

ISB
N 9
2890
5030
2
97
89
28
90
50
30
2
The rising burden of chronic illness, in particular the rapid increase in the number of people withmultiple health problems, is a challenge to health systems globally. Associated premature mortalityand reduced physical functioning, along with higher use of health services and related costs, areamong the key concerns faced by policy-makers and practitioners.
There is a clear need to redesign delivery systems in order to better meet the needs created bychronic conditions, moving from the traditional, acute and episodic model of care to one that bettercoordinates professionals and institutions and actively engages service users and their carers.Many countries have begun this process but it has been difficult to reach conclusions about thebest approach to take: care models are highly context-dependent and scientifically rigorous evaluations have been lacking.
Assessing chronic disease management in European health systems explores some of the key issues, ranging from interpreting the evidence base to assessing the policy context for, and approaches to, chronic disease management across Europe. Drawing on 12 detailed country reports(available in a second, online volume), the study provides insights into the range of care modelsand the people involved in delivering these; payment mechanisms and service user access; andchallenges faced by countries in the implementation and evaluation of these novel approaches.
This book builds on the findings of the DISMEVAL project (Developing and validating DISease Management EVALuation methods for European health care systems), led by RAND Europe andfunded under the European Union’s (EU) Seventh Framework Programme (FP7) (Agreement no. 223277).
The editors
Ellen Nolte, Hub Cordinator, European Observatory on Health Systems and Policies.
Cécile Knai, Senior Lecturer, London School of Hygiene & Tropical Medicine.
Richard B. Saltman, Professor of Health Policy and Management at the Rollins School of PublicHealth of Emory University in Atlanta and Associate Head of Research Policy at the EuropeanObservatory on Health Systems and Policies.
Observatory Studies Series No. 37
37
Obs
erva
tory
S
tudi
es S
erie
s
37Ed
ited
by
Elle
n N
olte
, Cé
cile
Kn
ai, R
ich
ard
B S
altm
an
AS
SES
SIN
G CH
RO
NIC D
ISEA
SE M
AN
AGEM
ENT IN
EUR
OPEA
N H
EALTH
SYSTEMS
Concepts and approaches
Assessing chronic disease management in European health systems
Edited by
Ellen Nolte
Cécile Knai
Richard B. Saltman
Cover_WHO_nr37_bis_Mise en page 1 5/02/15 15:39 Page 1

Assessing chronic disease management in European health systems

The European Observatory on Health Systems and Policies supports and promotes evidence-based health policy-making through comprehensive and rigorous analysis of health systems in Europe. It brings together a wide range of policy-makers, academics and practitioners to analyse trends in health reform, drawing on experience from across Europe to illuminate policy issues.
The European Observatory on Health Systems and Policies is a partnership, hosted by the WHO Regional Office for Europe, which includes the Governments of Austria, Belgium, Finland, Ireland, Norway, Slovenia, Sweden, the United Kingdom and the Veneto Region of Italy; the European Commission; the World Bank; UNCAM (French National Union of Health Insurance Funds); the London School of Economics and Political Science; and the London School of Hygiene & Tropical Medicine.

Assessing chronic disease management in European health systems
Concepts and approaches
Edited by
Ellen NolteCécile KnaiRichard B. Saltman
on Health Systems and Policies
European
a partnership hosted by WHO

iv Assessing chronic disease management in European health systems
Keywords:CHRONIC DISEASEDELIVERY OF HEALTH CARE, INTEGRATEDHEALTH CARE SYSTEMSHEALTH POLICYPUBLIC HEALTH
© World Health Organization 2014 (acting as the host organization for, and secretariat of, the European Observatory on Health Systems and Policies)
All rights reserved. The European Observatory on Health Systems and Policies welcomes requests for permission to reproduce or translate its publications, in part or in full.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the European Observatory on Health Systems and Policies concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the European Observatory on Health Systems and Policies in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the European Observatory on Health Systems and Policies to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the European Observatory on Health Systems and Policies be liable for damages arising from its use. The views expressed by authors, editors, or expert groups do not necessarily represent the decisions or the stated policy of the European Observatory on Health Systems and Policies or any of its partners.
ISBN 978 92 890 5030 2
Printed in the United Kingdom
Cover design by M2M
Address requests about publications to: Publications, WHO Regional Office for Europe, UN City, Marmorvej 51, DK-2100 Copenhagen Ø, Denmark.
Alternatively, complete an online request form for documentation, health information, or for permission to quote or translate, on the Regional Office web site (http://www.euro.who.int/pubrequest).
Contents
Preface vii
Acknowledgement ix
List of tables and boxes xi
List of abbreviations xiii
Volume I contributors xv
1 Introduction 1 1.1 Background 1 1.2 Approach to this book 3 1.2.1 Conceptualizing chronic disease and chronic disease management 4 1.2.2 Countries included in the review 7 1.3 About this book 7
2 What we know: a brief review of the evidence of approaches to chronic care 9 2.1Managingcareforpeoplewithchronicconditions:conceptsanddefinitions 9 2.1.1 Disease management 10 2.1.2 Integrated care 11 2.2 What we do know: a review of the evidence base on approaches to caring for people with chronic conditions 12 2.2.1 Disease management 12 2.2.2 Integrated care 15 2.2.3 Economic impacts of disease management or integrated care 18 2.3 What we need to know: limitations of the existing evidence base 19 2.4 Conclusions 21
3 Approaches to chronic disease management in Europe 23 3.1 Key features of the health care systems in 12 European countries 23 3.2 The policy context for chronic care in Europe 25 3.3 Overview of approaches to chronic disease management in 12 European countries 30 3.4 Financing, distribution and uptake of approaches to chronic disease management 42 3.5 Components of chronic disease management 55 3.6 Conclusions 70 3.6.1 The majority of approaches tend to focus on populations with definedconditions 70

vi Assessing chronic disease management in European health systems
3.6.2 There is a trend towards strengthening the role of nurses in care delivery and coordination 71 3.6.3 Approaches that seek to reduce barriers between sectors remain less common 71 3.6.4Theimplementationofapproachesfrequentlyinvolvesfinancial incentives 72 3.6.5 Levels of patient and clinician support vary 72
4 Looking ahead 73 4.1 Learning from existing approaches 74 4.1.1 Incorporating the patient perspective 80 4.2 Providing the (regulatory) context to enable innovation 83References 85

Preface
This book comprises two volumes and builds on the findings of the DISMEVAL project (Developing and validating DISease Management EVALuation methods for European health care systems), funded under the European Union’s (EU) Seventh Framework Programme (FP7) (Agreement no. 223277). DISMEVAL was a three-year European collaborative project conducted between 2009 and 2011. It contributed to developing new research methods and generating the evidence base to inform decision-making in the field of chronic disease management evaluation (www.dismeval.eu).
In this book, we report on the findings of the project’s first phase, capturing the diverse range of contexts in which new approaches to chronic care are being implemented and evaluating the outcomes of these initiatives using an explicit comparative approach and a unified assessment framework. In this first volume, we describe the range of approaches to chronic care adopted in 12 European countries. By reflecting on the facilitators and barriers to implementation, we aim to provide policy-makers and practitioners with a portfolio of options to advance chronic care approaches in a given policy context.
In volume II (available online at http://www.euro.who.int/en/about-us/partners/observatory/studies), we present detailed overviews of each of the 12 countries reviewed for this work and which informed the overview presented in the first volume of the book.
Ellen NolteEuropean Observatory on Health Systems and Policies
Cécile KnaiLondon School of Hygiene & Tropical Medicine
Richard B. SaltmanEmory University in Atlanta

