
Dr Tannouri.FCHU-NDS, Bybols Lebanon
MEIH, Bsalim, Lebanon
RHUH, Beirut Lebanon
ABLATION RENAL CELL CARCINOMA

RCC• Most common primary renal malignant neoplasm in
adults• 90% of renal tumors• Peaks 55-84 years old• 20% with metastatic disease• 2% with simultaneous bilateral disease• Increasing incidental detection in the early stage
( widespread use of medical imaging- incidentaloma)

CLASSIFICATION OF RENAL CORTICAL TUMORS
• Subdivided into benign and malignant neoplasms by documented genetic abnormalities
• Benign: Angiomyolipoma and Oncocytoma
• Malignant tumors sub-classified into: • Conventional • Papillary • Chromophobe • Collecting duct carcinoma• Medullary carcinoma• Unclassifiable

RCC PROGNOSIS• Depend on
• Size• Localization• Type• Renal function
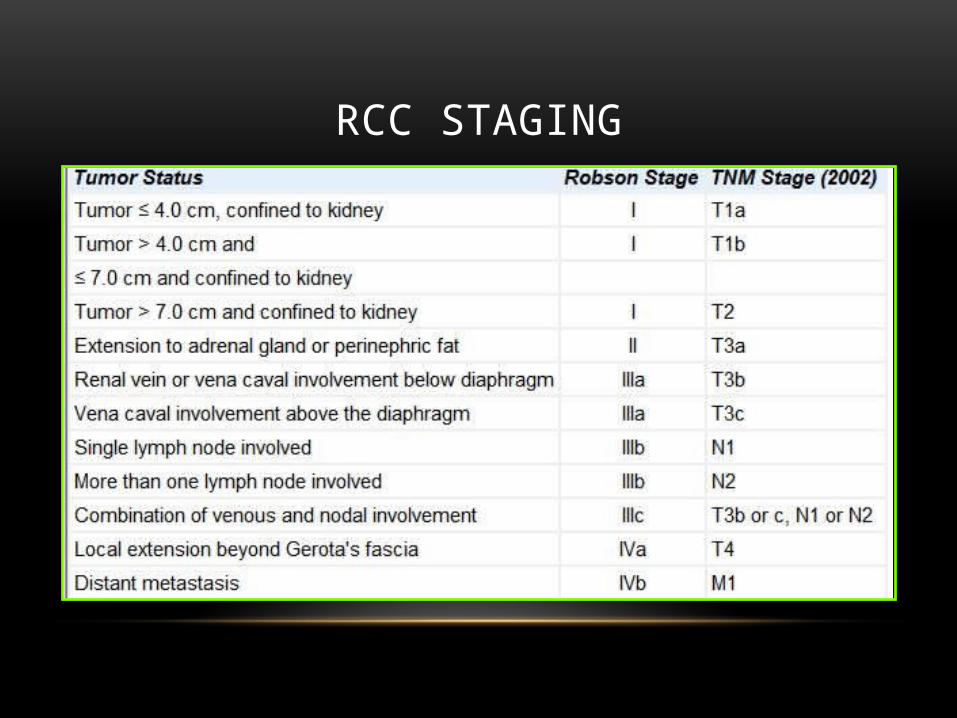
RCC STAGING

