the Behavior Therapist ISSN 0278-8403 VOLUME 42, NO. 4 • APRIL 2019 [continued on p. 91] ABCT s association for behavioral and cognitive therapies April • 2019 89 PRESIDENT ’ S MESSAGE What Does ABCT Stand For? Bruce F. Chorpita, UCLA THE THEME of the conven- tion and this year’s activities centers on purposeful reflec- tion about our organization’s collective impact. For a com- munity of members who share a commitment to sci- ence and its principles, such reflection can quickly take us out of our comfort zone, particularly when it comes to questions that are values-based, for which reason and facts cannot offer a clear answer (cf. Simon, 1947). Nevertheless, I hope we pose a few of these questions to each other at various points throughout the year, such that we each feel we have crafted suitable answers, at least for our- selves. The point is not to achieve consensus, but rather to establish or reestablish our beliefs, however diverse, so we have a sense of what guides our work, and to encourage conversation and perspective taking among our members. One seemingly perennial question that I would like to raise this month involves what ABCT stands for—not quite literally, of course, but almost. Do we in fact stand for the advance- ment of behavioral and cognitive therapies, in their various forms? Or do we stand for evi- dence-based therapies, which happen to be sub- stantially represented by cognitive and behav- ioral approaches? To be clear, this is precisely not a question of how the evidence lines up; rather, it is a question about our beliefs and values. If the evidence base were to evolve such that cognitive and behavioral therapies were eventually just unremarkable portions of a special issue CBT in DIVERSE CONTEXTS and PROFESSIONS Kate Wolitzky-Taylor Introduction to the Special Issue: Who Are We? What Do We Do? And Where Do We Do It? CBT in Diverse Contexts and Pro- fessions ● 92 Alyssa Ward, Cameo Stanick, Dakota McPherson Expanding Membership as a Method for Extending the Social Impact of Cognitive Behavioral Science ● 92 Suman Ambwani and Alyssa Minnick Mentoring Emerging Clinical Scientists While Maintaining Scholarly Productivity at a Small Liberal Arts College ● 97 Lisa S. Elwood Reflections and Advice Related to the Transition to a Practi- tioner-Scholar Training Environment: The Challenges and Rewards of Working as Part of a Professionally Diverse Team ● 103 Amanda A Bowling, Rebecca Y. Woo, Sarah Kate Bearman, Jessica L. Tauber More Than Psychometricians: School Psychologists as Prime Potential Disseminators of Cognitive Behavioral Therapies ● 107 Nicholas R. Farrell, Rachel C. Leonard, Bradley C. Riemann The “Behavioral Specialist” Model of Training Novice Parapro- fessional Clinicians: An Innovative, Cost-Effective Approach for Increasing the Scalability of CBT ● 111 President’s Message Bruce F. Chorpita What Does ABCT Stand For? • 89 (continued on p. 90) Editor: Kate Wolitzky-Taylor
Transcript
the Behavior TherapistI S S N 0 2 7 8 - 8 4 0 3
VOLUME 42, NO. 4 • APRIL 2019
[continued on p. 91]
ABCT
s
association forbehavioral andcognitive therapies
April • 2019 89
PRESIDENT’S MESSAGE
What Does ABCTStand For?Bruce F. Chorpita, UCLA
the theme of the conven-tion and this year’s activitiescenters on purposeful reflec-tion about our organization’scollective impact. For a com-munity of members whoshare a commitment to sci-ence and its principles, such
reflection can quickly take us out of our comfortzone, particularly when it comes to questionsthat are values-based, for which reason and factscannot offer a clear answer (cf. Simon, 1947).Nevertheless, I hope we pose a few of thesequestions to each other at various pointsthroughout the year, such that we each feel wehave crafted suitable answers, at least for our-selves. the point is not to achieve consensus,but rather to establish or reestablish our beliefs,however diverse, so we have a sense of whatguides our work, and to encourage conversationand perspective taking among our members.
One seemingly perennial question that Iwould like to raise this month involves whatABCt stands for—not quite literally, of course,but almost. Do we in fact stand for the advance-ment of behavioral and cognitive therapies, intheir various forms? Or do we stand for evi-dence-based therapies, which happen to be sub-stantially represented by cognitive and behav-ioral approaches? to be clear, this is preciselynot a question of how the evidence lines up;rather, it is a question about our beliefs andvalues. If the evidence base were to evolve suchthat cognitive and behavioral therapies wereeventually just unremarkable portions of a
special issue CBT in DIVERSECONTEXTS andPROFESSIONS
Kate Wolitzky-TaylorIntroduction to the Special Issue: Who Are We? What Do WeDo? And Where Do We Do It? CBT in Diverse Contexts and Pro-fessions ● 92
Alyssa Ward, Cameo Stanick, Dakota McPhersonExpanding Membership as a Method for Extending the SocialImpact of Cognitive Behavioral Science ● 92
Suman Ambwani and Alyssa MinnickMentoring Emerging Clinical Scientists While MaintainingScholarly Productivity at a Small Liberal Arts College ● 97
Lisa S. ElwoodReflections and Advice Related to the Transition to a Practi-tioner-Scholar Training Environment: The Challengesand Rewards of Working as Part of a Professionally DiverseTeam ● 103
Amanda A Bowling, Rebecca Y. Woo, Sarah Kate Bearman,Jessica L. TauberMore Than Psychometricians: School Psychologists as PrimePotential Disseminators of Cognitive Behavioral Therapies ●107
Nicholas R. Farrell, Rachel C. Leonard, Bradley C. RiemannThe “Behavioral Specialist” Model of Training Novice Parapro-fessional Clinicians: An Innovative, Cost-Effective Approach forIncreasing the Scalability of CBT ● 111
President’s MessageBruce F. ChorpitaWhat Does ABCT Stand For? • 89
(continued on p. 90)
Editor: Kate Wolitzky-Taylor
90
the Behavior TherapistPublished by the Association for
Behavioral and Cognitive Therapies305 Seventh Avenue - 16th Floor
New York, NY 10001 | www.abct.org(212) 647-1890 | Fax: (212) 647-1865
Subscription information: tBT is published in 8 issuesper year. It is provided free to ABCt members.Nonmember subscriptions are available at $40.00 peryear (+$32.00 airmail postage outside North America).Change of address: 6 to 8 weeks are required for addresschanges. Send both old and new addresses to the ABCtoffice.
ABCt is committed to a policy of equal opportunityin all of its activities, including employment. ABCt doesnot discriminate on the basis of race, color, creed, reli-gion, national or ethnic origin, sex, sexual orientation,gender identity or expression, age, disability, or veteranstatus.
All items published in the Behavior Therapist, includ-ing advertisements, are for the information of our read-ers, and publication does not imply endorsement by theAssociation.
the Association for Behavioral and Cog-nitive therapies publishes the BehaviorTherapist as a service to its membership.eight issues are published annually. thepurpose is to provide a vehicle for therapid dissemination of news, recentadvances, and innovative applications inbehavior therapy.
Feature articles that are approxi-mately 16 double-spaced manuscriptpages may be submitted.
Brief articles, approximately 6 to 12double-spaced manuscript pages, arepreferred.
Feature articles and brief articlesshould be accompanied by a 75- to100-word abstract.
Letters to the editor may be used torespond to articles published in theBehavior Therapist or to voice a profes-sional opinion. Letters should be lim-ited to approximately 3 double-spacedmanuscript pages.
Submissions must be accompanied by aCopyright Transfer Form (which can bedownloaded on our website: http://www.abct.org/Journals/?m=mJournal&fa=tBt): submissions will not be reviewed with-out a copyright transfer form. Prior topublication authors will be asked tosubmit a final electronic version of theirmanuscript. Authors submitting materi-als to tBT do so with the understandingthat the copyright of the published mate-rials shall be assigned exclusively toABCt. electronic submissions are pre-ferred and should be directed to theeditor, Kate Wolitzky-taylor, Ph.D., [email protected]. Pleaseinclude the phrase tBT submission andthe author’s last name (e.g., tBT Submis-sion - Smith et al.) in the subject line ofyour e-mail. Include the correspondingauthor’s e-mail address on the cover pageof the manuscript attachment. Please alsoinclude, as an attachment, the completedcopyright transfer document.
INSTRUCTIONS Ñçê AUTHORS
Kerrie G. Murphy, Christina M. Warner-Metzger,Angela D. MorelandChild-Adult Relationship Enhancement: Expanding Evidence-Based Child Behavior Management Skills to an AcademicMedical Center ● 118
Rosaura Orengo-Aguayo, Regan W. Stewart, Karen G. MartínezGonzález, Joy Lynn Suárez Kindy, María C. Christian Herrero,Inés Rivera ColónBuilding Collaborative Partnerships Across Professions toImplement Trauma-Focused Cognitive Behavioral InterventionsAfter Hurricane Maria in Puerto Rico ● 123
Alan L. Peterson, Casey L. Straud, Wyatt R. EvansTreating Combat-Related Posttraumatic Stress Disorder DuringMilitary Deployments: Importance, Challenges, and SpecialConsiderations ● 127
Jessica F. Magidson, Lena S. Andersen, Alexandra L. Rose,Steven A. SafrenTask Sharing Cognitive Behavioral Therapy in GlobalMental Health: Nurse- and Lay Counselor-DeliveredInterventions for Depression and Substance Use in HIVCare in South Africa ● 131
At ABCTVoluntary Contributors • 139
Welcome, New Members • 140
Call for Nominations: Champions • 143
Call for Nominations: Mentors • 143
(Contents continued)
W H A T D O E S A B C T S T A N D F O R ?
April • 2019 91
larger collection of effective approaches,where would our allegiance be?
this is perhaps hypothetical at themoment, but it is by no means trivial.many of us have probably contemplatedthis question privately, but, for better orworse, answering it publicly can be com-fortably avoided, so long as the evidencebase continues to support CBt and its vari-ants. But even that fact raises a corollaryquestion: Should we even aspire to theempirical dominance of CBt, or should wewish for and perhaps even work toward anever-increasing diversity of effectiveoptions?
I first encountered this question for-mally when Karen Wells served as a discus-sant at an ABCt symposium chaired byJohn Weisz and myself, which described anewly proposed multisite randomizedeffectiveness trial to compare differentmodels of cognitive and behavioral treat-ments against a usual-care comparisoncondition (Wells, 2005). the Child StePsmultisite trial was to be one of the first largetests of multiple evidence-basedapproaches for youth in communitymental health clinics and schools, and Dr.Wells raised her question just as she con-cluded her remarks, noting presciently thatthe trial may not turn out the way weexpect or the way we would like. Like theexpert in behavioral parent training thatshe is, Dr. Wells gently but firmly warnedthat if there were surprises, how webehaved afterward would define who weare. Would we discover ourselves empiri-cists, or would we be devoted advocates ofcognitive and behavioral treatments?Although the premise of the question both-ered me for years (how could 7 years ofhard work not produce an epic CBt suc-cess?!), the question itself gave me greatrelief. Dr. Wells essentially reminded usthat any results were an opportunity tolearn. Incidentally, the trial turned out toyield both good news and bad news forcognitive and behavioral treatments at thetime (for the interested reader, see Weisz etal., 2012), convincing me, among otherthings, that we had chosen a trulyprophetic discussant for the 2005 sympo-sium.
to explore this question a bit more asABCt members, we could choose to lookat our organization’s history. ABCt wasformed in the 1960s, at least in part as anintellectual and political reaction to thenonempirical practices of the time. thus,the focus on behavior therapy was quitepossibly incidental to a larger commitmentto empiricism. If we would like something
more current to consider, we could alsolook to our mission statement for guid-ance; it communicates a commitment toaddressing health and well-being using“behavioral, cognitive, and biological evi-dence-based principles,” which, to me,seems to cover all sides but maybe commitsto none. Finally, we could look at the com-position of the literature itself: A casualsearch of the youth mental health treat-ment literature performed as I wrote thiscolumn on march 5, 2019, yielded 602 ran-domized trials that summarized 736 proto-cols meeting evidence-based treatmentstandards (PracticeWise, 2019). Althoughroughly 80% of those would be consideredcognitive or behavioral by most judges,that still leaves approximately 150 non-cognitive-behavioral evidence-based treat-ments for youth, manualized and tested inat least one randomized controlled trialagainst an active treatment condition, andinclude such approaches as Adlerian grouptherapy, attachment therapy, case manage-ment, client-centered therapy, expression,hypnosis, play therapy, psychodynamictherapy, and social support. Although wecould debate some of these findings, theexact study counts, or treatment classifica-tions, the larger point is clear: there is lim-ited but increasingly conspicuous evidencesupporting a wide variety of treatmentapproaches other than behavioral and cog-nitive ones. What do we as members ofABCt make of that?
As we think this year about increasingABCt’s impact, and about the aim of dis-semination outlined in ABCt’s strategicplan, this question of our identity is worthyof reflection—not simply because we couldchange our name again, but because theanswer speaks to what we will pursue,showcase, and embrace at our convention,throughout the year’s activities, and in ourown professional endeavors. As Dr. Wellscautioned: the answer will define us.
Yielding to my own instincts, I think theissue is important enough to warrant abehavioral rehearsal. Yes, that’s right—Iam assigning homework for those of youreading this. It is quite simple: I encourageyou to seek out a peer or colleague, perhapsat lunch, over coffee, or at a happy hour.Ask for their thoughts on this question, andthen ask for their reaction to yours. I tried itseveral times this year with a few well-chosen colleagues, and every conversationwas a unique mixture of excitement, inspi-ration, challenge, and insight. I hope youfind it as rewarding and worthwhile as Ihave.
Evidence-Based Services (PWEBS) data-base. Satellite Beach, FL: Author.
Simon, h. A. (1947). Administrativebehavior: A study of decision-makingprocesses in administrative organization.New York, NY: macmillan.
Weisz, J.R., Chorpita, B.F., Palinkas, L.A.,Schoenwald, S.K., miranda, J., Bearman,S.K., Daleiden, e.L., Ugueto, A.m., ho,A., martin, J., Gray, J., Alleyne, A.,Langer, D.A., Southam-Gerow, m.A.,Gibbons, R.D., and the Research Net-work on Youth mental health. (2012).testing standard and modular designsfor psychotherapy with youth depres-sion, anxiety, and conduct problems: Arandomized effectiveness trial. Archivesof General Psychiatry, 69, 274-282.
Wells, K. C. (2005, November). Discussantin B. F. Chorpita & J. R. Weisz (Chairs),Bridging Science and Community Prac-tice: An Overview of the Child STEPsClinic Treatment Project. Symposiumpresented at the annual meeting of theAssociation for Behavioral and Cognitivetherapies, Washington, DC.
. . .
the author has no conflicts of interest orfunding to disclose.Correspondence to Bruce F. Chorpita,Ph.D., Franz hall 3227, Department of Psy-chology, University of California, Los Ange-les, Los Angeles, CA 90095;[email protected]
92 the Behavior Therapist
IN the eARLY DAYS of behavioral and cog-nitive therapies, the vast majority of profes-sionals who were developing, evaluating,disseminating, and delivering these inter-ventions were clinical psychologists whoprimarily worked as professors in psychol-ogy departments or in psychiatry depart-ments of academic medical centers; anddisseminating was typically limited totraining clinical psychology doctoral stu-dents in the context of their graduate pro-grams. even when we go to the ABCtAnnual Convention now, it is easy toassume that that remains the case. how-ever, as the field has progressed, cognitiveand behavioral therapies have reached a
variety of contexts because of the diverseprofessional experiences and activities ofbehavior therapists, many of whom callABCt their professional home. In this spe-cial issue, we highlight the unique careerpaths of our members and celebrate thecreative work they are doing to increaseCBt’s reach. the articles in this issue illus-trate how ABCt members positioned in avariety of career settings are training thenext generation of those who may deliverCBt or develop clinical research programs(beyond the traditional clinical psychologyPh.D. student in a clinical science or scien-tist-practitioner program). the articles alsohighlight several novel and exciting
approaches and programs for deliveringCBt in diverse, nontraditional settings.this issue aims to challenge our assump-tions about who we are, what we do, andwhere we do it as ABCt members, and tohighlight the diverse career paths anddiverse opportunities and models toexpand CBt’s reach in the community.
I would like to thank all of the authorsand the Behavior Therapist editorial Boardfor their contributions, and I would espe-cially like to thank Richard LeBeau and Bitamesri for their additional support inputting this special issue together. I hopeyou enjoy reading about the exciting workdescribed in this special issue.
. . .
the author has no conflicts of interest orfunding to disclose.
Correspondence to Kate Wolitzky-taylor,Ph.D.,UCLA Department of Psychiatry andBiobehavioral Sciences, 11075 Santa monicaBlvd., Suite 200, Los Angeles, CA 90025;[email protected]
INTRODUCTION TO THE SPECIAL ISSUE
Who Are We? What Do We Do? And WhereDo We Do It? CBT in Diverse Contexts andProfessionsKate Wolitzky-Taylor, UCLA
At the tIme OF thIS WRItING, we havearrived at the phase in the ABCt calendaryear where convention planning is in full-swing. We are all preparing for how we willcontribute to the evolving scientific conver-sation about what we continue to learnabout cognitive and behavioral therapiesand how we take that knowledge and turn itinto wisdom in action. As you have heardfrom Dr. Chorpita in his columns so far thisyear, the focus of his presidency and thetheme of the 2019 convention in Atlanta is“Wisdom of Purpose and Perspective:extending the Social Impact of CognitiveBehavioral Science.” As Program Chair andAssistant Program Chair, our humble role
alongside our team is to support how webring this theme to life through our call forpapers, rigorous review process, invitedspeaker presentations, and overall spirit ofthe convention program. As we have con-sidered our current social impact as an orga-nization, many of our conversations comeback to questions of our membership com-position and convention attendees. Whodoes our membership represent in the fieldof cognitive behavioral science? Whoattends our Annual Convention and how dowe use it as a venue to expand our socialimpact? how can we best support andamplify the voices of wisdom within ourmembership to impact a wider audience?
how do we encourage our membership towork across disciplines and fields of study totackle the “big questions” related to ourshared mission of advancing health andwell-being?
these are not new inquiries, and perhapsmany of you have had these conversationswithin your Special Interest Groups. DuringDr. Ward’s 3-year tenure as Special InterestGroups (SIG) chair, she noted growinginterest in collaboration between SIGs inconvention submissions and developmentof publications and a desire to break downtraditional silos within the organization tomake broader impact statements about theimplications of findings. the Disseminationand Implementation Science Special Inter-est Group (DIS SIG) has had a particularlystrong interest in these questions of mem-bership, as it has come to attract the affilia-tion of ABCt members from outside of aca-demic institutions.
In 2015, members of the DIS SIG wrotean article for the Behavior Therapist titled“Dancing With Ourselves: Reflections onIncreasing Stakeholder Involvement inABCt” (Stanick, et al., 2015). the articlewas a reflection on both the efforts of theDIS SIG to engage stakeholders with ABCt
Expanding Membership as a Method forExtending the Social Impact of CognitiveBehavioral ScienceAlyssa Ward, Virginia Department of Medical Assistance Services
Cameo Stanick, Hathaway-Sycamores Child and Family Services
This concise reference written by leading experts for busyclinicians provides practical and up-to-date advice oncurrent approaches to diagnosis and treatment of insomnia.Professionals and students learn to correctly identify anddiagnose insomnia and gain hands-on information on howto carry out treatment with the best evidence base: cognitivebehavioral therapy for insomnia (CBT-I). Copyable appendi-ces provide useful resources for clinical practice.
Expert, evidence-based guidance on persistent depressivedisorder (PDD) for busy practitioners who need to knowhow to assess, diagnose, and treat this difficult to identifyand potentially life-threatening disorder. The therapiesthat have the strongest evidence base are outlined, andin particular the cognitive behavioral analysis system ofpsychotherapy (CBASP), a treatment specifically developedfor PDD. Printable tools in the appendices can be used indaily practice.
www.hogrefe.com
Ric M. Procyshyn / Kalyna Z. Bezchlibnyk-Butler /J. Joel Jeffries (Editors)
Clinical Handbook ofPsychotropic Drugs23rd ed. May 2019, iv + 408 pp. + 50 pp. of printablePDF patient information sheets, spiral boundUS $99.80ISBN 978-0-88937-561-1Also available as online version
William K. Wohlgemuth /Ana Imia Fins
Insomnia
(Advances in Psychotherapy –Evidence-Based Practice –Volume 42)2019, viii + 94 pp.US $29.80ISBN 978-0-88937-415-7
The Clinical Handbook of Psychotropic Drugs has becomea standard reference and working tool for psychiatrists,psychologists, physicians, pharmacists, nurses, and othermental health professionals.
It is a must for everyone who needs an up-to-date, easy-to-use, comprehensive summary of all the most relevantinformation about psychotropic drugs.
New in this edition• New formulations/trade names:Adzenys ER (amphetamine),
Aristada (aripiprazole) … Jornay PM (methylphenidate) …Spravato (esketamine) ... Zelapar (selegiline), and many more
• Major updates: antipsychotic augmentation strategies,antidepressants, now including esketamine (Spravato),treatments for substance use and extrapyramidal effects,pharmacogenomics, unapproved treatments and lots more
J. Kim Penberthy
PersistentDepressiveDisorders
(Advances in Psychotherapy –Evidence-Based Practice –Volume 43)2019, x + 150 pp.US $29.80ISBN 978-0-88937-505-5
94 the Behavior Therapist
convention events and to highlight stake-holder-researcher collaborative projects inorder to emphasize the need for stakeholderrelationships in the ABCt mission of clos-ing the research-practice gap. the articlealso served as a charge to the ABCt mem-bership at large to ensure we are engaging,expanding, and embracing avenues forstakeholders to partner with research initia-tives, increase membership, and amplifytheir voice in the association. As the DIS SIGarticle suggested, if we are not involvingstakeholders across the research-to-practicespectrum, then we risk continuing to dia-logue only among ourselves, and the sciencestagnates.
We were asked to submit this article inpart because we both (AW and CS) beganour careers and our involvement withABCt from what seems to be the traditionalroute of most members, though our trajec-tories have taken us into roles where we sit ascognitive behavioral scientist practitionersin stakeholder systems. many of the storiesto be shared in this issue come from otherslike us, and we thought that describing a bitabout our journeys might illustrate our rec-ommendations for broadening the reach ofconvention attendees and organizationalmembership.
Both of us began attending ABCt duringour graduate school years while enrolled inour clinical psychology doctoral programs.We both wrote theses and dissertationsrelated to cognitive-behavioral evidence-based practice (eBP) under the mentorshipof long-time ABCt members. We met aspostdoctoral fellows working for the currentABCt President on a randomized, con-trolled effectiveness trial testing modular vs.standard approaches to eBP with childrenin community mental health settings. Weboth have been national trainers in evi-
dence-based practice approaches. Dr. Stan-ick took a traditional route following post-doc and went on to earn tenure at the Uni-versity of montana with a research programfocused on implementation science, withspecialty areas in childhood trauma andschool-based mental health. Dr. Warddeparted from the traditional academicroute and became an administrator in com-munity mental health, overseeing workforcetraining development and implementationof 11 eBPs at an agency with the largestmedicaid contract in Los Angeles County.When she left to accept an assistant profes-sorship in a medical school doing a combi-nation of research and practice with eBP forpediatric populations, Dr. Stanick left hertenured position to take over Dr. Ward’sformer position in Los Angeles County andhas expanded that role to include fortifica-tion of implementation science principlesand measurement, the development of atraining and research institute, andincreased focus on trauma-informed care.After 2 years back in academics, Dr. Wardwas lured back into “the real world” tobecome the Behavioral health ClinicalDirector at Virginia medicaid, where she isoverseeing the redesign of the public behav-ioral health system to an evidence-based,trauma-informed, prevention-focused sys-tem of care.
Both of us agree that without our rootswith our mentors and connection to the DISSIG, we would have terminated our ABCtmemberships and ceased attending the con-ference. Without being academically affili-ated, we lack consistent funding for mem-bership and convention costs. We bothattend numerous conferences for our work,but these are focused more specifically onthe real world of behavioral health systemsimplementation. We have remained con-
nected to the organizationbecause the DIS SIG has pro-vided a “professional home”for us as “recovering academi-cians” who are not as oftenproducing the kinds ofresearch traditionally pre-sented at our convention. theDIS SIG has valued our voicesand included us as “real-world” discussants on panelsof research that intend toinform system architects likeourselves, as well as in leader-ship positions within the SIG.We continue to be as inti-mately involved in service toABCt because we hope to fur-ther the mission of our mutual
mentor, Dr. Bruce Chorpita, to influence theorganization to move towards increasedfocus on how we can make the greatest dif-ference in the lives of those who we all hopebenefit from cognitive behavioral science.
the Call for Papers for the 2019 conven-tion specifically challenges us to reach outand partner with new and diverse popula-tions (e.g., global mental health, underuti-lized behavioral health audiences, under-served communities, intersecting interestsamong two or more Special InterestGroups) and encourages submissions thatstrive to solve problems meaningful tostakeholders in industry, behavioral andphysical health care, government agencies,and other contexts of our work. this themealso challenges us to apply the “lessonslearned” of the past 2 decades since theAmerican Psychological Association Divi-sion 12 task force highlighted the impor-tance of focusing on implementation con-texts where practitioner stakeholders areprimarily associated.
this brings us back around to the exist-ing composition of our organizationalmembership and questions as to whether wehave sufficiently propped open the doors toour dining room and then attracted, wel-comed, and integrated diverse voices to seatsaround our table. We have shared a bitabout our stories and why we have remainedwith the organization, but what about thosewho never had a traditional, academic routeto ABCt orientation? What about our col-leagues in public health settings? In technol-ogy contexts? In nursing? how are they rep-resented among us and how can wewelcome them into our conversations? Inseeking data to inform this question, werequested some information on member-ship trends from the ABCt central officeand will summarize that here.
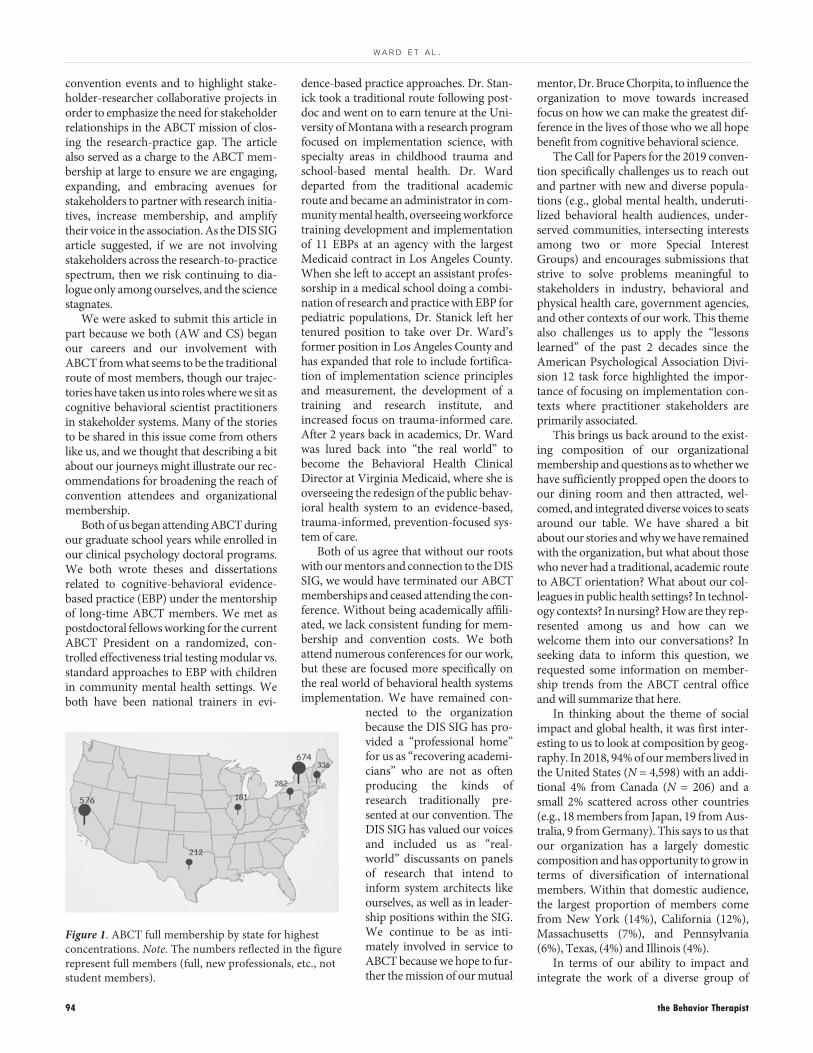
In thinking about the theme of socialimpact and global health, it was first inter-esting to us to look at composition by geog-raphy. In 2018, 94% of our members lived inthe United States (N = 4,598) with an addi-tional 4% from Canada (N = 206) and asmall 2% scattered across other countries(e.g., 18 members from Japan, 19 from Aus-tralia, 9 from Germany). this says to us thatour organization has a largely domesticcomposition and has opportunity to grow interms of diversification of internationalmembers. Within that domestic audience,the largest proportion of members comefrom New York (14%), California (12%),massachusetts (7%), and Pennsylvania(6%), texas, (4%) and Illinois (4%).
In terms of our ability to impact andintegrate the work of a diverse group of
Figure 1. ABCt full membership by state for highestconcentrations. Note. the numbers reflected in the figurerepresent full members (full, new professionals, etc., notstudent members).
W A R D E T A L .
April • 2019 95
full page adNewHarbinger.pdf
1-800-748-6273 | newharbinger.com
newharbingerpub l i ca t i ons
ESSENTI AL RESOURCESfor YOUR PR ACTICE
Learn more about evidence-based continuing education and training with praxiscet.com
Download a FREE e-book of our most popular tips: newharbinger.com/quicktips
ISBN: 978-1684031658 | US $16.95ISBN: 978-1684031474 | US $16.95
An Imprint of New Harbinger Publications
ISBN: 978-1684031443 | US $18.95
An Imprint of New Harbinger Publications
ForTeens
ForTeens
ISBN: 978-1684032426 | US $24.95
An Imprint of New Harbinger Publications
ISBN: 978-1684032358 | US $39.95 ISBN: 978-1684033348 | US $25.95ISBN: 978-1684032426 | US $24.95 ISBN: 978-1684033348 | US $25.95
NewEdition
96 the Behavior Therapist
W A R D E T A L .
domestic stakeholders, it appears that thecoasts have the highest representations, withrelatively low portrayal of the work happen-ing in the middle, northwest, and southernareas of the country. Given the distributionsof membership, it is not surprising thatmembership enrollment has been up duringyears when the Annual Convention is heldin particular locations, such as New York(membership total, including students, in2016 New York convention = 5,372) com-pared to more central locations (member-ship total, including students, in 2007Chicago convention = 4,684).
Other important distributions regardingmembership include the ratios of full mem-bers to students, as well as the primary “role”of members (e.g., the context in which theyspend 50% or more of their time). It is clearfrom membership data that ABCt fosters alarge student population (N Student 2018 =1,663 compared to N Full 2018 = 2,470).there are a number of opportunities for stu-dents, including the main conference pre-sentation possibilities as well as student-focused networking events such as specificpresentations and gatherings focused on theinternship match process. What is less clear,however, is if ABCt attracts students fromdiverse programs outside of psychology,counseling, and social work, such as psychi-atry, nursing, and/or organizational or otherhealth-care industry sectors. In addition,data supplied by the central office shows thata large proportion of our membership (52%,N = 1,218) spends 50% or more of their timein clinical roles; whereas only 12.8% (N =299) and 26% (N = 614), respectively, spend50% or more of their time in “academic” or“research” roles. We found these statisticsrather surprising, as we felt that much ofwhat we see in terms of convention pro-gramming tends to represent traditionalresearch from those with psychologydepartment affiliations. this data alsoshowed that only a small percentage (5%)reported spending 50% or more time inadministrative roles such as ours, though itmade us eager to seek out this subgroup andlearn about their careers and contributionsto ABCt.
Given what this glimpse of our member-ship data reveals, we think that there are sev-eral opportunities before us as an organiza-tion in terms of expanding the reach of ourscience. In order to create an appreciableimpact on the research-practice gap, ourorganizational efforts will require a multi-pronged approach. As an association, wemust elevate our members’ work that isinclusive of populations more representa-tive of community mental health settings
(e.g., transdiagnostic approaches, treat-ments geared toward complex comorbidi-ties, underrepresented populations, etc.).We must also increase efforts to engage pro-fessional partnerships across different sec-tors. In a tBT article from 2017, dissemina-tion and implementation experts wereinterviewed and asked if they had learnedlessons from other disciplines that could beapplied to their work. each interviewee, Drs.David Clark, Bruce Chorpita, Ann Garland,Rochelle hanson, and Shannon Dorsey,reported that they had relevant, workingpartnerships with colleagues in a number ofother fields and also that certain other disci-plines had done far more to address theresearch-practice gap than behavioral health(e.g., technology, economy, nursing, epi-demiology, etc.).
One immediate strategy that we canemploy is to collect richer data on our mem-bership. For instance, having a better under-standing of our members who are in clinicalcontexts—are these primarily direct-careroles? Are they in agencies or in privatepractice? how/do they utilize research andin what way? For the “other” category, whatjob functions make up this group? Further,to ensure we are sufficiently propping openthe doors to our dining room, we mustreturn to the questions posed in Stanick etal. (2015), which is to ask ourselves, What dostakeholders get from their involvement inABCT? Also, are the incentives that ABCtmembership offers actually what stakehold-ers across different sectors want? What doother stakeholder-focused associations,such the National Council for Behavioralhealth, target that are draws for providers?
We also know that accessibility is a fre-quently cited barrier to association and con-vention involvement; thus, below is a list ofsuggestions for our membership Commit-tee and our Board focused on increasing ourstakeholder reach:
1. Offering a reduced rate for practitionersto attend the convention.2. Offering a reduced rate for nonstudent,first-time attendees.3. Using technology to increase access toconvention presentations such as livestreaming sections of strategic talks onsocial media platforms and exploring meth-ods of “virtual” conference attendance for areduced rate but with CeU credit.4. Developing a “Welcome Project” that tar-gets new members or new attendees fromnonpsychology disciplines or nonacademicsettings. this could involve a specializedname badge at the convention and forming
a committee that greets these individuals,supports them in finding presentations ofinterest, connects them with relevant SIGs.5. Continue with convention themes thatemphasize and encourage submissions thatinclude nontraditional members as presen-ters, discussants, etc.6. Identify ABCt “Ambassadors” whowould be members who sit in nontradi-tional, nonacademic roles and highlight andreward these members for the type ofimpact they have on the organization andthe field of cognitive behavioral science.
What is clear is that a lot more work can bedone to increase reach and outreach tostakeholders within and across various sec-tors for our ABCt community. ABCt has acommitted membership and of course all ofus are invested in the promotion of bestpractices for the behavioral health con-sumers our work ultimately serves. In orderto ensure that ABCt continues to reflectgrowth in the field, this begins with mem-bership and the active inclusion of col-leagues and industry associates who histori-cally may not have seen the value ofmembership and/or are struggling to see thecontinued value of membership. We believeenhancing the social impact of cognitivebehavioral science will require an increasedprofessional diversity of our members, newpathways for nontraditional and juniormembers, and a dedicated collaboration.We hope the 2019 convention moves us fur-ther in that direction.
ReferencesBearman, S.K., & Ward, A. (2017).
Coming of age (professionally) in the ageof dissemination and implementation:D&I experts: Spotlight interviews. theBehavior Therapist, 40(7), 231-236.
Stanick, C., Yoman, J., Gallo, K., trent, L.,Reding, m., Kim, R., Guan, K., & Stein-feld, B. (2015). Dancing with ourselves?Reflections on increasing stakeholderinvolvement in ABCt. the BehaviorTherapist, 38(2), 38-42.
