This article was downloaded by: [University of Massachusetts], [Dr. Heidi M. Levitt] On: 05 August 2014, At: 11:00 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Psychotherapy Research Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/tpsr20 Wisdom and psychotherapy: Studying expert therapists' clinical wisdom to explicate common processes Heidi M. Levitt a & Elizabeth Piazza-Bonin b a Department of Psychology, University of Massachusetts Boston, Boston, MA, USA b Department of Psychology, The University of Memphis, Memphis, TN, USA Published online: 01 Aug 2014. To cite this article: Heidi M. Levitt & Elizabeth Piazza-Bonin (2014): Wisdom and psychotherapy: Studying expert therapists' clinical wisdom to explicate common processes, Psychotherapy Research, DOI: 10.1080/10503307.2014.937470 To link to this article: http://dx.doi.org/10.1080/10503307.2014.937470 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions
Transcript
This article was downloaded by: [University of Massachusetts], [Dr. Heidi M. Levitt]On: 05 August 2014, At: 11:00Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Psychotherapy ResearchPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/tpsr20
Wisdom and psychotherapy: Studying experttherapists' clinical wisdom to explicate commonprocessesHeidi M. Levitta & Elizabeth Piazza-Boninb
a Department of Psychology, University of Massachusetts Boston, Boston, MA, USAb Department of Psychology, The University of Memphis, Memphis, TN, USAPublished online: 01 Aug 2014.
To cite this article: Heidi M. Levitt & Elizabeth Piazza-Bonin (2014): Wisdom and psychotherapy: Studying expert therapists'clinical wisdom to explicate common processes, Psychotherapy Research, DOI: 10.1080/10503307.2014.937470
To link to this article: http://dx.doi.org/10.1080/10503307.2014.937470
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of theContent. Any opinions and views expressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon andshould be independently verified with primary sources of information. Taylor and Francis shall not be liable forany losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use ofthe Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Wisdom and psychotherapy: Studying expert therapists’ clinical wisdomto explicate common processes
HEIDI M. LEVITT1* & ELIZABETH PIAZZA-BONIN2
1Department of Psychology, University of Massachusetts Boston, Boston, MA, USA & 2Department of Psychology,The University of Memphis, Memphis, TN, USA
(Received 25 September 2013; revised 27 May 2014; accepted 14 June 2014)
AbstractObjective: This research study explores the concept of clinical wisdom. Method: Seventeen psychologists who werenominated multiple times by their peers as wise clinicians participated in an interview on clinical wisdom, analyzed usinggrounded-theory methods. Results: Participants described clinical wisdom as accepting that the best answers to clients’problems often were not immediately accessible and instead using their sense of their clients, their theory of psychotherapy,and their own experiences of adversity, diversity, and intimate relationships to help clients explore the ambiguities andvulnerabilities they experienced to craft idiosyncratic answers. Conclusions: An understanding of clinical wisdom is putforward, characterized by markers and principles for practice, to guide therapy processes within therapists’ intentionality anddirect research on common factors.
Meta-analyses have suggested that psychotherapyorientations contribute comparably little of the vari-ance in client outcome when compared to therapistdifferences. Reviews of this literature (e.g. Crits-Christoph et al., 1991) and studies of clients in bothinpatient and outpatient contexts (e.g. Laska, Smith,Wislocki, Minami, & Wampold, 2013; Wampold &Brown, 2005) have estimated that differences intrinsicto therapists, separate from their psychotherapy ori-entation, account for approximately 5–12% of thevariance in outcome change for clients. Research hassuggested, however, that in addition to these findings,a substantial amount of the correlation betweenalliance and outcome should be attributed to differ-ences between therapists.
In a study of 331 patients treated by 80 therapists,Baldwin, Wampold, and Imel (2007) found thatwhen separating therapist and client variation inclients’ alliance ratings, it was only the variationbetween therapists that predicted outcome and drovethe alliance–outcome correlation and not variation
between clients within therapists. These findings werecorroborated by other studies that also found thattherapist’s variability in the alliance significantly pre-dicted outcome but not client variability (Dinger,Strack, Leichsenring, Wilmers, & Schauenburg, 2008;Zuroff, Kelly, Leybman, Blatt, & Wampold, 2010).A recent meta-analysis of 69 studies from the alliance–outcome literature (Del Re, Flückiger, Horvath,Symonds, & Wampold, 2012) confirmed this patternin findings with therapist differences in the allianceaccounting for a much higher proportion of thealliance–outcome relationship. This body of researchsuggests that therapist differences are central to under-standing both alliance and outcome and that thedevelopment of empirical research on therapist qualit-ies might be a profitable avenue for psychotherapyresearchers.
Several researchers have made strides towardsanswering this question by exploring the empiricalbasis for relationship processes within the client–therapist relationships. Norcross and Wampold
*Correspondence concerning this article should be addressed to Heidi M. Levitt, Department of Psychology, University of MassachusettsBoston, Boston, MA, USA. Email: [email protected]
(2011) reviewed a body of meta-analytic research onthe psychotherapy relationship and found supportfor processes such as empathy, alliance, cohesion,client feedback, collaboration, and goal consensus.Although this innovative line of research identifiesimportant factors at play in therapy, it does notaddress how these factors are best enacted within therelationship or developed within the therapist.
Research that focuses on expert therapists’ processeswithin their sessions, however, augments these find-ings. For instance, Goldfried, Raue, and Castonguay(1998) coded sessions of master therapists nominatedby others in the cognitive–behavioral (CB) and psycho-dynamic-interpersonal (PI) traditions. They foundthat PI therapists were more likely to highlight emo-tional content and that the CB therapists were morelikely to emphasize situational factors. Also, CBtherapists were more likely to encourage clients tocompare their experiences to others and to encouragebetween-session experiences, while PI therapistsencouraged clients to relate their experiences tothemes within their own lives. Average effect sizeswere small across these comparisons but together theypaint an interesting picture of how therapists intervenedifferently.
Continuing this line of research, a series of articlesby Levitt and Williams (Levitt & Williams, 2010;Williams & Levitt, 2007a, 2007b) described qualitat-ive research that examined eminent therapists’moment-to-moment therapy processes. This researchfocused on decision-making points that emerged ininterviews with expert therapists about their processesof guiding psychotherapy (see Goldfried et al., 1998for a similar research strategy) and developed a set ofcross-orientation principles to help novice therapistsguide the change process. One of their main findingswas that relationship safety was prioritized to theextent that risk taking was necessary in session.Specifically, they found that CB therapists tended tostructure a didactic relationship that could bestsupport risk taking in exercises between sessions whilethe humanist, psychodynamic, and constructivisttherapists tended to prioritize the relationship overtasks in order to support in-session vulnerability andrisk taking. The second central finding was thattherapists across all orientations used a similar set ofstrategies to develop new awareness in clients: (i)stimulating curiosity about their own functioning to(ii) sustain exploration in connection with distressingexperiential states for (iii) the purpose of generatingexperiences of difference (i.e. based upon interper-sonal, emotional, cognitive, or behavioral patterns),(iv) stimulating reflexive symbolization of their devel-oping awareness, and (v) providing the structure toallow for the integration of these differences. Bytargeting therapists’ intentionality, this work is more
applicable for training purposes than research target-ing specific behaviors as it guides novices to considerthe motivations of expert therapists as they developresponses attuned to context within the interpersonaldynamics of evolving sessions. The current researchcontinues this tradition by exploring expert thera-pists’ intentionality, extending previous research byfocusing on therapists who have been nominated fortheir clinical wisdom.
Defining and Distinguishing Clinical Wisdom
Wisdom is not a concept easily understood, and therehave been many attempts to define this concept withina psychological framework. Researchers have soughtto understand wisdom by distinguishing it from arelated concept—intelligence. Robert Sternberg, aleading researcher in the area, has defined wisdom(1998) as a deeper understanding of reality usedtowards the common good encompassing the definingcharacteristics of concern for others, psychologicalunderstanding of others, capacity for self-knowledge,the ability to reframe information, the ability to take thelong view of problems, readily admitting to andlearning from mistakes, maturity, intuition, and theability to “see through” situations and circumstances(1990). He summarized that “the wise person resistsautomatization of thought but seeks to understand it inothers … [whereas] the intelligent person welcomesautomatization” (1990, p. 153, italics preserved).Lastly, Sternberg (1998) proposed that while intelli-gence includes the ability to solve a problem and thinkwithin context, wisdom embodies the ability to movebeyond this realm and surpass the immediate contex-tual limits.
Though empirical research directly linking wisdomto psychotherapy is rare, Baltes and his colleagueshave examined the link between psychological expert-ise and wisdom. Their first study assessed wisdom-related responses of participants who were asked tothink-aloud about a life-review task (Staudinger,Smith, & Baltes, 1992). Results demonstrated thatparticipants in professions related to human services(including clinical psychology) were rated higher thantheir nonhuman service counterparts. These findingswere replicated in a subsequent study conductedby Smith, Staudinger, and Baltes (1994) when clinicalpsychologists and other professionals were rated ontheir responses to wisdom-related dilemmas. Onceagain, psychologists outperformed the control group ofprofessionals with similar levels of education. Thisfinding suggests that perhaps there is an aspect ofwisdom-related knowledge that draws certain peopleto psychology or is taught in that profession. Anotherfinding in this study was that psychologists performedbetter on wisdom tasks in which the dilemmas were
2 H. M. Levitt and E. Piazza-Bonin
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
congruent with their own stage in life. Thus, olderpsychologists performed better on tasks related to lateadulthood, and younger psychologists answered morewisely about dilemmas of early adulthood.
