive power of the cornea. 2,3 The literature reports many problems with intracorneal implants, including corneal necrosis, epithelial and stro- mal opacification and vascularization, and complica- tions related to decentration and corneal nutrition 4–7 ; thus, few surgeons have adopted this procedure. Advances in femtosecond laser and biomaterial technology, along with a growing demand by informed patients for a reversible presbyopia treatment, has renewed the interest in the implantation of different types of corneal inlays. The Kamra small-aperture intracorneal inlay (for- merly the AcuFocus Corneal Inlay ACI 7000, AcuFocus, Inc.) is currently being investigated in U.S. Food and Q 2011 ASCRS and ESCRS Published by Elsevier Inc. 0886-3350/$ - see front matter 525 doi:10.1016/j.jcrs.2010.10.044 ARTICLE
Transcript
ARTICLE
Reading performan
ce after implantationof a small-aperture corneal inlay for the surgicalcorrection of presbyopia: Two-year follow-upAlois K. Dexl, MD, MSc, Orang Seyeddain, MD, Wolfgang Riha, MD, Melchior Hohensinn, MD,
Wolfgang Hitzl, PhD, MSc, G€unther Grabner, MD
Q 2011 A
Published
SCRS an
by Elsev
PURPOSE: To evaluate the change in reading-performance parameters after implantation of theKamra small-aperture intracorneal inlay over a 2-year follow-up.
SETTING: University Eye Clinic, Paracelsus Medical University, Salzburg, Austria.
DESIGN: Cohort study.
METHODS: This study comprised naturally emmetropic presbyopic patients. Bilateral reading acuity,reading distance, reading speed, and the smallest log-scaled sentence were evaluated ina standardized testing procedure using the Salzburg Reading Desk. The minimum postoperativefollow-up was 24 months.
RESULTS: The study enrolled 32 patients. The reading desk results showed a significant improvementin each parameter tested. After a mean follow-up of 24.2 months G 0.8 (SD), the mean readingdistance changed from the preoperative value of 48.1 G 5.5 cm to 38.9 G 6.3 cm (P < .0001), themean reading acuity at best distance improved from 0.3 G 0.14 logRAD to 0.24 G 0.11 logRAD(P < .000001), and the mean reading speed increased from 142 G 13 words per minute (wpm) to149 G 17 wpm (PZ.029). One patient lost 1 line, and 1 patient had no change. The improvementwas up to 6 log-scaled lines (mean improvement 2.7G 1.6 lines) in the other 30 patients.
CONCLUSIONS: After implantation of the small-aperture intracorneal inlay, there was an improvementin all tested readingperformance parameters in emmetropic presbyopic patients; the improvementwasthe result of an increased depth of field. These 2-year results indicate that the inlay is an effectivetreatment for presbyopia.
Financial Disclosure: Drs. Seyeddain, Riha, Hohensinn, and Hitzl have no financial or proprietaryinterest in any material or method mentioned. Additional disclosures are found in the footnotes.
In recent years, the focus of interest in refractive surgeryhas clearly shifted toward the correction of presbyopia.The increasing interest is stimulated by the sheer num-ber of potential patients who might seek permanentspectacle-free correction of this condition. This numberis projected to increase in the comingdecades.Althoughmost presbyopic people use spectacles and contactlenses with a near addition for reading, many extraocu-lar and intraocular surgical procedures have been intro-duced in clinical studies and clinical practice. However,none has emerged as the solution for the perfect correc-tion of presbyopia.
The idea of inserting intrastromal corneal implants tocorrect ametropiawas first proposed by J.I. Barraquer inthe middle of the 20th century.1 Other researchers
d ESCRS
ier Inc.
followedhis ideaby implantingcorneal inlays tomodifythe shape and overall refractive power of the cornea.2,3
The literature reports many problems with intracornealimplants, including corneal necrosis, epithelial and stro-mal opacification and vascularization, and complica-tions related to decentration and corneal nutrition4–7;thus, few surgeons have adopted this procedure.Advances in femtosecond laser and biomaterialtechnology, alongwith a growing demand by informedpatients for a reversible presbyopia treatment, hasrenewed the interest in the implantation of differenttypes of corneal inlays.