. . .
the authors have no conflicts of interest orfunding to disclose.Correspondence to Alyssa Ward, Ph.D.,LCP, Virginia Department of medical Assis-tance Services, 600 e Broad Street, Rich-mond, VA 23219; [email protected]
April • 2019 97
1/2-page adiPromptU.pdf
UNDeRGRADUAte ReSeARCh tRAINING inpsychology serves several essential func-tions, including professionalizing studentswithin the boundaries and expectations forthe discipline, helping them to developtheir critical thinking and research skills,and helping them to truly grasp the scien-tific basis of the discipline (Behar-horen-stein, Roberts, & Dix, 2010; Brewer,Dewhurst, & Doran, 2012; Van Vliet, Klin-gle, & hiseler, 2013). Although severalsources have described the opportunities,barriers, and recommended procedures forsupervising undergraduate research assis-tants, the vast majority of these reportsfocus on large research universities
wherein undergraduate research assistantstypically work in a lab along with graduatestudents who may occasionally serve astheir primary supervisors (e.g., evans,Perry, Kras, Gale, & Campbell, 2009;morales, Grineski, & Collins, 2017; thiry &Laursen, 2011). moreover, several of theseaccounts focus broadly on other Stemfields (e.g., Behar-horenstein et al., 2010;morales et al., 2017; thiry & Laursen)rather than on the more specific needs ofemerging scientists in clinical, counseling,or other applied health areas of psychology.Our purpose here is to describe a model ofmentorship for supervising undergraduateresearchers at a small liberal arts college
(SLAC) and share the perspective of a fac-ulty supervisor as well that of a (former)undergraduate student. Although there arevarious opportunities to mentor under-graduate psychology researchers throughclassroom instruction in researchdesign/analysis, or supervision of indepen-dent studies and honors projects, we focushere on one particular model—the stu-dent-faculty collaborative research model—and review strategies, recommendations,and the impact of this approach on the stu-dent’s development and on the facultymentor’s research program.
A Faculty Mentor’s PerspectiveGiven the multifaceted intellectual ben-
efits conferred by the practice of research,the Council on Undergraduate Research(CUR.org) recommends that undergradu-ate research opportunities “should beaccessible to as broad a range of students asis practical” (p. 3) rather than limited solelyto more advanced students (Rowlett,Blockus, & Larson, 2012). For many, thisrecommendation may pose a quandary: Isit feasible and beneficial to invest in the rel-
Mentoring Emerging Clinical Scientists WhileMaintaining Scholarly Productivity at a SmallLiberal Arts CollegeSuman Ambwani, Dickinson College
Alyssa Minnick, University of North Carolina, Charlotte
Originally designed for CBT homework,iPromptU now works for large-scaleresearch and scale development.
Just email your custom tasks or experi-mental scales to an unlimited number ofemail recipients. Users simply open theemail attachment to download the appand automatically populate it with yourmeasures.
Program it to run whenever the userpresses a button. Or program it to dorandom time sampling. Users can simplydictate their responses.
Display multiple questions on onescrollable page, or deliver only onequestion at a time.
As always, iPromptU is free, and ad-free.
Produced as a gift to the practice of science by:
Configure it for a patient, or for thousands of research participants
Displays any question, or series of questions, andprompts the user for written or dictated answers.Saves responses with date and time stamps so usercan email them to therapist or researcher.User can initiate prompting immediately, as theywould with a coping card or worksheet. Researchersand therapists can set prompting to occur atrandom time intervals, for truly random timesampling.All prompts are 100% customizable, and can bepresented singly or in sequential or random order.Researcher or therapist can install a securitypassword to prevent alteration by the user.Capable of virtually any non-branching EcologicalMomentary Assessment research.Capable of recording any CBT Activity Schedule,Thought Record, or Worksheet in the real world.Clean, no-nonsense user interface.
Cognitive Behavioral Institute of Albuquerque, LLCBradford C. Richards, Ph.D., ABPPDirector and Supervising Psychologist
Available free in both the App Store and Google Play
for iOS & Android has a new feature
98 the Behavior Therapist
A M B W A N I & M I N N I C K
atively time-intensive practice of mentor-ing student researchers across the spec-trum of knowledge and ability, particularlywhen many institutions do not offer teach-ing credit or tenure/promotion benefits fordoing so? Why would you do so? Accord-ing to one multisite investigation of formalundergraduate research training programs,faculty are more likely to serve as mentorsif they value increasing diversity throughmentorship of underrepresented groups,believe mentorship will be associated withinstitutional rewards (i.e., reviews and pro-motions), have unconstrained access toundergraduate research candidates, do notsee mentorship as very time consuming,and are mid-career (rather than late-career) faculty (morales et al., 2017).Although SLACs do prioritize teaching, myinstitution does not require or formallyconsider student-faculty collaborativeresearch for tenure or promotion, we havelimited access to formal undergraduateresearch programs geared toward increas-ing diversity, and, in my experience,research mentorship is always a time-con-suming activity. Nonetheless, my answer tothe “is it worth it?” question is an enthusi-astic yes, but with a qualifier: Students musthave completed at least one course inresearch design, have a good academicrecord, and be willing to commit to a year-long experience in my lab. As long as stu-dents meet these criteria, there are manyways for us to establish a mutually benefi-cial and productive research collaboration.
Several unique features of SLACs facili-tate student-faculty research collaborationsand thereby advance the research pro-grams of faculty supervisors. First, smallclassrooms allow faculty to work closelywith students and learn their individualstrengths and weaknesses, and this infor-mation can be used strategically to recruitlab research assistants: whereas one mightexcel at literature research, another mighthave a sophisticated understanding ofresearch design, while another mightdemonstrate strong attention to detail,time-management skills, and online surveydevelopment skills, and a fourth may bewell-versed in data set-up and basic analy-sis in SPSS. my goal is to generate a labgroup with a versatile skill set, where stu-dents can engage in peer mentoring andinstruction to emulate real-world researchgroups in which scientists are invited tocollaborate based on their unique contri-butions to a given project. Second, numer-ous classroom opportunities to designstudies, prepare IRB applications, collectand analyze data, practice scientific writ-
ing, and, perhaps most crucially, engage inscholarly discussion and debate regardingresearch, all serve to prepare students wellfor research collaboration. For instance,my (advanced) research methods in clini-cal psychology course (a 3-hour coursewith a 3-hour weekly lab component) is alargely discussion-based course thatinvolves critical review of the researchmethods and scholarship in the discipline.the curriculum itself therefore teaches stu-dents essential research, critical thinking,and communication skills that are usefulfor their work in faculty research labs or fortheir postgraduation endeavors. Group-based research projects teach them aboutthe complexities of psychological assess-ment (indeed, none of my students seemsto fully grasp the inherently complexnature of scale development until they readClark and Watson’s 1995 paper!), the rig-orous, time-consuming nature of research,the inevitable errors and need for transpar-ent reporting of these errors, the tempta-tion to take shortcuts and the ethicalresponsibility to avoid doing so, and, ofcourse, the benefits and challenges ofworking as part of a research team. third,SLACs are rooted in multidisciplinaryknowledge and lend themselves readily tocollaboration across diverse areas of study.For instance, my lab initially designed anew study comparing images of “over-weight” individuals engaging in positive(e.g., eating vegetables, exercising) andnegative (e.g., eating junk food, napping)stimuli to see if exposure to positive mediamight result in more favorable attitudestoward weight antidiscrimination legisla-tion. Although we had immersed ourselvesin relevant psychology literature, it wasonly when we consulted one of my col-leagues, an American Studies andWomen’s, Gender, and Sexuality Studiesscholar who is an expert on fat stigma, thatwe understood the inherently stigmatizingnature of our experimental design (i.e.,assumption that there is a “good-fatness”and a “bad-fatness”) and language (i.e.,“overweight” assumes that there is a“normal” weight that one is “over” and thepreferred term among fat activists is fat).Based on her recommendation, we con-sulted the multidisciplinary Fat StudiesReader (Rothblum & Solovay, 2009) andinterviewed a fat activist artist, strategiesthat helped us to significantly improve ourresearch design. throughout this process, Iwas excited to observe my RAs’ opennessand ability to integrate new knowledgewith information from their other nonpsy-chology courses. Although other academic
institutions likely do provide opportunitiesfor multidisciplinary collaboration, Ibelieve that the ease with which my stu-dents and I were able to learn from outsideour “psychology-silo” was unique to theSLAC experience.
In their summary of evidence-basedpractices for effective undergraduateresearch mentorship, Shanahan and col-leagues (2015) highlight the need to setclear, scaffolded expectations and buildcommunity among lab members. Indeed,one of the most essential components of asuccessful student-faculty research collabo-ration is a thorough lab orientation toassess the student’s knowledge and skillsand establish clear expectations. Unfortu-nately, I failed to appreciate the importanceof this step during my initial mentoringexperience in graduate school: Whilesupervising a team of undergraduateresearch assistants, I incorrectly assumedthat everyone understood the need for dili-gent and professional behavior in aresearch setting. During the data collectionphase for my dissertation, I stumbled uponone of my research assistants chattinginformally with a study participant whilethe participant completed a mood ques-tionnaire. When I followed up with theresearch assistant the next day to explainthe potential impact of her inappropriatebehavior on our data and to ask if she hadengaged in similar behavior with other par-ticipants, she denied other instances andtearfully attributed her behavior to herconsumption of alcoholic beverages athappy hour with her friends before ourdata collection session. Based on this star-tling disclosure, I made the difficult deci-sion to exclude all of her data from thestudy. Now, I make my expectations forresearch assistants explicit: Students mustcommit to a minimum of 8 hours ofresearch per week, attend (and be preparedto present at) weekly lab meetings, respondto lab emails within 24 hours, behave pro-fessionally in all research activities, com-plete assigned tasks in a timely manner,complete researcher training before com-mencing data collection, and produce workto the very best of their abilities. I alsoremind students that the stakes are higherfor research than for their regular coursework because of the opportunity to make ameaningful contribution to science, onethat other scientists may draw upon fortheir own work. moreover, once they jointhe lab, I treat them as junior colleagues(rather than undergraduate students),which helps to establish a sense of trust,responsibility, and mutual respect. When
April • 2019 99
M E N T O R I N G A N D S C H O L A R S H I P A T A S M A L L L I B E R A L A R T S C O L L E G E
1/2 page ad
Wiley-halfpage.pdf
considered research collaborators in thepursuit of scientific discovery, students areable to see the importance of their laborand need to carefully attend to detail andprioritize research activities. Finally, con-sistent with the recommendations to scaf-fold expectations and build community, Ihave adopted an apprenticeship model tohelp research assistants learn about theprocess of research from start to finishwhile fostering progressing levels of auton-omy and collaboration. After initiallyreviewing the basics for critically evaluat-ing published research, our weekly labmeetings often involve discussions aboutjournal articles, ethical issues and scientificmisconduct, issues of measurement relia-bility and validity, and practical aspects ofongoing research (e.g., data collectionissues, questions about data analysis,preparation for conference submissionsand journal articles). this model requiresthat assigned tasks be appropriate to theskill set of the student: Whereas a sopho-more might assist with literature research,annotated bibliographies, data collection,and IRB documentation, a junior mightconduct basic data analyses, draft methodsections, and assist with new project devel-
opment, and a senior might serve as labsupervisor, conduct more advanced analy-ses, and assist with drafts for conferencesubmissions and manuscripts. I encouragestudents to work in the lab for more than ayear (sometimes continuing postgradua-tion) so that they can continue to buildtheir skills, and in some cases, follow pro-jects from conception to completion.moreover, working as part of a researchteam not only serves to professionalize stu-dents, but also offers a unique opportunityfor peer mentorship, where more advancedstudents can train and supervise their morejunior peers, and thereby reduce the timecommitment for faculty supervisors.
there are, of course, costs that accom-pany working closely with undergraduateresearch assistants at a SLAC. First, thereare times when quickly approaching dead-lines may make it more expedient for fac-ulty to complete tasks themselves ratherthan assign them to student researchersand then undergo the necessary stages ofdrafting and revision. In those instances, Istill invite student researchers to offer feed-back on drafts and fill-in-the-blanks how-ever they can (such as by gathering infor-mation for different sections of the
manuscript, reviewing submission guide-lines, or formatting references) to maintainthe collaborative nature of our pursuit.Second, students often struggle to grasp thetime-span for a research project to evolvefrom initial conceptualization to publica-tion. For instance, when I was invited a fewyears ago to take the lead on two researchprojects that involved analyzing existingdatasets, one of my research assistantseagerly volunteered to take primaryresponsibility for both projects. encour-aged by her enthusiasm, I agreed to take onboth projects and we made some goodprogress by the end of the semester. how-ever, when we met the following semesterto continue our work, she indicated thatshe no longer had the time to take a leadingrole on the projects due to other commit-ments. Although I was disappointed and abit overwhelmed to realize that work wouldtherefore fall to me, I later realized that anundergraduate research assistant could notbe expected to automatically grasp thenotion that research projects are typicallymultisemester endeavors (in contrast tosemester-long classroom assignments). Iam now much more cautious about exter-nal commitments that rely heavily on the
What’s New in Wiley CognitiveBehavior Therapy 2019
Both books are available for purchase at Wiley.com
ISBN: 978-1-119-39629-1Price: $44.95
A Cognitive BehaviouralTherapy Workbookfor Adolescents andYoung Adults
ABOUT THE AUTHORPaul Stallard is Professor of Child and Family Mental Health at the University of Bath and Head of Psychological Therapies(CAMHS) for Oxford Health NHS Foundation Trust. He has worked with children and young people since qualifying as aclinical psychologist in 1980.
He is the author of “Think Good Feel Good: A cognitive Behaviour Therapy Workbook for Children and Young People”and Editor of the book series “Cognitive Behaviour Therapy with Children, Adolescents and Families”. He has contributed tothe development of CBT in many countries and has provided workshops for clinicians around the world. He is an activeresearcher and has published over 150 peer reviewed papers.
Use codeVBQ90
*Valid until31 Dec 2019
for 20% offpurchase
A M B W A N I & M I N N I C K
100 the Behavior Therapist
ongoing contributions of my undergradu-ate research assistants, but I also strive tomore clearly communicate the expectedtime line for projects. Finally, a third cost ofworking with undergraduate RAs is that allof the work must be checked carefully andcannot automatically be assumed to be cor-rect. Work will frequently include errors,even among the most experienced stu-dents. Part of the allure of working in aresearch team is that we can all serve aspeer-reviewers, ensuring that we do nothave typos or grammatical errors, that ourarguments are logical and clear, that wesubmit all of the required documentationto meet external deadlines, and that weinclude all of the measures that we want toinclude in our surveys. But how do weteach students to write in a concisemanner? how do we teach them to parsethe essential from nonessential informa-tion for a poster presentation? how do weteach them to thoroughly (rather thansuperficially) support their arguments withevidence from the research literature, andto include a balanced selection of sourcesrather than merely those that support thepoints that they want to make? It is admit-tedly sometimes tempting to just do thingsmyself, particularly when I have plannedpoorly and do not have time for extensiverevisions. however, at those times I remindmyself that I chose to pursue a career as afaculty member at a SLAC because I trulyenjoy being a teacher-scholar. And part ofthat responsibility involves facilitating thedevelopment of independent scholars whoare capable of critical thinking, scientificwriting, and honing their research and pro-fessional skills for graduate study or forentry into the workforce. moreover, weshould not underestimate the capabilitiesof undergraduate student researchers;indeed, I am often inspired by my students’ideas, thoughtfulness, and enthusiasm forscience and find opportunities to workclosely with them to be among the mostintellectually stimulating and enjoyableaspects of teaching at a SLAC.
A Student Researcher’s PerspectiveAlthough I started my undergraduate
career at a large university, I transferred toa SLAC because I was told that I wouldlikely not have an opportunity to partici-pate in student-faculty research until myjunior or senior year. this restriction ofresearch opportunities to more advancedstudents is unfortunately consistent withresearch on universities across multiple sci-entific fields (e.g., mathematics, computer
science, environmental science, etc.; Rus-sell, hancock, & mcCullough, 2007). Incontrast, within 2 months of transferring toa SLAC, I was able to join a clinical psy-chology faculty research lab and continuedto work there for my remaining 3 years atthe college.
there were several unique features tomy SLAC experience that were essential tomy research training. First, the greater stu-dent-faculty interaction stemming fromsmall class sizes helped me to learn aboutfaculty research interests and potentialmentorship styles, and gave me the courageto approach my professor about researchopportunities. I knew that my professorknew my name and likely had a sense of mycapabilities as a student, which may not beuniversally true for students at larger uni-versities. Second, I received intensive train-ing in psychology research methodology:Our curriculum required one introductoryresearch methods course, one introductorystatistics course, plus two advancedresearch methods courses in subdisciplinesof psychology (e.g., clinical psychology,cross-cultural psychology, social psychol-ogy), all of which included weekly labs andrequired completion of group-basedempirical research projects. these experi-ences not only helped me develop essentialskills in literature research and synthesis,scientific writing, and research design andanalysis, but they also taught me how towork as a part of a research team, whichresearch suggests helps students hone skillsin time management, collaboration, andcommunication (Colbeck, Campbell, &Bjorklund, 2000). For instance, when Ifound that one of my group research pro-jects was largely being completed by onlytwo of us in the group, we confronted ourother members to discuss group dynamicsand workload in an attempt to practiceeffective communication in a difficult situ-ation. Although this was a challenging con-versation, it taught me to assertivelyexpress my needs in a respectful mannerand begin to feel comfortable with beinguncomfortable. Finally, my SLAC educa-tion required me to take several coursesoutside of psychology, broadening my per-spective and helping me to understand theinteraction of multiple life factors, includ-ing psychological, biological, and socialfactors (among others; engel, 1977) inshaping the human experience. Forinstance, several of my courses focused onthe roles of culture, movement and expres-sion, and country of origin in understand-ing others (such as Introduction to LatinAmerican Studies, Dance and Culture, and
exploring German Cultures), which rein-forced the importance of cultural and envi-ronmental factors in shaping cognition,behavior, and relationships with one’sbody. moreover, part of this multidiscipli-nary education involved drawing uponexperiences outside the classroom, whetherthese were campus-wide events, residentiallife experiences, or interdepartmental col-loquia. In fact, my own research (for myundergraduate honors thesis) was inspiredby a speaker invited by the PsychologyClub, Dr. Carolyn Becker, who presentedher research on eating disorder prevention.my faculty supervisor and I collaboratedwith various campus constituents to orga-nize our first Fat talk Free Week (based onDr. Becker’s research) and when I observedthat many of my peers failed to take theprogramming seriously, I decided to inves-tigate the impact of these types of conver-sations on our student community. As myresearch was directly connected to campusprogramming, I was also able to solicitfunding from the Dean of Students Office(not a typical source for research funding),which further highlights the interactionbetween administration, cross-disciplinarycampus events, and student scholarship ata SLAC.
I benefited from several structures thatmade my student-faculty research experi-ence a positive one. First, my lab orienta-tion helped me to understand the expecta-tions for my work and the risk ofproducing and disseminating low-qualityinformation to other researchers and thegeneral public. Being treated as a junior sci-entist also fostered my investment in thelab’s research, and as the experience pro-gressed, I observed a shift in my prioritiestoward scheduling more time for researchduties and taking initiative to pursue addi-tional lab responsibilities. For instance, Ivolunteered to take the lead on a posterpresentation and worked late on severalevenings to draft and revise the posterbased on suggestions from my faculty advi-sor. had this merely been a classroomassignment, I would have just completedthe work and gone to bed at my usual time,but I was very invested in this poster pre-sentation (as an investment in my profes-sional development) and took a moremeticulous approach toward its comple-tion. my identity as a junior scientist wasalso fostered by attending and presentingour lab’s research at national and interna-tional scientific conferences, opportunitiesthat were made possible by student presen-tation travel grants through my SLAC.through these experiences, I learned about
April • 2019 101
M E N T O R I N G A N D S C H O L A R S H I P A T A S M A L L L I B E R A L A R T S C O L L E G E
the professional research community, chal-lenged myself to initiate conversations withscholars whose work I admired (even whenI found the prospect to be very intimidat-ing), and honed my skills in critical think-ing, scientific writing, and, perhaps mostimportant, verbal communication of scien-tific research in a clear, concise manner;these accomplishments have all been iden-tified as learning gains of undergraduateresearch training (Lopatto, 2004). Finally,the apprenticeship structure employed bymy faculty supervisor helped me to learnabout the scientific process in a mannerthat was personalized, developmentallyappropriate, and manageable. For instance,I transitioned from initially conducting lit-erature reviews and serving as a seconddata coder on a qualitative research projectduring my sophomore year; to assistingwith set-up, data collection, and technolog-ical troubleshooting for an ecologicalmomentary assessment study during myjunior year; to serving as lab coordinator,training, scheduling, and mentoring otherresearch assistants, and managing the pro-ject budget (in addition to conducting myown honors thesis research) during my
senior year. At the end of a research train-ing experience, both students and mentorsindicate significant improvements inresearch skills (Kardash, 2000), and at theend of my 3-year undergraduate researchassistant experience, I felt confident in myfoundational knowledge about scientificprinciples and research methodology andprepared for my current program of gradu-ate study in clinical psychology.
I also faced several challenges as anundergraduate researcher, some of whichmay offer useful guidance for aspiring stu-dent researchers at SLACs. For instance, Istruggled to critique scientific literature(who was I to identify limitations and cri-tique published work?) and found it diffi-cult to write in the clear, concise, andsomewhat repetitive manner valued by thesciences, which frequently contrastedexpectations for writing in my nonpsychol-ogy courses. During these times, I found itparticularly helpful to discuss the pros andcons of journal articles as a lab group and toreceive specific feedback on my writingstyle. For instance, my supervisor wouldsometimes rewrite a few of my sentences todemonstrate scientific writing, and I would
then use those sentences to guide the rest ofmy revisions. She also reviewed multipledrafts of posters and papers and pushed meto ask questions of my writing: Were myideas connected and coherent? Were myhypotheses and conclusions supported bythe research? And, perhaps most impor-tant, did I convince the reader that theresearch was worthy of consideration byproviding a strong argument to the all-important "so what?" question? Consistentwith previous research (Kardash, 2000),this training strengthened my ability tocontextualize research findings and advo-cate for the importance of our study results.to that end, I would recommend thatundergraduate students embrace criticalfeedback and recognize that drafts repletewith tracked-changes and editorial ques-tions are acts of thoughtfulness and com-mitment on the part of the research super-visor to facilitate your professional growth.Second, I also struggled to anticipate possi-ble sources of error in the process ofresearch. For example, when I discoveredthat a participant had unexpectedly takenthe food stimuli after completing ourexperiment, I was caught off-guard and
A M B W A N I & M I N N I C K
102 the Behavior Therapist
had to determine not only how to handleher data, but also how to prevent this situa-tion with future participants. I wouldtherefore recommend that undergraduateresearch assistants talk to their supervisorsabout unexpected situations or difficultiesstemming from their own research so therecan be a preemptive discussion of possibleerrors. they may also find it helpful toapproach research with a flexible stance,accepting that error is an inevitable part ofthe scientific process and that knowledge isgleaned cumulatively, rather than solelyfrom any one study. Finally, I found it dif-ficult to learn how to treat my research-related mistakes as opportunities forgrowth and I greatly appreciated that mysupervisor approached errors calmly andcompassionately. For instance, I was mor-tified when I accidentally deleted a variablefrom one of our datasets, but once I gath-ered the courage to tell my supervisor, sheexpressed concern but did not make mefeel bad or incompetent. Instead, shereviewed the dataset with me to under-stand how the error occurred and we devel-oped a plan to prevent future problems.this experience taught me that it is accept-able to occasionally make mistakes (as longas we can document them) and that we canuse these errors as learning tools ratherthan as indicators of scientific unworthi-ness or failure. Reflecting upon this experi-ence, I encourage student researchers topush past fear to frankly and precisely dis-close mistakes to their mentors so that theycan work collaboratively toward solving(and preventing) problems. I also urgeadvisors to approach errors in a compas-sionate manner similar to my advisor, as aharsher response may have dissuaded mefrom pursuing a career as an academic psy-chologist. In the future, I hope to adopt thesame approach to supervising studentresearchers to foster their learning andsense of self-efficacy in research.
Conclusionthe purpose of the current report was
to describe some of the opportunities, chal-lenges, and recommended steps for con-ducting student-faculty research in psy-chology at a SLAC. We posit that SLACsare uniquely positioned to provide facultylabs with undergraduate research assistantswho have received extensive classroominstruction in research methodology, andthe small class sizes and multidisciplinaryfocus foster student-faculty rapport andcreative approaches to investigating ques-tions relevant to clinical psychology.
Although working with undergraduateresearchers does pose unique challenges,certain structures are likely to reduceburden on faculty time and increase thelikelihood of positive outcomes. moreover,for teacher-scholars at SLACs, student-fac-ulty collaborative research offers an idealopportunity to mentor emerging scholarsand simultaneously benefit from theirimportant (and personally rewarding) con-tributions to the lab. We hope that sharingthe perspectives of both the faculty mentorand student will encourage student-facultyresearch endeavors at SLACs as well as atlarger institutions. Future investigationsmay focus on examining institutional bar-riers to these opportunities as well as alter-nate approaches to undergraduate researchmentorship and training. this informationcould help establish best practices for men-toring undergraduate students into thenext generation of scientific researchersand psychologists.
Dix, A.C. (2010). mentoring undergrad-uate researchers: An exploratory study ofstudents’ and professors’ perceptions.Mentoring & Tutoring: Partnership inLearning, 18, 269-291. doi:10.1080/13611267.2010.492945
Brewer, G., Dewhurst, A.m., & Doran, D.(2012). Undergraduate research projects:Practice and perceptions. PsychologyLearning and Teaching, 11, 208-217.http://dx.doi.org/10.2304/plat.2012.11.2.208
Clark, L.A., & Watson, D. (1995). Con-structing validity: Basic issues in objec-tive scale development. PsychologicalAssessment, 7, 309-319.
Colbeck, C. L., Campbell, S. e., & Bjork-lund, S. A. (2000). Grouping in the dark:What college students learn from groupprojects. Journal of Higher Education, 71,60-83.
Detweiler-Bedell, J.B., Bodenlos, J.S. &Friedman-Wheeler, D.G. (2016). theundergraduate researcher: Why, when,and how to collaborate with your stu-dents. the Behavior Therapist, 39, 193-205.
engel, G. L. (1977). the need for a newmedical model: A challenge for biomedi-cine. Science, 196, 129-136.
evans, S.e., Perry, A.R., Kras, A., Gale,e.B., & Campbell, C. (2009). Supervisingand mentoring undergraduates: A gradu-ate student perspective. the BehaviorTherapist, 32, 77-82.
hunter, A. B., Laursen, S. L., & Seymour,e. (2007). Becoming a scientist: the role
of undergraduate research in students'cognitive, personal, and professionaldevelopment. Science Education, 91, 36-74.
Kardash, C. m. (2000). evaluation ofundergraduate research experience: Per-ceptions of undergraduate interns andtheir faculty mentors. Journal of Educa-tional Psychology, 92, 191-201.
Lopatto, D. (2004). Survey of undergradu-ate research experiences (SURe): Firstfindings. Cell Biology Education, 3, 270-277.
morales, D.X., Grineski, S.e., & Collins,t.W. (2017). Faculty motivation tomentor students through undergraduateresearch programs: A study of enablingand constraining factors. Research inHigher Education, 58, 520-544. doi:10.1007/s11162-016-9435-x
Rothblum, e. & Solovay, S. (eds.). (2009).The fat studies reader. New York: NewYork University Press.
Rowlett, R.S., Blockus, L., & Larson, S.(2012). Characteristics of excellence inundergraduate research (COeUR). thebenefits of undergraduate research,scholarship, and creative activity. In N.hensel (ed.), Characteristics of excellencein undergraduate research (pp. 2-19).Washington, DC: Council on Under-graduate Research.
Shanahan, J.O., Ackley-holbrook, e., hall,e., Stewart, K., & Walkington, h. (2015).ten salient practices of undergraduateresearch mentors: A review of the litera-ture. Mentoring & Tutoring: Partnershipin Learning, 23, 359-376.doi:10.1080/13611267.2015.1126162
thiry, h., & Laursen, S.L. (2011). the roleof student-advisor interactions inapprenticing undergraduate researchersinto a scientific community of practice.Journal of Science Education and Tech-nology, 20, 771-784.
Van Vliet, K.J., Klingle, K.e., & hiseler,L.e. (2013) the mentorship of under-graduate students in counselling psychol-ogy research. Counselling PsychologyQuarterly, 26, 406-426. doi:10.1080/09515070.2013.844095
. . .
the authors do not have any conflicts ofinterest or funding to disclose.Correspondence to Suman Ambwani,Department of Psychology, DickinsonCollege, P.O. Box 1773, Carlisle, PA [email protected]
April • 2019 103
Celebrat ing Our 47th Year
Steven T. Fishman, Ph.D., ABPP | Barry S. Lubetkin, Ph.D., ABPPDirectors and Founders
Since 1971, our professional staff has treated over 30,000 patients with compassionate, empirically-based CBT.Our specialty programs include: OCD, Social Anxiety Disorder, Panic Disorder, Depression, Phobias, PersonalityDisorders, and ADHD-Linked Disorders, and Child/Adolescent/Parenting Problems.Our externs, interns, post-doctoral fellows and staff are from many of the area’s most prestigious universitiesspecializing in CBT, including: Columbia, Fordham, Hofstra, Rutgers, Stony Brook, St. John’s, and YeshivaUniversities.
Conveniently located in the heart of Manhattan just one block from Rockefeller Center. Fees are affordable,and a range of fees are offered.
New York CityINSTITUTE for BEHAVIOR THERAPY
For referrals and/or information, please call: (212) 692-928820 East 49th St., Second Floor, New York, NY 10017e-mail: [email protected] | web: www.ifbt.com
BeFORe ACCePtING A POSItION as a corefaculty member with a Psy.D. program, myprofessional training occurred exclusivelyin environments operating from a scien-tist-practitioner model. In addition toengagement in direct research activities,coursework in my graduate training prior-itized empirical literature and clinicaltraining highlighted science-based deci-sion-making and empirically supportedtreatments. Among students and faculty,diversity in clinical orientation was limited,generally representing a range from foun-dational empirically supported approaches(e.g., behaviorism) to approaches that werein earlier stages of evaluation at the time,such as third-wave behavioral therapies.
While emphases varied and the requisitestrengths and weaknesses were taught, I donot recall the scientist-practitioner modelbeing seriously questioned. my trainingcontinued with a postdoctoral fellowship asa project director of a treatment outcomestudy examining an empirically supportedtreatment. When it came time to apply foracademic positions, my professional expe-riences and the competitiveness of the aca-demic job market led me to apply to a widerange of openings. After spending 3 yearsdoing clinical research, I believed my expe-riences were well suited for both research-and practice-focused programs. A combi-nation of personal and professional reasonsled me to accept a position as a core faculty
member with a Psy.D. program that oper-ates from a practitioner-scholar model andpossesses a lot of professional diversityamong the faculty. Although I was aware atthe time that this would be a different envi-ronment than I was used to, I did not antic-ipate the challenges and rewards that enter-ing a workplace with a high degree ofprofessional diversity would bring.
the scientist-practitioner (based on theBoulder model) and the practitioner-scholar (based on the Vail model; e.g,Stoltenberg et al., 2000) models bothinclude training on the science and practicecomponents of psychology. many similar-ities exist across program types, and thedifferences lie more in the emphasis of thetraining than the activities themselves. Sci-entist-practitioner programs emphasizethe production of research in addition tothe prioritization of empirical findings indecision-making. While practitioner-scholar programs may involve a researchproduction component as well, the empha-sis is typically more on the consumption ofresearch and integration, along with otherfactors, into clinical decision-making andthere are typically lower research produc-
Reflections and Advice Related to the Transitionto a Practitioner-Scholar Training Environment:The Challenges and Rewards of Working as Partof a Professionally Diverse TeamLisa S. Elwood, University of Indianapolis
104 the Behavior Therapist
E L W O O D
tion expectations. Although graduatesfrom both types of programs end up work-ing in a wide range of professional posi-tions, a larger number of academic andresearch positions are comprised of indi-viduals with scientist-practitioner trainingand the majority of graduates from practi-tioner-scholar programs end up in applied,practice positions. While Ph.D. programsprimarily belong to the Council of Univer-sity Directors of Clinical Psychology(CUDCUP), which identifies with the sci-entist-practitioner model, most Psy.D. pro-grams and practitioner scholar programsare members of the National Council ofSchools and Programs of Professional Psy-chology (NCSPP). Although APA hasembraced the evidence-based practice(eBP) movement, evidence-based practiceconceptualizations include three parts:research evidence, clinician expertise, andclient characteristics, culture, and prefer-ences (APA Presidential task Force onevidence-Based Practice, 2006). Similar totraining approaches, models that vary inthe prioritization of these components canfall under the larger evidence-based prac-tice umbrella. For example, those prioritiz-ing the science component generally sup-port models that emphasize the quality ofempirical findings (see tolin, mcKay,Forman, Klonsky, & thombs, 2015, for aconsideration of a revised approach toempirically supported treatments [eSts]and Lilienfeld, Lynn, & Bowden, 2018, for acall for science-based practice). Alterna-tively, practitioner-focused models oftenprioritize individual client characteristics,clinician expertise, and the applicability ofresearch findings to the client and setting.For example, NCSPP endorses a local clin-ical scientist model (Peterson, Peterson,Abrams, & Stricker, 2006; Stricker & trier-weiler, 1995). Although both models con-sider the same components, the variationin emphases can result in markedly differ-ent conclusions. For the purposes of thisarticle, I will use the evidence-based prac-tice term to refer to decision-makingstrategies that are influenced by scholar-ship and experience broadly, without anemphasis on original and empirical/quan-titative research, and science-based prac-tice to refer to decision-making strategiesthat prioritize empirical/quantitativeresearch.
Although not incorporated into theprofessional identities themselves, scien-tist-practitioner and practitioner-scholarprograms also frequently differ in the theo-retical orientations represented. Scientist-practitioner models line up well with the
goal of identifying empirically supportedtreatments and often emphasize cognitivebehavioral therapy and other orientationsthat are well represented in research. Prac-titioner-scholar programs often include awider variety of theoretical orientations, agreater representation of orientations thatare less commonly represented in research,and an increased emphasis on the utiliza-tion of multiple orientations through inte-grative or eclectic practices. Our programcurriculum currently includes requiredstudent coursework in five clinical orienta-tion courses: cognitive, behavioral/learn-ing, humanistic, psychoanalytic/psychody-namic, and family systems. many facultymembers are licensed and courses aretaught by individuals trained, and oftenpracticing, in the orientation that is pre-sented. Academic freedom is valued andinstructors are allowed to teach theircourses in a manner consistent with theirphilosophy of teaching and professionalvalues. Consequently, students areexposed to different, and likely contradic-tory, information and interpretationsthroughout their training. All studentsmust pass each of the classes, thus gaining abasic familiarity with each approach. Asstudents proceed through the program, it isanticipated that students will begin todevelop their professional identities,including their preferred theoretical orien-tation. While many graduates identify aprimary orientation from which they prac-tice, others practice from a variety ofapproaches. Subsequently, our programincludes faculty and students with a widerange of approaches to clinical work. thetransition from largely homogeneous pro-fessional circles to one that embraces andcelebrates heterogeneity initiated consider-ation of my own professional identity. As Ireflect on the experience, I notice similari-ties between my personal journey and the-ories of intergroup contact and biases (e.g.,Dovidio, Gaertner, & Saguay, 2009; Petti-grew & tropp, 2006) and adolescent iden-tity development (e.g., marcia, 1966;Stephen, Fraser, & marcia, 1992).
One of the first things that happenedwhen I began working with individualsfrom different professional backgrounds isthat I became aware of my prior assump-tions about “the other,” specifically non-sci-entist-practitioners and individuals of dif-ferent theoretical orientations. Whileoperating in fairly homogeneous profes-sional groups, it was difficult to imagine theperspective of others who do not prioritizethe quantitative research process and resultsof randomized controlled trials. It was easy
to think of professionals with different per-spectives as outdated, uninformed, or evennegligent. Although a latent belief, I gener-ally presumed that the scientist-practitionermodel carried innate appeal and that expo-sure to and understanding of researchshould be sufficient for one to adopt a com-mitment to science-based practice. how-ever, consistent with intergroup contacttheory (e.g., Pettigrew & tropp, 2006), asmy interactions with individuals with differ-ing professional models and orientationsincreased, my views of the other changed aswell. my interactions revealed intelligent,well-trained, ethical, and caring cliniciansrepresenting a variety of training modelsand orientations and possessing a widerange of views of the role of research. Addi-tionally, as I began to work closely with indi-viduals from the other group, I realized thatwe shared similar opinions on many issuesthat were important to me. thus, an initialstep in my growth process was to realize thatthere were many similarities between mygroup and the others and that both groupscontained a wide variety of individuals.
