

Mechanisms of visceral pain and Mechanisms of visceral pain and hyperalgesiahyperalgesiaMechanisms of visceral pain and Mechanisms of visceral pain and hyperalgesiahyperalgesia
Fernando CerveroFernando Cervero
Director, The Alan Edwards Centre for Research on PainDirector, The Alan Edwards Centre for Research on Pain
McGill University, McGill University, Montreal, CanadaMontreal, Canada
President, IASPPresident, IASP
Working Working together together for pain relief for pain relief throughout the worldthroughout the world
Visceral pain is the most frequent form of pain
Few (if any) analgesics specifically directed at visceral pain conditions
• Sociological reasons:
VISCERAL PAIN and ANALGESIA
� Patients often seen by practitioners with no primary interest in pain
treatment
• Biological reasons:
� inadequate animal models of visceral pain
� unawareness of specifics of visceral pain

Sleep and pain tend to inspire poets and philosophers
(micturition and defecation do not)
An unglamorous kind of pain
with psychoanalysts is the other way round
(Peter Nathan)
Mechanistic features of visceral Pain
• Sensory receptors / Nociceptors:
– Intensity encoders as well as high threshold (summation?)
– Chemosensitive ( ischemia sensitive)
– Sensitization + profound changes in microenvironment (secretory, motility, hormonal…)
– Many “non-sensory” receptors (CNS actions). Can they become sensory under pathological conditions ? (IBS?)

SP in a mucosal afferent ending (ureter)
Semenenko & Cervero (1992)
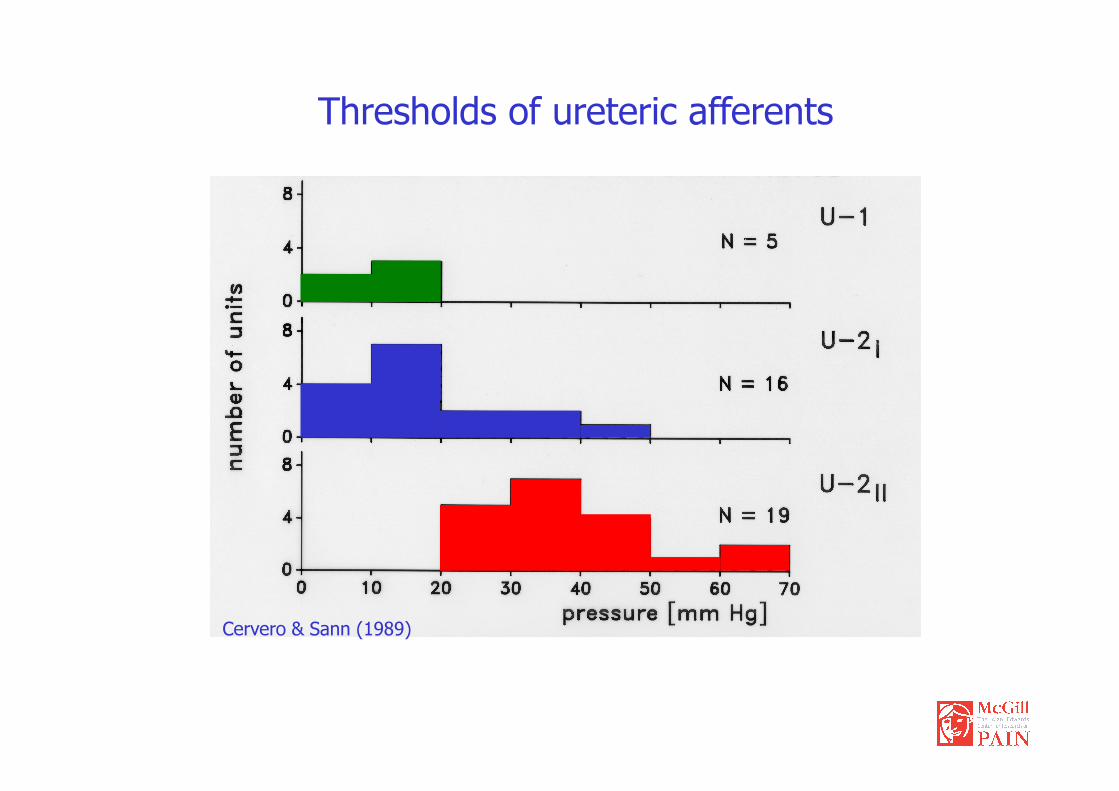
Thresholds of ureteric afferents
Cervero & Sann (1989)
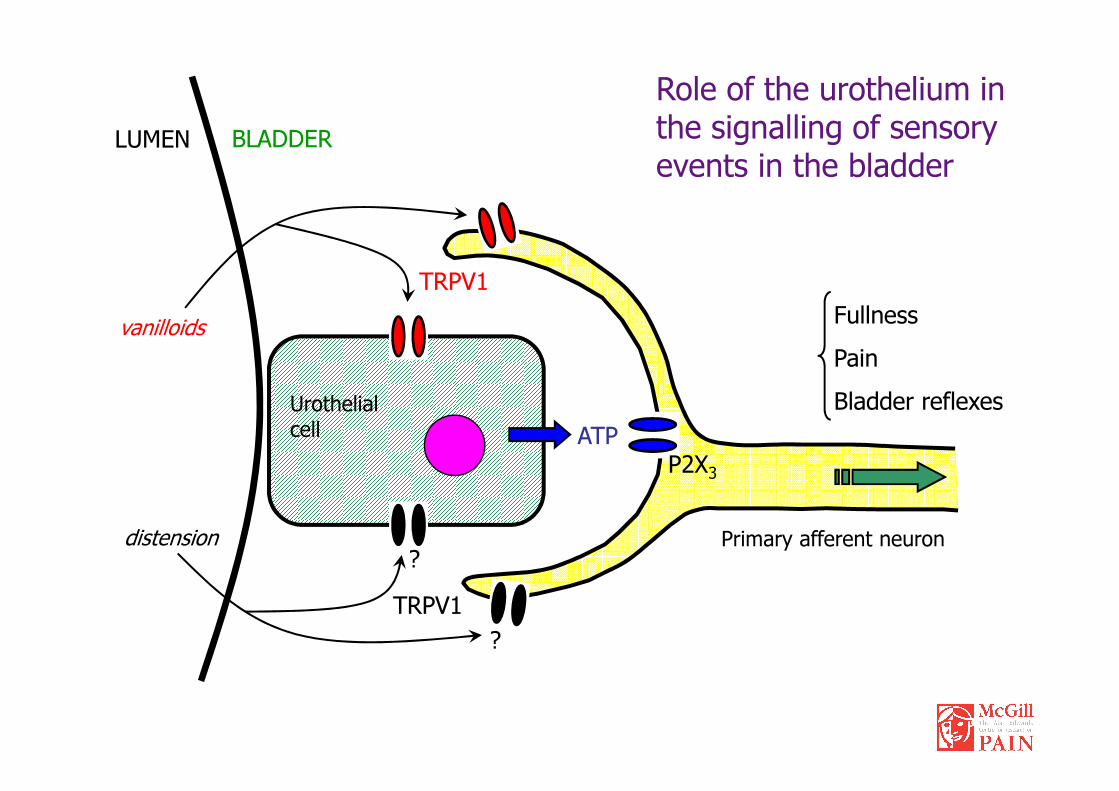
Fullness
Pain
Bladder reflexes
LUMEN BLADDER
TRPV1
vanilloids
Urothelial
Role of the urothelium in the signalling of sensory events in the bladder
Bladder reflexes
ATPP2X3
distension
TRPV1
?
?Primary afferent neuron
Urothelial cell