Acknowledgements
Led by RAND Europe, the DISMEVAL project brought together 10 partners in seven EU countries and a range of associates in five additional countries. The following members of and associates to this project contributed directly or indirectly to this book through the collection and synthesis of information and data, the drafting of country reports as presented in volume II of the book, and the review of chapters (affiliation at the time of the DISMEVAL project):
RAND Europe, Cambridge, UK: Laura Brereton, Annalijn Conklin, Saba Hinrichs, Ellen Nolte, Janice Pedersen, Martin Roland (special adviser to RAND Europe)
London School of Hygiene & Tropical Medicine, London, UK: Cécile Knai
Paracelsus Medizinische Privatuniversität, Salzburg, Austria: Maria Flamm, Andreas Sönnichsen
Københavns Universitet, Copenhagen, Denmark: Anne Frølich, Ramune Jacobsen
Université Paris Est Créteil Val de Marne, Paris, France: Matthias Brunn, Benjamin Cadier, Karine Chevreul, Isabelle Durand-Zaleski
Goethe Universität, Frankfurt am Main, Germany: Antje Erler, Birgit Fullerton
Universiteit Maastricht, the Netherlands: Arianne M.J. Elissen, Inge G.P. Duimel-Peeters, Cor Spreeuwenberg, Hubertus J.M. Vrijhoef
Centre Léon Bérard Lyon et Rhône-Alpes, Lyon, France: Fadila Farsi, Hélène Labrosse
Instituto de Salud Carlos III, Madrid, Spain: Zuleika Saz Parkinson, Antonio Sarria Santamera
AQUA Institut für angewandte Qualitätsförderung und Forschung im Gesundheitswesen, Göttingen, Germany: Robert Krohn, Boris Pöhlmann
In addition, the following experts contributed reports on individual countries not covered by the DISMEVAL partnership:
Estonia: Taavi Lai

x Assessing chronic disease management in European health systems
Hungary: Márton Csere, Peter GaalItaly: Antonio Giulio de Belvis, Walter Ricciardi, Maria Lucia Specchia, TD Luca ValerioLatvia: Maris TaubeLithuania: Liubove Murauskiene, Maria VeniuteSwitzerland: Isabelle Peytremann-Bridevaux, Bernard Burnand, Ignazio Cassis
Further, we would like to thank Jonathan North and Caroline White, as well as Peter Powell (typesetting) and Sonia Cutler (editing).

List of tables and boxes
Tables
Table 1.1 Differentiating acute and chronic conditions 4
Table 2.1 Review of reviews: evidence of the effect of disease management programmes 13
Table 3.1 Principlesofhealthcarefinancingin12Europeancountries 24
Table 3.2 Selected features of health care systems in 12 European countries 26
Table 3.3 Overview of approaches to chronic disease management or their equivalent in 12 European countries 33
Table 3.4 Financing, distribution and uptake of approaches to chronic disease management or their equivalent in 12 European countries 43
Table 3.5 Components of chronic disease management used in 12 European countries 57
Boxes
Box 1.1 Approaches to chronic disease management or chronic care: definitionofterms 5
Box 4.1 ReportedbarrierstoevaluationinfiveEuropeancountries 79
Box 4.2 Balancing the gap between policy intent and actual implementation: evidence from the DISMEVAL project 84

List of abbreviations
AIDS Acquired immunodeficiency syndromeASALEE Health Action by Teams of Self-employed Health Professionals (France)ASL Local Health Authority (Italy)AWBZ Exceptional Medical Expenses Act (Netherlands)BRASS Blaylock Risk Assessment Screening ScoreCAPI Contracts for Improved Individual Practice (France)CHD Coronary heart diseaseCHF Swiss francCCM Chronic Care ModelCCP Care coordination pilotCMP Care management programmeCNAM Caisse Nationale d’Assurance Maladie (France)COPA Coordinating Care for Older People (France)COPD Chronic obstructive pulmonary diseaseCVD Cardiovascular diseaseDBC Diagnosis and treatment combinations (Netherlands)DIEP Diabetes Interactive Education ProgrammeDDKM Danish Quality Model (Denmark)DKK Danish kroneDMP Disease management programmeDRG Diagnosis-related groupEBM Uniform Assessment Scale (Germany)EEP Evaluation of professional practice (France)EHIF Estonian Health Insurance FundEU European UnionFFS Fee-for-serviceFIQCS Intervention Fund for Quality and Care Coordination (France)GDP Gross domestic productGP General practitionerHAS National Authority for Health (France)HMO Health maintenance organizationICC Integrated care contractICP Integrated care pilotIGEA Diabetes Integration, Management and Assistance (Italy)IHD Ischaemic heart diseaseLKF Performance-based financing (Austria)MIGAC Missions d’intérêt général et à l’aide à la contractualisation (France)

xiv Assessing chronic disease management in European health systems
NIHFA National Health Insurance Fund Administration (Hungary) ÖDG Austrian Society of DiabetesOOP Out-of-pocketPbR Payment by result (England)PCT Primary Care Trust (England)PHC Primary health carePOPP Partnership for Older People Project (England)PPP Purchasing power parityPPS Personalized care programme (France)QALY Quality-adjusted life yearsQOF Quality and Outcomes Framework (England)RCP Multidisciplinary team meeting (France)ROSP Payment based on specific public health objectives (France)RSA Risk structure compensation scheme (Germany)SHI Statutory health insuranceSIKS Integrated Effort for People Living with Chronic Disease (Denmark)SSI State Serum Institute (Denmark)SSN National Health Service (Italy)URCAM Regional Unions of Insurance Funds (France)VerAH Care assistants in family practice (Germany)VHI Voluntary health insuranceWMO Social Support Act (Netherlands)ZiO Care in Development (Netherlands)

Volume I contributors
Cécile Knai is Senior Lecturer, Policy Innovation Research Unit, Faculty of Public Health and Policy, London School of Hygiene & Tropical Medicine, London, UK.
Ellen Nolte was the lead author and editor of the Volume. She is Hub Coordinator at the European Observatory on Health Systems and Policies, London School of Economics and Political Science, and London School of Hygiene & Tropical Medicine, London, UK.
Emma Pitchforth is Research Leader in the Health and Healthcare Research Programme at RAND Europe, Cambridge, UK.
Richard B. Saltman is Professor of Health Policy and Management at the Rollins School of Public Health of Emory University in Atlanta, Georgia, USA. He is also Associate Head of Research Policy at the European Observatory on Health Systems and Policies.

Chapter 1
IntroductionEllen Nolte, Cécile Knai
1.1 Background
Responding to the burden of chronic disease presents challenges for all health systems. As populations age and advances in health care allow those with once fatal conditions to survive, the prevalence of chronic conditions is rising in many countries (Yach et al., 2004). In the European Union (EU), in 2006, from 20 to over 40% of the population aged 15 years and over reported a long-standing health problem and one in four received long-term medical treatment (TNS Opinion & Social, 2007). Other studies have found the prevalence of common chronic disorders was found to be around 50% among adults aged 18 and over in seven high-income countries, including Germany, the Netherlands and the UK (Schoen et al., 2007).
Although the rising burden of chronic disease is driven, in part, by population ageing it is important to recognize that such conditions are not limited to the older population. Thus, increasing numbers of children and young people are developing some form of chronic health problem (Barnett et al., 2012; Van Cleave, Gortmaker & Perrin, 2010), with over 80% of premature mortality estimated to be attributable to noncommunicable diseases in Europe (Institute for Health Metrics and Evaluation, 2013a).
Assessing the precise level, distribution and nature of the chronic disease burden in Europe remains a challenge (Pomerleau, Knai & Nolte, 2008); yet, it is clear that chronic diseases are important, greatly impacting on the years of life lived in good health. In high-income countries, mental disorders (for example, depression and anxiety disorder), musculoskeletal disorders (for example, lower-back pain), chronic obstructive pulmonary disease (COPD) or asthma, and diabetes, are among the leading causes of chronic disability (Institute for Health Metrics and Evaluation, 2013b), with diabetes projected to rise further in importance during the next two decades, especially against the background