Further research by Baltes, Staudinger, Maercker,and Smith (1995) found that both older clinicalpsychologists and lay people nominated for theirwisdom, outperformed a cross-generational controlgroup of educated individuals. This study reaffirmsprevious findings regarding clinical psychologists’abilities on such tasks, but introduces the notionthat lay persons who are nominated as wise performas well—supporting the idea that nominators canrecognize wisdom in others. In this case, the nomi-nators were reputable journalists from various mediawho were asked to identify “wise” citizens of Berlinwho were active in public life. The clinical psychol-ogists in the study outperformed the wisdom nomi-nees in the life planning task, however, whichsuggests that training in this area may be an advant-age. Another study by Baltes and his colleaguesfound that training and practice in clinical psycho-logy was a predictor of wisdom-related performance(Staudinger, Maciel, Smith, & Baltes, 1998). In thissame study of professionals and clinical psycholo-gists, factors such as personality and intelligencealso were explored in relation to wisdom. Findingsshowed that personality variables were strongerpredictors of wisdom than intelligence variables.Personality predictors included openness to experi-ence and midrange scores on the introversion–extroversion continuum. This finding lends credib-ility to Sternberg’s (1990) model of wisdom in whichambiguity is welcomed.
Further research conducted by Staudinger andBaltes (1996) described wisdom-related perform-ance as fostered by interactive minds. The conceptof interactive minds
implies that the acquisition and manifestation ofindividual cognitions influence and are influencedby cognitions of others and that these reciprocalinfluences between minds contribute to the activa-tion and modification of already available cognitionsas well as to the generation of new ones. (Staudingerand Baltes, 1996, p 746)
They found that wisdom-related performance wasenhanced by a social-interactive setting or an ima-gined social context, such that imagining and reflect-ing upon the opinions of others who were valuedserved to increase wisdom-related ability. This topicis of relevance to psychotherapy—essentially a set-ting in which interactive minds are present andengaged. The aim of the current research study isto provide an understanding of wisdom and how it
functions within the psychotherapy of cliniciansknown for their clinical wisdom.
Hanna and Ottens (1995) surmised that psy-chotherapists need the capacity for intelligence, butthat wisdom also is needed to help the therapistnavigate through difficult interpersonal situations,and to guide therapists’ abilities to execute propertiming with clients. Furthermore, they theorized thattraditional research measures in psychology arebased on an erroneous model of intelligence,whereas psychotherapy calls for a therapist to usewisdom-based knowledge. They argued that thisincompatibility reduces practitioners’ interest inutilizing research results (Cohen, Sargent, & Sechr-est, 1986; Morrow-Bradley & Elliot, 1986; Stricker,1992) and instead encourages them instead to seekcounsel from colleagues when difficulties in therapyarise (Morrow-Bradley & Elliot, 1986). They sug-gested that qualitative research on clinical wisdommay help to “close the gap” between therapy researchand practice (p. 211). The current research has beendesigned to develop a definition and foundationalunderstanding of clinical wisdom where one hasbeen lacking. Grounded-theory methods are wellsuited for developing an empirically based theory ofa phenomenon where none has previously existed(Glaser & Strauss, 1967) and have been used towardthis end.
Method
Participants
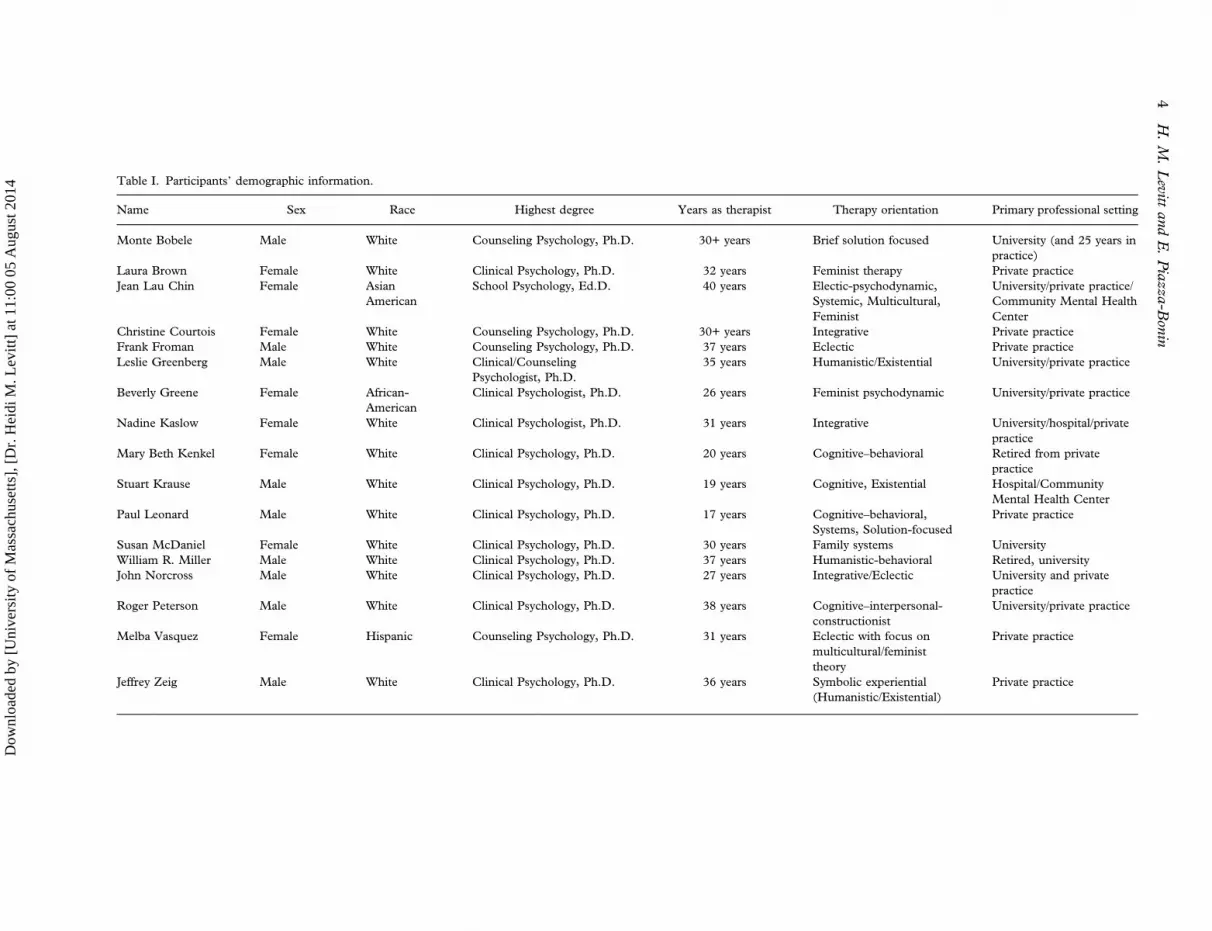
Interviewees. The interviewees all were psychol-ogists and psychotherapists nominated multiple timesfor their clinical wisdom. Demographic informationwas collected about their age, race, gender, years ofpractice, psychotherapy orientation, and professionalsetting (see Table I). They had a variety of psycho-therapy orientations and different educational back-grounds: one was a school psychologist, four werecounseling psychologists, and the others were clinicalpsychologists. They included eight women and ninemen who were mostly white with three participants ofcolor. They were experienced therapists with somerange in the years they had been in practice (17–40years). Psychologists from the United States weresought—both to create a manageable process ofnomination recruitment and so interviewees wouldshare a similar frame of reference. One Canadian alsowas interviewed who was a faculty member in aclinical psychology program approved by the APA.
Participants consented to have their identitiesdisclosed in this paper. The expert recruitmentprocess we used is in line with suggestions that thestudy of identified masters in an area could shed
Christine Courtois Female White Counseling Psychology, Ph.D. 30+ years Integrative Private practiceFrank Froman Male White Counseling Psychology, Ph.D. 37 years Eclectic Private practiceLeslie Greenberg Male White Clinical/Counseling
Psychologist, Ph.D.35 years Humanistic/Existential University/private practice
Beverly Greene Female African-American
Clinical Psychologist, Ph.D. 26 years Feminist psychodynamic University/private practice
Nadine Kaslow Female White Clinical Psychologist, Ph.D. 31 years Integrative University/hospital/privatepractice
Mary Beth Kenkel Female White Clinical Psychology, Ph.D. 20 years Cognitive–behavioral Retired from privatepractice
Stuart Krause Male White Clinical Psychology, Ph.D. 19 years Cognitive, Existential Hospital/CommunityMental Health Center
Paul Leonard Male White Clinical Psychology, Ph.D. 17 years Cognitive–behavioral,Systems, Solution-focused
Private practice
Susan McDaniel Female White Clinical Psychology, Ph.D. 30 years Family systems UniversityWilliam R. Miller Male White Clinical Psychology, Ph.D. 37 years Humanistic-behavioral Retired, universityJohn Norcross Male White Clinical Psychology, Ph.D. 27 years Integrative/Eclectic University and private
practiceRoger Peterson Male White Clinical Psychology, Ph.D. 38 years Cognitive–interpersonal-
constructionistUniversity/private practice
Melba Vasquez Female Hispanic Counseling Psychology, Ph.D. 31 years Eclectic with focus onmulticultural/feministtheory
Private practice
Jeffrey Zeig Male White Clinical Psychology, Ph.D. 36 years Symbolic experiential(Humanistic/Existential)
Private practice
4H.M.Levitt
andE.Piazza-B
onin
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
light upon effective processes (e.g. Goldfried et al.,1998; Greenberg, 1986). In this vein, our partici-pants’ identities are provided as contextual informa-tion can help establish their credibility.
