
4.3 Describe how staffing plans and practices are consistent with the ANA Principles of Nurse Staffing.
The MGH Department of Nursing (DON) embraces the recommendations and underlying
assumptions of the ANA Principles of Nurse Staffing. The evidence submitted in this document, as
well as OOD 15 and Forces 1, 4 and 5, demonstrates our strong commitment to and utilization of a
patient classification system to assure adequate staffing levels based on patient, staff and unit
variables; a well defined competency program for all direct care staff; a culture of valuing and
appreciating employees; and organizational policies that consider a balance of patient and staff
needs.
I. Patient Care Unit Related
a). Appropriate staffing levels for patient care unit reflect analysis of individual and aggregate
patient needs.
OOD 15 describes WinPFS® Acuity, Productivity and Benchmarking System (WinPFS®
System) used at MGH to identify individual patient care needs, classify patients, provide a measure
of nursing acuity, and calculate unit workload. The WinPFS® System groups patients into similar
categories based on nursing care needs and assigns a relative value to each category. Within each
category or patient type, the number of patients is multiplied by the relative value for that patient
type then the category workloads are added for a total unit workload. Thus, for any given time
period, information about specific patient needs, as well as overall unit workload, is available.
Previous Forces 1.5 and 1.6 describe how this system is used to monitor direct care staff
utilization, budget for direct care resources, and predict variable non-salary expenses. Forces 4 and
5 will include examples of how the data is used in scheduling and staffing plans. The WinPFS®
System has been used at MGH for over 20 years and is considered a credible tool for predicting and
justifying direct care resources to both nursing staff and those outside nursing, such as
administrators and financial officers.
b). There is a critical need either to retire or seriously question the usefulness of the concept
of nursing hours per patient day (NHPPD).
The data collected through the patient classification system is widely accepted at MGH.
When focusing on a measure of staffing effectiveness or adequacy, nursing leaders consistently use
the indicator of Hours Per Workload Unit (HPWI) provided by the classification system. HPWI is a
39

much more refined measure of staffing than NHPPD, as it incorporates not only census, but also
factors in patient acuity, providing a weighted census which is then used in a ratio to measure direct
care staff hours per workload. Nursing leaders are very familiar with HPWI as a productivity
measure. Real-time data is available electronically on all clinical computers and nursing leaders are
attentive to the weekly monitoring reports that provide an on-going measure of staff adequacy in
meeting patient care needs.
The routine measurement of NHPPD for budgeting or tracking purposes was infrequent at
MGH prior to 2002. Since that time, participation in national databases for benchmarking (e.g.,
National Database Nursing Quality Indicators (NDNQI), National Quality Forum) and new State
requirements for data submission (e.g., Patients First) has necessitated quantifying staffing by
NHPPD. As not all hospitals have patient classification systems, NHPPD has emerged as a
universal measure that allows for comparable evaluation. In addition, most of the recently-
published articles suggesting relationships between direct care staffing levels and patient outcomes
have also referenced NHPPD.
MGH currently submits patient days and nursing hours by role group to NDNQI to provide
a comparison of MGH unit performance for Total Nursing Care HPPD, RN HPPD, and RN Mix
to NDNQI benchmarks (provided by unit type for hospitals with more than 500 beds). In addition,
through participation in the state wide Patients First initiative, each unit’s staffing plan (i.e., the
budgeted number of shifts by role group and the resulting worked HPPD) is available to the public
on a website. Actual data for each unit’s worked HPPD, is also posted on the web-site on an annual
basis.
Despite this recent trend of reporting HPPD externally, MGH nursing leadership remains
conscious of the serious limitations of this measure, especially when a more refined measure such as
HPWI is available. There is also concern regarding the ability of the public to be able to interpret
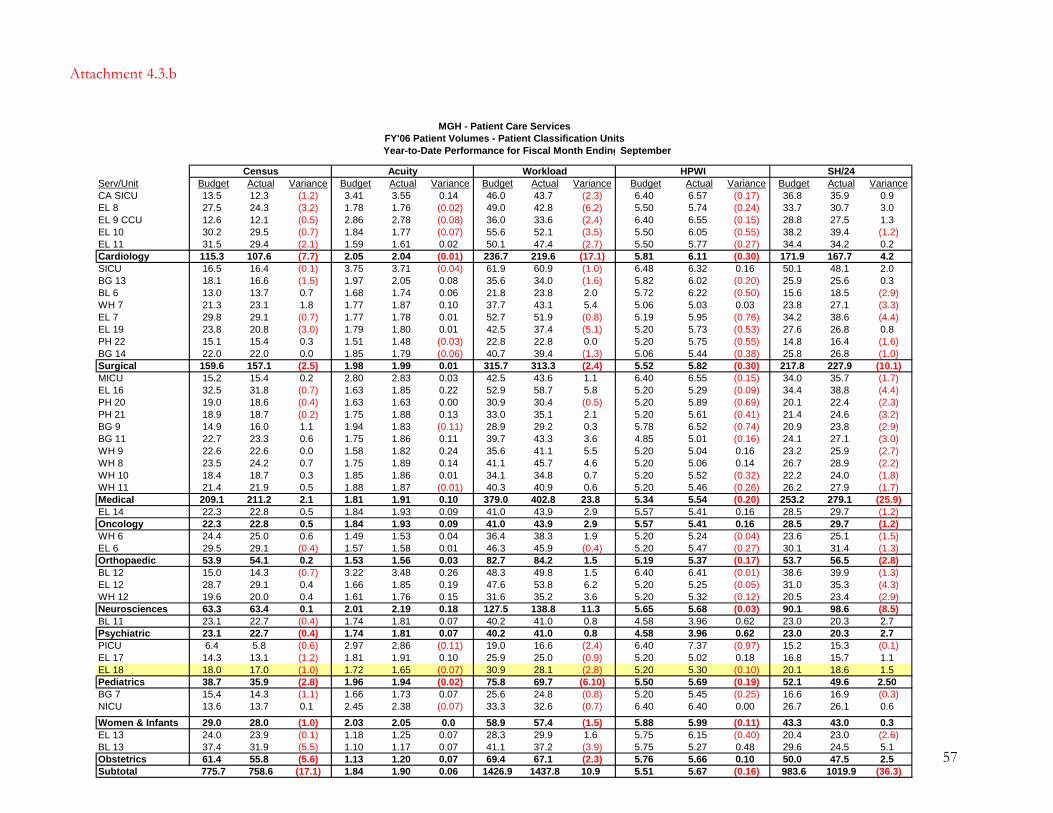
the NHPPD data in a meaningful way and to make accurate comparisons. For example, in 2006
MGH provided data for Ellison 18, one of the MGH pediatric general care units for the Patients
First initiative. This staffing plan included a planned or budgeted worked HPPD of 9.98
(attachment 4.3.a). The actual FY’2006 experience for Ellison 18, however, was a slightly lower
census (17.0 vs. 18.0 budget) and slightly lower patient acuity (1.65 vs. 1.72 budget), resulting in a
lower workload than expected (28.1 vs. 30.9 budget). To adjust to this variance, the unit used, on
average, 1.5 less direct care shifts per day (18.6 vs. 20.1 budget). The Workload/Productivity Report
for September 2006 YTD (attachment 4.3.b) demonstrated that despite this reduction in staffing, the
40
unit maintained an HPWI that was slightly above budget and within 5% of their target (5.30 vs. 5.20
budget), indicating an appropriate reduction based on workload. In contrast, the data provided for
the Patients First initiative included an annual report of actual utilization, which showed a worked
HPPD of 8.95 against the planned or budgeted worked HPPD of 9.98. There is concern that this
single measurement could be interpreted by the public as providing “inadequate” staffing, when it
fact the staffing was appropriate for patient care needs.
c). Unit functions necessary to support the delivery of quality patient care also must be
considered in determining staffing levels.
Consideration of unit functions in determining staffing levels is most clearly seen in the
decisions regarding establishing a target HPWI target for a nursing unit. The WinPFS® System
staffing framework describes an expected range of four to seven hours of direct care time per unit of
work (HPWI). The organization determines its own target within that range. The HPWI, or
intensity of resources, allocated to specific units may vary as a result of a variety of issues around
patients, staff, support, and structure or logistics of the unit as noted in the attached flow chart
depicting the relationship of staffing to workload (attachment 4.3.c).
In general, the critical care units are targeted at a higher HPWI than the routine units,
because of logistical issues of reasonableness. For example, if one patient requires 18 hours of care
in a 24-hour period, there is not likely to be in that same unit another patient who requires only 6
hours of care; thus, the available average HPWI for the unit will increase. As another example, the
Pediatric Intensive Care Unit (PICU) is a small unit and historically has had significant fluctuations
in census and workload. At times, the unit must meet minimum staffing requirements (i.e., two staff
nurses on each shift if there are any patients at all in the unit or 48 hours of care per 24-hour period)
even if the one or two patients in the PICU require only a total of 24 hours of care in the 24-hour
period. Again, the average HPWI for the unit will be greater than would be necessary without this
logistical challenge.