RCC /PROGNOSIS -STAGE• Survival after surgical resection
• Suvival for unresectable RCC is <20% at 5 years
5 Yrs 10Yrs
T1 95 91
T2 80 70
T3 59
T4 20
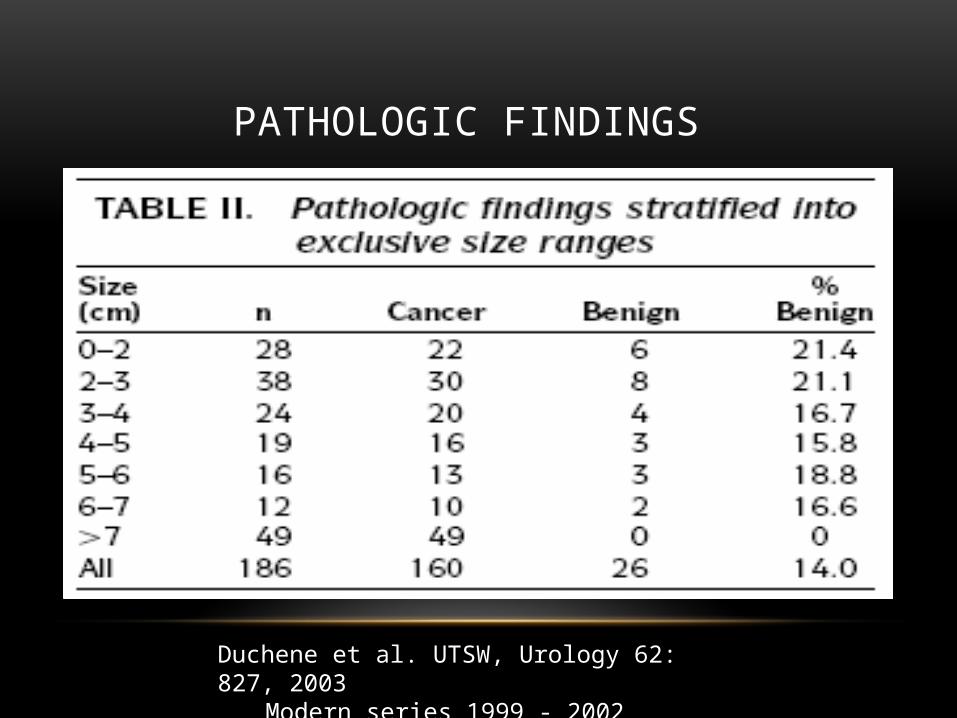
PATHOLOGIC FINDINGS
Duchene et al. UTSW, Urology 62: 827, 2003Modern series 1999 - 2002