The Kamra small-aperture intracorneal inlay (for-merly theAcuFocusCorneal InlayACI 7000, AcuFocus,Inc.) is currently being investigated in U.S. Food and
0886-3350/$ - see front matter 525doi:10.1016/j.jcrs.2010.10.044
526 PRESBYOPIA CORRECTION WITH A SMALL-APERTURE INLAY
Drug Administration clinical trials inside and outsidethe United States for the treatment of near-plano andplano presbyopia, with implantation performed in thenondominant eye only. The intracorneal inlay isdesigned to increase the depth of field based on theprinciple of small-aperture optics to restore near andintermediate visual acuity without a significant impactondistance vision. Recent studies8,9 support the efficacyandsafetyof this small-aperture intracorneal inlay in thetreatment of emmetropic presbyopia with a follow-upof up to 2 years.
Theassessmentof readingperformance is consideredone of the most important clinical examinations whenthe potential benefits of surgical presbyopia treatmentsare compared. One tool for measuring reading perfor-mance is the Salzburg Reading Desk. The system offerscomputerized testing under standardized conditionswhile simulating a “natural” reading process.10,11
The aimof this studywas to evaluate the effectivenessof the Kamra intracorneal inlay in improving differentaspects of reading performance. In particular, we usedthe Salzburg Reading Desk to assess uncorrected bilat-eral reading acuity, reading distance, reading speed,and the smallest log-scaled sentence the patient couldeffectively read over a follow-up of 2 years.
PATIENTS AND METHODS
This prospective nonrandomized noncomparative clinicaltrial comprised naturally emmetropic presbyopic patientsat the University Eye Clinic Salzburg, Austria, as part ofa multicenter trial with participating clinics in the U.S.,Asia, and Europe to evaluate the improvement in near andintermediate vision. This single-center trial evaluated thechanges in reading performance after the implantation ofthe Kamra small-aperture intracorneal inlay. The EthicsCommittee of the County of Salzburg approved the studyprotocol, and all patients provided informedwritten consentbefore enrollment. The study was performed in accordancewith the Declaration of Helsinki.
Patients were eligible for inclusion in the clinical trial ifthey were naturally emmetropic and presbyopic; between45 years and 55 years of age; had a preoperative sphericalequivalent (SE) of plano, defined as C0.50 to �0.75diopter (D) with no more than 0.75 D of refractive cylinder
Submitted: August 5, 2010.Final revision submitted: September 28, 2010.Accepted: October 5, 2010.
From the University Eye Clinic, Paracelsus Medical University,Salzburg, Austria.
Additional financial disclosures: Drs. Dexl and Grabner own thepatents on the Salzburg Reading Desk technology.
Corresponding author: Alois K. Dexl, MD, MSc, University EyeClinic, Paracelsus Medical University, M€ullner Hauptstraße 48,A-5020 Salzburg, Austria. E-mail: [email protected].
J CATARACT REFRACT SURG -
determined by cycloplegic refraction; and had a correcteddistance visual acuity of at least 20/20 in both eyes.
Key exclusion criteria were previous ocular surgery, ante-rior or posterior segment diseases or degeneration, and anytype of immunosuppressive disorders. In addition, patientsusing systemicmedicationswith significant ocular side effectsor patients with latent hyperopia, defined as a difference of1.00 D or higher between themanifest refraction and cyclople-gic refraction, were excluded.
Small-Aperture Intracorneal Inlay
The Kamra intracorneal inlay (Figure 1) is a 10.0 mm thin,microperforated artificial aperture (3.8 mm outer diameter;1.6 mm inner diameter) that is centered on the line of sight ofthe nondominant eye after a corneal flap is createdwith a fem-tosecond laser. The inlay is made of polyvinylidene fluoridewith nanoparticles of carbon incorporated to make the inlayopaque. Sixteen hundred small perforations (25 mmdiameter)arranged ina randomizedpatternallowa sufficientnutritionalflow through the inlay to sustain the viability of the anteriorstromal lamella and prevent corneal thinning and epithelialproblems. The holes allow additional (unwanted) light topass, for an average light transmission through the annulusof the inlay of 7.1%. Since the beginning of this trial, thecompany has changed the inlay in some specifications. Thecurrently available inlay is 5 mm thin and has 8400 laser-drilled porosity holes, creating a visible light transmissionthrough the annulus of the inlay of approximately 5%.
Reading Desk
The Salzburg Reading Desk system (Figure 2) consists ofa readingdesk, a computer, andadedicated softwarepackage.Continuousmeasurementof the readingdistance isperformedwith video–stereo photogrammetry and additional softwareprocessing.With this system,patients choose their readingdis-tance (that is, subjectivelymost convenient). It has been shownthat this stereo-photogrammetric technology is a valid and re-liable method to evaluate reading speed and reading distanceand to calculate the corresponding reading acuity at best dis-tance.10,11 A microphone continuously records the time ofthe reading process. Log-scaled Radner Reading Charts wereused with the reading desk setup. These charts consist of 14log-scaled sentences (1Z largest print size; 14Z smallest printsize); sentence 12 is equivalent to logMAR 0.0 at 40 cm.
