

Apport du score calcique
chez le diabétique asymptomatique
en prévention primaire
Pr Paul VALENSI
Service d’Endocrinologie Diabétologie Nutrition, Hôpital Jean Verdier, Bondy
Service d’Endocrinologie Diabétologie Métabolisme, Hôpital Avicenne, Bobigny
SSR Nutrition Obésité, Hôpital René Muret, Sevran
Université Paris Nord

Déclaration de conflits d’intérêt potentiels de Paul Valensi
Conférences à la demande de Abbott, Bayer, Bristol Myers Squibb (BMS)-AstraZeneca (AZ), Eli-Lilly,
GlaxoSmithKline (GSK), Merck Santé, Merck Sharp Dohme (MSD), Novo Nordisk, Novartis, Pierre Fabre,
Sanofi
Crédits de recherche de la part de Abbott, Bayer, BMS-AZ, GSK, Merck Santé, Novo Nordisk
Participation à des Comités d’Experts pour Abbott, Astra Zeneca, BMS, Boehringer Ingelheim,
Daiichi-Sankyo, GSK, Kowa, Lilly, MSD, Novo Nordisk, Sanofi
Expert pour l’HAS, l’AFSSAPS, l’ANSM
Membre de la Task Force ESC/EASD sur Diabetes, Prediabetes and CVD
2013 et 2019
Problématique des explorations cv
chez le diabétique asymptomatique
• Trop d’examens
• Efficience non démontrée
• Réduction considérable des complications cv grâce à la PEC moderne
multifactorielle
• Justifiant des prescriptions d’examens plus rationalisées et
individualisées
• Importance de préciser le risque cv: hétérogène dans cette population
• Et pratiquer des explorations complémentaires seulement chez les
patients à très haut RCV
• Adaptation thérapeutique également selon le niveau de RCV

Gregg et al. N Engl J Med 2014;370:1514-23

Gaede P et al. N Engl J Med 2008;358:580-91
Macrovascular complications
The STENO 2 Study - 13.3 yrs Follow-up
- 59% RR
but this lets a 40%
residual risk

Influence du contrôle des fdr sur les évènements cv
5 facteurs considérés: HbA1c, PAS, albuminurie, LDL-C, tabac
Registre national suédois: 271174 DT2 vs 1355870 contrôles. Suivi moyen 5,7 ans. 175345 décès
Rawshani et al. NEJM 2018;379:633-44

Rawshani et al. NEJM 2018;379:633-44
Influence du contrôle des fdr sur les évènements cv
5 facteurs considérés: HbA1c, PAS, albuminurie, LDL-C, tabac
Registre national suédois: 271174 DT2 vs 1355870 contrôles. Suivi moyen 5,7 ans. 175345 décès
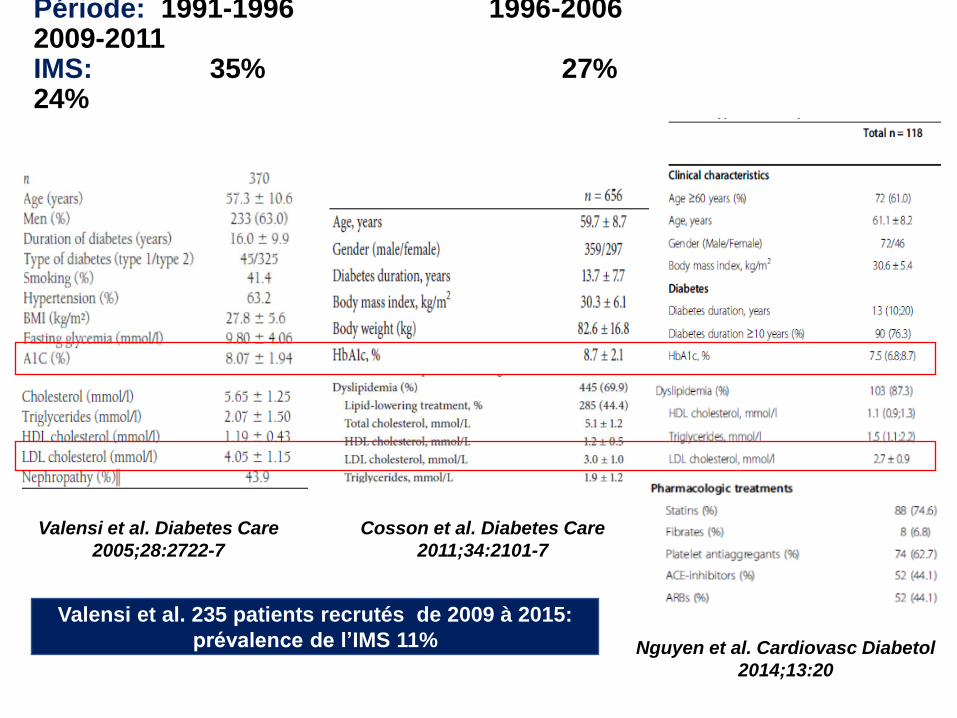
Période: 1991-1996 1996-2006 2009-2011 IMS: 35% 27% 24%
Valensi et al. 235 patients recrutés de 2009 à 2015:
prévalence de l’IMS 11%
Valensi et al. Diabetes Care
2005;28:2722-7
Cosson et al. Diabetes Care
2011;34:2101-7
Nguyen et al. Cardiovasc Diabetol
2014;13:20