There are also several units that include both critical care and general care patients that
receive care from one integrated staff, including the Burn Unit, the Transplant Unit, Ellison 14
(general oncology with designated bone marrow transplant), Bigelow 9 (chronic ventilator support
and general medicine) and Ellison 7 (general surgery with four bed Trauma Care Unit). The HPWI
for these units is calculated using a critical care-level HPWI for the critical care workload and a
routine-level HPWI for the general care workload. The result is a blended HPWI that reflects the
41
broad range of patient care requirement on the same geographical unit. The delivery model may also
affect the targeted HPWI. On Bigelow 11 General Medicine, which has an all-RN model, the
targeted HPWI is lower than that of similar medical units because delegation to and supervision of
non-RN staff is not required of the Staff Nurses. Originally, the unit had primarily experienced Staff
Nurses and the HPWI target was about 12% lower than that of other general medical units.
However, for the past few years the unit has focused on recruiting new graduates and the HPWI has
subsequently been increased to within 6% of other general care units to accommodate for the larger
number of inexperienced Staff Nurses.
In the Obstetrics areas, standards common to the specialty, as well as risk management
recommendations, are consulted in determining staffing requirements. In addition to the specialty
standards for care of patients in labor, delivery and recovery and of mother-baby couplets, standard
time requirements have been established for other obstetrical activities such as triage, observation,
non-delivery admissions and related surgical procedures. The volume of these activities is projected
as a ratio of activities to deliveries, based on current and historical experience, and the staffing
projections incorporate the care needs for patients across the continuum. HPWI targets for the
Family Care Units reflect the specialty standards for mother-baby couplets, the patients’ needs for
nursing care identified through the classification system, and the logistical challenges of staffing
separate post-partum and nursery areas.
II. Staff Related
a). The specific needs of various patient populations should determine the appropriate
clinical competencies required of nurses practicing in that area.
The Norman Knight Nursing Center for Clinical & Professional Development (Norman
Knight Nursing Center) oversees the orientation and competency programs for Department of
Nursing (DON) employees. In addition to the orientation and annual competency assessment
described later in this document, Staff Nurse new hires, including RN contract agency staff,
complete a unit-based orientation specific to their practice area. The unit-based program is
competency based, involves assignment with a preceptor and extends for a designated period of
time that is tailored to the individual.
The average length of time for employee unit orientation is two to six weeks for general care,
six to 12 weeks for critical care, and up to six months for procedural areas such as the operating
room. During the orientation, a unit-specific competency checklist is completed for all employees.
42

The competency checklists are created by the unit-based CNSs and include competencies specific to
the populations cared for on the unit. Agency Staff Nurses are required to complete the same unit-
specific competency checklist as MGH Staff Nurses. In general, the competency checklists have
several pages of competencies that are generic to nursing throughout the organization. Unit-specific
competencies that reflect the unit’s patient populations are then added to the form. Attachment
4.3.d contains samples of unit-specific items that have been added to the competency checklists for
the Yawkey Infusion Unit and Bigelow 9, the Respiratory Acute Care Unit.
b). Registered nurses must have nursing management support and representation at both the
operational and executive level.
As described in Force 2.1, the Chief Nurse represents Registered Nurses at the executive
level as a member of the senior management team, and as such, is responsible for coordinating the
development and implementation of programs to fulfill the patient care, research, and educational
missions of the organization. The Chief Nurse attends and participates in Board of Trustees and the
Chief’s Council, and is a voting member of the General Executive Committee and the Patient Care
Assessment Committee. The Chief Nurse is a strong advocate and support for nurses and patient
care in these executive level forums.
Force 2.3 describes the valuable role of the Associate Chief Nurses, who provide senior level
nursing management. The four Associate Chief Nurses provide oversight to their respective patient
care units and have high-level relationships with other leaders in the organization to support nursing
practice and promote patient care. Several examples are provided throughout the evidence to
demonstrate their role in strategic planning, program planning and facility changes, major
organizational projects (e.g., information system upgrades), service-line activities (e.g., Cancer
Center, Heart Center and Vincent Gynecology and Obstetrics), as well as unit leadership triad
suport.
Two of the members of the unit-based leadership triad, the Nursing Director and the
Clinical Nurse Specialist, provide nursing management support for unit-based operations. These key
nursing leadership positions assure that nursing is a strong presence and active participant in the
clinical operations of the unit, and that there is decentralized clinical decision-making and patient-
centered care.
c). Clinical Support from experienced RNs should be readily available to RNs with less
43

proficiency.
The DON leadership is committed to providing clinical support to all nurses providing
direct care. Resources such as the Clinical Nursing Supervisors, the Rapid Response Team Staff
Nurses, Resources Nurses, Clinical Nurse Specialists, and expert Advanced Practice Nurses are
available to assist all nurses, regardless of years of experience, length of service, or competence in a
clinical specialty. In addition, nurse preceptors are an important resource for the less proficient
nurse.
Clinical Nursing Supervisors – In addition to their administrative role involving the
prioritization and triage of internal bed and external transfer requests, the Clinical Nursing
Supervisors (Supervisor) play a key role in supporting the Staff Nurse at the bedside. Three Clinical
Nursing Supervisors are scheduled each shift, seven days a week including holidays and weekends.
The Supervisor brings a strong clinical knowledge and expertise to both the clinical and
administrative processes, as well as an understanding of the available resources (i.e., ICU beds) and
their established relationships with the staff on the patient care units. The role of the Supervisor in
supporting patient care is described in their position description:
3.0 Patient Care Management - Serves as a clinical resource in the management of patient care.
3.1 Performs the role of central code call nurse and responds to patient care emergency
situations
3.2 Provides clinical consultation to staff
3.3 Assists staff in managing unit activity
3.4 Collaborates with other departments to facilitate/support patient care.
Rapid Response Team - As presented in Forces 1.3 and 1.7, the Rapid Response Team can
be deployed to units at the request of the unit staff or at the direction of the Clinical Nursing
Supervisor. They provide staffing for short periods of time to support fluctuations in volume or
acuity, to travel with high-risk patients to procedural or test areas, to assist with unit to unit patient
transfers, or to act as clinical resource and staff support around unfamiliar procedures and
equipment.
Staff Nurse Preceptors – The Staff Nurse Preceptor (Preceptor) is an experienced, clinically
competent Staff Nurse who works with newly-hired nurses to assist in their orientation to the unit
and hospital. The Preceptor serves as an educator, role model, facilitator, and clinical “coach”, as
44

45
well as a partner in planning and guiding clinical experiences, professional socialization and role
transition. Force 4.7 highlights the improvement efforts involving the creation of a New Graduate
Task Force. This group held focus groups with new graduate nurses to obtain meaningful feedback,
which included positive remarks about the value of Preceptors.
Resource Nurses – The Resource Nurse role was developed in response to staff feedback
requesting additional support for unit-based, shift-to-shift operations. As described in Force 4.12,
the Resource Nurse supports the unit by “addressing staffing needs on an ongoing basis, facilitating
throughput of admissions and discharges, assisting with direct patient care as needed, and role
modeling effective collaboration and conflict management with patients, families and other
members of the healthcare team.” The Resource Nurse, in addition to the unit leadership triad, is
available to provide assistance to less experienced Staff Nurses, who often describe the transition
from orientation to Staff Nurse as stressful and clinically challenging.
Clinical Nurse Specialists – The Clinical Nurse Specialist (CNS) role is an integral part of the
unit leadership triad. Considered bedside “experts”, these master’s prepared Advanced Practice
Nurses provide clinical support to nursing staff and are responsible for unit-based educational and
competency programs. The CNSs also provide clinical specialty consultation to Staff Nurses on
other patient care units when requested (i.e., an obstetrical patient on the Burn Unit). As identified
in the CNS position description, the CNS “supports independent nursing practice of professional
nurses through collaborative, consultative, and role modeling activities, facilitates the acquisition of
advanced clinical skills in Staff Nurses through role modeling, practice, and consultation in the
clinical setting, develops, implements, and evaluates unit-based orientation programs, and supports,
participates, and designs educational programs for staff.”
In the past few years, as MGH has hired larger percentages of new graduate nurses. As a
result, nursing leadership has made a purposeful decision to continuously review the scope of the
CNSs responsibilities and to decrease the scope when appropriate (see example in Force 1.7). The
DON has been successful in adding CNS positions, to support the inexperienced nurse as well as
the specialized needs of particular patient populations.
Year 2003 2004 2005 2006 2007
Budget CNS FTEs 45.7 50.2 52.3 56.1 62.5
Centrally-Based Expert Clinical Nurses Specialists – The DON is fortunate to have a
number of nationally-known nurse experts who are centrally based and remain available to Staff
Nurses to support clinical decision making in specialized areas. Two examples of this are the
doctorally-prepared CNS nurse experts in ethical decision-making and wound/skin care.
