

Adherence in Pediatric Psychology
Melissa Stern
November 21, 2006
What is adherence?
“the extent to which a person’s behavior (in terms of taking medications, following diets, or executing life style changes) coincides with medical or health advice”
(Haynes, 1979, pp 2-3)
“a person’s behavior in relation to a prescribed medical regimen”
(La Greca & Bearman, 2003)
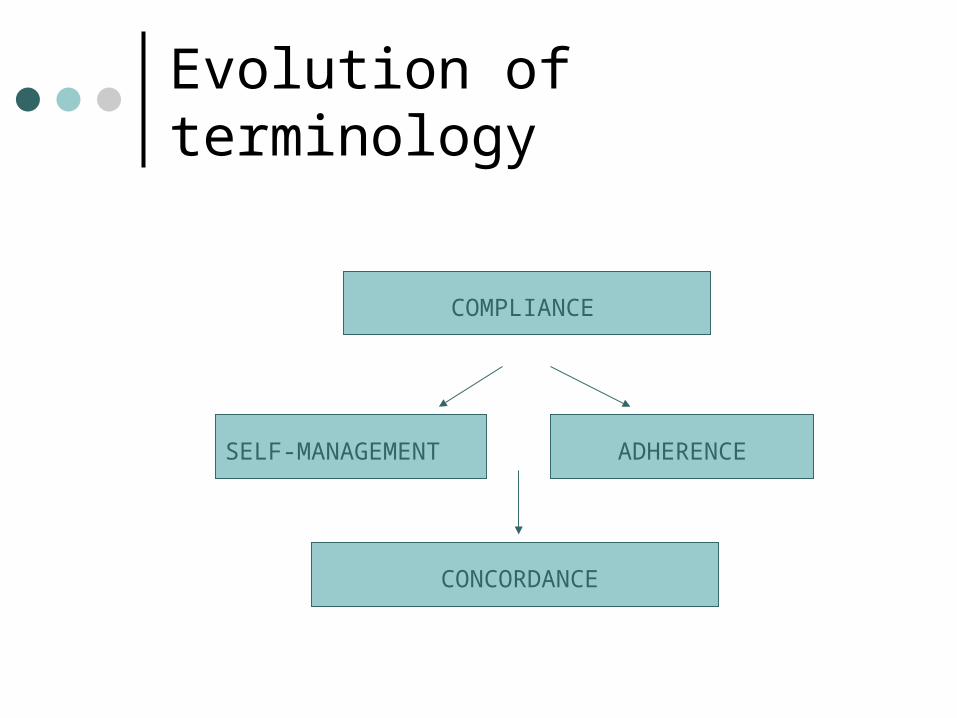
Evolution of terminology
COMPLIANCE
SELF-MANAGEMENT ADHERENCE
CONCORDANCE

Theories of Adherence
The Adherence/Compliance Approach Applies to patients with an existing problem Assumptions:
• Pt. needs to be treated• Pt. wants to initiate/maintain treatment and has
sought medical care for that purpose• Pt. should be motivated to comply for symptom
relief
Limitations: asymptomatic conditions, overlooks barriers
Theories of Adherence
Transtheoretical Model (Stages of Change) Five stages in the adoption of health-related
behaviors:• Precontemplation• Contemplation• Preparation• Action• Maintenance
Match intervention to stage Very difficult to apply to pediatric conditions!

Theories of Adherence
Health Belief Model Can be applied to preventative treatments Views patients as autonomous “decision
makers” Considers the patient’s perceptions of:
• Threat of illness• Effectiveness of treatment• Barriers to treatment
Again, difficult to apply to pediatric conditions!

Measuring Adherence
Categorical approach with adherence as a unitary construct
• adherent, nonadherent, or good, moderate, poor
Multidimensional, continuous construct
• Use multiple behaviors as indicators• Assess adherence along a continuum

Why is it important to measure adherence?
For life-threatening illnesses (post-transplant regimen)?
For chronic illnesses (asthma, diabetes)?
For acute illnesses (bacterial infection)?
For lifestyle medical issues (obesity)?
Measuring Adherence Self-reports
Easy and inexpensive but have questionable accuracy, social desirability effects, and parent/child disagreement
Health Provider ratings Easy and provider has extensive knowledge about
regimen but can be biased by history, health status, patient’s presentation
Behavioral monitoring Can be more accurate than retrospective report but
time intensive and susceptible to social desirability Pill counts
May overestimate adherence Medicine bottle cap removal counts
May overestimate adherence Daily blood draws to test levels
Extremely accurate, but highly unrealistic!!

Measuring Adherence
Electronic monitoring devices• MEMS caps, blood glucose monitors,
vests for CF Lab assays
• blood, urine, etc. tests• used mainly for medication adherence
Health status indicators• biological measures of disease status• pulmonary function tests, HgbA1c