Routine-
SMI-
Routine+
SMI-
Routine+
SMI+
Routine-
CS-
Routine-
CS+
Routine+
CS-
Routine+
CS+
Néanmoins l’existence d’une maladie coronaire silencieuse porte
un risque propre (en plus du risque estimé sur les fdr usuels)
Coronary stenoses SMI Hazard Function for patterns 1 - 4
PARTI EVMB
20181614121086420
Cu
m H
aza
rd
5
4
3
2
1
0
Combin Predicteur IM
IMS (+) FdR (+)
IMS (+) FdR (-)
IMS (-) FdR (+)
IMS(-) FdR (-)
Hazard Function for patterns 1 - 4
PARTI EVMB
20181614121086420
Cu
m H
aza
rd
5
4
3
2
1
0
Combin Predicteur CA
CAD (+) FdR (+)
CAD (+) FdR (-)
CAD (-) FdR (+)
CAD(-) FdR (-)
Routine-
SMI+
Risk estimated on routine factors including usual risk factors, peripheral vascular disease and nephropathy
Cosson et al. Diabetes Care 2011;34:2101-7

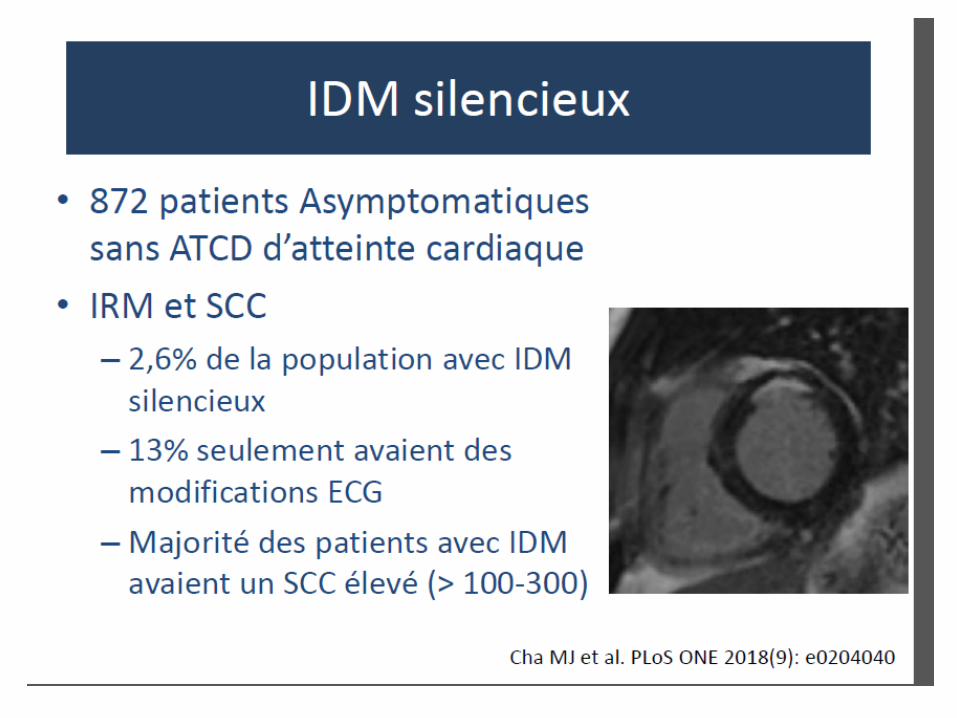
Infarctus du myocarde silencieux et insuffisance cardiaque silencieuse
• Encore une réalité
• ECG: les IDM silencieux représenteraient 40% des IDM
• Plus forte prévalence selon échocardiographie, scintigraphie
myocardique, IRM
Valensi et al. Arch Card Vasc Dis 2011;104:178-88
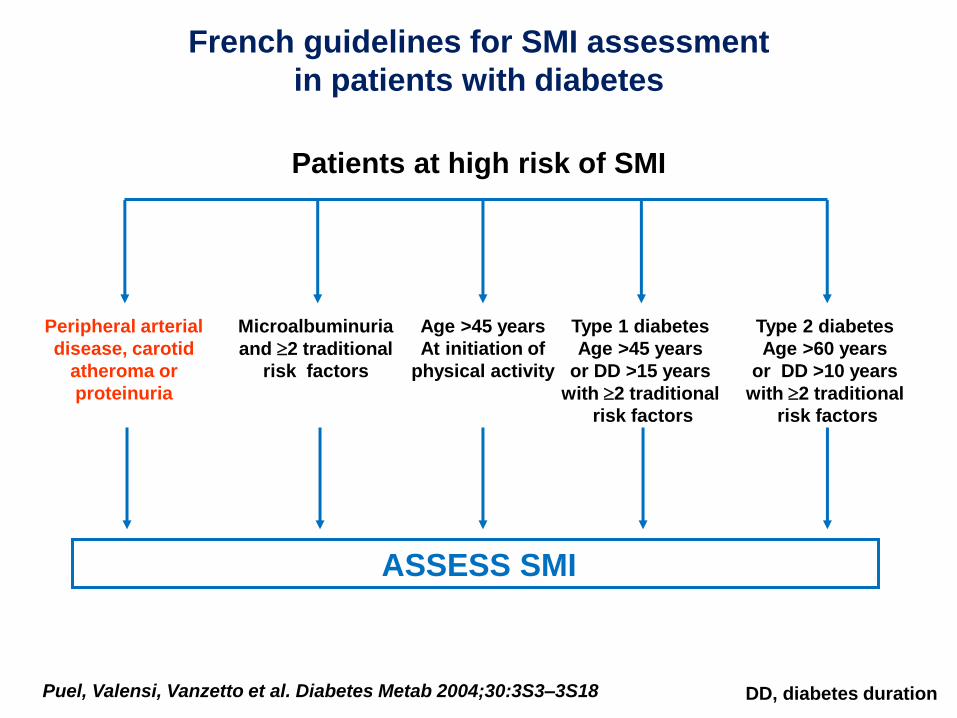
Puel, Valensi, Vanzetto et al. Diabetes Metab 2004;30:3S3–3S18
French guidelines for SMI assessment
in patients with diabetes