TYPE OF RCC AND METASTATIC POTENTIAL• McKiernan, et al. J Urol 2002
• Partial nephrectomy for renal cortical tumors (T1a) -pathologic findings and impact on outcome
• Histological findings• conventional 148 cases• papillary 54 • oncocytoma 32• chromophobe carcinoma 21
• 5-year recurrence rate of 12% for conventional• No recurrence seen in any other RCT
Tumor of low metastatic potential• Chromophobe RCC• Papillary RCC, Type 1
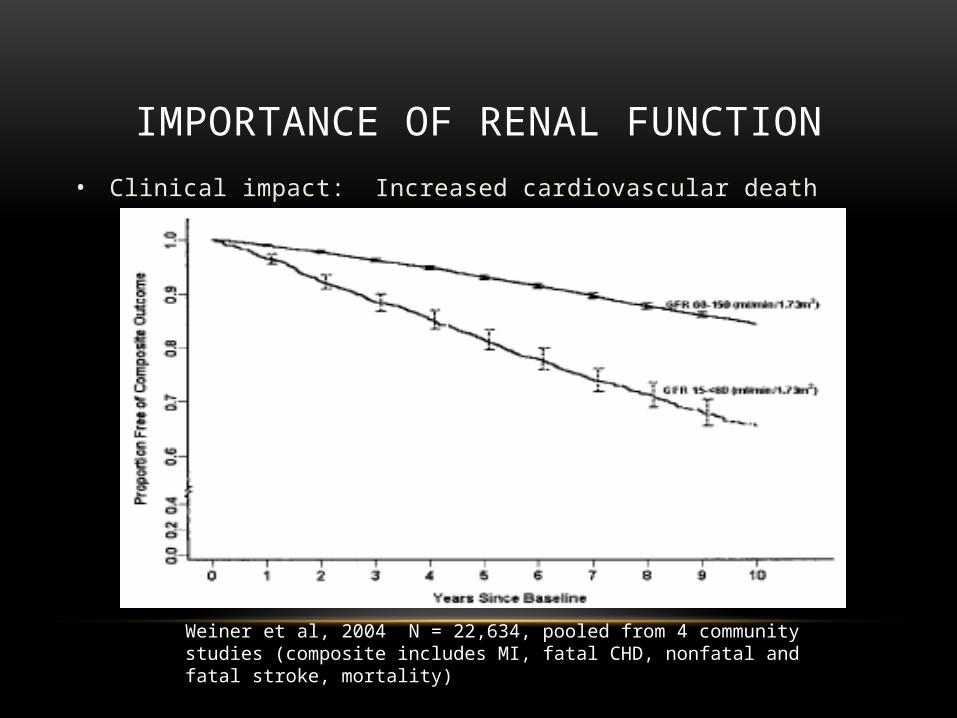
IMPORTANCE OF RENAL FUNCTION• Clinical impact: Increased cardiovascular death
Weiner et al, 2004 N = 22,634, pooled from 4 community studies (composite includes MI, fatal CHD, nonfatal and fatal stroke, mortality)
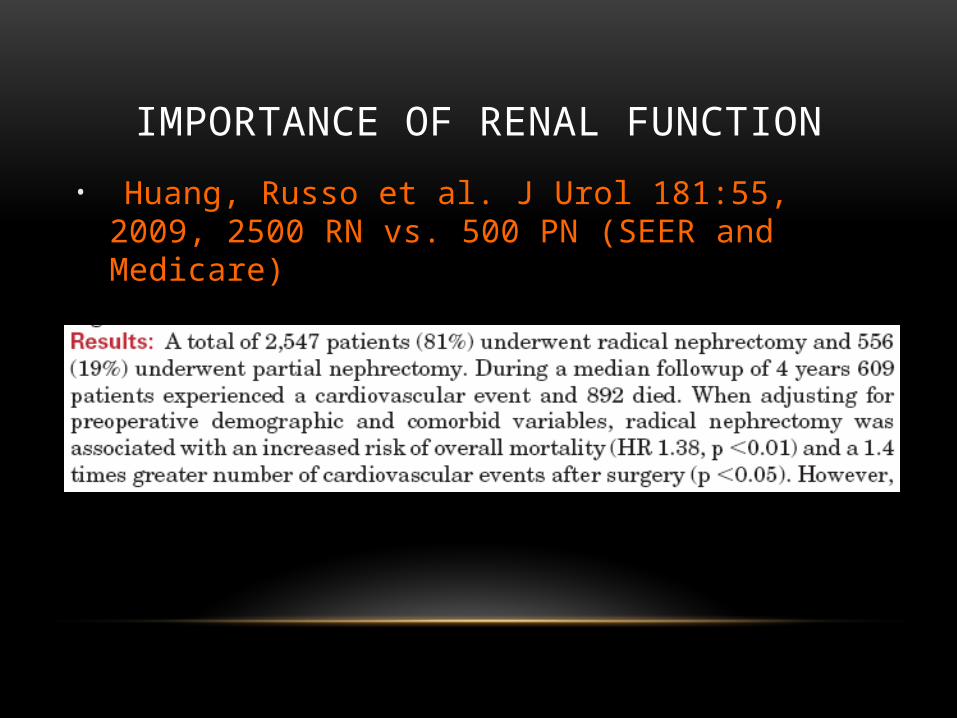
IMPORTANCE OF RENAL FUNCTION
• Huang, Russo et al. J Urol 181:55, 2009, 2500 RN vs. 500 PN (SEER and Medicare)
FUNDAMENTALS OF RENAL CORTICAL TUMOR MANAGEMENT
• 20% are benign• 30% of T1a RCC are low metastatic potential• Standard surgical treatments
• increase risk of developing CKD• CKD Stage 3
• 20% increase risk of death• 40% increase risk of cardiac event
• Saving kidney function more likely to impact survival!!!
RCC T1A SAVING RENAL FUNCTION
• Active surveillance• Nephron –conserving surgery Open or
laparoscopic partial nephrectomy (gold standard)• Minimal invasive technics
• Mainly in High risk patients
MINIMAL INVASIVE SURGERY• Radiofrequency ablation (RFA)• Renal cryotherapy (Cryo)
• Microwave thermotherapy (MW)• Irreversible Electroporation (IRE)• High intensity focused ultrasound (HIFU)• Intracavitary photon irradiation
• Recent studies report mid- and long-term oncology control equivalent to surgery(1)
1.Zagoria RJ, Pettus JA, Rogers M, et al. Long-term outcomes after percutaneous radiofrequency ablation for renal cell carcinoma. Urology. 2011;77(6):1393–7
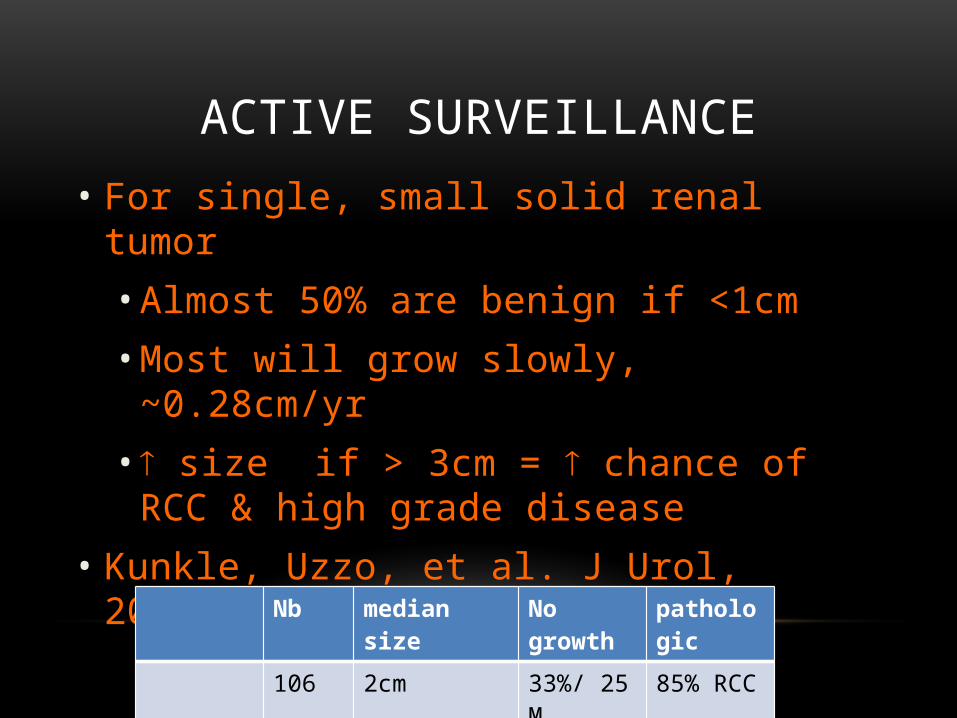
ACTIVE SURVEILLANCE
• For single, small solid renal tumor• Almost 50% are benign if <1cm • Most will grow slowly, ~0.28cm/yr• size if > 3cm = chance of RCC &
high grade disease • Kunkle, Uzzo, et al. J Urol, 2007.
Nb median size No growth pathologic106 2cm 33%/ 25 M 85% RCC
progression 1 2 to 8cm 1% 54 M
ACTIVE SURVEILLANCE DISADVANTAGE
• Outcome not predicted • Real metastatic potential
• Frequent surveillance studies (+ biopsy?)• Anxiety• Patients refuse the strategy
• Excision

