
CHAPTER 01: INTRODUCTION TO ANATOMY
ANALYZING PATIENT’S PROFILE FOROPTIMIZING CASE CLERKING
ERNI KOLOPAKING, SCHOOL OF PHARMACY, MSU

CHAPTER 01: INTRODUCTION TO ANATOMY
THE UNIVERSITY OF CHOICE

CHAPTER 01: INTRODUCTION TO ANATOMY
SCHOOL OF PHARMACY, MSU
• Established on 14th July 2007
• Aligned the standard set by the Malaysian Pharmacy Board (MPB) and Malaysian Qualification Agency (MQA)
• Currently running with 450 students
• Course available:– Bachelor of Pharmacy
– Diploma of Pharmacy
– Diploma in Traditional Chinese Medicine

CHAPTER 01: INTRODUCTION TO ANATOMY
SIX ACADEMIC UNITS

CHAPTER 01: INTRODUCTION TO ANATOMY
SIX ACADEMIC UNITS

CHAPTER 01: INTRODUCTION TO ANATOMY
SIX ACADEMIC UNITS
CHAPTER 01: INTRODUCTION TO ANATOMY
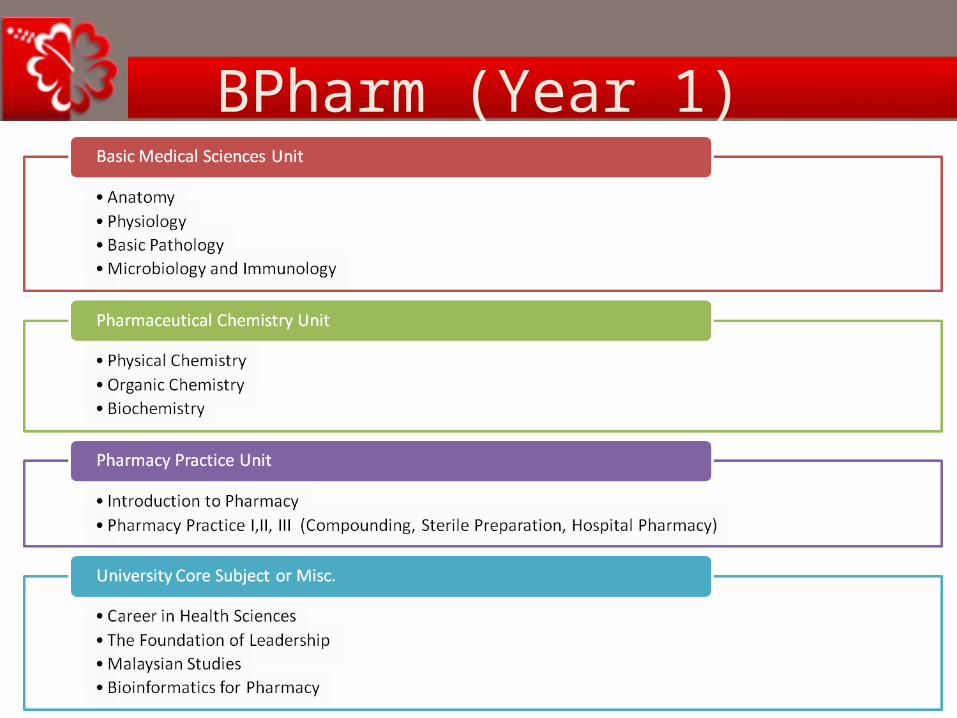
BPharm (Year 1)
CHAPTER 01: INTRODUCTION TO ANATOMY
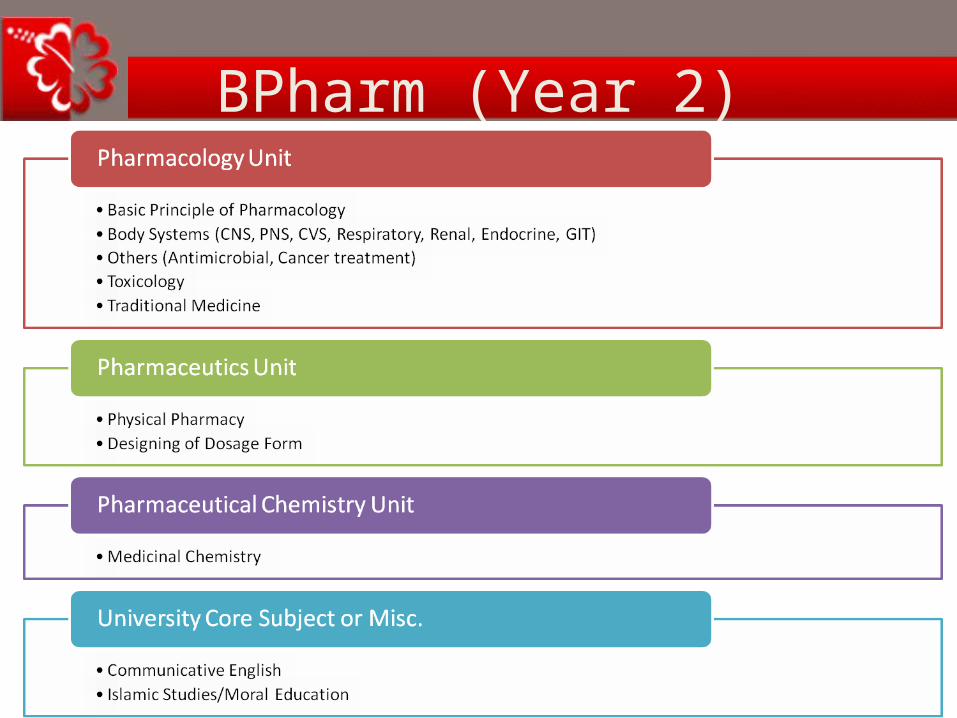
BPharm (Year 2)
CHAPTER 01: INTRODUCTION TO ANATOMY
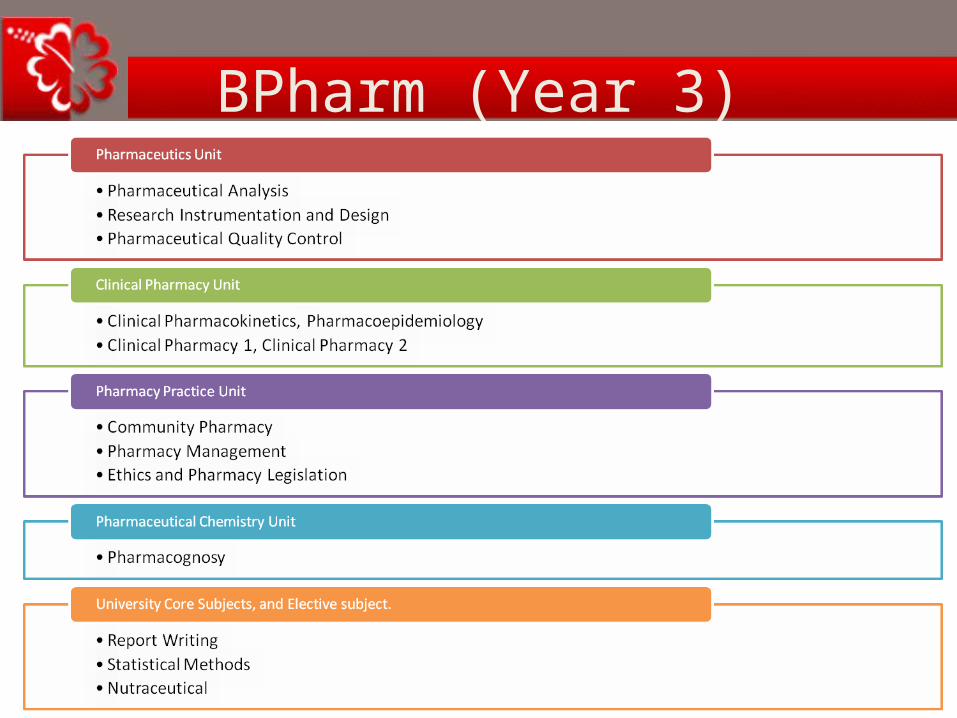
BPharm (Year 3)

CHAPTER 01: INTRODUCTION TO ANATOMY
BPharm (Year 4)
CHAPTER 01: INTRODUCTION TO ANATOMY
Attachments
1. Hospital Pharmacy Attachment– Year 2 (Semester 4), 4 weeks
2. Community Pharmacy Attachment– Year 3 (Semester 6), 4 weeks
3. Industrial Pharmacy Attachment– Year 4 (Semester 7), 4 weeks
4. Clinical Pharmacy I & II Attachment– Year 4 (Semester 7 and 8), 8 weeks
CHAPTER 01: INTRODUCTION TO ANATOMY
EXAMPLE