2 Assessing chronic disease management in European health systems
of increasing levels of overweight and obesity (Danaei et al., 2013; Finucane et al., 2011).
The implications for health systems and society as a whole are considerable. Chronic diseases pose a sizeable burden for national economies, with associated costs estimated at up to 7% of a country’s gross domestic product (Suhrcke et al., 2006). Societal costs arise partly as a result of direct health care costs, including from health care use, medication and potentially costly interventions, with additional indirect costs deriving from, for example, increased absenteeism, and reduced productivity at work (Suhrcke, Fahey & McKee, 2008). These challenges add to the complexity facing health systems, which require effective measures to prevent disease through reducing the major chronic disease risk factors and addressing influences that drive exposure (Novotny, 2008), while also providing services to meet the requirements caused by chronic health problems, thereby ensuring that people with established disease can participate in society.
The goals of care for those with chronic conditions are not to cure but to enhance functional status, minimize distressing symptoms, prolong life through secondary prevention and enhance the quality of life (Grumbach, 2003). These goals are unlikely accomplished through the traditional acute, episodic model of care, which tends to see the patient as passive recipient of care and where treatment aims at return to normal (Holman & Lorig, 2000). In particular, where people have multiple health problems, creating a range of diverse and sometimes contradictory needs, the conventional care model is insufficient (Piette, Richardson & Valenstein, 2004). Instead, what is needed is a delivery model that involves coordinated inputs from a wide range of health professionals over an extended period of time and that places patients at the centre as co-producers of care to optimize health outcomes (Nolte & McKee, 2008a).
However, service delivery has developed in ways that have tended to fragment care, both within and between sectors, for example, through structural and financial barriers at the interface between primary and secondary care and between health and social care, distinct organizational and professional cultures and differences in terms of governance and accountability (Glasby, Dickinson & Peck, 2006). There is thus a need for new service delivery models that are characterized by collaboration and cooperation among professions and institutions that have traditionally worked separately.
The growing recognition of this need is causing many countries to explore new approaches to health care delivery that can bridge the boundaries between professions, providers and institutions and therefore provide appropriate

3Introduction
support to patients with long-standing health problems. We have previously shown how countries vary in their attempts to do so, with many implementing some form of (chronic) disease management although the nature and scope of related approaches differ (Nolte, Knai & McKee, 2008). We have found that the strategies that are being implemented tend to reflect the characteristics of individual health systems with regard to the relationships between, and the responsibilities of, different stakeholders in the regulation, funding and delivery of health care. In particular, there is a suggestion that those health systems in which patients have traditionally chosen their provider without formal enrolment, paying for services episodically using fee-for-service as the predominant method of reimbursement, may face the greatest challenges in adapting towards providing effective chronic care (Busse & Mays, 2008).
However, there is a need to develop this evidence base further, using an explicit comparative approach and a unified framework for assessment to better understand the diverse range of contexts in which new approaches to chronic care are being implemented, and to evaluate the outcomes of these initiatives. There is also a need to better understand the content of these new models, which are frequently applied from different disciplinary and professional perspectives and are associated with different goals. In this book, we aim to contribute to this process by identifying the range of approaches to chronic care adopted in 12 European countries. By reflecting on facilitators and barriers to implementation we aim to provide policy-makers and practitioners with a portfolio of options to advance chronic care approaches in a given policy context.
1.2 Approach to this book
We build on earlier work which examined the health system context for chronic disease (Nolte & McKee, 2008a), assessed the evidence base for chronic care (Nolte & McKee, 2008b) and reviewed the experience in eight countries in Europe and beyond (Nolte, Knai & McKee, 2008). It seeks to extend this earlier work by drawing on information on approaches to (chronic) disease management and evaluation strategies in a range of European countries that was collected within the DISMEVAL (Developing and validating DISease Management EVALuation methods for European health care systems) project. DISMEVAL was a three-year European collaborative project, conducted between 2009 and 2011, which aimed to contribute to developing new research methods and to generating the evidence base to inform decision-making in the field of chronic disease management evaluation. It was funded under the European Commission’s Seventh Framework Programme.

4 Assessing chronic disease management in European health systems
1.2.1 Conceptualizing chronic disease and chronic disease management
Chronic conditions or chronic health problems have been described in different ways (Nolte, McKee & Knai, 2008); it is therefore important to briefly set out the terminology we will be using throughout this book. We adopted a general definition, which is principally based on the effects and associated care needs, rather than the cause of the condition in question (Unwin, Epping Jordan & Bonita, 2004). We distinguished acute conditions, which are potentially curable within a short period of time, from chronic conditions, which are either incurable or require prolonged treatment and care, and for which there is a chance of developing intercurrent episodes or acute illnesses associated with the chronic condition (Holman & Lorig, 2000). This differentiation is summarized in Table 1.1.
Table 1.1 Differentiating acute and chronic conditions
Acute condition Chronic condition
Onset Abrupt Generally gradual and often subtle
Duration Limited Lengthyorindefinite
Cause Typically single cause Typically multiple causes with changes over time
Diagnosis and prognosis Usually accurate Frequently uncertain
Technological intervention Usually effective Often indecisive, adverse effects common
Outcome Cure possible No cure
Uncertainty Minimal Pervasive
Knowledge Professionals knowledgeable, patients inexperienced
Professionals and patients have complementary knowledge and experiences
Sources: adapted from Department of Health (2004), based on Holman & Lorig (2000).
This definition includes a range of common, long-term health problems such as diabetes, heart disease or COPD, and progressive mental and neurological disorders. It also includes disabilities and impairments not defined as diseases, such as musculoskeletal disorders, and selected communicable diseases such as human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) (Nolte & McKee 2008a). We also consider cancer, as in some settings approaches to chronic disease management may also target certain cancer sites, for example, breast cancer disease management programmes in Germany or cancer networks in France (Nolte, Knai & McKee, 2008).
We restricted the scope of approaches reported in this book to the management of people with established chronic health problems although we also considered measures of secondary prevention targeted at people at high risk of developing a chronic disabling disease, such as vascular risk management. However, we

5Introduction
excluded measures of primary prevention or health promotion in the context of this work.
Although the DISMEVAL project focused on approaches that can be broadly subsumed under the heading of “disease management”, it is important to acknowledge that definitions of this concept vary widely (Krumholz et al., 2006; Nolte & McKee, 2008b). We discuss this variation in terminology, and its implications for deriving a robust evidence base, further in Chapter 2. At the outset, and for the purposes of the DISMEVAL project, we defined disease management as comprising the following components: (1) an integrated approach to care or coordination of care among providers, including physicians, hospitals, laboratories and pharmacies; (2) patient education; and (3) monitoring or collecting patients’ outcome data for the early detection of potential complications (Krumholz et al., 2006). However, we acknowledge that approaches that are being tested across Europe may not fully meet this definition. Our study sought to capture the range of models that use a subset of disease management interventions or are otherwise conceptualized while pursuing the same objective, that is, to improve the care for those with chronic health problems. We therefore included a wider range of approaches, which we considered as “chronic disease management” or chronic care. Box 1.1 provides an overview of the range of approaches reviewed in this study.
Box 1.1Approachestochronicdiseasemanagementorchroniccare:definitionofterms
Care pathway(s) (synonyms: clinical pathway; care map; integrated care pathway):
Task-oriented care plan(s) that specify essential steps in the care of patients with a
specificclinicalproblemanddescribethepatient’sexpectedclinicalcourse(Campbell
et al., 1998).
Case management: Intensive monitoring of a person with complex needs by a named
case manager – usually a (specialist) nurse – through the development of care or
treatment plans that are tailored to the needs of the individual patient who is at high risk
socially,financiallyandmedically(Krumholzetal.,2006).
Chronic care model (CCM): A conceptual framework that presents a structure
for organizing health care comprising of four key components: (1) self-management
support; (2) delivery system design; (3) decision support; and (4) clinical information
systems (Wagner et al., 1999).
Coordinated care (synonyms: care management): Development and implementation
of a therapeutic plan designed to integrate the efforts of medical and social service
providers, often involving designated individuals to manage provider collaboration.

