

2017 Spring Fling
Opioids: Do’s and Don'ts
cc: e_monk - https://www.flickr.com/photos/10676369@N07
"Among the remedies which it has pleased Almighty God to give to man to relieve his sufferings, none is so universal and so efficacious as opium."
-Thomas Sydenham (1624-1689)
cc: Anne Worner - https://www.flickr.com/photos/28652129@N06
Objectives• Discuss the basic pharmacology of opioids• Discuss the epidemiology of illicit opioid use• Describe common treatment modalities• Describe treatment variations for uncommon
presentations• Describe common pitfalls in the emergency care of
opioid overdoses
cc: alexdecarvalho - https://www.flickr.com/photos/51035823282@N01
• Steve Cole
• Ada County Paramedics for 18 years
• EMS for 25 (and counting) years
Disclaimer• I have no financial conflicts of interest
• This presentation is not a substitute for basic clinical judgment.
• Follow your protocols!
cc: karen_neoh - https://www.flickr.com/photos/50266725@N02
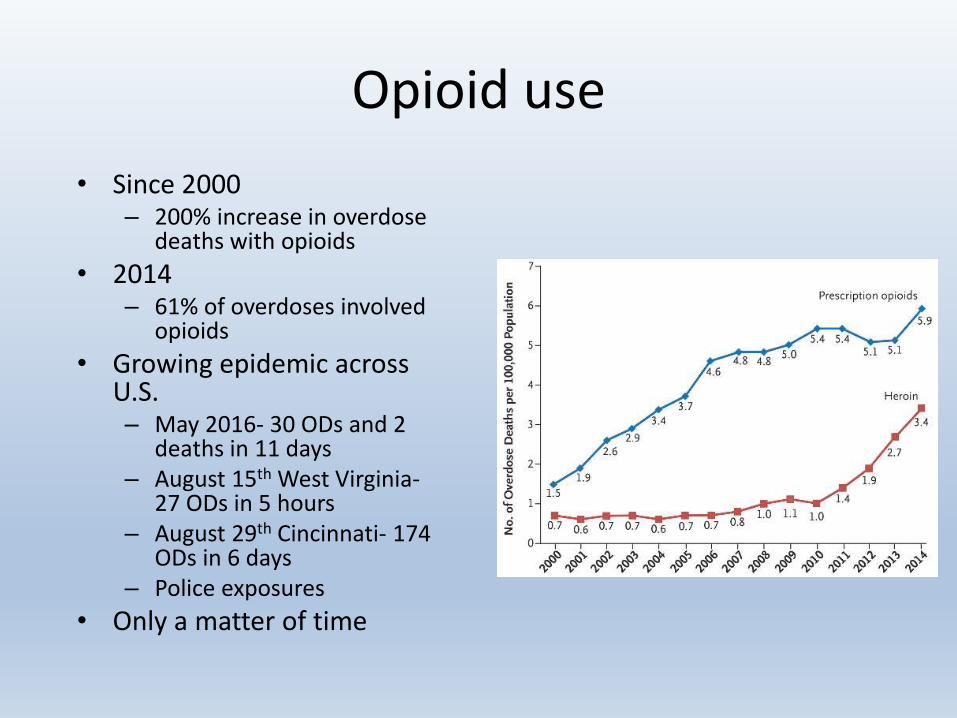
Opioid use
• Since 2000 – 200% increase in overdose
deaths with opioids
• 2014– 61% of overdoses involved
opioids
• Growing epidemic across U.S.– May 2016- 30 ODs and 2
deaths in 11 days– August 15th West Virginia-
27 ODs in 5 hours– August 29th Cincinnati- 174
ODs in 6 days– Police exposures
• Only a matter of time
Before we get started…..
• Doing your own research…
• Knowing where to look
• Staying up to date
Educating Yourself….

EMS Textbooks SUCK!

