
باليني شناسي آنزيم
Transaminases
• GOT or AST
• GPT or ALT
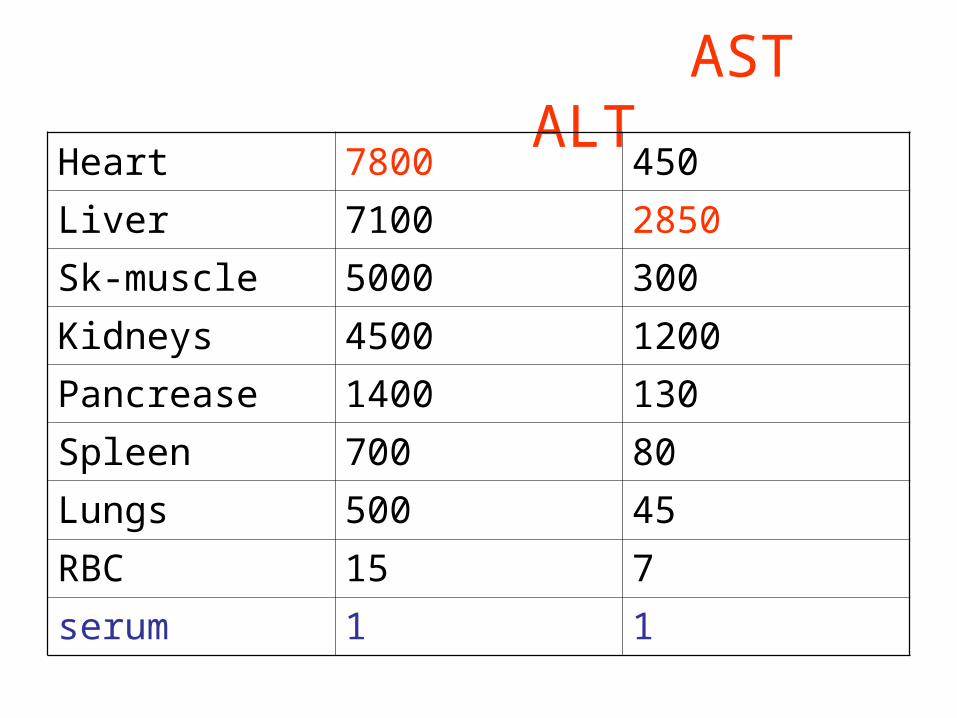
AST ALTHeart 7800 450
Liver 7100 2850
Sk-muscle 5000 300
Kidneys 4500 1200
Pancrease 1400 130
Spleen 700 80
Lungs 500 45
RBC 15 7
serum 1 1
گيري اندازه هاي روش
كالريمتريك•فتومتريك•

نرمال مقادير
adults infants Newborn
AST 8-20 9-80 47-150
ALT 10-40 7-40

CPK
• Mg coenzyme
• Inhibitors: Ca, Zn, Cu, Mn, iodoacetate
• Activators: N-acetylcysteine
• CK-MB- α2 glubolin

CK
Ck activity Ck3-MM %
Ck2-MB %
Ck1- BB %
SK-muscle
2500 98.9 1.1 0.06
brain 555 0 2.7 97.3
heart 473 78.7 20 1.3
liver ~ 1 0 0 100

Aldolase
• ALD A : FDP• ALD B : F1P• ALD C : ?• Disease of Skeletal muscle 10-50 times• Duchenne disease • Myasthenia gravis & MS • In MI 5-8 times• Pattern parallel AST• Injection of cortisone & ACTH 10-18 times
LDH
• pH optimum in L P = 8.8-9.8
• pH optimum in P L = 7.8
• Inhibitors: reagents against thiol (Hg), Borate & Oxalate, EDTA
• HBDH = LD1

ALP
• Isoenzyme: liver, bonebone, intestinal, placental, renal
• Activators: Mg, Co, Mn• Inhibotors: phosphate, borate, oxalate, cyanide• 56º & 65º• Urea inhibition• Phe inhibited intestinal & placental•

5‘-Nucleotidase (NTP)
• Localized in cytoplasmic cell membrane
• pH optimum = 6.6 – 7• In hepatobiliary disease increased 2-6 times
• increase: stone, tumor, biliary cirrhosis• In early hepatitis NTP normal or slightly elevated• In hepatobiliary disease ALP & NTP elevated similarly

