
A Rainbow Primary Care
for India
A Concept Paper Dr Shyam Ashtekar

In 1940!
The Pre-Independence Effort
In 1940!
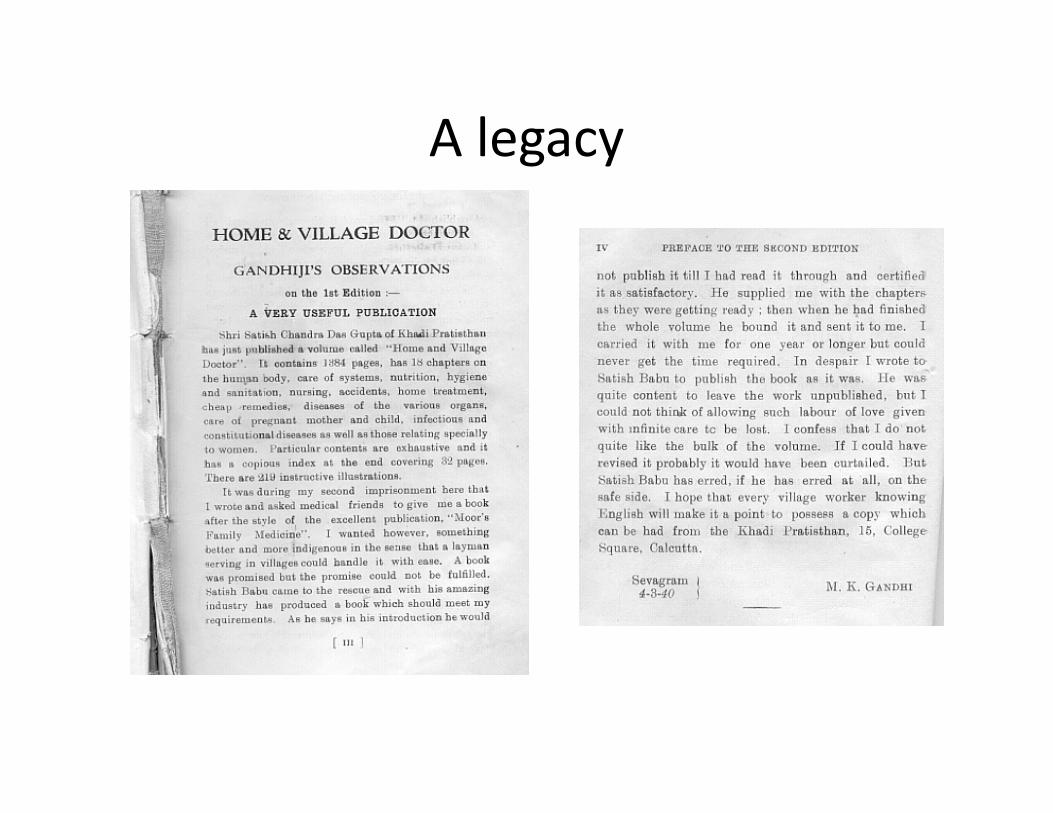
A legacy

Keywords
• Pluralistic Primary care,
• AYUSH,
• Draft NHP2015,
• National Health Assurance Mission, • National Health Assurance Mission,
• Flexi-learning,
• Health Centers,
• Legalities
A window of opportunity for new
primary care
• NHP 2015 and NHAM provide a free and
comprehensive primary care for all
• Intention of including AYUSH along with
AllopathyAllopathy
• Intention of taking primary care deeper in
public health system, and in private care
• Renewed commitment to B.Sc Health Science
• A separate ministry of AYUSH

The Large Ground Realities
Quacks galore in Purniya Bihar 2013
The ubiquitous Zolachhap doc in UP 2013