CHAPTER 01: INTRODUCTION TO ANATOMY
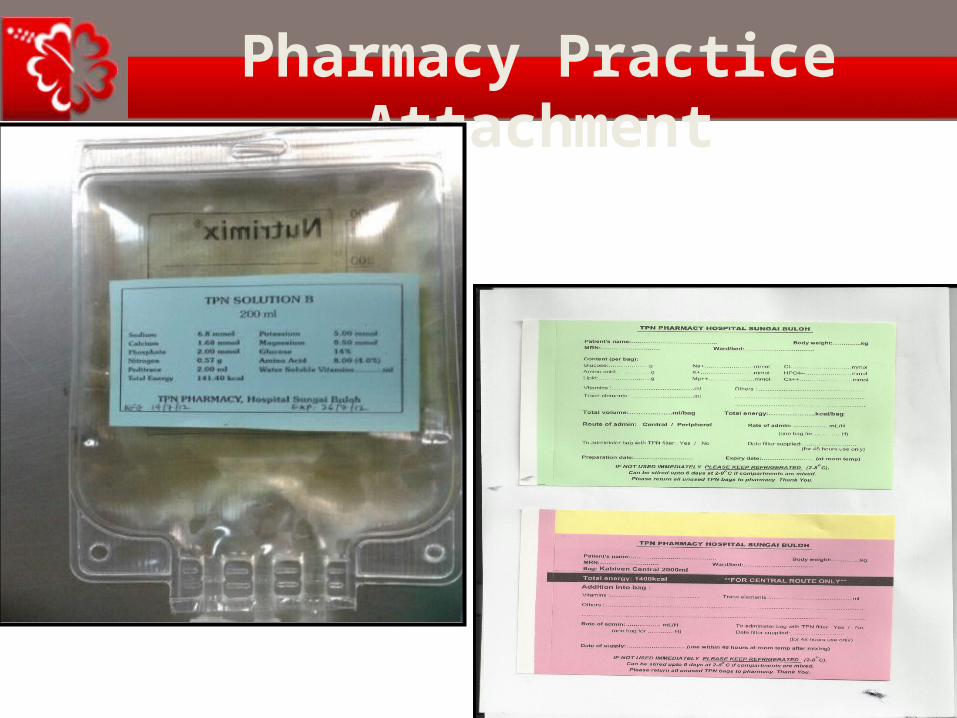
Pharmacy Practice Attachment
CHAPTER 01: INTRODUCTION TO ANATOMY
Pharmacy Practice Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Pharmacy Practice Attachment
CHAPTER 01: INTRODUCTION TO ANATOMY
Pharmacy Practice Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Pharmacy Practice Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Pharmacy Practice Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Pharmacy Practice Attachment
CHAPTER 01: INTRODUCTION TO ANATOMY
Pharmacy Practice Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Pharmacy Practice Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Pharmacy Practice Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Industrial Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Industrial Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
ODAWARA KANEBO R&D TECHNOLOGY DEPT.

CHAPTER 01: INTRODUCTION TO ANATOMY
Industrial Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Industrial Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Community Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Community Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Community Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Community Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment
CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment
CLINICAL ATTACHMENT at Hospital Sungai Buloh
Siewert Ⅲ carcinoma of cardia esophagus
Takeshi Oshizaka Josai University
CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment

CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment
CHAPTER 01: INTRODUCTION TO ANATOMY
Clinical Pharmacy Attachment
CHAPTER 01: INTRODUCTION TO ANATOMY
OBJECTIVES (1)
1. To prepare students to be able to help patient in solving their medical problems (especially with medications).
2. To prepare student to be able to work together with other people (health care providers: doctor, nurses, nutritionists, etc;
as well as with the hospital management, patient’s caregivers, and the community).
CHAPTER 01: INTRODUCTION TO ANATOMY
OBJECTIVES (2)
3. To teach student to have clinical knowledge, skill, intuition, and critical thinking to help patients.
4. To teach student to have the ability to communicate with other people, in order to express his/her opinion regarding patient care, for the best interest of the patients.
5. To teach students to act in professional manner, ethically and clinically.
CHAPTER 01: INTRODUCTION TO ANATOMY
HOW TO HELP PATIENT
A. Pharmacist should analyze three aspects:1. Patient’s profile.2. Disease(s) profile that patient has.3. Treatment for disease(s) that patient has.B. Then to come up with Pharmaceutical Care
Issues (PCI) in order to give the most appropriate treatment (safe and effective) for the patient.
CHAPTER 01: INTRODUCTION TO ANATOMY
1. TO LEARN PATIENT’S PROFILE (1)
1. Be able to read, understand, and analyze Patient’s Medical Record (PMR).
2. Be able to read, understand, and analyze the medical terms and medical abbreviations.
3. Be able to read, understand, and analyze all patient’s data and condition.
CHAPTER 01: INTRODUCTION TO ANATOMY
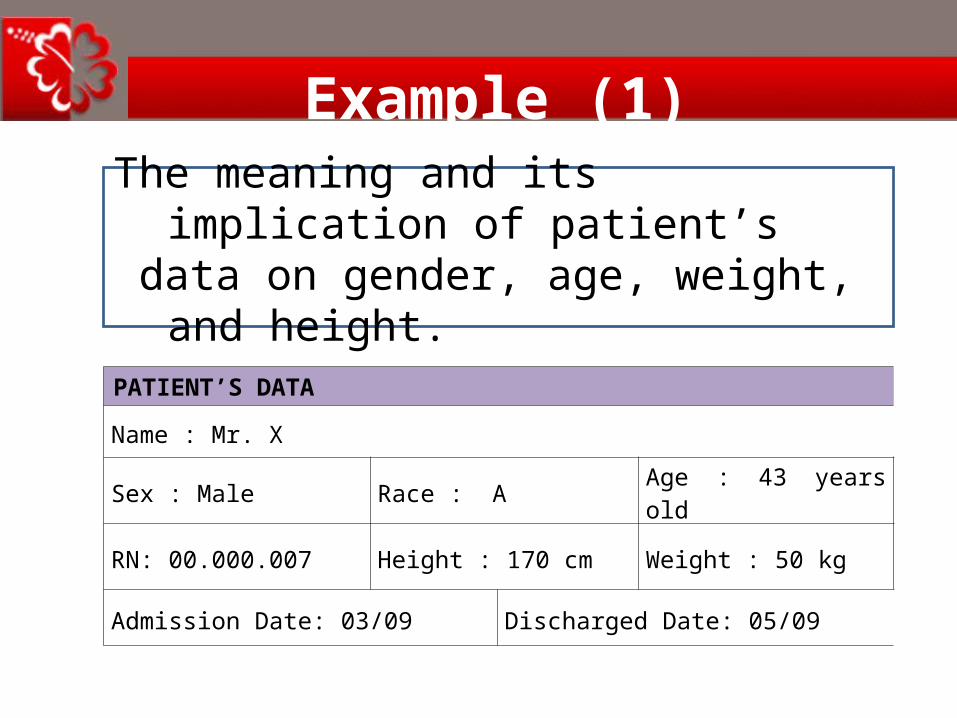
PATIENT’S DATA
Name : Mr. X
Sex : Male Race : A Age : 43 years old
RN: 00.000.007 Height : 170 cm Weight : 50 kg
Admission Date: 03/09 Discharged Date: 05/09
The meaning and its implication of patient’s data on gender, age, weight, and height.
Example (1)

CHAPTER 01: INTRODUCTION TO ANATOMY
PATIENT’S DATA
Name : Mrs. Y
Sex : Female Race : B Age : 56 years old
RN: 00.000.008 Height : 156 cm Weight : 82 kg
Admission Date: 12/01 Discharged Date: 27/02
The meaning and its implication of patient’s data on gender, age, weight, and height.
Example (1)

CHAPTER 01: INTRODUCTION TO ANATOMY
PATIENT’S DATA
Name : Chd. Z
Sex : Male Race : C Age : 10 years old
RN: 00.000.009 Height : 125 cm Weight : 25 kg
Admission Date: 03/12 Discharged Date: not yet discharged
The meaning and its implication of patient’s data on gender, age, weight, and height.
Example (1)