WWW.EROWID.ORG
Opioids: What are we talking about?
• Illicit vs. Legal?
• Synthetic vs. naturally occurring opioids?
• Clinical vs Recreational use?
What is Diversion?
• Diversion is the use of prescribed substances (Opioids are just one drug class that is often diverted) for illicit or recreational use.
• How are Drugs Diverted?– Hospice/Home Health Care
– Visitors
– Family
– Health Care providers
– Public Safety Workers
– Professional Patients.
The Opium Poppy•Use/Abuse goes back At least to 4000 BC
•The poppy contains numerous opioid alkaloids
•The most common Opioid Alkaloids are:
• Morphine (1-10%)
• Codeine
• Thebaine
• Oripavine
cc: fatboyke (Luc) - https://www.flickr.com/photos/8264376@N03

Opioid Receptors
Source: http://www.iuphar-db.org/DATABASE/FamilyIntroductionForward?familyId=50

What is a Toxidrome?
What is a Toxidrome?syn·drome (ˈsinˌdrōm/)
noun
1. a group of symptoms that consistently occur together or a condition characterized by a set of associated symptoms.
tox·i·drome(ˈtäksiˌdrōm/)
noun
1. a group of signs and symptoms constituting the basis for a diagnosis of poisoning.
In other words: A toxidrome is a “syndrome” that specifically relates to a specific toxinBe cautious, many syndromes/toxidromes are subtle and overlap their symptoms. Thorough assessment is essential

Opioid Toxidrome
• The Opiate Toxidrome consists of:– Altered mental status – Miosis*– Unresponsiveness – Shallow respirations – Slow respiratory rate – Decreased bowel sounds – Hypothermia– Hypotension*
• * these symptoms are very subjective, and may not be present in polypharmacy overdoses.
KEY POINT:
Miosis and Hypotension are not definitive for ruling in or
ruling out a opioid overdose.

Methods of
use:
• Shooting
• Skin Popping
• Muscle Popping
• Chasing the dragon
• Freebasing
• Plugging and Shelving
• Dirty Hit
• Tea
– With Grapefruit Juice
• Tincture
– Laudanum and Perigoric
So why do people overdose?
• IV opioid use
• Poly-pharmacy Overdose
• Returning to opioid use from abstinence
– Jail?
– Detox?
• The Weekend Warrior
• Using opioids alone
• New supply of Drug

Types of Opioids
cc: karen_neoh - https://www.flickr.com/photos/50266725@N02
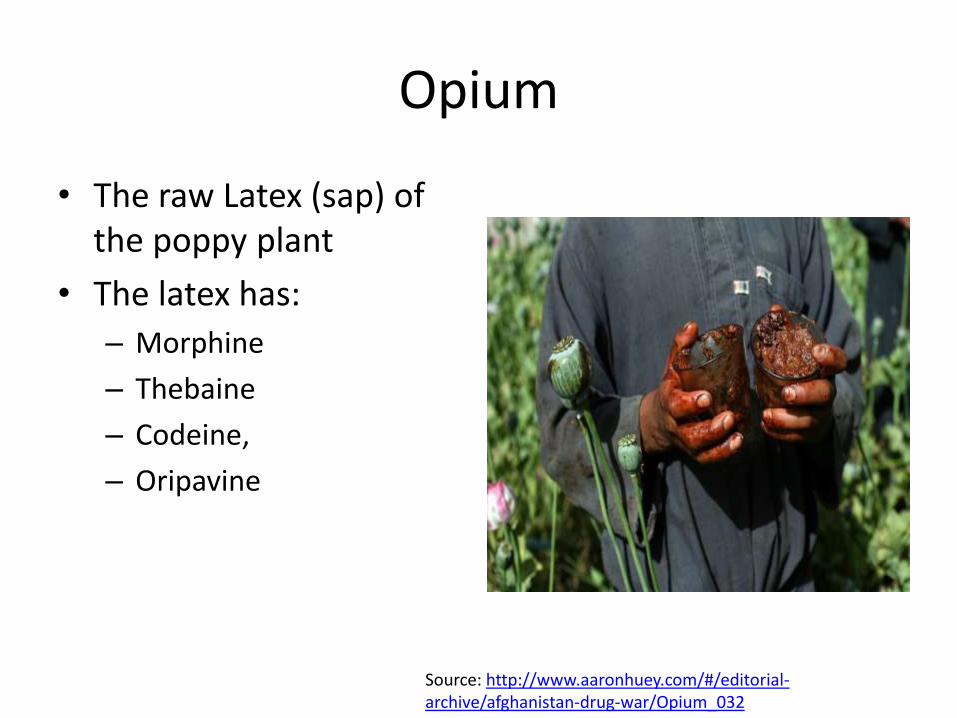
Opium
• The raw Latex (sap) of the poppy plant
• The latex has:
– Morphine
– Thebaine
– Codeine,
– Oripavine
Source: http://www.aaronhuey.com/#/editorial-archive/afghanistan-drug-war/Opium_032
Morphine •Naturally occurring in raw opium
• First isolated in 1804
• First IV opioid in 1857
•The gold standard by which other opioids are judged
•Potent Respiratory / CNS depressant
•“Equipotent” euphoria to Heroin, though slower onset.
•Intermediate Duration (3-6 hours)
•Many “ER” (extended release) formulations
cc: Dirty Bunny - https://www.flickr.com/photos/34728046@N00
Codeine, Hydrocodone•Codeine naturally occurs in the poppy plant
•Hydrocodone is a semi-synthetic derivative of codeine. Often taken as a oral tablet or an elixir•Often co-ingested
with an NSAID (such as APAP, Motrin or ASA)
•Norco, Vicodin
cc: compujeramey - https://www.flickr.com/photos/37171504@N00