The Clinical Nurse Specialist in Ethics is available to support Staff Nurses throughout the
organization providing consultation about ethical quandaries or cases. Although there are
committees available for formal ethics consultations (e.g., the Pediatric Ethics Committee, the
Optimum Care Committee), many nurses benefit from discussing a particular case or concern prior
to taking the step of formal consultation. The Clinical Nurse Specialist in Ethics serves as a
sounding board and is available to discuss a case individually or may suggest that a nursing meeting,
or team meeting take place to process the case or issue.
Serving in the role of consultant and educator, the Clinical Nurse Specialist in Wound Care
is an expert resource for skin care and wound management. When a unit-based CNS or Staff Nurse
encounters a challenging wound care issue, he/she may request a telephone or bedside consultation.
The Wound Care CNS usually examines the patient with the Staff Nurse involved, assesses the
etiology and status of the wound, and develops or revises the plan of care. Identified interventions
often involve the selection of specific products based on the clinical assessment of the wound bed.
III. Staff Related
a). Organizational policy should reflect an organizational climate that values registered
nurses and other employees as strategic assets and exhibits a true commitment to filling
budgeted positions in a timely manner.
The leadership of MGH and Patient Care Services (PCS) is keenly aware of the link between
the valuable assets of its employees and the organization’s ability to meet strategic goals, such as
quality patient care, the growth of specific services, and new program development. As described by
the Hospital President in the most recent annual report:
“While new magazines, scientific breakthroughs, buildings and programs are tangible results of a
productive year, what truly defines MGH are its people – the physicians, nurses, other professionals,
administrators, supports staff and volunteers – the dedicated individuals who tend to the needs of patients and
families and ensure that the institution runs smoothly and effectively.”
46

The PCS Collaborative Governance (CG) model (Force 2.3) also demonstrates the
importance and value of nurses and other health care professionals. CG places “the authority,
responsibility and accountability for patient care with practicing clinicians. CG is based on the beliefs
that a shared vision and common goals lead to a highly committed and productive workforce, that
participation is empowering and that people will make appropriate decisions when sufficient
knowledge is known and communicated.” CG optimizes staff participation in organizational
decision-making within and across disciplines.
MGH and PCS leaders appreciate the challenges and significant impact of shortages in
nursing and other clinical role groups, and believe that being positioned as the “employer of choice”
in Boston health care is essential. This inevitably involves multiple strategies aimed at both
recruitment of new staff and retention of employees. For PCS employees this includes competitive
wage programs, supportive work environments, recognition and rewards programs, and a dedicated
PCS Human Resource team. For Nursing Directors this requires organizational support, leadership
development, and local fiscal authority and accountability. Several years of MGH’s favorable
financial performance has allowed continuous growth in the organization, resulting in end-of-year
bonus checks for all PCS employees to recognize their contribution to the organization’s success
and further a positive work environment.
Once the fiscal personnel budget is approved, managers have the full authority to work with
Human Resources (HR) to fill all available positions. Each Director works with a designated HR
Generalist and/or Recruiter who is familiar with their unit and specialty area. The close working
relationship between HR and the Nursing Directors has resulted in a well-honed recruitment and
interview process. HR assists the Nursing Directors with resume distribution, prescreening of
candidates, scheduling of HR and Nursing Director interviews, checking references, extending offers
and managing the new hire process for candidates who accept a position. Although HR utilizes the
MGH website, other external websites, print advertisements, direct mail and recruitment fairs as
necessary to attract qualified staff, many candidates are referred by current employees.
To begin the hiring process, Nursing Directors communicate their staffing needs to HR. To
track vacancies and new hires, HR uses a vacancy tool, which is updated on a monthly or more
frequent basis by the Nursing Resource Coordinator. This process is extremely fluid, often involves
discussions with the Nursing Director to determine current or future unfilled positions on his/her
unit. If there are vacant positions within the annual approved budget, there is no further approval
47

process necessary and active recruitment begins at the request of the Nursing Director. Recruitment
for positions beyond the approved budget requires approval by an Associate Chief Nurse.
The Chief Nurse and Associate Chief Nurses consistently review and communicate the
expectation that Nursing Directors will fill vacant positions in a timely fashion. A Filled Position
Report that tracks budgeted Full Time Equivalents (FTEs), filled positions, employees hired into
positions but not yet started, vacant positions and percent of positions vacant is created on a
monthly basis and distributed to Nursing Directors and Associate Chief Nurses (attachment 4.3.e).
The unit level accountability for recruitment and hiring into approved positions has been
extremely effective. During most years, the Department of Nursing begins the year with a Staff
Nurse vacancy rate of about 5%, primarily due to the expectation for increased volume and the
resultant newly approved positions for the fiscal year. As the year progresses that vacancy rate
generally falls to about 1%.
b). All institutions should have documented competencies for nursing staff, including agency
or supplemental and traveling RNs, for those activities that they have been authorized to
perform.
The MGH Department of Nursing policy for Competence of Licensed and Unlicensed
Personnel is included as attachment 4.3.f. As is presented in that document, “The competence of
licensed clinicians who practice at Massachusetts General Hospital is maintained through a
combination of ongoing competence assessment and educational activities.” Competence
assessment includes assuring professional licensure, completion of a competency-based orientation
Month FY'06 FY'07
October 5.6% 4.9%November 5.3% 3.8%December 4.9% 4.6%January 5.9% 4.3%February 4.6% 4.1%March 4.6% 2.9%April 4.5% 2.9%May 3.6% 2.4%June 2.9%July 2.4%August 1.6%September 0.9%
Direct Care Staff Nurse Vacancy Rate
48

program, the performance appraisal process, annual required training, annual hospital, departmental
and/or unit-specific competency achievement, age specific competencies, and on-going educational
activities.
The Norman Knight Nursing Center for Clinical & Professional Development oversees the
orientation and competency programs for PCS employees. All new employees, including RN agency
contracted staff, complete a day of hospital orientation followed by a Department of Nursing
(DON) orientation that is tailored to various clinical role groups. The DON component provides
an overview of the nursing service, introduces staff to key clinical practices, and evaluates some of
the required clinical competencies. For direct care nurses, the content includes culturally competent
care, patient rights and confidentiality, delegation and supervision, emergency response and
preparedness, review of equipment, infection control practices, blood product administration, and
resources available to staff. Skill demonstration and competency evaluation is completed for point-
of-care testing, medication administration, and arrhythmia interpretation. Staff Nurse new hires,
including RN contract agency staff, also complete a unit-based orientation specific to their practice
area, as described earlier in the document.
Job-related training is provided for those employees hired as Patient Care Associates (PCA),
Operations Associates (OA), and Unit Service Associates (USA). The length of the orientation
programs vary by role: PCA (3 to7 weeks); OA (4 weeks); and USA (2 1/2 weeks). All programs
include didactic lecture and classroom practice sessions and instructor-led learning activities in the
work setting.
Yearly, assessment of competence is documented at the time of the employee’s annual
performance review. Employees in PCS are considered in five categories and annual training and
competences are specific to each group’s work responsibilities. The employee categories and annual
required competencies for 2007 are included below.
CATEGORIES OF REQUIRED TRAINING
CATEGORY A Employees in Category A are in roles that do not require them to have direct contact with patients. Only the basic level of required training must be completed at time of hire and annually. CATEGORY B Employees in this group have roles which require them to be in the patient environment but who do not have hands on contact with patients. In addition to the basic requirements, these employees must annually complete the sections pertaining to Infection Control, Precautions, Bloodborne Pathogens, TB education, and PPD Testing.