Figure 1. The Kamra intracorneal inlay in a patient’s eye with visiblesmall nutritional holes.
Figure 2. Patient’s reading performance examination with the Salz-burg Reading Desk. (Note: reading distance chosen by the patientis 52 cm.)
527PRESBYOPIA CORRECTION WITH A SMALL-APERTURE INLAY
Reading acuity is expressed in logRAD, which represents thereading equivalent of logMAR. A sentence of a log-scaledreading chart is accepted if it can be read by the patient witha minimum reading speed of 80 words per minute (wpm),which represents the lower limit for recreational sense-capturing reading.12,13
Patient Examinations
Table 1. Patient demographics and preoperative data (NZ 32).
Demographic Value
Age (y)Mean G SD 51.20 G 2.2Range 48 to 55
F/M sex (%) 78.1/21.9R/L eye with inlay (n) 12/20SE (D)Mean G SD 0.19 G 0.22Range �0.05 to C0.50
UDVA (lines)Mean G SD 20/16 G 0.6Range 20/20 to 20/12.5
Reading distance (cm)Mean G SD 48.1 G 5.4Range 35.2 to 56.2
Reading acuity at best distance (logRAD)Mean G SD 0.38 G 0.14Range 0.04 to 0.69
The preoperative examination includedmanifest and cyclo-plegic refractions, uncorrected distance visual acuity (UDVA),uncorrected reading performance, slitlamp examination, cor-neal topography (Keratron, Optikon Ophthalmic Equipment),and dilated fundus evaluation. The reading performance wasevaluated at the reading desk by assessing the followingparameters: reading distance, reading speed, reading acuityat bestdistance, and the smallest log-scaled sentence that couldbe read. The examinations were all performed at a standardillumination of 500 lux according to the European norm forthe illumination of reading surfaces in offices and libraries.14
The UDVA measurements were taken at a standardizedluminance level of 85 candelas/m2 (ie, photopic lighting)with an Optec 6500P vision tester (Stereo Optical Co., Inc.)by recording the number of logarithmic Early Treatment ofDi-abetic Retinopathy Study targets identified correctly andderiving the corresponding Snellen equivalent. Ocular domi-nance was determined using a motor-dominance preferen-tial-viewing test. Postoperative follow-up examinations werescheduled for 1, 3, 6, 9, 12, 18, and 24months.All examinationswereperformedby 3 experienced clinicians (O.S.,M.H.,W.R.).Manifest refraction, UDVA measurements, and readingperformance testing were performed at every follow-up visit.Cycloplegic refraction was performed at the 12-month and24-month visits. A detailed description of refraction andUDVA outcomes was published in a previous study.8
Reading speed (wpm)Mean G SD 142 G 13Range 124 to 173
Surgical Technique
Preop smallest log-scaled sentence (1–14)Mean G SD 7.4 G 1.3Range 5 to 11
SE Z spherical equivalent refraction, UDVA Z uncorrected distancevisual acuity; wpm Z words per minute
The same surgeon (G.G.) performed all corneal inlayimplantations between September 2006 and May 2007. Thesurgical preparation and technique have been described in de-tail.8,9 In brief, a superior-hinged flap was created in thenondominant eye with an IntraLase FS 60 kHz femtosecondlaser (Abbott Medical Optics, Inc.); the intended depth from
J CATARACT REFRACT SURG -
the corneal surface was 170 mm. The intracorneal inlay wasthen centered on the stromal bed, with the first Purkinje reflexin the center of the inner diameter of the intracorneal inlay,while the patient fixated on the microscope’s single lightsource. Thereafter, the flap was carefully repositioned.
Statistical Analysis
Descriptive analysis with 95% confidence intervals formeans was performed. A repeated-measures analysis of vari-ancewith 2-sidedpaired Student t testswas applied to analyzedata. A P value less than 0.05% was considered statisticallysignificant. All analyses were performed using Statistica soft-ware (version 6.1, StatSoft, Inc.).