CHAPTER 01: INTRODUCTION TO ANATOMY
Example (1)• He is a child of more than 2 years old, his BMI can be calculated with the formula of "BMI for age" (having discrepancy in age and gender).
• The result: his BMI is 16, it is 36%, means he has healthy body weight. • (Reference: http://kidshealth.org/
parent/general/body/bmi_charts.html)
CHAPTER 01: INTRODUCTION TO ANATOMY
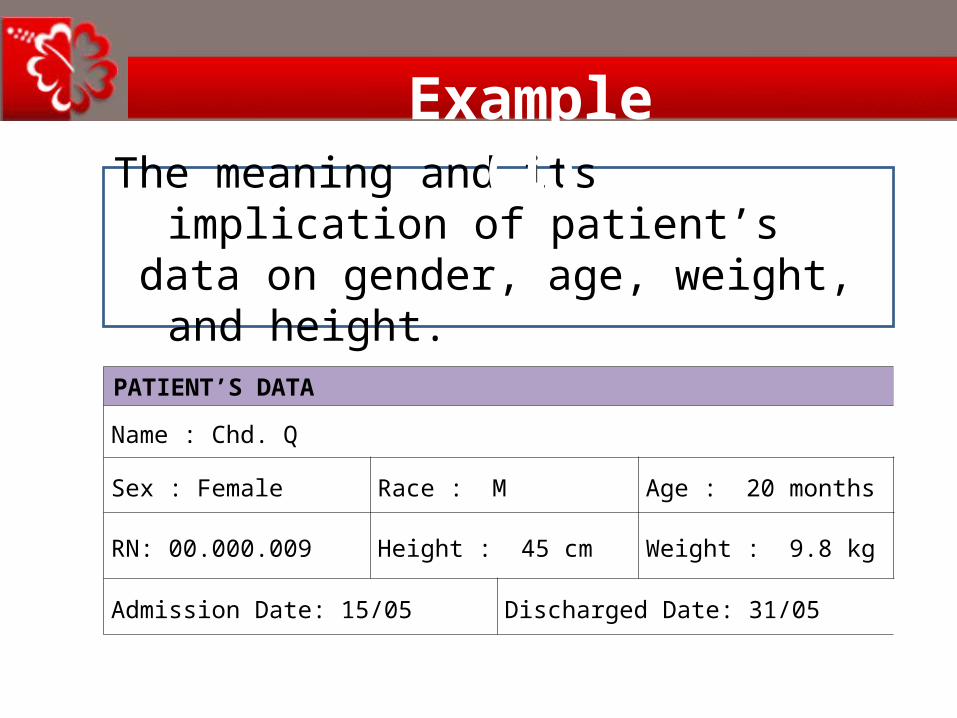
PATIENT’S DATA
Name : Chd. Q
Sex : Female Race : M Age : 20 months
RN: 00.000.009 Height : 45 cm Weight : 9.8 kg
Admission Date: 15/05 Discharged Date: 31/05
The meaning and its implication of patient’s data on gender, age, weight, and height.
Example (1)

CHAPTER 01: INTRODUCTION TO ANATOMY
Example (1)
She is a child of less than 2 years old, her healthy weight status can be calculated with the formula of : “her minimum weight should be 3 times of her weight when she was born.”

CHAPTER 01: INTRODUCTION TO ANATOMY
1. TO LEARN PATIENT’S PROFILE (2)
The meaning and its implication of patient’s chief complaint (sign and symptoms), history of present illness, past medical history, past medication history, family history, social history, allergic history, the results of physical and laboratory examination at the time patient arrived at the hospital.
CHAPTER 01: INTRODUCTION TO ANATOMY
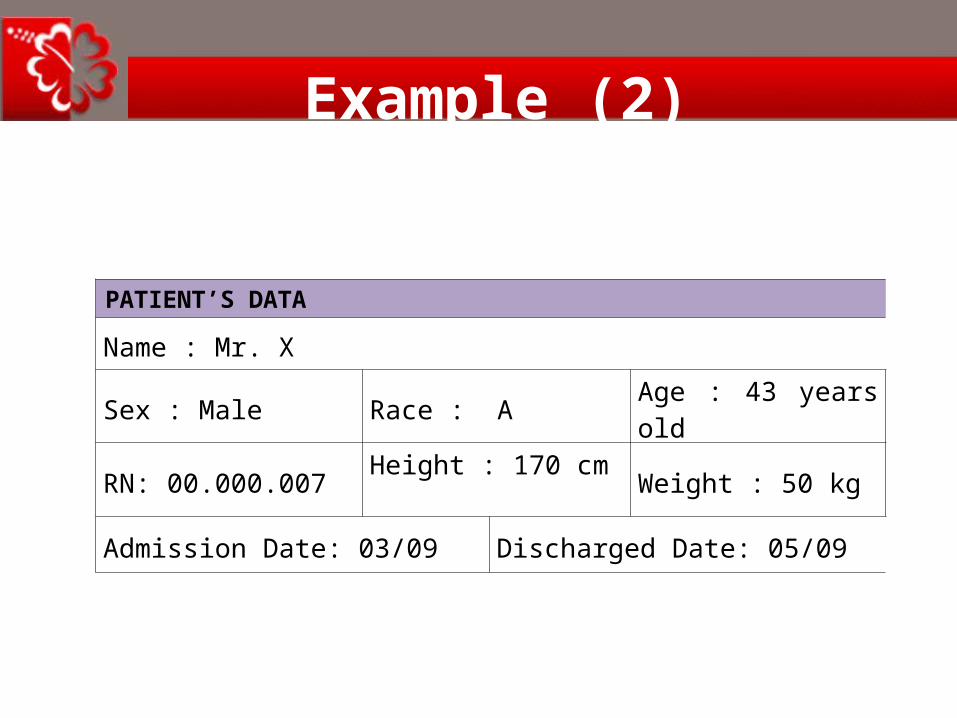
PATIENT’S DATA
Name : Mr. X
Sex : Male Race : A Age : 43 years old
RN: 00.000.007 Height : 170 cm Weight : 50 kg
Admission Date: 03/09 Discharged Date: 05/09
Example (2)

CHAPTER 01: INTRODUCTION TO ANATOMY
CHIEF COMPLAINTS
Shortness of Breath (SOB)
HISTORY OF PRESENT ILLNESSS
SOB since the morning of 03/09, progressively worsening, not resolved by MDI (not sure how many times), coughs with whitish sputum. Sudden onset, trigger factor was ice drink at night.
CHAPTER 01: INTRODUCTION TO ANATOMY
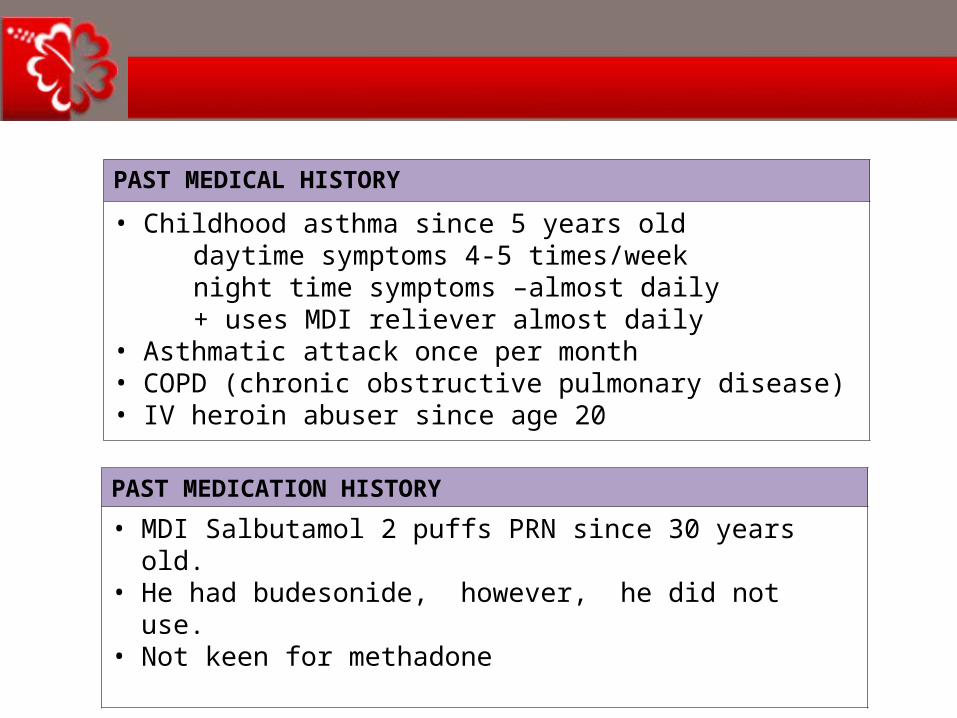
PAST MEDICAL HISTORY
• Childhood asthma since 5 years old daytime symptoms 4-5 times/week night time symptoms –almost daily + uses MDI reliever almost daily• Asthmatic attack once per month• COPD (chronic obstructive pulmonary disease)• IV heroin abuser since age 20
PAST MEDICATION HISTORY
• MDI Salbutamol 2 puffs PRN since 30 years old. • He had budesonide, however, he did not use. • Not keen for methadone
CHAPTER 01: INTRODUCTION TO ANATOMY
FAMILY HISTORY
Father and brother have asthma
ALLERGY
NKDA
SOCIAL HISTORY
Smoker 10 cigarettes/day since age of 15 Heroin abuser since age of 20 Working as a lorry driver Patient married without kids

CHAPTER 01: INTRODUCTION TO ANATOMY
PHYSICAL AND LABORATORY EXAMINATION
General : alert, conscious, not tachypnoeic, not using accessory muscle of respiration, talking in full sentences. GCS: Eye 4, Verbal 5, Motor 6, Total 15 CVS : BP (blood pressure) 132/62 mmHg : PR (pulse rate) 78 p/min, RR (respiration Rate) 22 b/min Lungs : occasional polyphonic wheeze Abdomen : soft, non tender
WORKING DIAGNOSIS
Acute exacerbation of bronchiral asthma probably by enviromental factors, underlying poorly controlled asthma
DIFFERENTIAL DIAGNOSIS
None
CHAPTER 01: INTRODUCTION TO ANATOMY
2. TO LEARN PATIENT’S DISEASE
The meaning of all results of physical, laboratory and radiology investigations, etc, on the second day.