Effect of the presence of an experimental calculus on the motility of the rat ureter in vivo.
(Laird, Roza & Cervero 1997)

• No role in responses to acute mechanical stimuli
• No role in responses to non-neurogenic inflammatory stimuli
• Required for sustained behavioral responses to neurogenic inflammatory stimuli
Role of Nav1.8 in hyperalgesia
neurogenic inflammatory stimuli
Therefore:
• Nav1.8 contributes to spontaneous activity in sensitized nociceptors
Laird, et al. (2002) J.Neurosci. 22, 8352

CoCo--expression of CBexpression of CB11 and P2Xand P2X33 receptorsreceptors
• CB1 receptors are expressed in the urothelium and in nerve fibers of the
muscular and sub-urothelial layers• CB1 and P2X3 are co-expressed in the urothelium
CB1 receptor P2X3 receptor Merged
L L LL L L
L L L
L L L
L = lumenBar = 20µm
Negative c
ontr
ol

CBCB11 receptorreceptor TRPVTRPV11 receptorreceptor MergedMergedO
vera
ll
L L L
CoCo--expression of CBexpression of CB11 and TRPVand TRPV11 receptorsreceptors• CB1 and TRPV1 are co-expressed in umbrella cells• Some nerve fibers of the sub-urothelial and muscular layers co-express CB1
and TRPV1 receptors
L L L
Musc
ula
r la
yer
Uro
theliu
m +
Suburo
thelia
l
layer
*
*
*
*L = lumenBar = 20µm
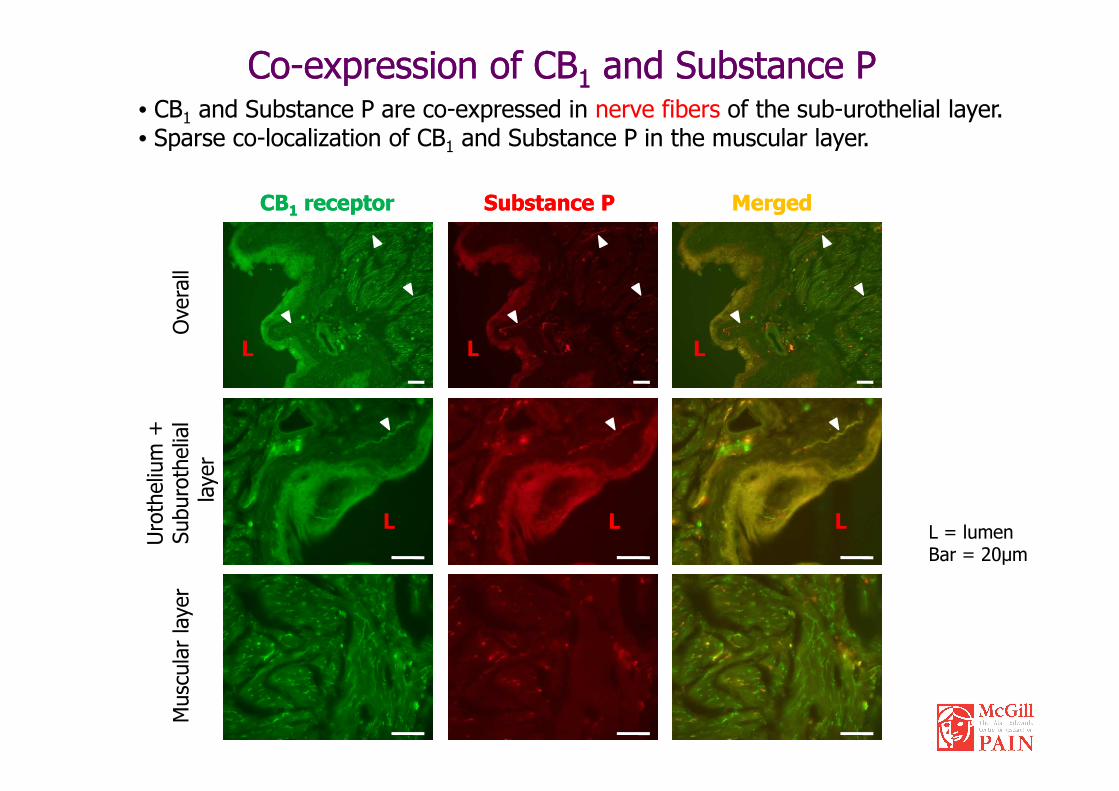
CBCB11 receptorreceptor Substance PSubstance P MergedMergedO
vera
ll
L L L
CoCo--expression of CBexpression of CB11 and Substance Pand Substance P• CB1 and Substance P are co-expressed in nerve fibers of the sub-urothelial layer.• Sparse co-localization of CB1 and Substance P in the muscular layer.
L L L
Musc
ula
r la
yer
Uro
theliu
m +
Suburo
thelia
l
layer
L = lumenBar = 20µm