49
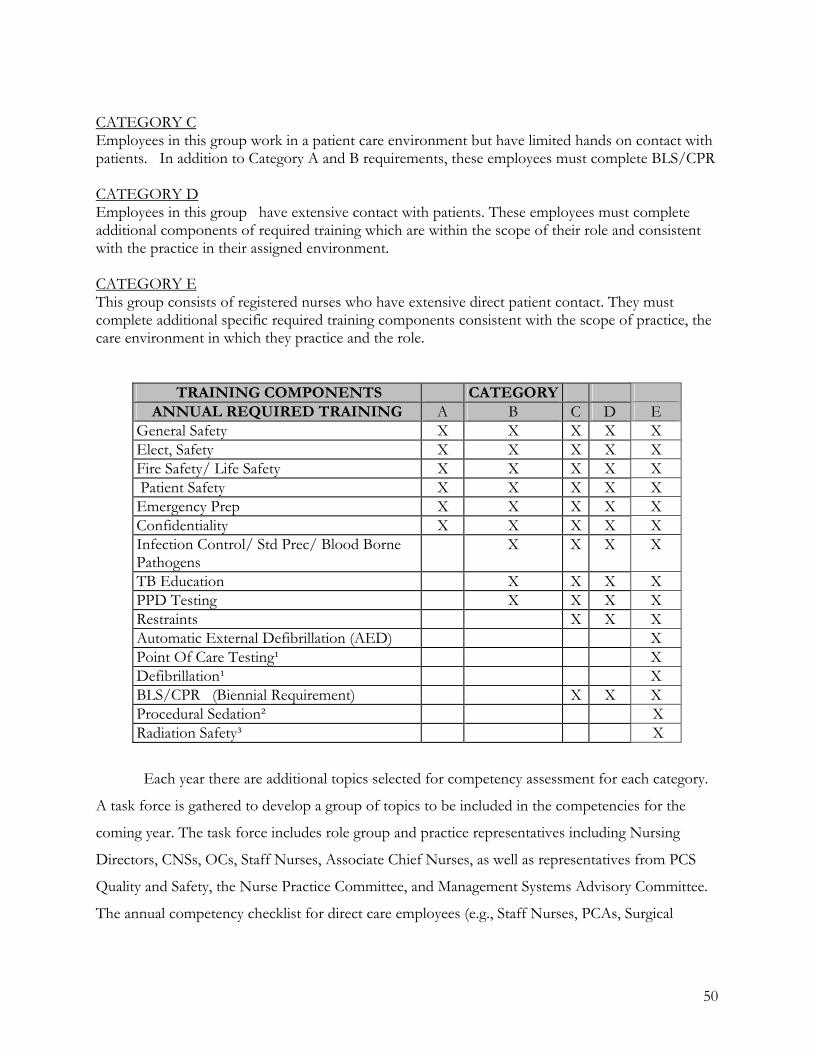
CATEGORY C Employees in this group work in a patient care environment but have limited hands on contact with patients. In addition to Category A and B requirements, these employees must complete BLS/CPR CATEGORY D Employees in this group have extensive contact with patients. These employees must complete additional components of required training which are within the scope of their role and consistent with the practice in their assigned environment. CATEGORY E This group consists of registered nurses who have extensive direct patient contact. They must complete additional specific required training components consistent with the scope of practice, the care environment in which they practice and the role.
TRAINING COMPONENTS CATEGORY ANNUAL REQUIRED TRAINING A B C D E
General Safety X X X X X Elect, Safety X X X X X Fire Safety/ Life Safety X X X X X Patient Safety X X X X X Emergency Prep X X X X X Confidentiality X X X X X Infection Control/ Std Prec/ Blood Borne Pathogens
X X X X
TB Education X X X X PPD Testing X X X X Restraints X X X Automatic External Defibrillation (AED) X Point Of Care Testing¹ X Defibrillation¹ X BLS/CPR (Biennial Requirement) X X X Procedural Sedation² X Radiation Safety³ X
Each year there are additional topics selected for competency assessment for each category.
A task force is gathered to develop a group of topics to be included in the competencies for the
coming year. The task force includes role group and practice representatives including Nursing
Directors, CNSs, OCs, Staff Nurses, Associate Chief Nurses, as well as representatives from PCS
Quality and Safety, the Nurse Practice Committee, and Management Systems Advisory Committee.
The annual competency checklist for direct care employees (e.g., Staff Nurses, PCAs, Surgical
50
Technicians) for 2007 is included as attachment 4.3.g. The annual competency checklists become a
part of the employee’s permanent human resource file.
c). Organizational policies should recognize the myriad needs of both patients and nursing staff.
The PCS Strategic and Operating Plan presented in Force 1.1 and OOD 13e clearly
demonstrates the commitment of the department to both patients and nursing staff. The Patient
Care Delivery Model (PCDM) is patient/family-focused and has environmental elements to enhance
patient outcomes. These elements include not only direct care staffing patterns, but also adequate
support and ancillary staff and effective communication systems that assure the reporting and
documentation of patient outcomes.
The PCDM is operationalized at the unit level through a leadership triad (Nursing Director,
Clinical Nurses Specialist, and Operations Coordinator (OC) and unit staff which includes Staff
Nurses, PCAs, OAs (clerical support) and USAs (environmental cleaning and other support). The
advantage of decentralized clerical and environmental cleaning staff, under the direction of the unit
OC, is timely attention to the environmental needs of patients and nursing staff.
Additional operational support is provided to the units by several ancillary service
departments, such as the Materials Management and Transportation Departments. The DON has
developed a close working relationship with the Materials Management Department, and in the past
few years has collaborated with them on various patient-focused, performance improvement
initiatives through the Nursing/Materials Management Task Force. During this fiscal year, a sub-
group of the task force was formed to focus on the availability of pediatric supplies, and in
particular, to consider moving some specific pediatric supplies from the special order process to the
MGH routine supply process so that nurses could access the items more easily and quickly.
The OCs from the two Pediatric General Care Units, the Pediatric Intensive Care Unit,
Neonatal Intensive Care Units, and Obstetric Units met with representatives from the Materials
Management Department and the hospital’s primary supply vendor. The group created a list of
current “special order” items for all of the Pediatric Units. Realizing there would be a need for
prioritization of selected items, and that decisions may involve standardization or alternative
products, the pediatric CNSs were added to the workgroup. The group has met every two weeks
since October 2006 and as of June 2007, over 40 pediatric items have been moved from special
order to unit-based supply carts. The group continues to use the list that was developed as a
valuable tool for future transitions from special order to routine pediatric stock items. In addition,
51
they have developed a process for requesting new items that should be considered for addition to
the pediatric supply carts.
Supportive technology for direct care providers is an important focus of the Massachusetts
General Hospital and Massachusetts General Physician Organization’s (MGH/MGPO) Strategic
and Financial Plan. As stated in this plan’s “Key Elements of MGH Vision 2011” (OOD 13b):
• Patient care is supported by an electronic medical record and other information technology
An Information Systems Steering Committee is overseeing the creation of an electronic record and
other information technology approaches that will ensure effective patient care, efficient operations,
and the organization’s financial health. The Committee identifies the projects that are most
important for achieving the organization’s strategic vision in the context of information technology
demand that continues to grow exponentially and outstrip available resources. There is now an
institution-wide longitudinal plan for implementing large IS systems such as the Electronic
Medication Administration Project (eMAP) and Acute Care Documentation (ACD). Both of these
initiatives are linked to achieving our strategic goals.
The MGH is the largest non-governmental employer in Boston, with over 20,000 employees.
The hospital has a long history of supporting and recognizing employees. This is evidenced in
policies and practices that support employee education, training, and professional development; in
rewards that recognize exceptional employee performance, special accomplishments, and length of
service; and in competitive wage and salary programs.
One example of this spirit of recognition is the annual Ether Day celebration held each
October, on the Friday closest to the anniversary of the first use of Ether as an anesthetic, a
remarkable medical milestone at MGH that transformed the field of surgery. Ether Day is the time
designated to celebrate the anniversaries of MGH employees who have worked at MGH for 5, 10,
15, 20, 25, 30, 35, 40, 45, 50 and 60 years. There are two separate celebrations each year, a reception
for all employees who are being recognized for their years of service and a formal cocktail/dinner
event for employees who have over 20 years of service. The 2006 celebration, held on Oct. 13, 2006
honored 2,747 employees.
MGH was recognized by the American Association for Retired Persons (AARP) in 2006 as a
“Best Employer” and by Working Mother Magazine as one of the top 100 companies for working
women. The following excerpts were included in the MGH Hotline, a weekly employee publication,
about these accomplishments:
52
AARP recognizes MGH as best employer for workers over 50
The MGH values all employees, particularly those who are close to retirement age or beyond. The many
benefits the MGH offers were recently recognized by the American Association of Retired Persons (AARP),
which is the leading nonprofit membership organization for people age 50 and over in the United States. The
hospital was selected as one of the best employers in the country for workers over the age of 50, making the
MGH one of two organizations – along with the Massachusetts Institute of Technology (MIT) – in
Massachusetts to earn this honor.
The MGH was selected because of the many programs and services the hospital offers that not only serve
more mature workers but also are valued by all of employees. These include the training and career
development programs, health benefits for current employees and for retirees, the range of options for retirement
savings plans, financial planning services, flexible work hours, accommodations made to work environments
and the many recognition awards and celebrations of service.
Working Mother magazine recognizes MGH as top company for working mothers
Because of the many benefits and services the MGH offers that support working mothers, the hospital
was recently selected as one of the top 100 companies in the nation for working mothers by Working Mother
magazine. In its 20th year of publishing the top 100 list, Working Mother evaluates thousands of
submissions and determines the list based on the submitting company’s on-site childcare options,
compensation, company culture that is family oriented, areas of work/life and family-friendly policies.
The hospital offers a variety of programs that help MGH working mothers take care of their families,
such as child care options, maternity and adoption leaves, flexible work schedules, and many of the Employee
Assistance Programs (EAP) that address family issues. The MGH also offers programs that help working
mothers with building their careers and refining their work skills through ongoing course offerings, on-the-job
training, career development opportunities as well as scholarships and grants. And the MGH has programs
that help working mothers take care of themselves, like health and wellness programs, support programs
through EAP and convenient on-site services that help employees take care of personal errands.