CHAPTER 01: INTRODUCTION TO ANATOMY
THE RESULTS OF LABORATORY INVESTIGATIONS Remarks
Parameters Units Normal range
Results on 3/09
Renal profile
Urea mmol/L 1.7-8.3 2.7 Normal
SCr umol/L 64-122 82 Normal
CrCl ml/min 80-120 80(indicated)
Normal
CHAPTER 01: INTRODUCTION TO ANATOMY
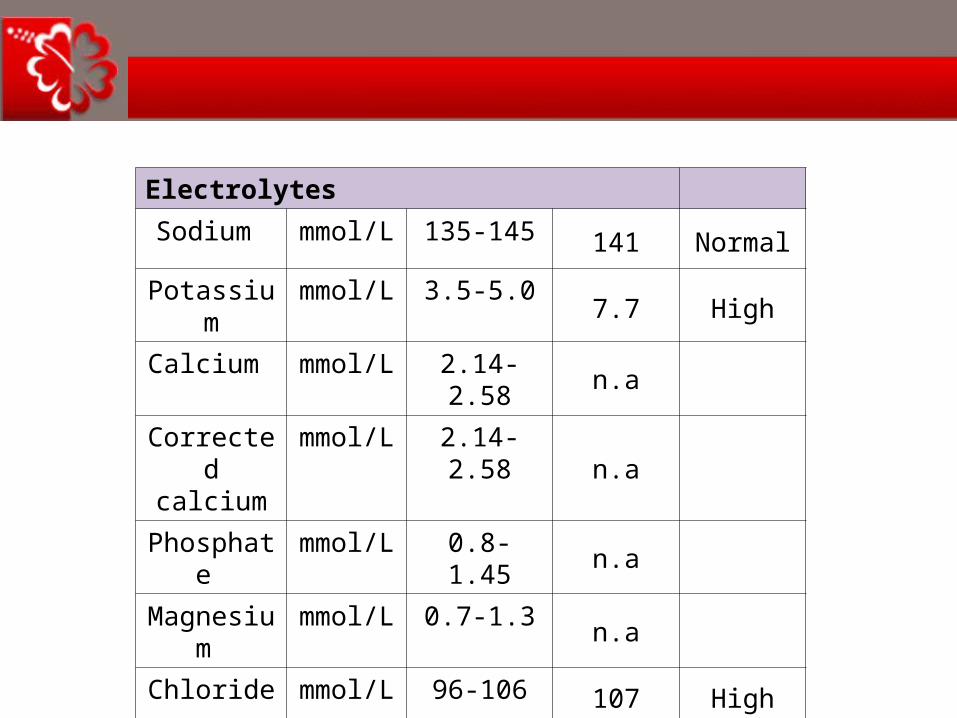
Electrolytes
Sodium mmol/L 135-145 141 Normal
Potassium mmol/L 3.5-5.0 7.7 High
Calcium mmol/L 2.14-2.58 n.a
Corrected calcium
mmol/L 2.14-2.58 n.a
Phosphate mmol/L 0.8-1.45 n.a
Magnesium mmol/L 0.7-1.3 n.a
Chloride mmol/L 96-106 107 High
CHAPTER 01: INTRODUCTION TO ANATOMY
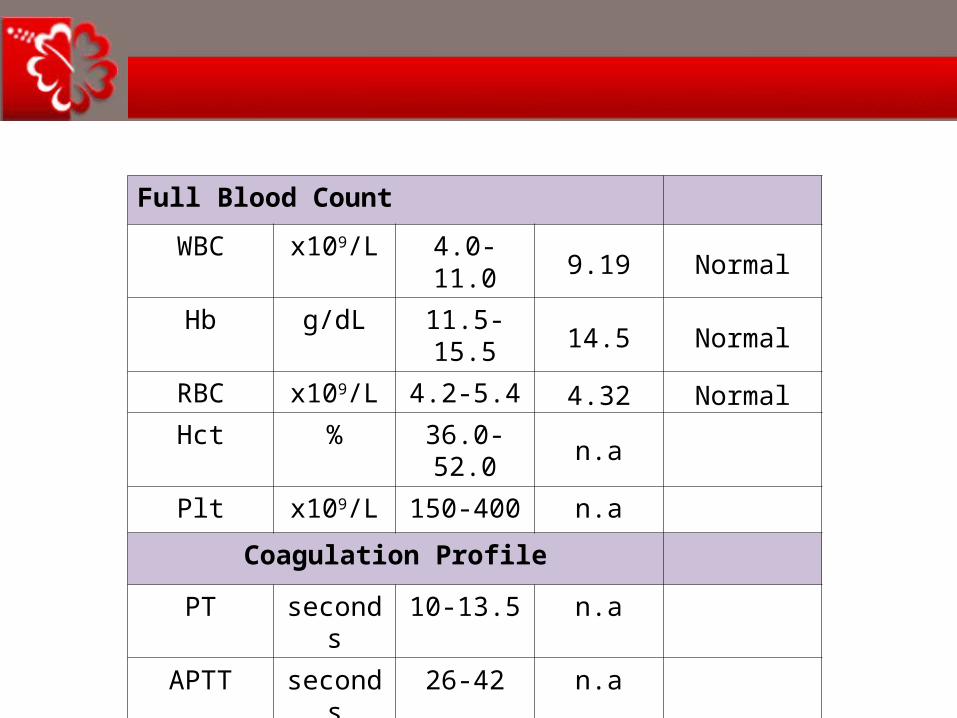
Full Blood Count
WBC x109/L 4.0-11.0 9.19 NormalHb g/dL 11.5-15.5 14.5 Normal
RBC x109/L 4.2-5.4 4.32 NormalHct % 36.0-52.0 n.a
Plt x109/L 150-400 n.a
Coagulation Profile
PT seconds 10-13.5 n.a
APTT seconds 26-42 n.a
INR <1.5 n.a