Number of abdominal contractions
(during 5 minute periods)
Number of micturitions
(during 20 minute periods)
12
14
16
18
20
Saline
CYP
8
10
12
14Saline
CYP
Cyclophosphamide Cystitis: BehaviorCyclophosphamide Cystitis: Behavior
0
2
4
6
8
10
12
0
2
4
6
8
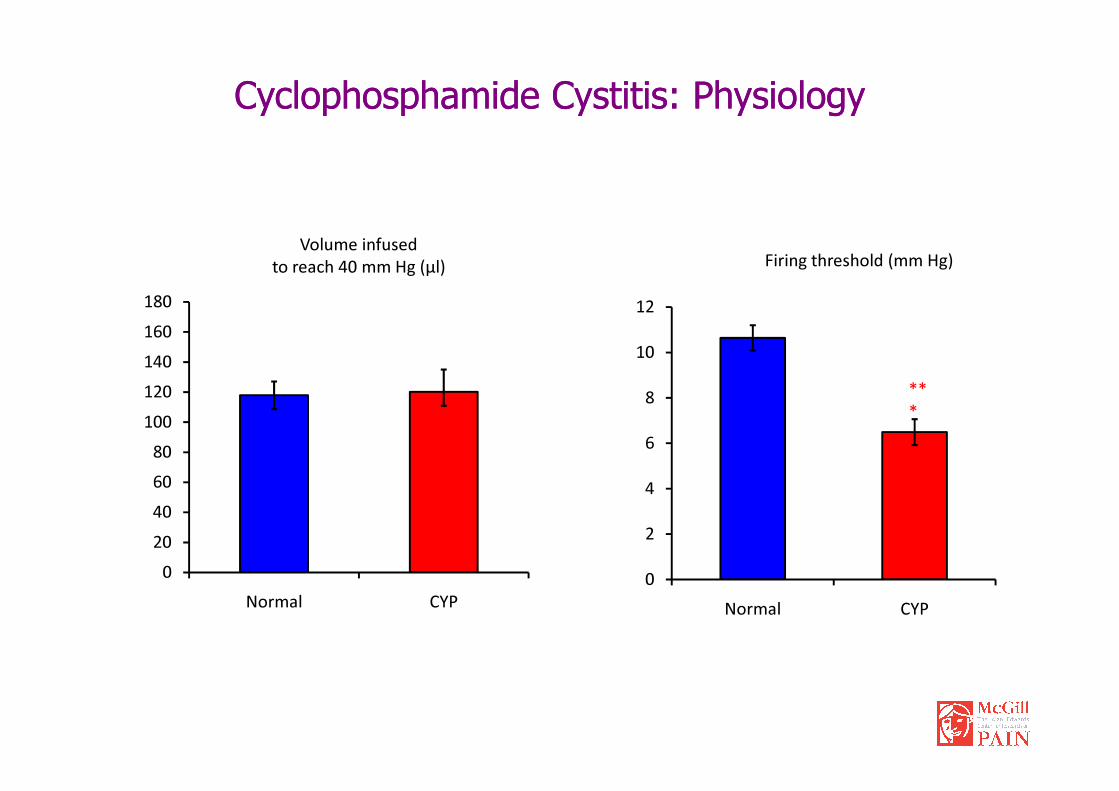
**
Firing threshold (mm Hg)
120
140
160
180
Volume infused
to reach 40 mm Hg (µl)
8
10
12
Cyclophosphamide Cystitis: PhysiologyCyclophosphamide Cystitis: Physiology
**
*
0
20
40
60
80
100
120
Normal CYP
0
2
4
6
8
Normal CYP
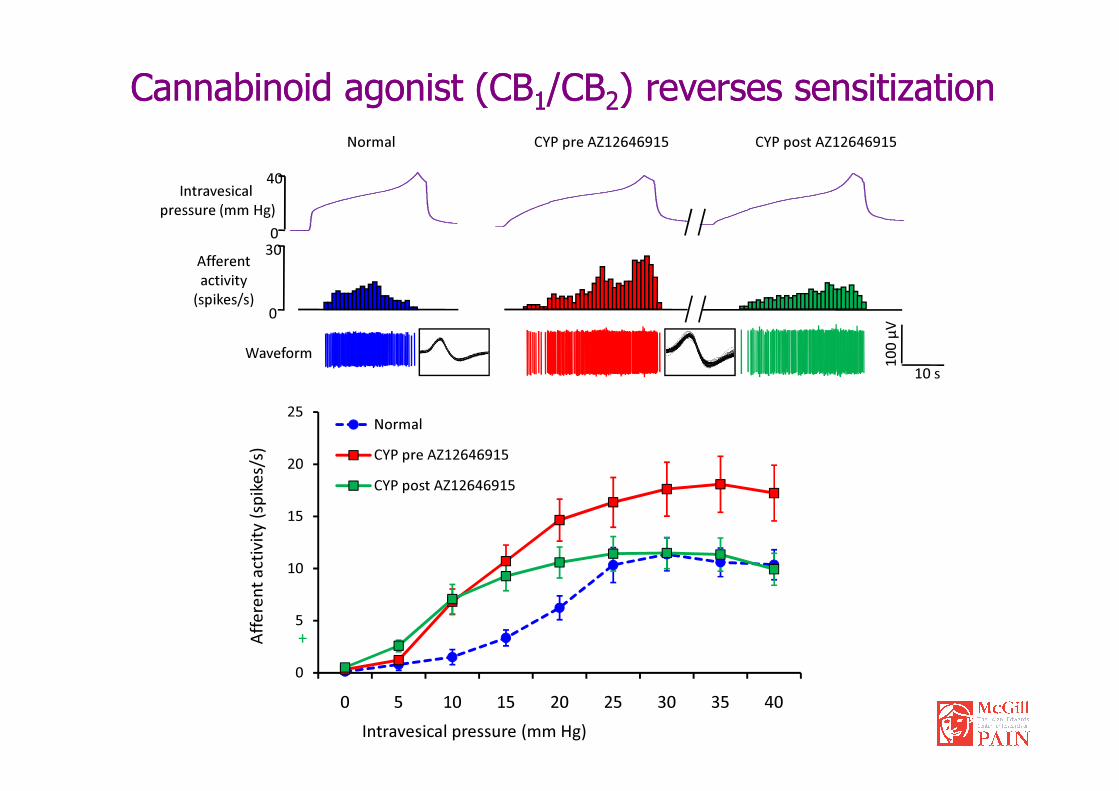
Normal CYP pre AZ12646915 CYP post AZ12646915
0
300
40Intravesical
pressure (mm Hg)
Afferent
activity
(spikes/s)
10
0 µ
V
10 s
Waveform
Cannabinoid agonist (CBCannabinoid agonist (CB11/CB/CB22) reverses sensitization) reverses sensitization
0
5
10
15
20
25
0 5 10 15 20 25 30 35 40
Normal
CYP pre AZ12646915
CYP post AZ12646915
Intravesical pressure (mm Hg)
Aff
ere
nt
act
ivit
y (
spik
es/
s)
+