That many of the participants are establishedfigures in psychology is not unexpected consideringthat wise therapists who are more well-known mayhave greater opportunity to have others observe theirpsychotherapy in trainings and videos than wisetherapists who work in isolation. Also, participantsmay become recognized figures on the basis of thewisdom they have contributed to the field of psy-chotherapy. Still, there is variety in the professionalprestige of the participants who were nominated.
Researchers. The authors’ psychotherapyapproaches are influenced most heavily by human-istic, feminist and constructivist therapies, however,both identify as integrationists. Before the comple-tion of this qualitative study, the researchers did nothave specific ideas on how wisdom influencedpsychotherapy, but believed that this general qualityfacilitated an optimal psychotherapy experience forclients. Researcher A was a clinical psychologist,who was awarded a grant from the John TempletonFoundation and University of Chicago’s WisdomProject, conducted the interviews, supervised thenomination and analytic process, and was a co-analyst of the data. Researcher B was a clinicalpsychology graduate student who conducted theco-analysis of this data and wrote up the initialfindings in a thesis project (Reference withheld).
Procedure
Recruitment. Prior research has found that anomination process has been successful in identify-ing people who function better on wisdom-relatedtasks than a random sample (Baltes et al., 1995).The 17 interviewees in this study (see Table I) werenominated multiple times in response to a call fornominations of psychologists noted for their clinicalwisdom. In all, approximately 400 individual leadersof national, state, and city psychology organizationswere contacted by email and asked to send on thecall to their members to nominate psychotherapists“who you think enact wisdom within the practiceof psychotherapy.” Nominations also were soughtfrom 140 psychotherapy-related organizations, 10American Psychological Association (APA) psycho-therapy-related journal editors, 64 counseling psy-chology and 178 clinical psychology doctoral pro‐grams, and 20 psychology groups with minorityinterests (e.g. Society for the Psychological Study ofLesbian, Gay and Bisexual Issues, Association for
Women in Psychology, The Society for the Psycho-logical Study of Ethnic Minority Issues).
In this way, the researchers sought variety in theirsample with regards to age, race/ethnicity, gender,and psychotherapy orientation. We also indicated inthe call that, “The definition of professional wisdomis quite broad and not meant to be confined to anyone demographic characteristic (e.g. age, gender orrace/ethnicity).” This process yielded 300 nomina-tions. Consensus between nominators was sought toreduce the likelihood that a nominee was nominatedbased upon an idiosyncratic definition of wisdom.Nineteen of the psychotherapists received multiplenominations and were invited to participate in aninterview, with 17 therapists accepting our requestand being interviewed. Most of the participants (11)were nominated twice with four being nominatedthree times, one nominated four times, and onenominated seven times.
We received from a small sample of the nomina-tors (N = 20) a description of the basis for thenominations in response to a question on thenomination form. Their answers indicated thatnominations were based upon watching or readingtranscripts of the person’s therapy, having receivedsupervision, sharing cases, or having read descrip-tions of the person’s therapy process. Theseresponses suggested that the nominations were basedupon the nominee’s clinical conceptualization andintervention skills as a therapist rather than uponother professional activities (e.g. theorizing, scientificexpertise).
Interviews. Interviews were recorded and con-ducted by phone, with the exception of one localparticipant who was interviewed in person. Theinterviews were approximately 1 hr in duration and,because the goal of this research was to develop anunderstanding of clinical wisdom grounded in theparticipants’ experiences, an a priori definition ofwisdom was not provided. Instead, interviewees wereasked to reflect upon their own understanding ofclinical wisdom and explore the ways it influencedtheir work as psychotherapy professionals. Thecentral question asked in each semi-structured inter-view was “How do you enact wisdom within psy-chotherapy?” Participants were asked to share anythoughts that they considered relevant to this ques-tion. Sub-questions were used to ask participants todefine clinical wisdom and to explain the conse-quences and outcomes of clinical wisdom withinpsychotherapy. For instance, to facilitate the pro-cess defining clinical wisdom, participants wereasked first to directly generate a definition and thento comment upon whether different factors influ-enced clinical wisdom (i.e. intelligence, emotion,
personality characteristics, communication styles).To facilitate the discussion of consequences ofclinical wisdom, participants were asked to describea story of a wise moment, and the effects of clinicalwisdom within psychotherapy. Questions were for-mulated to be nonleading and open-ended.
Qualitative Method
Grounded-theory analysis. Grounded-theoryanalysis (Glaser & Strauss, 1967) is a rigorousmethod that utilizes inductive analysis to exploresubjective experiences (e.g. Fassinger, 2005; Rennie,2000). The approach to grounded theory used in thisproject was developed by David Rennie (e.g. Rennie,Phillips, & Quartaro, 1988). After transcribing eachinterview, the Nvivo 8 software program was used toorganize the analysis of the data. Each interview wasexamined, first dividing the text into singular units oftext containing one meaning—that is, meaning units(Giorgi, 2009)—relevant to the topic of wisdom.These meaning units then underwent constant com-parison, in which every unit was compared to everyother unit, and were subsequently organized intocategories based on similar meanings. These initialcategories were given a label to represent thatcommon meaning. Then, these categories wereanalyzed and, based upon commonalities therein,organized into higher order categories. This processwas repeated until a hierarchy was formed which wascrowned with a core category that reflected a centralinterpretation of the data. Saturation was reached atinterview 15; it is the point at which incominginterview data no longer added new categories tothe hierarchy.
As is typical in grounded-theory analyses, personalbeliefs and assumptions about the data were recordedby memo writing throughout the research process.This form of documentation also aided in guiding theresearchers to communicate with each other aboutevolving ideas and analyses, to become aware of theways their ideas might influence the data, and to thinkthrough how to limit this influence.
Credibility checks. The researchers implemen-ted three credibility checks to assess the accuracy ofthe data. First, participants were given the oppor-tunity at the end of each interview to provide furtherinformation that might have been omitted. Thesequestions (i.e. “Was there anything that we didn’tdiscuss that you feel is relevant to share?”) helped toensure that the data collection was thorough.
The second credibility check used was a continualreview of the research analysis by both co-investiga-tors, who bring expertise in the qualitative methodsand share an intimate knowledge of the data. This
process of consensus can provide an opportunity forresearchers to contribute their understandings of thecomplex nature of the data and demonstrate thatresearchers with unique perspectives share an inter-pretation of the data (Hill et al., 2005).
The third credibility check utilized participant feed-back to comment upon the proposed model of clinicalwisdom. All of the interviewees were provided awritten summary of the findings and asked to providefeedback, with six responding to our request. Thefeedback was positive overall, with some suggestionsfor slight modifications (which will be further dis-cussed in the results section). For instance, participantPaul Leonard commented on the results saying, “Yourwork is very important. I wish these issues wereaddressed earlier in my training” (personal commun-ication, October 2010). Christine Courtois alsoremarked, “I appreciate your findings.… I will seek touse your information in some of my training, hoping topass on the wisdom of colleagues” (personal commun-ication, October 2010). Positive feedback was receivedfrom participants across orientations, which bolsteredour confidence in the findings.
Results
Participant interviews were transcribed and thendivided into 742 meaning units. A hierarchy wasdeveloped containing seven levels. The top threelevels will be discussed as these levels describe themost meaningful findings in the analyses. Thefollowing vocabulary will be used to make clear thelevel of hierarchy being discussed: The core categorythat emerged from this analysis contained fourclusters, which in turn subsumed 11 categories thatencompassed 27 subcategories. This section willreview each cluster in turn followed by a descriptionof the core category.
The number of therapists whose interview con-tributed to a category will be provided; however,these counts do not signify agreement (as the inter-views were semi-structured and so not all partici-pants were asked the same questions—as is typical inthis method) but provide a rough estimate of howsalient an idea was across the interviews. Similar toHill’s system (Hill, Nutt-Williams, Heaton, Thomp-son, & Rhodes, 1996) to describe these counts, thewords “few” will refer to 1–3 therapists, “some” to4–8 therapists, “many” to 9–11 therapists, “most” to12–16 therapists, and “all” to 17 therapists. Thesenumbers can best be interpreted by looking inTable II at the number of participants at the levelof the subcategories and then seeing how thesesubcategories were grouped together in forming thecategories and clusters. Readers can use Table II andnumbers within it as supplemental information to
Table II. Category titles and numbers of participants who contributed units.