6 Assessing chronic disease management in European health systems
Box 1.1 contd
Disease management (programme) (DMP):Definitionsofdiseasemanagement
(programmes) vary substantially. Common features are: (1) an integrated approach to
care/coordination of care among providers, including physicians, hospitals, laboratories
and pharmacies; (2) patient education; and (3) monitoring/collecting patient outcomes
data for the early detection of potential complications (Krumholz et al., 2006). DM
programmes do not normally involve general coordination of care. They also not
normallyincludepreventiveservicessuchasfluvaccination.
Integrated care: Types of collaboration, partnerships or networks between providers
of health and social care services that work together to meet the multidimensional
needs of an individual patient/client or a category of persons with similar needs/
problems (Kodner & Spreeuwenberg, 2002; Nies & Berman, 2004).
Managed discharge: Arrangements for the transfer of an individual from hospital to
an appropriate setting (primary care; community care) to ensure that any rehabilitation,
recuperationandcontinuinghealthandsocialcareneedsareidentifiedandmet.
Multidisciplinary team(s)/care: An “extension” of case management that also
normally involves the development of treatment plans tailored to the medical,
psychosocialandfinancialneedsofpatients.Itskeyfeatureistheuseofabroader
range of medical and social support personnel (including physicians, nurses,
pharmacists, dietitians, social workers and others) to facilitate transition from inpatient
acute care to long-term, outpatient management of chronic illness (Krumholz et al.,
2006)
Nurse-led clinic: A formalized and structured health care delivery arrangement in
whichanursewithadvancedcompetencetopractiseinaspecifichealthcarearea
(nursepractitioner,clinicalnursespecialist,specialistnurse)actsasthefirstpointof
contact of care. The nurse manages patients either independently or interdependently
with other members of a health care team in at least 80% of their work. The key
interventions are: nursing therapeutics, encompassing assessment and evaluation;
health teaching/counselling; treatment and procedures; and case management. (NB:
Nurse-led clinics are different from nurse-led care insofar as the former describe a
formalized and structured delivery arrangement, whereas the latter also includes other
arrangements, for example, case management, liaison nurses, discharge nurse, etc.)
(Wong & Chung, 2006).
Provider network(s): A group of providers bringing together different levels of care (for
example, health and social care or primary and secondary care).
Source: compiled by the authors

7Introduction
1.2.2 Countries included in the review
We selected 12 countries for review: Austria, Denmark, England, Estonia, France, Germany, Hungary, Italy, Latvia, Lithuania, the Netherlands and Switzerland (the only non-EU country). Five of these countries (Denmark, England, France, Germany and the Netherlands) were reviewed in previous work (Nolte, Knai & McKee, 2008), but as these have further developed existing approaches or have implemented new approaches, their experience can provide important insights into the factors that have made these developments possible (or indeed hindered further advancement).
The review was based on a structured template for the collection of data on approaches to chronic disease management in European systems, which was based on earlier work by Nolte, Knai and McKee (2008), and informed, to great degree, by the Chronic Care Model developed by Wagner and colleagues in the United States (Wagner, 1998). Data collection was undertaken by key informants in the countries under review. It was beyond the scope of this study to provide a comprehensive inventory of all approaches being implemented in a given country; key informants were asked to present a “sample” of approaches considered representative of a given health system in terms of the type and setting of delivery model, providers involved, key strategies employed and the population covered. Data presented here reflect information collected by the summer of 2011, with updates to early 2014 where necessary and appropriate. Country reports formed the basis of the systematic cross-country comparison presented in this book. Further detail on the data collection that informed country reports is provided in the accompanying volume to this book (Nolte & Knai, 2015).
1.3 About this book
We begin in Chapter 2 with a brief review of the peer-reviewed literature on chronic disease management. In Chapter 3, we report on the key observations from our survey of 12 European countries on approaches to chronic care. We conclude with Chapter 4, which provides a summary analysis of findings reported in earlier sections. We suggest that this book should be read in conjunction with a second volume, which presents detailed overviews of each of the 12 countries reviewed for this work and which informed the summary overview presented in this book (Nolte & Knai, 2015).

Chapter 2
What we know: a brief review of the evidence
of approaches to chronic care
Ellen Nolte, Emma Pitchforth
This chapter provides a brief overview of the evidence base for chronic care.1 Drawing on our earlier work (Nolte & McKee, 2008b; Nolte & Pitchforth, 2014), it summarizes the evidence on approaches to managing care for people with chronic conditions. It begins by briefly reflecting on concepts used in the context of chronic care, reviewing the commonalities and differences between terms such as disease management and integrated care. It then provides an overview of published evidence on the effectiveness of selected approaches to improving the care of people with chronic conditions. It concludes with a section outlining the major gaps in our understanding of effective approaches to chronic care.
2.1 Managing care for people with chronic conditions: concepts and definitions
One challenge to identifying effective approaches to managing care for people with chronic conditions remains the absence of common definitions of underlying concepts. There is a plethora of terminologies that have variously been described as integrated care, coordinated care, collaborative care, managed care, disease management, case management, patient-centred care, chronic (illness) care, continuity of care, and others (Nolte & McKee, 2008b). While these may differ conceptually, the boundaries between them are often unclear and terms are frequently used interchangeably (Kodner & Spreeuwenberg, 2002), 1 This chapter is based on a summary overview of ‘Best practice in chronic care’, which informed the 2013 International Symposium on Health Care Policy convened by the Commonwealth Fund, New York (unpublished).

10 Assessing chronic disease management in European health systems
reflecting the range of disciplines and professional perspectives involved, along with a diverse set of objectives around “chronic care” (Nolte & McKee, 2008b). This issue is not only of academic relevance but has important implications for practice. Empirical evidence of approaches that can be subsumed under the above terms is often difficult to compare because of a lack in clarity in defining and describing the approach being studied. It thus remains problematic to arrive at conclusions about the relative value of one approach versus another.
Take two common concepts that are frequently used in the context of managing chronic conditions, disease management and integrated care. We have previously argued that these two concepts may reflect two ends of a spectrum of approaches that, ultimately, aim to ensure cost-effective quality care for service users with varied needs (Nolte & McKee, 2008b). Disease management, by definition, traditionally targets patient groups with specific conditions, such as diabetes, while integrated care is typically aimed more broadly at people with complex needs that arise from multiple chronic conditions, coupled with increasing frailty at old age. However, with more recent definitions of disease management explicitly adopting a broader view towards a population-based approach that addresses multiple needs (Population Health Alliance, 2014; Geyman, 2007), boundaries are becoming increasingly blurred.
2.1.1 Disease management
Disease management was first described in the USA in the 1980s, with an initial focus on educational programmes to promote medication adherence and behaviour change among people with specific chronic conditions (Bodenheimer, 1999). From the mid-1990s, in parallel with an emerging body of evidence pointing to the potential for disease management to improve care quality and lead to cost savings, disease management strategies were adopted more widely across the private and public sector in the USA (Krumholz et al., 2006) and, more recently, in several European countries (Nolte & Hinrichs, 2012; Rijken et al., 2014) with related concepts also implemented in Australia (Glasgow et al., 2008). However, as noted in the introduction to this book, approaches vary widely in focus, scope of interventions and populations covered (Nolte & Hinrichs, 2012). In the USA, descriptions range from “discrete programs directed at reducing costs and improving outcomes for patients with particular conditions” (Rothman & Wagner, 2003:257) to “a system of coordinated health care interventions and communications for populations with conditions in which patient self-care efforts are significant” (Population Health Alliance, 2014). This second, comprehensive definition by the US-based Population Health Alliance suggests a shift from a single-disease focus towards a whole person model that addresses the needs of patients with comorbidities and multiple conditions.