Peripheral arterial
disease, carotid
atheroma or
proteinuria
Microalbuminuria
and 2 traditional
risk factors
Age >45 years
At initiation of
physical activity
Type 1 diabetes
Age >45 years
or DD >15 years
with 2 traditional
risk factors
Type 2 diabetes
Age >60 years
or DD >10 years
with 2 traditional
risk factors
ASSESS SMI
DD, diabetes duration
Patients at high risk of SMI

Recommandations ADA: Coronary Heart Disease
Screening
• In asymptomatic patients, routine screening for CAD
isn’t recommended & doesn’t improve outcomes
provided ASCVD risk factors are treated. A
• Consider investigations for CAD with: – Atypical cardiac symptoms (e.g. unexplained dyspnea, chest discomfort)
– Signs or symptoms of associated vascular disease incl. carotid bruits, transient ischemic attack, stroke, claudication or PAD
– EKG abnormalities (e.g. Q waves) E
American Diabetes Association Standards of Medical Care in Diabetes.
Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87

2013 ESC Guidelines on Diabetes,
Pre-diabetes and Cardiovascular Diseases Developed in Collaboration with EASD
Co-chairs
Lars Rydén (ESC; Sweden) Peter J. Grant (EASD; United Kingdom) Task Force Members
European Heart Journal doi:10.1093/eurheartj/eht108