Sizzurp(Codeine, ETOH, and Phenergan mixes
Heroin• Black Tar• China White• Speed Ball• Homicide, Buick,
super Buick, twilight sleep

Old verses New


By Todd Huffman from Phoenix, AZ - Needle Exchange, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=5170947
Oxycontin/Oxycodone•Oxycodone is another semi-synthetic
•Derived from Thebaine
•Roughly twice as potent as Morphine
•Also More potent than Hydrocodone
•Most often available in Tablet form• Like Hydrocodone, often co-ingested with an NSAID (such as APAP, Morin or
ASA)
• Percocet
•Extended release versions known as Oxycodone • “Oxy”
• May be crushed, diluted, and injected like traditional heroin
Methadone•Synthetic opioid
•Comparable with Oxycontin and Dilaudid.
•Longer acting than most other Analgesic• Typically 4-8 hours
•Like other prescription opiates, WIDELY Available
•One study showed of 18 methadone related deaths:• Less than ½ were prescribed methadone
• Only three were prescribed methadone through a methadone tx program

Imodium
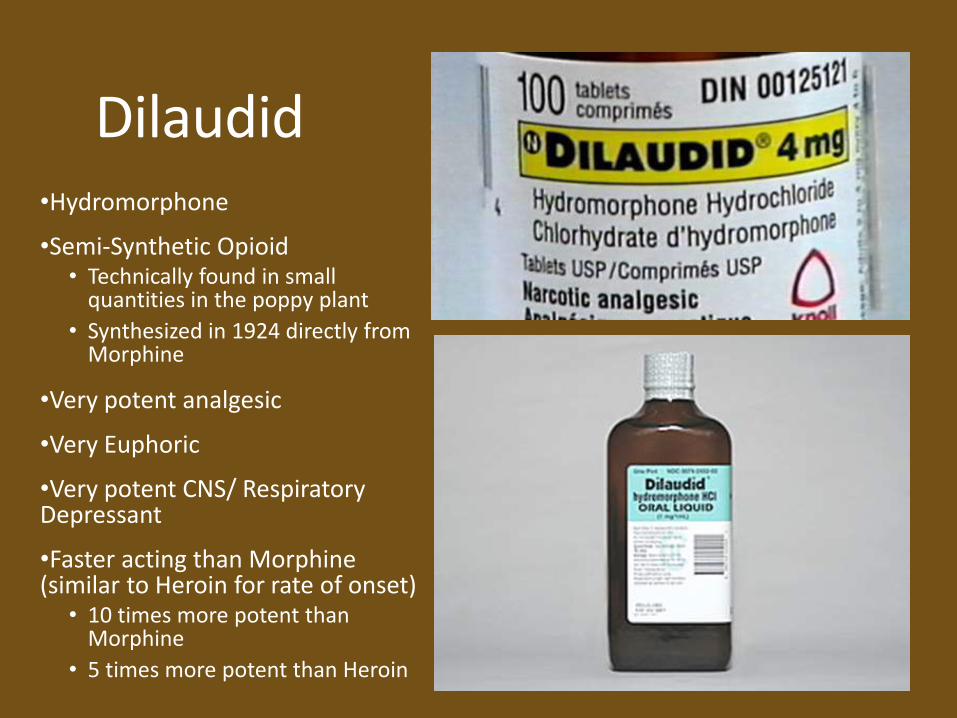
Dilaudid•Hydromorphone
•Semi-Synthetic Opioid• Technically found in small
quantities in the poppy plant
• Synthesized in 1924 directly from Morphine
•Very potent analgesic
•Very Euphoric
•Very potent CNS/ Respiratory Depressant
•Faster acting than Morphine (similar to Heroin for rate of onset)
• 10 times more potent than Morphine
• 5 times more potent than Heroin