11What we know: a brief review of the evidence of approaches to chronic care
Yet, although authors have increasingly adopted this broader definition, as discussed further on in this chapter, variation in what is referred to as disease management has remained (Coleman et al., 2009; Lemmens, Nieboer & Huijsman, 2009; Pimouguet et al., 2011). Importantly, in many settings the focus continues to be on single diseases, albeit with some adjustment to also consider comorbidity (Fullerton, Nolte & Erler, 2011), and there remain concerns overall about the suitability of current approaches to disease management to address the complex needs of those with multiple disease processes (Aspin et al., 2010; Nolte et al., 2012a; Rijken et al., 2014).
2.1.2 Integrated care
In contrast to disease management, the concept of integrated care has traditionally been discussed in the health and social care fields, with reference to linking the cure and care sectors (Kodner & Spreeuwenberg, 2002; Leutz, 1999). The application of the concept of integrated care to health and social care is not, however, clear-cut and different conceptualizations have been put forward, emphasizing, for example, the health care perspective (Gröne & Garcia-Barbero, 2001), or interpreting integration in terms of financing and delivery functions in the context of managed care (Øvretveit, 1998; Shortell, Gillies & Anderson, 1994). The common denominator of integrated care concepts and approaches is their primary aim of improving outcomes for, traditionally, frail older people and other population groups with diverse and complex needs. The focus is on service users with multifaceted problems who require assistance with activities of daily living (Nolte & McKee, 2008b).
From this perspective, the notion of integrated care can be seen to be distinct from disease management. But, with recent conceptualizations of disease management that encompass collaborative care models and broader population groups as advocated by the Population Health Alliance (2014), and an interpretation of integrated care that is often limited to linkages within the health sector, the lines between the two concepts are increasingly difficult to draw. A review of systematic reviews by Ouwens et al. (2005) illustrates this issue. It sought to assess the effectiveness, definitions and components of integrated care programmes for chronically ill patients; however, of the systematic reviews considered, the majority were reviews of disease management programmes.
This latter point highlights the continued challenges associated with differentiating approaches in the field of chronic care. Based on these observations, we argue that concepts of integrated care and narrower, health-sector-specific perspectives of disease management share a common goal of improving outcomes for those with (complex) chronic health problems by overcoming issues of fragmentation through linkage of services of different

12 Assessing chronic disease management in European health systems
providers along the continuum of care (Nolte & McKee, 2008b). However, while concepts of integrated care frequently (aim to) link with the social care sector, disease management programmes are typically limited to linkages within the health care sector. Furthermore, as noted previously, disease management tends to remain restricted to single diseases.
2.2 What we do know: a review of the evidence base on approaches to caring for people with chronic conditions
This section presents a summary overview of key observations from recent rapid evidence reviews of disease management and of integrated care published elsewhere (Nolte, 2015; Nolte & Pitchforth, 2014). Both reviews focused on published systematic reviews and meta-analyses in the relevant field, building on the aforementioned work by Ouwens et al. (2005). The precise scope of our earlier work differed, but in both cases, we limited our search to studies published from 2004 onwards since the review by Ouwens and colleagues (2005) had covered systematic reviews and meta-analyses that had been published during 1996 through to May 2004. Detailed overviews of these reviews are available at Nolte (2015) and Nolte & Pitchforth (2014). Where appropriate, we complement this summary with more recent evidence not captured in our earlier reviews.
2.2.1 Disease management
Our review of the effectiveness of programmes broadly defined as disease management identified 15 eligible systematic reviews or meta-analyses published between January 2004 and October 2012 (Nolte, 2015). A summary of key findings is presented in Table 1.1.
The conditions most frequently considered in the reviews were depression (Neumeyer-Gromen et al., 2004; Thota et al., 2012), heart failure (Drewes et al., 2012; Göhler et al., 2006; Gonseth et al., 2004; Roccaforte et al., 2005), diabetes (Egginton et al., 2012; Knight et al., 2005; Pimouguet et al., 2011), COPD or asthma (Adams et al., 2007; Peytremann-Bridevaux et al., 2008; Lemmens, Nieboer & Huijsman, 2009), or a combination of these (de Bruin et al., 2011; Ofman et al., 2004; Tsai et al., 2005). Definitions of disease management varied among studies, although all adopted a fairly comprehensive conceptualization, drawing, for example, on the definition by Ellrodt et al. (1997:1687), which defines disease management as “an approach to patient care that coordinates medical resources for patients across the entire delivery system”. Others built on the CCM proposed by Wagner (1998), which

13What we know: a brief review of the evidence of approaches to chronic care
Table
2.1
Rev
iew
of r
evie
ws:
evi
denc
e of
the
effe
ct o
f dis
ease
man
agem
ent p
rogr
amm
es
Dis
ease
Func
tio
nal s
tatu
s,
clin
ical
out
com
esH
ealt
h ca
re
use
Qua
lity
of
life
Pat
ient
sa
tisf
acti
on
Mo
rtal
ity
Pro
cess
Co
st
Chr
onic
hea
rt fa
ilure
Gon
seth
et a
l. (2
004)
(
)
Roc
cafo
rte
et a
l. (2
005)
?
+
Göh
ler
et a
l. (2
006)
Dre
wes
et a
l. (2
012)
+
Dia
bet
es
Kni
ght e
t al.
(200
5)+
/ (+
)(
)(+
)(+
)(+
)
Pim
ougu
et e
t al.
(201
1)+
=
Egg
into
n et
al.
(201
2)+
(+)
(+)
?C
OP
D
Ada
ms
et a
l. (2
007)
+ /
(+)
?
=(
)
Pey
trem
ann-
Brid
evau
x et
al.
(200
8)+
/ (+
)
?(?
)=
(+)
Lem
men
s, N
iebo
er &
Hui
jsm
an
(200
9)=
/
()
+(+
)(+
)
Dep
ress
ion
Neu
mey
er-G
rom
en e
t al.
(200
4)+
++
+?
Thot
a et
al.
(201
2)+
++
+C
omb
ined
Ofm
an e
t al.
(200
4)+
/ (+
)(
)(+
)+
()+
/ (+
)(
)
Tsai
et a
l. (2
005)
++
/ (+
)+
/ (+
)
de B
ruin
et a
l. (2
011)
()
Not
es:
= si
gnifi
cant
redu
ctio
n in
mor
e th
an h
alf o
f stu
dies
revi
ewed
; (
) = so
me
evid
ence
of r
educ
tion;
/
() =
sign
ifica
nt re
duct
ion
in so
me
outc
omes
; + =
sign
ifica
nt im
prov
emen
t in
mor
e th
an h
alf o
f stu
dies
revi
ewed
; (+)
= so
me
evid
ence
of i
mpr
ovem
ent;
+ / (
+) =
sign
ifica
nt im
prov
emen
t in
som
e ou
tcom
es; =
no
signi
fican
t cha
nge
in o
utco
me
conc
erne
d; ?
evid
ence
inco
nclu
sive.
CO
PD: c
hron
ic o
bstr
uctiv
e pu
lmon
ary
dise
ase.

14 Assessing chronic disease management in European health systems
considers six elements as essential for improving chronic illness care (see Box 1.1). Several reviews analysed primary studies that included a minimum of two discrete interventions considered beneficial for chronic illness care, such as patient self-management, provider feedback, structured follow-up or role redesign (Lemmens, Nieboer & Huijsman, 2009; Peytremann-Bridevaux et al., 2008; Pimouguet et al., 2011), or a variation of this conceptualization (Egginton et al., 2012; Göhler et al., 2006; Neumeyer-Gromen et al., 2004; Roccaforte et al., 2005). Typically, around half of primary studies covered by the reviews were set in the USA, followed by Australia, the United Kingdom, Canada, Sweden and the Netherlands. Two reviews focused on studies set in the USA only (Egginton et al., 2012; Neumeyer-Gromen et al., 2004).
Studies reported on a diverse set of outcomes, reflecting the condition being targeted. In brief, available reviews provided fairly consistent evidence of a positive impact of disease management interventions targeting those with depression. These demonstrated, for example, significant improvements in depression severity (Neumeyer-Gromen et al., 2004), as well as depression symptoms, patient adherence to treatment, response to treatment and satisfaction with care, among other outcomes (Thota et al., 2012). One meta-analysis of 102 experimental or quasi-experimental studies targeting 11 conditions found that disease management interventions for those with depression had the highest proportion of studies demonstrating substantial improvements in patient care (48% statistically significant) (Ofman et al., 2004).
A similar consistency was found for disease management interventions targeting heart failure. These showed, for example, statistically significant reductions in the frequency of disease-specific and all-cause readmissions of between 10 and 30% (Gonseth et al., 2004; Roccaforte et al., 2005), with some evidence of a reduction in all-cause mortality (Roccaforte et al., 2005; Göhler et al., 2006; Savard, Thompson & Clark, 2011; Drewes et al., 2012). There was also some evidence that programmes that had incorporated a multidisciplinary team approach had a stronger impact on outcome measures (Roccaforte et al., 2005; Göhler et al., 2006). However, Savard, Thompson and Clark (2011), in a meta-review of meta-analyses of heart failure disease management programmes found the quality of reviews to be moderate and very mixed across reviews, with studies not adequately taking account of programme complexity and heterogeneity.
Evidence for the impact of disease management on diabetes also tended to show beneficial effects overall, with significantly improved glycaemic control among diabetes disease management populations compared to usual care, although the overall clinical significance of observed improvements remains uncertain (Knight et al., 2005; Pimouguet et al., 2011; Egginton et al.; 2012). However,