As my exposure to alternative view-points increased and I began to understandsome of the arguments raised, I foundmyself critically evaluating my viewpoints,engaging in self-reflection, and in the midstof a mini professional identity crisis. expo-sure to critiques of the empirically sup-ported treatment literature revealed somechallenging and valid points (e.g., Westen,Novotny, & thompson-Brenner, 2004). Iconsidered points raised regarding statisti-cal versus clinical significance, dropoutrates, and the influence of researcher alle-giance. Furthermore, consideration ofchallenges to the research and publicationprocess, such as publication bias, the filedrawer problem, and the subjectivity that isinvolved in the peer review process reveallegitimate concerns. Regardless of an indi-vidual’s commitment to the researchprocess, it seems impossible to ignore someof the weaknesses of the current system.
Consideration of these points led toquestioning if my scientist-practitioneridentity was one that I critically consideredand chose, or if it was a consequence ofadopting my professional parents’ valuesand practices. Although it may haveoccurred, I do not recall ever intentionallyconsidering alternative perspectives beforechoosing an orientation. I wondered if Ineglected to question or examine my viewsbecause the environment in which I devel-oped as a professional maintained a scien-tist-practitioner focus. Additionally, I con-sidered how challenging it would be to
April • 2019 105
P R A C T I T I O N E R - S C H O L A R T R A I N I N G E N V I R O N M E N T
spend considerable time, effort, and profes-sional resources investing in and success-fully practicing a treatment approach, onlyto be told by other professionals later that Ineeded to abandon my learned skills andexpertise and essentially start over with anew approach. It is easy for me to imaginea scenario in which I would be the one whowould be skeptical of alternative ap-proaches, even as they gained professionaland empirical support.
my reflection process ultimately led meto reaffirm my commitment to the scien-tist-practitioner approach and science-based practice. my professional commit-ment to the field and to the best interest ofpatients leads me to prioritize clientsreceiving treatment that is well suited fortheir needs, gives them the best chance atrecovery and improved quality of life, andthat will reduce symptoms as quickly aspossible. Despite the flaws in the researchand publication processes, I continue tobelieve that research is an essential tool formaking decisions about treatment choice.however, I have come to believe that theperspectives of both researchers and practi-tioners have strengths and weaknesses andthat dialogue, communication, and collab-oration across groups will strengthen bothresearch and practice. Research being con-ducted related to dissemination and imple-mentation provides some encouragingexamples of what can develop from suchpartnerships (e.g., Becker, Stice, Shaw, &Woods, 2009).
As my beliefs solidified I found they alsoevolved. For example, rather than viewingmyself as an individual who is committedto a specific treatment approach, I realizedthat my larger commitment is to providingbest practice treatments based upon theavailable data. therefore, I must remainopen and prepared to participate in addi-tional training and alter my approach ifneeded in order to provide the best avail-able services to my clients and education tomy students. Additionally, I consideredthat my commitment to science-basedpractice should not be restricted to mytreatment choices. I felt challenged tobecome more familiar with best practicesin teaching and to aim for science-basedteaching, as well.
my role as a faculty member involved inthe training of future psychologists chal-lenges me to consider how I interact withstudents in my generalist environment. Irealized my goal for my students is thatthey think critically and make informeddecisions based on available data. Ulti-mately, it is important to me that their deci-
sions are made thoughtfully, that they con-sider available evidence and theory, andthat they are able to justify their choices.Combined with the opportunity to developand teach an evidence-based practicecourse, I found myself considering how topromote critical thinking, informed deci-sion-making, and, hopefully, science-basedpractice in students who enter with a rangeof intrinsic interests and initial affiliations.As I consider my experiences, I amreminded that, cliché as it may be, my stu-dents are here because they genuinely dowant to help people. they are bright indi-viduals who are committed to their train-ing and want to do what is best for theirclients. If they come to believe that practic-ing in a science-based manner is in the bestinterest of their clients and we sufficientlyprepare them to do so, they will adopt theapproach and carry it with them into prac-tice. Furthermore, receiving a theoreticallydiverse training experience may result inthe students participating in the profes-sional identity development process earlyin their careers. Rather than loosely adopt-ing professional family values, our studentscan be encouraged to engage in a profes-sional moratorium (i.e., exploration ofoptions and preparation for making a com-mitment; marcia, 1966) and progresstowards their professional identities earlier.
Finally, I find my reflections returning tomy decision to accept the position with mycurrent program. Prior to joining the facultyhere, I had very little exposure to or knowl-edge of Psy.D. programs. the information Ihad heard primarily highlighted weaknessesof some versions of the model. As I consid-ered accepting the position, I nervouslywondered how my mentors and colleagueswould view the decision. Although thespecifics are a little blurry at this point, Irecall a conversation with a valued andrespected mentor. to my surprise, heresponded positively to the decision, andnoted that it is also important for emergingclinicians to be trained in critical thinkingand that the education provided could havean impact on those who are providing thebulk of the clinical services in our field.Rather than viewing the choice as a compro-mise, he spoke of it as an opportunity.
As I gain experience in my position, Ihave been pleased to observe the profes-sional development of our students. I haveheard students discuss the disconnect (attimes) between the classroom and the fieldand express desire for more supervision ineSts and science-based practice while intheir training. I have had the opportunityto watch students in our program progress
through their development and join us inmentoring through roles as teachers andsupervisors and begin to fill some of thegaps they observed. Some of my proudestmoments have been hearing my studentsdescribe engagement in difficult conversa-tions with other professionals about theutilization of clinical practices that are notsupported by research. Consistent with thediversity of the environment, though, Ihave also observed highly competent stu-dents make different choices than I wouldand have been challenged to respect thosedecisions also.
there are times when I tire of feeling theneed to argue for positions that wouldnever be questioned in other environmentsand long for the simplicity of being part ofa more unified group. While it would beeasier in many ways, I know that the diver-sity of my recent environment hasexpanded my views and resulted in a moremature and intentional professional iden-tity. I have also come to believe that as afield, we have a lot we can learn from eachother and that increased collaborationbetween individuals with varying empha-ses within the evidence-based practicemodel will be beneficial for our field inboth the research and practice domains.While not a new idea, it is one that remainsrelevant, as evidenced by Behavior Ther-apy’s decision to republish in 2016 an arti-cle on bridging the gap between scientistsand practitioners that was originally writ-ten in 1996 (Sobell, 1996, 2016). morerecent publications written by leaders fromdifferent perspectives have come to similarconclusions about the need for increasedcollaboration (e.g., Lilienfeld et al., 2013;mcWilliams, 2017). In the end, I havedecided that as comfortable as it may be toremain in professionally homogeneousenvironments, there is much to gain fromcommunication and participation in gen-eralist training teams, both for individualsand the field.
As I enter mid-career stage and reflecton my journey thus far, I hope that consid-erations of my experiences may be useful toothers in the field, particularly those enter-ing theoretically diverse professional envi-ronments or practitioner-scholar pro-grams, and offer a few pieces of advice.First, I recommend focusing on the simi-larities, including shared goals and values,before the differences. even if you may notagree on the exact strategy to get there, itcan be reassuring to realize the members ofyour team are all working towards the samegoals (e.g., training high-quality clinicians).Second, become comfortable with areas of
106 the Behavior Therapist
E L W O O D
respectful disagreement, particularly forless important issues. Rather than viewingdisagreements as battles to be won, learnwhen to step away from topics and justaccept the possession of different view-points. third, be open to discussion andconsideration of alternate viewpoints. Rec-ognize the likelihood that other approachesmay possess some knowledge, strengths,and skills that may be missing from yourstandard approaches. It may be useful toidentify methods of having these conversa-tions that increase the likelihood of success.I, personally, have found some individualsin my program who describe differentviewpoints than mine using rationales andlanguage that are familiar to me. Conversa-tions with these individuals have increasedmy understanding of the other perspective.Additionally, avoid the temptation of view-ing your own perspective as a panacea. Ibelieve our field would benefit from anincreased willingness to acknowledge limi-tations, recognition of instances when anapproach is not the best option, willingnessto acknowledge when very differentapproaches may be more useful, and com-fort referring accordingly. Gain practicecommunicating with others, especiallytrainees, in a way that clearly communi-cates personal beliefs without criticizingalternatives. Finally, identify mentors andpeers with similar experiences to yours.the normalization and validation of expe-riences, combined with advice whenappropriate, can provide a sense of sup-port, guidance, and hope during tensemoments. I am hopeful that members frommany different perspectives in our field willanswer the call for increase communica-tion and collaboration, and that the resultwill be a stronger field.
ReferencesAPA Presidential task Force on evidence-
Based Practice. (2006). evidence-basedpractice in psychology. American Psychol-
Becker, C. B., Stice, e., Shaw, h., & Woda, S.(2009). Use of empirically supportedinterventions for psychopathology: Canthe participatory approach move usbeyond the research-to-practice gap?Behaviour Research and Therapy, 47, 265–274. http://dx.doi.org/10.1016/j.brat.2009.02.007
Dovidio, J. F., Gaertner, S. L., & Saguay, t.(2009). Commonality and the complexityof “we”: Social attitudes and social change.Personality and Social Psychology Review,13, 3–20. doi: 10.1177/1088868308326751
Lilienfeld, S. O., Lynn, S. J., & Bowden, S. C.(2018). Why evidence-based practice isn’tenough: A call for science-based practice.the Behavior Therapist, 41, 42–47.
Lilienfeld, S. O., Ritschel, L. A., Lynn, S. J.,Brown, A. P., Cautin, R. L., Latzman, R. D.(2013). the research-practice gap: Bridg-ing the schism between eating disorderresearchers and practitioners. Interna-tional Journal of Eating Disorders, 46, 386-394. doi: 10.1002/eat.22090
marcia, J. e. (1966). Development and vali-dation of ego-identity status. Journal ofPersonality and Social Psychology, 3, 551 –558. http://dx.doi.org/10.1037/h0023281
mcWilliams, N. (2017). Integrative researchfor integrative practice: A plea for respect-ful collaboration across researcher andclinician roles. Journal of PsychotherapyIntegration, 27, 283 – 295.http://dx.doi.org/10.1037/int0000054
Peterson, R. L., Peterson, D. R., Abrams, J.C., & Stricker, G. (2006). the NationalCouncil of Schools and Programs of Pro-fessional Psychology education model.Training and Education in ProfessionalPsychology, S, 17–36.
Pettigrew, t. F., & tropp, L. R. (2002). Ameta-Analytic test of intergroup contacttheory. Journal of Personality and SocialPsychology, 90, 751–783.http://dx.doi.org/10.1037/0022-3514.90.5.751
Sobell, L. C. (1996). Bridging the gapbetween scientists and practitioners: the
challenge before us. Behavior Therapy, 27,297–320. http://dx.doi.org/10.1016/S0005-7894(96)80019-0.
Sobell, L. C. (2016). Bridging the gapbetween scientists and practitioners: thechallenge before us. [Republished article].Behavior Therapy, 47, 906-919. doi:10.1016/j.beth.2016.11.007
Stephen, J., Fraser, e., & marcia, J. e.(1992). moratorium-Achievement(mama) cycles in lifespan identity devel-opment: Value orientations and reasoningsystem correlates. Journal of Adolescence,15, 283–300. http://dx.doi.org/10.1016/0140-1971(92)90031-Y
Stoltenberg, C. D., Pace, t. m., Kashubeck-West, S., Biever, J. L., Patterson, t., &Welch, I. D. (2000). training models incounseling psychology: Scientist-practi-tioner versus practitioner-scholar. TheCounseling Psychologist, 28, 622–640.http://dx.doi.org/10.1177/0011000000285002
Stricker, G., & trierweiler, S. J. (1995). thelocal clinical scientist: A bridge betweenscience and practice. American Psycholo-gist, 50, 995–1002. http://dx.doi.org/10.1037/0003-066X.50.12.995
tolin, D. F., mcKay, D., Forman, e. m.,Klonsky, e. D., & thombs, B. D. (2015).empirically supported treatment: Recom-mendations for a new model. Clinical Psy-chology Science and Practice, 22, 317–338.http://dx.doi.org/10.1111/cpsp.12122
Westen, D. Novotny, C. m., & thompson-Brenner, h. (2004). the empirical statusof empirically supported psychotherapies:Assumptions, findings, and reporting incontrolled clinical trials. Psychological Bul-letin, 130, 631–663. http://dx.doi.org/10.1037/0033-2909.130.4.631
. . .
the author has no conflicts of interest orfunding to disclose.Correspondence to Lisa S. elwood, Ph.D.,School of Psychological Sciences, Universityof Indianapolis, Indianapolis, IN [email protected]
Did you knowyour membershipgives you free onlineaccess to our journalsBehavior Therapyand Cognitive andBehavioral Practice?
Students Ô First, access your ABCT Journal Access ID, whichis printed on the top left of the mailing label on
your journal mailings and tBT newsletter ORavailable online when you log in atwww.abct.org (and then click on MY MEMBER
ACCOUNT). You can also use the ID and passwordfinder on ABCT’s website.
Ô Enter your Journal Access ID at:https://www.sciencedirect.com/science/activate/abct
April • 2019 107
ChILDReN ReCeIVe meNtAL heALth ser-vices from schools more often than fromany other service system (Adelman &taylor, 2010; Burns et al., 1995; Farmer,Burns, Phillips, Angold, & Costello, 2003;hoagwood et al., 2007). Schools are in aunique position to provide mental healthintervention because parents and schoolstaff are often the first to notice youthmental health issues (Loades & mastroy-annopoulou, 2010). School-based mentalhealth interventions increase the accessibil-ity of services to youth and help decreasebarriers to mental health care (Owens et al.,2002; Weist, Lever, Bradshaw, & Owens,2014). School providers also have theadvantage of potentially communicatingwith and observing a student’s interactionswith peers, teachers, and parents, as well astheir academic functioning more easilythan community-based providers, whoseservices are often limited to outpatient clin-ics (mennuti & Christner, 2005). Becauseyouth spend the majority of their days inschool, an understanding of school ecologyalso enables effective mental health treat-ment regardless of the setting in whichyouth are treated.
We outline the unique position ofschool psychologists, at both the master’sand doctoral levels, to provide and influ-ence the use of cognitive behavioral ther-apy (CBt) in school settings. the use ofCBt in schools and school psychology as adiscipline are described and applied exam-ples provided.
CBT in SchoolsCBt has been shown to be effective in
the treatment of numerous childhood dis-orders (Kazdin & Weisz, 1998; Ollendick &King, 2004; Weisz & Kazdin, 2010, 2018)and has been advocated for use withinschool settings (hoagwood & erwin, 1997;mennuti & Christner, 2013). CBt fits wellwith the existing structure and culture oftraditional school settings, which may helpto increase its acceptance by school staff(mennuti & Christner, 2005). the struc-ture of CBt is familiar to both students and
educators: agenda setting, psychoeduca-tion, in-session practice, and the assigningof practice or homework are already com-monplace within education systems (men-nuti & Christner, 2005). CBt protocols arerelatively short in duration, adaptable forindividual youths’ current needs, and solu-tion-focused (Reinecke, Dattilio, & Free-man, 2003), allowing providers working inschools to utilize CBt on three differentlevels: prevention, early identification, anddirect service to youth (mennuti & Christ-ner, 2013). CBt also works well withinschools because it is often more time-lim-ited than other approaches, and time isoften tightly constrained at schools, bothwithin the day and across the academicyear (mennuti & Christner, 2005).
School Psychologythe field of school psychology encom-
passes the delivery of psychological servicesand supports to children and adolescents,often (although not solely) in schools, par-ticularly with regards to students’ academicgoals and learning. School psychologistscan hold either a master’s degree with aspecialist license, with which they can prac-tice in schools, or a doctoral degree, withwhich they can become a licensed psychol-ogist through the same avenues that Ph.D.sin clinical or counseling psychology or doc-torates in psychology (Psy.D.) becomelicensed. Practice settings for doctoral-levelschool psychologists vary immensely, fromtraditional school settings, to academicpositions, community mental health set-tings, private practices, and pediatric psy-chology settings, such as hospitals, primarycare, and specialty care clinics.
In practice, master’s-level school psy-chologists typically work in schools, assess-ing students for learning difficulties andcoordinating a variety of services to sup-port students’ academic success and psy-chological functioning. these services caninclude direct psychological services, iden-tifying and implementing specialized pro-grams targeting specific academic skills,and coordinating services among general
and special education teachers, schoolcounselors and social workers, families,and community-based services. Generally,school psychologists working withinschools do not administer interventionsthemselves and instead provide recom-mendations for interventions and consul-tation to specialists or teachers implement-ing them. In fact, school psychologists arethe only professional psychologists specifi-cally trained in indirect service delivery(D’Amato, Zafiris, mcConnell, & Dean,2011). Behavioral consultation with teach-ers is a core practice of school psychologiststhat is rooted in learning theory to identifythe function of student behaviors in class-rooms and design an intervention toresolve the problem (Sheridan & Kra-tochwill, 2007). School consultation oftenalso incorporates other evidence-basedpractices, such as motivational interview-ing, to address teachers’ ambivalence aboutchange (holdaway & Owens, 2015; Reinke,herman, & Sprick, 2011).
historically, school psychologists inschool settings have focused on the popula-tion of students served by Section 504 andspecial education services. more specifi-cally, the school psychologists’ role focusedon assessing whether students qualify toreceive those services, and coordinatingwith school personnel to deliver them, pri-marily in response to an increasing legaldemand to serve students with disabilitiesas mandated by the Individuals with Dis-abilities education Act (IDeA) of 1990.Because of increased demand for individ-ual assessments for services, school psy-chologists spent much more of their timein the 1990s conducting intelligence testsand writing psychological reports detailingstudents’ eligibility for services than everbefore. Subsequent legislation—the NoChild Left Behind Act of 2001 and the re-authorization of IDeA in 2004—pushedthe field of school psychology towards aResponse to Intervention (RtI) model,whereby assessment requirements werereduced so that intervention was targetedtowards addressing individual needs beforethey could be designated as having a learn-ing disability (Ball, Pierson, & mcIntosh,2011). this expanded role means thatschool psychologists can be an importantpart of prevention by intervening withyouth who are showing some early signs ofdifficulty but do not yet have a level ofimpairment necessitating referral for ther-apy. thus, school psychologists are well-positioned to use CBt for prevention at theuniversal, targeted, and indicated levels.most practitioners of CBt come into con-
More Than Psychometricians: SchoolPsychologists as Prime Potential Disseminatorsof Cognitive Behavioral TherapiesAmanda A. Bowling, Rebecca Y. Woo, Sarah Kate Bearman,and Jessica L. Tauber, University of Texas at Austin
108 the Behavior Therapist
B O W L I N G E T A L .tact with youth only once they are alreadyexperiencing serious mental health con-cerns; school psychologists can intervene atan earlier stage and hopefully limit the neg-ative impact experienced by youth (Kra-tochwill, 2007).
Compared to their master’s-level coun-terparts, Ph.D.-level school psychologistsobtain advanced training in psychoeduca-tional and psychosocial assessment andtherapy along with additional courseworkand practice in research methods. trainingin research methodology qualifies schoolpsychologists to organize and evaluatemental health delivery systems in a varietyof contexts with validated tools. Further-more, the bulk of training for school psy-chologists focuses on the needs of childrenand adolescents and the systems of care inwhich they already operate, such asschools. even when doctoral-level schoolpsychologists are not practicing in schoolsettings, their foundational experiences inschools help them develop expertise collab-orating across disciplines with teachers,administrative personnel, and other educa-tional specialists, and working withindelivery systems of care. All of these expe-riences make school psychology traineeswell-poised to work in multidisciplinaryspaces, serving as ambassadors for psychol-ogy and evidence-based practices such asCBt in mental health.
the school psychology program at theUniversity of texas at Austin, the firstschool psychology program to be accred-ited by the American Psychological Asso-ciation, is an exemplar training model. theprogram is interdisciplinary and followsthe scientist-practitioner model in its doc-toral and master’s-level training, whichinclude the same courses in the first 2 yearsof the programs. these courses provide keyfoundations in research methodology,development, learning, family interven-tions, social/emotional and behavioralassessment, and behavioral and cognitive-behavioral mental health interventions, aswell as school psychology–specific course-work on the law, ethics, and history ofschool psychology, psychoeducationalassessment and intervention, and consulta-tion. Courses emphasize a multicultural,evidence-based lens to interventions andresearch. master’s and doctoral students allcomplete a 1-year school-based practicumand gain a diversity of experiences con-ducting assessments, consultation, anddelivering therapy in school settings. Doc-toral students take additional courses forspecialty emphases, some of which includediversity, pediatric psychology, neuropsy-
chology, academic/research, and child clin-ical.
After the initial school practicum intheir second year, doctoral students obtainvarious practicum experiences pertainingto individual interests, including in com-munity mental health clinics, school-basedtherapy clinics, and integrated behavioralhealth settings, such as a pediatric cancercenter, community primary care centers,and hospital consultation-liaison servicesfor youth and families. Since 2009, 98% ofdoctoral students who have applied tointernships obtained them and 96% ofthese internship sites were APA/CPAaccredited. Internship placement sites pre-dominantly include medical centers, inte-grated behavioral health settings, commu-nity mental health clinics, schools, andjuvenile justice centers. the perspectives ofdoctoral students within these settings areenriched by their understanding of theschool context because they have multipleexperiences coordinating within a child’smesosystem among diverse personnelfrom the school, medical clinic, and gov-ernmental agencies, such as the juvenilejustice system.
School Psychologists as Ambassadorsfor CBT in Schools
Research suggests that school psycholo-gists working in schools spend more oftheir time than they would like on writingpsychological reports and IQ testing, andless time than they would like on workingin primary and secondary screening andprevention, consultation, research andprogram evaluation, and conducting ther-apy, even after the historical push towardan RtI model (Filter, ebsen, & Dibos,2013). however, technological advances indelivering psychometric tools and the con-tracting of cheaper psychometricians toconduct psychoeducational evaluationswill likely make conducting assessmentsless of a central focus of master’s-levelschool psychologists’ jobs, such that exist-ing school psychologists may focus morecentrally on indirect services, such as con-sultation with teachers and systems-levelscreening and intervention. School psy-chologists in the future may also spendmore time doing therapy than the typicalschool psychologist in school settings cur-rently does.
Both master’s and Ph.D.-level schoolpsychologists have potentially importantand unique qualifications that would allowthem to contribute to the dissemination ofCBt. Ph.D.-level school psychologists are
particularly well trained to integrate prac-tices at the systems level and advocate forpolicy-level changes to include mentalhealth services with other school services.Ph.D.-level school psychologists can alsoinitiate collaborations between schools andlocal academic institutions, such as the Act& Adapt project (described below), to workwith school personnel in implementingCBt and evidence-based interventions. Asthose in charge of recommending, andoften coordinating, services for students,master’s-level school psychologists are inan excellent position to advocate for morestudents to receive both effective preven-tive and targeted mental health care ser-vices and to coordinate their delivery withallied providers. Additionally, their train-ing in consultation makes them uniquelyqualified to work with school counselors,social workers, and teachers to disseminateelements of CBt effectively within class-rooms and other settings. For example,school psychologists are particularly pre-pared to coordinate with teachers to dis-seminate evidence-based classroom-levelinterventions, such as the Good BehaviorGame, that have been shown to affect awide variety of long-term child mentalhealth outcomes, such as drug use and anti-social behavior (Bradshaw et al., 2009;embry, 2002). Indeed, school psychologistshave key access to critical change agentsthat play important roles in children’s lives,allowing them to increase the ecologicalvalidity of the interventions they deliver.
this article describes three examples ofschool psychologists fostering the use ofCBt in school settings from the Universityof texas at Austin’s (Ut Austin) SchoolPsychology program: (a) two faculty in theUt Austin School Psychology programhave collaborated with three local middleschools to conduct a feasibility study tosupport school providers’ use of a CBt-based depression prevention program foryouth in schools, called Act & Adapt (Bear-man & Weisz, 2009; Polo, Bearman, Short,ho, & Weisz, 2006); (b) A graduate of thisschool psychology program has openedVida Clinic, a school co-located mentalhealth organization that specializes inschool-based mental health services; (c)Another graduate of Ut Austin, along withcurrent graduate students of Ut Austin’sschool psychology program, has developeda webinar series to train school nurses inCBt-based mental health care.
Act & AdaptAct & Adapt is a CBt-based coping
skills intervention that has been adapted
April • 2019 109
S C H O O L P S Y C H O L O G I S T S
for use in the school setting, adjusting fortime, financial, and training constraints(Bearman & Weisz, 2009; Polo et al., 2006).It is a manualized, video-guided groupdepression prevention program thatteaches youth to learn how to “act” inresponse to problems that are in their con-trol and “adapt” to stressors that are out-side of their control using coping skills,such as behavioral activation and cognitiverestructuring. Groups were co-led bymaster’s and doctoral students in theschool psychology program at Ut Austinand school staff, interns, and social work-ers already embedded in the middleschools. the Act & Adapt program wasmodified to fit into the typical school con-text, with shortened sessions (30 minutesof content) and more flexible delivery thanin the initial design. In addition to expand-ing service capacity at the schools, a keygoal of this research collaboration was totransfer CBt knowledge to school person-nel so that they could independently pro-vide these groups to future students with-out school psychology student support.
School-based mental health providers(N = 8) completed surveys before and afterimplementing the depression preventionprogram. Providers’ knowledge and use ofevidence-based practices were measuredusing the Practice elements Checklist(PeC; Weist et al., 2009) and their attitudestoward the use of evidence-based practiceswas measured using the evidence-BasedPractices Attitudes Scale (eBPAS; Aarons,2004). T-tests were used to examine pre-and postimplementation scores on the PeCand eBPAS. the PeC subscales, PeC totalscores, and eBPAS total scores, except forthe ADhD subscale score on the PeC, hadmedium effect sizes (range from d = .43–.64; Cohen, 1988). Provider scores onknowledge and use of evidence-baseddepression techniques improved by a largeeffect size (d = .81; Cohen, 1988), a findingconcordant with the goals of the CBt-based preventive depression intervention.As expected, given the small sample size, t-tests revealed no significant differencesbetween providers’ knowledge, use, andattitudes pre- and postimplementation. Itis difficult to interpret and generalize theseresults because of the small sample size andlack of a control group. Nevertheless, thesubstantial effect sizes do suggest that aca-demic-practice partnerships amongschools and school psychology programscan influence the use, knowledge, and atti-tudes of CBt by school-based mentalhealth providers.
Vida ClinicVida Clinic is a mental health organiza-
tion that focuses on school-based mentalhealth programs founded by a graduate ofUt Austin’s School Psychology doctoralprogram. the founder’s background inschool psychology facilitated a partnershipbetween Vida Clinic and the Austin Inde-pendent School District; Vida Clinic cur-rently has 23 co-located elementary school-based clinics, one middle school clinic, andthree high-school-based clinics. Despitebeing physically located on school cam-puses, Vida Clinic is an embedded clinicthat works as a separate entity from theschool. By operating directly on schoolcampuses, the clinics can serve a popula-tion that has had trouble accessing tradi-tional mental health services, specificallyminority and low-income families (Farmeret al., 2003; Levy & Land, 1994). On-campus locations also allow Vida Clinic toprovide services to children, their families,and staff, through teacher consultations,trainings, and school-wide workshops inaddition to individual, family, and grouptherapy. Also, clinicians can pull studentsdirectly from the classroom for therapy,working with teachers to ensure that stu-dents do not miss important instructionaltime. the clinic follows a multisystemicapproach and emphasizes the use of evi-dence-based assessment, monitoring clientprogress through frequent interviews andthe use of the Behavior Assessment Systemfor Children–third edition (BASC-3; Kam-phaus & Reynolds, 2015).
many of the therapists at the clinics uti-lize CBt with their clients. Vida Clinic isone of the practicum sites for Ut Austin’sSchool Psychology graduate programthrough which practicum students engagein CBt with clients. Individual interven-tions conducted within the school settinghave excellent external validity for stu-dents. For example, the school setting facil-itates working with teachers on classroommanagement strategies to address disrup-tive behavior in the classroom. Further-more, in-school exposure-based CBt foranxiety can be particularly effective if theydirectly address the situations in whichchildren experience anxiety, such as eatingin the cafeteria, using public bathrooms, ortalking in class.
Training School Nurses in CBTDell Children’s medical Center’s edu-
cational Advocacy Program (DCeAP) is aprogram created in fall of 2016 to help fam-ilies navigate the stressors related to theirtransition from hospital- to school-based
care following an illness. In addition toproviding families with an advocate tocommunicate with the school and facilitatestudent reentry, DCeAP team members,who are all affiliated with the school psy-chology program in the educational psy-chology department at Ut Austin, strive tofind new ways to educate school personnelin effective behavioral health interventions.Recently, the DCeAP team created an 8-part webinar series for Austin-area schoolnurses to increase knowledge of mentalhealth issues, reduce barriers to mentalhealth screening and empirically supportedintervention, and strengthen the school-hospital connection. Webinar speakerswere all experts in the field who have a CBtorientation and backgrounds in schoolpsychology or child psychology. Webinartopics were selected by graduate researchassistants in school psychology using feed-back from previous trainings and currenttrends in mental health research withyouth. School nurses (n = 79) from oneAustin school district have received train-ing via monthly webinars on topics includ-ing: (a) motivational interviewing, (b) anoverview of cognitive behavioral therapy,(c) CBt coping skills for depression, (d)CBt for anxiety, and (e) CBt for self-inju-rious behavior. Screening tools and addi-tional information on webinar topics wereprovided to viewers after each webinar.Preliminary pre- and postwebinar surveyresults suggest that this method of dissem-inating of CBt to school nurses is effectivein increasing knowledge of CBt founda-tions and practice.
Conclusionthe majority of youth who receive
mental health care are served by schoolsand, thus, locating mental health serviceson school campuses and integrating themwith other services increases youth accessi-bility to mental health treatment. CBt fitswell in a school context because it coincideswith the existing structure in schools andcan conform to time and resource restric-tions. Schools are also informative micro-cosms of knowledge for practice-basedresearch on how evidence-based interven-tions can better fit the needs of schools andtheir diverse populations.
School psychologists are uniquely qual-ified to disseminate CBt in schools and toallied professionals that work in schools. Asdemonstrated by programs like Act &Adapt, school psychologists are highlyfamiliar with school systems and contexts,which allows them to design research stud-
110 the Behavior Therapist
ies that fit with school settings and appro-priately adjust interventions to workwithin schools. Furthermore, knowledge ofmental health interventions at the univer-sal, targeted, and individual level makeschool psychologists well-suited to bring acognitive-behavioral lens to each of theselevels, to adapt CBt interventions to bemost useful given children’s ecologies inschools, and to intervene with effective carebefore problems cause considerableimpairment. School psychologists’ exper-tise in interdisciplinary collaboration alsomake them excellent candidates for coordi-nating between service systems, such aswith medical professionals and schools.
While there are still substantial barriersto the implementation of CBt-based inter-ventions in school settings, including thehigh existing workload of school psycholo-gists and lack of policy and resources facil-itating school psychologists’ involvementin mental health service delivery, the role ofa school psychologist can and shouldextend far beyond that of assessor for spe-cial education services. School psycholo-gists at the master’s and doctoral levels canbe particularly valuable coordinators ofservices and principle disseminators ofCBt.
ReferencesAarons, G. A. (2004). mental health
provider attitudes toward adoption ofevidence-based practice: the evidence-based practice attitude scale (eBPAS).Mental Health Services Research, 6(2),61–74. doi: 10.1023/B:mhSR.0000024351.12294.65
Adelman, h. S., & taylor, L. (2010).Mental health in schools: Engaging learn-ers, preventing problems, and improvingschools. thousand Oaks, CA: CorwinPress.
Ball, C., Pierson, e., & mcIntosh, D. e.(2011). the expanding role of school psy-chology. In m. A. Bray & t. J. Kehle(eds.), The Oxford handbook of schoolpsychology (pp. 47-60). New York, NY:Oxford University Press.
Bearman, S. K., & Weisz, J. R. (2009). Pri-mary and secondary control enhance-ment training (PASCet): Applying thedeployment-focused model of treatmentdevelopment and testing. In C. A. essau(ed.), Treatments for adolescent depres-sion: Theory and practice (pp. 97–121).New York, NY: Oxford University Press.doi: 10.1093/med:psych/9780199226504.003.0005
Bradshaw, C. P., Zmuda, J. h., Kellam, S.G., & Ialongo, N. S. (2009). Longitudinalimpact of two universal preventive inter-
ventions in first grade on educationaloutcomes in high school. Journal of Edu-cational Psychology, 101(4), 926. doi:10.1037/a0016586
Burns, B. J., Costello, e. J., Angold, A.,tweed, D., Stangl, D., Farmer, e. m., &erkanli, A. (1995). Children's mentalhealth service use across service sectors.Health Affairs, 14(3), 147-159.
Cohen, J. (1988). Statistical power analysisfor the behavioural sciences (2nd ed.).hillsdale, NJ: Lawrence earlbaum.
D’Amato, R. C., Zafiris, C., mcConnell, e.,& Dean, R.S. (2011). the history ofschool psychology: Understanding thepast to not repeat it. In m. A. Bray & t. J.Kehle (eds.), The Oxford handbook ofschool psychology (pp. 9-46). New York,NY: Oxford University Press.
embry, D. D. (2002). the Good BehaviorGame: A best practice candidate as a uni-versal behavioral vaccine. Clinical Childand Family Psychology Review, 5(4), 273-297. doi: 1096-4037/02/1200-0273/0
Farmer, e. m. Z., Burns, B. J., Phillips, S.D., Angold, A., & Costello, e. J. (2003).Pathways into and through mental healthservices for children and adolescents.Psychiatric Services, 54(1), 60–66. doi:10.1176/appi.ps.54.1.60
Filter, K. J., ebsen, S., & Dibos, R. (2013).School psychology crossroads in Amer-ica: Discrepancies between actual andpreferred discrete practices and barriersto preferred practice. International Jour-nal of Special Education, 28(1), 1-13.
hoagwood, K., & erwin, h. D. (1997).effectiveness of school-based mentalhealth services for children: A 10-yearresearch review. Journal of Child &Family Studies, 6(4), 435–451. doi:10.1023/A:1025045412689
hoagwood, K. e., Serene Olin, S., Kerker,B. D., Kratochwill, t. R., Crowe, m., &Saka, N. (2007). empirically based schoolinterventions targeted at Academic andmental health functioning. Journal ofEmotional and Behavioral Disorders,15(2), 66–92. doi:10.1177/10634266070150020301
holdaway, A. S., & Owens, J. S. (2015).the effect of training and consultationcondition on teachers’ self-reported like-lihood of adoption of a daily report card.Journal of Educational Psychology,107(1), 222–235. doi: 10.1037/a0037466
Kamphaus, R. W., & Reynolds, C. R.(2015). Behavior assessment system forchildren—third edition (BASC-3): Behav-ioral and emotional screening system(BeSS). Bloomington, mN: Pearson.
Kazdin, A. e., & Weisz, J. R. (1998). Identi-fying and developing empirically sup-ported child and adolescent treatments.Journal of Consulting and Clinical Psy-chology, 66(1), 19.
Kratochwill, t. R. (2007). Preparing psy-chologists for evidence-based schoolpractice: Lessons learned and challengesahead. American Psychologist, 62(8),829–843. https://doi.org/10.1037/0003-066X.62.8.829
Levy, A. J., & Land, h. (1994). School-based interventions with depressedminority adolescents. Child and Adoles-cent Social Work Journal, 11(1), 21-35.