Fentanyl Citrate
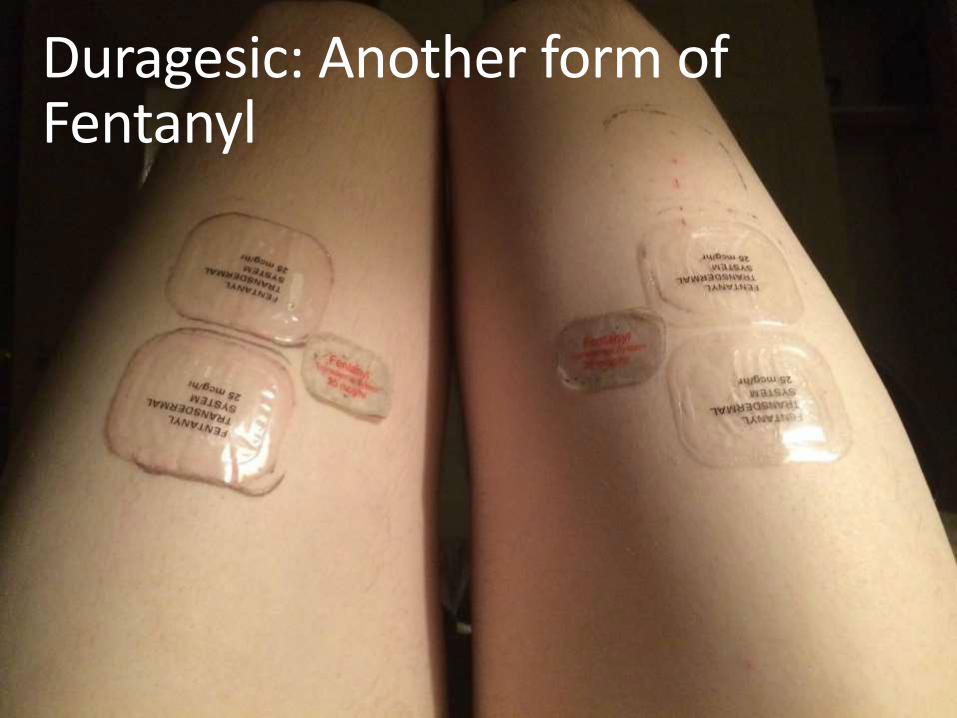
Duragesic: Another form of Fentanyl

Poly-Opioid Mixes
• Increasingly common practice of mixing one type of opioid (typically Heroin) with another , more potent opioid.
– This increases the “potency” (increasing profit) without increasing the “purity” (i.e. the cost)
– Retains the eurphoric effects of some opioids while getting the heavier nod of others.
Photo credit: NPR.orgTamika Moore/AL.com/Landov