15What we know: a brief review of the evidence of approaches to chronic care
there was evidence that disease management may be more effective for patients with poor glycaemic control (Pimouguet et al., 2011). The review by Knight et al. (2005) further showed that observed effects were larger for studies conducted in the USA, although the number of trials outside the USA considered in the review was small (Knight et al., 2005). Overall there was considerable variation across studies included in individual reviews in terms of intervention delivery methods, duration and populations, and such a variation was also observed in studies that examined the evidence base for disease management targeted at people with COPD or asthma. Among these, there was evidence of reduced health service use, such as hospitalizations, among those receiving disease management (Adams et al., 2007; Peytremann-Bridevaux et al., 2008), while impacts on clinical outcomes were mixed across reviews, with some evidence of a reduction in all-cause mortality among targeted patients (Peytremann-Bridevaux et al., 2008). This last review considered trial evidence from a range of countries, including Canada, the Netherlands, New Zealand, Spain, Sweden and the USA.
2.2.2 Integrated care
Our review of integrated care focused on the economic impacts of relevant approaches (Nolte & Pitchforth, 2014). We identified 19 systematic reviews and meta-analyses published between 2004 and 2012, although it is important to note that of the reviews included, none explicitly defined the term integrated care. Instead, the most commonly used strategies were described as case management (Chiu & Newcomer, 2007; Smith & Newton, 2007; Oeseburg et al., 2009; Pimouguet et al., 2010), collaborative care (Gilbody, Bower & Whitty, 2006; Brink-Huis, van Achterberg & Schoonhoven, 2008; van Steenbergen-Weijenburg et al., 2010), or a combination of these (Phillips et al., 2004; Langhorne et al., 2005; Shepperd et al., 2008; Steffen et al., 2009; Althaus et al., 2011; Smith et al., 2012; Tappenden et al., 2012), alongside notions such as seamless care (Simoens et al., 2011). Four reviews focused on disease management interventions that involved multicomponent approaches (Neumeyer-Gromen et al., 2004; Maciejewski, Chen & Au, 2009; Steuten et al., 2009; de Bruin et al., 2011). Of these, two were also considered in our review of disease management reported previously in this chapter; therefore, we do not report on these two reviews in this section (Neumeyer-Gromen et al., 2004; de Bruin et al., 2011).
Reviews considered a wide range of interventions or initiatives that targeted a diverse group of people or populations. Several studies focused on adults with specific chronic conditions including pain (Brink-Huis, van Achterberg & Schoonhoven, 2008), depression (Gilbody, Bower & Whitty, 2006; van

16 Assessing chronic disease management in European health systems
Steenbergen-Weijenburg et al., 2010), stroke (Langhorne et al., 2005), asthma (Maciejewski, Chen & Au, 2009), COPD (Steuten et al., 2009), or those with multimorbidity (Smith et al., 2012). Four reviews considered integrated care approaches for older people in the community considered to be frail (Oeseburg et al., 2009) or have long-term medical or social care needs (Tappenden et al., 2012), those with specific chronic conditions, such as heart failure (Phillips et al., 2004), or those who were to be discharged from hospital (Chiu & Newcomer, 2007). Three reviews focused on adults with dementia or memory loss (Pimouguet et al., 2010), those with severe mental health problems (Smith & Newton, 2007), or those who received mental health care services (Steffen et al., 2009), while the remainder addressed populations defined by patterns of health service use (Shepperd et al., 2008; Althaus et al., 2011; Simoens et al., 2011).
Initiatives frequently targeted the interface between hospitals and primary care or community services, most often in the context of discharge planning or care transition (Phillips et al., 2004; Langhorne et al., 2005; Chiu & Newcomer, 2007; Steffen et al., 2009; Althaus et al., 2011; Simoens et al., 2011). Several studies examined initiatives that sought to coordinate primary care and community services, often, although not always, involving medical specialists (Gilbody, Bower & Whitty, 2006; Brink-Huis, van Achterberg & Schoonhoven, 2008; van Steenbergen-Weijenburg et al., 2010; Smith et al., 2012) or extending further into social care services (Smith & Newton, 2007; Pimouguet et al., 2010; van Steenbergen-Weijenburg et al., 2010; Tappenden et al., 2012). The latter type of interventions tended to target older people with multiple care needs, those with dementia or with mental health problems. The definition of what constitutes community services or social care differed across the individual studies reviewed, making any generalization of the extent of integration across sectors difficult. This last point also reflects the differences in settings, with typically about half of primary studies considered by reviews set in the USA, followed by the United Kingdom, Australia, Canada, New Zealand, the Netherlands, Spain, Italy and Sweden.
Similar to studies of the effectiveness of disease management, reviews of the impacts of integrated care reported on a diverse set of outcomes that we attempt to summarize here. We should reiterate that our original review focused on the economic impacts of approaches considered as integrated care (Nolte & Pitchforth, 2014). Therefore, our review captured only a subset of relevant studies that included cost measures and that did not necessarily cover the broader range of outcomes. These limitations reflect our selection process rather than an absence of evidence; where appropriate we complement our discussion with evidence from systematic reviews not included in our initial review.
17What we know: a brief review of the evidence of approaches to chronic care
Categorizing reviews by type of integrated care strategy or approach, we found mixed evidence for the impact of case management. One review of case management in mental health, which focused on studies assessing assertive community treatment or intensive case management, reported some limited evidence of increased patient satisfaction (Smith & Newton, 2007). Two reviews, focusing on case management for dementia (Pimouguet et al., 2010)
or chronic illness among older or frail people (Oeseburg et al., 2009), reported reduced service use. A more recent review of case management for heart failure patients being discharged from hospitals provided evidence for significant reductions in readmission rates, as well as all-cause mortality at the 12-month follow-up (Takeda et al., 2012). Reviews that assessed interventions targeting interactions between hospitals and primary care or community services through care coordination activities pointed to improved satisfaction among those receiving the intervention (Langhorne et al., 2005; Simoens et al., 2011), as well as improved quality of life (Phillips et al., 2004; Steffen et al., 2009), but not reduced mortality (Langhorne et al., 2005; Chiu & Newcomer, 2007; Simoens et al., 2011).
There was consistency in findings across two reviews examining collaborative care approaches for those with depression, but as with the evidence on disease management approaches reported previously, studies were almost exclusively set in the USA (Gilbody, Bower & Whitty, 2006; van Steenbergen-Weijenburg et al., 2010). A more recent Cochrane review of collaborative care for depression and anxiety problems, which also included studies from countries outside the USA, found improvements in outcomes across several studies, but statistically significant improvements were not always maintained over time (Archer et al., 2012). Brink-Huis, van Achterberg & Schoonhoven (2008) reviewed collaborative organizational models in relation to pain management among adult cancer patients, finding that pain intensity and relief improved using integrated care processes.
Evidence from reviews that considered strategies involving a combination of case management, care coordination or collaborative care for a range of patient groups was difficult to summarize. In general, they tended to show improvements in clinical or functional outcomes and, in some cases, a trend towards reduced mortality rates (Shepperd et al., 2008; Tappenden et al., 2012). One review of interventions targeting patients with coexisting, multiple chronic conditions in primary and community care settings found limited evidence for these to impact outcomes, although a number of process indicators, such as provider behaviour did improve (Smith et al., 2012).