CHAPTER 01: INTRODUCTION TO ANATOMY
Liver Profile
Total Protein
g/L66-87 70 Normal
Albumin g/L 35-50 37 Normal
T. Bilirubin umol/L<20 12 Normal
ALT IU/L <32 14 Normal
AST IU/L n.a
ALP IU/L 53-141 54 Normal
CHAPTER 01: INTRODUCTION TO ANATOMY
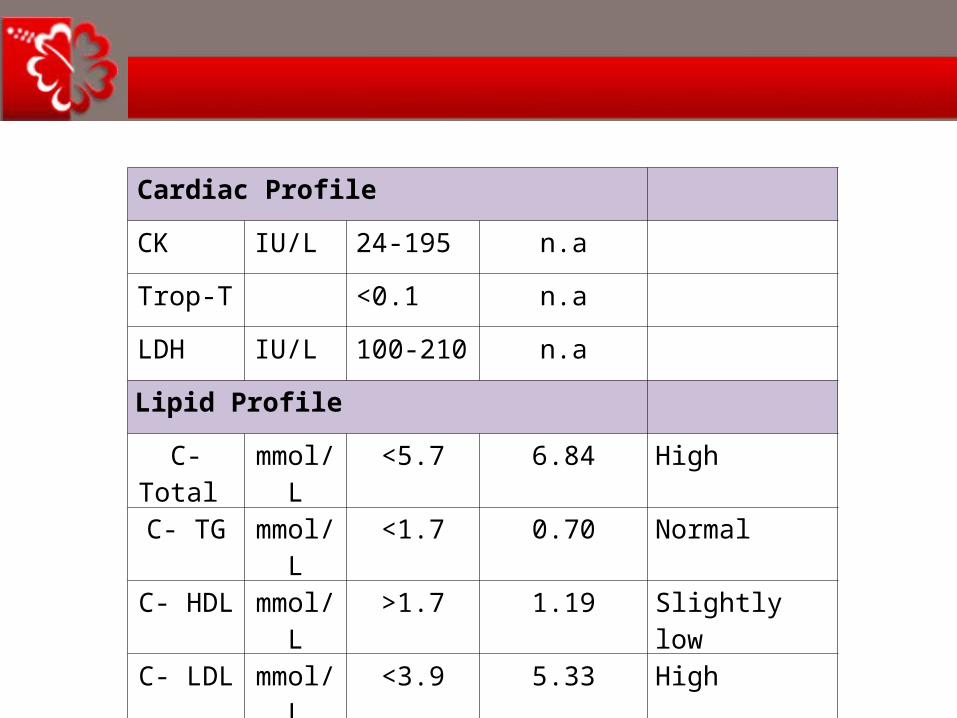
Cardiac Profile
CK IU/L 24-195 n.a
Trop-T <0.1 n.a
LDH IU/L 100-210 n.a
Lipid Profile
C- Total mmol/L <5.7 6.84 High
C- TG mmol/L <1.7 0.70 Normal
C- HDL mmol/L >1.7 1.19 Slightly low
C- LDL mmol/L <3.9 5.33 High
CHAPTER 01: INTRODUCTION TO ANATOMY
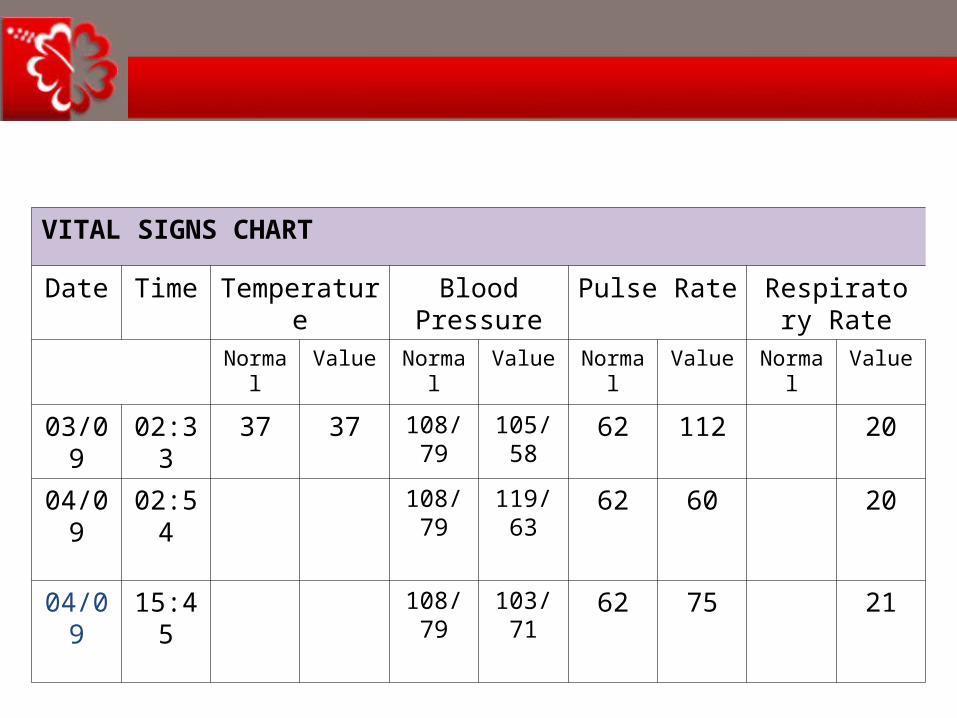
VITAL SIGNS CHART
Date Time Temperature Blood Pressure
Pulse Rate Respiratory Rate
Normal Value Normal Value Normal Value Normal Value
03/09 02:33 37 37 108/79 105/58 62 112 20
04/09 02:54 108/79 119/63 62 60 20
04/09 15:45 108/79 103/71 62 75 21

CHAPTER 01: INTRODUCTION TO ANATOMY
3. TO LEARN TREATMENT PROFILE
1. To learn progress note
2. To learn diagnose test
3. To learn treatment plan