RESULTS
All 32 patients enrolled in this study completed everyscheduled follow-up examination through 24 months.Themean follow-upwas 24.2monthsG 0.8 (SD) (range24 to 26 months). Table 1 shows the patients’ demo-graphics and preoperative data, including readingparameters. The preoperative UDVA in the surgicaleye was 20/12.5 in 5 patients (15.6%), 20/16 in 18patients (56.3%), and 20/20 in 9 patients (28.1%).
Postoperative Reading Performance
Onemonthpostoperatively, themean readingdistancedecreased to 40.6 G 4.3 cm (range 32.6 to 48.4 cm) and
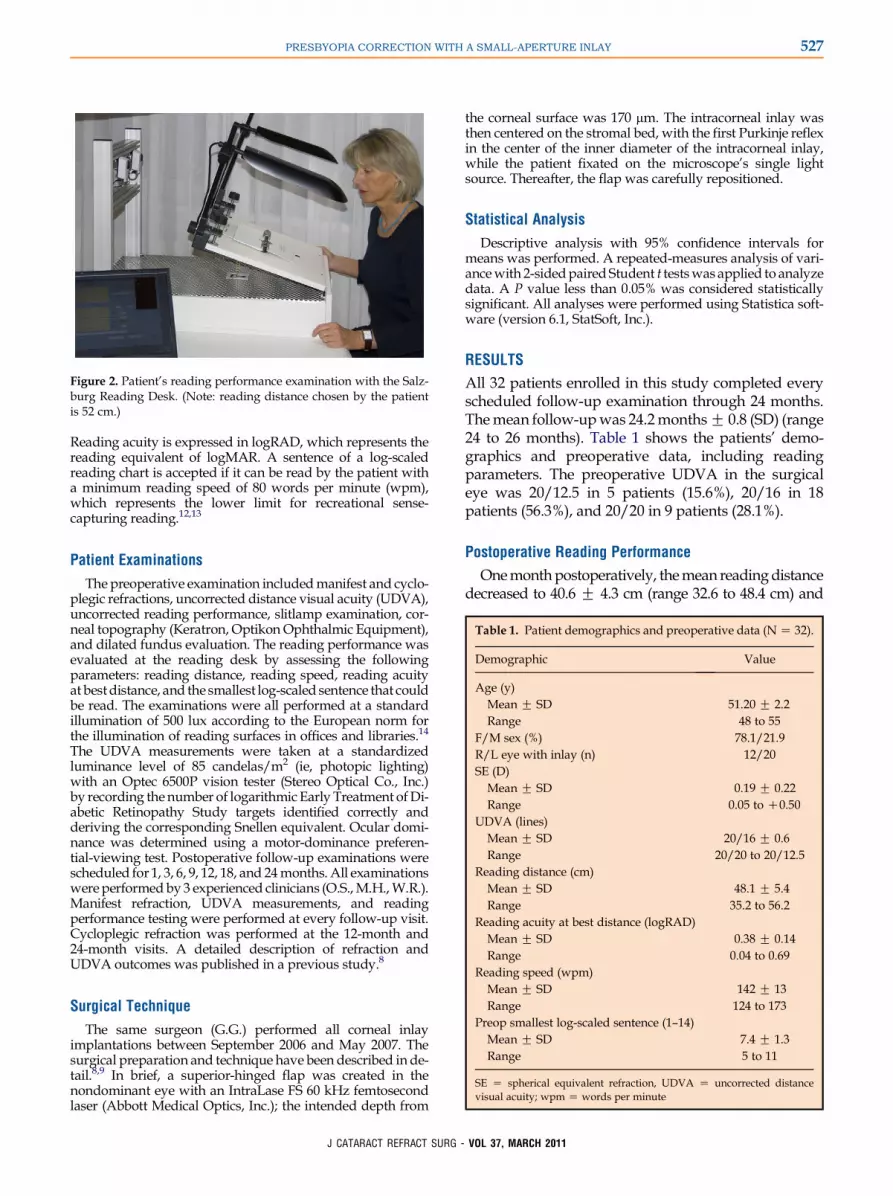
Figure 4. Bilateral uncorrected reading acuity "at best distance"(CI Z 95%confidence interval).
528 PRESBYOPIA CORRECTION WITH A SMALL-APERTURE INLAY
remained stable during the follow-up period (Figure 3).At the 24-month follow-up, the mean reading distancewas 38.9 G 6.3 cm (range 27.4 to 48.9 cm), which wasa statistically significant change (P!.0001).
The mean reading acuity at best distance improvedafter 1 month to 0.27 G 0.13 logRAD (range 0.01 to0.53 logRAD). The mean at the last visit (after 24months) was 0.24 G 0.11 logRAD (range 0.03 to 0.43logRAD), which was a statistically significant change(P!.000001) (Figure 4).