OPEN VERSUS LAPAROSCOPIC PARTIAL NEPHRECTOMY
Item Lap. Open P valueNo. of pts. 100 100Med. Tumor size.
2.8 cm 3.3 cm 0.005Solitary kidney 7 28 0.001Central tumor 35% 33% 0.83Med.Preop. Creatinine
1.0 mg/dL 1.0 mg/dL
Med. Surgical time
3 hours 3.9 hours < 0.001
Gill IS,Matin,Desai, et al;J Urol. 2003

OPEN VERSUS LAPAROSCOPIC PARTIAL NEPHRECTOMY
Item Lap. Open P valueBlood loss 125ml 250ml < 0.001Warm ischemia time
28 min 18 min < 0.001
Analgesia requirement
20.2 mg MS 252.5 mg MS < 0.001
Hospital stay 2 days 5 days < 0.001Convalescence 4 weeks 6 weeks < 0.001Intraop. Comp. 5% 0% 0.02Postop. Comp. 9% 14% 0.27
Gill IS,Matin,Desai, et al;J Urol. 2003

OPEN VERSUS LAPAROSCOPIC PARTIAL NEPHRECTOMY
Item Lap. Open P valueTumor size 2.4 cm 2.5 cm 0.50Intraop. Cost 20.1%
greater< 0.001
Postop. cost 55% lesser < 0.001Overall hospital cost
15.6% lesser
0.002
Gill IS,Matin,Desai, et al;J Urol. 2003

COMPLICATIONS

PERCUTANEOUS ABLATION

MINIMAL INVASIVE SURGERY - ADVANTAGES
• Nephron-sparing
• Many tumors are slow growing/ low aggressiveness
• Low morbidity
• Fewer complications
• Outpatient (or overnight stay only)

MINIMAL INVASIVE SURGERY - POSSIBLE RISK
• Tumor left in situ
• Ablation success defined as NO enhancement on CT/MRI and tumor shrinkage (Secure margins?)
• Long term RCC control unknown

ABLATION RCC
• Specific consideration in RCC ablation comparing to liver ablation• Anatomical consideration (tumor localization)• Higher risk of adjacent organ injury• Higher Heat –sink effect due to high
vascularity if using RF

ANATOMICAL CONSIDERATION• Anterior or Posterior location• Central location
• Lower success rate• risk of collecting system or vascular injury
• Tumor size • <3cm single session • 3< T>5 multiple session
ANATOMICAL CONSIDERATION
• CT scan the best medical imaging tool (US MRI)• Adjacent organs
• Small and large bowel• Ureters• Genitofemoral and ilioinguinal nerves• Psoas muscle• Adrenal gland