18 Assessing chronic disease management in European health systems
2.2.3 Economic impacts of disease management or integrated care
We report the economic impacts of disease management and integrated care, respectively drawing from our reviews. In the review of disease management, few studies explicitly considered costs, and where they did, the evidence tended to be inconsistent (Ofman et al., 2004). De Bruin et al. (2011) examined the impact of disease management programmes on health care expenditures for patients with diabetes, depression, heart failure or COPD. Of 31 studies considered in their review, 21 reported incremental health care costs per patient per year, and of these, 13 found evidence of cost savings, but these were typically not statistically significant or not tested for statistical significance. The authors noted substantial variation across studies with regard to the interventions (content and type), the economic evaluative approach used, the type of direct health care costs and cost categories considered, alongside a lack of reporting on reliability of estimates, highlighting the need for higher-quality studies. Consequently, the authors concluded that “although it is widely believed that disease management programs reduce health care expenditures, the present study shows that evidence for this claim is still inconclusive” (de Bruin et al., 2011:105), thereby calling for well-designed economic evaluations.
In our review of integrated care approaches, the most common economic outcome measures were use and cost, but reporting of measures was inconsistent and the quality of the evidence was often low (Nolte & Pitchforth, 2014). The majority of economic outcomes focused on hospital use through (re)admission rates, length of stay or admission days and emergency department visits. For example, among reviews that considered care coordinating activities at the hospital–primary care or community services interface reported evidence of reduced hospital use (Phillips et al., 2004; Langhorne et al., 2005; Chiu & Newcomer, 2007; Steffen et al., 2009; Simoens et al., 2011).
Most studies reported cost in terms of health care cost savings, most frequently in relation to hospital costs. There was some evidence of cost reduction in a number of reviews although findings were frequently based on a small number of original studies, or studies that only used a before/after design without control, or both (Phillips et al., 2004; Chiu & Newcomer, 2007; Brink-Huis, van Achterberg & Schoonhoven, 2008; Shepperd et al., 2008; Steffen et al., 2009; Althaus et al., 2011; Simoens et al., 2011). Philips et al. (2004) highlighted the impact of a health system setting on costs, demonstrating how pooled cost differences for comprehensive discharge planning for those with heart failure ranged from US$359 compared to usual care in non-US-based trials to US$536 in trials based in the USA. Tappenden et al. (2012) further noted, in a review of structured home-based, nurse-led health promotion, the importance of differentiating between initial and longer-term costs. Thus,

19What we know: a brief review of the evidence of approaches to chronic care
they reported how a community-based nursing programme for patients with Parkinson’s disease had initially increased costs, whereas over two years costs were lower.
Neumeyer-Gromen et al. (2004) and van Steenbergen-Weijenburg et al. (2010), both reporting on care approaches targeted at those with depression, reported an increase in costs associated with the intervention, but the cost per successfully treated patient was lower (Neumeyer-Gromen et al., 2004). A review by Jacob et al. (2012) of 30 studies of collaborative care for the management of depressive disorders also provided some evidence of potential cost savings associated with collaborative care compared with usual care. All three reviews drew on primary studies set in the USA.
Reviews also pointed to cost–effectiveness of selected integrated care approaches, although again the evidence base was weak, frequently relying on single trials of a given intervention. For example, one review of approaches targeting frequent hospital emergency department users found one trial that reported the intervention to be cost-effective (Althaus et al., 2011). Another review of structured home-based, nurse-led health promotion for older people at risk of hospital or care home admission concluded, based on three economic studies, that there was a high likelihood of cost savings associated with the intervention (Tappenden et al., 2012). However, one of the three studies suggested that there was little or no evidence for gains in quality-adjusted life years (QALYs) over usual care. Four reviews reported on cost per QALY as a measure of cost utility, providing mixed evidence of increased cost with integrated care approaches (Gilbody, Bower & Whitty, 2006; Steuten et al., 2009; van Steenbergen-Weijenburg et al., 2010; Simoens et al., 2011). Jacob et al. (2012) reported collaborative care for the management of depressive disorders to be cost-effective. Overall the evidence was difficult to interpret.
2.3 What we need to know: limitations of the existing evidence base
This overview of the evidence on approaches to enhance chronic care is arguably limited in that it considers published systematic reviews only. This means that, by necessity, we have had to rely on authors’ reporting of findings of original studies, which limits objective assessment, in particular, where observations from original studies were not described in detail. Furthermore, even the most recent reviews will not capture primary studies published over the past 12 months or so, and which might have provided additional insights into the overview presented here. At the same time, and echoing concerns reported by Ouwens et al. (2005) in their assessment of the evidence of integrated care programmes

20 Assessing chronic disease management in European health systems
as described earlier, it remains challenging to interpret the evidence from existing primary studies. Thus, as reviews reported here have shown, studies of what can broadly be subsumed under the heading of chronic care strategies or programmes tend to be very heterogeneous. Lack of precision in reporting of interventions, alongside variation in definitions and components of care, does make arriving at overarching conclusions at what is the best approach difficult. Indeed, as Ouwens et al. (2005) noted, such heterogeneity might lead to inappropriate conclusions about programme effectiveness and the application of findings. This further underlines the continued need for the use of consistent definitions and of better description of the content of interventions to enable comparison.
However, at the same time, and at the risk of simplifying what is inherently complex, we can derive some tentative observations from the evidence presented here. Specifically, what seems to be emerging is the value of targeted approaches to enhance outcomes of those with complex care needs. For example, evaluations that examined the impact of different care components point to an association between the format or modality of the intervention and reported outcomes. Thus, evidence from collaborative care models for the management of depressive disorders suggests that interventions were more effective when based in the community or when they involved nurses as case managers (Thota et al., 2012). Similarly, for persons with heart failure, the impact on outcomes was found to be stronger for those interventions that incorporated a multidisciplinary team approach (Roccaforte et al., 2005; Göhler et al., 2006). These observations concur with other review evidence that examined the effects of different coordinated care interventions (Powell Davies et al., 2008). That review showed that interventions using multiple strategies tended to be more successful in enhancing the health outcomes of patients than those using single strategies only. Specifically, approaches that helped structuring relationships between providers and between providers and patients through, for example, case management or multidisciplinary teams were found to be more likely to be effective.
Other evidence points to the need to develop approaches that more specifically target those who are most likely to benefit. For example, Pimouguet et al. (2011) showed how diabetes disease management may be more effective for patients with poor glycaemic control. Similar findings were recently reported for a large, population-based diabetes care intervention in the Netherlands (Elissen et al., 2012), although requiring further confirmation (Elissen et al., 2013a). Evidence supporting the use of targeted approaches was also provided in the review by Smith et al. (2012) of models of care for those with multimorbidity cited earlier. While highlighting the paucity of research into related strategies, the

21What we know: a brief review of the evidence of approaches to chronic care
review noted that organizational interventions that focus on the management of specific risk factors or that targeted specific areas of concern for patients, such as functional ability or the management of medicines, may be more effective than approaches not similarly targeted.
The review by Smith et al. (2012) further highlighted the need to integrate new interventions with the existing health care delivery structure to enhance their effectiveness. Related observations noted how the evidence of impact tended to be stronger for primary studies undertaken in the USA than for those done elsewhere, as was the case for studies of disease management for diabetes (Knight et al., 2005). Given that much of the available evidence tends to originate from the USA, the findings highlight a need for caution when considering transferring models across countries with different health systems, and for developing a more robust evidence base that takes account of the European context (Nolte & McKee, 2008a). Overall, these findings also point to the need for more systematic evaluation of new models of care as a means to inform the development of efficient and effective interventions to address the growing burden of chronic conditions in Europe and elsewhere.
2.4 Conclusions
In this chapter, we have reviewed the recent evidence on the effectiveness of various approaches to improving care for people with chronic conditions. We have highlighted the difficulties in differentiating and defining terms associated with different models of care. This is not only of academic concern but makes collating evidence to support assessments of best practice in the management of chronic illnesses very difficult.
Furthermore, evidence of the cost–effectiveness of different models is lacking, particularly in the European context. Findings from the USA that suggest certain chronic care approaches may yield cost savings may not be transferable to other health systems. In this context, it is important to note that it is clear from the literature that it is easier to improve processes of care than costs. The assumption that providing better care will save money will need to be scrutinized carefully. Policy-makers and payers need to be clear about whether their goal is quality improvement or cost reduction as these two are not necessarily compatible with one another (Øvretveit, 2009).
We have shown that, overall, strategies that involve multiple organizational strategies that are set in the community, involve nurses as case managers and incorporate a multidisciplinary team approach are more likely to be effective. The evidence that is available tends to be limited to a small set of conditions only, although arguably, by restricting the review reported here to published