Recommendations for Cardiovascular Risk
Assessment in Dysglycaemia
Recommendations Class Level
It should be considered to classify patients with DM as at very high or high risk for CVD depending on the presence of concomitant risk factor and target organ damage.
IIa B
It is not recommended to assess the risk for CVD in patients with DM based on risk scores developed for the general population.
III B
It is indicated to estimate the urinary albumin excretion rate when performing risk stratification in patients with DM.
I A
Screening for silent myocardial ischaemia may be considered in selected high risk patients with DM.
IIb C
Patients at very high risk include in particular those with evidence of target organ damage:
proteinuria or renal failure, peripheral artery disease, left ventricle hypokinesia,
or other markers: high CAC score, ankle brachial index, pulse wave velocity
ESC guidelines in collaboration with EASD. Ryden et al. Eur Heart J 2013

Comment évaluer le RCV chez les diabétiques ?
• Equations ou scores de risque de la population générale:
non valides
• Scores spécifiques aux diabétiques: non valides
• Considérer les fdr classiques: qualitatif ou semi-quantitatif
- âge, HTA, atcd familiaux cv précoces, tabac, lipides, AOMI
- spécifiques: durée diabète, néphropathie (micro, macro, IR), HbA1c,
et…dysfonction érectile, rétinopathie, NAC…
• Combien pèse chaque fdr? Influence de durée d’exposition, intensité,
correction?
Et combien pèse l’ensemble?
• Intérêt d’un intégrateur ou modificateur de risque
• Surtout si risque intermédiaire ou élevé
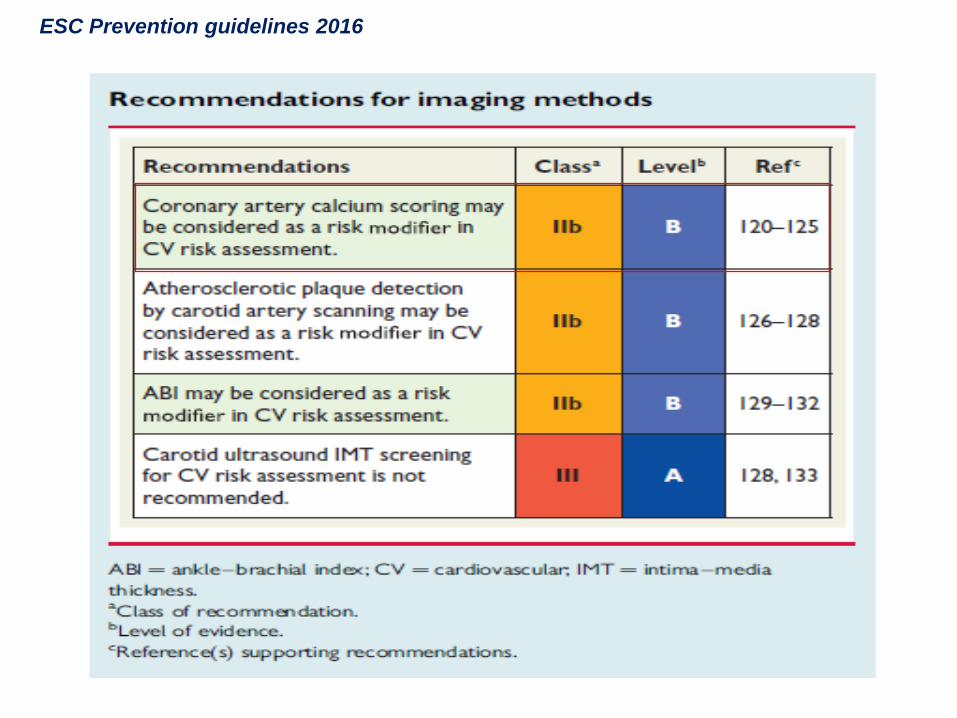
ESC Prevention guidelines 2016


Very high risk Patients with DM and established CVD
or other target organ damage *
or three or more major risk factors **
High risk Patients with DM without target organ damage, with DM duration ≥ 10 yrs plus any
other additional risk factor
Moderate risk
Young patients (T1DM < 35 yrs; T2DM < 50 yrs) with DM duration (<10 yrs)
and without other risk factors
* proteinuria / renal failure (GFR <30 ml/min/m2), CAC score > 100 or 400,
ABI < 0.85, ECG or echocardiographic abnormalities (LV hypokinesia, dilatation…)
** hypertension/ smoking/ family history of early CVD / dyslipidemia/ cardiac autonomic neuropathy
Stratification du RCV chez les diabétiques

Score calcique coronaire
• Examen simple, non invasif, peu coûteux
• Evaluation du risque cv. « Risk modifyer »
• Première étape dans la recherche d’une maladie
coronaire silencieuse
• Modifie les objectifs et les modalités thérapeutiques
• Personnalisation du traitement