CHAPTER 01: INTRODUCTION TO ANATOMY
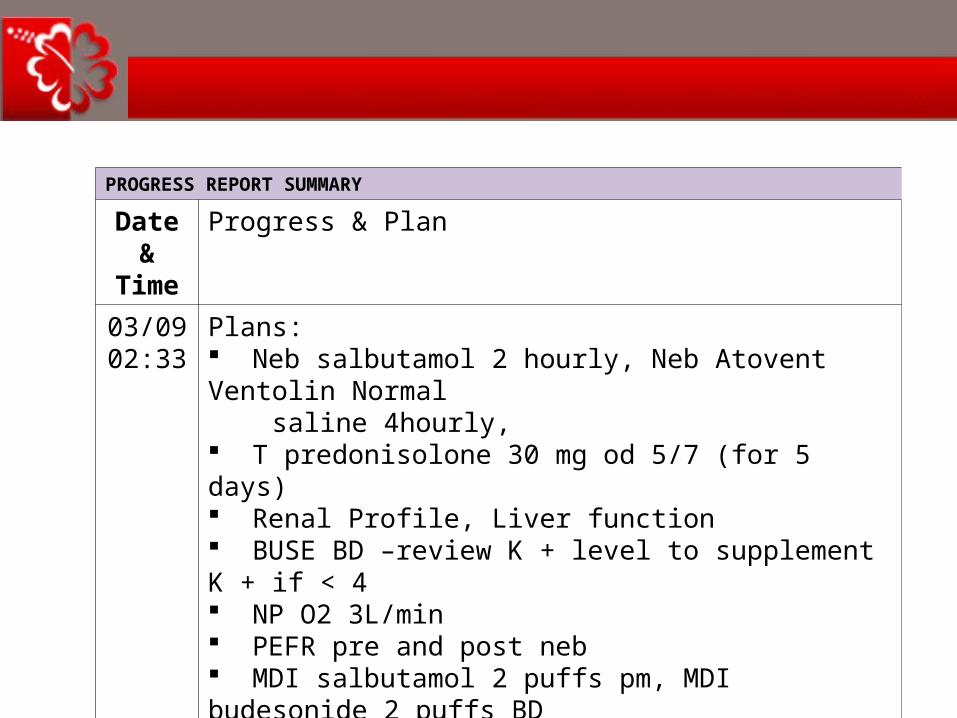
PROGRESS REPORT SUMMARY
Date & Time
Progress & Plan
03/0902:33
Progress: Presented with SOB since early this morning, sudden onset Unrelieved even though he used his MDI salbutamol multiple times (not sure how many times) Trigger factor: took an ice drink last night Has intermittent cough, productive whitish sputum No chest pain Presence of reduced effort tolerance No fever Still actively chasing heroine, last taken the night before Takes heroine daily, however claims that he wants to quit now, wants to take methadone
CHAPTER 01: INTRODUCTION TO ANATOMY
PROGRESS REPORT SUMMARY
Date & Time
Progress & Plan
03/0902:33
Plans: Neb salbutamol 2 hourly, Neb Atovent Ventolin Normal saline 4hourly, T predonisolone 30 mg od 5/7 (for 5 days) Renal Profile, Liver function BUSE BD –review K + level to supplement K + if < 4 NP O2 3L/min PEFR pre and post neb MDI salbutamol 2 puffs pm, MDI budesonide 2 puffs BD Pharmacist to assess MDI technique Refer to psychiatry for methadone therapy and advise to stop smoking
CHAPTER 01: INTRODUCTION TO ANATOMY
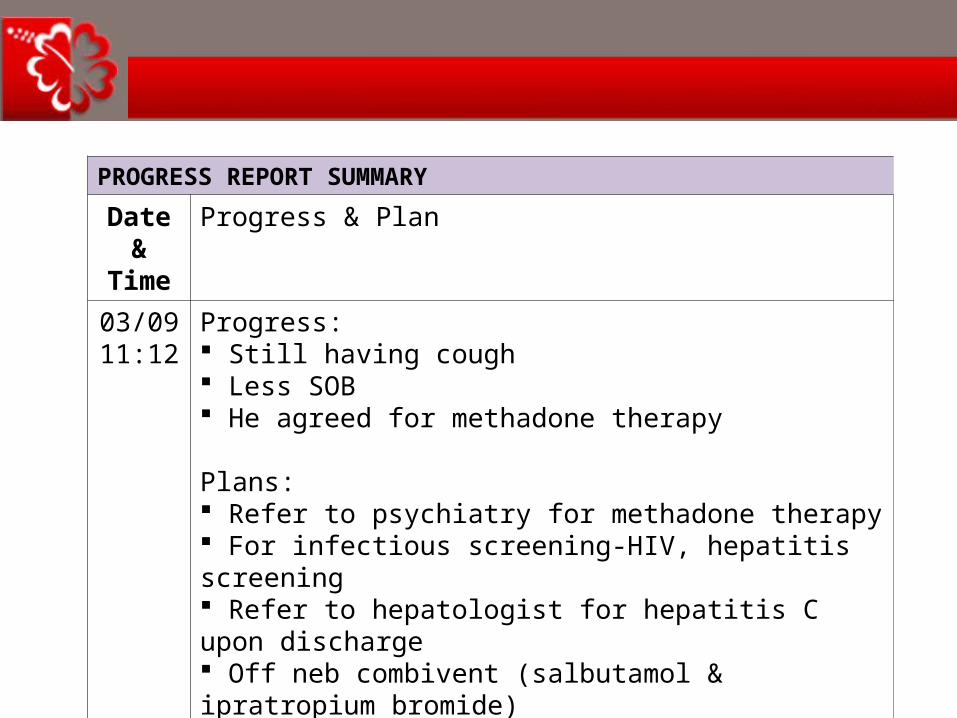
PROGRESS REPORT SUMMARY
Date & Time
Progress & Plan
03/0911:12
Progress: Still having cough Less SOB He agreed for methadone therapy
Plans: Refer to psychiatry for methadone therapy For infectious screening-HIV, hepatitis screening Refer to hepatologist for hepatitis C upon discharge Off neb combivent (salbutamol & ipratropium bromide) Change to neb salbutamol 6 hourly MDI ventolin 2 puffs PRN
CHAPTER 01: INTRODUCTION TO ANATOMY
PROGRESS REPORT SUMMARY
Date & Time
Progress & Plan
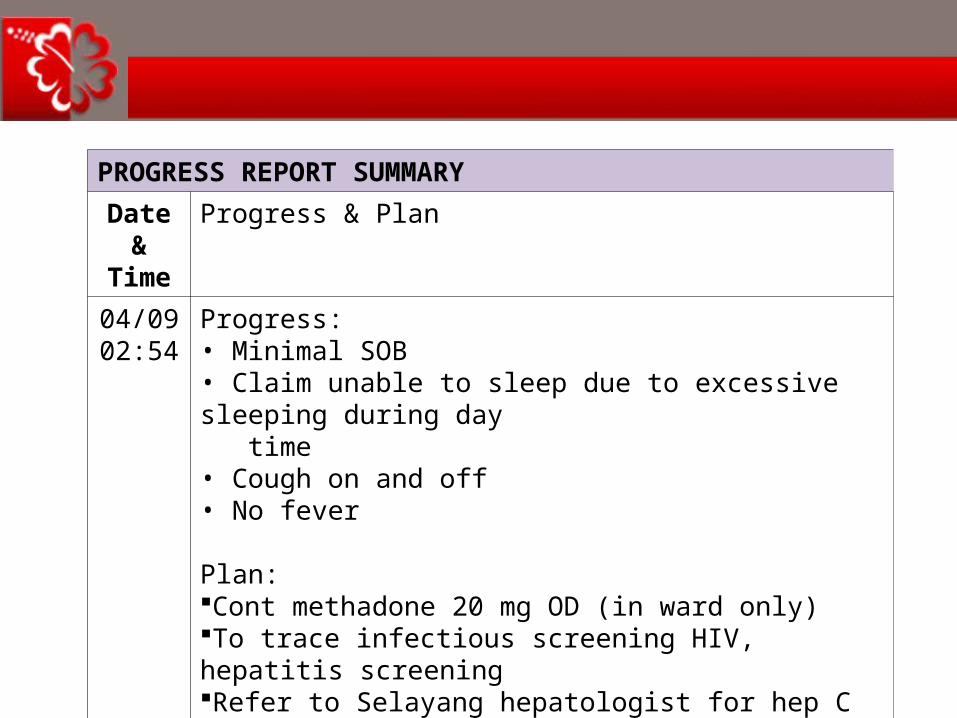
04/0902:54
Progress:• Minimal SOB• Claim unable to sleep due to excessive sleeping during day time• Cough on and off• No fever
Plan:Cont methadone 20 mg OD (in ward only)To trace infectious screening HIV, hepatitis screeningRefer to Selayang hepatologist for hep C upon dischargeContinue to neb salbutamol 6 hrlyMDI Ventolin 2 puffs PRN
CHAPTER 01: INTRODUCTION TO ANATOMY
PROGRESS REPORT SUMMARY
Date & Time
Progress & Plan
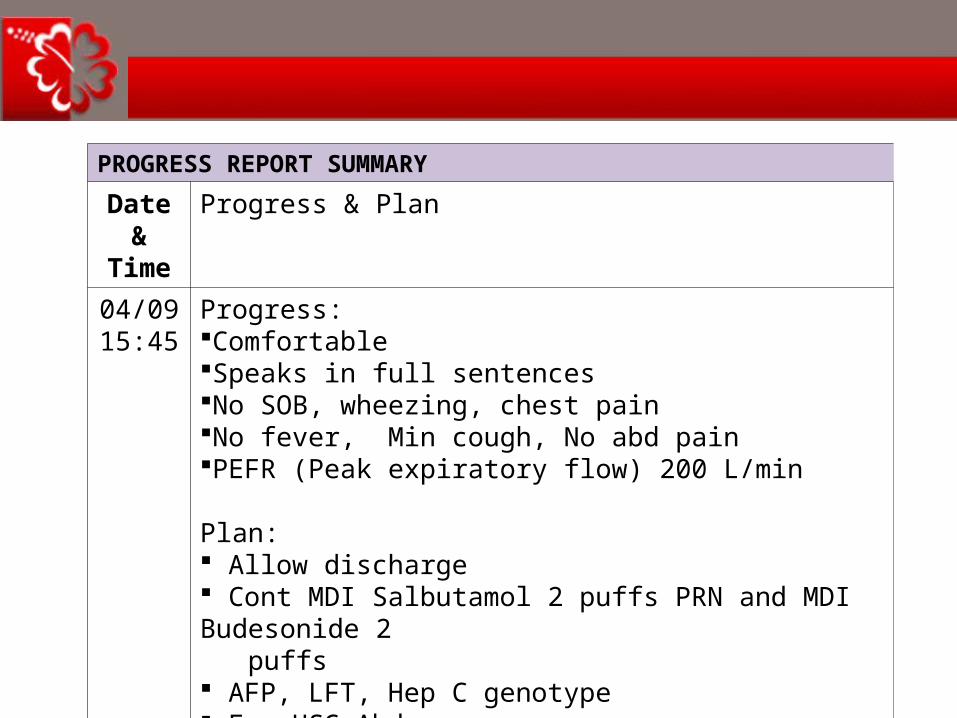
04/0915:45
Progress:ComfortableSpeaks in full sentencesNo SOB, wheezing, chest painNo fever, Min cough, No abd painPEFR (Peak expiratory flow) 200 L/min
Plan: Allow discharge Cont MDI Salbutamol 2 puffs PRN and MDI Budesonide 2 puffs AFP, LFT, Hep C genotype For USG Abdomen TCA MOPD after US abdomen
CHAPTER 01: INTRODUCTION TO ANATOMY
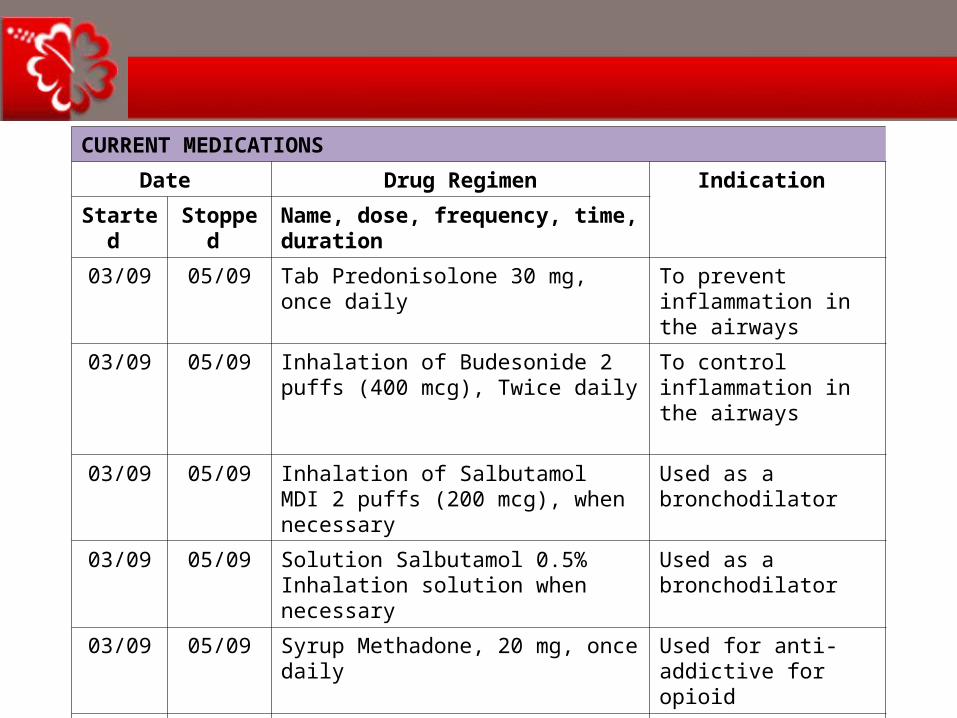
CURRENT MEDICATIONS
Date Drug Regimen Indication
Started Stopped Name, dose, frequency, time, duration
03/09 05/09 Tab Predonisolone 30 mg, once daily To prevent inflammation in the airways
03/09 05/09 Inhalation of Budesonide 2 puffs (400 mcg), Twice daily
To control inflammation in the airways
03/09 05/09 Inhalation of SalbutamolMDI 2 puffs (200 mcg), when necessary
Used as a bronchodilator
03/09 05/09 Solution Salbutamol 0.5% Inhalation solution when necessary
Used as a bronchodilator
03/09 05/09 Syrup Methadone, 20 mg, once daily Used for anti-addictive for opioid
03/09 05/09 Tab Simvastatin 20 mg, at night To control elevated cholesterol
CHAPTER 01: INTRODUCTION TO ANATOMY
4. TO COME UP WITH PCI
• To give opinion to the other health care team members regarding issues from the pharmacist point of view.
• To give suggestions to overcome the issues.
CHAPTER 01: INTRODUCTION TO ANATOMY
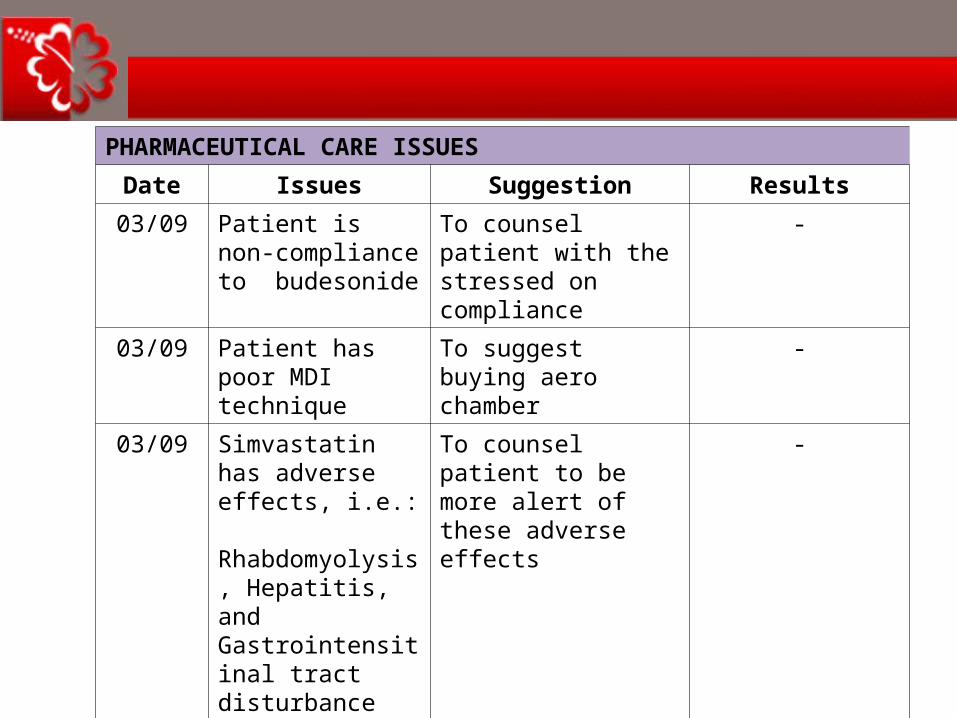
PHARMACEUTICAL CARE ISSUES
Date Issues Suggestion Results
03/09 Patient is non-compliance to budesonide
To counsel patient with the stressed on compliance
-
03/09 Patient has poor MDI technique
To suggest buying aero chamber
-
03/09 Simvastatin has adverse effects, i.e.: Rhabdomyolysis, Hepatitis, and Gastrointensitinal tract disturbance
To counsel patient to be more alert of these adverse effects
-
03/09 Patient is addicted to heroin, he needs to use methadone instead
To counsel in how important in using methadone for him, and how to use it.