PCS also embraces this philosophy of employee recognition. Several awards and recognition
programs are conducted each year to celebrate practice at MGH:
• Ben Corrao-Clanon Memorial Scholarship
The scholarship was created in 1987 by Regina Corrao and Jeffery Clanon to recognize a
Newborn Intensive Care Unit Staff Nurse whose practice demonstrates excellence and a
53

commitment to primary nursing.
Eligibility: NICU Staff Nurses Award $500 (one recipient)
• Orren Carrere Fox Award for NICU Caregivers
The award was created in 1997 by Henry Fox and Elizabeth DeLana to acknowledge the
exceptional care given their son at the time of his birth. The award is for all individuals,
professional and non-professional alike, who work in the Newborn Intensive Care Unit.
Eligibility: Professional and non-professional NICU staff Award $1000 (one recipient)
• Stephanie M. Macaluso, RN, Excellence in Clinical Practice Award
The award was established in 1996 to recognize direct care providers whose practice
exemplifies the expert application of the values reflected in our vision. The award provides a
means to make this practice more visible and to enhance the image of MGH health
professionals on campus as well as in the community.
Eligibility: Professional staff in PCS Award $1000 (multiple recipients)
• Yvonne L. Munn, RN, Nursing Research Award
The Department of Nursing established the Yvonne L. Munn Nursing Research Awards
program to enhance MGH nursing and its tradition of, and commitment to, research-based
practice. The Yvonne L. Munn Nursing Research Award will support research initiated by
MGH staff for the purpose of improving the care of their patients and families by advancing
nursing knowledge and theory.
Eligibility: Nurses at all levels in PCS Award (support of research)
• Marie C. Petrilli Oncology Nursing Award
Each year two MGH nurses are recognized for their commitment and compassion in caring
for cancer patients.
Eligibility: Nursing staff in PCS that care for cancer patients. Award $1000 (two
recipients)
• Paul W. Cronin and Ellen S. Raphael Award for Patient Advocacy
Paul and Ellen, as well as their families, were so impressed with the care provided by the
staff of Phillips House 21 they established an endowment fund for the staff on this unit.
Beginning in 2000, this endowment has funded an annual award for all staff of Phillips
House 21.
Eligibility: Staff on PH 21(nurses and support staff alternate) Award $500 (one recipient)
54
• Anthony Kirvilaitis Partnership in Caring Award
The purpose of this award is to recognize and celebrate those in non-clinical roles that
exemplify excellence in service and therefore share some of the same attributes that Tony
demonstrated.
Eligibility: MGH employees in non-clinical roles Award $1000 (each for two recipients)
• Cancer Career Development Award
The award is administered by the Cancer Affairs Nursing Subcommittee to recognize a
professional staff nurse for meritorious practice. The award provides financial assistance for
the recipient for continuing education that will further the nurse’s professional goals.
Eligibility: Nursing staff in PCS that care for cancer patients. Award $1000 (one recipient)
• Norman Knight Preceptor of Distinction Award
The Norman Knight Preceptor of Distinction Award is designed to recognize a clinical staff
nurse who consistently demonstrates excellence in educating, precepting, mentoring, and
coaching nurses.
Eligibility: Staff nurses in PCS Award (one recipient – tuition or buyout time)
• Brian M. McEachern Extra Ordinary Care Award
The purpose of this award is to recognize staff whose passion and tenacity exceeds the
expectations of patients, families and colleagues by demonstrating extraordinary acts of
compassionate patient care and service.
Eligibility: PCS staff across all role groups Award $1000 (one recipient)
• Norman Knight Clinical Support Excellence Award
This award recognizes direct care clinical support staff members within Patient Care Services
who demonstrate patient advocacy, provide care that is compassionate and thoughtful and a
commitment to quality patient care.
Eligibility: PCS direct care clinical support staff Award: $1000 (one recipient)
• Jean M. Nardini, RN, Nurse of Distinction Award
Award was designed to recognize a clinical staff nurse who consistently demonstrates
excellence in clinical practice, leadership and a strong dedication to the profession of
nursing.
Eligibility: Staff nurses in PCS Award: $1000 (one recipient)
55

Attachment 4.3.a
16.15,877
Direct Caregivers
Scheduled Hours Mon Tues Wed Thurs Fri Sat Sun Total Weekly
Shifts
RN 7am-3pm 6.50 6.50 6.50 6.50 6.50 6.00 6.00 44.50
PCA 7am-3pm 2.00 2.00 2.00 2.00 2.00 2.00 2.00 14.00
58.5
RN 3pm-11pm 6.00 6.00 6.00 6.00 6.00 5.00 5.00 40.00
PCA 3pm-11pm 1.50 1.50 1.50 1.50 1.50 1.00 1.00 9.50
49.5
RN 11pm-7am 5.00 5.00 5.00 5.00 5.00 4.00 4.00 33.00
11pm-7am
33.0
141.00
Budgeted FY 2006
Subtotal Shifts
Number of Staff
DAY SHIFT
EVENING SHIFT
NIGHT SHIFT
Pediatrics Med/Surg Combined
Avg. Number of Pts Per Day:Total Patient Days:
Massachusetts General Hospital902 Licensed Beds
Tertiary - Academic Medical Center
Pediatrics Ellison 18
Budget Worked Hours Per Patient Days (WHPPD) 9.98
56
57
MGH - Patient Care ServicesFY'06 Patient Volumes - Patient Classification UnitsYear-to-Date Performance for Fiscal Month EndingSeptember
Census Acuity Workload HPWI SH/24Serv/Unit Budget Actual Variance Budget Actual Variance Budget Actual Variance Budget Actual Variance Budget Actual VarianceCA SICU 13.5 12.3 (1.2) (2.3) (0.17)
