

6/4/10
1
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics University of California, San Francisco
Quantify increased lifetime risk of cancer attributable to head CT’s in kids
Understand the current state of evidence regarding prediction of intracranial injury in kids with minor head trauma
Develop a strategy for selective imaging of infants and children with minor head trauma
Review available guidelines for back to play after minor head trauma
Horus is a 9 month old boy brought in by babysitter after the dog knocked him over in his high chair
She heard a crash and found Horus on the tile floor “stunned”, started to cry immediately
She called mom at work, fed him 15 minutes later and he spit up a small amount
A nurse in the ED recommended she bring him in

6/4/10
2
VS in normal range for age Somewhat fussy but consolable Smiles, drinks from a bottle Neuro exam: non-‐focal 1X2 cm hematoma/abrasion on forehead
A. Head CT scan B. Plain skull films C. Head Ultrasound D. Observation in ED for 4-‐6 hours E. Discharge with reliable caregiver
Intracranial injury (ICI) occurs in ~3%-‐7% of children <18 with apparently minor HT
The minority (<1%) are clinically significant Goals of selective imaging strategies:
Identify kids with clinically significant ICI Minimize unnecessary radiation, sedation

6/4/10
3
Intracranial injury (ICI) occurs in ~3%-‐7% of children <18 with apparently minor HT
The minority (<1%) are clinically significant Goals of selective imaging strategies:
Identify kids with clinically significant ICI Minimize unnecessary radiation, sedation
A. 10 CXR’s B. 100 CXR’s C. 200 CXR’s D. 500 CXR’s
A. 10 CXR’s B. 100 CXR’s C. 200 CXR’s D. 500 CXR’s
The DOG scan has considerably less radiation….

6/4/10
4
Ionizing radiation quantified in Grays or Sieverts Gray = unit of absorbed radiation/mass = j/kg Sievert = unit of biological effect ▪ Sv =Gy X Q (Q = 1 for Xrays)
Background rates of radiation: 3 mSv/year (1-‐10 depending on region of US)
Single Head CT (adult) 10-‐14 mSv Many centers do not use reduced doses for kids
Standard-dose (220-mA) head CT
(Abdelhalim, 2009)
Low-dose (80-mA) head CT

6/4/10
5
Estimated % of cancers in the US attributable to CT scan radiation: 0.4-‐>2%
Up to 20 % of these are in individuals exposed as kids!
Increase in lifetime cancer mortality rates attributable to head CT’s in kids: 1 year old child: 0.07% (1/1500) Kids <15: 600,000 abdominal/head CT scans/year ▪ 500 kids will die of cancer (0.35% increase over baseline)
While difficult to quantify, radiation from CT scans causes a small increase in the lifetime risk of cancer
The increase in risk is Dose-‐dependent Greatest in the youngest infants
Our goal: Identify children with minor head trauma who can be safely managed without head CT…