Feb 8th to 9th , 2017
* Normal is 22 opioid a day in this system



Treatment of Opioid Overdose’s
REMEMBER: Opioid overdoses are AMS calls first, opioid overdoses last
A - alcohol, alcohol withdrawal, and anoxiaE -epilepsy and other neurological disordersI - insulin (Hyper or Hypo-glycemia)O - overdose (Poly-pharmacy?)U - uremia, underdose of current medications.T - traumaI - infectionP - psychiatricS - stroke, shock states
cc: Wade Morgen - https://www.flickr.com/photos/31845391@N04
In order to treat an opioid patient we need to understand HOW opioids kill…
Primary Causes of Mortality:• Respiratory failure
• Airway Failure
Secondary Causes of Mortality• Aspiration
• (Rarely) hypothermia and hypotension
• Situational Factors
• MIS-TREATMENT by providers
cc: Peter O'Connor aka anemoneprojectors - https://www.flickr.com/photos/58414938@N00
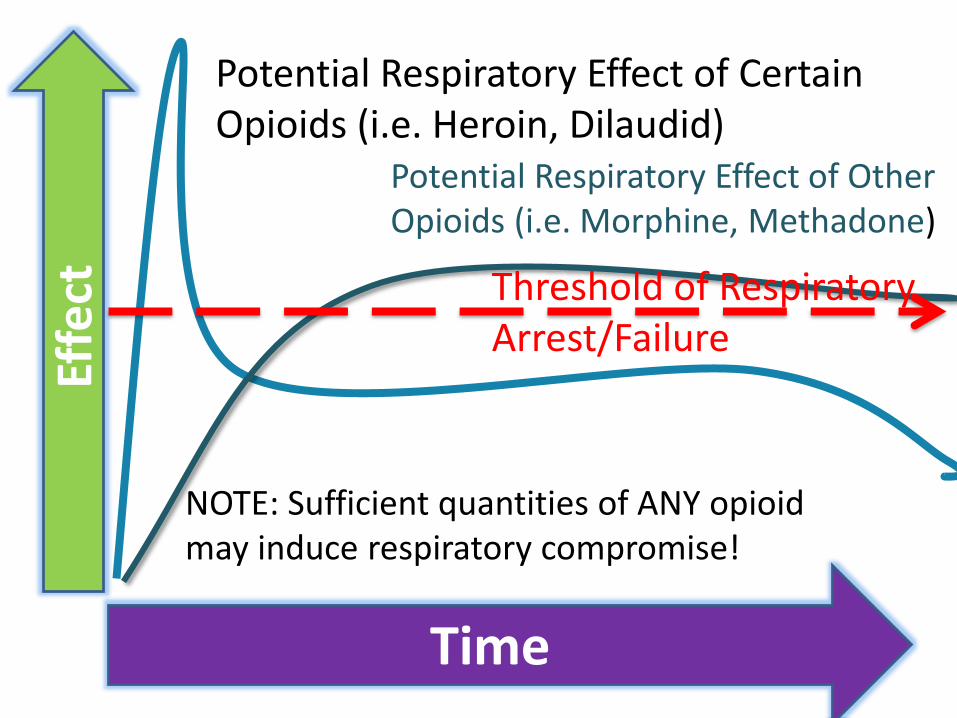
Effe
ct
Time
Potential Respiratory Effect of Certain Opioids (i.e. Heroin, Dilaudid)
Potential Respiratory Effect of Other Opioids (i.e. Morphine, Methadone)
NOTE: Sufficient quantities of ANY opioid may induce respiratory compromise!
Threshold of Respiratory Arrest/Failure

THIS IS YOUR FIRST LINE TREATMENT AT ALL LEVELS
But what if????
• Remember:
– No one ever died of a naloxone deficit
– Patient die from Airway Failure
– Patients die from Respiratory Failure
– Patients die from complications of Aspiration
– and rarely heart problems and blood pressure problems
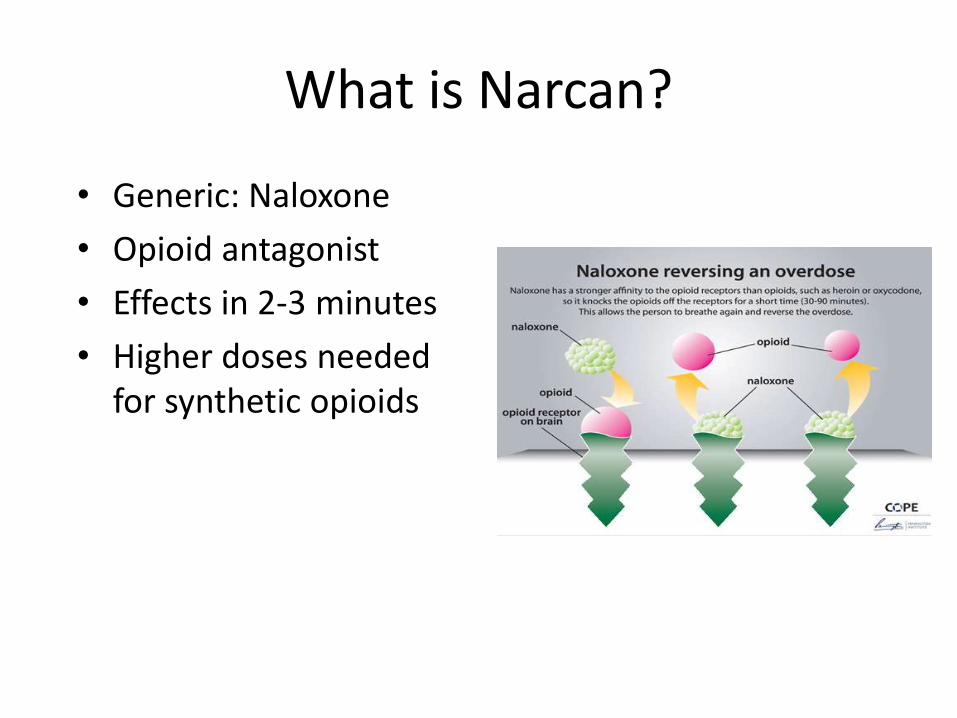
What is Narcan?
• Generic: Naloxone
• Opioid antagonist
• Effects in 2-3 minutes
• Higher doses needed for synthetic opioids
What is an antagonist?
• Binds to a “receptor” but doesn’t allow it to be activated.
Potency vs. Affinity
Potency = How hard the drug punchesAffinity= How hard the drug “handshakes” the receptor site.