Loades, m. e., & mastroyannopoulou, K.(2010). teachers’ recognition of chil-dren’s mental health problems. Child andAdolescent Mental Health, 15(3), 150–156. doi: 10.1111/j.1475-3588.2009.00551.x
mennuti, R., & Christner, R. W. (2005).School-based therapy. In A. Freeman, S.h. Felgoise, C. m. Nezu, A. m. Nezu, &m. A. Reinecke (eds.), Encyclopedia ofcognitive behavior therapy (pp. 343–347).New York: Springer-Verlag. doi:10.1007/0-306-48581-8_96
mennuti, R. B., & Christner, R. W. (2013).An introduction to cognitive-behavioraltherapy with youth. In R. W. Christner,R. B. mennuti, & A. Freeman (eds.), Cog-nitive-behavioral interventions in educa-tional settings: A handbook for practice.New York, NY: Routledge.
Ollendick, t. h., & King, N. J. (2004).empirically supported treatments forchildren and adolescents: Advancestoward evidence-based practice. hand-book of interventions that work withchildren and adolescents: Prevention andTreatment, 3-25.
Owens, P. L., hoagwood, K., horwitz, S.m., Leaf, P. J., Poduska, J. m., Kellam, S.G., & Ialongo, N. S. (2002). Barriers tochildren’s mental health services. Journalof the American Academy of Child &Adolescent Psychiatry, 41(6), 731–738.doi: 10.1097/00004583-200206000-00013
Polo, A. J., Bearman, S. K., Short, K. h., &Weisz, J. R. (2006). Strengtheningschool-research collaborations whiledeveloping effective youth depressionprograms. Report on Emotional andBehavioral Disorders in Youth, 6, 27-28.
Reinecke, m. A., Dattilio, F. m., & Free-man, A. (eds.). (2003). Cognitive therapywith children and adolescents: A casebookfor clinical practice (2nd ed.). New York,NY: Guilford Press.
Reinke, W. m., herman, K. C., & Sprick,R. (2011). Motivational interviewing foreffective classroom management: Theclassroom check-up. New York, NY: Guil-ford Press.
Sheridan, S. m., & Kratochwill, t. R.(2007). Conjoint behavioral consultation:Promoting family-school connections andinterventions. New York: Springer Sci-ence & Business media.
B O W L I N G E T A L .
April • 2019 111
Weist, m. D., Lever, N. A., Bradshaw, C.P., & Owens, J. S. (2014). Furtheradvancing the field of school mentalhealth. In m. D. Weist, N. A. Lever, C. P.Bradshaw, & J. S. Owens (eds.), Hand-book of school mental health: Research,training, practice, and policy (pp. 1–14).Boston, mA: Springer. doi: 10.1007/978-1-4614-7624-5_1
Weist, m. D., Lever, N., Stephan, S.,Youngstrom, e., moore, e., harrison, B.,. . . Stiegler, K. (2009). Formative evalua-tion of a framework for high qualify, evi-dence-based services in school mentalhealth. School Mental Health, 1(4), 196-211. doi: 10.1007/s12310-009-0918-5
Weisz, J. R., & Kazdin, A. e. (eds.). (2010).Evidence-based psychotherapies for chil-dren and adolescents (2nd ed.). NewYork, NY: Guilford Press.
Weisz, J. R., & Kazdin, A. e. (eds.). (2018),Evidence-based psychotherapies for chil-dren and adolescents (3rd ed., pp. 577–595). New York, NY: Guilford Press.
. . .
We thank erin Rodríguez, Ph.D., Universityof texas at Austin, for her collaboration onthe Act & Adapt project described in thispaper. We thank elizabeth minne, Ph.D.,L.P., for allowing us to share details aboutVida Clinic, and marcella m. maxwell,m.A., L.m.F.t., L.P.C., University of texasat Austin, Dell Children’s medical Center,for allowing us to share details about herwork training school nurses in CBt.the Act and Adapt Research-Practice Part-nership was funded by a faculty grant madeto Dr. Bearman by the University of texasOffice for the Vice President of Research.Vida Clinic is partially funded by a Victimsof Crime Act (VOCA) grant. DCeAP’sWebinar Series is funded by a grant fromthe Covalent Foundation.Correspondence to Amanda Bowling,Department of educational Psychology,University of texas at Austin, 1912 Speed-way Ste 504, Austin, tX [email protected]
COGNItIVe BehAVIORAL theRAPY (CBt)is a structured, time-limited approach topsychotherapy that has reliably shown tobe an efficacious option for addressing avariety of common mental health disorders(e.g., hoffman, Asnaani, Vonk, Sawyer, &Fang, 2012). the types of disorders forwhich CBt has well-established efficacyinclude anxiety disorders (Olatunji, Cisler,& Deacon, 2010), obsessive-compulsiveand related disorders (mcKay et al., 2015),eating disorders (Linardon, Wade, de laPiedad Garcia, & Brennan, 2017), anddepression (DeRubeis, Siegle, & hollon,2008), among others. Relative to otherleading treatments (e.g., pharmacother-apy), CBt has been demonstrated to be acost-effective approach, thereby reducingsignificant burden on afflicted individualsand health care systems (e.g., Dickerson etal., 2018; heuzenroeder et al., 2004). Addi-tionally, treatment-seeking patients as wellas their family members show a preferencefor CBt over pharmacotherapy and alter-native treatments (Brown, Deacon,Abramowitz, & Whiteside, 2007; Deacon &Abramowitz, 2005). taken together, theabove evidence supports a strong case forCBt as the treatment of choice for manycommon mental health problems.
In spite of the substantial evidence basesupporting the effectiveness of CBt, thetreatment has persistently struggled withwhat is now a well-documented dissemina-tion problem: the availability of CBt topatients in need is dwarfed by the demand(mchugh & Barlow, 2010; Shafran et al.,2009). this dissemination problem haspersisted in spite of efforts to enhance thescalability of CBt, such as increased effortsto develop CBt-based group therapies aswell as technology-based CBt interven-tions (Kazdin & Blase, 2011). moreover,the insufficient availability of CBt unfor-tunately appears consistent across a widerange of disorders, including anxiety disor-ders (Gunter & Whittal, 2010), eating dis-orders (hart, Granillo, Jorm, & Paxton,2011), and depression (Simons et al., 2010).
the negative effects of this limited avail-ability of CBt are significant; the substan-tial majority of individuals who experiencea common mental health disorder areunable to access evidence-based treatment(Goisman, Warshaw, & Keller, 1999; Steinet al., 2004; Young, Klap, Sherbourne, &Wells, 2001; Young, Klap, Shoai, & Wells,2008).
A variety of barriers hinder efforts tomake CBt more available to individuals inneed. Some of these barriers are practical,such as limited availability of training andongoing consultation in CBt, the prohibi-tive cost and time required to seek suchtraining, and a lack of organizational sup-port in implementing the treatment(Becker, Zayfert, & Anderson, 2004; Beidas& Kendall, 2010; Gray, elhai, & Schmidt,2007; Stewart, Chambless, & Baron, 2012;Weissman et al., 2006). Other barriers toincreasing availability of CBt are moreideological in nature; many therapistsendorse a host of negative beliefs related toCBt. Some of these beliefs apply broadly toall evidence-based treatments, such as thebelief that treatments delivered with adher-ence to a protocol or manual are compro-mising to the therapeutic relationship andstifling of therapist creativity (Addis,Wade, & hatgis, 1999). Other beliefs aremore unique to specific CBt components,such as the belief that exposure therapyposes unreasonable risk for harm topatients (Deacon et al., 2013).
Whereas much previous literature haselucidated the role that these practical andideological barriers play in hindering thedissemination of CBt, one barrier that hasreceived considerably less attention is thelimited range of professionals who havehistorically been eligible to receive trainingin CBt. that is, those clinicians who aremost often the intended recipients of CBt-oriented training and supervision are pre-dominantly doctoral or master’s-levelpractitioners with previous experience inmental health practice (Barlow, Levitt, &Bufka, 1999). the minimal inclusion of
The “Behavioral Specialist” Model of TrainingNovice Paraprofessional Clinicians: An Innova-tive, Cost-Effective Approach for Increasing theScalability of CBTNicholas R. Farrell, Rachel C. Leonard, and Bradley C. Riemann,Rogers Behavioral Health
112 the Behavior Therapist
individuals in CBt training who do nothave a doctoral or master’s degree may runthe risk of creating an unnecessary ceilingon the volume of mental health profession-als that can competently deliver CBt.there may be an “untapped resource” ofnovice paraprofessionals who, in spite oflimited credentials and experience, are ableto implement CBt proficiently underappropriate training and supervision. Sucha change within mental health-care sys-tems would have the potential to signifi-cantly increase the availability of CBt ser-vices that are offered, thereby reducing theburden of accessing effective treatment forindividuals in need (Kazdin & Blase, 2011).
there is a small yet promising body ofliterature attesting to the feasibility andeffectiveness of training novice paraprofes-sionals to use CBt. One of the first knownexplorations of using novice paraprofes-sionals to deliver CBt was done by Pruitt,miller, and Smith (1989), who documentedthe exposure-based treatment of an elderlyfemale patient with severe, refractoryobsessive-compulsive disorder (OCD) by asmall group of undergraduate studentswho received intensive supervision.Although the patient in this case study hadnot responded to a myriad of previouspharmacological and psychological inter-ventions, she benefitted remarkably fromthe course of exposure-based CBt deliv-ered by the undergraduate students (Pruittet al., 1989). more recently, a handful ofexperimental studies have provided furtherevidence that CBt can be competentlydelivered by novice paraprofessionals.Solem, hansen, Vogel, and Kennair (2009)showed that a group of 10 inexperiencedstudents were able to successfully provideexposure therapy for patients with OCDafter receiving relatively little training andsupervision (i.e., 90 hours). Additionally, asimilarly designed study found that inexpe-rienced student paraprofessionals wereable to deliver exposure therapy forpatients with OCD with comparable effi-cacy as compared to experienced therapists(van Oppen et al., 2010). the successfulimplementation of CBt by novice para-professionals is not unique to exposuretherapy for OCD. A recent large random-ized controlled trial for depression treat-ment found that relatively inexperiencedparaprofessionals were able to successfullyuse behavioral activation (BA), yieldingefficacy that was equivalent to a more all-encompassing CBt “package” that wasdelivered by experienced therapists(Richards et al., 2016). In sum, a growingbody of literature provides evidence that
novice paraprofessionals can be trainedwithin a relatively brief period of time toeffectively deliver CBt-based interventionsfor common mental health problems.
Greater usage of novice paraprofession-als as front-line facilitators of CBt in vari-ous clinical settings has the potential tomake inroads into the aforementioned dis-semination problem. Accordingly, theobjective of this article is to provide readerswith a comprehensive description of amodel for training and supervising noviceparaprofessionals that we have been able touse to good effect in our organization overthe past two decades. herein, we describethe history, development, and ongoingrefinement of a training/supervision modelfor novice paraprofessionals known as“behavioral specialists” in our organiza-tion. We also provide brief overviews ofseveral treatment outcome studies we havepublished in which the primary treatmentwas CBt that was administered primarilyby our behavioral specialists. Finally, weconclude with a discussion of advantagesand disadvantages of this training model, afew lessons learned from our experiencewith the model, and suggestions for thosepotentially considering the inclusion ofnovice paraprofessionals as CBt-orientedtreatment facilitators in their clinical prac-tice setting.
The “Behavioral Specialist” Modelof Training and Supervision
History and Developmentthe behavioral specialist role was devel-
oped out of necessity. An adult intensiveoutpatient program (IOP) for OCD wasdeveloped at a private, not-for-profit psy-chiatric facility in 1997. the particular sitewas also in a small, rural, midwest commu-nity. It treated up to four individuals at atime and met for 3 hours per day, 4 daysper week. this program was created anddesigned in this fashion for two reasons.First, traditional outpatient “dosage” (i.e., 1or 2 hours per week) of exposure andresponse prevention (eRP) was enough formany individuals with OCD but not for all.Some more severe and complex casesneeded an intensive outpatient level of careto benefit fully from eRP. Second, provid-ing individual one-on-one intensive treat-ment limits the number of patients aprovider can treat. this model allowed fora combination of therapist-aided and self-directed exposure and could treat fourindividuals at a time instead of just one.this latter point was critical as a combina-tion of high demand for intensive, specialty
OCD treatment and a lack of trainedproviders created a serious “bottleneck” forthese services. Prospective patients werewaiting months for an intensive opening ina provider’s schedule. there are obviouslimits to what one clinician can do seeingpatients on an individual basis.
Given the program’s initial small size,staffing this program was not a problem.An experienced psychologist provided thetreatment directly. however, demand forthe program grew quickly and treatmentslots needed to be added to minimize treat-ment-seeking individuals’ wait time. Itbecame apparent that continuing to staffthis program with experienced OCD spe-cialists would be problematic due to a lackof trained providers in the geographic area.A potential solution to this problem was toreplicate the model of training experiencedin graduate school settings, in which a non-credentialed student is trained in the essen-tials, assigned cases and supervised by apsychologist with expertise in that area.the training would focus on a narrow bandof clinical skills (e.g., eRP) and ongoing,weekly supervision would be essential toensure fidelity to the model and quality ofcare delivered.
the idea was piloted first with doctoralcandidates in a new position we termedbehavioral specialists (BSs). these initialdoctoral candidate BSs had alreadyreceived basic didactic and experientialclinical training, but lacked specialty expe-rience in OCD. they shadowed an experi-enced psychologist and learned quicklyhow to develop exposure hierarchies andassign and conduct exposure trials. thisworked very well; however, there remainedtwo problems with limiting BSs to doctoralcandidates: (a) the need for the programcontinued to grow, both in terms ofnumber of treatment slots offered and alsoin terms of population served, as there wasa need to extend services to children andadolescents as well as adults, and (b) doc-toral candidates would inevitably graduateand may move on to full-time psychologistpositions elsewhere. Scalability was againbeing limited for intensive OCD services bythe lack of providers.
therefore, the next step in the processwas to attempt to apply this concept toindividuals with a master’s or bachelor’slevel of training. A more formal, structuredtraining program was developed includingdidactic training and a reading list (see“the training model,” below). In additionto the training program, weekly individualsupervision was continued in order to dis-cuss cases, answer questions and mentor
F A R R E L L E T A L .
April • 2019 113
these young clinicians. With proper train-ing and ongoing supervision, master’s andbachelor’s-level staff were also able toadhere to the standard model and performwell. Clinical outcomes have been moni-tored closely since the inception of the pro-gram and match or exceed those found inpublished randomized controlled trials(see “treatment Outcomes,” below).
the success of the BS model has allowedscaling these intensive programs signifi-cantly to disseminate empirically sup-ported CBt to a greater number of individ-uals in need of services. there are now 44different OCD intensive programs offeredin seven different states and three residen-tial programs located at the system’s head-quarters (see table 1). three additionallocations are slated to open in 2019.
Given the success of the BS model inintensive OCD treatment, attempts weremade to broaden the clinical scope to otherareas of clinical subspecialty within thisbehavioral health system. the first attemptwas made in the eating disorders (eDs)programs. It was speculated that, given theexposure-based emphasis of the treatmentprovided in the eD programs, noncreden-tialed BSs could also deliver this treatmentin a high-quality manner. the training pro-gram was modified to be applicable to thepopulation served and weekly supervisionwas again provided by a psychologist withspecialty experience. treatment outcomesagain proved strong. In addition to OCDand eDs, BSs currently provide treatmentto mood disorders, posttraumatic stressdisorder (PtSD), and those diagnosed withdual substance use and mental health dis-orders (see table 2 for other BS programs).
Identifying Appropriate BS CandidatesA BS hiring process was developed in
the early stages of this model’s deployment.A series of screening questions were usedduring interviews to identify appropriatecandidates. In addition to basic hiring cri-teria (e.g., a minimum of a bachelor’sdegree), an assessment of compatibilitywith the CBt model and its key principleswas conducted. the basic tenets of the CBtmodel were described and candidates wereasked to confirm whether this was consis-tent with their personal approach or howthey thought “the world worked” (i.e.,emotions are a result of the way we thinkand the way we behave and therefore emo-tions are often not the direct target of treat-ment). those that agreed with a “CBtmindset” moved on in the process andthose that did not were eliminated fromconsideration. they were also asked about
two key areas of eRP work: contaminationand religious-themed exposures. examplesof common exposures for each of thesesymptom subtypes were given and theywere asked to confirm that they would beable to conduct these types of exposureswithout hesitation. Once again, those thatcould confirm their ability to do this typeof work moved on in the process and thosethat could not were eliminated. Anattempt to normalize any hesitation wasmade by explaining that not all people are“cut out” to be BSs in an OCD program andefforts would be made to place them inother subspecialty programs that did notrequire this type of work.
most of the BSs that have been hiredover the last two decades have been young,intelligent, and passionate individuals.With youth comes inexperience, but whatalso comes with it is a lack of bad therapeu-tic habits. We have found that attemptingto “stick a square peg into a round hole” or“teaching an old dog new tricks” has notworked out very well in the BS model. OurBSs have used their youth and energy com-bined with standardized training and con-sistent supervision to successfully treatover 30,000 patients with severe and com-plicated OCD, mood disorders, eDs, PtSDand dual addiction and mental health diag-noses over the past 20 years. Additionally,many BSs have been able to use their train-
ing and clinical experience as a “spring-board” to gain admission to doctoral pro-grams in clinical or counseling psychology.
The Training ModelAll BSs are required to complete a com-
prehensive training program consisting ofthree components: didactic instruction, jobshadowing, and required readings. thefirst component involves intensive didacticinstruction and takes place in “CBt Acad-emy,” which includes 10 days of workshop-based instruction on specific CBt strate-gies most often utilized in the CBt-basedtreatment programs within our system(e.g., exposure therapy).
many of the workshops require thatparticipants engage in role-playing activi-ties and other experiential tasks (e.g., creat-ing a small exposure hierarchy) to furtherfacilitate skills acquisition. the presentersare licensed clinical psychologists who haveconsiderable training and experiencewithin their topic areas, often includingpublished academic articles related to thetopics on which they present. traineescomplete a quiz on each of the contentareas and are given two opportunities topass each quiz with a score of 80% orhigher.
the second component of the BS train-ing program involves shadowing currentBSs working within different CBt-based
ProgramsBSs
Slots Offered
122496
1326104
102080
1326104
31470
51110454
AdultIOP
AdultPHP
PediatricPHP Residential Total
PediatricIOP
Table 1. Patient Capacities of Our System’s Intensive Obsessive-CompulsiveDisorder Programs Across 12 United States Programs
B E H A V I O R A L S P E C I A L I S T M O D E L O F T R A I N I N G
114 the Behavior Therapist
treatment programs. General trainees, orthose who would like a BS role but forwhom there is not yet a specific role identi-fied, shadow within diverse programs togain experience with different levels of careand patient populations. this includesshadowing within residential as well as par-tial hospitalization and intensive outpa-tient levels of care; shadowing within pro-grams that provide treatment to children,adolescents, and adults; and shadowingwithin programs that provide specializedtreatment for OCD and other anxiety dis-orders, eDs, mood disorders, and PtSD.At times, trainees have already been identi-fied to fill specific roles, pending their per-formance throughout the training process.For these individuals, their shadowingschedule may be more targeted towardtheir eventual role. As the course of shad-owing progresses, trainees are encouragedto increase their involvement in the facili-tation of various CBt techniques as theirskill proficiency allows.
trainees are required to complete askills checklist indicating which skills theyhave performed, whether or not they wereobserved performing the skill, and anyadditional notes or questions they hadabout the skill. Some examples of skillsincluded on this checklist are as follows:providing psychoeducation (e.g., rationalefor exposure therapy), developing an expo-sure or BA hierarchy, and “coaching” apatient during an exposure task. traineesprovide a confidence rating for how wellthey feel they can perform each of the skillsincluded in the checklist. Further, BS train-ers complete a corresponding survey toevaluate trainees’ skills. the supervisingpsychologist then may review these evalua-tions to determine additional trainingneeds.
Finally, the third component of trainingincludes required readings from a collec-tion of manuals, books, and journal articleson CBt-based treatment interventions uti-lized across our programs. trainees arerequired to read and provide a writtensummary for each of the required readingsand are given feedback on their writtensummaries. With guidance from theirsupervising psychologist, trainees areexpected to integrate key aspects of thesereadings into their clinical practice of CBt(e.g., discouraging avoidance of scheduledBA activities).
Ongoing SupervisionOnce a BS has completed the training
process and started their role within a spe-cific program, they receive weekly group
and individual supervision from a licensedpsychologist working within their pro-gram. Individual supervision covers arange of topics but typically includes dis-cussion of patients’ progress, including rel-evant assessment scores and progress in theexposure/BA hierarchy; additional skillstraining (e.g., providing additional infor-mation about a technique, role-playing,modeling, etc.); discussion of any legal, eth-ical, cultural, or safety concerns; and over-all clinical direction (i.e., which strategiesto use with specific patients). Group super-vision occurs during multidisciplinaryteam meetings where specific cases are dis-cussed and guidance is provided regardingclinical direction and the use of specificinterventions. the clinical practices of allnonlicensed paraprofessionals are con-ducted under the licenses of the programclinical psychologists.
Treatment OutcomesInitial examinations indicate that use of
this BS treatment model is associated withexcellent treatment outcomes, often whileworking with severe and complex patientpresentations. Leonard and colleagues(2016) examined outcomes within asample of 172 adolescents who receivedresidential treatment for OCD. treatmentprimarily consisted of eRP as delivered bya BS under the supervision of a licensedpsychologist. treatment also includedmedication management and CBt inter-ventions to address co-occurring symp-toms (e.g., activity scheduling for depres-sive symptoms, interoceptive exposure forelevated anxiety sensitivity), which wasnecessary given the high rate of comorbid-ity within the sample. the majority of thesample had at least two diagnoses andnearly half had three or more diagnosesupon admission to the program. Partici-pants experienced significant improve-ment in OCD symptoms, going from thesevere (M = 25.39, SD = 5.36) to the mildrange (M = 13.16, SD = 7.57) on the Chil-dren’s Yale Brown Obsessive-CompulsiveScale–Self Report (CY-BOCS-SR; Piacen-tini, Langley, & Roblek, 2007; t(171) =19.04, p < .001). Participants also experi-enced significant improvement in depres-sive symptoms, moving from the moderate(M = 20.22, SD = 12.90) to the minimalrange (M = 7.66, SD = 8.12) on the BeckDepression Inventory-II (BDI-II; Beck,Steer, & Brown, 1996; t[125] = 11.74, p <.001). Benchmarking data demonstratedthat these reductions in OCD symptomswere in line with those from several ran-domized controlled trials (RCts) examin-
ing CBt alone or in combination with psy-chotropic medication (e.g., Bolton et al.,2011; Franklin et al., 2011; Piacentini et al.,2011; Pediatric OCD treatment Study[POtS] Group, 2004; Storch et al., 2007).Further, follow-up data provided by a sub-sample indicated that improvement inOCD symptom severity was maintained onaverage 1.5 years posttreatment.
the BS treatment model has alsoyielded promising outcomes in the contextof eDs. Simpson and colleagues (2013)examined outcomes within a sample of 56individuals who completed a multimodalresidential treatment program for co-occurring eDs and OCD. treatment pri-marily consisted of exposure-based CBtprovided by BSs for both the eD and theOCD. On average, patients experiencedsignificant improvement in eD symptomseverity, going from an average eating Dis-order examination–Questionnaire (eDe-Q; Fairburn & Beglin, 2008) global score atadmission of 3.8 (SD = 1.5) to an averagescore at discharge of 2.2 (SD = 1.4, t[55] =8.70, p < .001). Patients also improved sig-nificantly with regard to OCD symptomseverity, going from the severe (M = 24.6,SD = 7.2) to the mild (M = 13.3, SD = 7.2)range on the Yale-Brown Obsessive Com-pulsive Scale–Self-Report (Y-BOCS-SR;Steketee, Frost, & Bogart, 1996; t(55) =10.90, p < .001). Body mass index (kg/m2)significantly increased as well in thissample, primarily among those under-weight at admission. Lastly, recent workshowed that eD treatment delivered pri-marily by BSs produced positive prelimi-nary outcomes in a severe inpatientsample. In this study, despite a relativelyshort length of stay (M = 23.8 days, SD =12.6), a brief food-based exposure therapyintervention was successful in reducingpatients’ eating-related fear, avoidancebehaviors, and feared consequences relatedto exorbitant weight gain (Farrell et al., inpress).
this treatment model is also associatedwith favorable outcomes within adult sam-ples receiving intensive treatment forOCD. Blakey, Abramowitz, Reuman,Leonard, and Riemann (2017) reportedtreatment outcome data for adults whoreceived residential OCD treatment. theyfound that scores on the DimensionalObsessive-Compulsive Scale (DOCS;Abramowitz et al., 2010) significantlydecreased over the course of treatment,from an average score of 32.73 (SD = 15.07)at admission to an average score of 16.59 atdischarge (SD = 11.74, t[123] = 13.22, p <.001). Similarly, manos and colleagues
F A R R E L L E T A L .
April • 2019 115
(2010) reported outcomes from a com-bined sample of adults receiving OCDtreatment within either a partial hospital-ization program or a residential treatmentprogram. they found that OCD severity asmeasured by the Y-BOCS-SR significantlyimproved from the severe range (M =26.67, SD = 6.66) to the mild range (M =15.24, SD = 7.03, t[106] = 16.195, p < .001)following treatment.
It is important to note that these out-comes were gathered within naturalisticintent-to-treat samples; therefore, the sam-ples were not limited to those who receiveda complete course of treatment. Often, dueto financial concerns or other reasons,patients have to leave treatment or stepdown to a lower level of care earlier thanproviders would prefer.
Advantages and Disadvantagesthere are several advantages to the BS
model of treatment delivery. the primaryadvantage is that empirically supportedCBt is much more accessible to a greaternumber of individuals struggling withmental illness than would be the case if thistreatment was provided only by psycholo-gists or other highly trained professionals.this is possible due to a greater number ofavailable candidates for the position andbecause of the lower cost of employingthem. this lower cost also allows for morerobust treatment teams. For example,within residential treatment programs inour organization, each patient meets regu-larly with a licensed therapist and psychia-trist or advanced practice nurse practi-tioner in addition to their BS, with dutiesoutside of the BS training scope delegatedto these other members of the treatmentteam (e.g., assisting suicidal patients in cre-ating a safety plan). the supervising psy-chologist often also meets with patients toassist in providing clinical direction andsupervision to the BSs. Further, the use ofthis treatment model is associated withexcellent outcomes, indicating that treat-ment quality is not adversely impacted bythe use of novice paraprofessional treat-ment providers.
there are some disadvantages associ-ated with this model compared to a tradi-tional model using a psychologist or morehighly trained treatment provider. First,some patients may lack confidence in a BSto a greater extent than they would with apsychologist. this often improves ratherquickly in the treatment process but can bea barrier for some patients early on. Fur-ther, BSs are often young adults who fre-quently aspire to gain further education
and training in mental health or otherfields. therefore, there is greater turnoverthan there likely would be for a psycholo-gist role, which adds to the training burden.the frequency and intensity of the trainingand ongoing supervision require a numberof skilled and specialized clinical psycholo-gists. An additional disadvantage is that,given the very specialized nature of the BStraining, there often may be clinical con-cerns that arise outside of their scope.these concerns are often addressed byother members of the treatment team butcan pose challenges to those cliniciansworking in the BS role.
Lessons Learned and Suggestions forUsing Novice Paraprofessionals inCBT Delivery
In closing, we offer our readers a fewimportant lessons we have learned fromour experience implementing this modelthroughout our organization as well assome suggestions for those considering theuse of novice paraprofessionals to enhancethe volume of CBt availability in their clin-ical work setting. First, it is very importantto thoroughly screen trainee candidates inthis model, as selecting appropriate candi-dates is a critical prerequisite for the modelto be successful. Suitable candidates oughtto be “believers” in the CBt model and itskey underpinnings as well as possess a rea-sonably high degree of professional matu-rity. As mentioned previously, individualswho occupy these novice paraprofessionalpositions are often relatively young andprofessionally inexperienced. As such,supervisors may find themselves dealingwith just as many issues surrounding pro-fessionalism (e.g., wearing appropriatework attire) as they do clinical ability. Wehave found it beneficial to use trainees’ jobshadowing as a means to evaluate not onlytheir clinical proficiency but also theircapability to bring an appropriate degree ofprofessionalism and maturity to their role.Related to this, we recommend a thoroughcourse of job shadowing with a range ofexperiences with different clinical popula-tions as well as different clinical care set-tings. Such a thorough training course notonly provides trainees with well-roundedclinical skill sets but also provides supervi-sors with ample opportunity to evaluatetrainees’ clinical aptitude and conduct inorder to ascertain their readiness for clini-cal practice of CBt.
Another important lesson we havelearned about this training model is thatpreparing novice paraprofessionals todeliver CBt effectively necessitates an
unusually high degree of structure in devel-oping and enduring fidelity to detailedtreatment protocols. the youth and inex-perience that often typifies novice parapro-fessional clinicians seemingly contribute toa tendency to “drift” from established prac-tices unless these practices are spelled outclearly in a structured protocol. We havebeen pleasantly surprised to observe manyof our novice trainees thrive when pro-vided this high degree of structure. how-ever, we found it less likely that thesenovice clinicians will succeed when train-ing and supervision emphasizes only broadtheoretical principles of CBt that aremeant to be applied flexibly to patientswith a variety of symptom presentations(Kendall, Gosch, Furr, & Sood, 2008). Inorder to establish such a high degree ofstructure to maximize the effectiveness ofnovice paraprofessional clinicians, it seemsan understatement to say that a great dealof time and resources are needed. Not onlyare multiple highly experienced clinicalleaders needed to develop a trainingcourse/materials and facilitate ongoingsupervision, but there is also considerableorganizational backing that is needed in theform of financial and administrative sup-port. As cliché as it may sound, our experi-ence suggests that successfully implement-ing this training model takes a wholevillage working in tandem.
ConclusionDespite good efforts in recent years to
overcome barriers to disseminating CBtmore effectively, a substantial number ofindividuals who would likely benefit fromthis treatment remain unable to access it. Inthis article, we have highlighted one partic-ularly overlooked barrier: CBt-orientedtraining and supervision has seldom beenavailable to clinicians without relativelyadvanced credentials and experience. Wehave also described one example of abroader solution to this problem, whichinvolves using novice paraprofessionals toimplement various CBt-oriented inter-ventions (e.g., exposure therapy) for arange of common mental health condi-tions. Although our behavioral specialistmodel contains its own unique set of chal-lenges, our experience with it over the pasttwo decades suggests that with appropriateorganizational support, it is a feasible wayto increase the scalability of evidence-basedCBt to meet the growing need for theseservices. It is our hope that this paper mayinspire others in our field to undertake
B E H A V I O R A L S P E C I A L I S T M O D E L O F T R A I N I N G
similar endeavors with the global aim ofimproving the dissemination of CBt.
ReferencesAbramowitz, J. S., Deacon, B., Olatunji, B.,
Wheaton, m. G., Berman, N., Losardo,D., . . . hale, L. R. (2010). Assessment ofobsessive-compulsive symptom dimen-sions: Development and evaluation of thedimensional obsessive-compulsive scale.Psychological Assessment, 22, 180-198.
Addis, m. e., Wade, W. A., & hatgis, C.(1999). Barriers to dissemination of evi-dence-based practices: Addressing prac-titioners concerns about manual-basedpsychotherapies. Clinical Psychology: Sci-ence and Practice, 6, 430-441.
Barlow, D. h., Levitt, J. t., & Bufka, L. F.(1999). the dissemination of empiricallysupported treatments: A view to thefuture. Behaviour Research and Therapy,37, 147-162.
Beck, A. t., Rush, A. J., Shaw, B. F., &emery, G. (1987). Cognitive therapy ofdepression. New York: Guilford.
Beck, A. t., Steer, R. A., & Brown, G. K.(1996). Manual for the Beck DepressionInventory (2nd ed). San Antonio, tX:Psychological Corporation, harcourtBrace.
Becker, C., Zayfert, C., & Anderson, e.(2004). A survey of psychologists’ atti-tudes toward utilization of exposuretherapy for PtSD. Behaviour Researchand Therapy, 42, 277-292.
Beidas, R. S., & Kendall, P. C. (2010).training therapists in evidence-basedpractice: A critical review of studies froma systems-contextual perspective. ClinicalPsychology: Science and Practice, 17, 1-30.
Blakey, S. m., Abramowitz, J. S., Reuman,L., Leonard, R. C., & Riemann, B. C.(2017). Anxiety sensitivity as a predictorof outcome in the treatment of obsessive-compulsive disorder. Journal of BehaviorTherapy and Experimental Psychiatry, 57,113-117.
Bolton, D., Williams, t., Perrin, S., Atkin-son, L., Gallop, C., Waite, P., &Salkovskis, P. (2011). Randomized con-trolled trial of full and brief cognitive-behaviour therapy and wait-list for pae-diatric obsessive-compulsive disorder.Journal of Child Psychology and Psychia-try, 52, 1269-1278.
Brown, A., Deacon, B. J., Abramowitz, J.S., & Whiteside, S. P. (2007). Parents’perceptions of pharmacological and cog-nitive-behavioral treatments for child-hood anxiety disorders. BehaviourResearch and Therapy, 45, 819-828.
Deacon, B. J., & Abramowitz, J. S. (2005).Patients’ perceptions of pharmacologicaland cognitive-behavioral treatments for
anxiety disorders. Behavior Therapy, 36,139-145.
Deacon, B .J., Farrell, N. R., Kemp, J. J.,Dixon, L. D., Sy, J. t., Zhang, A. R., &mcGrath, P. B. (2013). Assessing thera-pist reservations about exposure therapyfor anxiety: Development and validationof the therapist Beliefs about exposureScale. Journal of Anxiety Disorders, 27,772-780.
DeRubeis, R. J., Siegle, G. J., & hollon, S.D. (2008). Cognitive therapy versus med-ication for depression: treatment out-comes and neural mechanisms. NatureReviews Neuroscience, 9, 788-796.
Dickerson, J. F., Lynch, F. L., Leo, m. C.,DeBar, L. L., Pearson, J., & Clarke, G. N.(2018). Cost-effectiveness of cognitivebehavioral therapy for depressed youthdeclining antidepressants. Pediatrics,141. doi:10.1542/peds.2017-1969.
Fairburn, C. G., & Beglin, S. (2008). eatingDisorder examination Questionnaire(eDe-Q 6.0). In C. G. Fairburn (ed.),Cognitive Behavior Therapy and EatingDisorders. New York: Guilford Press.
Farrell, N. R., Bowie, O. R., Cimperman,m. m., Smith, B. e. R., Riemann, B. C., &Levinson, C. A. (in press). exploring thepreliminary effectiveness and acceptabil-ity of food-based exposure therapy foreating disorders: A case series of adultinpatients. Journal of Experimental Psy-chopathology.
Franklin, m.e., Saptya, J., Freeman, J.B.,Khanna, m., Compton, S., Almirall, D.,. . . march, J. S. (2011). Cognitive behav-ior therapy augmentation of pharma-cotherapy in pediatric obsessive-compul-sive disorder: the pediatric OCDtreatment study II (POtS II) randomizedcontrolled trial. Journal of the AmericanMedical Association, 306, 1224-1232.
Goisman, R. m., Warshaw, m. G., &Keller, m. B. (1999). Psychosocial treat-ment prescriptions for generalized anxi-ety disorder, panic disorder, and socialphobia, 1991-1996. American Journal ofPsychiatry, 156, 1819-1821.
Gray, m. J., elhai, J. D., & Schmidt, L. O.(2007). trauma professionals' attitudestoward and utilization of evidence-basedpractices. Behavior Modification, 31, 732-748.
Gunter, R. W., & Whittal, m. L. (2010).Dissemination of cognitive-behavioraltreatments for anxiety disorders: Over-coming barriers and improving patientaccess. Clinical Psychology Review, 30,194-202.
hart, L. m., Granillo, m. t., Jorm, A. F., &Paxton, S. J. (2011). Unmet need fortreatment in the eating disorders: A sys-tematic review of eating disorder specifictreatment seeking among community
cases. Clinical Psychology Review, 31,727-735.
heuzenroeder, L., Donnelly, m., haby, m.m., mihalopoulos, C., Rossell, R., CarterR., Andrews, G., & Vos, t. (2004). Cost-effectiveness of psychological and phar-macological interventions for generalizedanxiety disorder and panic disorder. Aus-tralia and New Zealand Journal of Psychi-atry, 38, 602-612.
hoffman, S. G., Asnaani, A., Vonk, I. J.,Sawyer, A. t., & Fang, A. (2012). theefficacy of cognitive behavioral therapy:A review of meta-analyses. CognitiveTherapy and Research, 36, 427-440.