CHAPTER 01: INTRODUCTION TO ANATOMY
PHARMACEUTICAL CARE ISSUES
Date Issues Suggestion Results
03/09 Patients has to achieve the objective of the treatments.
To monitor efficacy of all drugs that have been given to the patient
-
03/09 Patients has to be prevented from ADRs, Drug Interactions, etc.
To monitor Adverse effects of Simvastatin, i.e.: Rhabdomyolysis, Hepatitis, and Gastrointensitinal Tract disturbance
-
CHAPTER 01: INTRODUCTION TO ANATOMY
SUMMARY

CHAPTER 01: INTRODUCTION TO ANATOMY
1. REVIEWING PATIENT'S MEDICAL CHARTS
1. Step ONE
CHAPTER 01: INTRODUCTION TO ANATOMY
REVIEWING PMR
Read PMR and assess the data
CHAPTER 01: INTRODUCTION TO ANATOMY
2. BUILDING A PHARMACIST’S PATIENT DATA BASE
2. Step TWO
CHAPTER 01: INTRODUCTION TO ANATOMY
From PMR, nurses
Ward round with doctor
COLLECTING PATIENT’S DATA BASE (1)

CHAPTER 01: INTRODUCTION TO ANATOMY
COLLECTING PATIENT’S DATA BASE (2)
Interview with npatient and their
care giver
CHAPTER 01: INTRODUCTION TO ANATOMY
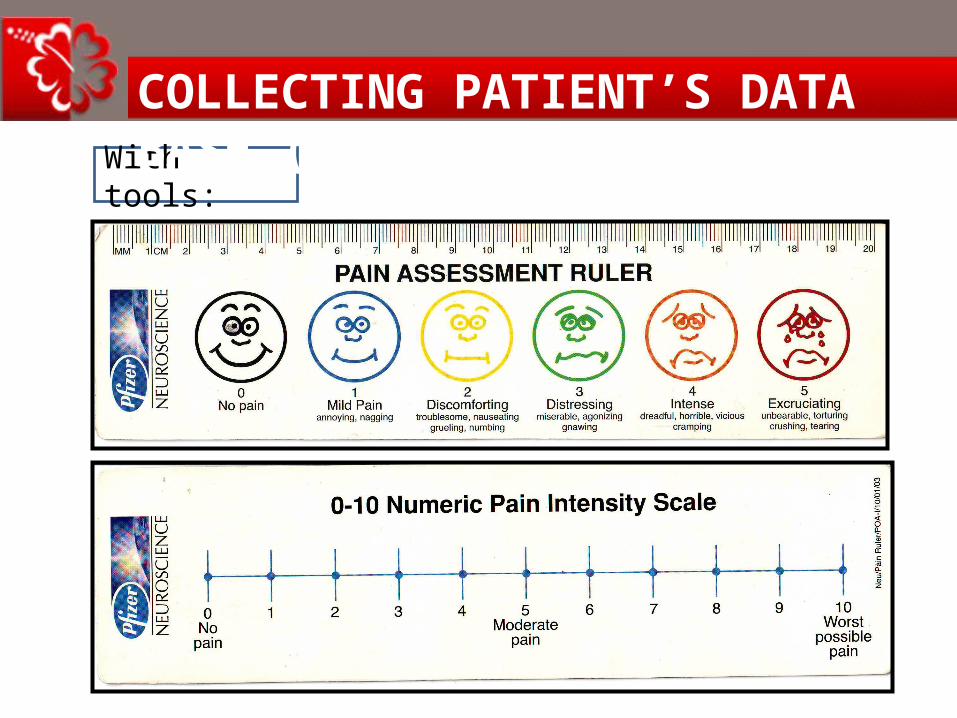
With tools:
COLLECTING PATIENT’S DATA BASE (3)
CHAPTER 01: INTRODUCTION TO ANATOMY
3. CONSTRUCTING A PATIENT'S DRUG THERAPY PROBLEM LIST
3. Step THREE