ABLATION RCC TRICKS• Cold Pyeloperfusion Technique
• Used when the renal tumour is centrally located • Or the treated tumour margin was close to the
ureter• Hydrodissection Technique
• Close proximity to bowel loops during treatment• Location of the tumour (anterior and mid-polar ) • Lack of intra-abdominal fat
HEAT SINK EFFECT• More heat-sink effect due to high perfusion organ
• Repeat ablation cycle especially in high perfused tissue• Delay impedance rises• Lower temperatures during or just after RF
ablation
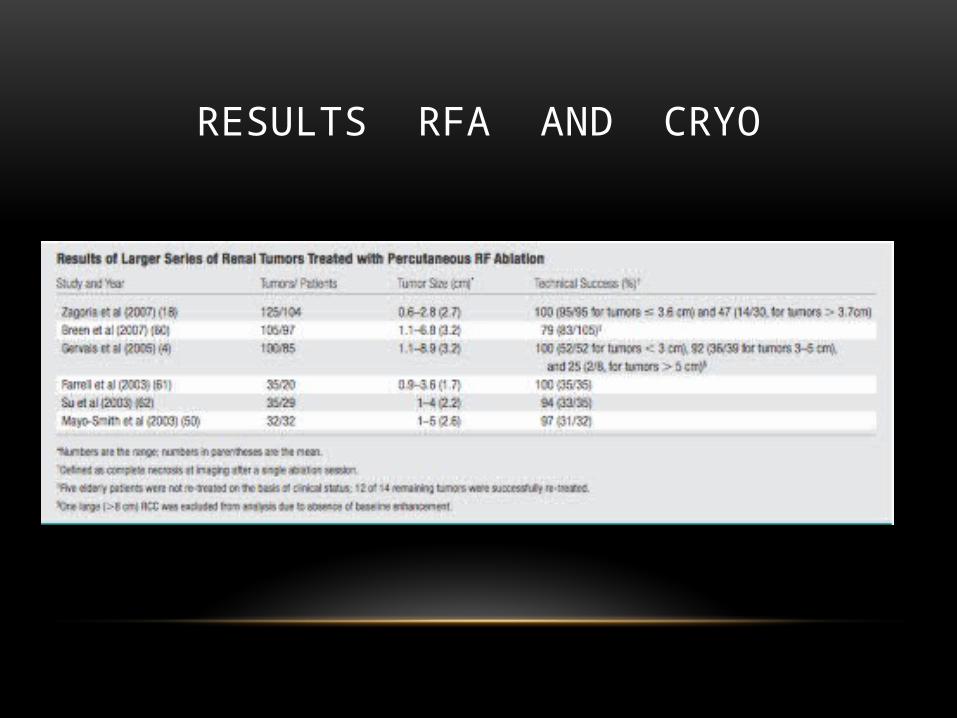
RESULTS RFA AND CRYO
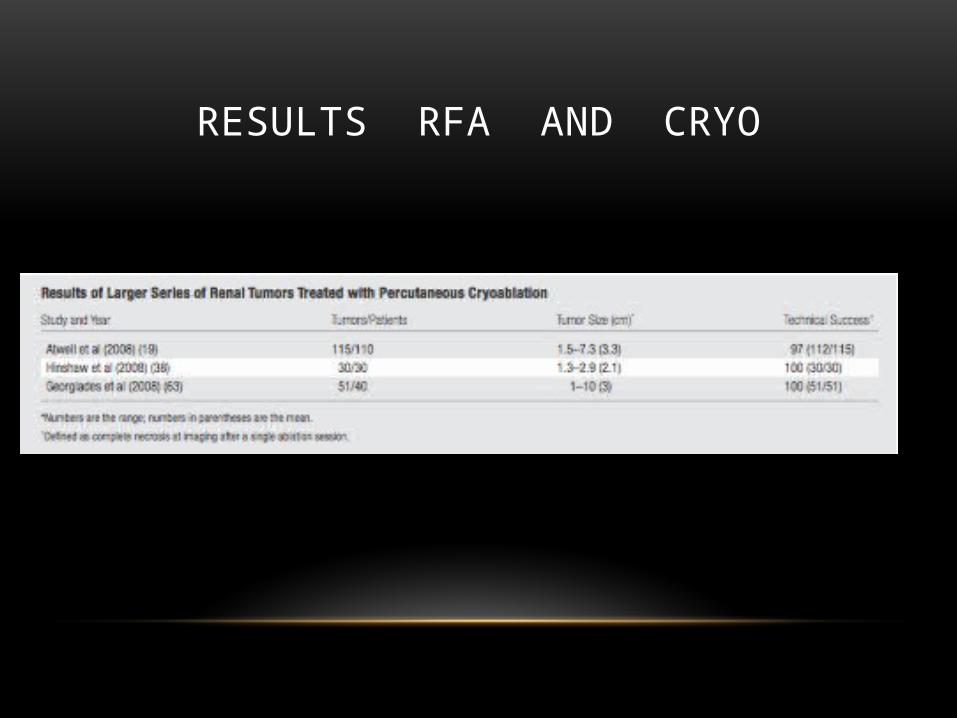
RESULTS RFA AND CRYO
COMPLICATIONS• RF and Cryo:
• Postablation syndrome, • Low-grade fever (37.5°–38.5°C)• Delayed pain, N+, V+, malaise, and myalgias • Self limited (cetaminophen or nonsteroidal anti- inflammatory agents)
• Mild Hematuria (self-limited), increased with ablation of centrally located tumors
• Pain or paresthesias at the percutaneous probe insertion site (most common)• Bladder outlet obstruction may result from clot formation • Perinephric hematomas (cauterization while electrode withdrawal) not
applicable for Cryo (Injection of gelfoam)