Category Subcategory
Cluster 1: Overcoming aFear of the Dark and theIntimate: BeyondRational IntelligenceTowards Wisdom ViaIntrospection and LivedExperience ofStruggle. (17)
1.1 Intelligence is not enough:Wise therapists have emotionalintelligence grounded in difficultlife experiences to betterunderstand how to work throughpainful and powerfulemotions. (16)
1.1a Intelligence is necessary but insufficient tobe wise. (11)1.1b Intelligence is separate from wisdom:Intelligent people are not always wise, as theycan be too busy trying to be smart, whileoblivious to understanding human beings. (7)1.1c A wise therapist has emotional intelligencegrounded in own difficult life experiences,attending to own emotions in order toempathically guide clients into understandingand utilizing their emotions. (13)
1.2 Wise therapists have socialintelligence: Intelligence alone canblock wisdom because it resistsambiguity andunpredictability. (16)
1.2a A wise psychotherapist has intelligence andbroad knowledge base, but an even greater senseof knowledge about people, relationships, andpersonality, with life experience to drawfrom. (16)1.2b Intelligence alone can impede wisdom. (2)1.2c Need to have experienced intimaterelationships to be able to understand the needs,feelings, and dynamics of a relationship withclients. (1)
1.3 We must strive to knowourselves before we can know ourclients: Being vulnerable andauthentic allows us to appreciatethe human experience. (14)
1.3a Therapists must engage in introspection toknow their own emotions in order to empathizewith clients. (12)1.3b We must be willing to be vulnerable andauthentic about our own pain and suffering, andthe darker parts of our selves, helping us to relateto clients as equals struggling through the samejourney of being human beings. (9)
Cluster 2: Staying withVulnerability andAmbiguity HelpsTherapists to work fromwithin the Clients’ ValueFramework andFacilitate Openings forEither Acceptance orChange. (17)
2.1 Therapists’ valuing clients’authority begets clients’empowerment: Creating agency byadvocating with, not for, clients,and engaging their own values,preferences, and experientialwisdom. (11)
2.1a Avoiding resistance: Soliciting clientpreferences while being perceptive to clientvalues and differences. (6)2.1b Wise psychotherapists are collaborative andequal partners with clients while utilizing clientsvalues, preferences, and experiential wisdom intherapy, helping clients to generate their owninsights. (7)2.1c Wise therapists raise difficult questionsabout self and the world that clients might havenever considered, especially important for clientsfrom marginalized groups. (3)
2.2 Shifting perspectives byexploring threat and uncertainty:A valuing of relational attunementover decontextualized interventionenactment. (15)
2.2a Must be willing to develop a relationship bybeing ignorant about your client and curiouswithout imposing your own categories, becausewe never know who is sitting in front of us. (14)2.2b A wise psychotherapist is optimistic andenthusiastic, often with appreciation for humorin therapy, looking for client strengths, providinghope that clients can survive and move past theirpain. (8)2.2c A wise psychotherapist fostersunderstanding, connection, and insight byslowing down and genuinely empathizing withclients in session. (6)
Psychotherapy Research 7
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
see how the data that were organized into sub-categories on the basis of commonalities withinmeaning units and then were grouped into categoriesand higher order clusters as the hierarchy developed.
Cluster 1: Overcoming a Fear of the Dark andthe Intimate: Beyond Rational Intelligencetowards Wisdom via Introspection and LivedExperience of Struggle
All the participants contributed to this cluster,describing the dynamic interplay between wisdomand intelligence, and the qualities that divide thetwo. Intelligence was thought to facilitate the abilityto learn theory and techniques, while wisdom guidedthe application of that knowledge in therapy. Therewere three categories in this cluster.
Category 1: Intelligence is not enough:Wise therapists have emotional intelligencegrounded in difficult life experiences to betterunderstand how to work through painful andpowerful emotions. While many therapists (6 of 17)viewed intelligence as separate from wisdom, others(11 of 17) expressed that rationale intelligence was anecessary, but insufficient, underpinning of wisdom inpsychotherapy. Most interviewees (13 of 17) explainedthat to develop clinical wisdom, therapists neededcertain forms of intelligence. One participant said:
I don’t think you have to be genius level, but …emotional intelligence is critical … because you’re… sharing an affect state with them. Or mayberegistering something that they’re not registeringand being able to feed it back to them (ChristineCourtois)
Another participant described the need to guideclients to explore intense emotion:
You need the capacity to be in the presence of strongemotion and not go “Eek!” … to just be there … to
be at home with somebody sobbing or raging orshaking in your office and say, “Alright.… You’rehaving very intense feelings.… What are your intensefeelings telling you? … How can that give youinformation?” (Laura Brown)
Wise therapists were thought to not only toleratethreatening emotions but also have the interpersonalsensitivity to guide clients to stay in contact withthem in order to recognize their meaning.
The capacity for emotional intelligence was thoughtto be enhanced by therapists’ personal experiences ofloss and pain, as they could draw from their ownexperiences. John Norcross explained this, saying thattherapists need
An empathic ability to see it [a situation] from bothsides.… [to have] emotional experiences with thefundamentals of life … birth, death, joy, grief, loss …[so] there’s an emotional counterpoint, and it needsto be grounded … within sufficient emotionalexperiences.
Therapists thought that connecting to the spectrumof their own emotional experiences, especially thosegrounded in life struggles, could help them guideclients in utilizing and understanding their ownemotions more effectively.
Category 2: Wise therapists have socialintelligence: intelligence alone can block wisdombecause it resists tolerance for ambiguity andunpredictability. In addition to emotional intelli-gence, the majority of participants (16 of 17)expressed that it was necessary for wise therapiststo have relational and social intelligence. LeslieGreenberg described,
I can’t see people having wisdom if they … haven’treally lived [in] an intimate relationship … [an]attachment relationship.… Having struggled to beintimate with another … gives you an understanding
Table II. (Continued)
Category Subcategory
2.3 Wise psychotherapists do notrely upon standardized approachesto eliminate uncertainty becausethey understand that not having apredetermined path is oftennecessary for attunement. (13)
2.3a A wise psychotherapist is able to remaincalm when facing uncertainty, crisis, andambiguity in therapy. (4)2.3b Wise psychotherapists have a strong moral,ethical, and value-related compass to rely on. (5)2.3c Wise PT sits with humility, being aware ofwhat they don’t know, and accepting that thisunderstanding is uncomfortable and scary. (9)
Core category: Clinical wisdom is taking the risk not to know: Openly exploring clients’ ambiguity and vulnerability to intervene within theirvalues and context.
8 H. M. Levitt and E. Piazza-Bonin
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
of … life in a relationship … what they feel, or whatthey need, and what relationships are all about.
The experience of relational vulnerability and nego-tiating states of conflict and feelings of rejection wereidentified as prerequisites to wisdom.
Participants (2 of 17) raised concerns that over-reliance on rational intelligence could impede wis-dom, especially if therapists-in-training are taught toprovide quick answers rather than to tolerate andexplore ambiguity. One participant described howthis skill could be useful:
I did tremendous work in terms of my neuropsy-chology classes … understand[ing] why somebodyis, um, experiencing these memory problems.…However, that knowledge I don’t think is going tobe, or that intelligence is going to be, useful unless Ican convey in some way to the individual I’mworking with … what that knowledge means interms of being more effective in their own life ordealing with [their] problems.… [An] understandingof people and why they act the way they do and feelthe way they do is probably more important thaninformational knowledge … or the knowledge ofdifferent theories. (Mary Beth Kenkle)
Therapists described that social intelligence allowedfor more effective communication and allowed themto remain attuned to the complexities of clients’interpersonal responses.
Category 3: We must strive to know ourselvesbefore we can know our clients: being vulnerableand authentic allows us to appreciate the humanexperience. Most therapists (14 of 17) expressedthat their clinical wisdom was developed by goingbeyond textbook knowledge and pushing themselvesto accept their own difficult experiences, especiallythose that felt dark and uncomfortable to explore.This candid introspection was thought to aid thera-pists in connecting to their clients by
show[ing] some willingness to be accessible, reach-able, approachable. I am a flawed person like youare. The difference between you and me – the onlydifference that I’m really aware of right now – is thatyou’re diagnosed and I’m not” (Stuart Krause).Leslie Greenberg described emotions that exist ineveryone: “an odious rage … spite and vengeanceand hate and jealously … [by] recognizing the darkerpart … [therapists help] people to integrate thatrather than to deny it … to understand that that’swhat it is to be human.
Being reflexive about their internal experiences,helped participants go beyond an objective, intellec-tual appraisal of clients’ difficulties to a joinedunderstanding of clients’ suffering and anguish.
Participants suggested that self-reflection couldcome via many routes, with personal therapy beingmentioned most often (12 of 17). One therapistexplained:
My understanding of how slow that process is …how, um, difficult, emotionally, it can be to intro-spect … I gained a lot of that, not from anintellectually distant study of therapy, but [from]that state of being a patient … the affective progres-sion of sloshing through that is very laborious. (PaulLeonard)
Therapists expressed the need to be constantlyrequiring themselves to engage in the emotionalwork that they expect of their clients and to confrontfeelings necessary for their own growth.
While therapists thought it important to developan understanding of clients’ difficulties, a fewparticipants (2 of 17) highlighted the need to balancebeing empathic while maintaining a sense of bound-aries when identifying with clients’ stories. BeverlyGreene described how therapists from marginalizedgroups might have an inherent capacity to developthis skill:
When you’re at the margin … you have an oppor-tunity to see the center from a distance … what wecall therapeutic distance is that capacity to be emo-tionally present and available in the present … andto take a step back and sort of be able to look at theinteraction as its taking place … even though you’reparticipating in it.
Shifting back and forth in this manner requires notonly the ability to intellectually assess the interactionbetween client and therapist but also the capacity forexperiencing emotional contact with a client whilereserving the distance to continue to guide the clientforward—a capacity that was a hallmark of clinicalwisdom.
The following principles were developed fromCluster 1:
Principle 1.1: To develop clinical wisdom, therapistsshould learn to become comfortable with the emo-tions that they find most threatening or ambiguousin themselves so that they can understand theseaspects in their clients.
Principle 1.2: To develop clinical wisdom, therapistsshould learn about how the ways they relate to andare experienced by others interpersonally—especiallyin intimate, vulnerable, and dependency-based rela-tionships—so they can better navigate their therap-ist–client relationships and understand their clients’relationship patterns.
One participant suggested a slight modification tothe principles to emphasize ambiguity, which we
Psychotherapy Research 9
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
agreed was helpful and changed, though he agreedwith the findings overall.