The varying contexts of primary care in India.
• States vary widely in doc density.
• This changes the primary care scenario in various states
• South, western and Delhi • South, western and Delhi Punjab JK have higher doc density and may be difficult for a new primary care
• But many other states need and can benefit from new primary care,
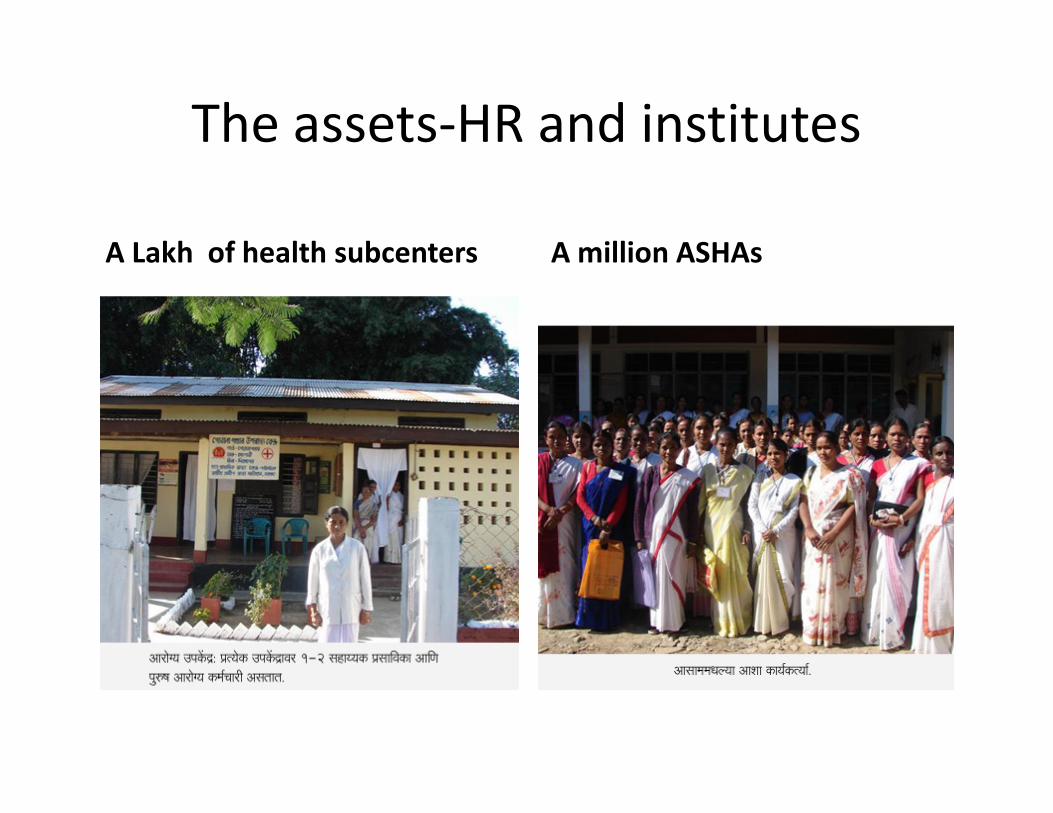
The assets-HR and institutes
A Lakh of health subcenters
100000 Health subcenters
A million ASHAs

To rebuild new primary care..
• HR--AYUSH doctors, ASHAs, paramedics, informal doctors
• Institutes-health subcenters, village panchayats equipped with 72ndpanchayats equipped with 72amendment.
• NHAM, CSR (Corporate Social Responsibility) and AYUSH funds
• New courses and bridge courses for primary care