Fréquence d’un score calcique élevé et
déterminants chez les diabétiques
• Dans une population de 510 DT2 asymptomatiques (Anand et al. Eur Heart J 2006;27:713-21)
CAC > 100 chez 28% des patients
Prédicteurs du CAC: âge, sexe masculin, ethnicité, HTA, ancienneté du diabète,
traitement par statine, score UKPDS et score de Framingham
• Dans l’étude RACED, CAC déterminé chez 301 DT2 participant à l’étude VADT
(Reaven et al. Diabetes 2009;58:2642-8), âge moyen 61 ans, durée moyenne de diabète 12 ans
- CAC nul dans 16% des cas
- CAC > 100 chez 62% et même > 400 chez 40% des patients
- relation significative entre rétinopathie et CAC (Reaven et al. Diabetes Care 2008;31:952-7)
• Etude chez 2018 patients en IRC, > 40% diabétiques (He J et al. Am J Cardiol 2012;110:1735-41)
CAC > 100 chez 35% et corrélé à la sévérité de l’IR


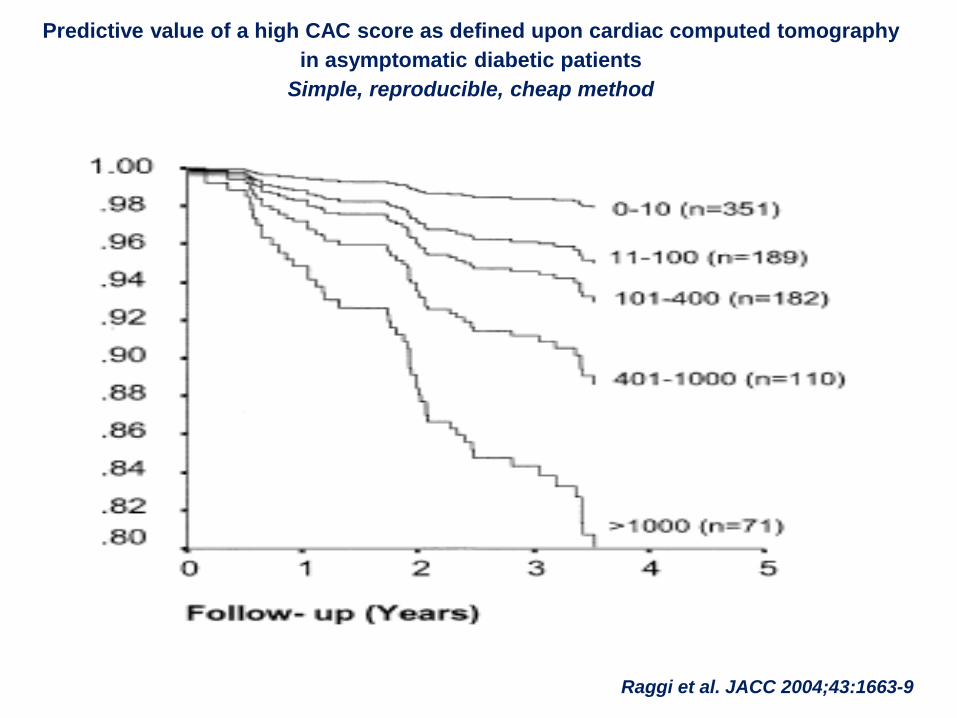
Predictive value of a high CAC score as defined upon cardiac computed tomography
in asymptomatic diabetic patients
Simple, reproducible, cheap method
Raggi et al. JACC 2004;43:1663-9

Valeur prédictive de décès cv ajoutée par le CAC score
Subhashish A et al. Diabetes Care 2013 36:972–77

Un CAC score élevé est associé à la mise en évidence
d’une ischémie silencieuse à la scintigraphie
myocardique de stress
D’après Hacker et al. J Nucl Cardiol 2011;18:700-11

r=0,318; p<0,0001
Relation entre CAC et âge dans notre population de DT2

Valensi et al. ADA 2016
Prospective series of 235 T2Ds recruited between 2009 and 2015
All with a very high risk as evidenced on nephropathy,
peripheral vascular disease or ≥ 3 associated risk factors
SMI+
CAC score ≥ 100 14.6%
CAC score < 100 7.8%
SMI, n (%)
24 (10.2%)
Significant coronary stenosis on
angiography, n
8 / 18 (3.4%)
CAC score ≥ 100 Agatston units, n (%)
82 (34.9%)