Indications:
• Unconscious and not responding to any verbal stimuli– If the patient “mumbles words” or has semi
purposeful movement, roll on side and then monitor closely
• No detectable breathing, OR has poor respiratory effort such as: – agonal breaths– loud snoring respirations– occasional gasping breaths or cyanosis.
• The patient has pinpoint pupils along with the respiratory depression or arrest (ineffective or absent breathing).

Do you need pinpoint pupils?
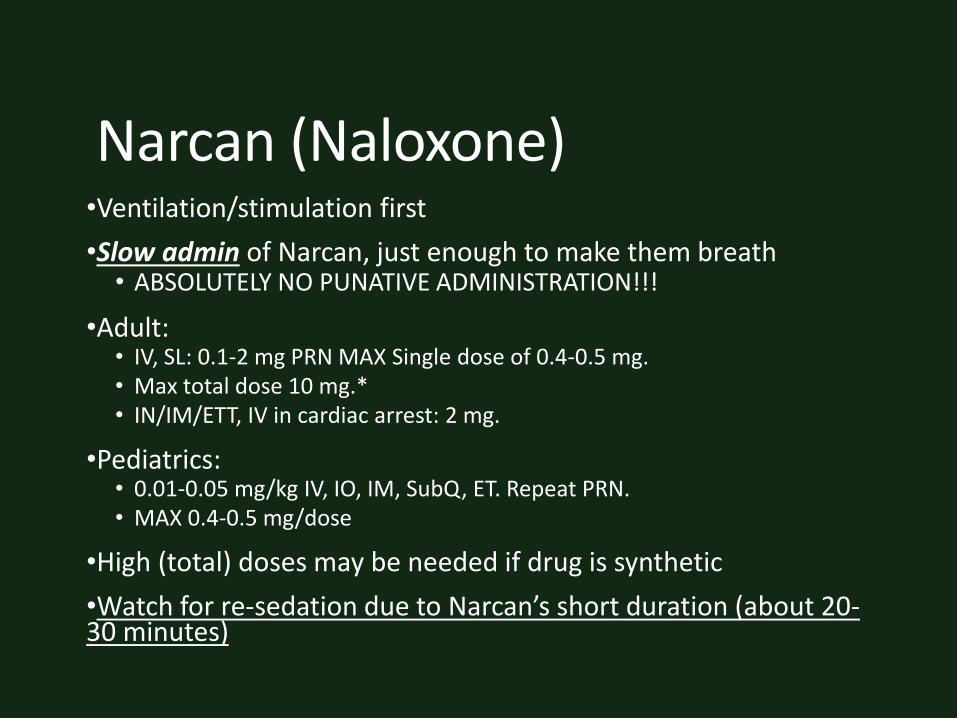
Narcan (Naloxone)•Ventilation/stimulation first
•Slow admin of Narcan, just enough to make them breath• ABSOLUTELY NO PUNATIVE ADMINISTRATION!!!
•Adult:• IV, SL: 0.1-2 mg PRN MAX Single dose of 0.4-0.5 mg. • Max total dose 10 mg.*• IN/IM/ETT, IV in cardiac arrest: 2 mg.
•Pediatrics:• 0.01-0.05 mg/kg IV, IO, IM, SubQ, ET. Repeat PRN.• MAX 0.4-0.5 mg/dose
•High (total) doses may be needed if drug is synthetic
•Watch for re-sedation due to Narcan’s short duration (about 20-30 minutes)