Kazdin, A. e., & Blase, S. L. (2011).Rebooting psychotherapy research andpractice to reduce the burden of mentalillness. Perspectives on Psychological Sci-ence, 6, 21-37.
Kendall, P. C., Gosch, e., Furr, J. m., &Sood, e. (2008). Flexibility within fidelity.Journal of the American Academy ofChild and Adolescent Psychiatry, 47, 987-993.
Leonard, R. C., Franklin, m. e., Wetter-neck, C. t.., Riemann, B. C., Simpson, h.B., Kinnear, K., Cahill, S. P., & Lake, P.m. (2016). Residential treatment out-comes for adolescents with obsessive-compulsive disorder. PsychotherapyResearch, 26, 727-736.
Linardon, J., Wade, t. D., de la PiedadGarcia, X., & Brennan, L. (2017). theefficacy of cognitive-behavioral therapyfor eating disorders: A systematic reviewand meta-analysis. Journal of Consultingand Clinical Psychology, 85, 1080-1094.
manos, R. C., Cahill, S. P., Wetterneck, C.t., Conelea, C. A., Ross, A. R., & Rie-mann, B. C. (2010). the impact of expe-riential avoidance and obsessive beliefson obsessive-compulsive symptoms in asevere clinical sample. Journal of AnxietyDisorders, 24, 700-708.
mchugh, R. K., & Barlow, D. h. (2010).the dissemination and implementationof evidence-based psychological treat-ments. American Psychologist, 65, 73-84.
mcKay, D., Sookman, D., Neziroglu, F.,Wilhelm, S., Stein, D. J., Kyrios, m.,matthews, K., & Veale, D. (2015). effi-cacy of cognitive-behavioral therapy forobsessive-compulsive disorder. Psychia-try Research, 225, 236-246.
Olatunji, B. O., Cisler, J. & Deacon, B. J.(2010). efficacy of cognitive behavioraltherapy for anxiety disorders: A review ofmeta-analytic findings. Psychiatric Clin-ics of North America, 33, 557-577.
Pediatric OCD treatment Study (POtS)Group. (2004). Cognitive-behavior ther-apy, sertraline, and their combination forchildren and adolescents with obsessive-compulsive disorder. Journal of the
116 the Behavior Therapist
F A R R E L L E T A L .
American Medical Association, 292,1969-1975.
Piacentini, J., Bergman, L., Chang, S., Lan-gley, A., Peris, t., Wood, J.J., &mcCracken, J. (2011). Controlled com-parison of family cognitive behavioraltherapy and psychoeducation/relaxationtraining for child obsessive-compulsivedisorder. Journal of the American Acad-emy of Child & Adolescent Psychiatry, 50,1149-1161.
Piacentini, J., Langley, A., & Roblek, t.(2007). Cognitive-behavioral treatment ofchildhood OCD: It’s only a false alarm,therapist guide. New York, NY: OxfordUniversity Press.
Pruitt, S. D., miller, W. R., & Smith, J. e.(1989). Outpatient behavioral treatmentof severe obsessive-compulsive disorder:Using paraprofessional resources. Jour-nal of Anxiety Disorders, 3, 179-186.
Richards, D. A., ekers, D., mcmillan, D.,taylor, R. S., Byford, S., Warren, F. C., . .. Finning, K. (2016). Cost and outcome ofbehavioural activation versus cognitivebehavioural therapy for depression(COBRA): a randomised, controlled,non-inferiority trial. The Lancet, 388,871-880.
Shafran, R. Clark, D. m., Fairburn, C. G.,Arntz, A., Barlow, D. h., ehlers, A., . . .Wilson, G. t. (2009). mind the gap:Improving the dissemination of CBt.Behaviour Research and Therapy, 47,902-909.
Simons, A. D., Padesky, C. A., mon-temarano, J., Lewis, C. C., murakami, J.,Lamb, K., . . . Beck, A. t. (2010). trainingand dissemination of cognitive behaviortherapy for depression in adults: A pre-liminary examination of therapist com-petence and client outcomes. Journal ofConsulting and Clinical Psychology, 78,751-756.
Simpson, h. B., Wetterneck, C. t., Cahill,S. P., Steinglass, J. e., Franklin, m. e.,Leonard, R. C., Weltzin, t. e., & Rie-mann, B. C. (2013). treatment of obses-sive compulsive disorder complicated bycomorbid eating disorders. CognitiveBehaviour Therapy, 42, 64-76.
Solem, S., hansen, B., Vogel, P. A., & Ken-nair, L. e. O. (2009). the efficacy ofteaching psychology students exposureand response prevention for obsessive-compulsive disorder. Scandinavian Jour-nal of Psychology, 50, 245-250.
Stein, m. B., Sherbourne, C. D., Craske, m.G., means-Christensen, A., Bystritsky,A., Katon, W., Sullivan, G., & Roy-Byrne,P. P. (2004). Quality of care for primarycare patients with anxiety disorders.American Journal of Psychiatry, 161,2230-2237.
Steketee, G., Frost, R., & Bogart, K. (1996).the Yale-Brown Obsessive Compulsive
Scale: Interview versus self-report.Behaviour Research and Therapy, 34,675-684.
Stewart, R. e., Chambless, D. L., & Baron,J. (2012). theoretical and practical barri-ers to practitioners' willingness to seektraining in empirically supported treat-ments. Journal of Clinical Psychology, 68,8-23.
Storch, e. A., Geffken, G. R., merlo, L. J.,mann, G., Duke, D., munson, m., . . .Goodman, W. K. (2007). Family-basedcognitive-behavioral therapy for pedi-atric obsessive-compulsive disorder:Comparison of intensive and weeklyapproaches. Journal of the AmericanAcademy of Child & Adolescent Psychia-try, 46, 469-478.
van Oppen, P., van Balkom, A. J., Smit, J.h., Schuurmans, J., van Dyck, R., &emmelkamp, P. (2010). Does the therapymanual or the therapist matter most intreatment of obsessive-compulsive disor-der? A randomized controlled trial ofexposure with response or ritual preven-tion in 118 patients. Journal of ClinicalPsychiatry, 71, 1158-1167.
Weissman, m. m., Verdeli, h., Gameroff,m. J., Bledsoe, S. e., Betts, K., mufson, L.,Fitterling, h., & Wickramaratne, P.(2006). National survey of psychotherapytraining in psychiatry, psychology, andsocial work. Archives of General Psychia-try, 63, 925-934.
Young, A. S., Klap, R., Sherbourne, C. D.,& Wells, K. B. (2001). the quality of carefor depressive and anxiety disorders inthe United States. Archives of GeneralPsychiatry, 58, 55-61.
Young, A. S., Klap, R., Shoai, R., & Wells,K. B. (2008). Persistent depression andanxiety in the United States. PsychiatricServices, 59, 1391-1398.
. . .
the authors wish to note no conflicts ofinterest or financial support to disclose inthe preparation of this manuscript.Correspondence to Nicholas R. Farrell,Ph.D., Rogers Behavioral health, 34700Valley Road, Oconomowoc, WI [email protected]
findCBT.org
Find a CBT Therapist
ABCT’s Find a CBT Therapistdirectory is a compilation of prac-
titioners schooled in cognitive and
behavioral techniques. In addition
to standard search capabilities
(name, location, and area of exper-
tise), ABCT’s Find a CBT Therapist
offers a range of advanced search
capabilities, enabling the user to
take a Symptom Checklist, review
specialties, link to self-help books,
and search for therapists based on
insurance accepted.
We urge you to sign up for the
Expanded Find a CBT Therapist(an extra $50 per year). With this
addition, potential clients will see
what insurance you accept, your
practice philosophy, your website,
and other practice particulars.
To sign up for the Expanded Find
a CBT Therapist, click MEMBER
LOGIN on the upper left-hand of the
home page and proceed to the
ABCT online store, where you will
click on “Find CBT Therapist.”
For further questions, call the
ABCT central office at 212-647-
1890.
April • 2019 117
B E H A V I O R A L S P E C I A L I S T M O D E L O F T R A I N I N G
Child Behavior ProblemsDisruptive behavior problems in childrenare among the most common mental andbehavioral health concerns impacting fam-ilies. Prevalence estimates for disruptivebehavior problems range from 4% to 16%,affecting nearly 113 million youth world-wide (Briggs-Gowan et al., 2000; Bultas etal., 2015; Polancyzk et al., 2015; Weitzman& Wegner, 2015). Specifically, disruptivebehavior problems include the following:noncompliance (e.g., not listening to or fol-lowing adult commands), defiance towardadults (e.g., disrespectful attitude, deliber-ately annoying others, frequent arguingwith adults), verbal and physical aggres-sion, hyperactivity, difficulty sustainingattention and focus, destructive behavior,lying, whining, and school behavior prob-lems, among others. Youth with clinicallysignificant disruptive behavior problemsmay meet criteria for attention-deficit/hyperactivity disorder (ADhD),oppositional-defiant disorder (ODD), orconduct disorder (CD), among other diag-noses. however, many more youth displaysubclinical externalizing behavior prob-lems, which are challenging for familiesand frequently lead to significant familystress.
Children with disruptive behaviorproblems are at increased risk for variousnegative outcomes, including maltreat-ment, health problems, substance use, pooracademic outcomes, peer relationship diffi-culties, antisocial behaviors, and risk forinvolvement with the juvenile justicesystem (Barkley et al., 1990; Burke et al.,2010; Copeland et al., 2007; Gurwitch et al.,2016). there is also increased risk for neg-ative family outcomes, including increasedparenting stress, reduced confidence inparenting, tension in the parent-child rela-tionship, and increased risk for marital dis-
cord (Anastopoulos et al., 1993; Burke etal., 2010; Cunningham, Benness, & Siegel,1988; mash & Johnston, 1983). thesebehaviors often contribute to significantfamily conflict, school suspensions, andimpairment in a family’s daily functioning(Burke et al., 2010; Gurwitch et al., 2016;Kim-Cohen et al., 2005).
Treatment for DisruptiveBehavior Problems
Parent behavior management training(Pmt) is widely acknowledged as the gold-standard evidence-based treatment for dis-ruptive behavior problems in children(Comer et al., 2013; eyberg, Nelson, &Boggs, 2008). many empirically supportedPmts for young children specificallyderive from a two-phase approach firstimplemented by Constance hanf todecrease disruptive behaviors within theparent-child relationship (Kaehler, Jacobs,& Jones, 2016; Reitman & mcmahon,2013). hanf-based Pmt models, such asDefiant Children (DC; Barkley, 2013),helping the Noncompliant Child (hNC;mcmahon & Forehand, 2003), IncredibleYears (IY; Webster-Stratton, 2006), andParent-Child Interaction therapy (PCIt;eyberg & Funderburk, 2011), similarlyfocus on initially developing relationshipskills between parent and child, while laterincorporating behavioral managementapproaches to build parental capacity forconsistency and follow-through. Whenconsidering the essential common compo-nents of such Pmt models, a meta-analysisconducted by the Center for Disease Con-trol (CDC; 2009) indicates the followingcore elements lead to successful acquisitionof parenting skills and decreased child dis-ruptive behaviors: increasing positive com-munication and interactions between care-
giver and child, and providing caregiverswith opportunities to practice skills withtheir child during therapeutic sessions.Additionally, the CDC concluded teachingcaregivers effective methods for time-outand for consistent application of conse-quences and household rules contributes todecreased child misbehaviors.
Limitations of PMTDespite ample evidence of the benefits
of evidence-based Pmts to treat disruptivebehavior problems in children, many fam-ilies who are referred for therapy either donot pursue treatment or do not successfullycomplete treatment (Pavuluri, Luk, &mcGee, 1996; Wang et al., 2005). there area number of reasons for barriers to treat-ment and high attrition rates, includingsystems-based (e.g., long wait lists, fewerqualified providers) and individually based(e.g., high parenting stress, low social sup-port, financial stressors) factors (Comer etal., 2015; Sandler et al., 2005; Weisz et al.,2005). While the problem of accessibility totreatment and attrition is common inmany areas of mental health treatment (Sil-verman, Kurtines, & hoagwood, 2004;Stirman, Crits-Christoph, & DeRubeis,2004), it is especially problematic whenconsidering a developmental and preven-tion lens, as untreated childhood disruptivebehaviors create a trajectory of various neg-ative outcomes, including delinquency(Broidy et al., 2003).
Further, there are many children whoexhibit behavior problems but who do notmeet formal criteria for a diagnosis. that is,challenging behaviors in children areextremely common and may cause sub-stantial stress within families withoutmeeting a clinical threshold. Not all chil-dren with subclinical symptoms require thelevel of intervention provided by an inten-sive therapy, such as one of the Pmts.moreover, the public health model of pre-vention highlights various points of inter-mediation between children and develop-ing behavioral problems. Specifically,Gordon (1983) indicates three levels of eti-ological impact: (a) primary or universalapproaches to promote health beforesymptoms develop, (b) secondary or tar-geted approaches to assist those identifiedwith emerging symptoms and at-risk fordeveloping further symptoms, and (c) ter-tiary or intensive approaches to treat thosewith clinically significant symptomatology.When applying the framework specificallyto mental health, the World health Orga-nization (WhO, 2001) emphasizes the
Child-Adult Relationship Enhancement (CARE):Expanding Evidence-Based Child BehaviorManagement Skills to an Academic MedicalCenterKerrie G. Murphy, Medical University of South Carolina
Christina M. Warner-Metzger, DePaul University Family andCommunity Services
Angela D. Moreland, Medical University of South Carolina
118 the Behavior Therapist
importance of integrating mental healthprevention into general public healthapproaches.
Overview of Child-AdultRelationship Enhancement
to address a growing need for universalapproaches, Child-Adult Relationshipenhancement (CARe; messer, et al., 2017)was developed to meet communitydemand for training in effective and evi-dence-based behavior management princi-ples and skills for use by a range of individ-uals expanding beyond clinicians withmental and behavioral health backgrounds.Consequently, CARe uses interaction skillsdrawn from hanf-based Pmt conceptsand teaches caregivers and professionals atrauma-informed approach to interactingand working with children in a variety ofsettings (Gurwitch, Fernandez, Pearl, &Chung, 2013; Gurwitch et al., 2016; Pearl,2008; Schilling et al., 2017). therefore,while the methods are applicable to a widerange of populations, CARe also particu-larly targets children who are at risk formaltreatment or disruptive behaviors. thegeneral CARe model is typically presentedin a 3- to 6-hour workshop format using acombination of didactic, multimedia, andexperiential activities, with the trainingduration contingent upon the target clientpopulation, the setting, and agency goals(messer et al., 2017). While some exten-sions of the dissemination model include aseries of learning sessions (e.g., initialworkshop, booster workshop) and actionphases (e.g., live observation, coding, andcoaching in a practical setting; Warner-metzger, 2018), the basic CARe principlesremain a universal or primary interventionfor “simply a way for any adult to interactwith any child” (p. 4, messer et al., 2017).
A Growing Evidence Base for CARECARe was developed using evidence-
based parent training interventions.Demonstrative of its versatility, CARe hasbeen implemented with military families(Gurwitch et al., 2013), child welfare/trauma-impacted populations (Gurwitchet al., 2016; Wood et al., 2017), and primarycare medical settings (Schilling et al., 2017).Although in exploratory phases via pilotprojects, CARe applications to the educa-tional setting (“CARe in the Classroom”)suggest promising preliminary data forteacher satisfaction, knowledge, and appli-cation with students in urban neighbor-hoods with high rates of exposure to com-
munity violence and trauma (Warner-metzger, 2018).
In a randomized controlled trial (RCt)examining mandated foster care training,foster caregivers who received a 6-hourCARe training used significantly morepositive parenting statements during codedcaregiver-child interactions at 1 monthpostintervention and reported fewertrauma-related anxiety symptoms at 3months postintervention when comparedto foster caregivers who received standardparent training (messer, et al., 2018). AnRCt in a medical setting examined the effi-cacy of CARe in Primary Care (PriCARe)using a 6-week caregiver group curriculumtargeting a racially diverse sample of chil-dren with high rates of economic disadvan-tage (Schilling et al., 2017). the studyrevealed caregivers receiving PriCARereported significantly more positive par-enting attitudes for demonstrating empa-thy toward children’s needs, using alterna-tives to corporal punishment, andencouraging children’s power and inde-pendence when compared to their waitlistcontrol counterparts. Caregivers in Pri-CARe also reported significantly decreasedchild disruptive behaviors on a parentquestionnaire compared to caregivers inthe waitlist control. Notably, the meanchange scores in disruptive behaviors inthe PriCARe study demonstrated greatergains than the mean change scores on thesame measure in a study examining a 10-week IY intervention adapted for primarycare (Perrin et al., 2014).
CARE in an Academic Medical CenterAs a logical extension of previous CARe
applications, disseminating CARe trainingto staff within an academic medical centerseemed an optimal fit. Given the broadutility of relationship-building skills thatcould be used by a wide range of health careproviders, CARe fits a need both for med-ical trainees (e.g., medical students, resi-dents, fellows) and for staff members (e.g.,nursing staff, administrative and supportstaff, other clinical staff) who work indepartments with a pediatric population.these trainees and staff members regularlyinteract with children, but they infre-quently have formal training in evidence-based behavior management techniques.
Within these initial 3- to 4-hour CARetrainings at an academic medical center,participants were taught how to use CAReskills with children they encounter withintheir respective clinical settings. thus,CARe skills were presented with several
main aims: (a) for providers to use directlywith children to build rapport, improverelationships, and reduce disruptive behav-iors in the clinical encounter; (b) forproviders to model directly with childrenwhile caregivers observe to illustrate thebenefits of these skills for families; and (c)for providers to teach caregivers for use athome with their children. Further, becausemental health services are often underuti-lized, CARe broadens the reach of univer-sal evidence-based services by trainingother professionals with whom families arelikely to encounter in medical settings(Schilling et al., 2017; Spector et al., 2012).CARe also helps to foster a culture oftrauma-informed care (Gurwitch et al.,2016), as the training flexibly includesformal psychoeducation about develop-mental trauma in children and how traumaresponses in children may present as dis-ruptive behaviors. thus, CARe traininghelps participants become more attuned torecognize trauma reactions in children andprovides effective trauma-informed skillsfor individual providers to use in theirwork with children and families. Byincreasing knowledge about childhoodtrauma, CARe facilitates a more cohesivereferral system, helping providers betterdelineate challenging behaviors that arewithin typical developmental norms frommore severe behaviors. In particular,because CARe is a universal approach,providers may monitor a specific child’sresponse to CARe-informed interactionsand refer the child with more significantdisruptive behaviors for specialized mentalhealth services (such as Pmts or trauma-specific interventions).
Strengths and Lessons Learned FromPilot Dissemination Efforts
CARe training was completed with fivecohorts as a pilot dissemination effortwithin a large academic medical center.Four of these trainings occurred within thedepartment of psychiatry, including pre-doctoral psychology interns, child and ado-lescent psychiatry fellows, clinical staff(e.g., nursing staff, therapeutic aides) fromthe child and adolescent inpatient psychia-try unit, and clinical staff (e.g., nursingstaff, therapeutic aides) from the child andadolescent psychiatry day treatment pro-gram. the fifth training was completedoutside the department of psychiatry with agroup of medical center staff working asconsultants in child health, welfare, andearly intervention. In evaluating the train-ing program, pre- and posttraining mea-
April • 2019 119
C H I L D - A D U L T R E L A T I O N S H I P E N H A N C E M E N T
sures were administered to participants (N= 58). these measures assessed knowledgeof child behavior management techniques,attitudes toward training, self-efficacy, andtraining satisfaction.
Training Needs and SatisfactionSeveral important benefits and lessons
for future directions were gained fromthese initial implementation efforts ofCARe for staff within an academic medicalcenter. First, training was extremely well-received by both stakeholders/administra-tors as well as by individual CARe partici-pants. When potential stakeholders (e.g.,training directors, clinic and division direc-tors) were approached with informationabout the proposed training, most com-mented on the distinct need for broadtraining in evidence-based behavioralmanagement skills that provides concreteand practical skills. In particular, stake-holders were enthusiastic about trainingboth medical trainees and clinical staff, asboth groups typically had limited formaltraining in evidence-based child behaviormanagement techniques.
Further, the participant response wasalso very positive. While this positiveresponse was observed anecdotally duringtrainings by the engagement of partici-pants, our posttraining surveys supportthis view, as 100% of participants rated thequality of the training as “excellent” or“good”; 94.4% of participants reportedbeing “mostly” or “very” satisfied with thequality of training; and 93.6% of partici-pants agreed they would recommend thetraining to a coworker. therefore, CARetraining addressed a specific gap in struc-tured, evidence-based training on behaviormanagement principles for a diverse groupof participants in an academic medicalcenter. It is particularly notable that CARetraining was well received both by partici-pants with relatively little experience work-ing with children in a behavioral health set-ting, as well as by those with moreexperience. For example, one participantwith previous formal training in somePmts reflected that the novelty of activitiesand method by which concepts were pre-sented in CARe were especially helpful,providing this participant with new ideasand flexibility in how to approach workingwith children and families in a universalmanner. this participant’s observationaligned with an overarching goal of thetraining, which was to promote active andengaging adult learning concepts.
Session Length and FrequencyAnother strength of CARe training
within an academic medical center was theflexible implementation. CARe trainingcan be completed in 3 to 6 hours over oneor several sessions. the overall flexibilityand relative brevity of training was key inallowing broader dissemination. In com-paring and contrasting training logisticsand format of workshops, one distinct ben-efit of multiple shorter sessions (i.e., a seriesof three 1-hour workshops) was the abilityto schedule CARe training during existingstaff didactic or meeting times. thisincreased accessibility and reduced logisti-cal barriers to scheduling within a busyacademic medical center. Further, spread-ing CARe training over multiple sessionsallowed participants incremental exposureto the material over several sessions, givingnatural opportunities for participants toreflect upon a subset of skills while apply-ing them in the practical setting betweenworkshops. One limitation of multiplelearning sessions is the possibility of attri-tion from session to session, as all partici-pants may not be able to attend all the ses-sions. this potential barrier can beaddressed by clear advertising that thetraining includes multiple sessions andencouraging (or even requiring) atten-dance at all sessions. In contrast, benefits ofsingle-session CARe trainings (i.e., one 3-to 4-hour workshop) include increasedattendance (ensuring more participantsreceive the entire training), as well as step-wise engagement. hence, experiencing theentire training in a single session providesan immediate additive effect and gestaltframework to increase staff buy-in. Over-all, while there were legitimate pros andcons to the single- or multiple-sessionformat of CARe training, its adaptableimplementation format met the diversetraining and scheduling needs within theever-changing academic medical centerenvironment.
Scheduling and Logistical BarriersWhile CARe training was well received
and initial implementation efforts weresuccessful, several valuable lessons werelearned from these efforts and can guidefuture dissemination. First, despite theenthusiasm of stakeholders/administratorsin bringing CARe training to their units,there were often scheduling challenges toovercome. many of these challenges wereaddressed due to the inherent flexibilitypermitted within the CARe model (asnoted above); however, barriers arosewhen determining staff appropriate for the
training, coverage for essential roles toallow identified staff to participate, andscheduling. these barriers were often moreapparent when implementing CARe withclinical staff, who typically had limited pro-tected time on the job for continuing edu-cation experiences amid increaseddemands to meet productivity require-ments. In this respect, scheduling amongmedical trainees posed fewer barriers, astraining programs require some protectedtime for didactics and training, albeittrainee didactic schedules were set far inadvance and limited immediate implemen-tation.
Scheduling ongoing CARe trainingswas an additional challenge encounteredduring these inaugural disseminationefforts. CARe aims to create a more lastingculture of trauma-informed care and helpadults build positive relationships withchildren, particularly those who exhibitchallenging behaviors. Although initialCARe training was a vital first step towardthis goal by providing a concise overview ofrelationship-building and behavior-man-agement approaches, continued boostersessions or follow-up trainings are advisedto foster practical use of skills withintegrity. however, scheduling proved dif-ficult in developing consistent, ongoingtraining support beyond the initial coreCARe concepts. therefore, follow-uptraining remains an area of identifiedgrowth for the sustainability of CARe in anacademic medical center.
A related limitation was how to assessparticipants' actual use of CARe skills intheir professional roles. While the ability todisseminate CARe broadly among variousmedical professionals who work with chil-dren is a distinct benefit of the training,directly assessing some outcome measures(e.g., actual use of skills, participant’s per-ceived competence in using skills, impactof CARe skills on child outcomes) was notfeasible during our initial disseminationefforts. Comparison of such objective andsubjective outcomes is necessary in futureefforts to ascertain the full efficacy of CARein a medical setting.
Future Directionsthis inaugural implementation of
CARe training for staff within an academicmedical center suggested that this model fitwell with the varied demands of the med-ical environment. Because the training wasso well-received and fulfilled a critical needfor training and education, CARe couldinstinctively become a sustainable part of
120 the Behavior Therapist
M U R P H Y E T A L .
medical training programs in child andfamily medical specialties. While these ini-tial efforts were primarily within psychia-try, future expansion to other departmentswith a pediatric emphasis (e.g., generalpediatrics, developmental pediatrics, pedi-atric emergency services, family medicine)is worth exploration. Because medicaltrainees are in the early stages of careerdevelopment, disseminating CARe skillsduring these formative training years is acrucial way to expand universal evidence-based behavior management skills withchildren and families. While specific CAReskills are helpful for trainees in their indi-vidual interactions with children and fam-ilies, the training highlights how and whento refer families for Pmt interventionwhen they present with severe behaviorproblems. thus, a secondary benefit ofCARe training within medical trainingprograms is to strengthen the knowledgebase of future providers regarding appro-priate referrals for evidence-based behav-ioral therapies.
For clinical staff members working inan academic medical center with childrenbut who lack formal training in evidence-based behavioral health techniques, CAReprovided practical skills to use in their dailyinteractions with children. moreover,given the perceived benefits of CARe train-ing for those who are newly entering pro-fessional work with youth, training staffmembers (particularly among groups withhigh rates of staff turnover) is necessary tokeep CARe skills active. to this end,including CARe training in the onboard-ing or orientation process for these unitsensures that all new staff obtain similarfoundational training and gain more confi-dence in the application of CARe skillswith children.
Finally, an essential next step in CARedissemination is to assess participants'actual use of CARe skills as well as theimpact on child and family outcomes. thelatter is difficult to assess in an academicmedical center, as CARe is not a therapyand participants are using skills in a widerange of settings with differing goals forchild and family outcomes. however,assessing participant use of skills followingthe initial CARe training is a feasible addi-tion. Following a sequential roll-outincluding an initial CARe workshop fol-lowed by planned booster sessions creates apathway to further assess and reinforce theuse of these skills while troubleshootingdifficulties related to implementation.
to summarize, CARe is a flexible andwell-received model to disseminate univer-
sal evidence-based behavior managementand relationship skills for use by a broadpopulation of adults working with chil-dren. Initial dissemination efforts withinan academic medical center appear verypromising. there may be particular benefitfor expanding CARe training within med-ical training programs and among staff inpediatric settings without prior training inevidence-based behavior managementapproaches. Future directions for growthinclude expansion to other departmentswith a pediatric focus within academicmedical centers, development of ongoingand sustainable trainings, and implemen-tation of formal assessment of CARe skillsvia practice in booster sessions.
ReferencesAnastopoulos, A. D., Shelton, t. L., DuPaul,
G. J., & Guevremeont, D. C. (1993).Parent training for attention-deficithyperactivity disorder: Its impact onparent functioning. Journal of AbnormalChild Psychology, 21(5), 581-596.
Barkley, R. A. (2013). Defiant children, thirdedition: A clinician's manual for assess-ment and parent training. New York, NY:the Guilford Press.
Barkley, R. A., Fischer, m., edelbrock, C.S.,Smallish, L. (1990). the adolescent out-come of hyperactive children diagnosedby research criteria: I. An 8-year prospec-tive follow-up study. Journal of the Ameri-can Academy of Child and Adolescent Psy-chiatry, 29, 546-557. doi: 10.1097/00004583-199007000-00007
Briggs-Gowan, m.J., horwitz, S.m.,Schwab-Stone, m.e., Leventhal, J. m., &Leaf, P. J. (2000). mental health in pedi-atric settings: Distribution of disordersand factors related to service use. Journalof the American Academy of Child Adoles-cent Psychiatry, 39, 841–849.
Broidy, L. m., Nagin, D. S., tremblay, R. e.,Bates, J. e. Brame, B., Dodge, K. A., . . .Vitaro, F. (2003). Developmental trajecto-ries of childhood disruptive behaviors andadolescent delinquency: A six-site, cross-national study. Developmental Psychology,39(2), 222-245. http://dx.doi.org.ezproxy.depaul.edu/10.1037/0012-1649.39.2.222
Bultas, m., mcmillin, S., Broom, m., &Zand, D. h. (2015). Brief, rapid response,parenting interventions within primarycare settings. Journal of Behavioral HealthServices and Research, 44, 695-699.
Burke, J.D., Waldman, I., & Lahey, B.B. Pre-dictive validity of childhood oppositionaldefiant disorder and conduct disorder:Implications for the DSm-V. (2010). Jour-nal of Abnormal Psychology, 119 (4), 739-51.Centers for Disease Control and Pre-
vention (2009). Parent training programs:insight for practitioners. Atlanta (GA):Centers for Disease Control.https://www.cdc.gov/violencepreven-tion/pdf/parent_training_brief-a.pdf(accessed on 01/20/2019).
Comer, J. S., Chow, C., Chan, P., Cooper-Vince, C., & Wilson, L. (2013). Psychoso-cial treatment efficacy for disruptivebehavior problems in very young children:A meta-analytic examination. Journal ofthe American Academy of Child & Adoles-cent Psychiatry, 52(1), 26-36.
Comer, J. S., Furr, J. m., Cooper-Vince, C.,madigan, R. J., Chow, C., Chan, P. t., . . .eyberg, S. m. (2015). Rationale and con-siderations for the internet-based deliveryof Parent–Child Interaction therapy.Cognitive and Behavioral Practice, 22 (1),302-316. doi:10.1016/j.cbpra.2014.07.00
Copeland, W.e., miller-Johnson, S., Keeler,G., Angold, A., Costello, e.J. (2007).Childhood psychiatric disorders andyoung adult crime: A prospective, popula-tion-based study. American Journal ofPsychiatry, 167 (11), 1668-1675.
Cunningham, C. e., Benness, B. B., &Siegel, L. S. (1988). Family functioning,time allocation, and parental depressionin the families of normal and ADhD chil-dren. Journal of Clinical Child Psychology,17, 169-177.
eyberg, S. e., Nelson, m. m., & Boggs, S. R.(2008). evidence-based psychosocialtreatments for children and adolescentswith disruptive behavior. Journal of Clini-cal Child & Adolescent Psychology, 37 (1),215-237. doi:10.1080/15374410701820117.
Gordon, R. S. (1983). An operational classi-fication of disease prevention. PublicHealth Reports, 98(2), 107–109.
Gurwitch, R., Fernandez, S., Pearl, e., &Chung, G. (2013). Utilizing parent-childinteraction therapy to help improve theoutcome of military families. Children,Youth, and Families Newsletter. Retrievedfrom the American Psychological Associ-ation website: http://www.apa.org/pi/families/resources/newslet-ter/2013/01/index.aspx
Gurwitch, R. h., messer, e. P., masse, J.,Olafson, e., Boat, B. W., & Putnam, F. W.(2016). Child-adult relationship enhance-ment (CARe): An evidence-informedprogram for children with a history oftrauma and other behavioral challenges.Child Abuse & Neglect, 53, 138-145.
Kaehler, L. A., Jacobs, m., & Jones, D. J.(2016). Distilling common history andpractice elements to inform dissemina-tion: hanf-model BPt programs as anexample. Clinical Child & Family Psycho-
April • 2019 121
C H I L D - A D U L T R E L A T I O N S H I P E N H A N C E M E N T
Kim-Cohen, J., moffitt, t.e., taylor, A.,Pawlby, S.J., & Caspi, A. (2005). maternaldepression and children's antisocialbehavior: Nature and nurture effects.Archives of General Psychiatry, 62, 173-81.
mash, e. J., & Johnston, C. (1983). Parentalperceptions of child behavior problems,parenting self-esteem, and mother'sreported stress in younger and olderhyperactive and normal children. Journalof Consulting and Clinical Psychology, 51,68-99.
mcmahon, R. J., & Forehand, R. (2003).Helping the noncompliant child: Family-based treatment for oppositional behavior(2nd ed.). New York, NY: the GuilfordPress.
messer, e. P., Greiner, m. V., Beal, S. J., eis-mann, e. A., Cassedy, A., Gurwitch, R. h.,. . . eiler-Sims, P. (2018). Child adult rela-tionship enhancement (CARe): A brief,skills-building training for foster care-givers to increase positive parenting prac-tices. Children and Youth Services Review,90, 74-82. doi:10.1016/j.childy-outh.2018.05.017
messer, e. P., Gurwitch, R. h., Boat, B. W.,Olafson, e., Dougherty, S., Warner-met-zger, C., . . . Sharp, D. (2017). Child-AdultRelationship Enhancement (CARE): Trainthe trainer curriculum 2017. Unpublishedtreatment manual.
Pavuluri, m. N. F., Luk, S. L., & mcGee, R.(1996). help-seeking for behavior prob-lems by parents of preschool children: Acommunity study. Journal of the Ameri-can Academy of Child and Adolescent Psy-chiatry, 35, 215–222. http://dx.doi.org/10.1097/00004583-199602000-00015
Pearl, e. (2008). Child Adult Relationshipenhancement (CARe). In Models forDeveloping Trauma: Informed BehavioralHealth Systems and Trauma-Specific Ser-vices. National Association for Statemental health Program Directors(NASmhPD).
Perrin, e. C., Sheldrick, R. C., mcmenamy,J. m., henson, B. S., & Carter, A. S. (2014).Improving parenting skills for families of
young children in pediatric settings. Arandomized clinical trial. Journal of theAmerican Medical Academy of Pedi-atrics,168, 16–24. doi:10.1001/jamapedi-atrics.2013.2919
Polanczyk, G. V., Salum, G.A., Sugaya, L.S.,Caye, A., & Rodhe, L.A. (2015). Annualresearch review: A meta-analysis of theworldwide prevalence of mental disordersin children and adolescents. Journal ofChild Psychology and Psychiatry, 56 (3),345-365.https://doi.org/10.1111/jcpp.12381
Reitman, D., & mcmahon, R. J. (2013).Constance “Connie” hanf (1917-2002):the mentor and the model. Cognitive andBehavioral Practice, 20 (1), 106-116. doi:10.1016/j.cbpra.2012.02.005
Sandler, I., Ostrom, A., Bitner, m.J., Ayers,t.S., Wolchik, S., & Daniels, V.S. (2005).Developing effective prevention servicesfor the real world: a prevention servicedevelopment model. American Journal ofCOmmunity Psychology, 35 (3-4), 127-42.
Schilling, S., French, B., Berkowitz, S.J.,Dougherty, S.L., Scribano, P.V., & Wood,J.N. (2017). Child-adult relationshipenhancement in a primary care (Pri-CARe): A randomized trial of a parenttraining for child behavior problems. Aca-demic Pediatrics, 17 (1), 53-60.
Silverman, W.K., Kurtines W.m., & hoag-wood K. (2004). Research progress oneffectiveness, transportability, and dissem-ination of empirically supported treat-ments: Integrating theory and research.Clinical Psychology: Science and Practice,11, 295–299. doi: 10.1093/clipsy.bph084.
Spector, L., Polka, L., toy, S., hoffman, A.,Nyp, S., & Andrews, S. (2012). Teachingparenting skills one resident at a time. Pre-sented at the 12th Annual PCIt Confer-ence. Sacramento, CA.