No SMI SMI, no
stenoses SMI, stenoses p
Number of patients 211 10 8
CAC AU, median (range) 213 (0-2796) 428 (0-2720) 1558 (27-3518) <0.01
% of patients
with CAC ≥ 100 AU
33.2 %
40.0 %
75.0 % < 0.05
% of patients
with CAC ≥ 400 AU
15.6 % 30.0 % 62.5 % < 0.01
Valensi et al. ADA 2016
Prospective series of 235 T2Ds recruited between 2009 and 2015
All with a very high risk as evidenced on nephropathy,
peripheral vascular disease or ≥ 3 associated risk factors
CAC ≥ 100:
sensitivity 50%, specificity 69%, PPV 15%, NPV 92%

Néphropathie patente et/ou macroangiopathie
IMS+ CAC ≥ 100 UA IMS + parmi les CAC < 100 UA
Oui: n=72 10 (13.9%) 38 (53%) 4/34 (12%)
Non: n=132 12 (9%) 25 (19%) 7/107 (7%)
CAC et IMS selon le niveau de risque a priori
VPN
88%
93%
Valensi et al. SFD 2017
Chez les patients à RCV intermédiaire ou élevé le CACS fait passer un patient sur 5 dans le RCV
très élevé et revêt une bonne VPN permettant de s’abstenir du dépistage dans environ 80% des cas
CACS élevé plus souvent
chez les patients avec
néphropathie patente ou
atteinte macroangiopathique
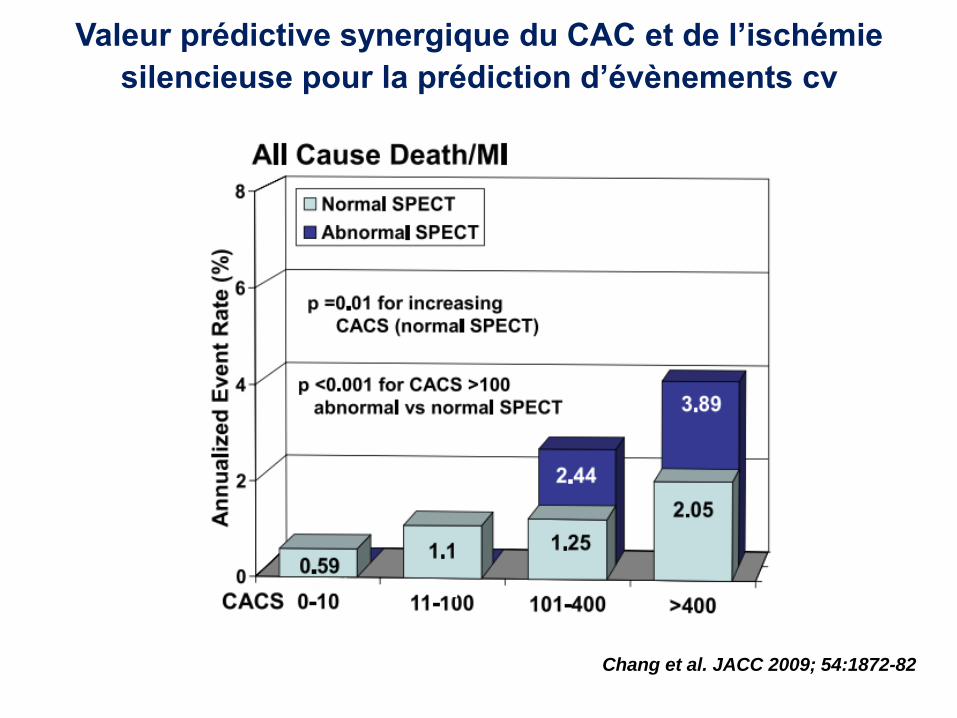
Valeur prédictive synergique du CAC et de l’ischémie
silencieuse pour la prédiction d’évènements cv
Chang et al. JACC 2009; 54:1872-82

Comment évaluer le RCV chez les diabétiques ?
• Considérer les fdr classiques: qualitatif ou semi-quantitatif
- âge, HTA, atcd familiaux cv précoces, tabac, lipides, AOMI
- spécifiques: durée diabète, néphropathie, HbA1c, et…
dysfonction érectile, rétinopathie, NAC…
• Combien pèse chacun? Durée d’exposition, intensité, correction
Et combien pèse l’ensemble?
• Intérêt d’un intégrateur ou modificateur de risque
• Surtout si risque intermédiaire ou élevé
Le CAC fait changer de strate le risque d’évènements cv
et aussi le risque de détecter une maladie coronaire silencieuse

Si CAC élevé
contrôler plus intensément les facteurs de risque
chercher une ischémie myocardique silencieuse
Et faut-il modifier le traitement médical ?
Selon le niveau de RCV
Selon CAC ?