Cluster 2: Staying with Vulnerability andAmbiguity Helps Therapists Work from withinthe Clients’ Value Framework and FacilitateOpenings for either Acceptance or Change
Seventeen participants contributed to this clusterand described how they sought to create change intheir clients that was coherent with clients’ valuesand perspectives. Therapists described acting as aguide, typically encouraging clients to come to theirown insights rather than attempting to foist solutionsupon them. There were three categories in thiscluster.
Category 1: Therapists’ valuing clients’authority begets clients’ empowerment: creatingagency by advocating with, not for, clients, andengaging their own values, preferences, andexperiential wisdom. Many participants (7 of 17)expressed adopting a collaborative stance with clientsto foster client empowerment in therapy. One ther-apist described how the clinically wise therapistnavigates therapy in this manner:
It’s about being able to co-construct. I think I’mmuch less likely to go from A to Z with my patientsthan I used to be. I’m much more, “Let’s figure thisout together, and I’ll help you to take the nextstep.” … I used to get more into making, you know,interesting interpretations. … [but] it was like “Ok,well, that might be right, but it’s not helpful. …[instead we should] end up doing it together.(Nadine Kaslow)
Therapists who enacted a more collaborativestance with clients explained that whether facilitatingchange or acceptance, it was best for insights andsolutions to unfold from clients. One particip-ant said:
There are two Latin verbs I use…. There’s docere …related to a deficit model, that “I have what you needand I’m going to impart it to you.” … Then there’sducere … “to call forth from” … “to pull out of.” …A verb used to draw water from a well … [the latteris related to wisdom because] it’s using the client’swisdom … taking advantage of a rather vast store ofknowledge and experience that the person has.(William Miller)
Guiding clients to come to their own insights andmeaning was thought to empower clients by helpingthem develop the ability and confidence to rely upontheir own wisdom when confronted with problemsoutside of therapy.
Participants described helping clients tap into theirinternal wisdom by using experiential exercises intherapy. One therapist said:
You can’t say to people, “cheer up” if they’redepressed, and you know, give them a book about… how to cheer up.… People get caught up inaffective states. So, if you want to do something thathelps people to change, uh, a state, an emotion, youhave to rely on methods that are more artistic …rather than using didactics. (Jeff Zeig)
He later described these methods as building from“lots of little experiential gains or moments youcreate in experiences by using … metaphors …allusion … anecdotes … poems.… The art ofpsychotherapy is how to make simple ideas comealive.” Creatively helping clients attend to theirexperiences in an emotionally vivid manner wasthought to encourage more memorable and access-ible insights, helping clients extend these lessonsbeyond the therapy room.
Some therapists (6 of 17) said that working withinclients’ unique perspectives and values could reduceresistance and fear of the therapeutic process. LeslieGreenberg explained, “Being wise is … knowing howto say things in a way that other people can hearand … being able to adapt it so that they will hear.”Clients were thought to become more invested in thechange process when therapists’ solutions incorpo-rated the complexities of clients’ cultures, socialrelationships, and pragmatic limitations.
A few participants (3 of 17), however, thought thatstimulating and challenging clients’ thinking byposing novel, provocative questions could generatenew ways of conceptualizing their struggles and theirneeds. One interviewee explained that therapistsshould encourage clients to “not just uncriticallyaccept whatever it is they’re told about themselves orthe world. But, to use their own experiences andtheir own intuitions to … guide, supplement andevaluate that information” (Beverly Greene). Thisform of inquiry was thought to be especially import-ant for clients from marginalized groups, helpingthem to articulate needs and feelings that might bedisenfranchised. This approach was still collaborat-ive, as challenges did not stem from the therapists’knowledge but rather from contrasting the clients’own conflicting experiences.
While working with clients in this egalitarianmanner, some interviewees (4 of 17) describedadopting transparency about issues that might bedifficult to talk about but are important in thetherapeutic relationship (e.g. rifts in the alliance,value differences). Being honest and upfront withclients, no matter how challenging, was thought to
10 H. M. Levitt and E. Piazza-Bonin
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
create a more equal and respectful partnership. Thisapproach was thought to further client agency.
Category 2: Shifting perspectives by exploringthreat and uncertainty: a valuing of relationalattunement over decontextualized interventionenactment. Therapists described exploring ambigu-ities in the experiences clients convey in order todevelop a more complete understanding. Most of theparticipants (14 of 17) described the wise therapist aslacking preconceived notions about clients, allowingthem to explore these uncertainties with respectfulinterest and curiosity. One participant said:
Wisdom is knowing what you don’t know.… Beingable to trust that what’s really important is what’shappening in the relationship, and that you’re not incharge of that.… You cannot know what’s going tohappen.… You have to be willing to trust the processrather than impose some kind of, um, presupposi-tions on it. (Laura Brown)
Therapists valued this relational attunement,humbly acknowledging clients as the owners andteachers of their experiences. Another participantexplained that therapists need to “be able to seeit [the experience] from their [the client’s] perspect-ive.… Otherwise, you’re not able to provide the kindof intervention that would … effect behaviorchange … and [generate] meaning for the client”(Jean Lau Chin). Yet another therapist said that thewise therapist knows
when to shut up.… The patient is going to informyou about what they are … which is not the same asacquiescing to whatever a patient wants you to do,but, you have to listen in order to understand. And,you shouldn’t be acting on anything you really don’tunderstand. (Beverly Greene)
Therapists thought that using their curiosity andintrigue as guides in therapy increased their attune-ment to each client’s circumstances and needs.
The participants (6 of 17) also described formingmeaningful connections with clients by taking timein therapy to hone in on what clients are commun-icating within session, attending to cues beyond theclients’ words. One therapist articulated the value ofthis attunement, saying:
Being able to slow them [clients] down. … [makes]the relationship become special. It’s not just, um,“Here’s what happened, here’s my problem, duh-duh-duh.” It’s more like, “Hold on. You just had alook on your face that didn’t look happy. Can youtell me about that?” And then it becomes more realand genuine and deeper. (Paul Leonard)
Therapists thought that attending to clients in thismanner could help clients feel genuinely cared forwhile also providing an opportunity to uncovertopics needing further exploration that might havebeen missed if the therapist were too focused onenacting a specific intervention. They said to do thiswork, therapists should value relational attunementabove specific interventions.
Therapists (8 of 17) also described attentivelyresponding to clients’ hardships through an optim-istic lens, even utilizing humor in the face of pain toprovide new perspectives, hope, and ultimately self-acceptance. Frank Froman described that usinghumor with clients,
gives them something which is unique and special tolook back on … and … gives them a sense of hope.…When people are laughing … when they find humorin their situation … they learn to look at things indifferent ways.… It [therapy] should be extraordin-arily memorable.
Therapists described using humor and optimismwithin the therapist–client relationship as an effectiveway of shifting clients’ perspectives towards hope,outside of any particular interventions.
Category 3: Wise psychotherapists do not relyupon standardized approaches to eliminateuncertainty because they understand that nothaving a predetermined path is often necessaryfor attunement. Most participants (13 of 17)discussed the value of humility in the wise practiceof psychotherapy, acknowledging that clients arecomplex—often beyond apprehension. Though par-ticipants valued being empirically informed, theytended to emphasize a greater need to be flexiblewith interventions and to translate standardizedapproaches into more dynamic forms. One particip-ant said of evidence-based therapy:
It [evidence-based therapy] can have a lot of rigor-ous, black and white, methodological stuff going on.Well, I applaud that. I think it’s a necessary, butinsufficient condition, for real therapy.… There aresome problems that evidence-based therapies don’ttouch anyway.… Not everything that a client walksin the door with, you can flip through your evidence-based manual and, “Aha! Here it is!” (Stuart Krause)
Participants (9 of 17) confessed that not havingclear-cut answers could invoke fear in therapists,but that wisdom entails the ability to remain calmand adaptable in the face of uncertainty (4 of 17).Therapists (5 of 17) described mitigating this fear bylooking to their professional and personal ethics,morals, and values. One interviewee said, “I think
Psychotherapy Research 11
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
wisdom comes with a kind of flexibility and creativ-ity … and I can only be creative and flexible if I amconfident that I can do that ethically [and] withintegrity” (Nadine Kaslow). Participants thoughtthat having solid moral and ethical groundings gavethem a sense of direction when ambiguity arose intherapy, allowing wise therapists to be more adaptivewith their interventions.
The following principles were developed fromcluster 2:
Principle 2.1: Wise clinical practice entails exploringclients’ ambiguous understandings yet havingoptimism that new understandings and acceptancescan arise when the clients are able to wrestle withvulnerability and uncertainty within a saferelationship.
Principle 2.2: Wise clinical practice entails comingto each client with curiosity and humility—beingopen to tailoring your practice to each client.
Principle 2.3: Wise clinical practice entails knowingthat sometimes the answer may be facilitatingacceptance of experience instead of change. Accept-ance in a therapeutic relationship can help clientsdevelop self-acceptance and self-awareness, whichcan be as important as change.
Principle 2.4: Wise clinical practice is informed byempirical support in a way such that interventionsare adapted creatively and flexibly to each client.
When providing feedback, one participant suggestedthat we explicitly include mention of therapist’spersonal therapy in one of the principles. Therewere different perspectives about this idea in thedata, however. Although the participants agreed thattherapy was helpful, participants described manymethods of learning to be self-aware (e.g. travel,reading literature, multi-cultural awareness, feed-back from others) and some expressed concernsabout the idea of mandating psychotherapy. Anotherparticipant suggested a principle stating more clearly“the first and necessary and often sufficient com-ponent of all psychotherapy treatment must be thetherapist-client relationship, apart from any specifiedtreatments that are implemented later” (Paul Leo-nard, personal communication, October, 2010).This feedback was consistent with the data in thehierarchy and led to the formation of principle 2.3.