6/4/10
6
Population of interest: GCS>14, relatively minor mechanism
Brief LOC no longer considered predictive Previous guidelines suggest a “lower threshold” for imaging children <2 Selective imaging more important in infants Risks of sedation, radiation
Only study large enough to derive and validate rules in kids <2 as well as 2-‐18 Kids < 2: NPV 100% Kids 2-‐18: NPV 99.5%
6/4/10
7
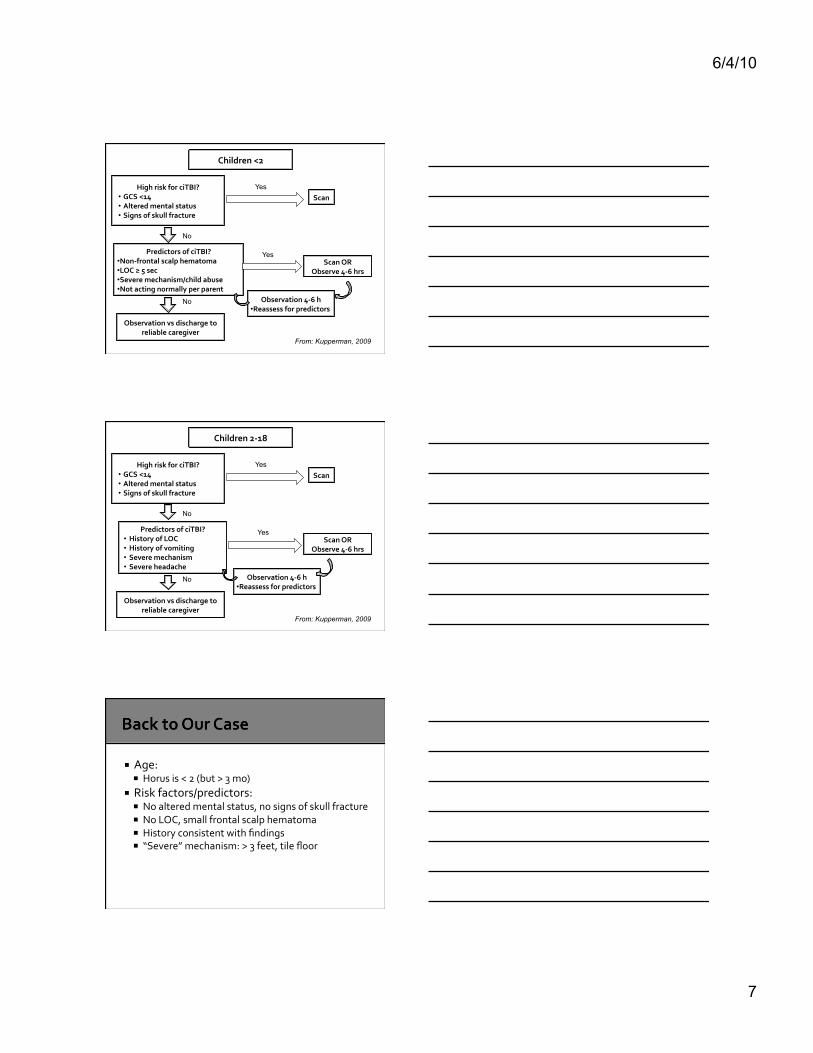
Children <2
Scan
Scan OR Observe 4-‐6 hrs
No
No
No
Yes
Yes
High risk for ciTBI? • GCS <14 • Altered mental status • Signs of skull fracture
Predictors of ciTBI? • Non-‐frontal scalp hematoma • LOC ≥ 5 sec • Severe mechanism/child abuse • Not acting normally per parent
Observation vs discharge to reliable caregiver
From: Kupperman, 2009
Observation 4-‐6 h • Reassess for predictors
Children 2-‐18
Scan
Scan OR Observe 4-‐6 hrs
No
No
No
Yes
Yes
High risk for ciTBI? • GCS <14 • Altered mental status • Signs of skull fracture
Predictors of ciTBI? • History of LOC • History of vomiting • Severe mechanism • Severe headache
Observation vs discharge to reliable caregiver
From: Kupperman, 2009
Observation 4-‐6 h • Reassess for predictors
Age: Horus is < 2 (but > 3 mo)
Risk factors/predictors: No altered mental status, no signs of skull fracture No LOC, small frontal scalp hematoma History consistent with findings “Severe” mechanism: > 3 feet, tile floor

6/4/10
8
Age: Horus is < 2 (but > 3 mo)
Risk factors/predictors: No altered mental status, no signs of skull fracture No LOC, small frontal scalp hematoma History consistent with findings “Severe” mechanism: > 3 feet, tile floor
A. CT scan B. Plain skull films C. Head Ultrasound D. Observation for 4-‐6 hours E. Discharge if caregiver is reliable
Reliable caregiver Instructions understood No other indications for admission Normal neuro exam and mental status No suspicion for abuse or neglect

6/4/10
9
Isis, a 16 yo girl, strikes another player in the head going for a ball
She has brief LOC on the field, and sits out the game, feeling “dizzy”
Her father brings her to your office the next day, asking if she can play in the championship next week.
She had a headache last night, but is now asymptomatic
A. If asymptomatic, she can return to play immediately
B. She should wear a helmet to protect her from future concussions
C. She can return to play in graduated way, if she remains asymptomatic
D. She should not return to play this season

6/4/10
10
Risk of chronic sequelae Headaches, vertigo, epilepsy, neurocognitive impairment
Risk of recurrent /severe TBI Higher after first concussion ?”Second impact syndrome”
Goals: Prevent further injury/neurologic sequelae
No prospectively validated practice guidelines
General consensus seems to agree on: NO athlete should return to play until asymptomatic
Younger athletes should be managed more conservatively
Complex concussion demands special consideration
No prospectively validated practice guidelines
General consensus seems to agree on: NO athlete should return to play until asymptomatic
Younger athletes should be managed more conservatively
Complex concussion demands special consideration

6/4/10
11
A 6-‐day graded approach (Zurich Consensus) 1 Complete rest 2 Light aerobic exercise 3 Sport-‐specific exercise 4 Non-‐contact training drills 5 Full contact practice 6 Game play
Cancer risks from CT scans are dose and age-‐dependent Strategies: reduce dose of radiation, identify pts who can be safely managed without a scan
The Kupperman Decision Rule has been prospectively validated, and has a very high negative predictive value Consider observation vs scan in patients who are low risk, but have some predictors of TBI

6/4/10
12
For simple concussion, consensus supports a graded return to play when asymptomatic
For complex (prolonged or severe symptoms) or recurrent concussion More conservative management, consider no return to play this season
Consider TBI specialist referral
Isis Mother of Horus Protective goddess Associated with thrones, as her lap was Horus’ first “throne”
Horus God of the sky, and protective ruler of Egypt
His eye is the symbol of protection
5 8 26