Comparison of ALP & NTP
• In hepatobiliary disease ALP & NTP elevated similarly
• In Skeletal disease, late pregnancy, childhood ALP increased & NTP normal
Gamma-glutamyl transferase (GGT)
• GGT present in all cells except muscle
• Small in cytosol & large fraction in cell membrane
• GGT elevated in all liver disease
• GGT more sensitive than ALP, NTP, LAP, GOT, GPT in obstructive jaundice
• Normal: skeletal disease, children older than 1 y, pregnancy
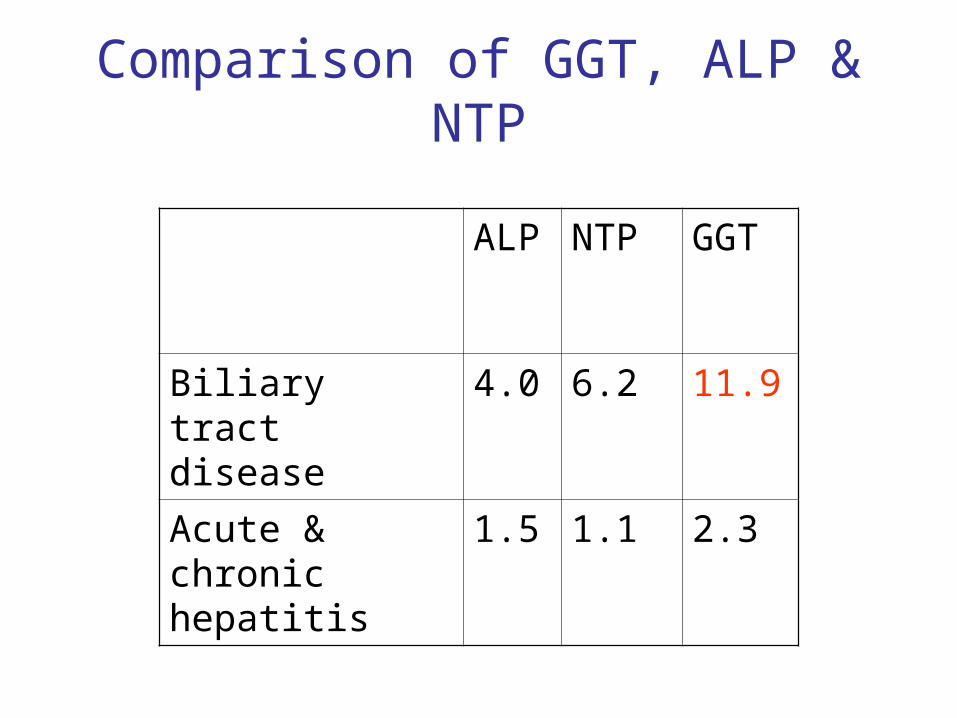
Comparison of GGT, ALP & NTP
ALP NTP GGT
Biliary tract disease
4.0 6.2 11.9
Acute & chronic hepatitis
1.5 1.1 2.3
Amylase
• Amylase hydrolased α-1,4 linkage
• Types of amylase:– Beta: plant & bacterial. Terminal reducing,
splits a maltose at a time– Alpha: animal & human. Random hydrolased
α-1,4 linkage
Human amylase
• pH optimum = 6.9 – 7
• Q10 =1.6 , up to 50° active
• Calcium metalloenzyme
• Activator ions: chloride, bromide, nitrate, phosphate
• MW= 55000 – 60000
• Electrophoresis: β & γ globulins
Types of human amylase
• P – type & S – Type (ptyalin)
• Macroamylase : usually S-type with IgA, IgG or other normal proteins
Causes of hyperamylasemia
• Pancreatic disease (P)
• Renal insufficiently (mixed)
• Mumps (s)
• Diabetic ketoacidosis (M)
• Acute alcoholism (M)
• Medicinal opiates (p)
• Heroin lung (s)
Amylase/creatinine clearance ratio (ACCR)
• ACCR (%) = (urine clearance of amylase/ urine clearance of creatinine) X 100
• ( urine amylase (U/L) X serum creatinine (mg/L) / serum amylase (U/L) X urine creatinine (mg/L) X 100
• Normal ACCR = 2 – 5 %• Acute pancreatitis > 8%• Macroamylasemia < 2%

Lipase
• Glycoprotein
• MW = 54000
• Concentration lipase in pancreas ~ 20000 serum
• alpha position carbons
• Lipase activated by NaCl
Cholinesterase
• Choline esterase I = true cholinesterase– RBC, lung, spleen, nerve endings, gray matter of the
brain
• Choline esterase II = pseudocholinesterase– Serum, Liver, pancreas, heart, white matter of the
brain
Cholinesterase
• Liver function
• Insecticide poisoning
• Normal range – 4000-12000 U/L– Level at birth = ¼ adults– In 2 month = adults
Cholinesterase
• 30-50% decrease– Acute & chronic hepatitis
• 50-70% decrease– Advanced cirrhosis & carcinoma
• Decrease slightly in pregnancy
Acid phosphatase
آنها مهمترین که دارد زیادی های ایزوآنزیماست پروستاتیک .ایزوآنزیم
پروستات بدخیم و خیم خوش اختالالت تشخیص دردارد .نقش
است تارتارات به حساس پروستاتیک .ایزوآنزیمفعالیت کاهش سبب یخچال در حتی سرم نگهداری
گردد می فسفاتاز .اسیدآزمایش انجام جهت نمونه نگهداری راه بهترین
باشد می سرم کردن اسیدی اسیدفسفاتاز
Angiotensine converting enzyme (ACE)