Core Category: Clinical Wisdom Is Taking theRisk Not to Know: Openly Exploring Clients’Ambiguity and Vulnerability to Intervenewithin Their Values and Context
Therapists described wise clinical practice as rootedin an in-depth exploration of clients’ idiosyncraticexperiences. Although most of the therapist–
participants were advocates of empirical research onclinical treatments, they emphasized the humilityneeded to recognize the limits of their knowledgeto be open to tailoring treatments for each client.They described the profound challenge entailed instepping into and working within clients’ internalworlds, value systems, and cultural contexts—and inparticular their experiences of uncertainty andthreat. Therapists’ experiences of personal pain andstruggle and their experience with others’ emotionsguided them to step into clients’ framework andnotice what aspects of clients’ issues were mostneeding integration and were in need of understand-ing. They repeatedly emphasized therapists’ need forself-awareness, interpersonal sensitivity, and theability to tolerate ambiguity and develop comfortwith not knowing while engaged in this exploration.In this way, clinical wisdom required therapists to beable to step into clients’ framework of values whileholding their own professional and personal valueson a metacognitive level to guide the change process.
This focus upon clients’ ambiguity and interper-sonal vulnerability helped therapists identify oppor-tunities for change by noticing material that has yetto be integrated into the client’s framework ofunderstanding (e.g. discrepancies in clients’ experi-ences or conflicting needs). Exploring these frag-mented experiences could lead to a context-sensitivebasis for increased client awareness and help them toeither change or accept aspects of themselves. Thisapproach encouraged therapists to apply techniquesfrom across orientations in a way that maximizedclients’ agency by allowing them to come to indivi-dualized insights and choices (Williams & Levitt,2007a). Obstacles to wise practice were associatedwith modes of practice that were inflexible (e.g.rigidly standardized interventions, session-limitedpractice).
In the development of this core category, wereceived specific suggestions from two participantson a prior version. The first participant requestedmore “neutral” language and “less jargony terms”and the second advised us to make the inherentprocess more explicit (John Norcross and LeslieGreenberg, personal communications, August,2010). The researchers took this information intoaccount, when refining the category presented here.The other four participants who provided feedbackon this overarching theme provided only positivefeedback and suggested no changes.
Discussion
In this study, an understanding of clinical wisdom wasdeveloped based upon the reports of therapists nomi-nated for their expertise as wise clinicians. Results of
12 H. M. Levitt and E. Piazza-Bonin
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
this analysis described clinical wisdom as predicatedupon a tolerance for ambiguity and vulnerability. Thediscussion of these findings focuses upon how the taskof seeking support for evidence-based psychotherapymight be transformed in the light of findings thatemphasize locating openings for change in relation tothese process markers and the proposed principles.
The Automatization of Psychotherapy versusProcesses Driven by Clients
This study suggested that clinical wisdom entailstaking the risk not to know. Sternberg (2004) arguedthat intelligent people are not necessarily wise andthat knowledge and wisdom are not synonyms.While an intelligent person embraces automatizationof thought within a particular context to increaseefficiency, the wise person resists automatization andtries to understand its limits across contexts. Simi-larly, the psychotherapists in this study appeared tobe concerned that an evidence-based psychotherapyparadigm which emphasizes experimentally sup-ported interventions and manualized treatmentsmight lead to automatization of psychotherapy.Although they tended to strongly support the quest forconducting research on psychotherapy approachesand processes, most of the participants expressedsome concerns that an emphasis on manualizedinterventions could obscure the focus on responsivepsychotherapy. Participants who have participatedactively in the development of ESTs and manualizedapproaches to treatment offered some of thesecautions while reflecting upon their own experiencesdoing this work. Although ESTs by definition arelinked to client improvement, empirical studies havefound that adherence to EST protocols can bedetrimental to treatment in some cases (Castonguay,Goldfried, Wiser, Raue, & Hayes, 1996) and thattreatments usually found to be effective can beproblematic when used rigidly and without regardto other important factors such as proper timing(Castonguay, Boswell, Constantino, Goldfried, &Hill, 2010).
A wise approach to psychotherapy does notnecessitate the abandonment of the quest for empir-ical support, however, or the writing and using oftherapy manuals. Some treatment developers haveexplicitly advised against therapists using their treat-ments in a rigid manner (Beck, Rush, Shaw, &Emery, 1979; Duncan & Miller, 2006). Others haveproposed ways to use manualized treatments asguides where the manual is “flexible, vibrant andalive, requiring creativity and clinical skill to beoptimally successful” (Kendall, Chu, Gifford, Hayes,& Nauta, 1998, p. 179). A promising way toconceptualize psychotherapy that directs therapists’
attention to client processes within interventions isthe “marker” driven approach to flexibly outline taskstrategies (e.g. Greenberg, Rice, & Elliot, 1993).These approaches direct therapists to attend to indi-cators that signal when the client is ready to engage inwork on a problem or task and which intervention isappropriate.
The present research suggests that clinical wisdomcan be enhanced within treatments (and treatmentmanuals) when they are developed to target markersof clients’ ambiguity and vulnerability. These pro-cesses can alert therapists to opportunities to exploreclients’ experiences that might be challenging. An in-depth exploration of these moments can provide astronger foundation for the subsequent initiation ofinterventions from across approaches to therapy asthey can provide an understanding of the values,preferences, and cultural factors that converge withinthese experiences. The principles for practicedeveloped in this paper can be used to enhanceclinical wisdom and tailor interventions to clients’experiences.
Also, wise treatment development might emphas-ize the development of the therapist. Sternberg(2004) proposed that people who are high in intel-ligence are more likely to engage in egocentrism,omniscience, omnipotence, and invulnerability. Incontrast, the participants indicated that therapistsutilizing wisdom in therapy have to become com-fortable with their own pain and relationship strug-gles. This process was described as helping therapiststo: (1) learn from their struggles so they can moresensitively guide clients as they explore their owndifficult experiences; (2) demonstrate a comfort andoptimism in the face of distress; and (3) be humblein approaching client’s experiences and understand-ing their clients’ unique experiences within theirpreferences, values, and cultures. The participantsexpressed concern that the professions’ increasingfocus on intervention strategies might eclipse thera-pists’ development of these professional processesthat help engage clients in using their own wisdom tosolve problems—especially in relation to findingssuggesting the importance of therapist effects relativeto treatment effects (e.g. Del Re et al., 2012). Thisfoundational study has produced a definition ofclinical wisdom and principles for practice thatfuture researchers can use to explore to the extentto which clinical wisdom is related to outcome.
Working Wisely with Markers of Vulnerability,Ambiguity and Acceptance
To increase the clinical utility of the findings,principles for practice have been generated fromthis analysis. It has been argued that conceptualizing
Psychotherapy Research 13
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
psychotherapy as guided by principles instead ofrules is more useful because it allows for flexibility inapplication, recognizing that therapy is a complextask that is continually in flux (Levitt, Neimeyer, &Williams, 2004). Based upon this understanding, theprinciples described herein are not to be used asprescriptive rules to be applied without regard tocontext, but as heuristics that can increase clinicians’awareness of choices to consider. Themes tied to theuse of ambiguity and vulnerability as markers in theclinically wise psychotherapy process emerged ascentral in the current study. Psychotherapy researchon these concepts are sparse, so we looked to thedescriptions of these concepts and the clinical vign-ettes provided in the interviews to shed light on howthey might be used as clinical tools across psycho-therapy orientations, fostering either client change oracceptance.
Interpersonal vulnerability. The therapist–par-ticipants described becoming comfortable with inter-personal vulnerability by acknowledging the threatsthat relationships posed in their own lives androutinely introspecting about their relationshipswith significant others and with clients. In doing so,therapists could better understand their clients’relational, emotional, cognitive, and behavioral pat-terns and appreciate the slow progression towardclarity and the importance of patience.
Moments of interpersonal vulnerability have beendefined as those “brief periods when a person risksexposing and experiencing parts of the self that arehabitually hidden from others or even from the self”(Livingston, 2003, p. 649). Livingston describedhow the therapist’s “empathic immersion in thepatient’s subjective experience” is central in allowinga client’s vulnerability to unfold and is supported byresearch that has found that empathy has a moder-ately strong positive influence on client outcome(e.g. Elliott, Bohart, Watson, & Greenberg, 2011;Truax & Mitchell, 1971). Also, therapists in thisstudy described the alliance as central for supportingvulnerability, which has strong ties to both therapyoutcome (Horvath & Symonds, 1991; Martin,Garske, & Davis, 2000) and therapy termination(Samstag, Batchelder, Muran, Safran, & Winston,1998). This research indirectly supports the idea thatvulnerability could be conceptualized as a commonfactor that is at the heart of some of these relation-ships. Further research on vulnerability itself withintherapy, however, is necessary.