Stirman S., Crits-Christoph P., & DeRubeisR.J. (2004). Achieving successful dissemi-nation of empirically supported psy-chotherapies: A synthesis of disseminationtheory. Clinical Psychology: Science andPractice, 11, 343–359. doi:10.1093/clipsy.bph091.
Wang, P. S., Berglund, P., Olfson, m.,Pincus, h. A., Wells, K. B., & Kessler, R. C.
(2005). Failure and delay in initial treat-ment contact after first onset of mentaldisorders in the National ComorbiditySurvey Replication. Archives of GeneralPsychiatry, 62, 603–613. http://dx.doi.org/10.1001/archpsyc.62.6.603
Warner-metzger, C. m. (2018). CARe inschools: meeting mental health needs ofstudents in communities facing violenceand civil unrest. In R. Gurwitch (Chair) &J. P. Abner (Discussant), Child-AdultRelationship Enhancement: Building newbridges in the PCIT and parent trainingworld. Symposium presented to the 2018Parent-Child Interaction therapy WorldCongress, Schweinfurt, Germany.
Webster-Stratton, C. (2006). The IncredibleYears: A trouble-shooting guide for parentsof children aged 2-8 years. Seattle, WA:Incredible Years.
Weisz, J.R., Sandler, I.N., Durlak, J.A., &Anton, B.S. (2005). Promoting and pro-tecting youth mental health through evi-dence-based prevention and treatment.American Psychologist, 60 (6), 628-648.
Weitzman, C., & Wegner, L. (2015). Pro-moting optimal development: screeningfor behavioral and emotional problems.Pediatrics, 135, 384–395.
Wood, J.N., Dougherty, S.D., Long, J.,messer, e.P. & Rubin, D. (2017). A pilotinvestigation of a novel intervention toimprove behavioral well-being for chil-dren in foster care. Journal of Emotionaland Behavioral Disorders.doi:10.1177/1063426617733715
World health Organization. (November2001). Prevention and promotion inmental health. Department of mentalhealth and Substance Dependence.https://www.who.int/mental_health/media/en/545.pdf (accessed on 01/20/2019).
. . .
the authors have no relevant financial, per-sonal, or other relationships which consti-tute conflicts of interest to disclose.Correspondence to Angela moreland,Ph.D., 67 President Street, Charleston, SC20425; [email protected]
Rumination-Focused CBT forDepression and Anxiety— Ed Watkins• 11 am–12:30 pm Eastern | 10 am–11:30 pm Central
9 am–10:30 am Mountain | 8 am–9:30 am Pacific
APRIL 12
122 the Behavior Therapist
M U R P H Y
ON SePtemBeR 20, 2017, hurricane mariadevastated the island of Puerto Rico, killingthousands, destroying property, and desi-mating infrastructure. the hurricane leftthe entire island without access to electric-ity, water, or communication for months(and for many up to a year), resulted in anestimated 4,645 hurricane-related deaths(Kishore et al., 2018), and led to over200,000 Puerto Ricans migrating to themainland U.S. in search of housing, accessto basic needs, and employment (hinojosa& meléndez, 2018). each year an estimated175 million children around the world willexperience a natural disaster (Seballos,tanner, tarazona, & Gallegos, 2011),which increases their risk for developingposttraumatic stress disorder (PtSD),depression, traumatic grief, anxiety disor-ders, externalizing problems, and sub-stance use disorders (Bonanno et al., 2010).Postdisaster mental health interventionguidelines recommend a three-phase,trauma-focused approach addressing thebasic and socioemotional needs of childrenand adolescents at various stages of recov-ery (La Greca & Silverman, 2009). DuringPhase 1: Immediate Aftermath (day of dis-aster to a few weeks), the focus should beon restoring access to basic needs (e.g.,food, water, clothing, medical attention,shelter) and promoting a sense of safetyand security through interventions that arebrief and present-focused (hobfoll et al.,2007). Phase 1 interventions, such as Psy-chological First Aid (PFA; Brymer et al.,2006), seek to reduce or prevent long-termdistress and dysfunction. During Phase 2:Short-term Recovery and Rebuilding (1
month up to a year), interventions such asSkills for Psychological Recovery(Berkowitz et al., 2010) focus on teachingsurvivors evidence-based coping skills(based on CBt principles) that have beenshown to bolster resiliency, increase self-efficacy, and reduce ongoing distress fol-lowing a traumatic event. During Phase 3:Long-term Recovery (1 year up to a fewyears), the focus is on children with moder-ate-to-severe levels of mental health symp-toms receiving evidence-based cognitivebehavioral interventions that have beenshown to effectively treat these trauma-related problems in children and adoles-cents. examples of Phase 3 interventionsinclude Cognitive Behavioral Interventionfor trauma in Schools (Jaycox, Langley, &hoover, 2018) and trauma-Focused Cog-nitive Behavioral therapy (Cohen, man-narino, & Deblinger, 2017).
the evidence supporting the effective-ness of cognitive-behavioral interventionsin diverse postdisaster contexts is encour-aging (Bonanno et al., 2010), as is a guidingthree-phase framework focused on pri-mary, secondary, and tertiary interventionstargeting the various needs of affected chil-dren postdisaster (La Greca & Silverman,2009). Nevertheless, implementing evi-dence-based interventions postdisasterrequires establishing collaborative partner-ships across diverse professionals and keystakeholders, and understanding the needsof the local partners who have undergonethe disaster. this is particularly salientwhen the researcher is not geographicallylocated in the affected area and desires tohelp by establishing collaborations with
local partners. Shortly after hurricanemaria made landfall, our team establisheda partnership with the Puerto Rico Depart-ment of education and local mental healthprofessionals to implement a multiphase,trauma-focused intervention model guidedby postdisaster best-practice guidelines.the current paper describes the key chal-lenges faced by our key partners postdisas-ter, what they found helpful and unhelpfulin working with other agencies and acade-mic institutions, and recommendations forestablishing respectful and fruitful partner-ships within a postdisaster context withlocal partners, especially when one is notlocated in the affected area. the challengesand recommendations presented below arewritten from the perspectives of our part-ners themselves (third through sixthauthors from the Puerto Rico Depatmentof education, Carlos Albizu University,and University of Puerto Rico) and arewritten in fist-person plural format,directly quoted or pharaphrased from theinterviews.
Challenges Faced in the ImmediateAftermath of the Disaster
Challenge #1: Magnitude of Impactthe entire island of Puerto Rico and all
of its inhabitants were impacted by thishurricane. We had to figure out how tohelp over 350,000 public school students.Almost everyone on the island had sufferedsome type of loss or damage to their homesand were trying to find out how theirfamily members were doing (roads wereimpassable, cell phone towers were down,and landlines were not functioning). theneed was unprecedented. In prior hurri-canes (e.g., hurricane Georges in 1998),only part of the island had been impactedand thus there was access to electricity,water, communications, gasoline, and shel-ter in other parts of the island, which madeit much easier to coordinate relief efforts.hurricane maria did not allow for thisoption. the first 2 to 3 weeks were thehardest. there was a sense of urgency andimpotence. We had no place to meet ini-tially as a staff. Due to roads being closedand lack of transportation (limited gasolinesupply, impassable roads), the responsibil-ity of restarting the public-school educa-tion system of an entire island fell on a fewstaff who were able to get to work, whilealso dealing with their own personal lossand needs. most government buildingswere closed and those opened had no elec-tricity, water, or Internet. Never in the his-tory of Puerto Rico had we had an event
Building Collaborative Partnerships AcrossProfessions to Implement Trauma-FocusedCognitive Behavioral Interventions AfterHurricane Maria in Puerto RicoRosaura Orengo-Aguayo and Regan W. Stewart,Medical University of South Carolina, Charleston
Karen G. Martínez González,University of Puerto Rico, Medical Sciences Campus
Joy Lynn Suárez Kindy,Carlos Albizu University and Puerto Rico Department of Education
María C. Christian Herrero and Inés Rivera Colón,Puerto Rico Department of Education
April • 2019 123
like this. An entire country was destroyed.the magnitude of the impact did not allowfor mobility, communications, flexibility orcreativity. We kept asking ourselves,“Where do you even start?”
Challenge #2: Inability to CommunicateFor weeks there was limited-to-no cell
phone signal, Internet service, or ability tocommunicate with colleagues, family, etc.this made it difficult to coordinate acade-mic and mental health relief efforts and toform a coordinated strategy between vari-ous agencies. We had emergency plans inplace, but we could not talk to each other.this also made it difficult to coordinateroles and responsibilities that fell under thepurview of a school principal versus centrallevel administration, for instance. mes-sages about where relief supplies werelocated were not getting to the communi-ties and schools. In many instances, socialworkers were going by foot and using wordof mouth to relay vital information. Welearned the importance of capitalizing onexisting resources, such as social workers,who are trained to do community needsassessments, visit homes, and connectpeople in need with resources. We werehumbled by the strong commitment ofsocial workers, psychologists, school staff,graduate school students, medical resi-dents, etc., to help community members,even while dealing with their own personalcrises.
Challenge #3: Balancing Various Basic,Emotional, and Academic Needs
School social workers tasked themselveswith going out into their communities,conducting a needs assessment, and pro-viding support. however, when theyarrived at the homes, families were desper-ate for food and water. When the socialworker explained that they were there tooffer emotional support and assess theirneeds first, the families were disappointed.this highlights the importance of sendingout your team with supplies to hand out tofamilies. that is what families need in theimmediate aftermath of a disaster. After afew weeks, children had been out of schooland their routines had been disrupted. Wehad to create a space to engage communi-ties and families to get access to basic needswhile also offering academic and recre-ational activities, as well as offer socioemo-tional support. Another challenge was bal-ancing these basic and socioemotionalneeds with the academic needs of studentsand guidance on how to prioritize thesewithin a postdisaster context, especially
because so many schools were completelydestroyed.
Challenge #4: Lack of Protocols,Guidelines, or Information
We set up community shelters in someschools, but were not exactly sure how toset them up, what the best-practice guide-lines were, what academic and socioemo-tional activities we should offer within thatspecific postdisaster period, or how thisplan would evolve months or years afterthe disaster. A disaster of this magnitudehad never impacted the island and, as such,we were unprepared. We are experts in ourlocal context, but we needed guidance fromoutside experts on what they had observedafter other natural disasters of this magni-tude and guidelines as to how to bestapproach children’s needs at various stagespostdisaster. We also needed to know frompostdisaster experts about the challengesthat were yet to come (not just in the short-term but also in the long-term recoveryperiods) and what interventions to imple-ment in the immediate aftermath to helpmitigate those effects. We were constantlywondering, “What can we do to help pre-vent lasting socioemotional and learningconsequences later?”
What Did Collaborators DoThat Was Helpful?
Helpful Strategy #1: Provide RespectfulExpertise and Guidance
We really appreciated partners who hadexpertise in postdisaster and trauma andprovided recommendations in a very con-crete, step-by-step way, and then invitedour comments and suggestions for tailor-ing these evidence-based guidelines to ourlocal context. Partners who were respectfuland flexible in integrating our suggestionswere the best collaborations we established.these partners shared their previous expe-riences and lessons learned and providedsuggestions, but reminded us that, ulti-mately, we were the experts on the localcontext. Some of our biggest questionswere as follows: What do we need to makesure we do now, to help mitigate the impactof this natural disaster one year or twodown the road? What are the challengesthat we need to prepare for and preventnow? What tools can we give our staff tohelp themselves and our students? Weneeded someone to explain complexresearch findings in easy-to-understandbullet points. Giving us a paper to read orfact sheets was not enough. We also appre-
ciated being able to discuss ideas with eachother and have ongoing communicationand tailoring of the plan with our partners.
Helpful Strategy #2: Be Flexible andAdjust to Our Needs
We greatly appreciated partners who,after hearing our unique needs or con-cerns, adapted flexibly. For instance, ourmUSC partner originally suggested imple-menting a PFA workshop with a certainnumber of teachers; however, we providedfeedback that we needed larger groups anda train-the-trainer approach, and theyagreed to accommodate to our needs. It’stough for us, when we are in crisis, to hear“No, we can’t do what you are asking.” Itwas also hard to be asked by so many part-ners, “What do you need?” We were over-whelmed with so many people wanting tohelp and were not always able to commu-nicate what we needed or when. this disas-ter was a new experience for us. We neededpartners who could say to us, “this is whatwe have to offer, based on the best availableevidence, and this is how we could do it—what are your thoughts?” We also appreci-ated partners who understood our realityand the limited resources we had available,who adapted protocols to the local contextwith feedback from local stakeholders, andwho welcomed our concerns or sugges-tions. Collaborations that started by askingfor our opinion about the needs of PuertoRico, instead of talking about their ideas,are the collaborations that have continuedto have an impact on the island today. Wealso appreciated partners who were willingto recognize the limits of their scope ofwork and willing to partner with other localor international partners in order to com-bine efforts and help us.
Helpful Strategy #3: Acknowledge LocalExpertise and Leverage It
When we collaborated with partnerswho were located in the mainlaid U.S., weappreciated those who recognized the localexpertise of mental health professionalswithin Puerto Rico. For example, at theUniversity of Puerto Rico (UPR) Center forthe Study and treatment of Fear and Anx-iety, we have been culturally adapting evi-dence-based psychotherapies since 2010.When hurricanes Irma and maría hitPuerto Rico on September 2017, we hadalready validated instruments in Spanish toassess for the most common posttraumaticsymptoms. Based on our research, we alsoknew what components of cognitive-behavioral therapy (CBt) were most effec-tive for our Puerto Rican population. In
124 the Behavior Therapist
O R E N G O - A G U A Y O E T A L .
our case, what we really needed guidanceon was how to administer assessments in apostdisaster setting. how can you imple-ment CBt in a population that has no elec-tricity, potable water, or food? We had thebenefit of being located in the major med-ical center of the island. this area was givena priority in terms of electricity and Inter-net access, which meant that 2 weeks afterhurricane maría, our Center was opened,and we focused our energy on seeking theevidence on how to deliver postdisastermental health care. In collaboration withour mUSC partners, we evaluatedresources from the National Child trau-matic Stress Network and created a train-ing on Psychological First Aid for thehealth professional students and faculty ofthe UPR medical Sciences Campus.During those first weeks after the hurri-cane, those training sessions also turnedinto a support mechanism for those healthprofessionals who were on the front linemanaging hurricane related emergencies.We appreciated partners who acknowl-edged our existing efforts and asked howthey could help us continue or expand ourefforts, rather than take over or replacethem.
Helpful Strategy #4: Help Builda Network of Collaborators
As our communications system startedto improve, we were able to connect withprofessionals outside of the UPR medicalSciences Campus. the Puerto Rico Chap-ter of the American Academy of Child andAdolescent Psychiatry (AACAP) helpedconnect us with the Disaster Committee ofAACAP, who provided information ongroups from the mainland U.S. who werestarting mental health initiatives in PuertoRico. We were appreciative of partnerswho were willing to act as liaisons and con-nect us with other efforts on the island sothat we would not be duplicating services,but rather uniting to achieve a commongoal.
Helpful Strategy #5: Provide Experien-tial (and Not Just Didactic) Workshops
Our school staff were ready to gainpractical skills and techniques that theycould implement within their communitiesand schools. We appreciated partners thatprovided some theory and relevantresearch, but whose focus was primarily onproviding us with concrete tools and skillsthat we could then use in our communitiesto help children and families cope withstress and loss. We also appreciated work-shops that explained common reactions
following traumatic events and the varioustrajectories of recovery in children. Forexample, understanding the concept ofresiliency and that not all students wouldexperience devastating long-term mentalhealth consequences gave us hope and arenewed commitment to help bolsterresiliency in our students through utilizingthe coping skills we were learning. Addi-tionally, we appreciated learning aboutwhat to expect in the immediate aftermath,but also what to look out for in the next 6months to 1 year so that school staff andmental health providers could be preparedand ready to identify and refer students forappropriate services across all stages ofpostdisaster recovery.
What Did Collaborators DoThat Was Unhelpful?
Unhelpful Strategy #1: Not Listeningto Our Needs First and Not AdaptingFlexibly
Partners that did not ask us what weneeded first and who did not adapt flexiblyto our concerns made collaborations diffi-cult. We appreciated their expertise, ofcourse, but we were not sure they would besuccessful in helping achieve our goals ifthey first did not take into account ourunique needs and situation. Additionally,partners who asked us what we needed, butdid not have a menu of options for us tochoose from, made it overwhelming for us.
Unhelpful Strategy #2: Asking forAcknowledgment or Publicity
Agencies or individuals who offeredhelp but required a press release or a publicannouncement in return were off-puttingand burdensome. We strongly encourageagencies and individuals who do postdisas-ter work to examine their motivations firstand only engage if there is a genuine desireto help, even if it goes unrecognized.
Partners who required our agencies ororganizations to coordinate all logistics ofa workshop or translate materials in timesof crisis and lack of access to electricity andtransportation, made things harder for us.We were more than willing to help, butwould have preferred that partners assistwith the coordination of such efforts andengage in creative problem-solving with usas well. Although we appreciated the inter-national support, we had difficulties coor-dinating relief efforts and activities forindividuals who did not speak Spanish, but
who expected an interpreter would be pro-vided. Coordinating this level of logisticalsupport during the aftermath of a disasteradds undue burden to the local partners.Interested partners who do not speak thelocal language should provide their owninterpretation personnel or expand theirteam to include individuals who speak thelocal language.
Recommendations for BuildingStrong Partnerships Post-Disaster
Recommendation #1: Understand theLocal Context and the Effects of theDisaster First
establish respectful conversations (inthe main language spoken in the area) tofirst understand what your local stakehold-ers and partners have experienced. Under-stand the nuances of a postdisaster contextand how taxing and difficult this experi-ence has been for your local partner.
Learn to communicate evidence-basedinterventions and approaches in an easy-to-understand manner, using bullet points.Develop a potential menu of options, basedon the best available evidence, that is sensi-tive to what you learned about the localcontext and unique needs. then, listen tothe local partners’ feedback and concerns,be flexible, and adapt your approaches to fitthe local needs, language, and culture. Aone-size-fits-all approach is not likely to befruitful.
Recommendation #3: AcknowledgeLocal Expertise and Leverage It
Your local partners have a plethora ofexisting resources, experiences, and work-force that should not only be acknowl-edged and respected, but incorporated intoany postdisaster intervention approach.
Recommendation #4: Commit toHelping Long Term If Possible
It is common for most of the help after amajor disaster to come in the immediateaftermath. however, local partners needthe help in both the short- and long-termrecovery phases. It is important to designpostdisaster intervention plans that takeinto consideration the long-term mentalhealth needs of the population as well as thelong-term needs of your partnering localorganization.
April • 2019 125
T R A U M A - F O C U S E D C B T I N P U E R T O R I C O
Oftentimes we wait to establish partner-ships until after a disaster has occured. Weencourage partnerships to be built before adisaster to allow time to develop a plan,train the local mental health workforce inevidence-based CBt interventions that willbe useful in the event of a disaster, and haveongoing communication established sothat when a disaster does strike, protocolswill be in place and a plan can be easilyenacted.
Recommendation #6: Build Partner-ships Across Professionals and Encour-age an Active Exchange of Ideas
Social workers, psychologists, psychia-trists, counselors, teachers, doctors, andreseachers can do more to improve themental health of children postdisasterwhen they partner together than when theytry to enact efforts in silos. the biggestlesson learned in the establishment of thesepartnerships post–hurricane maria wasthe value of adding unique and rich per-spectives across professionals. these estab-lished partnerships and collaborations arehelping inform targeted and sustainableevidence-based practices aimed at improv-ing mental health outcomes for PuertoRico’s youth following the devastation ofhurricane maria.
ReferencesBerkowitz, S., Bryant, R., Brymer, m., ham-
blen, J., Jacobs, A., Layne, C., . . . Watson,P. (2010). The National Center for PTSD& the National Child Traumatic StressNetwork, Skills for Psychological Recovery:Field Operations Guide. Washington, DC:U.S. Department of Veterans Affairs.
Bonnano, G. A., Brewin, C. R., Kaniasty, K.,& Greca, A. m. L. (2010). Weighing thecosts of disaster: Consequences, risks, andresilience in individuals, families, andcommunities. Psychological Science in thePublic Interest, 11, 1-49.doi:10.1177/1529100610387086
Brymer, m., Jacobs, A., Layne, C., Pynoos,R., Ruzek, J., Steinberg, A., Vernberg, e.,& Watson, P. (National Child traumaticStress Network and National Center forPtSD). (2006). Psychological First Aid:Field Operations Guide (2nd ed., July,2006). Retrieved from www.ncptsd.va.gov
Cohen, J.A., mannarino, A.P., & Deblinger,e. (2017). Treating trauma and traumaticgrief in children and adolescents (2nd ed.).New York: Guilford Press.
from https://www.fema.gov/media-library-data/15336432621956d1398339449ca85942538a1249d2ae9/2017FemAhurricaneAARv20180730.pdf
hinojosa, J., & meléndez e. (2018). thehousing crisis in Puerto Rico and theimpact of hurricane maria. Center forPuerto Rican Studies (RB2018-04).Retrieved from https://centropr.hunter.cuny.edu/sites/default/files/data_briefs/housingPuertoRico.pdfhttps://centropr.hunter.cuny.edu/sites/default/files/data_briefs/housingPuertoRico.pdf.
hobfoll, S. e., Watson, P., Bell, C. C.,Bryant, R. A., Brymer, m. J., Friedman, m.J., . . . Ursano, R. J. (2007). Five essentialelements of immediate and mid-termmass trauma intervention: empirical evi-dence. Psychiatry, 70, 283-315. doi:10.1521/psyc.2007.70.4.283
Kishore, N., marqués, D., mahmud, A.,Kiang, m.V., Rodriguez, I., Fuller, A., . . .Buckee, C. (2018). mortality in PuertoRico after hurricane maria. New EnglandJournal of Medicine, 379, 162-170.
La Greca, A.m. & Silverman, W.K. (2009).treatment and prevention of posttrau-matic stress reactions in children and ado-lescents exposed to disaster and terrorism:What is the evidence? Child DevelopmentPerspectives, 3, 4-10
Seballos, t., tanner, m., tarazona, & Galle-gos, J. (2011). Children and disasters:Understanding impact and enablingagency. Retrieved from https://www.unc-clearn.org/sites/default/files/inventory/unicef09.pdf
. . .
this work was funded in part by a SubstanceAbuse and mental health Services Adminis-tration (SAmhSA) National Child trau-matic Stress Network Category III Grant(1U79Sm063224). the views presented inthis article do not represent the views of theSubstance Abuse and mental health Ser-vices Administration, the National Childtraumatic Stress Network, the Puerto RicoDepartment of education, Carlos AlbizuUniversity, or the University of Puerto Rico.Correspondence to Rosaura Orengo-Aguayo, Ph.D., medical University of SouthCarolina, Department of Psychiatry &Behavioral Sciences, National Crime Vic-tims Research & treatment Center, 67thPresident Street, mSC 861, Charleston, SC29425; [email protected]
ABCT’sMedicalEducatorDirectoryInclusion Criteria1. Must teach or have recently taught CBTand/or CB interventions in a medical set-ting. This may include psychiatric residents,medical students, nursing, pharmacy, den-tistry, or other allied health professionals,such as PT, OT, or RD. Teachers who exclu-sively train psychology graduate students,social workers, or master’s level therapistsdo not qualify and are not listed in thisdirectory.2. “Teaching” may include direct training orsupervision, curriculum development, com-petency evaluation, and/or curriculumadministration. Many professionals on thelist have had a central role in designing anddelivering the educational interventions,but all educational aspects are important.3. Training should take place or be affiliatedwith an academic training facility (e.g. med-ical school, nursing school, residency pro-gram) and not occur exclusively in privateconsultations or paid supervision.
Please note that this list is offered as a ser-vice to all who teach CBT to the medicalcommunity and is not exhaustive.
To submit your name for inclusion in theMedical Educator DirectoryIf you meet the above inclusion criteria andwish to be included on this list, please sendthe contact information that you would likeincluded, along with a few sentencesdescribing your experience with trainingphysicians and/or allied health providers inCBT to Shona Vas at [email protected] include “Medical Educator Directory” inthe subject line.
DIsClaIMER. Time and availability to participate insuch efforts may vary widely among the educa-tors listed. It is up to the individuals seeking guid-ance to pick who they wish to contact and to eval-uate the quality of the advice/guidance theyreceive. ABCT has not evaluated the quality ofpotential teaching materials and inclusion on thislist does not imply endorsement by ABCT of anyparticular training program or professional. Thepeople in this listing serve strictly in a volunteercapacity.
126 the Behavior Therapist
O R E N G O - A G U A Y O E T A L .
BeGINNING SOON AFteR September 11,2001, U.S. military personnel whodeployed to Afghanistan, Iraq, and othernearby locations have been at significantrisk for the development of combat-relatedposttraumatic stress disorder (PtSD).After several years of sustained militaryconflict, several studies highlightedcombat-related PtSD as one of the signa-ture psychological wounds of war in thisnew generation of warfighters (hoge et al.,2004; Institute of medicine, 2008;tanielian & Jaycox, 2008). these studiesalso highlighted combat-related PtSD inactive-duty military personnel as a condi-tion of significant military and nationalpublic health interest.
Initial research on the treatment ofcombat-related PtSD in military veteransbegan in the early 1980s by terence Keaneand colleagues and focused on imaginalflooding (Black & Keane, 1982; Keane &Kaloupek, 1982). the initial series of largePtSD randomized clinical trials focused oncivilian female sexual assault victims (Foa,Rothbaum, Riggs, & murdock, 1991;Resick & Schnicke, 1992). these studies ledto the proliferation of prolonged exposuretherapy (Foa, hembree, & Rothbaum,2007) and cognitive processing therapy(Resick, monson, & Chard, 2017), the twomost popular and thoroughly researchedtreatment approaches for PtSD.
Up until very recently, there has been adearth of research on the treatment ofcombat-related PtSD in active-duty mili-tary personnel. to help address theimpending national public health crisis ofcombat-related PtSD in post-9/11 militarypersonnel, the U.S. Congress approved a900-million dollar Department of Defense(DoD) appropriation in 2007. this appro-priation helped establish the Psychologicalhealth and tBI Research Program as part
of the Congressionally Directed medicalResearch Program under the direction ofthe U.S. Army's medical Research andmateriel Command at Fort Detrick, mary-land. the StRONG StAR Consortium(South texas Research OrganizationalNetwork Guiding Studies on trauma AndResiliency) was funded in 2008 as a 5-yearaward as part of the defense appropriation.the StRONG StAR Consortium included14 research projects and 5 research coresand was focused on the assessment andtreatment of combat-related PtSD and co-occurring conditions in active-duty mili-tary personnel. StRONG StAR includedthe collaboration of many of the nation'sleading civilian, DoD, and VeteransAdministration (VA) investigators andinstitutions.
During the past decade, more than 30additional StRONG StAR–affiliated pro-jects have been funded to continue thework on combat-related PtSD and co-occurring conditions (e.g., suicide, insom-nia, chronic pain, substance use disorders,tinnitus, etc.) in active-duty military andveteran populations. StRONG StARinvestigators have now successfully com-pleted several of the largest clinical trials inDoD history, demonstrating that combat-related PtSD can be effectively treated ingarrison (after returning from deploy-ment) using cognitive processing therapy(Resick et al., 2015, 2017), prolonged expo-sure therapy (Foa et al., 2018), and anabbreviated version of prolonged exposuredelivered in military primary-care settingsusing internal behavioral health consul-tants (Cigrang et al., 2011, 2015, 2017).these studies have shown that approxi-mately half of the service members nolonger meet diagnostic criteria for PtSDafter the completion of treatment and thattheir treatment gains are maintained over a
6-month follow-up period. Although thesefindings are the strongest to date regardingthe treatment of combat-related PtSD inactive-duty military personnel, there isample room for improvement.
One approach to potentially improveoutcomes for combat-related PtSD is tointervene early, soon after exposure tocombat trauma. early interventions forcombat-related acute stress disorder (3days to 1 month after trauma exposure) orPtSD (more than 1 month after traumaexposure) delivered during militarydeployments have the potential to signifi-cantly reduce the long-term consequencesof chronic PtSD. there are strong datafrom civilian populations demonstratingthat early cognitive behavioral therapy(CBt) interventions soon after traumaexposure can prevent the development ofPtSD. For example, several studies haveshown that only about 20% of patientstreated with brief CBt for acute stress dis-order after trauma exposure meet criteriafor PtSD at the posttreatment follow-uppoint (Bryant, harvey, & Dang, 1998;Bryant, moulds, & Nixon, 2006; Bryant,Sackville, & Dang, 1999; Shalev et al., 2012).this compares favorably, for example, withthe 57% of participants who were in a wait-list condition in the Shalev et al. study whomet criteria for PtSD at the 5-monthfollow-up point.
Although treating PtSD during mili-tary deployments is of great importance,there are a number of challenges and spe-cial considerations in treating PtSD in themilitary combat zone. As a result, only afew studies have been conducted on thetreatment of PtSD in the combat theater,and relatively few deployed military behav-ioral health providers have employed evi-dence-based treatments for PtSD. thisarticle provides a brief review of the impor-tance, challenges, and special considera-tions in the treatment of PtSD in a nontra-ditional setting—the military combattheater.
The Importance of Treating PTSDDuring Military Deployments
If PtSD can be successfully treatedwhile service members are still deployed, itincreases the chances that they can remainwith their unit to successfully completetheir deployment. Undoubtedly, there areenormous psychological health benefits ofremaining with one’s unit to successfullycomplete a military deployment. militaryunit cohesion has been found to be a signif-icant protective factor related to PtSD and
Treating Combat-Related Posttraumatic StressDisorder During Military Deployments:Importance, Challenges, and SpecialConsiderationsAlan L. Peterson, University of Texas Health Science Center at SanAntonio, South Texas Veterans Health Care System, University ofTexas at San Antonio
Casey L. Straud and Wyatt R. Evans, University of Texas HealthScience Center at San Antonio
April • 2019 127
psychological resiliency (Dickstein et al.,2010; Zang et al., 2017). however, for avariety of reasons, many military behav-ioral health providers do not believe thatcombat-related PtSD should be treatedduring deployments. Instead, they believePtSD should only be treated in garrison, orafter the service member has returned fromdeployment. Unfortunately, this leavesdeployed military behavioral healthproviders in a bind regarding the appropri-ate disposition of PtSD patients: (a) treatpatients in theater using evidence-basedtreatments for PtSD such as prolongedexposure or cognitive processing therapy;(b) classify service members as havingcombat operational stress reactions, nor-malize their symptoms, provide brief sup-portive counseling, and encourage them tocontinue their deployed military duties; or(c) aeromedically evacuate service mem-bers with PtSD out of the combat theaterso they can be treated in garrison.
Unfortunately, research has shown thatpsychiatric aeromedical evacuation out ofthe combat theater can significantlyincrease the likelihood of a medical dis-charge from the military. the inability tocomplete a military deployment—arguablythe most important assignment of a servicemember’s military career—because of apsychiatric condition is a strong indicationthat an individual may not be fit for mili-tary service. Peterson et al. (2018) foundthat service members who were aeromed-ically evacuated from the deployment the-ater for a psychiatric disorder were almostfour times as likely to be subsequently sep-arated from the military. this finding hasimportant clinical and military operationalimplications regarding the utility of treat-ing psychiatric conditions in theater, whenclinically appropriate, as opposed to a psy-chiatric aeromedical evacuation.
Challenges in Treating Combat-Related PTSD During Military
Deploymentsthere are a number of challenges in
treating combat-related acute stress disor-der and PtSD during military deploy-ments. these challenges have limited theuse of evidence-based treatments for thetreatment of these conditions by deployedmilitary mental health providers. the chal-lenges have also made it very difficult toconduct prospective, Institutional ReviewBoard–approved research on these topicsin deployed settings.
Combat Operational Stress ReactionsOne challenge in treating acute stress
disorder and PtSD in deployed settings isthat many military behavioral healthproviders are reluctant to give these diag-noses in an active combat zone. Some mil-itary providers believe that acute stress dis-order or PtSD cannot be diagnosed ortreated while active combat operations areongoing. Instead, the term “combat opera-tional stress reactions” is used, which refersto transient reactions to stressors present incombat and everyday operations indeployed environments (Potter, Baker,Sanders, & Peterson, 2009).
the U.S. Army’s published guidelineson Combat and Operational Stress Control(Department of the Army, 2006, 2016) sup-port these general principles. A combat andoperational stress reaction is described as“a negative adaptation to high stress eventsand potentially traumatic stress exposure”(Department of the Army, 2016, p. 5-3).these guidelines recommend that combatand operational stress interventions beused to treat combat and operational stressreactions. Although the use of the termcombat operational stress reactions mayhelp reduce the stigma of PtSD and nor-malize combat stress reactions, it mayinadvertently also lead to confusion onhow to treat this condition. Whereas sev-eral empirically supported treatments existfor acute stress disorder and PtSD, no suchtreatments exist for combat operationalstress reactions. If acute stress disorder andPtSD are not diagnosed during militarydeployments, then evidence-based inter-ventions for these disorders are not likelyto be employed.
Combat Operational Stress Controlthe distinctions between acute stress
disorder, PtSD, and combat operationalstress reactions are not clear. If combatoperational stress reactions are consideredsubthreshold acute stress disorder andPtSD, then the DoD guidelines to use gen-eral combat and operational stress inter-ventions makes sense. the mental healthconcept of operations for treating combatoperational stress reactions during deploy-ments is based on the BICePS (brevity,immediacy, contact, expectancy, and sim-plicity) or PIeS (proximity, immediacy,expectancy, and simplicity) models(Department of the Army, 2006, 2016).Although both models have strong facevalidity, minimal empirical data supporttheir efficacy, and neither outline the use ofany specific evidence-based treatments foracute stress disorder or PtSD.
the U.S. military employs many of theworld’s most intensive and sophisticatedcombat operational training methods. As aresult, the majority of deployed militarypersonnel (about 85%) exposed to combatand operational stressors manage theseevents exquisitely and do not requirebehavioral health treatment (hoge et al.,2004). those who experience combat oper-ational stress reactions, or subthresholdsymptoms of acute stress disorder orPtSD, may benefit from general combatand operational stress interventions, whileothers are likely to recover without anyformal treatment. however, those whomeet the Diagnostic and Statistical Manualof Mental Disorders (5th ed.; AmericanPsychiatric Association, 2013) criteria foracute stress disorder and PtSD may notrespond to the standard combat and oper-ational stress interventions.
Common Concerns About TreatingPTSD During Military Deployments
A common concern among militaryclinicians and policymakers is that the useof trauma-focused therapies—such as pro-longed exposure or cognitive processingtherapy—in deployed locations will lead toincreased distress, decompensation,increased suicide risk, and the possibleneed for psychiatric hospitalization oraeromedical evacuation. Unfortunately,although most of these concerns are likelyto be unfounded, that lack of research con-ducted in deployed locations prevents astrong argument to counter these con-cerns.
Another concern among military healthproviders is that it is not possible to delivera full CBt protocol based on provider andpatient availability. Standard outpatienttreatment protocols for PtSD, such as pro-longed exposure and cognitive processingtherapy, involve weekly 60- to 90-minutesessions over the course of 3 to 4 months.this format may not be practical indeployed locations. the expectations that aservice member will engage in weekly ses-sions and homework over a period of sev-eral months may be too demanding fordeployed service members who are alsomanaging daily occupational demands.the combination of these factors presentsobstacles to adherence to the traditionalformats of evidence-based PtSD psy-chotherapy protocols. however, researchsuggests evidence-based protocols can beflexibly adapted and modified for use indeployed locations.
128 the Behavior Therapist
P E T E R S O N E T A L .