CHAPTER 01: INTRODUCTION TO ANATOMY
4. DESIGNING AND RECOMMENDING A PHARMACIST’ S CARE PLAN
4. Step FOUR
CHAPTER 01: INTRODUCTION TO ANATOMY
5. MONITORING PHARMACIST’S CARE PLAN
5. Step FIVE
CHAPTER 01: INTRODUCTION TO ANATOMY
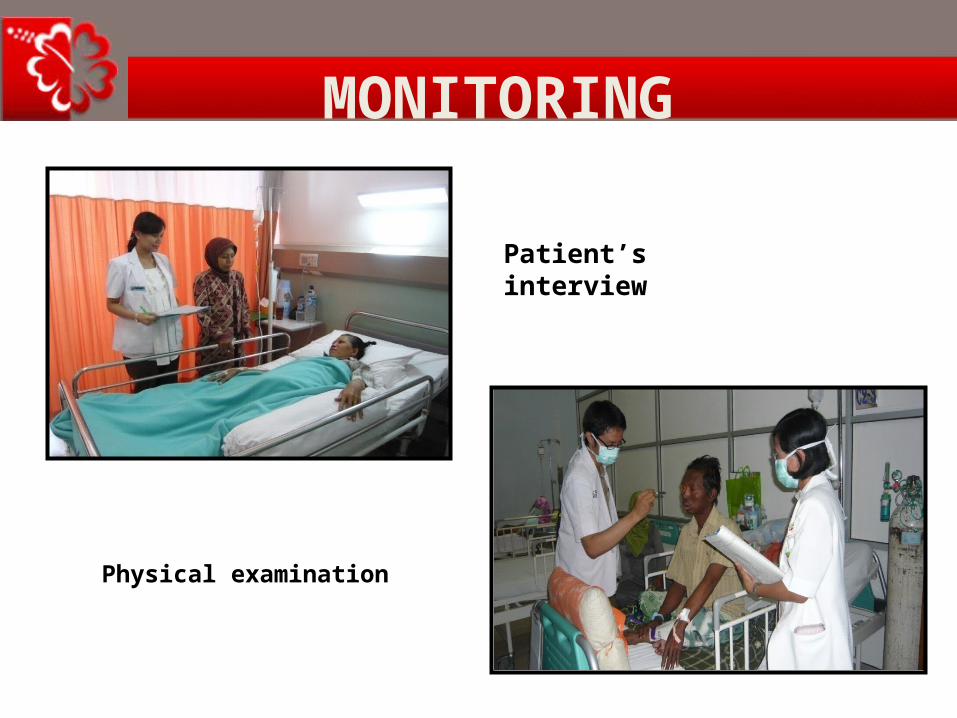
MONITORING
Physical examination
Patient’s interview

CHAPTER 01: INTRODUCTION TO ANATOMY
Steven Johnson's Syndrome

CHAPTER 01: INTRODUCTION TO ANATOMY
Steven Johnson's Syndrome

CHAPTER 01: INTRODUCTION TO ANATOMY
Red man’s syndrome

CHAPTER 01: INTRODUCTION TO ANATOMY
NaBic injeksi
CHAPTER 01: INTRODUCTION TO ANATOMY
TOOLS WHICH ARE NEEDED
1. Patient Medical Record (PMR)2. Understanding PMR3. Clinical Practice Guidelines4. Drug Use Guidelines5. Results of recent clinical trials6. Professional communication with other
health care providers

CHAPTER 01: INTRODUCTION TO ANATOMY
CRITICAL APPRAISAL
• A method of assessing and interpreting the evidence by systematically considering its validity, results and relevance to the area of work considered.
• Balance assessment of the benefit/strengths and flaws/weaknesses of a study
• Assessment of research protocol• Consideration of quantitative and
qualitative aspects
CHAPTER 01: INTRODUCTION TO ANATOMY
CRITICAL APPRAISAL CHECKLIST• CASP (Critical Skills Appraisal Programme) - http://www.phru.nhs.uk/casp/critical_appraisal_tools.htm
• JAMA Users’ Guides to the Medical Literature– http://www.cche.net/usersguides/main.asp
• Greenhalgh T (2001) How to Read a Paper, BMJ Books, London
• Crombie I (1996) The Pocket Guide to Critical Appraisal, BMJ Books, London
• BestBETs CA database– http://www.bestbets.org/cgi-bin/browse.pl?~show=appraisal
CHAPTER 01: INTRODUCTION TO ANATOMY
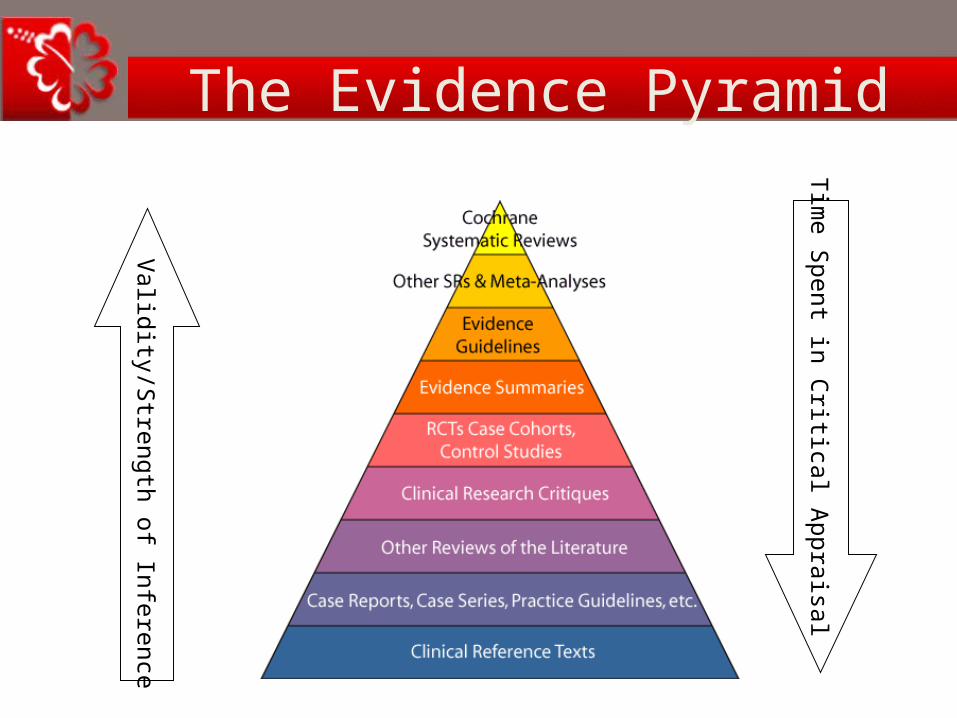
HIERARCHY OF EVIDENCE
Evidence is presented in many forms, and it is important to understand the basis on which it is stated. The value of evidence can be ranked according to the following classification in descending order of credibility:
I. Strong evidence from at least one systematic review of multiple well-designed randomised controlled trials.
II. Strong evidence from at least one properly designed randomised controlled trial of appropriate size.
III. Evidence from well-designed trials such as non-randomised trials, cohort studies, time series or matched case-controlled studies.
IV. Evidence from well-designed non-experimental studies from more than one centre or research group.
V. Opinions of respected authorities, based on clinical evidence, descriptive studies or reports of expert committees.

CHAPTER 01: INTRODUCTION TO ANATOMY
SOURCES OF SYSTEMATIC REVIEWS
• The Cochrane Library www.library.nhs.uk • DARE (in Cochrane Library ‘Other reviews’)• Health Technology Assessments (in Cochrane
Library ‘Technology Assessments’) • Medline, Cinahl, Embase search on ‘systematic
review’ in title, abstract• PubMed – Systematic Review in Limits > Topic• TRIP www.tripdatabase.com
CHAPTER 01: INTRODUCTION TO ANATOMY
The Evidence Pyramid
Validity/S
trength of Inference
Tim
e Spent in C
ritical Appraisal

CHAPTER 01: INTRODUCTION TO ANATOMY

CHAPTER 01: INTRODUCTION TO ANATOMY
CLINICAL PRACTICE GUIDELINES (CPG)
• Ministry of Health Malaysia. “Management of Type 2 Diabetes Mellitus”,
Malaysian MOH, May 2009.
• World Health Organization, CDC, NICE,
• Association of Medical Specialty.

CHAPTER 01: INTRODUCTION TO ANATOMY
THE CLINICAL PRACTICE GUIDELINES
CPG of Palliative Care

CHAPTER 01: INTRODUCTION TO ANATOMY
DRUG USE GUIDELINES
• Antibiotic Guidelines• Analgesic Guidelines• Respiratory Drugs Guidelines• Cardiology Drugs Guidelines• Endocrine Drugs Guidelines• Psychiatry Drugs Guidelines • Standard Operating Procedures
CHAPTER 01: INTRODUCTION TO ANATOMY
EXAMPLE OF AN EDUCATION BOOKLET

CHAPTER 01: INTRODUCTION TO ANATOMY
TERIMAKASIH

CHAPTER 01: INTRODUCTION TO ANATOMY
PLEASE VISIT MALAYSIA !