Ambiguity and uncertainty. The expert thera-pists suggested that by carefully attending to thepresence of ambiguity in verbal and nonverbalcommunication, content marked by uncertainty
could be noted, signaling areas warranting furtherexploration. The use of this process marker couldallow therapists to direct interventions across orien-tations in a responsive manner. Our participantsdescribed approaching clients without preconceivednotions, instead using their own curiosity as a tool tofacilitate exploration of associated inchoate thoughtsand emotions. This finding supports the priorresearch of Jennings, Sovereign, Bottorff, Mussell,and Vye (2005) that found that master therapistswere open to complexity and ambiguity and valuedself-awareness. Similar to working with vulnerability,thorough explorations of the marker of uncertaintycan provide foundations for interventions that have abasis in the clients’ values, preferences, and cultures.For instance, exploring the meaning and experienceof uncertainty can be the basis for helping clientsresolve incongruent thoughts in a CB therapy,fragmented experiences and emotions in an emotion-focused therapy, and conflicting motives in patterns ofrelationships in a psychodynamic therapy.
The therapists described not only noticing thesignals of ambiguity in therapy but also heighteningclients’ ability to stay focused upon, contemplate,and resolve confusing issues. This progression hasbeen studied within process measure research.Honos-Webb and Stiles (2002) identified a progres-sion of increasing awareness in their Assimilation ofProblematic Experiences Scale. This scale outlines a“developmental sequence though which problematicexperiences pass on their way to being assimilated insuccessful psychotherapy” (p. 85) and has beenlinked to good therapy outcome (Laska et al., 2013;Rudkin, Llewelyn, Hardy, Stiles, & Barkham, 2007).Within the initial stages, therapists facilitate anexperiential understanding of a new awareness sothat the client can eventually clarify a problem/difficulty and gain insight. Techniques from acrosstheoretical orientations can be used to help clientsmove through these stages.
Self-acceptance. If therapists and clients are ableto navigate this terrain of ambiguity and vulnerabilityeffectively, the information they learn can help thetherapist decide upon next steps in the therapeuticprocess. The participants suggested that therapistequipped with clinical wisdom would not solelyfocus on changing clients’ emotions, behaviors,thoughts, or interpersonal dynamics but also lookfor opportunities to facilitate self-acceptance. Thisform of exploration and meaning making has beenutilized across different therapies to allow room forthe experience of troubling experiences as opposedto actively avoiding and changing them. Thesetherapies include humanist approaches broadly (e.g.Dryden & Still, 2006; Lambie & Sias, 2007),
14 H. M. Levitt and E. Piazza-Bonin
Dow
nloa
ded
by [
Uni
vers
ity o
f M
assa
chus
etts
], [
Dr.
Hei
di M
. Lev
itt]
at 1
1:00
05
Aug
ust 2
014
including emotion-focused therapy (e.g. Elliott,Watson, Goldman, & Greenberg, 2004) and exist-ential-phenomenological approaches (e.g. Bolling,1995), as well as mindfulness-based CB therapies,such as dialectical behavior therapy (Linehan, 1993),acceptance-based behavioral therapy (Roemer &Orsillo, 2005), mindfulness-based cognitive therapy(Segal, Williams, & Teasdale, 2002), and acceptanceand commitment therapy (Blackledge & Hayes,2001). All of these approaches have been structuredto help clients stay in contact with distressingthoughts and emotions. Interventions that guideclients to attend to, instead of flee from, difficultemotional states toward facilitating self-acceptancecan allow a broad range of flexibly applied solutions,supporting the application of clinical wisdom.
Limitations and Strengths
Readers should be mindful that this study focusedon doctoral-level psychotherapists who were trainedas psychologists and thought to be wise by theirpeers, and did not look at counselors with master’sdegrees, novice therapists, or psychotherapiststrained in other professions. And our sample prim-arily included American therapists who conductadult and individual therapy. Also, because the studyrelied on nomination, wise therapists who work inisolation or who are less recognized were less likelyto be nominated multiple times than wise therapistswho were well-known. Furthermore, we asked parti-cipants about their perceptions of what they do intherapy to enact wise practice, and we did not collectdata to analyze how close their descriptions matchthe interventions they actually provide in theirsessions. In addition, although the study includedtherapists influenced by all the major psychotherapyorientation approaches (i.e. psychodynamic, CB,humanistic-existential, feminist-multicultural appr‐oaches), it was not possible to include therapistsfrom each specific orientation within these groups.For instance, although two therapists describedtheir orientation as influenced by psychodynamicapproaches, the participants did not include a psy-choanalytic therapist. Future studies could focus ontherapists who specialize in group, family, and otherforms of psychotherapy, research the connectionsbetween what therapists say they do and their in-session behavior, or study therapists from withinpsychotherapy orientation approaches.
The current study used a grounded-theory ana-lysis, and therefore, the results represent our inter-pretation of the data. The researchers carefullyexamined participant’s interviews over a period ofapproximately 1 year, however, and utilized severalchecks on their interpretation, such as consensual
understandings of the data between researchers,interview checks, and participant feedback. Theresearchers also utilized a memoing process to aidin the recognition of personal biases and achievedsaturation in the analyses, suggesting that the datawere comprehensive in scope. Finally, the sampleincluded diversity in terms of gender and theoreticalorientation and so was based upon a range ofperspectives. Although we actively encourageddiversity in nominees’ race and ethnicity, the major-ity of the therapists were White. Still, we obtainedsome diversity in this realm and the analyses sug-gested that the majority and minority therapistsconverged in their understanding of wise practiceas being related to explorations of vulnerabilities andambiguities.
This research, based upon therapists from acrosspsychotherapy orientations, furthers previous worksuggesting that wisdom might be a common factoracross psychotherapy orientations (e.g. Hanna &Ottens, 1995), underlying processes of client growthand change. The participants, selected for theirperceived clinical wisdom, identified interpersonalvulnerability and ambiguity as factors within theirtherapy practice that oriented them toward explora-tion. Therapists can use the proposed principles forpractice to consider how to form interventions atthese points from across a variety of psychotherapyorientations—as these holistic processes entail emo-tional, cognitive, behavioral, and interpersonalaspects to be examined. Developing marker-drivenresponses to explore these processes can provide abasis for the engagement of clinical interventionsthat are attuned to clients’ unique experiences,contexts, and cultures (e.g. Brown, 2007). Concep-tualizing clinical wisdom as driven by explorations ofthese processes, while engaging therapists’ self-awareness and ability to tolerate uncertainty, candrive innovative clinical research on a potentialcommon factor and shed light on some of thecontributions that therapists might bring to theirsessions.
References
Baldwin, S. A., Wampold, B. E., & Imel, Z. E. (2007). Untan-gling the alliance-outcome correlation: Importance of therapistand patient variability in the alliance. Journal of Consulting andClinical Psychology, 75, 842–852. doi:10.1037/0022-006X.75.6.842
Baltes, P. B., Staudinger, U. M., Maercker, A., & Smith, J.(1995). People nominated as wise: A comparative study ofwisdom-related knowledge. Psychology and Aging, 10, 155–166.doi:10.1037/0882-7974.10.2.155
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979).Cognitivetherapy of depression. New York, NY: The Guilford Press.
Blackledge, J. T., & Hayes, S. C. (2001). Emotion regulationin acceptance and commitment therapy. Journal of Clinical
Bolling, M. Y. (1995). Acceptance and dasein. The Human-istic Psychologist, 23, 213–226. doi:10.1080/08873267.1995.9986825
Brown, L. S. (2007). Empathy, genuineness – and the dynamics ofpower: A feminist responds to Rogers. Psychotherapy: Theory,Research, Practice, Training, 44, 257–259. doi:10.1037/0033-3204.44.3.257
Castonguay, L. G., Boswell, J. F., Constantino, M. J., Goldfried,M. R., & Hill, C. E. (2010). Training implications of harmfuleffects of psychological treatments. American Psychologist, 65,34–49. doi:10.1037/a0017330
Castonguay, L. G., Goldfried, M. R., Wiser, S., Raue, P. J., &Hayes, A. M. (1996). Predicting the effect of cognitive therapyfor depression: A study of unique and common factors. Journalof Consulting and Clinical Psychology, 64, 497–504. doi:10.1037/0022-006X.64.3.497
Cohen, L. M., Sargent, M. M., & Sechrest, L. B. (1986). Use ofpsychotherapy research by professional psychologists. AmericanPsychologist, 49, 997–1000. doi:10.1037/0003-066X.49.12.997
Crits-Christoph, P., Baranackie, K., Kurcias, J., Beck, A., Carroll,K., Perry, K., … Zitrin, C. (1991). Meta-analysis of therapisteffects in psychotherapy outcome studies. PsychotherapyResearch, 1(2), 81–91. doi:10.1080/10503309112331335511
Del Re, A. C., Flückiger, C., Horvath, A. O., Symonds, D., &Wampold, B. E. (2012). Therapist effects in the therapeuticalliance–outcome relationship: A restricted-maximum likeli-hood meta-analysis. Clinical Psychology Review, 32, 642–649.doi:10.1016/j.cpr.2012.07.002
Dinger, U., Strack, M., Leichsenring, F., Wilmers, F., &Schauenburg, H. (2008). Therapist effects on outcome andalliance in inpatient psychotherapy. Journal of Clinical Psycho-logy, 64, 344–354. doi:10.1002/jclp.20443
Dryden, W. &Still, A. (2006). Historical aspects of mindfulness andself-acceptance in psychotherapy. Journal of Rational-Emotive &Cognitive-Behavior Therapy, 24(1), 3–28. doi:10.1007/s10942-006-0026-1
Duncan, B., & Miller, S. (2006). Treatment manuals do notimprove outcomes. In J. Norcross, R. Levant, & L. Beutler(Eds.), Evidence-based practices in mental health (pp.140–149).Washington, DC: APA Press.