0
20
40
60
80
100
0 5 10 15 20 25 30 35 40
CYP pre AZ12646915
CYP post AZ12646915
Intravesical pressure (mm Hg)
No
rma
lize
d a
ctiv
ity (
%)
(ve
rsu
s p
re-d
rug
ma
xim
al
act
ivit
y)
Sensitization reversal is mediated by CBSensitization reversal is mediated by CB11 receptorsreceptors
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 25 30 35 40
CYP pre
AZ12646915 +
AM630CYP post
AZ12646915 +
AM630
Intravesical pressure (mm Hg)
No
rma
lize
d a
ctiv
ity (
%)
(ve
rsu
s p
re-d
rug
ma
xim
al
act
ivit
y)
0
20
40
60
80
100
120
140
0 5 10 15 20 25 30 35 40
CYP pre
AZ12646915 +
AM251
CYP post
AZ12646915 +
AM251

•• Cannabinoid receptor CBCannabinoid receptor CB11 mRNA is present in the urinary bladder mRNA is present in the urinary bladder
(urothelium, and nerve fibers). CB1, TRPV1 and P2X3 (urothelium, and nerve fibers). CB1, TRPV1 and P2X3 receptors are receptors are coco--expressed.expressed.
•• Intravesical administration of a cannabinoid receptor agonist reduces the Intravesical administration of a cannabinoid receptor agonist reduces the mechanicallymechanically--evoked activity of bladder afferents. This effect is evoked activity of bladder afferents. This effect is abolished by the previous administration of a CB1 antagonist.abolished by the previous administration of a CB1 antagonist.
• Afferent activity in inflamed bladders is increased for intravesical pressures
Cannabinoids and visceral nociceptorsCannabinoids and visceral nociceptors