Need for AYUSH in mainstream
primary care
• Despite limited and disputed evidence of efficacy, the current Allopathy practice is driven by its industry and market network
• The four solid reasons for integration are (a) internal medical value of AYUSH (b) Wide internal medical value of AYUSH (b) Wide resource base in terms of HR and material (c) Cost advantages (d) an alternative pathway for our health system.
• AYUSH is one way of avoiding the rising hegemony of Modern Medicine over the national health system.
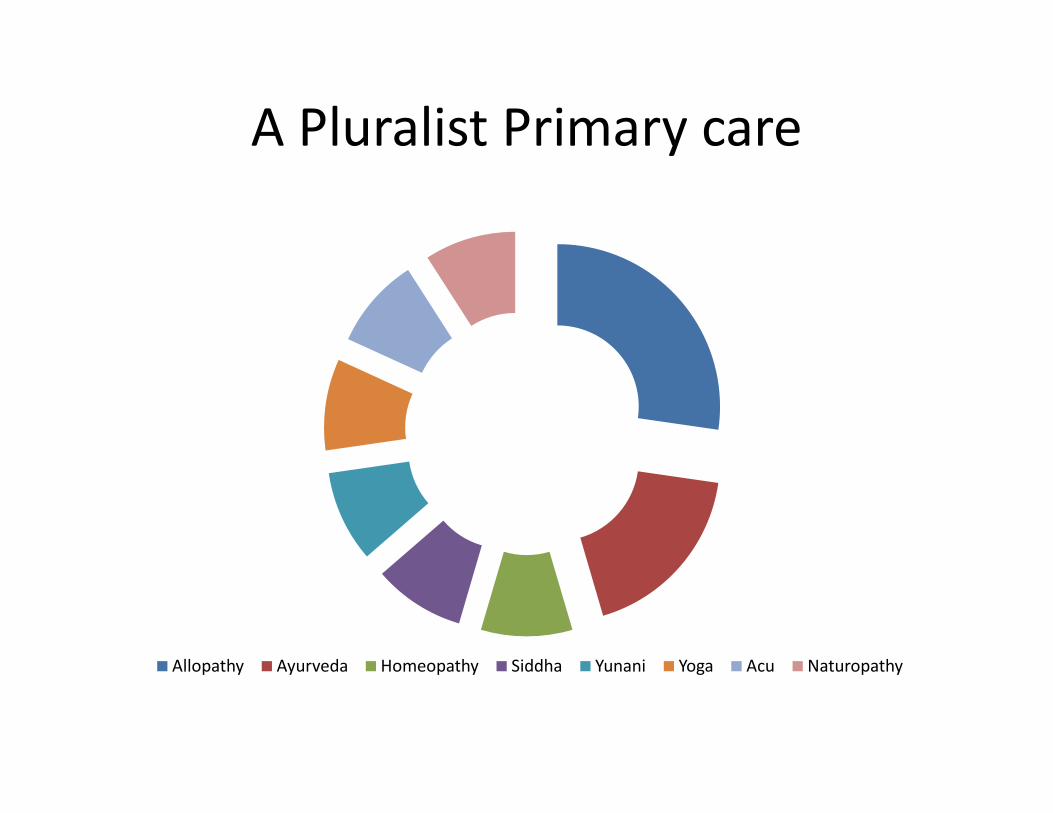
A Pluralist Primary care
Allopathy Ayurveda Homeopathy Siddha Yunani Yoga Acu Naturopathy
Academic Framework for new primary care
• We need an Omnibus GP or primary care program, preferably registered with a separate board that will allow a pluralistic care. But this is a long term solution.
• Two levels of training programs are necessary—(a) paramedics/nurses and (b) GPs/basic doctors. At Subcenter level we will need new paramedics with essential skills in primary care.primary care.
• Along with basics of various healing systems, a problem based approach, with an epidemiological/regional selection of 50-100 problems is helpful for specifics. (like for instance what are the various options/approaches for common cold or back pain)
• (Ref Manual-My book on primary care: Health & Healing (Orient Longman 2000) now out of print.)
Institutes and methods
• We will need genuine institutes and integrated hospitals for training in new primary care.
• Customized Academic programs are necessary combining (a) face to face conventional combining (a) face to face conventional education with (b) distance learning components for practicing professionals.
• A system of credit points will be suitable for Continuous Medical Education (CME) and distance learning programs.

Using IT platforms
• Using IT platforms for all the learning
material, CME, tests and updating will help us
build curricula in short span of time (say even
one year) and even launch programs as we one year) and even launch programs as we
develop such material.