KEY POINT:
•It should be noted that a response to (or failure to respond) naloxone is not considered a reliable diagnostic tool in determining if a patient has consumed opioids.
•Failure to respond to a total dose of 10 mg of naloxone usually indicates:• That poisoning is not due to opioids (or opioids alone);• Or that hypoxic brain damage has occurred.• Or that the AMS is not opioid related at all
• (A-E-I-O-U-T-I-P-S)
cc: CarbonNYC [in SF!] - https://www.flickr.com/photos/15923063@N00
AHA statement
• Naloxone is a potent antagonist of the binding of opioid medications to their receptors in the brain and spinal cord. Administration of naloxone can reverse central nervous system and respiratory depression caused by opioid overdose. Naloxone has no role in the management of cardiac arrest.
Narcan doesn’t help in Cardiac Arrest, Or does it?•Poorly studied but very reasonable
• In one AHA study:• Small study , 36 patients
• Asytole and PEA were predominant rhythm. Down times varied but were typically extended.
• 42% of cardiac arrest patients with a suspected opioid etiology showed improvement in EKG rhythm s/p Narcan administration
• 27% had ROSC by arrival at ER
• 1% had survival to discharge.
• “…Although we cannot support the routine use of naloxone during cardiac arrest, we recommend its administration with any suspicion of opioid use. Due to low rates of return of spontaneous circulation and survival during cardiac arrest, any potential intervention leading to rhythm improvement is a reasonable treatment modality.”
•Why?• Inhibits the adverse effects of the opioids in cardiac arrest, specifically hypotension
• Narcan may cause a endogenous sympathetic response (i.e. release of endogenous epinephrine) in the opioid addicted patient
• May have indirect, poorly understood antiarrhythmic effects
•Source : Resuscitation. 2010 Jan;81(1):42-6. doi: 10.1016/j.resuscitation.2009.09.016. Epub 2009 Nov 13. Naloxone in cardiac arrest with suspected opioid overdoses. SayboltMD1, Alter SM, Dos Santos F, Calello DP, Rynn KO, Nelson DA, Merlin MA.
cc: Bushtick - https://www.flickr.com/photos/67197620@N00

Narcan, OPIOID Withdrawal, and adverse events?•OPIOID WITHDRAWAL IS RARELY FATAL.
• WHY DO WE HAVE FATAL EVENTS WITH NARCAN INDUCES WITHDRAWAL?
•Have you ever heard Narcan causing :• Seizures• Cardiac Arrest (VT)• Stroke?
•MOST (not all ) WITHDRAWAL SYNDROMES ARE RELATED DIRECTLY TO THE EFFECTS OF THE DRUG/SUBSTANCES INVOLVED.
• Then WHY do these S/S occur?
•FOUR REASONS:• SYNPATHETIC RESPONSE• HYPOXIA• HYPERCARBIA• ACIDOSIS
cc: LendingMemo - https://www.flickr.com/photos/92802060@N06
Avoiding BAD OUTCOMES•SYNPATHETIC RESPONSE
• EPINEPHERINE RELEASE!
•RESPIRATORY DEPRESSION CAUSES:• HYPOXIA
• HYPERCARBIA
• ACIDOSIS
•We Treat Sympathetic response by SLOWING DOWN NARCAN ADMIN with SMALLER DOSES
•We treat the RESPIRATORY CAUSES WITH CORRECTIVE BVM THERAPY!
cc: @icandidyou - https://www.flickr.com/photos/24423223@N02
No patient should suffer a delay in care “waiting for Narcan to work”

NARCAN Treat & Release Criteria• Criteria:
• The patient can mobilize as usual; • The patient has an oxygen saturation on room air of >92%; 3) have a respiratory
rate >10 breaths/min and <20 breaths/min; • The patient has a temperature of >35.0°C and <37.5°C; • The patient has a heart rate >50 beats/min and <100 beats/min; and• The patient has a Glasgow Coma Scale score of 15.
• Follow up with IM (or SQ) Narcan
•References:• Christenson J, Etherington J, Grafstein E, et al. Early discharge of patients with
presumed opioid overdose: development of a clinical prediction rule. Acad Emerg Med 2000;7(10);1110-18.
• Wanger K, Brough L, MacMillan I, et al. Intravenous vs subcutaneous naloxone for out-of-hospital management of presumed opioid overdose. Acad Emerg Med1998;5(4);293-9.