• Afferent activity in inflamed bladders is increased for intravesical pressures between 10 and 40 mmHg. Local treatment with a CB1/CB2
cannabinoid agonist significantly reduces afferent activity at intravesical pressures above 20 mmHg. This effect is mediated by CB1
receptors.
•• Cannabinoid CBCannabinoid CB11 receptors are implicated in the peripheral modulation of receptors are implicated in the peripheral modulation of bladder sensory information by a bladder sensory information by a direct action of cannabinoids on nociceptive afferents
Mechanistic features of visceral Pain
• CNS / central organization:
– Evidence against brief/short lived nociceptive pain (no visceral “tail flick” equivalent)
– Alarm system with widespread motor and autonomic reactions (“trip-wire” arrangement)
– fMRI data: some (relatively minor) differences in activated brain areas (mostly concerned with non-sensory aspects: emotional, affective)
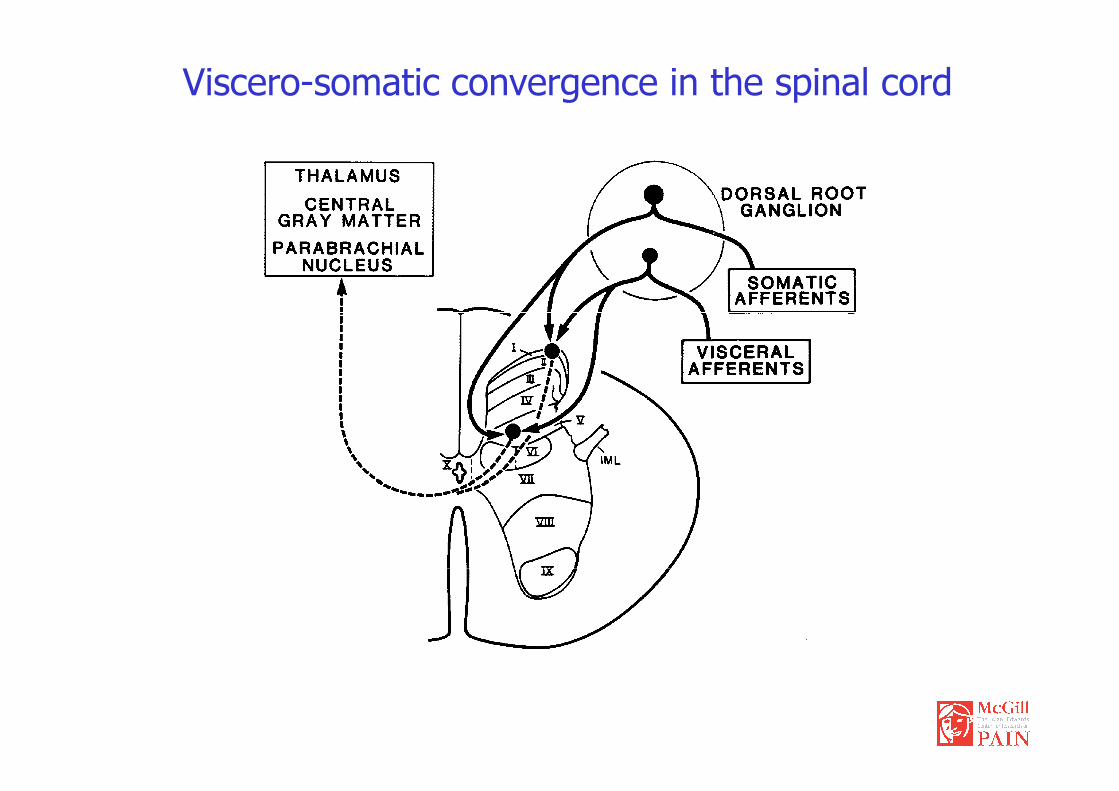
Viscero-somatic convergence in the spinal cord
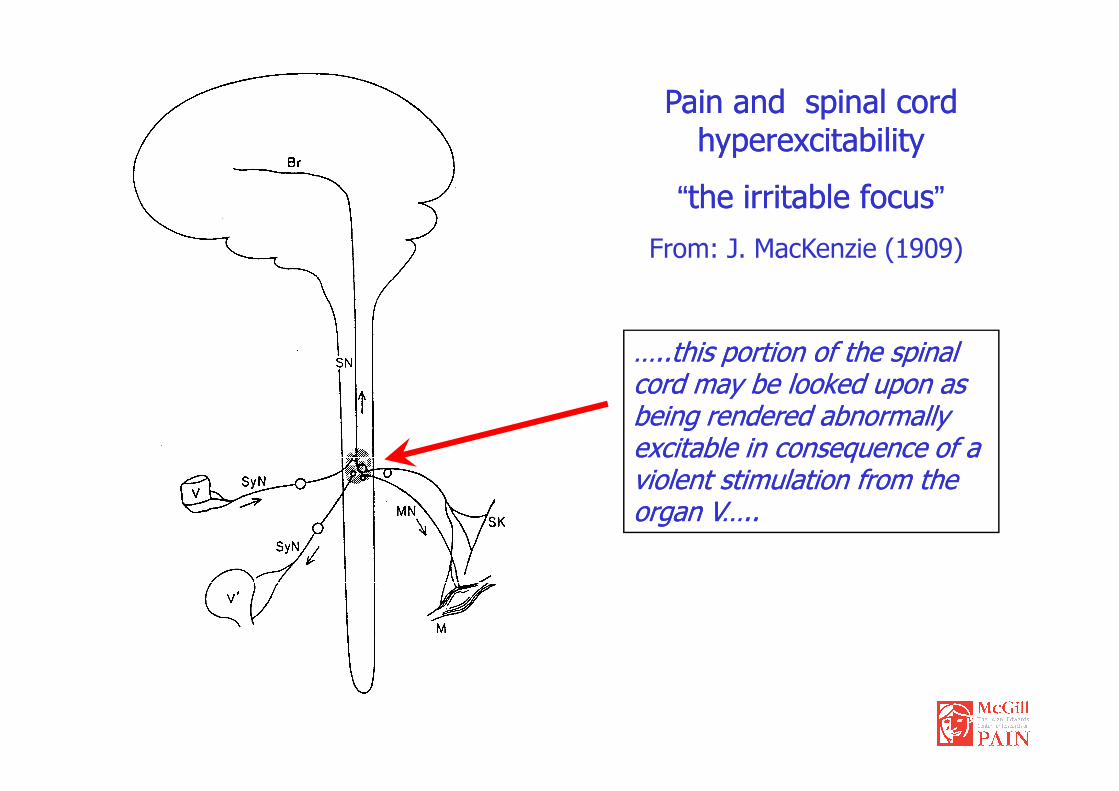
Pain and spinal cord Pain and spinal cord hyperexcitabilityhyperexcitability
““the irritable focusthe irritable focus””
From: J. MacKenzie (1909)
…..this portion of the spinal …..this portion of the spinal cord may be looked upon as cord may be looked upon as cord may be looked upon as cord may be looked upon as being rendered abnormally being rendered abnormally excitable in consequence of a excitable in consequence of a violent stimulation from the violent stimulation from the organ V…..organ V…..