Special Consideration for theTreatment of PTSD During
Military Deploymentsthe first study to evaluate the use of an
evidence-based treatment for combat-related PtSD was a clinical case series con-ducted by three military clinical psycholo-gists (including one of the co-authors forthe current manuscript; AP) deployed toIraq during 2004–2005 (Cigrang, Peterson,& Schobitz, 2005). each of the patientstreated had experienced multiple deploy-ment-related traumas, but there had beenone recent trauma that was the most dis-tressing trauma (i.e., the DSm Criterion Aevent) that led them to seek treatment.
the Posttraumatic Stress DisorderChecklist for military personnel (PCL-m)was used to assess PtSD symptoms(Weathers, Litz, herman, huska, & Keane,1993). each of these military psychologistsadapted the standard prolonged exposureprotocol for use in the deployed setting. Atotal of four prolonged exposure therapysessions were completed for each of thepatients, referred to as Cases A, B, and C.Imaginal exposure focused on the reviewand processing of the traumatic event. Invivo exposure targeted avoidance, isola-tion, and withdrawal. Common items onan in vivo hierarchy included relatively safeactivities that were being avoided by thepatients that were part of normal deploy-ment life on a Forward Operating Base.Such activities included going to the diningfacility for a meal or going to the commu-nications center to make a phone call orsend an email to friends or family.
the results indicated that there weresignificant reductions over the four pro-longed exposure treatment sessions foreach of the patients. Case A’s PCL-m scoredecreased from 69 to 24, Case B’s PCL-mdecreased from 59 to 39, and Case C’s PCL-m decreased from 67 to 20. A 10-pointreduction on the PCL-m is commonlyidentified as a clinically meaningfulchange. By this common rubric, all threepatients demonstrated significant PtSDsymptom reductions following a briefPtSD intervention and were able to suc-cessfully return to duty and complete theirfull deployment rotations.
A second case series of combat-relatedPtSD treatment in a deployed setting wasconducted by psychologists deployed toCamp Fallujah, Iraq (mcLay, mcBrien,Widerhold, & Wiederhold, 2010). tenactive-duty service members were treatedwith a modified prolonged exposure proto-col or a virtual reality–based prolonged
exposure protocol. A retrospective reviewof their clinical records indicated that 90%of patients no longer met criteria for PtSDat posttreatment and that both treatmentmodalities demonstrated significant bene-fits. Service members also reporteddecreases in depression and anxiety, andno service member had to be aeromedicallyevacuated from theater due to PtSD.
Pelton, Wangelin, and tuerk (2015)delivered prolonged exposure therapy to adeployed service member with a combinedface-to-face and telehealth treatmentmodality. Initial stages of prolonged expo-sure therapy were completed at a largerForward Operating Base followed by tele-health videoconferencing to the servicemember’s smaller, remote combat outpost.the service member reported markedimprovements at posttreatment. Findingsfrom this study highlight the benefits ofprolonged exposure in a deployed settingand the utility of telehealth technology toenhance treatment accessibility todeployed service members.
the largest prospective, military Insti-tutional Review Board–approved clinicaltrial to date on the treatment of PtSD in adeployed combat zone was funded by theDoD as part of the StRONG StAR Con-sortium, and it evaluated treatment out-comes in 12 active-duty service membersdeployed to Iraq or Afghanistan (Petersonet al., under review). Service members weretreated by deployed military behavioralhealth providers using prolonged exposure(n = 6) or cognitive processing therapy (n =6). the prolonged exposure adaptationswere similar to what was described previ-ously in the Cigrang et al. (2005) study.Cognitive processing therapy targetedunhealthy cognitions that could interferewith military duties during deploymentsuch as “No one can be trusted!”
the results indicated that participantstreated with prolonged exposure reportedsignificant symptom reductions (averagereduction of 19.2 points on the PCL-m),indicative of a large treatment effect (d =-1.28). Participants treated with cognitiveprocessing therapy demonstrated a clini-cally meaningful mean reduction on thePCL-m (10.5 point reduction), but thesechanges were not statistically significant.these findings suggest that prolongedexposure and cognitive processing therapycan be safely and effectively used indeployed settings.
Summarythe deployed combat theater is an
unconventional setting for the delivery ofCBt interventions. Although it is often notfeasible to deliver the same trauma-focusedtreatment protocols for PtSD that are usedin traditional settings, many CBt interven-tions are remarkably robust and flexibleand can be adapted to a variety of nontra-ditional settings. the initial results of caseseries reports and a small clinical trial forthe treatment of acute stress disorder andPtSD in the combat theater are remark-ably similar to the results found in civiliansettings. Brief, four- to five-session treat-ment protocols, similar to those developedby Bryant and colleagues for acute stressdisorder in civilian populations (Bryant etal., 1998, 1999, 2006), have been shown toyield similar results for military personnelin deployed settings (Cigrang et al., 2005;mcLay et al., 2010; Pelton et al., 2015;Peterson et al., under review).
evidence from these studies suggeststhat adapting the traditional CBt protocolsfor use in deployed settings does notdiminish treatment outcomes. Larger clin-ical trials conducted in deployed settingswith long-term follow-up are needed.Unfortunately, this is unlikely to occur atany time in the near future. Conductingresearch in deployed combat locations isextremely difficult. the specific challengesto this process are beyond the scope of thecurrent paper. Suffice it to say that the firstauthor of this manuscript (AP) spent over 4years obtaining regulatory approvals (mili-tary Institutional Review Board, JointCombat Casualty Research team, and thehuman Research Protection Office at FortDetrick, maryland) and then collectingdata on 12 deployed service memberstreated by deployed military clinicians whoserved as individual site principle investi-gators at multiple locations throughoutIraq and Afghanistan (Peterson et al.,2018). With the official end date of Opera-tion Iraqi Freedom in 2010 and Operationenduring Freedom in 2014, the JointCombat Casualty Research team was dis-banded and redeployed to their home mil-itary stations. As a result, research indeployed U.S. military locations is nolonger permitted.
most cognitive behavioral therapies areincredibly robust and the standard treat-ment protocols can be adapted or modifiedfor use in nontraditional settings. Pro-longed exposure and cognitive processingtherapy are two battle-hardened CBtinterventions that have been found to be
April • 2019 129
C O M B A T - R E L A T E D P T S D
safe and effective when adapted fordeployed military settings. It is essentialthat the U.S. military continue to train mil-itary behavioral health providers to deliverevidence-based CBt protocols in nontra-ditional settings across the globe.
Diagnostic and statistical manual ofmental disorders (5th ed.). Washington,DC: Author.
Black, J. L., & Keane, t. m. (1982). Implo-sive therapy in the treatment of combatrelated fears in a world war II veteran.Journal of Behavior Therapy and Experi-mental Psychiatry, 13, 163-165.
Bryant, R.A., harvey, A. G., & Dang, S. t.(1998). treatment of acute stress disor-der: A comparison of cognitive-behav-ioral therapy and supportive counseling.Journal of Consulting and Clinical Psy-chology, 66, 862-866.
Bryant, R. A., moulds, m.L., & Nixon, R.D. V. (2006). hypnotherapy and cogni-tive behavior therapy of acute stress dis-order: A 3-year follow-up. BehaviourResearch and Therapy, 41, 489-494.
Bryant, R.A., Sackville, t., & Dang, S. t.(1999). treating acute stress disorder: Anevaluation of cognitive behavior therapyand supporting counseling techniques.American Journal of Psychiatry, 156,1780-1786.
Cigrang, J. A., Peterson, A. L., & Schobitz,R. P. (2005). three American troops inIraq: evaluation of a brief exposure ther-apy treatment for the secondary preven-tion of combat-related PtSD. PragmaticCase Studies in Psychotherapy, 1(2), 1-25.
Cigrang, J. A., Rauch, S. A., Avila, L. L.,Bryan, C. J., Goodie, J. L., hryshko-mullen, A., Peterson, A. L., & theStRONG StAR Consortium. (2011).treatment of active-duty military withPtSD in primary care: early findings.Psychological Services, 8(2), 104-113.doi:10.1037/a0022740
Cigrang, J. A., Rauch, S. A. m., mintz, J.,Brundige, A., Avila, L. L., Bryan, C. J., …Peterson, A. L., & the StRONG StARConsortium (2015). treatment of activeduty military with PtSD in primary care:A follow-up report. Journal of AnxietyDisorders, 36, 110-114.
Cigrang, J. A., Rauch, S. A., mintz, J.,Brundige, A. R., mitchell, J. A., Najera,e., … Peterson, A. L., for the StRONGStAR Consortium. (2017). movingeffective treatment for posttraumaticstress disorder to primary care: A ran-domized controlled trial with active dutymilitary. Family, Systems, and Health, 35,450-462.
Department of the Army. (2006). Combatand operational stress control. [Fieldmanual Number 4-02.51] (8-51). Wash-ington, DC: headquarters, Departmentof the Army. Retrieved from https://fas.org/irp/doddir/army/fm4-02-51.pdf
Department of the Army. (2016). Aleader’s guide to soldier health and fit-ness. Army Techniques Publication 6-22.5. Washington, DC: headquarters,Department of the Army. Retrieved fromhttps://armypubs.army.mil/epubs/DR_pubs/DR_a/pdf/web/atp6_22x5.pdf
Dickstein, B. D., mcLean, C. P., mintz, J.,Conoscenti, L. m., Steenkamp, m. m.,Benson, t. A., . . . Litz, B. t. (2010). Unitcohesion and PtSD symptom severity inAir Force medical personnel. MilitaryMedicine, 175, 482-486.doi:10.7205/mILmeD-D-09-00178
Foa, e. B., hembree, e. A., & Rothbaum,B. O. (2007). Prolonged exposure therapyfor PTSD: Emotional processing of trau-matic experiences therapist guide. NewYork: Oxford University Press.
Foa, e. B., mcLean, C. P., Zang, Y., Rosen-field, D., Yadin, e., Yarvis, J. S., … Peter-son, A. L., for the StRONG StAR Con-sortium. (2018). effect of prolongedexposure therapy delivered over 2 seeksvs 8 seeks vs present centered therapy onPtSD severity in military personnel: Arandomized clinical trial. Journal of theAmerican Medical Association, 319, 354-364. https://doi.org/10.1001/jama.2017.21242
Foa, e. B., Rothbaum, B. O., Riggs, D. S., &murdock, t. B. (1991). treatment ofposttraumatic stress disorder in rape vic-tims: A comparison between cognitive-behavioral procedures and counseling.Journal of Consulting and Clinical Psy-chology, 59, 715-723.
hembree, e. A., Foa, e. B., Dorfan, N. m.,Street, G. P., Kowalski, J., & tu, X.(2003). Do patients drop out prematurelyfrom exposure therapy for PtSD? Jour-nal of Traumatic Stress, 16, 555-562.
hoge, C. W., Castro, C. A., messer, S. C.,mcGurk, D., Cotting, D. I., & Koffman,R. L. (2004). Combat duty in Iraq andAfghanistan, mental health problems,and barriers to care. New England Jour-nal of Medicine, 351, 13-22.doi:10.1056/NeJmoa040603
Institute of medicine. (2008). Treatment ofposttraumatic stress disorder: An assess-ment of the evidence. Washington, DC:National Academies Press.
Keane, t. m., & Kaloupek, D. G. (1982).Imaginal flooding in the treatment of aposttraumatic stress disorder. Journal ofConsulting and Clinical Psychology, 50,138-140.
mcLay, R. N., mcBrien, C., Wiederhold,m. D., & Wiederhold, B. K. (2010). expo-
sure therapy with and without virtualreality to treat PtSD while in the combattheater: A parallel case series. Cyberpsy-chology, Behavior, and Social Networking,13(1), 37-42.
Pelton, D., Wangelin, B., & tuerk, P.(2015). Utilizing telehealth to supporttreatment of acute stress disorder in atheater of war: Prolonged exposure viaclinical videoconferencing. TelemedicineJournal and E-Health, 21, 382-387.http://dx.doi: 10.1089/tmj.2014.0111
Peterson, A., Foa, e., Resick, P., hoyt, t.,Straud, C. L., moore, B., … mintz, J.; forthe StRONG StAR Consortium. (underreview). A nonrandomized trial of pro-longed exposure and cognitive process-ing therapy for the treatment of combat-related posttraumatic stress disorder indeployed settings.
Peterson, A. L., hale, W. J., Baker, m. t.,Cigrang, J. A., moore, B., Straud, C. L., …mintz, J., for the StRONG StAR Con-sortium. (2018). Psychiatric aeromedicalevacuations of deployed active duty U.S.military personnel during Operationsenduring Freedom, Iraqi Freedom, andNew Dawn. Military Medicine, 183, 649-658.
Potter, A. R., Baker, m. t., Sanders, C. S.,& Peterson, A. L. (2009). Combat-stressreactions during military deployments:evaluation of the effectiveness of combatstress control treatment. Journal ofMental Health Counseling, 31, 137-148.
Resick, P. A., & Schnicke, m. K. (1992).Cognitive processing therapy for sexualassault victims. Journal of Consulting andClinical Psychology, 60, 748-756.
Resick, P. A., Wachen, J. S., Dondanville,K. A., Pruiksma, K. e., Yarvis, J. S., Peter-son, A. L., mintz, J. & the StRONGStAR Consortium. (2017). A random-ized controlled trial comparing groupwith individual cognitive processingtherapy in active duty military seekingtreatment for PtSD. JAMA Psychiatry,74, 28-36. Published online November23, 2016. doi:10.1001/jamapsychia-try.2016.2729
Resick, P. A., Wachen, J. S., mintz, J.,Young-mcCaughan, S., Roache, J. D.,Borah, A. m., … Peterson, A. L., onbehalf of the StRONG StAR Consor-tium. (2015). A randomized clinical trialof group Cognitive Processing therapycompared with group Present-Centeredtherapy for PtSD among active dutymilitary personnel. Journal of Consultingand Clinical Psychology, 83, 1058-1068.doi:10.1037/ccp0000016
130 the Behavior Therapist
P E T E R S O N E T A L .
Shalev, A. Y., Ankri, Y., Israeli-Shalev, Y.,Peleg, t., Adessky, R., & Freedman S.(2012). Prevention of posttraumaticstress disorder by early treatment:Results from the Jerusalem trauma Out-reach and Prevention study. Archives ofGeneral Psychiatry, 69, 166-176.doi:10.1001/archgenpsychiatry.2011.127.doi:10.1002/jts.20270
tanielian, t., & Jaycox, L. h. (eds.).(2008). Invisible wounds of war: Psycho-logical and cognitive injuries, their conse-quences, and services to assist recovery.Santa monica, CA: RAND Corporation.
Weathers, F. W., Litz, B. t., herman, D.S., huska, J. A., & Keane, t. m. (1993,October). The PTSD Checklist (PCL):Reliability, validity, and diagnostic util-ity. Paper presented at the 9th annualmeeting of the International Society fortraumatic Stress Studies, San Antonio,tX.
Zang, Y., Gallagher, t., mcLean, C. P.,tannahill, h., Yarvis, J.S., Foa, e. B., &the StRONG StAR Consortium. (2017).the impact of social support, unit cohe-sion, and trait resilience on PtSD intreatment-seeking military personnelwith PtSD: the role of posttraumaticcognitions. Journal of PsychiatricResearch, 86, 18-25. http://dx.doi.org/10.1016/j.jpsychires.2016.11.005. StRONGStAR Consortium group authorsinclude (alphabetically): e.V. Borah,K.A. Dondanville, B. t. Litz, J. mintz, A.L. Peterson, J. D. Roache, e. Yadin & S.Young-mcCaughan.
. . .
the authors do not have any conflicts ofinterest or funding to disclose.Correspondance to Alan L. Peterson,Ph.D., ABPP, Department of Psychiatry,School of medicine, University of texashealth Science Center at San Antonio, 7550Interstate highway 10 West, Suite 1325, SanAntonio, tX [email protected]
Global Mental Health (GMH)Treatment Gap
the needs for mental health and substanceuse treatment far overwhelm the capacityof currently available services globally, withlow- and middle-income countries(LmICs) being disproportionately bur-dened by this treatment gap. major depres-sive disorder (mDD) is now the singlelargest contributor to disability worldwideof any physical or mental disorder, in addi-tion to the burden of disease attributable toall other psychiatric disorders (Worldhealth Organization [WhO], 2017). thelimited capacity of currently available ser-vices to meet this enormous need has beendriven by historically limited fundingavailable for dedicated mental health ser-vices and a dearth of health care workerswith training in mental health care(DeSilva, Samele, Saxena, Patel, & Darzi,2014; Kakuma et al., 2011). Across all typesof mental health providers, low-incomecountries have on average 1.6 mentalhealth providers per 100,000 population(WhO, 2018). As of 2015, these humanresource shortages resulted in an estimatedshortage of 1,710,000 full-time equivalentmental health providers across 144 coun-tries (Scheffler et al., 2011). these nationalshortages are exacerbated by the dispro-portionate distribution of mental healthproviders in urban areas and within theprivate sector, meaning that ratio of mentalhealth providers to 100,000 population canbe much lower than 1–2 to 100,000 in prac-tice (Rathod et al., 2017; Vergunst, 2017;WhO, 2018). Given the scarcity of trainedmental health providers in many underre-sourced settings, particularly in rural areas,there is a need not only to expand opportu-nities for training mental health providersbut also an urgent need to understand how
to train and supervise lay health workers inbehavioral interventions and extend theworkforce for mental health care to addressthe Gmh treatment gap. these efforts relyon intensive ongoing supervision in com-bination with training (Lund, Caldas deAlmeida, Whiteford, & mahoney, 2013;monson et al., 2018; Smith et al., 2017).Given its relatively straightforward, time-limited, efficient and evidence-basedapproach, cognitive behavioral therapy(CBt) may be a good candidate for effi-cient and effective delivery using task-shar-ing models in resource-limited settingsglobally. CBt’s structured, time-limitedapproach is also appealing in that it canimprove the ease of training (Papas et al.,2010) and offers a clear model for ongoingstructured support.
Indeed, there are increasing efforts todevelop and evaluate effective training,supervision, and delivery methods for CBtwhen implemented by lay health workersusing “task shifting” or “task-sharing”models. task-shifting models have beendefined as delegating tasks to less special-ized health care workers, whereas tasksharing represents a further developmentin that it focuses on use of existing special-ists to provide ongoing support, consulta-tion, and training to less specializedproviders, instead of merely shifting addi-tional clinical responsibilities to lay healthworkers without ongoing monitoring andsupport (Padmanathan & De Silva, 2013).the models of task shifting and task shar-ing originated outside of mental healthcare in response to the hIV epidemic, par-ticularly in settings such as sub-SaharanAfrica that faced the greatest burden ofhIV/AIDS with limited resources to meetthe biomedical and behavioral needs of theepidemic (mwai et al., 2013). the high hIVburden combined with severe health care
Task Sharing Cognitive Behavioral Therapy inGlobal Mental Health: Nurse- and Lay Coun-selor–Delivered Interventions for Depressionand Substance Use in HIV Care in South AfricaJessica F. Magidson, University of Maryland, College Park
Lena S. Andersen, University of Cape Town
Alexandra L. Rose, University of Maryland, College Park
Steven A. Safren, University of Miami
April • 2019 131
workforce shortages forced the need toexpand and upskill the available workforceto appropriately address the disease-man-agement needs related to the hIV epidemic(WhO, 2008). task sharing has been a keyimplementation strategy for increasingaccess to antiretroviral therapy (ARt), thelife-saving medications now available thereto treat hIV/AIDS across sub-SaharanAfrica (trickey et al., 2017; WhO, 2013).Indeed, in the past 10 years, given the highprevalence of hIV/AIDS, various countriesin sub-Saharan Africa have dramaticallyscaled up the availability and accessibilityof ARt (Joint United Nations Programmeon hIV/AIDS, 2017).
Applying Task-Sharing Models FromHIV Care to the GMH Treatment Gap
Similar to the shortage of trained med-ical providers in sub-Saharan Africa, thereis also a shortage of trained mental healthproviders in LmICs, including many coun-tries in sub-Saharan Africa. Among theworld’s regions, countries within Africareport the largest shortages of mentalhealth providers (Bruckner et al., 2011;Scheffler et al., 2011; WhO, 2018). Whileon average LmICs have 1.6 mental healthprovider per 100,000 population, Africancountries have on average 0.9 mentalhealth providers per 100,000 population(WhO, 2018). this ratio ranges betweencountries and some, such as Sudan, have aslittle as 0.06 psychiatric specialists per100,000 population (Bruckner et al.). Com-pared to other world regions, Africa alsoreports the largest shortage of psychiatristsand psychologists within its mental healthworkforce, with the bulk of the Africanmental health workforce made up of psy-chiatric nurses and other paid mentalhealth workers (WhO, 2018). In SouthAfrica as of 2014, there were only a total of207 psychiatrists and 364 psychologists inthe employment of the entire SouthAfrican National Department of health(South African minister of health, 2014).With a current population of over 56 mil-lion, this amounts to only 0.39 psychiatristsper 100,000 and 0.7 psychologists per100,000 in the public health system. Fur-ther, national shortages for African coun-tries may even be underestimated due to alack of quality data on workforce numbersin many of the continent’s countries(Bruckner et al.; Upadhaya et al., 2016).Like in many other LmICs, the distributionof available mental health providers is clus-tered in urban areas, with little to no cover-age in rural areas, which is, in many cases,
where the majority of the population lives(Rathod et al., 2017; Vergunst, 2017;WhO, 2018). In combination with thehIV epidemic and the frequency of comor-bidities between psychiatric disorders andhIV (moore & Posada, 2013; Nedelcovychet al., 2017; thames & Jones, 2017), thereare clear needs for task sharing of mentalhealth care for individuals with hIV/AIDSin sub-Saharan Africa.
As such, researchers have suggested thatone way to meet the dire mental healthneeds in this setting is to leverage thelessons learned from task sharing in hIVcare in sub-Saharan Africa to noncommu-nicable diseases (Rabkin & el-Sadr, 2011),including behavioral health problems. evi-dence on the effectiveness of task-sharingmodels for delivering biomedical hIV careand adherence support in sub-SaharanAfrica has informed ongoing efforts to usetask-sharing models to deliver evidence-based CBt interventions for adherence,mental health, and substance use, forpeople living with hIV (PLWh) andbeyond. As the global disease burden fromnoncommunicable diseases, including psy-chiatric disorders such as depression andsubstance use disorders, continues to grow(Vos et al., 2017, 2016; WhO, 2017), it is animportant time to utilize and evaluateinnovative models such as task sharingCBt interventions that have been used toexpand access to hIV services to alsoincrease access to evidence-based mentalhealth and substance use treatment(magidson et al., 2017).
In this article, we provide examplesfrom our work task sharing CBt in hIVcare in sub-Saharan Africa. We providecase examples of implementing task shar-ing models of CBt for medication adher-ence, and integrated CBt-based interven-tions to address depression and adherence,and substance use and adherence in hIV.We discuss considerations when adaptingand implementing CBt using a task-shar-ing model in this population and discussimportant future directions and priorities,including an emphasis on implementationscience methods to promote sustainabletreatment models.
Addressing Adherence, Depression,and Substance Use in South Africa
Within sub-Saharan Africa, SouthAfrica has the largest number of peopleliving with hIV/AIDS in the world, withover 7 million PLWh and high rates ofmental health comorbidity, includingdepression and co-occurring substance use
(Southern African hIV Clinicians Society,2013; Woollett & hatcher, 2016), which areboth associated with poorer hIV treatmentoutcomes (Nakimuli-mpungu et al., 2012;Uthman, magidson, Safren, & Nachega,2014). Globally, rates of depressive symp-toms among PLWh have been shown torange from 12.8% to 78% (Uthman et al.,2014), and do not vary by country incomegroup. Among PLWh in sub-SaharanAfrica, a meta-analysis focused on depres-sion and alcohol use disorders found an18% pooled estimate rate of major depres-sion, and 31% of individuals across studieshad elevated depressive symptoms(Nakimuli-mpungu et al.). Although docu-mented less frequently than depression,rates of alcohol use disorders also reachedup to 31% (Nakimuli-mpungu et al., 2012).In South Africa specifically, a recent studyof a cohort of 1,482 PLWh presenting athealth services in South Africa founddepression rates to be approximately 33%(using the PhQ-9; Rane et al., 2018).Another recent study examining the preva-lence of alcohol use among PLWh initiat-ing ARt in sub-Saharan Africa (n = 401)found that rates of harmful alcohol usemeasured using a biomarker phos-phatidylethanol (Peth) were approxi-mately 31.6% in South Africa (magidson etal., 2018). this was consistent with rates ofself-reported harmful alcohol use in thissample (30%) and in other work examiningalcohol use among PLWh in South Africa(huis in t' Veld, Pengpid, Colebunders,Skaal, & Peltzer, 2016). When untreated,substance use and depression are associ-ated with poor antiretroviral adherenceacross multiple studies and contribute toworse hIV/AIDS treatment outcomes(Nakimuli-mpungu et al.; Uthman et al.,2014).
CBt has been used to address a range ofbehavioral health needs among individualsliving with hIV/AIDS, including toimprove hIV medication nonadherence,reduce symptoms of depression, and prob-lematic substance use (magidson et al.,2017). CBt also has empirical support forimproving adherence in combination withother evidence-based CBt interventionsfor co-occurring conditions. Prior research(Safren et al., 2001) has demonstrated thatto achieve improvements in adherencewhen co-occurring behavioral health prob-lems, such as depression symptoms, arepresent, it is important to address both thesymptoms of depression and the self-careproblems in the same intervention. thereis support for treatment approaches thatintegrate CBt for adherence and depres-
132 the Behavior Therapist
M A G I D S O N
sion in diabetes (Safren et al., 2014),hIV/AIDS (Safren et al., 2009; Safren et al.,2016), and among individuals with co-occurring depression, substance use, andhIV (Daughters et al., 2010; Safren et al.,2012). Although the majority of empiricalsupport for CBt interventions amongindividuals living with hIV/AIDS is fromthe U.S. and other developed countries,there is accumulating empirical support forCBt interventions in sub-Saharan Africa,including using task-sharing models (Abaset al., 2018; Andersen et al., 2016; Bere etal., 2017; myers et al., 2018; Nyamayaro etal., 2019; Papas et al., 2011; Papas et al.,2010). CBt’s structured, time-limitedapproach has been viewed as particularlysuitable for the demands of task sharing(i.e., to improve ease of training, supervi-sion; Papas et al., 2010).
Our team has conducted a series ofstudies aiming to task share evidence-basedCBt interventions to address the mentalhealth treatment gap in South Africa at theintersection of hIV/AIDS. We first led aseries of studies to task share CBt for hIVmedication adherence (known as Life-Steps; Case #1), followed by task-sharingintegrated CBt models to address depres-sion and ARt adherence simultaneouslyusing nurse-led delivery (“Ziphamandla”;Case #2), and a peer-delivered integratedbehavioral activation intervention foradherence and substance use (“Khanya”;Case #3). In the following section, webriefly describe the relevance of CBtmodels applied to the behavioral aspects ofhIV-related self-care and adherence andthe need to address co-occurring depres-sion and substance use, followed by adescription of our efforts to task share CBtin this setting.
Case Studies: Task Sharing CBTin the South African Context
Case Example 1: Adapting “Life-Steps”to Improve ART Adherence in SouthAfrica
the primary strategy for ARt adher-ence support in South Africa is throughindividual counseling sessions provided bylay counselors known as adherence coun-selors. historically adherence counselors,employed by nongovernmental organiza-tions, were trained in egan’s skilled helpermodel of counseling (Dewing et al., 2013).Adherence counselors would typicallyadminister three counseling sessions over a3- to 4-week period before the patient wasinitiated on ARt. Several challenges with
this approach emerged, including lack ofstructure in the counseling sessions, coun-seling content consisting mainly of advice-and information-giving (often with somedegree of moralizing), and suboptimalretention in care rates of patients prior toARt initiation (Dewing et al.).
to address these challenges andimprove ARt initiation rates, a workinggroup led by médecins Sans Frontières(mSF; “Doctors Without Borders”), whichincluded members of our team, designed arevised counseling model (Andersen,Joska, & Safren, 2013; Wilkinson et al.,2015). the revised counseling model wasdesigned to allow ARt initiation to occurwithin a week of being deemed eligible forARt. the new model proposed that thefirst adherence counseling session wouldtake place when the patient is deemed eligi-ble for ARt. the second adherence coun-seling session would take place a week laterwhen ARt is prescribed. the third coun-seling session would take place a week afterARt initiation to check in on the patient’sexperience with ARt and to problem-solveany difficulties that had arisen. Further-more, the content of the adherence coun-seling sessions needed to be replaced withan empirically supported adherence inter-vention to strengthen the adherence coun-seling program. A culturally adapted CBtintervention for ARt adherence calledLife-Steps (Safren, Otto, & Worth, 1999)was chosen to serve as the content in therevised counseling model.
Life-Steps is a structured ARt adher-ence intervention that has a strong evi-dence base in the U.S. (Safren et al., 1999)and in a number of LmICs (Abas et al.,2018; Andersen et al., 2016; Bere et al.,2017; Simoni et al., 2011). It consists of 10informational, problem-solving, and cog-nitive-behavioral steps; each step addressesa potential barrier to medication adher-ence. A structured format is employed ineach step: (a) set the goal; (b) identifypotential barriers to accomplishing thegoal; and (c) formulate a plan and back-upplan to overcome the barriers. Our teamconducted formative research and con-sulted with local health providers andstakeholders to customize Life-Steps to theSouth African context. three locally rele-vant adherence barriers were incorporatedinto Life-Steps: (a) plan for accessing ARtwhen traveling outside Cape town forextended periods; (b) plan for taking ARtwhen under the influence of substances;and (c) plan for accessing social support(Andersen et al., 2013). Additional modifi-cations included using culturally appropri-
ate examples, using comprehensible vocab-ulary, and translating the manual into isiX-hosa (Andersen et al., 2016).
mSF piloted the revised counselingmodel, including the culturally adaptedLife-Steps adherence intervention, with449 patients at a primary care clinic run bythe City of Cape town in a peri-urban area(Wilkinson et al., 2015). the revised coun-seling model produced promising out-comes. high ARt initiation rates (96%)were documented, and of those patients,the majority (n = 273; 63%) were initiatedwithin a week of being deemed eligible. Ofthose initiated, 86% were retained in careafter 6 months and 94% of those retainedobtained viral suppression. Due to the suc-cess of the pilot project, this revised coun-seling model became official Western CapeProvincial policy in 2015 and was endorsedin the national adherence guidelines (mSF,2015). this example depicts a local adapta-tion of an evidence-based CBt interven-tion to support adherence that includedplans for sustainability and scale up.
the above case example suggests thattask sharing CBt for adherence may be afeasible, sustainable solution for addressingadherence in resource-limited settings. Laycounselors’ abilities to deliver more com-plicated integrated interventions that focuson both behavioral health problems andself-care outcomes in chronic conditionsneeded to be examined next to clarify thecomplexity of interventions that lay coun-selors can deliver. these ongoing effortsneed to weigh the advantages and disad-vantages of incorporating multiple treat-ment targets into an integrated treatmentprotocol (i.e., improved efficiency yet alsoadded complexity that may hinder feasibil-ity or acceptability for training and super-vision).
Following from the research pointing todepression and substance use being two ofthe most commonly comorbid psychiatricdisorders in hIV/AIDS that also interferewith successful treatment outcomes(Nakimuli-mpungu et al., 2012; Uthman,magidson, Safren, & Nachega, 2014), ourteam has ongoing work in South Africa toevaluate task sharing models for integratedtreatments to address depression and sub-stance use (currently in separate protocols)and also improve hIV treatment adher-ence. In this next section, we provideexamples of our ongoing work task sharingevidence-based, integrated CBt interven-tions to address comorbid psychiatric dis-orders and improve ARt adherenceamong individuals living with hIV/AIDSin sub-Saharan Africa. Following these
April • 2019 133
T A S K S H A R I N G C B T I N G L O B A L M E N T A L H E A L T H
examples, we discuss considerations forfuture efforts when adapting and imple-menting CBt using a task sharing model inthis population.
Case Example 2: Ziphamandla—Integrated CBT Intervention forDepression and HIV MedicationAdherence
there are ongoing efforts to integrateCBt for depression with an evidence-based CBt intervention for adherence(Life-Steps; Safren, Gonzalez, & Soroudi,2008; Safren et al., 1999). Andersen et al.(2012) evaluated a task-shared CBt treat-ment for depression and hIV medicationadherence in South Africa. the nurse-delivered treatment was a 6- to 8-sessionintervention based on CBt for adherenceand depression (CBt-AD; Safren et al.,2012, 2009). Primary modifications to theoriginal treatment included cultural adap-tations and the removal of the cognitiverestructuring module due to its complexity.treatment modules included psychoedu-cation, motivational interviewing, problemsolving, behavioral activation, relaxationtraining, and Life-Steps. Initial evidencesuggests the adapted, task-shared treat-ment was acceptable to participants(everitt-Penhale et al., 2019) and associ-ated with significant improvements indepression, functioning, and modestimprovements in hIV medication adher-ence (Andersen et al., 2016). Yet, imple-mentation was challenging, requiringextensive weekly supervision, initial train-ing (88 hours), supplemented with regularongoing training (Andersen et al.).
to further examine the efficacy of thetreatment, a randomized controlled effec-tiveness trial of this treatment withdepressed ARt-users with unsuppressedviral loads is currently under way (clinical-trials.gov identifier: NCt02696824). Asbefore, nurses are the interventionists,trained in the assessment of depression aswell as the delivery of the manualized CBt-AD intervention and supervised weekly bya clinical psychologist with CBt expertisewho is based in South Africa (LA). Addi-tionally, we moved from a written manualto a “flip-chart” style manual that the nurseinterventionists bring with them to the ses-sions and go through with the participant.this is designed to enhance fidelity to thetreatment and delivery of the interventioncomponents, as we have found that in thiscontext, there is a need for balancing theperceived need for providing supportivecounseling with present-focused skills-based treatment that directly addresses
self-care and depression. the study willhelp determine whether this nurse-deliv-ered CBt treatment is associated withlong-term improvements in key health andpsychological outcomes, and is feasible andsustainable for delivery in this setting.
Case Example 3: Task Sharing an Inte-grated Intervention for Substance Useand HIV Medication Adherence inSouth Africa: Project Khanya
to improve health outcomes alongsideefforts to reduce alcohol use among hIV-infected patients, efforts are under way inSouth Africa to evaluate a primary healthclinic–delivered behavioral activation–based intervention for both substance useand hIV medication adherence. A qualita-tive formative stage on barriers, facilitators,and preferences for substance use treat-ment within hIV care with clinic patientsstruggling with both substance use andhIV medication adherence and variedclinic providers produced key feedback forintervention adaptation. this includedfeedback from patients that they wouldprefer delivery of substance use treatmentby peer interventionists, in part due toexperiences of stigma of substance use(magidson et al., in press). Providers alsorecommended leveraging existing commu-nity health worker cadres conductinghousehold assessments to engage sub-stance using PLWh who had fallen out ofcare, an approach that will be tested infuture work. the adapted intervention cur-rently being evaluated, locally named“Khanya,” is being delivered by a peerinterventionist in the health clinic wherepatients access hIV treatment.
the Khanya intervention includes Life-Steps, behavioral activation adapted forsubstance use in this setting, and relapseprevention skills (behavioral and mindful-ness-based skills adapted for this setting).the intervention is delivered over six ses-sions, with the option for an additional sixmonthly booster sessions to allow patientstime for additional support and practice ofskills. Like in Ziphamandla, the interven-tionist also has a flip-chart style manual foruse in sessions. the flip-chart outlines keycomponents in each session, while alsoincluding some prompts for the interven-tionist to share her own personal exampleswhen relevant, for instance, in how she hasapplied skills in her own life, which is dis-cussed regularly in supervision. Supervi-sion is provided via videoconferencing by aU.S.-based licensed clinical psychologistwith substantial experience working inSouth Africa (Jm), supplemented by in-
person visits approximately three times peryear, both to ensure fit of supervision to thelocal context. A randomized, hybrid type1 effectiveness-implementation trial of theKhanya intervention compared toenhanced treatment as usual with patientswith hIV who are struggling with bothadherence and substance use is currentlyunder way (clinicaltrials.gov identifier:NCt03529409). this trial will help deter-mine whether this peer-delivered CBtintervention is feasible and acceptable fordelivery in this setting, and associated withimprovements in hIV medication adher-ence (measured using real-time electronicadherence monitoring, self-report, andbiomarkers), and improvements in sub-stance use (also measured using self-reportand biomarkers).