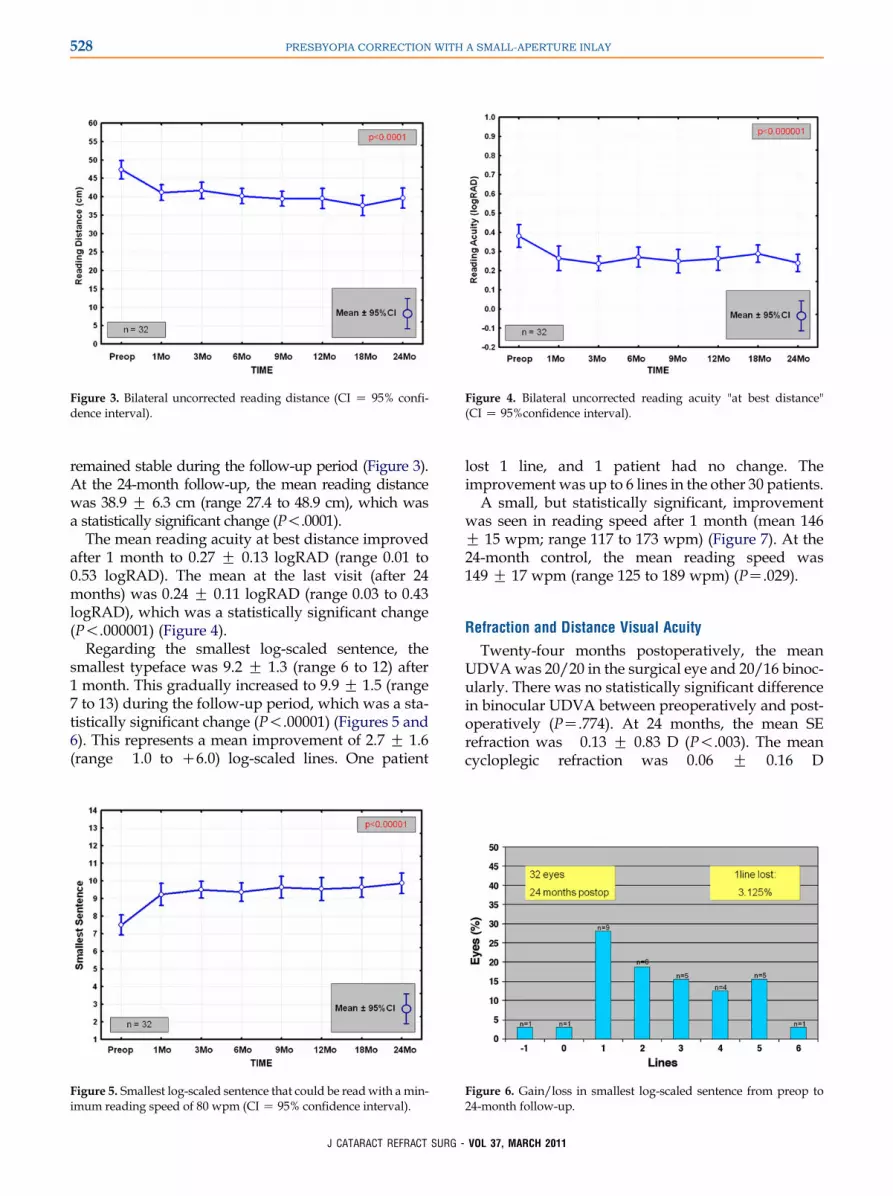
Regarding the smallest log-scaled sentence, thesmallest typeface was 9.2 G 1.3 (range 6 to 12) after1 month. This gradually increased to 9.9 G 1.5 (range7 to 13) during the follow-up period, which was a sta-tistically significant change (P!.00001) (Figures 5 and6). This represents a mean improvement of 2.7 G 1.6(range �1.0 to C6.0) log-scaled lines. One patient
Figure 5. Smallest log-scaled sentence that could be readwith amin-imum reading speed of 80 wpm (CI Z 95% confidence interval).
J CATARACT REFRACT SURG -
lost 1 line, and 1 patient had no change. Theimprovement was up to 6 lines in the other 30 patients.
A small, but statistically significant, improvementwas seen in reading speed after 1 month (mean 146G 15 wpm; range 117 to 173 wpm) (Figure 7). At the24-month control, the mean reading speed was149 G 17 wpm (range 125 to 189 wpm) (PZ.029).