CNS
How visceral pain worksHow visceral pain works
P
Aδδδδ / CPrimaryPrimaryHyperalgesiaHyperalgesia
Aββββ
Nociceptor
sensitization
1
Synaptic
strengthening by
incoming
afferent volleys
(sensitization)2
AllodyniaReferredReferredHyperalgesiaHyperalgesia Aδδδδ / C
T
Aββββ
P
Aδδδδ / CActivation of
nociceptive
neurons by LT
afferents3

Synaptic strengthening by incoming afferent volleys (sensitization)
Visceral Hyperalgesia and CNS hypersensitivity:
Role of glutamate receptor trafficking
A. Contractor, S.F.Heinemann Sci. STKE 2002, RE14 (2002)
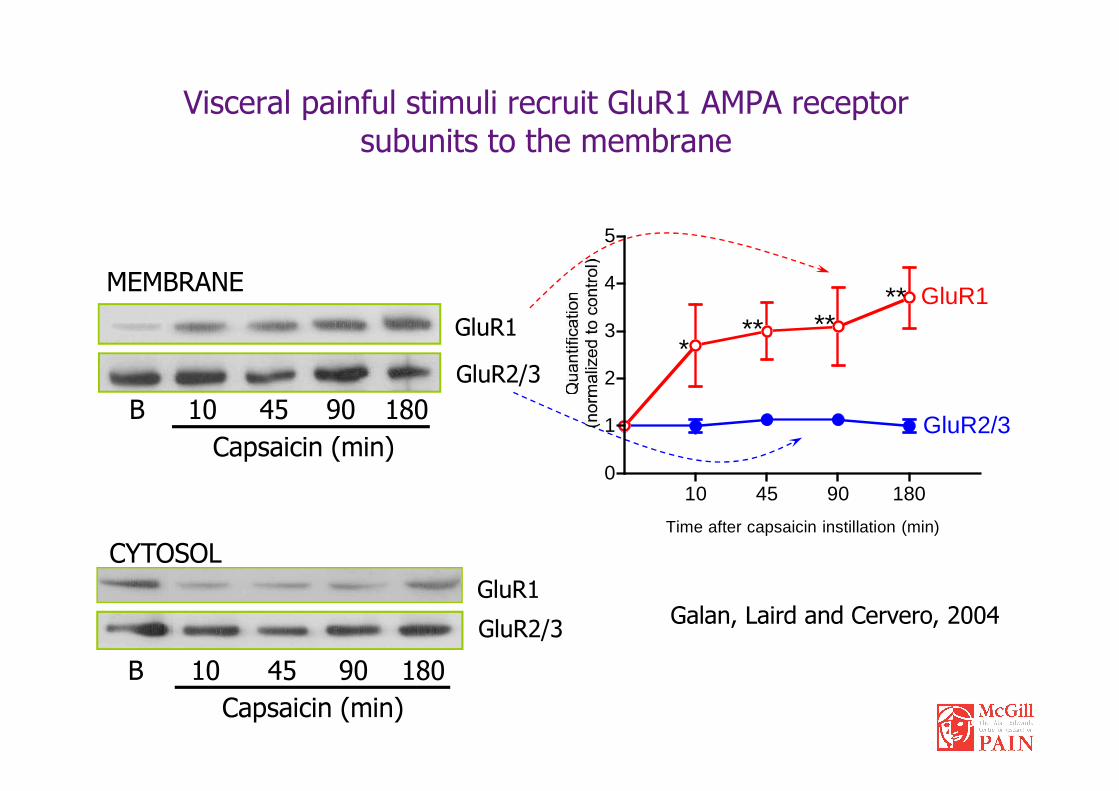
Visceral painful stimuli recruit GluR1 AMPA receptor subunits to the membrane
GluR1
B 10 45 90 180
GluR2/3
MEMBRANE
2
3
4
5
*** **
** GluR1
CYTOSOL
GluR1
B 10 45 90 180
GluR2/3
Capsaicin (min)
B 10 45 90 180
Capsaicin (min)
Galan, Laird and Cervero, 2004
10 45 90 1800
1
Time after capsaicin instillation (min)
GluR2/3