(3.2) (0.02) (6.2) (0.24)(0.5) (0.08) (2.4) (0.15)(0.7) (0.07) (3.5) (0.55) (1.2)(2.1) 0.02 (2.7) (0.27) 0.2(7.7) (0.01) (17.1) (0.30)(0.1) (0.04) (1.0) 0.16(1.5) 0.08 (1.6) (0.20)0.7 2.0 (0.50) (2.9)
0.03 (3.3)(0.7) (0.8) (0.76) (4.4)(3.0) (5.1) (0.53) 0.80.3 (0.03) 0.0 (0.55) (1.6)
(0.06) (1.3) (0.38) (1.0)(2.5) 0.01 (2.4) (0.30) (10.1)0.2 1.1 (0.15) (1.7)(0.7) (0.09) (4.4)(0.4) (0.5) (0.69) (2.3)(0.2) 2.1 (0.41) (3.2)1.1 (0.11) (0.74) (2.9)
0.11 (0.16) (3.0)0.16 (2.7)
(2.2)(0.32) (1.8)
(0.01) (0.26) (1.7)0.10 (0.20) (25.9)
0.16 (1.2)(1.2)
(0.04) (1.5)(0.4) (0.4) (0.27) (1.3)0.2 1.5 (0.17) (2.8)(0.7) (0.01) (1.3)0.4 (0.05) (4.3)
(0.12) (2.9)(0.03) (8.5)
(0.4) 0.62 2.7(0.4)(0.6) (0.11) (2.4) (0.97) (0.1)(1.2) 0.10 (0.9) 0.18 1.1(1.0) (0.07) (2.8) (0.10)(2.8) (0.02) (6.10) (0.19)(1.1) 0.07 (0.8) (0.25) (0.3)0.1 (0.07) (0.7) 0.00 0.6
(1.0) (1.5) (0.11)(0.1) 1.6 (0.40) (2.6)(5.5) (3.9) 0.48 5.1(5.6) (2.3)(17.1) 10.9 (0.16) (36.3)
3.41 3.55 0.14 46.0 43.7 6.40 6.57 36.8 35.9 0.9EL 8 27.5 24.3 1.78 1.76 49.0 42.8 5.50 5.74 33.7 30.7 3.0EL 9 CCU 12.6 12.1 2.86 2.78 36.0 33.6 6.40 6.55 28.8 27.5 1.3EL 10 30.2 29.5 1.84 1.77 55.6 52.1 5.50 6.05 38.2 39.4EL 11 31.5 29.4 1.59 1.61 50.1 47.4 5.50 5.77 34.4 34.2Cardiology 115.3 107.6 2.05 2.04 236.7 219.6 5.81 6.11 171.9 167.7 4.2SICU 16.5 16.4 3.75 3.71 61.9 60.9 6.48 6.32 50.1 48.1 2.0BG 13 18.1 16.6 1.97 2.05 35.6 34.0 5.82 6.02 25.9 25.6 0.3BL 6 13.0 13.7 1.68 1.74 0.06 21.8 23.8 5.72 6.22 15.6 18.5WH 7 21.3 23.1 1.8 1.77 1.87 0.10 37.7 43.1 5.4 5.06 5.03 23.8 27.1EL 7 29.8 29.1 1.77 1.78 0.01 52.7 51.9 5.19 5.95 34.2 38.6EL 19 23.8 20.8 1.79 1.80 0.01 42.5 37.4 5.20 5.73 27.6 26.8PH 22 15.1 15.4 1.51 1.48 22.8 22.8 5.20 5.75 14.8 16.4BG 14 22.0 22.0 0.0 1.85 1.79 40.7 39.4 5.06 5.44 25.8 26.8Surgical 159.6 157.1 1.98 1.99 315.7 313.3 5.52 5.82 217.8 227.9MICU 15.2 15.4 2.80 2.83 0.03 42.5 43.6 6.40 6.55 34.0 35.7EL 16 32.5 31.8 1.63 1.85 0.22 52.9 58.7 5.8 5.20 5.29 34.4 38.8PH 20 19.0 18.6 1.63 1.63 0.00 30.9 30.4 5.20 5.89 20.1 22.4PH 21 18.9 18.7 1.75 1.88 0.13 33.0 35.1 5.20 5.61 21.4 24.6BG 9 14.9 16.0 1.94 1.83 28.9 29.2 0.3 5.78 6.52 20.9 23.8BG 11 22.7 23.3 0.6 1.75 1.86 39.7 43.3 3.6 4.85 5.01 24.1 27.1WH 9 22.6 22.6 0.0 1.58 1.82 0.24 35.6 41.1 5.5 5.20 5.04 23.2 25.9WH 8 23.5 24.2 0.7 1.75 1.89 0.14 41.1 45.7 4.6 5.20 5.06 0.14 26.7 28.9WH 10 18.4 18.7 0.3 1.85 1.86 0.01 34.1 34.8 0.7 5.20 5.52 22.2 24.0WH 11 21.4 21.9 0.5 1.88 1.87 40.3 40.9 0.6 5.20 5.46 26.2 27.9Medical 209.1 211.2 2.1 1.81 1.91 379.0 402.8 23.8 5.34 5.54 253.2 279.1EL 14 22.3 22.8 0.5 1.84 1.93 0.09 41.0 43.9 2.9 5.57 5.41 28.5 29.7Oncology 22.3 22.8 0.5 1.84 1.93 0.09 41.0 43.9 2.9 5.57 5.41 0.16 28.5 29.7WH 6 24.4 25.0 0.6 1.49 1.53 0.04 36.4 38.3 1.9 5.20 5.24 23.6 25.1EL 6 29.5 29.1 1.57 1.58 0.01 46.3 45.9 5.20 5.47 30.1 31.4Orthopaedic 53.9 54.1 1.53 1.56 0.03 82.7 84.2 5.19 5.37 53.7 56.5BL 12 15.0 14.3 3.22 3.48 0.26 48.3 49.8 1.5 6.40 6.41 38.6 39.9EL 12 28.7 29.1 1.66 1.85 0.19 47.6 53.8 6.2 5.20 5.25 31.0 35.3WH 12 19.6 20.0 0.4 1.61 1.76 0.15 31.6 35.2 3.6 5.20 5.32 20.5 23.4Neurosciences 63.3 63.4 0.1 2.01 2.19 0.18 127.5 138.8 11.3 5.65 5.68 90.1 98.6BL 11 23.1 22.7 1.74 1.81 0.07 40.2 41.0 0.8 4.58 3.96 23.0 20.3Psychiatric 23.1 22.7 1.74 1.81 0.07 40.2 41.0 0.8 4.58 3.96 0.62 23.0 20.3 2.7PICU 6.4 5.8 2.97 2.86 19.0 16.6 6.40 7.37 15.2 15.3EL 17 14.3 13.1 1.81 1.91 25.9 25.0 5.20 5.02 16.8 15.7EL 18 18.0 17.0 1.72 1.65 30.9 28.1 5.20 5.30 20.1 18.6 1.5Pediatrics 38.7 35.9 1.96 1.94 75.8 69.7 5.50 5.69 52.1 49.6 2.50BG 7 15.4 14.3 1.66 1.73 25.6 24.8 5.20 5.45 16.6 16.9NICU 13.6 13.7 2.45 2.38 33.3 32.6 6.40 6.40 26.7 26.1
Women & Infants 29.0 28.0 2.03 2.05 0.0 58.9 57.4 5.88 5.99 43.3 43.0 0.3EL 13 24.0 23.9 1.18 1.25 0.07 28.3 29.9 5.75 6.15 20.4 23.0BL 13 37.4 31.9 1.10 1.17 0.07 41.1 37.2 5.75 5.27 29.6 24.5Obstetrics 61.4 55.8 1.13 1.20 0.07 69.4 67.1 5.76 5.66 0.10 50.0 47.5 2.5Subtotal 775.7 758.6 1.84 1.90 0.06 1426.9 1437.8 5.51 5.67 983.6 1019.9
Attachment 4.3.b

Attachment 4.3.c
STAFFINGSHIFTS
RN SHIFTS
NON RN SHIFTS
PATIENTISSUES
STAFFISSUES
SUPPORTISSUES
STRUCTUREISSUES
LOGISTICISSUES
HOMOGENEITY OFPATIENT
POPULATION
DESIREDOUTCOMES
CARE STANDARDS
PATIENTEXPECTATIONS
EXPERIENCE/KNOWLEDGE
COMPETENCE/CAPABILITIES
DELIVERY MODEL
STAFF TURNOVER
LEADERSHIP/CLINICAL
OTHERPROFESSIONAL
OTHERANCILLARY
CLERICAL/SERVICE
PHYSICALLAYOUT
SUPPLIES/EQUIPMENT
SYSTEMS
TECHNOLOGY
VARIABILITY OFWORKLOAD
PATIENTTURNOVER
MINIMUMSTAFFING
WHAT ISREASONABLE
HPWI /Resource Intensity Staffing Mix
WORKLOAD / STAFFING
WORKLOAD
VOLUME
CENSUS
UNITS OFSERVICE
ACUITY
COMPLEXITY
CARE NEEDS
58
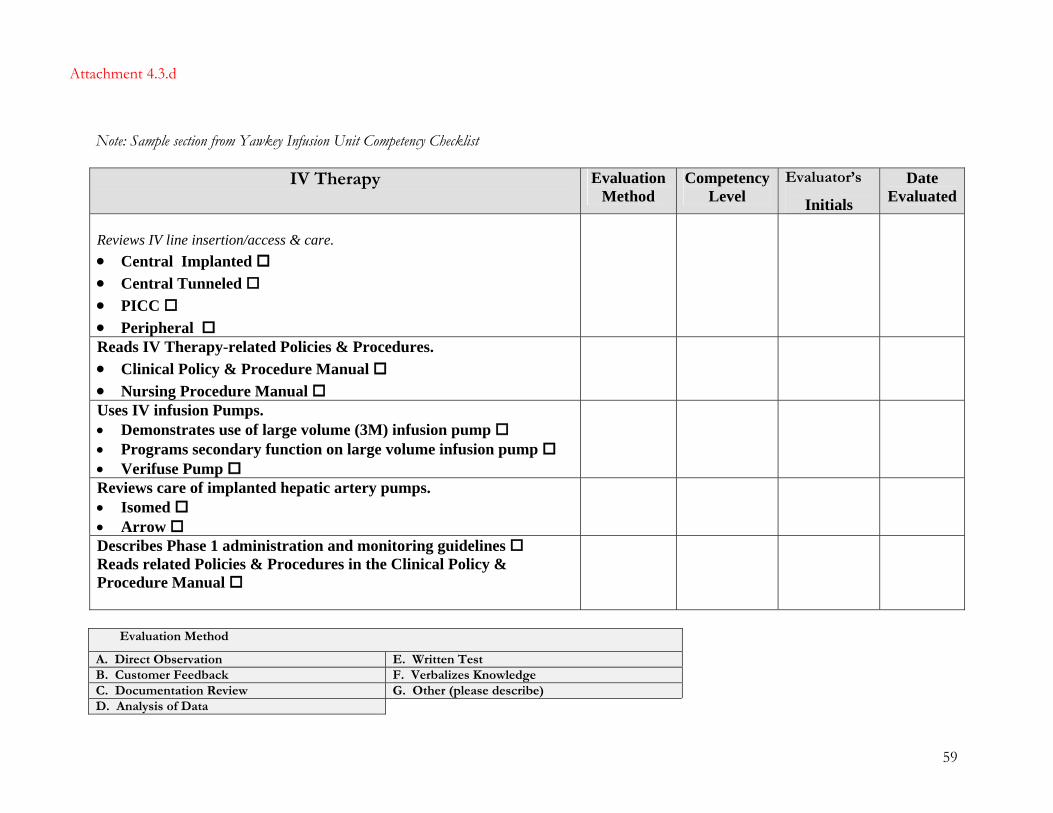
Note: Sample section from Yawkey Infusion Unit Competency Checklist
IV Therapy
Evaluation Method
Competency Level
Evaluator’s
Initials
Date Evaluated
Reviews IV line insertion/access & care. • Central Implanted • Central Tunneled • PICC • Peripheral
Reads IV Therapy-related Policies & Procedures. • Clinical Policy & Procedure Manual • Nursing Procedure Manual
Uses IV infusion Pumps. • Demonstrates use of large volume (3M) infusion pump • Programs secondary function on large volume infusion pump • Verifuse Pump
Reviews care of implanted hepatic artery pumps. • Isomed • Arrow
Describes Phase 1 administration and monitoring guidelines Reads related Policies & Procedures in the Clinical Policy & Procedure Manual
Evaluation Method
A. Direct Observation E. Written Test B. Customer Feedback F. Verbalizes Knowledge C. Documentation Review G. Other (please describe) D. Analysis of Data
Attachment 4.3.d
59

Attachment 4.3.d continued
Sample section from Bigelow 9 (Respiratory Acute Care Unit) Competency Checklist