Elliott, R., Bohart, A. C., Watson, J. C., & Greenberg, L. S.(2011). Empathy. Psychotherapy, 48(1), 43–49. doi:10.1037/a0022187
Elliott, R., Watson, J. C., Goldman, R. N., & Greenberg, L. S.(2004). Learning emotion-focused therapy: The process-experientialapproach to change. Washington, DC: American PsychologicalAssociation.
Fassinger, R. E. (2005). Wisdom in public policy. In R. J.Sternberg & J. Jordan (Eds.), A handbook of wisdom: Psycholo-gical perspectives (pp. 272–296). New York, NY: CambridgeUniversity Press.
Giorgi, A. (2009). The descriptive phenomenological method inpsychology. Pittsburgh, PA: Duquesne University Press.
Glaser, B., & Strauss, A. (1967). The discovery of grounded theory:Strategies for qualitative research. Chicago, IL: Aldine.
Goldfried, M. R., Raue, P. J., & Castonguay, L. G. (1998). Thetherapeutic focus in significant sessions of master therapists:A comparison of cognitive-behavioral and psychodynamic-interpersonal interventions. Journal of Consulting and ClinicalPsychology, 66, 803–810. doi:10.1037/0022-006X.66.5.803
Greenberg, L. S. (1986). Change process research. Journal ofConsulting and Clinical Psychology, 54, 4–9.
Greenberg, L. S., Rice, L. N., & Elliott, R. (1993). Facilitatingemotional change: The moment-by-moment process. New York,NY: Guilford Press.
Hanna, F. J., & Ottens, A. J. (1995). The role of wisdom inpsychotherapy. Journal of Psychotherapy Integration, 5, 195–219.Retrieved from http://www.apa.org/pubs/journals/int/
Hill, C. E., Knox, S., Thompson, B. J., Williams, E. N., Hess, S. A.,& Ladany, N. (2005). Consensual qualitative research: Anupdate. Journal of Counseling Psychology, 52, 196–205.doi:10.1037/0022-0167.52.2.196
Hill, C. E., Nutt-Williams, E., Heaton, K. J., Thompson, B. J., &Rhodes, R. H. (1996). Therapist retrospective recall ofimpasses in long-term therapy: A qualitative analysis. Journalof Counseling Psychology, 43, 207–217. doi:10.1037/0022-0167.43.2.207
Honos-Webb, L., & Stiles, W. B. (2002). Assimilative integrationand responsive use of the assimilation model. Journal ofPsychotherapy Integration, 12, 406–420. doi:10.1037/1053-0479.12.4.406
Horvath, A. O., & Symonds, B. D. (1991). Relation betweenworking alliance and outcome in psychotherapy: A meta-analysis. Journal of Counseling Psychology, 38(2), 139–149.doi:10.1037/0022-0167.38.2.139
Jennings, L., Soverign, A., Bottorff, N., Mussell, M. P., & Vye, C.(2005). Nine ethical values of master therapists. Journal ofMental Heath Counseling, 27, 32–47.
Kendall, P. C., Chu, B., Gifford, A., Hayes, C., & Nauta, M.(1998). Breathing life into a manual: Flexibility and creativitywith manual-based treatments. Cognitive and Behavioral Prac-tice, 5, 177–198. doi:10.1016/S1077-7229(98)80004-7
Lambie, G. W., & Sias, S. M. (2007). Striving for meaningfulnessand self-acceptance: An existential-humanistic group therapyactivity. In D. Viers (Ed.), The group therapists’ notebook:Homework, handouts, and activities for use in psychotherapy (pp.49–54). New York, NY: Haworth.
Laska, K. M., Smith, T. L., Wislocki, A. P., Minami, T., &Wampold, B. E. (2013). Uniformity of evidence-based treat-ments in practice? Therapist effects in the delivery of cognitiveprocessing therapy for PTSD. Journal of Counseling Psychology,60, 31–41. doi:10.1037/a0031294
Levitt, H. M., Neimeyer, R. A., & Williams, D. C. (2004). Rulesversus principles in psychotherapy: Implications of the quest foruniversal guidelines in the movement for empirically supportedtreatments. Journal of Contemporary Psychotherapy, 35(1), 117–129. doi:10.1007/s10879-005-0807-3
Levitt, H. M. &Williams, D. C. (2010). Facilitating client change:Principles based upon the experience of eminent psychothera-pists. Psychotherapy Research, 20, 337–352. doi:10.1080/10503300903476708
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderlinepersonality disorder. New York, NY: Guilford Press.
Livingston, M. S. (2003). Vulnerability, affect, and depth in grouppsychotherapy. Psychoanalytic Inquiry, 23, 646–677.doi:10.1080/07351692309349058
Martin, D. J., Garske, J. P., & Davis, M. K. (2000). Relation ofthe therapeutic alliance with outcome and other variables: Ameta-analytic review. Journal of Consulting & Clinical Psycho-logy, 68, 438–450. doi:10.1037/0022-006X.68.3.438
Morrow-Bradley, C., & Elliott, R. (1986). Utilization of psycho-therapy research by practicing psychotherapists. American Psy-chologist, 41, 188–197. doi:10.1037/0003-066X.41.2.188
Norcross, J. C., & Wampold, B. E. (2011). Evidence-basedtherapy relationships: Research conclusions and clinical prac-tices. Psychotherapy, 48(1), 98–102. doi:10.1037/a0022161
Rennie, D. L. (2000). Grounded theory methodology asmethodical hermeneutics: Reconciling realism and relativism.Theory and Psychology, 10, 481–501. doi:10.1177/0959354300104003
Rennie, D. L., Phillips, J. R., & Quartaro, G. K. (1988).Grounded theory: A promising approach to conceptualization
in psychology? Canadian Psychology/Psychologie canadienne,29(2), 139–150. doi:10.1037/h0079765
Roemer, L., & Orsillo, S. M. (2005). An acceptance-basedbehavior therapy for generalized anxiety disorder. In S. M.Orsillo & L. Roemer (Eds.), Acceptance and mindfulness-basedapproaches to anxiety: Conceptualization and treatment (pp. 213–240). New York, NY: Springer.
Rudkin, A., Llewelyn, S., Hardy, G., Stiles, W. B., & Barkham,M. (2007). Therapist and client processes affecting assimilationand outcome in brief psychotherapy. Psychotherapy Research,17, 613–621. doi:10.1080/10503300701216298
Samstag, L. W., Batchelder, S., Muran, J. C., Safran, J. D., &Winston, A. (1998). Predicting treatment failure from in-session interpersonal variables. Journal of Psychotherapy Practiceand Research, 5, 126–143. Retrieved from http://jppr.psychiatryonline.org
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2002).Mindfulness based cognitive therapy for depression: A new approachto preventing relapse. New York, NY: Guilford Press.
Smith, J., Staudinger, U. M., & Baltes, P. B. (1994). Occupationalsettings facilitating wisdom-related knowledge: The samplecase of clinical psychologists. Journal of Consulting and ClinicalPsychology, 62, 989–999. doi:10.1037/0022-006X.62.5.989
Staudinger, U. M., & Baltes, P. B. (1996). Interactive minds: Afacilitative setting for wisdom-related performance? Journal ofPersonality and Social Psychology, 71, 746–762. doi:10.1037/0022-3514.71.4.746
Staudinger, U. M., Maciel, A. G., Smith, J., & Baltes, P. B.(1998). What predicts wisdom-related performance? A firstlook at personality, intelligence, and facilitative experimentalcontexts. European Journal of Personality, 12(1), 1–17.doi:10.1002/(SICI)1099-0984(199801/02)12:1<1::AID-PER285>3.0.CO;2-9
Staudinger, U. M., Smith, J., & Baltes, P. B. (1992). Wisdom-related knowledge in a life review task: Age differences and the
role of professional specialization. Psychology and Aging, 7, 271–281. doi:10.1037/0882-7974.7.2.271
Sternberg, R. J. (1990). Wisdom: Its nature, origins, and develop-ment. New York, NY: Cambridge University Press
Sternberg, R. J. (1998). A balance theory of wisdom. Review ofGeneral Psychology, 2, 347–365. doi:10.1037/1089-2680.2.4.347
Sternberg, R. J. (2004). What is wisdom and how can we developit? American Academy of Political and Social Science, 591, 164–174. doi:10.1177/0002716203260097
Stricker, G. (1992). The relationship of research to clinicalpractice. American Psychologist, 47, 543–549. doi:10.1037/0003-066X.47.4.543
Truax, C. B., & Mitchell, K. M. (1971). Research on certaintherapist interpersonal skills in relation to process and out-come. In A. E. Bergin & S. L. Garfield (Eds.), Handbook ofpsychotherapy and behavior change (pp. 299–344). New York,NY: Wiley.
Wampold, B. E., & Brown, G. S. (2005). Estimating variability inoutcomes attributable to therapists: A naturalistic study ofoutcomes in managed care. Journal of Consulting and ClinicalPsychology, 73, 914–923. doi:10.1037/0022-006X.73.5.914
Williams, D. C., & Levitt, H. M. (2007a). Principles forfacilitating agency in psychotherapy. Psychotherapy Research,17(1), 66–82. doi:10.1080/10503300500469098
Williams, D. C., & Levitt, H. M. (2007b). A question of values:Developing principles for change. Journal of PsychotherapyIntegration, 17, 159–184. doi:10.1037/1053-0479.17.2.159
Zuroff, D. C., Kelly, A. C., Leybman, M. J., Blatt, S. J., &Wampold, B. E. (2010). Between-therapist and within-therap-ist differences in the quality of the therapeutic relationship:Effects on maladjustment and self-critical perfectionism. Jour-nal of Clinical Psychology, 66, 681–697.