Mobilization by exocytosis?
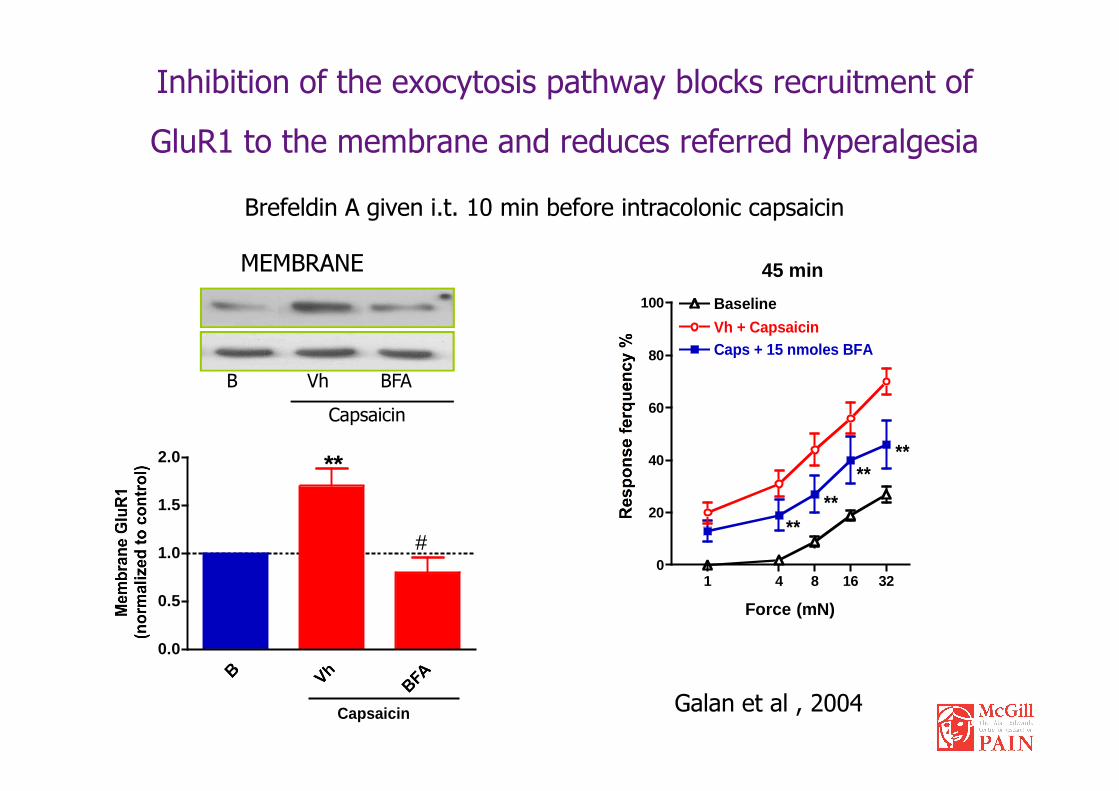
Inhibition of the exocytosis pathway blocks recruitment of
GluR1 to the membrane and reduces referred hyperalgesia
MEMBRANE
B Vh BFA
Brefeldin A given i.t. 10 min before intracolonic capsaicin
45 min
80
100 Baseline
Vh + CapsaicinCaps + 15 nmoles BFA
Capsaicin
Galan et al , 2004
1 4 8 16 320
20
40
60
****
****
Force (mN)
0.0
0.5
1.0
1.5
2.0
Capsaicin
**
#
AMPA trafficking and visceral painAMPA trafficking and visceral pain
• Acute painful stimuli induce trafficking (membrane delivery) of GluR1 AMPA receptors in vivoGluR1 AMPA receptors in vivo
• Inhibition of AMPA trafficking reduces secondary hyperalgesia induced by acute stimuli

Functional Pain
Spontaneous and persistent pain in the
absence of an apparent cause
• Frequent form of chronic pain (Irritable Bowel Syndrome, Interstitial Cystitis, (Irritable Bowel Syndrome, Interstitial Cystitis, Chronic Pelvic Pain, Fibromyalgia….)
>30% all chronic pain
• More prevalent in women (> 65%)
• Unknown mechanisms (a role for estrogen?)

Functional Pain and HyperalgesiaFunctional Pain and Hyperalgesia
Spinal Cord
Aββββ
Genetic factorsPersistent painHormonesCognitive factors
SecondarySecondaryHyperalgesiaHyperalgesia
AllodyniaAδδδδ / C
T
Aββββ
P
50
75
100
OVX
Control
Sham
req
uen
cy (%
)
50
75
100
* ** *
req
uen
cy (%
)
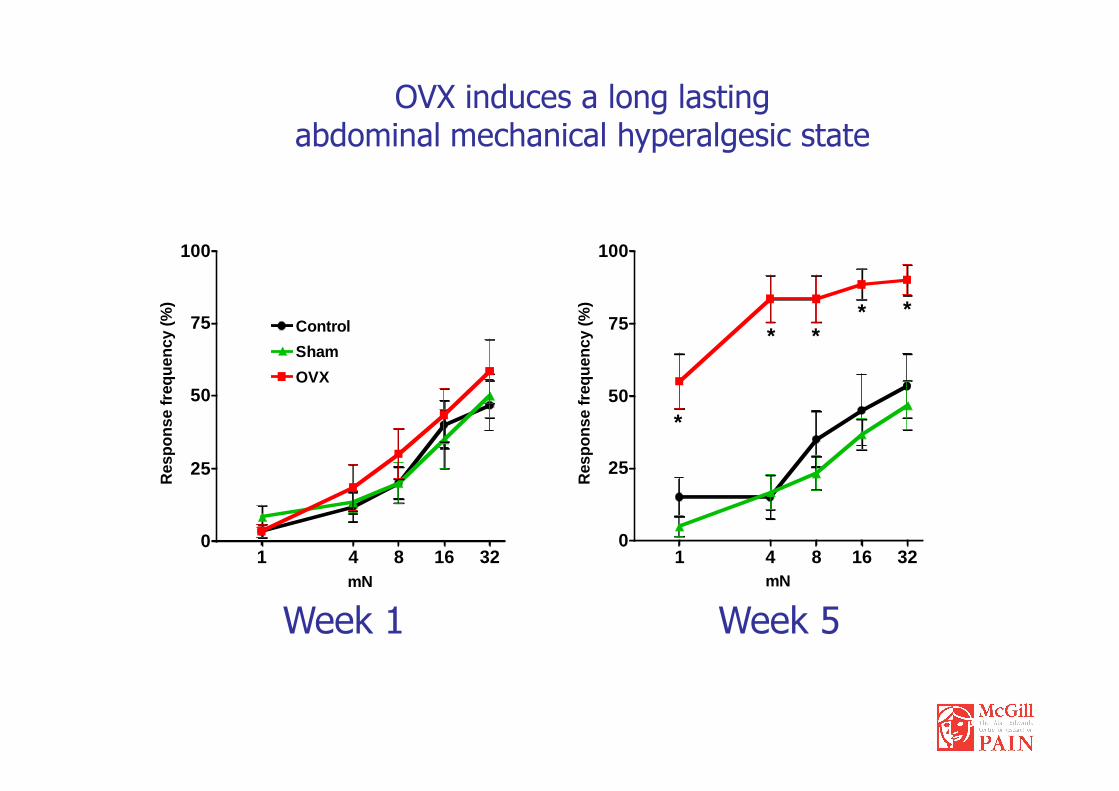
OVX induces a long lasting abdominal mechanical hyperalgesic state
1 4 8 16 320
25
50
mN
Res
po
nse
fr
1 4 8 16 320
25
50
*
mNR
esp
on
se fr
Week 1 Week 5