Adaptation thérapeutique si CAC élevé
• Contrôle lipidique:
Objectif LDL-C < 0,70 g/l
Statines
Autres désordres lipidiques: non-HDL C
• Contrôle tensionnel:
130-140 mmHg / <80 mmHg
Bloqueur du SRA
• β – si ischémie
• Aspirine
• Objectif glycémique:
~ 7%, sans hypoglycémie
Classes réduisant le RCV

CAC et objectif glycémique
Among VADT participants intensive glucose-lowering therapy
reduces CVD events only in patients with lower CAC
Reaven et al. Diabetes 2009;58:2642-8

0 6 12 18 24 30 36 42 48 54
0
5
10
15
20
P la ce b o
Pa
tie
nts
with
an
eve
nt (%
)
Time from randomisation (months)
Composite MACE-3: CV death, non-fatal myocardial infarction, or non-fatal
stroke
Patients at risk
Liraglutide
Placebo
4668
4672
4593
4588
4496
4473
4400
4352
4280
4237
4172
4123
4072
4010
3982
3914
1562
1543
424
407
HR=0.87 95% CI (0.78 ; 0.97)
p<0.001 for non-inferiority p=0.01 for superiority
Marso SP et al. N Engl J Med 2016
0 6 12 18 24 30 36 42 48 54
0
5
10
15
20
L ira g lu t id e
0 6 12 18 24 30 36 42 48 54 0
5
10
15
20
GLP1-RA
LEADER
Bénéfice plus marqué chez les patients avec atcd cv