Care for a Patient Requiring Ventilatory Assistance/Respiratory Support
Evaluation Method
Competency Level
Evaluator’s
Initials
Date Evaluated
Demonstrates set-up of pulse oximeter A Demonstrates set-up of oxygen delivery system. A Moniters mechanical ventilation A Ambus and suctions artificial airways, NT suctioning A Changes ET tube tape and rotates tube A Performs tracheostomy care A Interperts ABG’s F Collects sterile tracheal sputum specimen A Assists with intubation/extubation A Assists with weaning A Cares for the patient on noninvasive ventilation A Flolan Administration Packet F Mechanical Ventilation Packet F Score >85 on Respiratory Exam E
Evaluation Method
A. Direct Observation E. Written Test B. Customer Feedback F. Verbalizes Knowledge C. Documentation Review G. Other (please describe) D. Analysis of Data
60
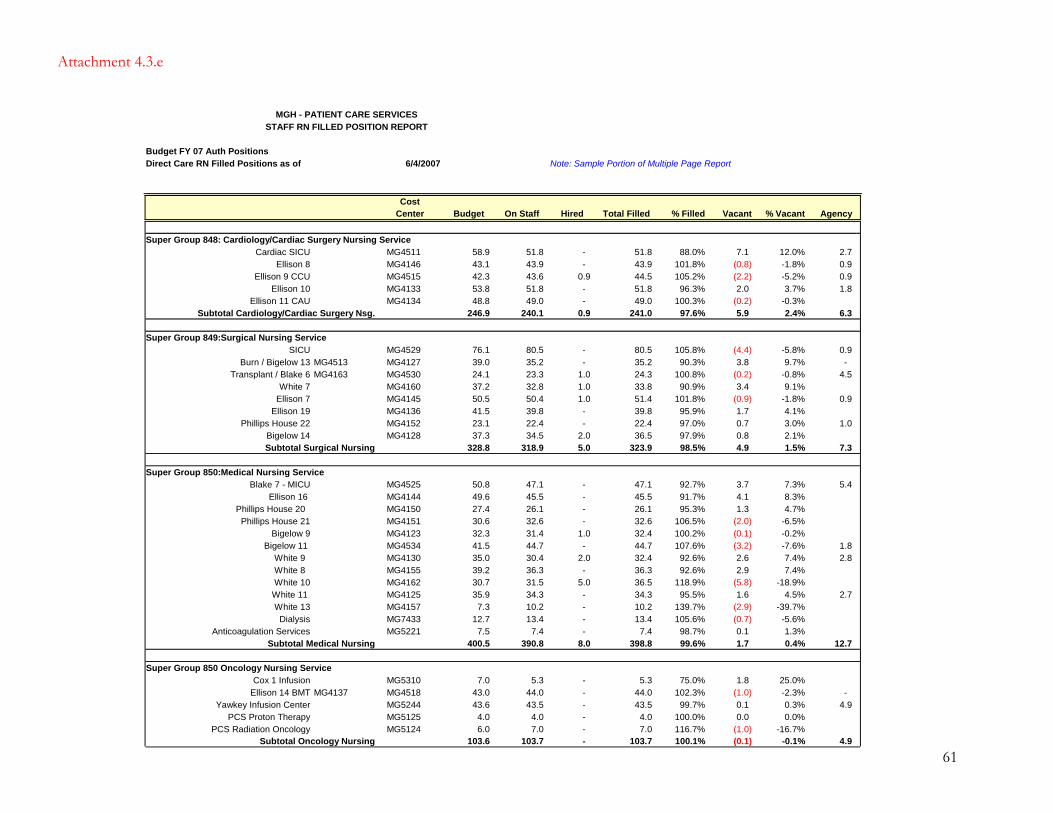
MGH - PATIENT CARE SERVICESSTAFF RN FILLED POSITION REPORT
Budget FY 07 Auth Positions Direct Care RN Filled Positions as of 6/4/2007 Note: Sample Portion of Multiple Page Report
CostCenter Budget On Staff Hired Total Filled % Filled Vacant % Vacant Agency
Super Group 848: Cardiology/Cardiac Surgery Nursing ServiceCardiac SICU MG4511 58.9 51.8 - 51.8 88.0% 7.1 12.0% 2.7
Ellison 8 MG4146 43.1 43.9 - 43.9 101.8% (0.8)(2.2)2.0
(0.2)5.9
(4.4)3.8
(0.2)3.4
(0.9)1.7
(2.0)(0.1)(3.2)2.6
(5.8)1.6
(2.9)(0.7)0.1
(1.0)0.1
-1.8% 0.9 Ellison 9 CCU MG4515 42.3 43.6 0.9 44.5 105.2% -5.2% 0.9
Ellison 10 MG4133 53.8 51.8 - 51.8 96.3% 3.7% 1.8 Ellison 11 CAU MG4134 48.8 49.0 - 49.0 100.3% -0.3%
Subtotal Cardiology/Cardiac Surgery Nsg. 246.9 240.1 0.9 241.0 97.6% 2.4% 6.3
Super Group 849:Surgical Nursing ServiceSICU MG4529 76.1 80.5 - 80.5 105.8% -5.8% 0.9
Burn / Bigelow 13 MG4513 MG4127 39.0 35.2 - 35.2 90.3% 9.7% - Transplant / Blake 6 MG4163 MG4530 24.1 23.3 1.0 24.3 100.8% -0.8% 4.5
White 7 MG4160 37.2 32.8 1.0 33.8 90.9% 9.1%Ellison 7 MG4145 50.5 50.4 1.0 51.4 101.8% -1.8% 0.9
Ellison 19 MG4136 41.5 39.8 - 39.8 95.9% 4.1%Phillips House 22 MG4152 23.1 22.4 - 22.4 97.0% 0.7 3.0% 1.0
Bigelow 14 MG4128 37.3 34.5 2.0 36.5 97.9% 0.8 2.1%Subtotal Surgical Nursing 328.8 318.9 5.0 323.9 98.5% 4.9 1.5% 7.3
Super Group 850:Medical Nursing ServiceBlake 7 - MICU MG4525 50.8 47.1 - 47.1 92.7% 3.7 7.3% 5.4
Ellison 16 MG4144 49.6 45.5 - 45.5 91.7% 4.1 8.3%Phillips House 20 MG4150 27.4 26.1 - 26.1 95.3% 1.3 4.7%
Phillips House 21 MG4151 30.6 32.6 - 32.6 106.5% -6.5%Bigelow 9 MG4123 32.3 31.4 1.0 32.4 100.2% -0.2%
Bigelow 11 MG4534 41.5 44.7 - 44.7 107.6% -7.6% 1.8 White 9 MG4130 35.0 30.4 2.0 32.4 92.6% 7.4% 2.8 White 8 MG4155 39.2 36.3 - 36.3 92.6% 2.9 7.4%White 10 MG4162 30.7 31.5 5.0 36.5 118.9% -18.9%White 11 MG4125 35.9 34.3 - 34.3 95.5% 4.5% 2.7 White 13 MG4157 7.3 10.2 - 10.2 139.7% -39.7%
Dialysis MG7433 12.7 13.4 - 13.4 105.6% -5.6%Anticoagulation Services MG5221 7.5 7.4 - 7.4 98.7% 1.3%
Subtotal Medical Nursing 400.5 390.8 8.0 398.8 99.6% 1.7 0.4% 12.7
Super Group 850 Oncology Nursing ServiceCox 1 Infusion MG5310 7.0 5.3 - 5.3 75.0% 1.8 25.0%
Ellison 14 BMT MG4137 MG4518 43.0 44.0 - 44.0 102.3% -2.3% - Yawkey Infusion Center MG5244 43.6 43.5 - 43.5 99.7% 0.3% 4.9
PCS Proton Therapy MG5125 4.0 4.0 - 4.0 100.0% 0.0 0.0%PCS Radiation Oncology MG5124 6.0 7.0 - 7.0 116.7% (1.0) -16.7%
Subtotal Oncology Nursing 103.6 103.7 - 103.7 100.1% (0.1) -0.1% 4.9
Attachment 4.3.e
61
62
Attachment 4.3.f
MASSACHUSETTS GENERAL HOSPITAL Department of Nursing
TITLE: COMPETENCE OF LICENSED AND UNLICENSED PERSONNEL POLICY: The manager is accountable for assessment of staff competency. A manager may delegate
this function to a designee who is skilled in competency assessment. COMPETENCE OF LICENSED CLINICIANS
The competence of licensed clinicians who practice at Massachusetts General Hospital is maintained through a combination of ongoing competence assessment and educational activities. Documentation of competence assessment is required and includes the following elements:
A. Licensure B. Completion of a competency based orientation with a preceptor C. Performance appraisal D. Annual required training E. Hospital, departmental and/or unit-specific competency achievement F. Management of age specific needs of patients (Attachment A) G. Inservice and educational activities H. Completion of cross-training (if applicable)
Optional Element: I. Professional certification
COMPETENCE OF UNLICENSED PERSONNEL POLICY: The competence of unlicensed personnel who practice at Massachusetts General Hospital
is maintained through a combination of ongoing competence assessment and educational activities. Documentation of competence assessment is required and includes the following elements:
A. Completion of a competency based orientation B. Performance Appraisal C. Annual required training D. Hospital, departmental and/or unit-specific competency achievement E. Age-specific care of patients (Attachment B) F. Inservice and educational activities G. Completion of cross-training (if applicable)
Attachment 4.3.f continued ADMINISTRATIVE PROCEDURE: 1. Annually, The Knight Nursing Center for Clinical and Professional Development will coordinate
review and/or revision of competencies to be assessed. 2. The Knight Nursing Center will communicate the competencies to clinical leadership prior to the
implementation time-line. 3. The manager will designate an evaluator(s) for his/her practice area. 4. The evaluator will document on the Annual Competency Assessment and Required Training Record,
the employee’s ability to meet identified competencies. The remainder of Record will be completed by each employee and reviewed by the evaluator at the time of performance evaluation.