OVx – Preventive Hormone Replacement Therapy
25
50
75
100R
esp
on
se f
req
uen
cy (%
)
25
50
75
100
***
**
Res
po
nse
fre
qu
ency
(%)
OVX + 17β-Estradiol
OVX + placebo
Control
Sham
1 4 8 16 320
mN
R
1 4 8 16 320
mN
R
Week 1 Week 5
Prevention of abdominal mechanical hyperalgesia(pellets on week 1)

OVx – Restorative Hormone Replacement Therapy
25
50
75
100
Res
po
nse
freq
uen
cy (%
)
25
50
75
100
Res
pon
se fr
equ
ency
(%)
25
50
75
100
Res
po
nse
freq
uen
cy (%
)
OVX + 17β-Estradiol
OVX + placebo
Control
Sham
Week 1 Week 5 Week 6
Reversal of abdominal mechanical hyperalgesia(pellets on week 5)
1 4 8 16 320
mN
1 4 8 16 320
mN1 4 8 16 32
0
mN
(Sanoja and Cervero, 2008)

Activation of ERK1/2 in OVX mice (7 weeks post-surgery)
Lumbo-Sacral Spinal Cord
C S OVX
C S OVX
- p-ERK 1/2 (44/42 kDa)
- ERK 1/2 (44/42 kDa) -
GAPDH (37 kDa) -
C S OVX
*
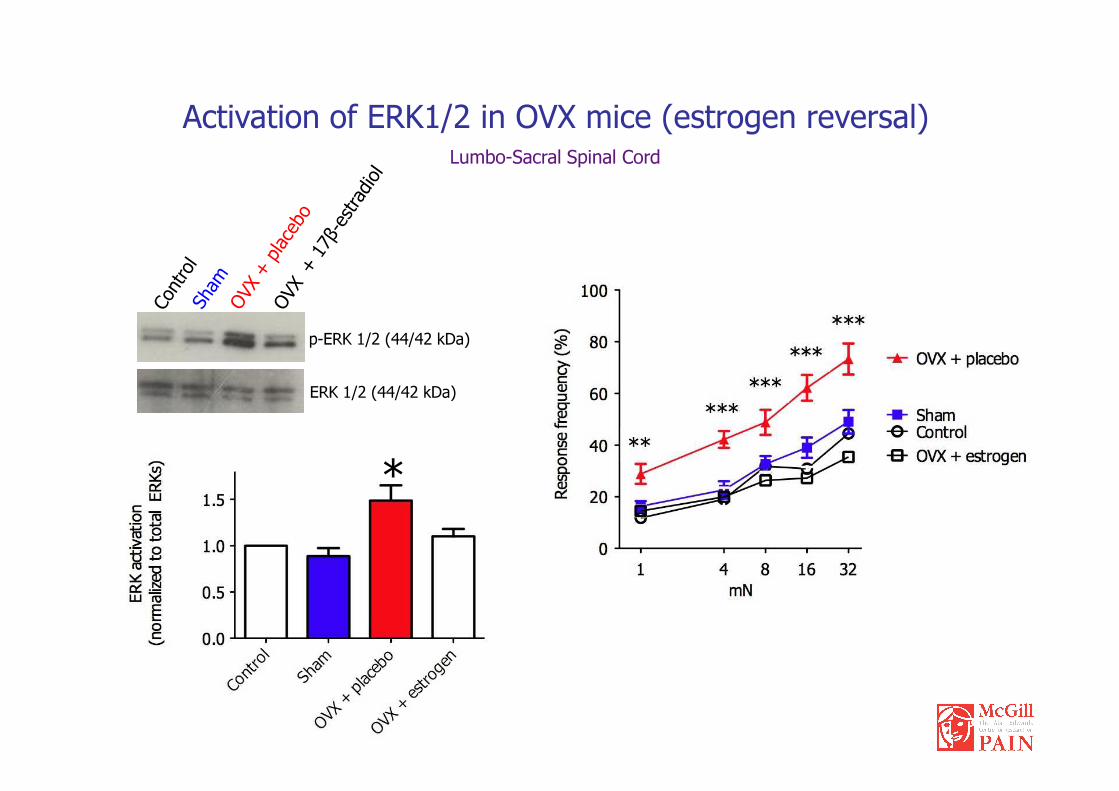
Activation of ERK1/2 in OVX mice (estrogen reversal)Lumbo-Sacral Spinal Cord
p-ERK 1/2 (44/42 kDa)
ERK 1/2 (44/42 kDa)ERK 1/2 (44/42 kDa)
*

Visceral Pain
– The most frequent form of clinically relevant pain
– Inadequately managed and poorly treated
– Mechanistically: an alarm system with widespread motor and autonomic reactions
– Periphery: close relation with visceral function (motility, secretion, epithelial transport)
– CNS: hormonal / metabolic influences – slow time course
– Animal models of visceral pain should reproduce a functional process

Whereas acute symptomatic pain serve
the useful purpose of warning, chronic
pain is a malefic force which imposes
severe emotional, physical and economic
stresses on the patient
John J. Bonica
John J. John J. BonicaBonica (1917(1917--1994) 1994)
What to do to relieve pain?
- Increase our knowledge: Study pain
- Apply our knowledge: Treat pain
- Create a communication vehicle
between those who study and
John J. John J. BonicaBonica (1917(1917--1994) 1994)
between those who study and
those who treat pain

Working Working together together for pain relief for pain relief throughout the worldthroughout the world
www.IASP-pain.org