Summary: Considerations forTask Sharing CBT in
Resource-Limited Settingsthese case examples of task sharing
CBt for behavioral health needs amonghIV-infected individuals in sub-SaharanAfrica present a promising approach fornot only improving adherence but also co-occurring psychiatric disorders. In somecases, lay counselor or peer delivery, asillustrated in formative qualitative work inSouth Africa to develop alcohol/adherenceinterventions (magidson et al., in press.;morojele et al., 2014), may even be prefer-able, which can be understood in the con-text of other leading peer-led addictionprograms globally, such as AlcoholicsAnonymous. Across our case examples andother studies adapting CBt techniques forresource-limited settings, often key consid-erations in the adaptation are culturalmodification and adaptation for lay coun-selor delivery, while also maintaining thecore components of the intervention(Chibanda, Cowan, healy, Abas, & Lund,2015; ekers, Richards, mcmillan, Bland, &Gilbody, 2011; magidson et al., 2015;murray et al., 2013; Patel, Chowdhary,Rahman, & Verdeli, 2011; Patel et al., 2017;Purgato et al., 2018; Richards et al., 2016).Given that many CBt approaches aretested and developed using highly trainedacademic therapists in high-income coun-tries, adaptations to training and supervi-sion methods are essential. Often thesemodifications include (a) focusing on howtraining is conducted; (b) simplifyingterms and avoiding clinical jargon; and (c)adapting the structure of supervision.Regarding cultural adaptations, changesmay include ensuring appropriate delivery
134 the Behavior Therapist
M A G I D S O N
within a local context, linguistic modifica-tions, and including local idioms,metaphors, and stories, as well as adaptingfor low-literacy populations.
CBt has been considered a good candi-date for lay counselor delivery, given itsstructured format. Although easier fortraining purposes, the structured formatmay be challenging in learning how tomaintain a primary focus on the key inter-vention target (e.g., adherence), particu-larly when patients may also requestaddressing other health behaviors in thecontext of the intervention or other urgentpsychosocial stressors (morojele et al.,2014). Further, it is necessary to under-stand how to adapt CBt interventions toalso incorporate the unique identities ofpeers and ChWs while maintainingfidelity. As mentioned above, our team hasutilized a flipchart manual to promotefidelity (with some prompts to shareaspects about oneself and allow for flexibil-ity of delivery, e.g., in Case #3). technologycan also be useful to promote fidelity forCBt delivery in task-sharing models, forinstance by providing multimedia plat-forms to increase fidelity to interventiondelivery (Remien et al., 2013; Robbins et al.,2015). Additional research is needed todemonstrate how multimedia-based plat-forms may be a potentially sustainablestrategy when sharing models of CBt. Yet,alongside these efforts to promote fidelity,it also is important to note that the moreflexible the delivery of an intervention, thegreater the likelihood for ultimate adoptionin clinical settings (Damschroder et al.,2009; Glasgow, Vogt, & Boles, 1999;thorpe et al., 2009). As such, finding a bal-ance between providing structure andallowing for some flexibility in delivery—for instance, using a modular approach(Safren et al., 2012, 2009)—is necessary.
Alongside the promising results ofeffectiveness trials of CBt using task-shar-ing models, clear implementation chal-lenges emerge from these examples of tasksharing CBt in this setting. Primary imple-mentation challenges identified in previouswork (Petersen, Fairall, egbe, & Bhana,2014) include poor role definition or clarityon scope of work for lay counselors, lack ofstandardized training, and inadequatesupervision, support, and compensation.For long-term sustainability, a primaryconsideration is whether interventionsdelivered as part of research studies wouldbe feasible if conducted in a clinic-basedsetting without any additional researchresources. For instance, the amount oftraining and supervision described in each
of the examples may likely not be sustain-able in a real-world clinical setting. Fur-ther, it also is essential to always considerhow we can promote capacity building forthe trainers and supervisors as to not relysolely on outside experts to promote long-term sustainability. When we reach a laterstage of implementation outside the con-text of a research study, ongoing evaluationis needed as to when clinic-based coun-selors, as opposed to lay counselors hiredfor research purposes, are feasibly andcompetently able to deliver the CBt inter-vention. efforts in South Africa are ongo-ing to understand the barriers and facilita-tors to using designated vs. dedicatedclinic-based staff (myers et al., 2018).
Another important consideration whenexamining efforts to implement CBt inclinical settings outside of a research con-text will be how to standardize selection oflay counselors. Preliminary work has beendone to develop metrics of lay counselorcompetence in implementing task-sharedpsychological interventions (Kohrt et al.,2015; Singla et al., 2014), but more work isneeded to guide the selection of lay coun-selors for these roles. If task sharing CBtfor behavioral health problems proves to befeasible and effective in the ongoing work,it may be a particularly appealing approachfor expanding access to evidence-basedmental health care and CBt interventionsat scale globally.
In summary, numerous lessons can belearned from responses to meeting thebehavioral treatment needs in the hIV epi-demic in sub-Saharan Africa that caninform efforts to expand access to evi-dence-based care for mental health amongPLWh and beyond. Addressing ARtadherence concerns and the co-occurringpsychiatric disorders which disrupt ARtadherence are key to the success of bio-medical treatment as prevention efforts tocurbing the hIV/AIDS epidemic in sub-Saharan Africa. Given the ways in whichpsychiatric disorders such as depressionand substance use interfere with hIV self-care, task sharing of biomedical ARt pro-grams may only succeed in the context ofalso task sharing evidence-based interven-tions to promote ARt adherence and viralsuppression. this work offers importantlessons for expanding access to evidence-based mental health care globally usingtask sharing of evidence-based CBt inter-ventions.
there are many pressing implementa-tion science priorities in global mentalhealth that are specific to task sharing CBt.more research is needed regarding what
types of training and supervision methodsare most efficient and effective (Dorsey etal., 2018; Lucid et al., 2018; Pullmann et al.,2018), and what types of CBt interventionsare most suitable for lay counselor delivery.these decisions will likely need to considerthe advantages and disadvantages of incor-porating multiple treatment targets in aunified treatment protocol—for instance,following the innovative, important workexamining task sharing an adapted unifiedprotocol intervention in LmICs (Bolton etal., 2014; Bonilla-escobar et al., 2018;Dorsey, Berliner, Lyon, Pullmann, &murray, 2016; murray et al., 2014). Prelim-inary work suggests that task sharing CBtinterventions may be a promising solutionfor increasing access to evidence-basedmental health care worldwide.
ReferencesAbas, m. Nyamayaro, P., Bere, t.,
Saruchera, e., mothobi, N., Simms, V., …O’Cleirigh, C. (2018). Feasibility andacceptability of a task-shifted interventionto enhance adherence to hIV medicationand improve depression in people livingwith hIV in Zimbabwe, a low-incomecountry in Sub-Saharan Africa. AIDS andBehavior, 22(1), 86–101.https://doi.org/10.1007/s10461-016-1659-4
Andersen L.S, Joska, J., & Safren S.A.(2013). Life Steps for ART Adherence:Manual for adherence counsellors, patientsand HIV health care workers. GSh-hIVmental health Group.
Andersen, L.S., Joska, J., O’Cleirigh, C., &Safren, S. A. (2012). Adapting cognitive-behavioral therapy for adherence anddepression in HIV to the South Africancontext. Presentation at IAPAC, Interna-tional Conference on hIV treatment andPrevention Adherence. miami, FL.
Andersen, L.S., magidson, J. F., O’Cleirigh,C., Remmert, J. e., Kagee, A., Leaver, m.,… Joska, J. (2016). A pilot study of anurse-delivered cognitive behavioral ther-apy intervention (Ziphamandla) foradherence and depression in hIV inSouth Africa. Journal of Health Psychol-ogy, 1359105316643375. https://doi.org/10.1177/1359105316643375
Bere, t., Nyamayaro, P., magidson, J. F.,Chibanda, D., Chingono, A., munjoma,R., & Abas, m. (2017). Cultural adaptationof a cognitive-behavioural intervention toimprove adherence to antiretroviral ther-apy among people living with hIV/AIDSin Zimbabwe: Nzira Itsva. Journal ofHealth Psychology, 22(10), 1265–1276.
Bolton, P., Lee, C., haroz, e. e., murray, L.,Dorsey, S., Robinson, C., … Bass, J.(2014). A transdiagnostic community-based mental health treatment for comor-
April • 2019 135
T A S K S H A R I N G C B T I N G L O B A L M E N T A L H E A L T H
bid disorders: development and outcomesof a randomized controlled trial amongBurmese refugees in thailand. PLoS Med-icine, 11(11), e1001757–e1001757.https://doi.org/10.1371/journal.pmed.1001757
Bonilla-escobar, F. J., Fandiño-Losada, A.,martínez-Buitrago, D. m., Santaella-tenorio, J., tobón-García, D., muñoz-morales, e. J., … Bolton, P. (2018). A ran-domized controlled trial of atransdiagnostic cognitive-behavioralintervention for Afro-descendants’ sur-vivors of systemic violence in Colombia.PloS One, 13(12), e0208483–e0208483.https://doi.org/10.1371/journal.pone.0208483
Bruckner, t. A., Scheffler, R. m., Shen, G.,Yoon, J., Chisholm, D., morris, J., …Saxena, S. (2011). the mental healthworkforce gap in low- and middle-incomecountries: a needs-based approach. Bul-letin of the World Health Organization, 89,184–194.https://doi.org/10.2471/BLt.10.082784
Chibanda, D., Cowan, F. m., healy, J. L.,Abas, m., & Lund, C. (2015). Psychologi-cal interventions for common mental dis-orders for people living with hIV in low-and middle-income countries: Systematicreview. Tropical Medicine & InternationalHealth, 20(7), 830–839.https://doi.org/10.1111/tmi.12500
Damschroder, L. J., Aron, D. C., Keith, R.e., Kirsh, S. R., Alexander, J. A., & Lowery,J. C. (2009). Fostering implementation ofhealth services research findings intopractice: a consolidated framework foradvancing implementation science. Imple-mentation Science, 4, 50.https://doi.org/10.1186/1748-5908-4-50
Daughters, S. B., magidson, J. F., Schuster,R. m., & Safren, S. A. (2010). ACtheALthY: A combined cognitive-behavioral depression and medicationadherence treatment for hIV-infectedsubstance users. Cognitive and BehavioralPractice, 17(3), 309–321.
DeSilva, m., Samele, C., Saxena, S., Patel, V.,& Darzi, A. (2014). Policy actions toachieve integrated community-basedmental health services. Health Affairs,33(9), 1595–1602.
Dewing, S., mathews, C., Schaay, N., Cloete,A., Louw, J., & Simbayi, L. (2013). “It’sImportant to take Your medicationeveryday Okay?” An evaluation of coun-selling by lay counsellors for ARV adher-ence support in the Western Cape, SouthAfrica. AIDS & Behavior, 17(1), 203–212.
Dorsey, S., Berliner, L., Lyon, A. R., Pull-mann, m. D., & murray, L. K. (2016). Astatewide common elements initiative forchildren’s mental health. Journal of Behav-ioral Health Services & Research, 43(2),
Dorsey, S., Kerns, S. e. U., Lucid, L., Pull-mann, m. D., harrison, J. P., Berliner, L.,… Deblinger, e. (2018). Objective codingof content and techniques in workplace-based supervision of an eBt in publicmental health. Implementation Science,13(1), 19–19. https://doi.org/10.1186/s13012-017-0708-3
ekers, D., Richards, D., mcmillan, D.,Bland, J. m., & Gilbody, S. (2011). Behav-ioural activation delivered by the non-spe-cialist: phase II randomised controlledtrial. British Journal of Psychiatry, 198(1),66–72. https://doi.org/10.1192/bjp.bp.110.079111
everitt-Penhale, B., Kagee, A., magidson, J.F., Joska, J., Safren, S. A., O’Cleirigh, C., …Anderson, L. S. (2019). ‘I went back tobeing myself’: Acceptability of a culturallyadapted task-shifted cognitive-behav-ioural therapy (CBt) treatment fordepression (Ziphamandla) for SouthAfrican hIV care settings. Psychology,Health, and Medicine. https://doi.org/10.1080/13548506.2019.1566624
Glasgow, R. e., Vogt, t. m., & Boles, S. m.(1999). evaluating the public healthimpact of health promotion interventions:the Re-AIm framework. American Jour-nal of Public Health, 89(9), 1322–1327.
huis in t’ Veld, D., Pengpid, S., Colebun-ders, R., Skaal, L., & Peltzer, K. (2016).high-risk alcohol use and associatedsocio-demographic, health and psychoso-cial factors in patients with hIV infectionin three primary health care clinics inSouth Africa. International Journal of STD& AIDS, 28(7), 651–659. https://doi.org/10.1177/0956462416660016
Joint United Nations Programme onhIV/AIDS. (2017). UNAIDS Data 2017.Joint United Nations Programme onhIV/AIDS. Retrieved fromhttp://www.unaids.org/sites/default/files/media_asset/20170720_Data_book_2017_en.pdf
Kakuma, R., minas, h., van Ginneken, N.,Dal Poz, m. R., Desiraju, K., morris, J. e.,… Scheffler, R. m. (2011). humanresources for mental health care: currentsituation and strategies for action. TheLancet, 378(9803), 1654–1663.https://doi.org/10.1016/S0140-6736(11)61093-3
Kohrt, B. A., Jordans, m. J. D., Rai, S.,Shrestha, P., Luitel, N. P., Ramaiya, m. K.,… Patel, V. (2015). therapist competencein global mental health: Development ofthe enhancing assessment of commontherapeutic factors (eNACt) rating scale.Behaviour Research and Therapy, 69, 11–21. doi: 10.1016/j.brat.2015.03.009
Lucid, L., meza, R., Pullmann, m. D., Jung-bluth, N., Deblinger, e., & Dorsey, S.
(2018). Supervision in community mentalhealth: understanding intensity of eBtfocus. Intersection of Implementation Sci-ence and Behavioral Health, 49(4), 481–493. https://doi.org/10.1016/j.beth.2017.12.007
Lund, C., Caldas de Almeida, J. m., White-ford, h., & mahoney, J. (2013). Policydevelopment and implementation. In V.Patel, h. minas, A. Cohen, & m. Prince(eds.), Global Mental Health: Principlesand Practice. New York, NY: Oxford Uni-versity Press.
magidson, J.F., Fatch, R., Orrell, C.,Amanyire, G., haberer, J.A., hahn, J.A.,the metA team. (2018). Biomarker-mea-sured unhealthy alcohol use in relation toCD4 count among individuals startingARt in sub-saharan Africa. AIDS andBehavior. https://doi.org/10.1007/s10461-018-2364-2.
magidson, J.F., Gouse, h., Psaros, C., Rem-mert, J. e., O’Cleirigh, C., & Safren, S. A.(2017). task shifting and delivery ofbehavioral medicine interventions inresource-poor global settings: hIV/AIDStreatment in sub-Saharan Africa. In A. m.Vranceanu, J. A. Greer, & S. A. Safren(eds.), The Massachusetts General Hospi-tal Handbook of Behavioral Medicine.New York, NY: humana Press.
magidson, J.F., Joska, J., Regenauer, K. S.,Satinsky, e., Andersen, L. S., Seitz-Brown,C. J., … myers, B. (in press). “Someonewho is in this thing that I am sufferingfrom”: the role of peers and other facilita-tors for task sharing substance use treat-ment in South African HIV Care.
magidson, J.F., Lejuez, C. W., Kamal, t.,Blevins, e. J., murray, L. K., Bass, J. K., …Pagoto, S. (2015). Adaptation of commu-nity health worker-delivered behavioralactivation for torture survivors in Kurdis-tan, Iraq. Global Mental Health (Cam-bridge, england), 2, e24. https://doi.org/10.1017/gmh.2015.22
médecins Sans Frontières (Doctors With-out Borders). (2015). ART/TB/PMTCTinitiation patient education and coun-selling model: Report and toolkit (pp. 1–21). Khayelitsha, South Africa.
monson, C. m., Shields, N., Suvak, m. K.,Lane, J. e. m., Shnaider, P., Landy, m. S.h., … Stirman, S. W. (2018). A random-ized controlled effectiveness trial of train-ing strategies in cognitive processing ther-apy for posttraumatic stress disorder:Impact on patient outcomes. BehaviourResearch and Therapy, 110, 31–40.https://doi.org/10.1016/j.brat.2018.08.007
moore, D. J., & Posada, C. (2013). hIV andpsychiatric comorbidities: What do weknow and what can we do? (Psychologyand AIDS exchange Newsletter). Ameri-can Psychological Association. Retrievedfrom https://www.apa.org/pi/
morojele, N. K., Kitleli, N., Ngako, K., Kek-waletswe, C. t., Nkosi, S., Fritz, K., &Parry, C. D. h. (2014). Feasibility andacceptability of a bar-based sexual riskreduction intervention for bar patrons intshwane, South Africa. SAHARA J: Jour-nal of Social Aspects of HIV/AIDSResearch Alliance / SAHARA, Human Sci-ences Research Council, 11(1), 1–9.https://doi.org/10.1080/17290376.2014.890123
murray, L.K., Dorsey, S., haroz, e., Lee, C.,Alsiary, m. m., haydary, A., … Bolton, P.(2014). A common elements treatmentapproach for adult mental health prob-lems in low- and middle-income coun-tries. Cognitive and Behavioral Practice,21(2), 111–123. https://doi.org/10.1016/j.cbpra.2013.06.005
murray, L.K., Dorsey, S., Skavenski, S.,Kasoma, m., Imasiku, m., Bolton, P., …Cohen, J. A. (2013). Identification, modifi-cation, and implementation of an evi-dence-based psychotherapy for childrenin a low-income country: the use of tF-CBt in Zambia. International Journal ofMental Health Systems, 7(1), 24–24.https://doi.org/10.1186/1752-4458-7-24
mwai, G. W., mburu, G., torpey, K., Frost,P., Ford, N., & Seeley, J. (2013). Role andoutcomes of community health workersin hIV care in sub-Saharan Africa: A sys-tematic review. Journal of the Interna-tional AIDS Society, 16(1), 18586–18586.https://doi.org/10.7448/IAS.16.1.18586
myers, B., Joska, J., Lund, C., Levitt, N.,Butler, C., Naledi, t., … Sorsdahl, K.(2018). Patient preferences for the integra-tion of mental health counseling andchronic disease care in South Africa.Patient Preference and Adherence, 12,1797–1803. https://doi.org/10.2147/PPA.S176356
myers, B., Lund, C., Lombard, C., Joska, J.,Levitt, N., Butler, C., Cleary, S., Naledi, t.,milligan, P., Stein, D. J., … Sorsdahl, K.(2018). Comparing dedicated and desig-nated models of integrating mental healthinto chronic disease care: study protocolfor a cluster randomized controlled trial.Trials, 19(1), 185. doi:10.1186/s13063-018-2568-9
Nakimuli-mpungu, e., Bass, J. K., Alexan-dre, P., mills, e. J., musisi, S., Ram, m., &Nachega, J. B. (2012). Depression, alcoholuse and adherence to antiretroviral ther-apy in sub-saharan Africa: A systematicreview. AIDS and Behavior, 16(8), 2101–2118.
Nedelcovych, m. t., manning, A. A.,Semenova, S., Gamaldo, C., haughey, N.J., & Slusher, B. S. (2017). the psychiatricimpact of hIV. ACS Chemical Neuro-
Nyamayaro, P., Bere, t., magidson, J. F.,Simms, V., O’Cleirigh, C., Chibanda, D.,& Abas, m. (2019). A task-shifting prob-lem-solving therapy intervention fordepression and barriers to antiretroviraltherapy adherence for people living withhIV in Zimbabwe: Case series. Cognitiveand Behavioral Practice. https://doi.org/10.1016/j.cbpra.2018.10.003
Padmanathan, P & De Silva, m.J. (2013).the acceptability and feasibility of task-sharing for mental healthcare in low- andmiddle-income countries: A systematicreview. Social Science and Medicine, 97,82-86.
Papas, R.K., Sidle, J. e., Gakinya, B. N.,Baliddawa, J. B., martino, S., mwaniki, m.m., … maisto, S. A. (2011). treatmentoutcomes of a stage 1 cognitive-behavioraltrial to reduce alcohol use among humanimmunodeficiency virus-infected out-patients in western Kenya: RCt alcoholoutcomes in Kenya. Addiction, 106(12),2156–2166. https://doi.org/10.1111/j.1360-0443.2011.03518.x
Papas, R.K., Sidle, J. e., martino, S., Balid-dawa, J. B., Songole, R., Omolo, O. e., …Nafula, t. (2010). Systematic culturaladaptation of cognitive-behavioral ther-apy to reduce alcohol use among hIV-infected outpatients in western Kenya.AIDS and Behavior, 14(3), 669–678. doi:10.1007/s10461-009-9647-6
Patel, V., Weobong, B., Weiss, h. A.,Anand, A., Bhat, B., Katti, B., … Fairburn,C. G. (2017). the healthy Activity Pro-gram (hAP), a lay counsellor-deliveredbrief psychological treatment for severedepression, in primary care in India: Arandomised controlled trial. The Lancet,389(10065), 176–185. https://doi.org/10.1016/S0140-6736(16)31589-6
Petersen, I., Fairall, L., egbe, C. O., &Bhana, A. (2014). Optimizing lay counsel-lor services for chronic care in SouthAfrica: A qualitative systematic review.Patient Education and Counseling, 95(2),201–210.https://doi.org/10.1016/j.pec.2014.02.001
Pullmann, m. D., Lucid, L., harrison, J. P.,martin, P., Deblinger, e., Benjamin, K. S.,& Dorsey, S. (2018). Implementation cli-mate and time predict intensity of super-vision content related to evidence-basedtreatment. Frontiers in Public Health, 6,280–280. https://doi.org/10.3389/fpubh.2018.00280
Purgato, m., Gastaldon, C., Papola, D., vanOmmeren, m., Barbui, C., & tol, W.(2018). Psychological therapies for thetreatment of mental disorders in low‐ andmiddle‐income countries affected byhumanitarian crises. Cochrane Databaseof Systematic Reviews, (7).https://doi.org/10.1002/14651858.CD011849.pub2
Rabkin, m., & el-Sadr, W.m. (2011) Whyreinvent the wheel? Leveraging the lessonsof hIV scale-up to confront non-commu-nicable diseases. Global Public Health,6(3), 247 256, https://doi.org/10.1080/17441692.2011.552068
Rane, m.S., hong, t., Govere, S., thulare,h., moosa, m-Y., Celum, C., & Drain,P.K. (2018). Depression and anxiety asrisk factors for delayed care-seekingbehavior in human immunodeficiencyvirus–infected individuals in South Africa.Clinical Infectious Diseases, 67(9), 1411–1418, https://doi.org/10.1093/cid/ciy309
Rathod, S., Pinninti, N., Irfan, m., Gorczyn-ski, P., Rathod, P., Gega, L., & Naeem, F.(2017). mental health service provision inlow- and middle-income countries.Health Services Insights, 10. doi:10.1177/1178632917694350
Remien, R. h., mellins, C. A., Robbins, R.N., Kelsey, R., Rowe, J., Warne, P., …Abrams, e. J. (2013). masivukeni: devel-opment of a multimedia based antiretro-viral therapy adherence intervention forcounselors and patients in South Africa.AIDS and Behavior, 17(6), 1979–1991.doi: 10.1007/s10461-013-0438-8
Richards, D. A., ekers, D., mcmillan, D.,taylor, R. S., Byford, S., Warren, F. C., …Finning, K. (2016). Cost and outcome ofbehavioural activation versus cognitivebehavioural therapy for depression(COBRA): a randomised, controlled, non-inferiority trial. The Lancet, 388(10047),871–880. https://doi.org/10.1016/S0140-6736(16)31140-0
Robbins, R. N., mellins, C. A., Leu, C.-S.,Rowe, J., Warne, P., Abrams, e. J., &Remien, R. h. (2015). enhancing laycounselor capacity to improve patient out-comes with multimedia technology. AIDSand Behavior, 19(2), 163–176.
Safren, S.A., Gonzalez, J., & Soroudi, N.(2008). Coping with Chronic Illness: ACognitive-Behavioral Therapy Approachfor Adherence and Depression. TherapistGuide. New York, NY: Oxford UniversityPress.
Safren, S.A., O’Cleirigh, C. m., Bullis, J. R.,Otto, m. W., Stein, m. D., & Pollack, m.h. (2012). Cognitive behavioral therapyfor adherence and depression (CBt-AD)in hIV-infected injection drug users: arandomized controlled trial. Journal ofConsulting and Clinical Psychology, 80(3),
April • 2019 137
T A S K S H A R I N G C B T I N G L O B A L M E N T A L H E A L T H
404–415. https://doi.org/10.1037/a0028208
Safren, S.A., O’Cleirigh, C., tan, J. Y., Ram-inani, S. R., Reilly, L. C., Otto, m. W., &mayer, K. h. (2009). A randomized con-trolled trial of cognitive behavioral ther-apy for adherence and depression (CBt-AD) in hIV-infected individuals. healthPsychology: Official Journal of the Divi-sion of Health Psychology, American Psy-chological Association, 28(1), 1–10.https://doi.org/10.1037/a0012715
Safren, S.A, Bedoya, C. A., O’Cleirigh, C.,Biello, K. B., Pinkston, m. m., Stein, m. D.,… mayer, K. h. (2016). Cognitive behav-ioural therapy for adherence and depres-sion in patients with hIV: A three-armrandomised controlled trial. The Lancet.HIV, 3(11), e529–e538. https://doi.org/10.1016/S2352-3018(16)30053-4
Safren, S.A., Gonzalez, J. S., Wexler, D. J.,Psaros, C., Delahanty, L. m., Blashill, A. J.,… Cagliero, e. (2014). A randomized con-trolled trial of cognitive behavioral ther-apy for adherence and depression (CBt-AD) in patients with uncontrolled type 2diabetes. Diabetes Care, 37(3), 625–633.https://doi.org/10.2337/dc13-0816
Safren, S.A, Otto, m. W., & Worth, J. L.(1999). Life-Steps: Applying cognitive-behavioral therapy to patient adherence inhIV medication treatment. CognitiveBehavioral Practice, 6, 332–341.
Safren, S.A, W. Otto, m., Worth, J. L.,Salomon, e., Johnson, W., mayer, K., &Boswell, S. (2001). two strategies toincrease adherence to hIV antiretroviralmedication: Life-Steps and medicationmonitoring. Behaviour Research andTherapy, 39(10), 1151–1162.https://doi.org/10.1016/S0005-7967(00)00091-7
Scheffler, R. m., Bruckner, t. A., Fulton, B.D., Yoon, J., Shen, G., Chisholm, D., …Saxena, S. (2011). human resources formental health: Workforce shortages inlow- and middle-income countries.Human Resources for Health Observer, 8.Geneva, Switzerland: World health Orga-nization. Retrieved from http://apps.who.int/iris/bitstream/handle/10665/44508/9789241501019_eng.pdf;jsessionid=00A59F318e13Fe123247021D35eAFC69?sequence=1
Simoni, J. m., Chen, W.-t., huh, D.,Fredriksen-Goldsen, K. I., Pearson, C.,Zhao, h., … Zhang, F. (2011). A prelimi-nary randomized controlled trial of anurse-delivered medication adherenceintervention among hIV-positive outpa-tients initiating antiretroviral therapy inBeijing, China. AIDS and Behavior, 15(5),919–929. https://doi.org/10.1007/s10461-010-9828-3
Singla, D. R., Weobong, B., Nadkarni, A.,Chowdhary, N., Shinde, S., Anand, A., …
Patel, V. (2014). Improving the scalabilityof psychological treatments in developingcountries: an evaluation of peer-led ther-apy quality assessment in Goa, India.Behaviour Research and Therapy, 60(100),53–59. https://doi.org/10.1016/j.brat.2014.06.006
Smith, S. L., Kayiteshona, Y., misago, C.,Iyamuremye, J. D., Dusabeyezu, J. D.,mohand, A. A., … Raviola, G. J. (2017).Integrating mental health care into pri-mary care: the case of one rural district inRwanda. Intervention, 15(2), 136–150.https://doi.org/10.1097/WtF.0000000000000148
South African minister of health. (2014).Reference in response to question in par-liament.
Southern African hIV Clinicians Society.(2013). management of mental health dis-orders in hIV-positive patients. SouthernAfrican Journal of HIV Medicine, 4(4).Retrieved from https://sajhivmed.org.za/index.php/hivmed/article/view/50/70
thames, A. D., & Jones, J. D. (2017). Psy-chiatric comorbidities in hIV infection. InP. Shapshak (ed.), Global Virology II -HIV and NeuroAIDS. New York, NY:Springer.
thorpe, K. e., Zwarenstein, m., Oxman, A.D., treweek, S., Furberg, C. D., Altman,D. G., … Chalkidou, K. (2009). A prag-matic–explanatory continuum indicatorsummary (PReCIS): a tool to help trialdesigners. Canadian Medical AssociationJournal, 180(10), e47–e57.https://doi.org/10.1503/cmaj.090523
trickey, A., may, m. t., Vehreschild, J.-J.,Obel, N., Gill, m. J., Crane, h. m., …Sterne, J. A. C. (2017). Survival of hIV-positive patients starting antiretroviraltherapy between 1996 and 2013: A collab-orative analysis of cohort studies. TheLancet HIV, 4(8), e349–e356. https://doi.org/10.1016/S2352-3018(17)30066-8
Upadhaya, N., Jordans, m. J. D., Abdulma-lik, J., Ahuja, S., Alem, A., hanlon, C., …Gureje, O. (2016). Information systemsfor mental health in six low- and middle-income countries: cross country situationanalysis. International Journal of MentalHealth Systems, 10(60).
Uthman, O. A., magidson, J. F., Safren, S.A., & Nachega, J. B. (2014). Depressionand adherence to antiretroviral therapy inlow-, middle- and high-income countries:A systematic review and meta-analysis.Current HIV/AIDS Reports, 11(3), 291–307. https://doi.org/10.1007/s11904-014-0220-1
Vergunst, R. (2017). From global-to-local:rural mental health in South Africa.Global Health Action, 11(1). doi:10.1080/16549716.2017.1413916
Vos, t., Abajobir, A. A., Abate, K. h.,Abbafati, C., Abbas, K. m., Abd-Allah, F.,
… murray, C. J. L. (2017). Global,regional, and national incidence, preva-lence, and years lived with disability for328 diseases and injuries for 195 coun-tries, 1990–2016: A systematic analysis forthe Global Burden of Disease Study 2016.The Lancet, 390(10100), 1211–1259.https://doi.org/10.1016/S0140-6736(17)32154-2
Vos, t., Allen, C., Arora, m., Barber, R. m.,Bhutta, Z. A., Brown, A., … murray, C. J.L. (2016). Global, regional, and nationalincidence, prevalence, and years lived withdisability for 310 diseases and injuries,1990–2015: A systematic analysis for theGlobal Burden of Disease Study 2015. TheLancet, 388(10053), 1545–1602.https://doi.org/10.1016/S0140-6736(16)31678-6
Wilkinson, L., Duvivier, h., Patten, G.,Solomon, S., mdani, L., Patel, S.,…Baert,S. (2015). Outcomes from the implemen-tation of a counselling model supportingrapid antiretroviral treatment initiation ina primary healthcare clinic in Khayelitsha,South Africa. Southern African Journal ofHIV Medicine, 16(1), 1–7.
Woollett, N., & hatcher, A. m. (2016).mental health, intimate partner violenceand hIV. South African Medical Journal,106, 969–972.
World health Organization. (2008). Taskshifting: Rational redistribution of tasksamong health workforce teams: Global rec-ommendations and guidelines. Geneva,Switzerland: Author.
World health Organization. (2013). Con-solidated Guidelines on the Use of Anti-retroviral Drugs for Treating and Prevent-ing HIV Infection: Recommendations for aPublic Health Approach. Geneva, Switzer-land: Author.
World health Organization. (2017).Depression and Other Common MentalDisorders: Global Health Estimates.Geneva, Switzerland: Author. Retrievedfrom http://apps.who.int/iris/bitstream/handle/10665/254610/WhO-mSD-meR-2017.2-eng.pdf
World health Organization. (2018). MentalHealth Atlas 2017. Geneva, Switzerland:Author.
. . .
Dr. Steven Safren receives royalties fromOxford University Press for treatment man-uals in cognitive behavioral therapy. Noother authors have funding or conflicts ofinterest to disclose.Correspondence to Jessica F. magidson,Ph.D., 1147B Biology-Psychology, Univer-sity of maryland, College Park, mD, 20742;[email protected]
New Professional 3Katherine CunninghamBridget DavidsonRuth ellingsenmeredith GinleyJennifer marceronmia RomanoJeremy SalzmanJulianna SapienzaAliza ShapiroSarah tannenbaumGina VueAlia Warner
This award recognizes outstanding individuals who have shown exceptional dedication, influence, and social impactthrough the promotion of evidence-based interventions and who have thereby advanced the mission of ABCT.Champions may not be members of ABCT at the time of their nomination.
Potential CandidatesWhen considering making a nomination, think about decision-makers, funders,government officials, business people, consumers, or well-known people who have shared their struggles andbenefited from CBT treatment.
Nominees should demonstrate the characteristics of champions, broadly construed, as recognized in the imple-mentation science literature (see Knudsen,Gutner, & Chorpita, 2019, for examples relevant to ABCT; http://www.abct.org/docs/PastIssue/42n1.pdf). Briefly, ideal candidates should have demonstrated one or more of the following: (1) an endur-ing commitment to the application and impact of one or more evidence-based intervention; (2) the promotion ofinnovation, even in the face of social or organizational indifference or resistance, (3) a willingness to riskreputation as a result of a commitment to change, (4) leadership in the service of the broad mission of positivesocial change, and (5) a willingness to go above and beyond their regular professional duties.
RecognitionNominees will be reviewed in March, June, and October by the ABCT Awards Committee and those meeting criteriawill be forwarded to the ABCT Board of Directors for approval. Recipient will be notified by the ABCT President, andtheir names and photographs will be posted on the ABCT website, along with the rationale for their recognition. Eachyear's champions will also be acknowledged at our annual awards ceremony at the ABCT Convention.
How to NominateEmail your nomination to [email protected] (nomination form available athhttttpp::////wwwwww..aabbcctt..oorrgg//AAwwaarrddss//ddooccss//22001199__CChhaammppiioonnss__NNoommiinnaattiioonn__FFoorrmm..ppddff). Be sure to put "Champions Nomination" in the subject line. Once a nomi-nation is received, an email will be sent from staff, copying the Awards and Recognition Committee Chair. The nomi-nation will be reviewed by the Awards and Recognition Committee and if deemed appropriate for our program, will beforwarded to the ABCT Board of Directors for final approval. Once reviewed and approved by the Board of Directors,the nominee will be contacted directly by the President and followed up with an ABCT staff member for a final reviewof the copy to be posted on the ABCT website.
Champions of Evidence-Based Interventionss
ABCT's Academic Training and Education Standards Committee is currently soliciting nominations for the Spotlight ona Mentor program. The purpose of the Spotlight on a Mentor program is to highlight the diversity of excellent researchmentors within the membership ranks of ABCT. Its goal is to spotlight promising early career and well-established men-tors across all levels of academic rank, areas of specialization, and type of institution.
Nomination Form www.abct.org/Resources/?m=mResources&fa=MentorNominationForm
To submit a nomination, please complete the nomination form and email it to [email protected] by June 1, 2019at 23:59 EST/20:59 PST. Nominations from multiple mentees are encouraged.
s Nominate a Mentor — Spotlight on a Mentor Program
April • 2019 143
PRSRT STDU.S. POSTAGE
PAIDHanover, PAPermit No. 4
the Behavior TherapistAssociation for Behavioraland Cognitive Therapies305 Seventh Avenue, 16th floorNew York, NY 10001-6008212-647-1890 | www.abct.org
ADDRESS SERV ICE REQUESTED
Full Members,New Member Professionals,and Fellows of ABCT:
Remember to cast your electronic vote!If we do not have your email in our system, then we mailedyou a paper ballot. If you did not receive voting materials,please contact Dakota McPherson: [email protected]
This year’s candidates:
PresidentMarc S. AtkinsDavid F. Tolin
is election monthAprils
Representative-at-LargeAmie E. GrillsLaura A. PayneKamila White
ABCT candidates’ biographicaland position statements athttp://www.abct.org/Members/?m=mMembers&fa=Election