GLP1-RA
SUSTAIN-6
Marso et al. NEJM 2016

EMPAREG Outcome study
SGLT2-i
Surtout réduction des hospitalisations pour insuffisance cardiaque
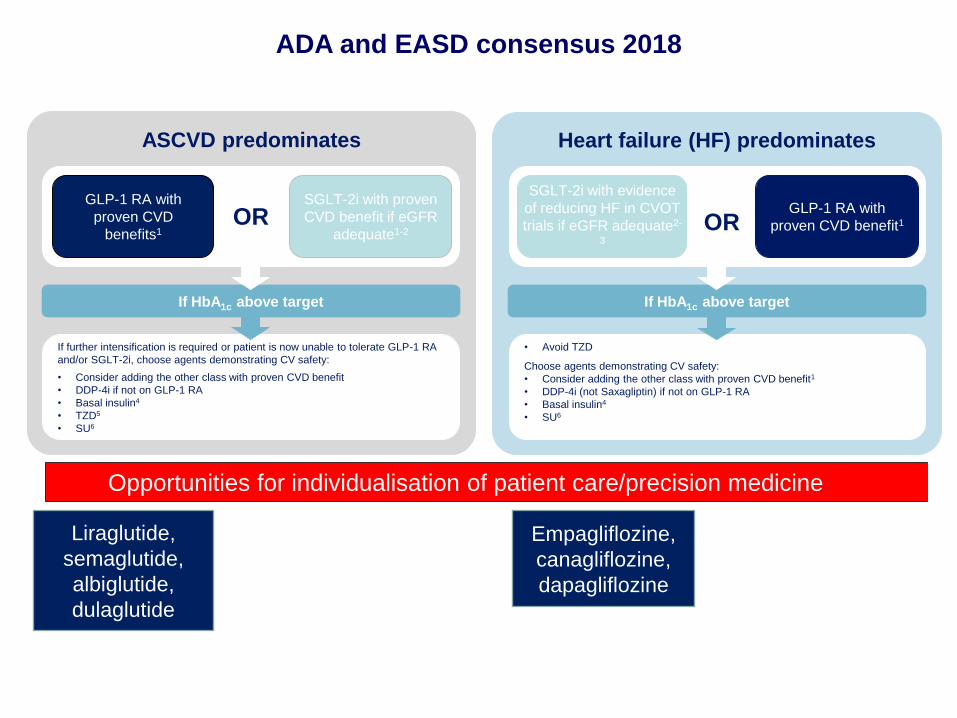
ADA and EASD consensus 2018
ASCVD predominates
If further intensification is required or patient is now unable to tolerate GLP-1 RA
and/or SGLT-2i, choose agents demonstrating CV safety:
• Consider adding the other class with proven CVD benefit
• DDP-4i if not on GLP-1 RA
• Basal insulin4
• TZD5
• SU6
If HbA1c above target
GLP-1 RA with
proven CVD
benefits1
SGLT-2i with proven
CVD benefit if eGFR
adequate1-2 OR
Heart failure (HF) predominates
• Avoid TZD
Choose agents demonstrating CV safety:
• Consider adding the other class with proven CVD benefit1
• DDP-4i (not Saxagliptin) if not on GLP-1 RA
• Basal insulin4
• SU6
If HbA1c above target
SGLT-2i with evidence
of reducing HF in CVOT
trials if eGFR adequate2-
3
GLP-1 RA with
proven CVD benefit1 OR
Opportunities for individualisation of patient care/precision medicine
Liraglutide,
semaglutide,
albiglutide,
dulaglutide
Empagliflozine,
canagliflozine,
dapagliflozine
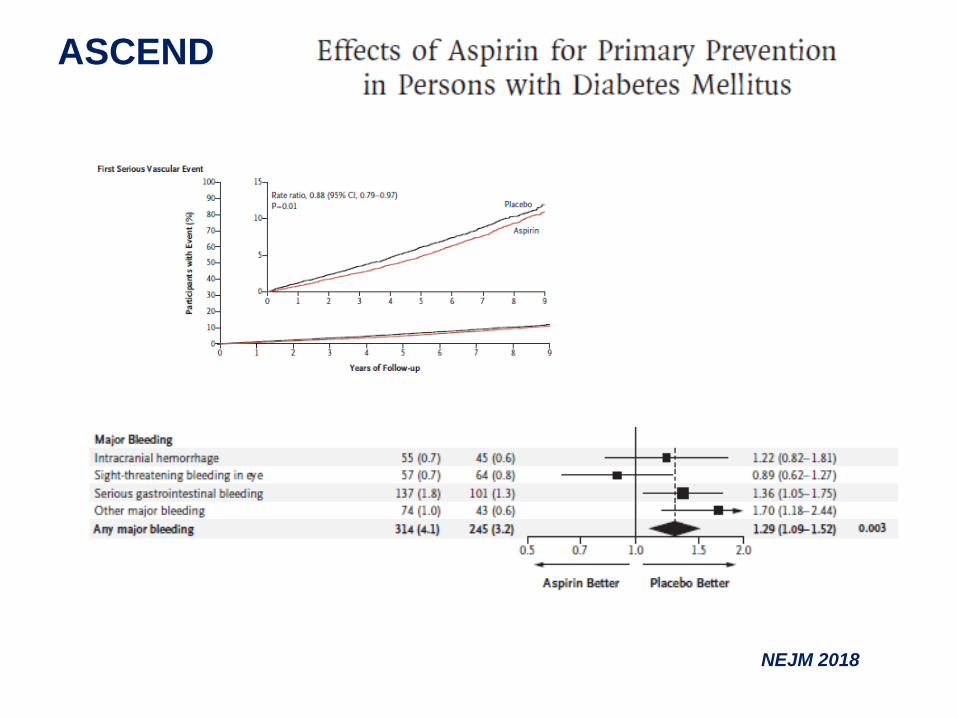
ASCEND
NEJM 2018

Rosanski et al. JACC 2011;57:1622-32
Avec meilleur contrôle des fdr dans le groupe Scan CAC


Risque modéré:
< 50 ans avec durée
diabète <10 ans
et sans autre fdr
Très haut RCV
CAC
0 – 10 11-100 >400
Pas d’autre
exploration
Faible capacité
à l’effort *
Diabétiques en prévention primaire, asymptomatiques, avec ECG normal
100-399
ou >75è
percentile
Et faible capacité
à l’effort*
Non Oui Oui Non
Scinti ou écho de stress
* Capacité d’effort < 2 étages ou effort <7 Mets
Scinti ou écho de stress
Suivi habituel
Haut RCV
Bilan avant
sport vigoureux
EE ou
scinti
ou
echo
stress Traitement cardio-protecteur