Research and Development for new Primary care
• Modern medicine has banked too much on clinico- pathological diagnosis
• But ISM and Homeopathy have different approaches.
• We need more brainstorming and EBM (Evidence • We need more brainstorming and EBM (Evidence Based Medicine) to develop guidelines for an integrated primary care.
• These guidelines will be used in a public/Government system across states and hence need to be legally defensible.

Beyond RCTs
• In the long run, we will need a body of EBM on integrated primary care, and for that we may need more research models than just the RCTs (Randomized Control Trials).
• There are academic and research methodology • There are academic and research methodology issues about testing and proving holistic approaches versus the reductionist approaches of Allopathy.
• This subject needs a closer look for working out solutions within the larger framework of inter pathy research and AYUSH mission.
Legal issues of integration for new primary care
• To start with, all three councils –Modern Medicine or Allopathy, Indian Medicine, Homeopathy are separate entities.
• In ISM, Ayurveda, Sidha and Yunani have separate registries.
• Naturopathy and Yoga are not recognized as healing • Naturopathy and Yoga are not recognized as healing systems for separate registration.
• Essentially, any academic program has to have a mandate from the respective council, list of institutes offering an approved course like this one, and individual registration with respective state council for the said practice of that science/healing system.

One law for ‘two
countries’
• We are straddling ‘two countries’--
India and Bharat with one MCI
act. While regulation looks right in
India (cities & towns mainly), it
renders most of Bharat’s doctors renders most of Bharat’s doctors
and practice illegal.
• We need accomodative/ promtive
legal provisions for rural areas.
Legal Options
• The Parliament will have to revisit the council acts, find a solution to successful integration of AAYUSH at the level of primary care.
• One way is to merge the various councils and make a single HHR (Health Human Resources) council
• Another way, for the short term, is to get the MCI to • Another way, for the short term, is to get the MCI to run 1-2 year bridge courses for other graduates allowing limited list of remedies (say 30-50), get appropriate separate registration for them with state councils.
• We can have a shortcut by decontrolling some 30-50 essential primary generic medicines on the counter

Need--A new Board for primary care
• For primary care/integrated GP, we may finally
need a new Board that can run such
courses, register practitioners and function
like a state council mandated by the three like a state council mandated by the three
central councils.

A Roadmap to AAYUSH Primary Care
Area Short term measures Long term measures Remarks
1 Legal issues Need to free some 30-50
allopathic medicines for
popular use, with adequate
information in local languages
Parliamentary legal remedy to
pool various councils, launch a
AAYUSH Graduate program
Calls for advocacy and take
IMA along.
2 Academic Prepare a syllabus for AAYUSH
level 1 (1 yr bridge for
practicing) & level 2 (4Y) for
Integrated and EBM research
through academic and service
institutes
Need to work out
integrated protocols,
research protocols and practicing) & level 2 (4Y) for
fresh students programs
institutes research protocols and
approval mechanisms
3 Infrastructure Start AYUSH OPDs at
Subcenters with help of part
time AYUSH doctors
Integrated AAYUSH hospitals
for learning centers
Need to review the
National AYUSH Mission &
NHAM policy
4 Finance The AYUSH mission has
provisions for health system
institutes
Need to popularize AAYUSH
through NHAM, non-profit
and private providers, so that
it gets its shares in private
spending.
It is necessary that AYUSH
not be equated with Govt
facilities alone.
Conclusion
• Primary care is an essential foundation for building any national
health system.
• However we need to rework the existing systems.
• An integrated AAYUSH based primary care is essential to the
health of the people and to that of the larger health system.
• We need to build the academic system support for this, find • We need to build the academic system support for this, find
legal remedies at central /state levels and decide strategies in
various states to work in both public and private sector.
• AYUSH has been waiting to join the mainstream for long,.
• A political solution is necessary to break the impasse between
systems. May be the Parliament takes a call.
• Such an integrated effort will be a lasting national asset.

Our Hindi
website for
primary care

Thanks
Dr Shyam Ashtekar
Website: bharatswasthya.net &
arogyavidya.net
Nashik, Maharashtra, Cell
09422271544