Health Status & Adherence
Health status and adherence are not interchangeable terms
Health status measures are widely used by medical providers because they have been linked to long-term outcomes of morbidity and mortality
Most medical providers (and psychologists, too!) infer than health status = adherence
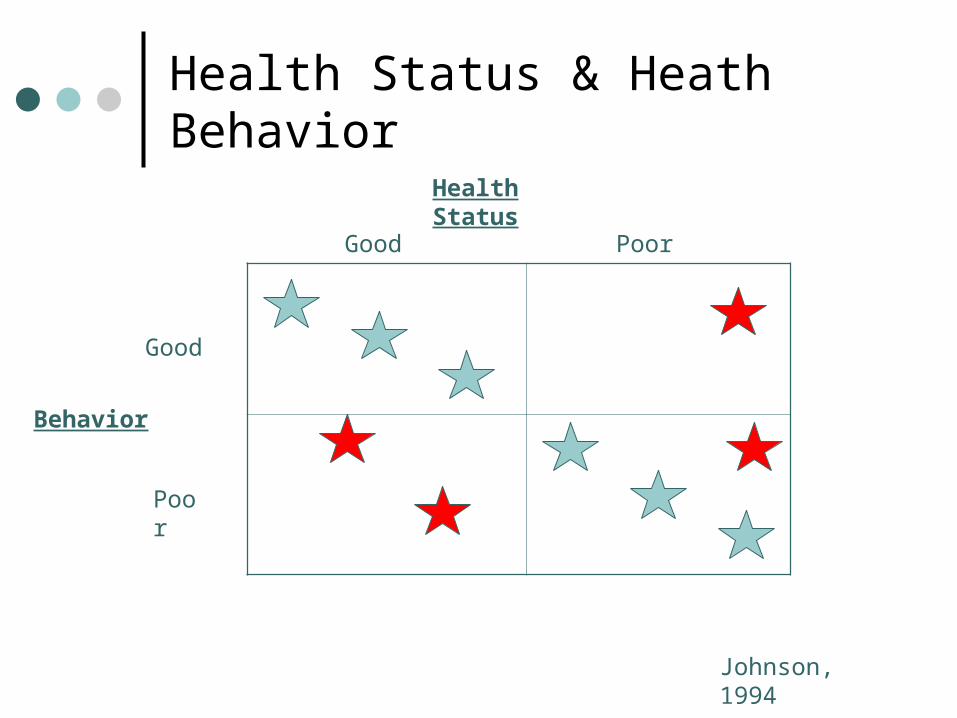
Health Status & Heath Behavior
Behavior
Health Status
Good Poor
Good
Poor
Johnson, 1994

Health Status & Heath Behavior: Pediatric Diabetes
30 % 18 %
24 % 28 %
Behavior:
Adherence
Health Status: Metabolic Control
Good
(HgbA1c < 7.7)
Poor
(HgbA1c > 10.1)
Good
Poor
Johnson, 1994

Why the discrepancy??
Imperfect measurement of adherence• e.g., poor measures, patients may report good
adherence but may not be performing behaviors accurately
Treatment effectiveness can affect the health status-adherence relationship Chemo/radiation for a 10 y/o with leukemia Adults taking glucosamine chondroitin for
arthritis

Health Status & Adherence: Importance of Tx Effectiveness
Strong Tx
Weak Tx
Inert Tx
Adherence
Poor Good
Health Status
Poor
Good

Nonadherence:The norm rather than the exception
“ . . . patients do not fail to comply, rather, they choose another course of behavior. The doctor’s advice is just one input among many in how to handle health and illness. Providers may consider the decisions that patients make irrational, but they may be quite rational from the patients’ perspective.” (Bauman, 2004)
10,000 journal articles on adherence—yet, rates of nonadherence remain high
“adaptive noncompliance” (La Greca & Bearman, 2003)

Prevalence of Nonadherence
Nonadherence occurs regardless of age, race, gender, and disease
In pediatric populations, nonadherence is estimated at 50%
Rates are higher for chronic conditions Adherence declines over time Adolescents are generally less adherent
than younger children

Types of Nonadherence
Volitional nonadherence —patient hears and understands the medical advice, but chooses not to adhere
Inadvertent nonadherence —patient accepts medical advice and believes that they are following it
• “Good enough” adherence• Barriers to adherence• Misunderstood treatment regimen

Risk Factors for Volitional Nonadherence
1. Difficulty & disruptiveness of regimen
2. Skepticism about efficacy
3. Side effects
4. Patient beliefs, fears, concerns
5. Cost of treatment
6. Denial of diagnosis
7. Physician prescribing practices

Risk Factors for Inadvertent Nonadherence
1. Patient characteristics Intellectual functioning, memory, stress, lack
of resources, lack of social support, disease knowledge
2. Developmental considerations Medication refusal Cognitive abilities of children Adolescents’ independence/autonomy
Risk Factors for Inadvertent Nonadherence
3. Provider/System characteristics• Poor patient-provider communication• Lack of patient education • Long waiting times, geographic
distance, unfriendly staff
4. Regimen characteristics• Complexity• Frequency of regimen-drift over time
Special Considerations for Pediatric Patients Barriers can exist for the parent and the
child Importance of family interactions Developmental issues:
• Toddlers—may be oppositional with painful procedures, bad tasting meds, activity restrictions
• School-aged—may not adhere if they are teased at school
• Adolescents—may experiment with meds to exert control, struggle for independence from parents

Special Considerations for Pediatric Patients Disagreements between parent/child report of
adherence Child behavior/psychological diagnoses may be a
significant barrier Environment in which adherence behavior needs to
occur (e.g., at school) Disease knowledge is important for family member
who is responsible for treatment Transfer of responsibility for disease management
from child to parent• When should this occur?

Adherence & Self-Care Autonomy in Diabetes Calculated self-care index based on ratio of
self-care autonomy and psychological maturity (cognitive function, academic achievement, social-cognitive development)
Youth were grouped into 3 categories: constrained, maximal, and excessive autonomy
Those with excessive autonomy had poorer adherence (and poorer metabolic control and disease knowledge)
Suggests that parents should remain involved in adolescents’ self-management
Adherence Interventions
Types of interventions:Educational approachesBehavioral approaches
• Medical supervision/monitoring• Visual cues and reminders• Self-monitoring• Reinforcement
Family Interventions

Adherence Interventions
Peer interventions
Barrier reduction?
Multicomponent interventions“Self Management Training”