Refraction and Distance Visual Acuity
Twenty-four months postoperatively, the meanUDVAwas 20/20 in the surgical eye and 20/16 binoc-ularly. There was no statistically significant differencein binocular UDVA between preoperatively and post-operatively (PZ.774). At 24 months, the mean SErefraction was �0.13 G 0.83 D (P!.003). The meancycloplegic refraction was 0.06 G 0.16 D
Figure 6. Gain/loss in smallest log-scaled sentence from preop to24-month follow-up.
529PRESBYOPIA CORRECTION WITH A SMALL-APERTURE INLAY
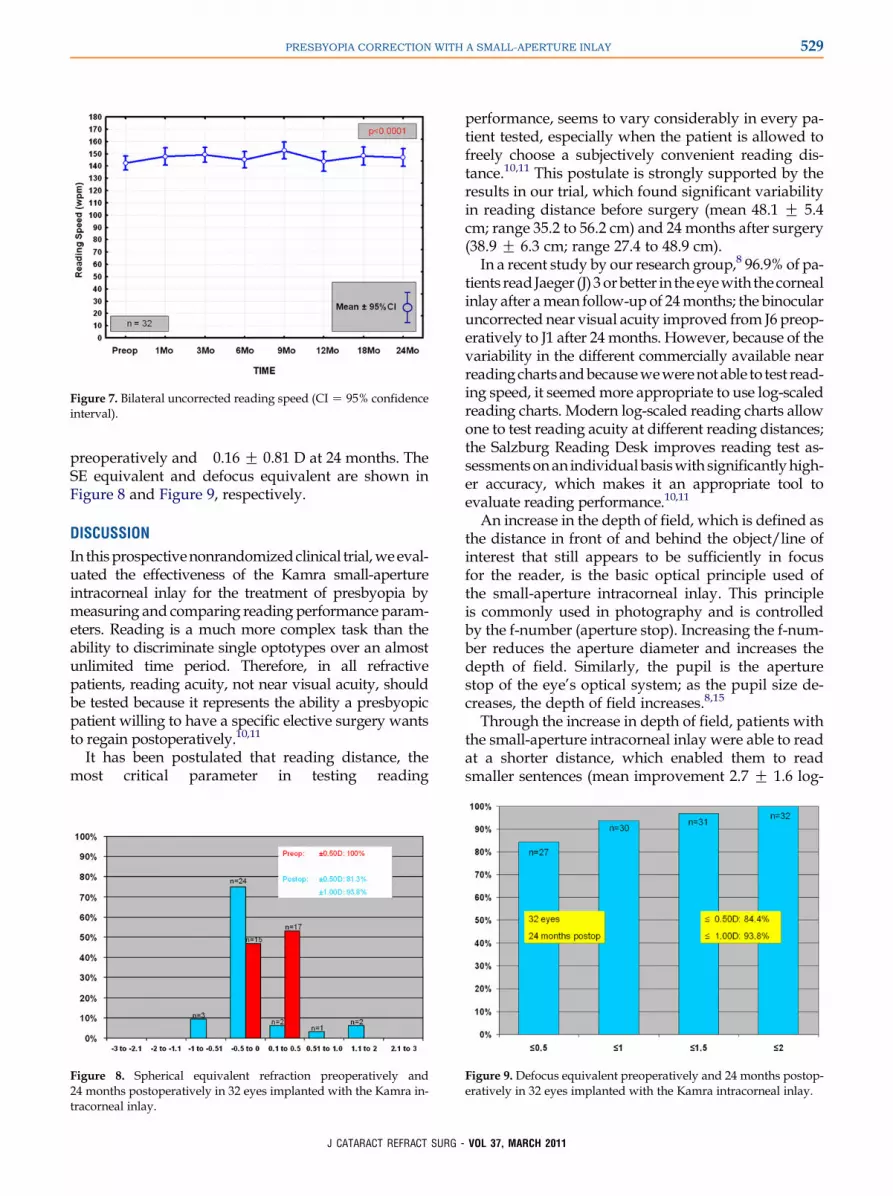
preoperatively and �0.16 G 0.81 D at 24 months. TheSE equivalent and defocus equivalent are shown inFigure 8 and Figure 9, respectively.