5. The Annual Competency Assessment and Required Training Record will be attached to the
completed Performance Appraisal at the time of evaluation and retained in the employee’s file in Staff Records. (see Performance Evaluation policy in the Human Resources Policy and Procedure Manual, http://is.partners.org/hr/manual/manual/manual/perfomance.htm)
Revised and approved: Department of Nursing 8/20/02 Revised and approved: Nursing Executive Operations 08/06
63

Attachment 4.3.g Massachusetts General Hospital Department of Nursing
Annual Competency Assessment 10/1/06-9/30/07
Direct Care Providers
Employee Name: Number:
Evaluation Method Competency Levels A. Direct Observation B. Customer Feedback C. Documentation Review D. Analysis of Data
E. Written Test F. Verbalizes Knowledge G. Other (please describe)
1. Competency Met 2. Competency Not Met 3. Not Applicable
Competency Suggested
Evaluation Method
Competency Level
Competency Evaluator’s Signature
Date Evaluated
Verifies patient identification using two identifiers prior to providing care.
A, B, F
Uses on-line safety reports for all patient, employee and visitor incidents/events.
A, B, C, D, F
Provides age-specific care (Nursing Practice Manual 1.42.01). Check all that apply: Neonate Infant
Toddler Preschool School Age Adolescent Adult
Elder (Older Adult)
A, B, C, E
RN’s only: Performs read-back of critical lab values, verbal and telephone orders
A, B
RN’s only: Transcribes patient orders utilizing approved abbreviations
A, C
RN’s only: Performs safe handoffs of patients
A, B
RN’s only: Completes medication reconciliation process on assigned patients
A, C, D, F
RN’s only: Administers blood products in accordance with MGH policies/procedures*see below
A, B, C, D, E, F
Note: For any unmet competencies, please include your comments and a developmental action plan for improvement in Section X of the employee’s performance appraisal. * Blood Transfusion Competency: • Blake 11 is excluded from this requirement – RNs will remain verifiers only • General care units will have Blood Transfusion Post-test and Transfusion Competency
Assessment with administration of a blood product • Specialty care units will answer post-test questions in annual competency assessment
materials packet
64
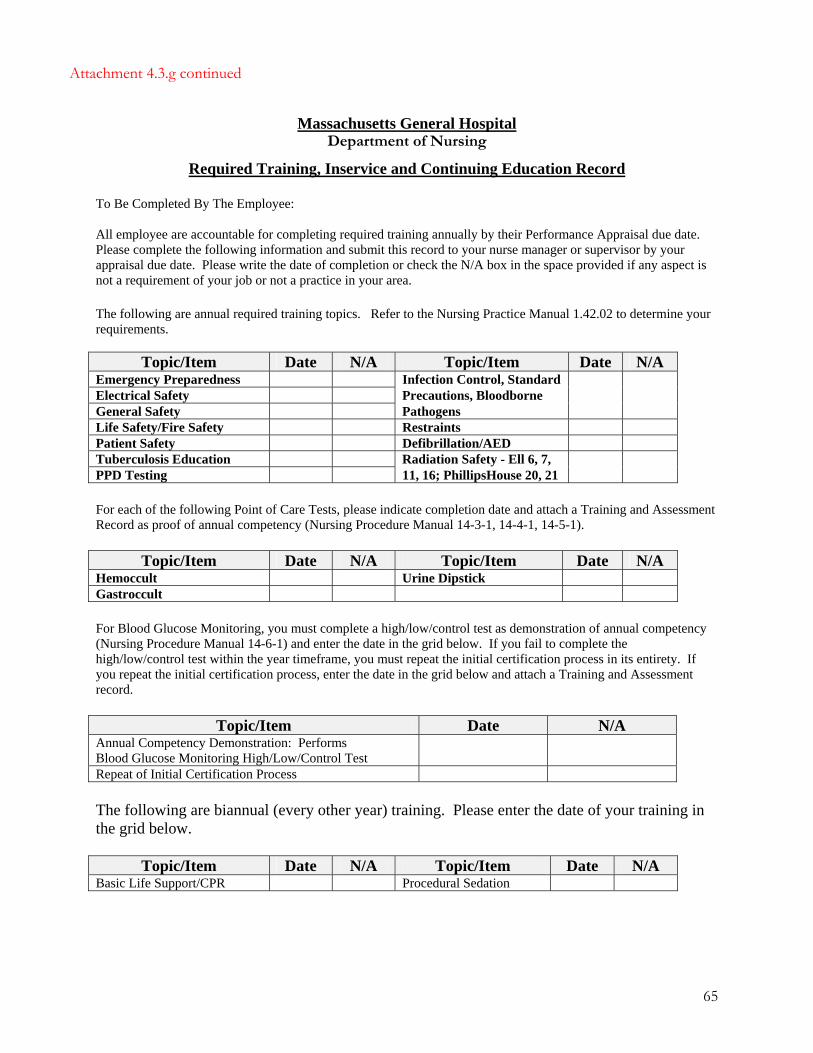
Attachment 4.3.g continued
Massachusetts General Hospital Department of Nursing
Required Training, Inservice and Continuing Education Record
To Be Completed By The Employee: All employee are accountable for completing required training annually by their Performance Appraisal due date. Please complete the following information and submit this record to your nurse manager or supervisor by your appraisal due date. Please write the date of completion or check the N/A box in the space provided if any aspect is not a requirement of your job or not a practice in your area. The following are annual required training topics. Refer to the Nursing Practice Manual 1.42.02 to determine your requirements.
Topic/Item Date N/A Topic/Item Date N/A Emergency Preparedness Infection Control, Standard Electrical Safety Precautions, Bloodborne General Safety Pathogens Life Safety/Fire Safety Restraints Patient Safety Defibrillation/AED Tuberculosis Education Radiation Safety - Ell 6, 7, PPD Testing 11, 16; PhillipsHouse 20, 21 For each of the following Point of Care Tests, please indicate completion date and attach a Training and Assessment Record as proof of annual competency (Nursing Procedure Manual 14-3-1, 14-4-1, 14-5-1).
Topic/Item Date N/A Topic/Item Date N/A Hemoccult Urine Dipstick Gastroccult For Blood Glucose Monitoring, you must complete a high/low/control test as demonstration of annual competency (Nursing Procedure Manual 14-6-1) and enter the date in the grid below. If you fail to complete the high/low/control test within the year timeframe, you must repeat the initial certification process in its entirety. If you repeat the initial certification process, enter the date in the grid below and attach a Training and Assessment record.
Topic/Item Date N/A Annual Competency Demonstration: Performs Blood Glucose Monitoring High/Low/Control Test
Repeat of Initial Certification Process The following are biannual (every other year) training. Please enter the date of your training in the grid below.
Topic/Item Date N/A Topic/Item Date N/A Basic Life Support/CPR Procedural Sedation
65

66
Attachment 4.3.g continued Continuing Education and Training: Include any internal/external presentations, programs, seminars and/or job training you have attended. Include the date you attended in the space provided. Attach additional sheets as required. Inservice Education: Include any equipment and policy/procedure inservices you have attended in the past year. Include the date you completed the training/education in the space provided. Attach additional sheets as required. Other Activities and Certifications: Include items such as committee memberships, special projects, publishing, or advanced certifications such as ACLS or CCRN. _____ _________________ __________________
Employee Signature Date