LE Naloxone?
LE (can be) quicker than EMS
Myerburg RJ, Fenster J, Velez M, et al. Impact of community-wide police car deployment of automated external defibrillators on survival from out-of-hospital cardiac arrest. Circulation. 2002; 106:1058–1064


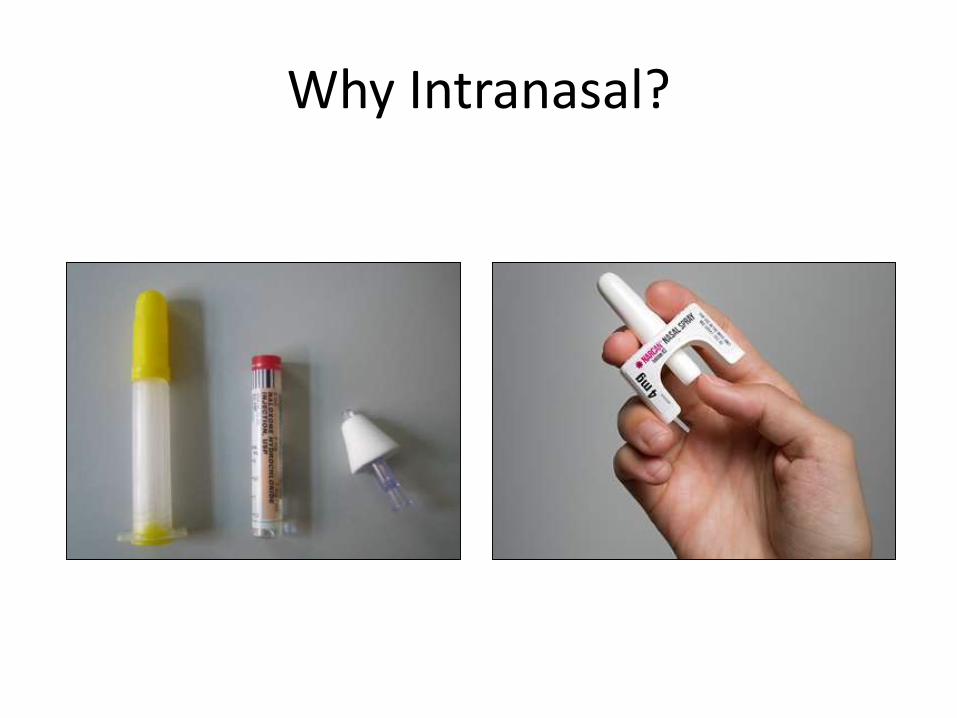
Why Intranasal?
Feb 2016

When to avoid Narcan all together
• Semi- Awake patients
• Pregnancy
• Aspiration
• POLY PHARM OD’s
cc: rishibando - https://www.flickr.com/photos/27590002@N04




Source: http://www.elephantjournal.com/2013/10/love-it-all-a-husbands-farewell-to-his-dying-wife-photos/
It is generally unwise to treat these patients with an opioid antagonist unless life threateningrespiratory depression is a reasonable concern..
"Inappropriate use of naloxone in cancer patients with pain.." J Pain Symptom Manage. 11(2)(1996): 131-134.

In the End•Stay up to date
•Don’t believe the Hype
•Overdose patients are AMS patients first, opioid overdoses last
•CORRECT HYPOXIA, ACIDOSIS , HYPERCARBIA BEFORE NARCAN
•When giving Narcan: SLOW and LOW (Slow Push and Low Doses repeated)
• Goal is airway and respiratory correction, not to wake them up
cc: jayneandd - https://www.flickr.com/photos/8180853@N07
Questions?
Source: http://paindr.com/wp-content/uploads/2013/04/Poppy-smiley-157x195.jpg

Links
• https://www.youtube.com/watch?v=1yPrGNr4TQY
• https://www.youtube.com/watch?v=sMuvTlU_mJg
• https://www.youtube.com/watch?v=Mo6cfAnP7sc
• https://www.youtube.com/watch?v=EFZzX9J_wXg
• https://www.youtube.com/watch?v=WaAnGXRvv80
• https://www.youtube.com/watch?v=veomoaFzroc
• https://www.youtube.com/watch?v=8a18abrzpEY