DISCUSSION
In thisprospectivenonrandomizedclinical trial,weeval-uated the effectiveness of the Kamra small-apertureintracorneal inlay for the treatment of presbyopia bymeasuring and comparing reading performance param-eters. Reading is a much more complex task than theability to discriminate single optotypes over an almostunlimited time period. Therefore, in all refractivepatients, reading acuity, not near visual acuity, shouldbe tested because it represents the ability a presbyopicpatient willing to have a specific elective surgery wantsto regain postoperatively.10,11
It has been postulated that reading distance, themost critical parameter in testing reading
Figure 8. Spherical equivalent refraction preoperatively and24 months postoperatively in 32 eyes implanted with the Kamra in-tracorneal inlay.
J CATARACT REFRACT SURG -
performance, seems to vary considerably in every pa-tient tested, especially when the patient is allowed tofreely choose a subjectively convenient reading dis-tance.10,11 This postulate is strongly supported by theresults in our trial, which found significant variabilityin reading distance before surgery (mean 48.1 G 5.4cm; range 35.2 to 56.2 cm) and 24 months after surgery(38.9 G 6.3 cm; range 27.4 to 48.9 cm).
In a recent study by our research group,8 96.9% of pa-tients read Jaeger (J) 3orbetter in theeyewith the cornealinlay after amean follow-up of 24months; the binocularuncorrected near visual acuity improved from J6 preop-eratively to J1 after 24months. However, because of thevariability in the different commercially available nearreadingchartsandbecausewewerenot able to test read-ing speed, it seemedmore appropriate to use log-scaledreading charts. Modern log-scaled reading charts allowone to test reading acuity at different reading distances;the Salzburg Reading Desk improves reading test as-sessmentsonan individualbasiswith significantlyhigh-er accuracy, which makes it an appropriate tool toevaluate reading performance.10,11
An increase in the depth of field, which is defined asthe distance in front of and behind the object/line ofinterest that still appears to be sufficiently in focusfor the reader, is the basic optical principle used ofthe small-aperture intracorneal inlay. This principleis commonly used in photography and is controlledby the f-number (aperture stop). Increasing the f-num-ber reduces the aperture diameter and increases thedepth of field. Similarly, the pupil is the aperturestop of the eye’s optical system; as the pupil size de-creases, the depth of field increases.8,15
Through the increase in depth of field, patients withthe small-aperture intracorneal inlay were able to readat a shorter distance, which enabled them to readsmaller sentences (mean improvement 2.7 G 1.6 log-
Figure 9. Defocus equivalent preoperatively and 24 months postop-eratively in 32 eyes implanted with the Kamra intracorneal inlay.
VOL 37, MARCH 2011
Figure 10. Topography showing the 6 and 24 month results on theupper side, andthe differencemap on the lower side. The localizationof the inlay is indicated by the black annulus in the difference map.
530 PRESBYOPIA CORRECTION WITH A SMALL-APERTURE INLAY
scaled lines). They also had improved reading acuityat best distance (preoperative: 0.38 G 0.14 logRAD;24-month follow-up: 0.24 G 0.11 logRAD).
We consider the small improvement in readingspeed, although statistically significant, to be clinicallyirrelevant. It may represent some aspect of a trainingeffect because within the 2 years of follow-up, patientscompleted the same reading test 8 times.
Whereas most patients (30/32) gained up to 6 linesin log-scaled sentences, 1 patient had no gain and 1patient lost 1 line. Patient 6 (48-year-old woman) hadvery good reading performance at the time of inclu-sion. Her reading acuity at best distance was 0.21logRAD, the reading distancewas 50.9 cm, the readingspeed was 124 wpm, and the smallest log-scaled sen-tence was 10. At the end of the study, the resultswere 0.22 logRAD, 48.0 cm, 130 wpm, and 10, respec-tively Although there appeared to be no large gain forthe patient, she reported being happy with the proce-dure, did not opt for explantation of the inlay, andindicated she “would do it again” on a subjectivequestionnaire.