COMPLICATIONS• Thermal injury
• Ureters (urinoma, ureteral obstruction, and chronic stricture )• Cooled 5% dextrose in water retrograde pyelographie
• Genitofemoral nerve• Chronic pain and diminished sensitivity in the ipsilateral groin
• Psoas major muscle• Isolated impairment of hip flexion
• Small and large bowel• Serious. Colonic perforation and colonephric fistula have also been reported
• 5mm FAT• Strategic patient positioning• Hydrodissection may be performed to prevent complications by injecting
300–500 mL of 5% dextrose before and during ablation Hyponatremia syndrome
• Adrenal gland • Hypertensive crisis
FOLLOW-UP
• Follow-up imaging is mandatory
• Controversies exist concerning how often and for how long follow-up imaging should be performed.
• Immediate, 3 , 6 and one year
• Areas of contrast enhancement at initial follow-up (>10 HU or >15% with CT and MR imaging, respectively) usually indicate residual viable RCC and primary treatment failure
• Manifests as a focus of nodular or crescentic enhancement on postablation contrast-enhanced CT scans and MR images
• In cryoablation, a thin peripheral rim of enhancement often persists for several months following therapy

Microwave thermotherapy (MW)
• No significant clinical data have been reported to date using this modality.
• Major experience with the prostate.• Maintaining temperature greater than 60°C for 60 sec.,
causes coagulative necrosis.
• Can be done by laparoscopic or percutaneous approach.
Irreversible Electroporation (IRE)
• Relative newcomer to the field of tumor ablation
• Very notable because it is inherently nonthermal (no heat is produced to cause cell death)
• Cells are eradicated by using several microsecond-to-millisecond–long pulses of electrical current.
• The pulses generate electric fields up to 3 kV/cm, which cause irreversible damage to the cell membrane, thereby inducing apoptosis
• Heat sink should have a smaller influence on the ablation zone
• lesser damage to adjacent organs
HIFU
• Potentially the least invasive tumor ablation technique (Extracorporeal).
• Employs beams of ablative US frequency,generated by piezoelectric element,focused by a paraboloid reflector.
• This beam is focused on the lesion, US lithotripsy.• Resulting in thermal destruction - tissue cooking (temp.
raise by 70-80 °C in the target lesion).• Lots of concerns in regard to incomplete tumor ablation,
and superficial skin burns.
INTRACAVITARY PHOTON RADIATION
• A steriotactic radio-surgery.• Used initially for brain tumors.• Also applied for radio-resistant RCC metastatic lesions.• Deliver targeted high dose radiation for a precise site
causing coagulative necrosis, while preserving normal surrounding tissues.
• Additional experimental and clinical work is necessary to evaluate its role in renal cancer

CONCLUSION
• Extensive clinical experience supports the role of percutaneous RF ablation and cryo in the treatment of early-stage RCC in patients who are nonsurgical candidates or unwilling to undergo surgery.
• Both RF ablation and cryo are well-tolerated procedures that have demonstrated acceptable short- to inter- mediate-term outcomes and a low rate of complications
• Patients at risk for renal compromise may undergo this procedure effectively with preservation of their renal function

THANK YOU