Patient 27 (50-year-old woman) lost 1 log-scaledsentence (inclusion: line 8; 24-month follow-up: line7), had a decrease in reading acuity at best distance(inclusion: 0.33 logRAD; 24-month follow-up: 0.43logRAD), and had a minor change in reading distance(inclusion: 47.6 cm; 24-month follow-up: 46.2 cm).However, there was a slight improvement in readingspeed (inclusion: 127 wpm; 24-month follow-up:133 wpm). We believe this decrease in basically allparameters (the improvement in reading speed mighthave been a training effect) was caused by an increas-ing amount of hyperopia, which was first observed atthe 12-month follow-up. Even though cycloplegicrefraction was performed before inclusion (after 2applications of cyclopentolate hydrochloride 1% eye-drops), the preexisting amount of latent hyperopia atthe time of inclusion (cycloplegic SE 0.00 D), whichbecame clinically relevant over time, might havebeen underestimated. Until the 9-month follow-up,the SE was G0.00 D, after which it increased to 0.50D at the 12-month follow-up and 2.00 D at the 18-month and 24-month follow-ups. A recent study9
found that after removal of the small-aperture intra-corneal inlay, refraction returned to within G1.00 Dof the preoperative value, with no loss of correctedacuity. Nevertheless, patient 27 did not want to havethe inlay explanted, although she was undecidedwhether she would do the procedure again. The to-pography showed a trend toward central corneal flat-tening from 6 to 24 months (Figure 10), and there wasa small decrease in central corneal thickness (6 months:647 mm; 24 months: 633 mm) measured by ultrasoundpachymetry (DGH 2000AP, DGH Technology, Inc.).
J CATARACT REFRACT SURG -
The decrease might also have caused some hyperopicshift. Another potential explanation is found in the epi-demiologic trials, in which there was a general trend to-ward a hyperopic shift in this age group. The BeaverDam Eye Study16 reports a mean change in refractionof C0.48 D for persons 43 to 59 years of age within 10years of follow-up, with nearly 50% of the populationunder the age of 60 years having a shift toward hyper-opia greater than 0.50D; only 4%had a shift towardmy-opia more than �0.50 D. In the Liwan Eye Study,17 theSE tended to become hyperopic at 60 years of age andthen shifted toward myopia at 75 years.
With the small-aperture intracorneal inlay, most pa-tients (27/32) were not able to read sentence 12 (equalto logMAR 0.0 at a standard reading distance of 40 cm)after 24 months. However, the small letter size of therunning text of newspapers or an insert in drug pack-age is normally between 1.5 to 3.0 mm (equal to sen-tence 5 [2.9 mm] to 8 [1.45 mm] on the log-scaledreading charts). Thus, basically all patients who seebetter than this reading corridor (at least sentence 9)would be able to see sufficiently for all kinds of every-day reading tasks. In our study, 5 patients could readsentence 8 and 1 could read sentence 7 at the 24-monthfollow-up. The other 26 patients could read at leastsentence 9 (mean 10.4 G 1.1; range 9 to 13), which en-abled them to perform reading tasks in which the typewas smaller than in newspapers.
VOL 37, MARCH 2011
531PRESBYOPIA CORRECTION WITH A SMALL-APERTURE INLAY
Optimum centration of the Kamra inlay over the lineof sight (first Purkinje reflex on the corneal surface) isessential for excellent distance and near visual acuity.Seyeddain et al.8 report the data of 2 patients who hadinlay recentration 6 months after initial implantation,leading to a significant increase in near, intermediate,and distance vision.
An advantage of the corneal inlay procedure is itspotential for complete reversibility because no ablationis performed over the optical axis, such as in a laser insitu keratomileusis (LASIK) (presbyopic LASIK ormonovision) treatment.8 This technique can also beperformed safely in patients with hyperopia ormyopicpresbyopia LASIK as a combined refractive procedureto simultaneously correct ametropia and presbyopia.9
In summary, implantation of the Kamra cornealinlay produced improvement in several readingparameters in emmetropic presbyopic patients by in-creasing the depth of field. Although the longestfollow-up published to date covers only 24 months,it seems from the data in this and in previous clinicaltrials8 that the corneal inlay has the potential to bea safe, stable, and effective treatment for presbyopia.
REFERENCES1. Barraquer JI. Modification of refraction by means of intracorneal
inclusions. Int Ophthalmol Clin 1966; 6(1):53–78
2. Dohlman CH, Refojo MF, Rose J. Synthetic polymers in corneal
surgery. I. Glyceryl methacrylate. Arch Ophthalmol 1967;
77:252–257
3. Barraquer JI, Gomez ML. Permalens hydrogel intracorneal
lenses for spherical ametropia. J Refract Surg 1997; 13:342–348
4. Reim M. Chirurgische Anatomie, Physiologie, Biochemie sowie
Fragen der Inlay-Technik [Surgical anatomy, physiology,
biochemistry and questions on the inlay technique]. Ophthalmo-
loge 1992; 89:109–118
5. Ali�o JL,MuletME, Zapata LF, VidalMT,DeRojasV, Javaloy J. In-
tracorneal inlay complicated by intrastromal epithelial opacifica-
tion. Arch Ophthalmol 2004; 122:1441–1446. Available at: http://