22 Assessing chronic disease management in European health systems
systematic reviews, we will have missed more recent evidence from primary studies that have investigated the impact of disease management on a broader range of conditions.
One fundamental issue remains, which is related to the need to develop a system-wide model of care for patients with chronic disease. Disease-specific approaches, such as disease management programmes, are ill-suited to meet the needs of the typical patient in primary care who typically has multiple health problems with complex needs (Nolte & McKee, 2008a). Integrated care, which is most commonly associated with aiming to meet the needs of populations groups with diverse and complex needs, has been associated with improved patient and clinical outcomes. The challenge in this case is that it is not clear for how long initial improvements are sustained. Furthermore, evidence of interventions designed to improve outcomes in patients with coexisting multiple chronic conditions in primary and community care settings suggests that this may be an area with the most inconsistent evidence. Despite the need for more robust evaluations and general strengthening of the evidence base, we have drawn common lessons around modalities of interventions that are likely to be more effective.
Chapter 3
Approaches to chronic disease management in
EuropeEllen Nolte, Cécile Knai
This chapter provides an overview of the policy context for chronic disease management in 12 European countries and examines approaches to chronic disease management and models of care delivery that have been or are being implemented in these countries. It draws on detailed country reports, which are presented in an accompanying volume (Nolte & Knai, 2015. We begin with a concise overview of selected key features of the health care systems in each of the countries reviewed. We then describe the main types of chronic care approaches countries are employing, the nature and scope of professionals and health care providers involved, the extent to which patients are actively engaged or supported, the use of support structures, such as decision-making tools and guidance, approaches to financing and the use of financial incentives, and population(s) covered.
As noted earlier, it is beyond the scope of this book to provide a comprehensive inventory of all approaches being implemented in a given country; instead we have focused on a sample of approaches considered representative of a given health care system.
3.1 Key features of the health care systems in 12 European countries
Before discussing the specific policy context for chronic disease in the countries reviewed, it is important to understand some of the key characteristics of the health care systems and the principles of health service delivery in each of the countries to help placing into context the efforts to implement chronic care policies as described further on in this chapter.

24 Assessing chronic disease management in European health systems
All countries have a similar commitment to providing universal and reasonably equitable access to health care for their populations, but do so in different ways. Four countries (Denmark, England, Italy and Latvia) operate primarily tax-funded systems, while the health care systems in Austria, Estonia, France, Germany, Hungary, Lithuania and the Netherlands are primarily funded through statutory health insurance. Switzerland operates a mandatory private insurance system (Table 3.1).
Countries reviewed vary in relation to principal health care governance structures, with systems in England, France, Hungary, Latvia and Lithuania characterized by structures that tend to concentrate governance functions at the central (national) level, with decentralization of some functions to bodies at arm’s length from government. Elsewhere, administrative and political responsibility is partly or fully devolved to local or regional authorities (Denmark, Estonia, Italy) or federal states (Austria, Germany, Switzerland). In Austria, Germany and the Netherlands, corporate actors (for example, statutory health insurance (SHI), providers) also play an important role.
Table 3.1Principlesofhealthcarefinancingin12Europeancountries
Country Health expenditure (2012)
Main sources of funding for health care (% of total current health expenditure in 2012)
% of GDP US$ PPP
Austria 11.5 5065 Combination of SHI (40.5) and general taxation (35.0), VHI (4.0), OOP (15.2)
Denmark 11.2 4720 General taxation (85.5), VHI (1.8), OOP (12.6)
England (UK) 9.4 3495 General taxation (82.5), VHI (1.1), OOP (9.9)
Estonia 5.9 1385 National health insurance (69.1), general taxation (10.8), OOP (18.4)
France 11.7 4260 SHI (71.0), VHI (13.8), OOP (7.4), general taxation (5.9)
Germany 11.3 4617 SHI (67.6), general taxation (8.7), VHI (9.5), OOP (12.1)
Hungary 7.8 1729 SHI (52.3), general taxation (11.4), VHI (2.7), OOP (27.1)
Italy 9.2 3040 National and regional taxation (78.2), OOP (20.2)
Latvia 6.0 1188 General taxation (56.7), VHI (2.5), OOP (37.4)
Lithuania 6.7 1426 SHI (60.1), taxation (10.7), OOP (28.5)
Netherlands 12.4 5384 SHI (72.6), taxation (7.3), VHI (5.2), OOP (5.6)
Switzerland 11.3 6062 Mandatory health insurance (43.7), taxation (18.0), VHI (9.4), OOP (28.1)
Source: World Health Organization (2014).Notes: GDP: gross domestic product; PPP: purchasing power parity/capita (national currency unit per US$); SHI: statutory health insurance; VHI: voluntary health insurance; OOP: (household) out-of-pocket (expenditure).
Countries also vary in the organization of health care, with differences in the settings within which the different levels of care are being provided (Table 3.2). Focusing on primary care, most countries reviewed here offer a choice of primary care physician, usually a general practitioner (GP) or family physician

25Access to health care services within and between countries of the European Union
operating in independent practice. The only exceptions are Denmark and England where choice of primary care provider is presently restricted to within (small) geographical areas. All but four countries require registration with a primary care provider who typically acts as gatekeeper to specialist services. Exceptions are Austria, France, Germany and Switzerland, which principally offer almost unrestricted access to primary and specialist care providers in the ambulatory care system, with France and Germany recently introducing voluntary GP gatekeeping schemes to enhance care coordination; selected managed care schemes in Switzerland also restrict direct access to specialists.
Where gatekeeping is in place, some direct access to specialists may still be possible, with certain specialties exempted from requiring a GP referral, such as in Denmark, Estonia, Hungary, Italy and Latvia. Also, where registration with a GP (practice) is in place, payment of the primary care provider tends to be based on capitation, frequently in combination with fees for specific services or activities and, less frequently, performance-related elements (for example, England, Estonia, France, Hungary). Systems that do not require patient enrolment typically reimburse their primary care providers on a fee-for-service basis (France, Switzerland), while elements of capitation may also be used (Austria, Germany).
We have previously noted that health care systems in which patients have traditionally chosen their provider without formal enrolment, and where payment for services is mainly based on fee-for-service , may face the greatest challenges in adapting towards providing effective chronic care (Busse & Mays, 2008). These observations provide important context for better understanding the general approaches taken by individual countries to enhance care for people with chronic conditions, and the extent to which existing structures facilitate, or indeed hinder, the implementation of related policies and approaches.
3.2 The policy context for chronic care in Europe
Fragmentation of care, particularly between ambulatory or primary care and hospital or secondary care, and between the health and social care sectors remains a key concern in most health care systems (Nolte, Knai & McKee, 2008; Nolte & McKee, 2008c). In recent years, therefore, many European countries have sought to create a regulatory and policy framework to respond to chronic disease, generally aiming to promote approaches that better integrate care and improve coordination between sectors and levels of care. Detailed descriptions of the policy context in the countries reviewed for this book are provided in its accompanying volume (Nolte & Knai, 2015). In brief, in Germany, for example, the 2000 Health Care Reform Act introduced provisions for the

26 Assessing chronic disease management in European health systems
Table
3.2
Sel
ecte
d fe
atur
es o
f hea
lth c
are
syst
ems
in 1
2 E
urop
ean
coun
trie
s
Co
untr
yG
ove
rnan
ce o
f th
e p
ublic
hea
lth
syst
emP
rinc
iple
s o
f he
alth
car
e p
rovi
sio
n o
utsi
de
hosp
ital
Pay
men
t o
f p
rovi
der
sP
rovi
sio
n o
f p
rim
ary/
gen
eral
ist
and
sp
ecia
list
care
out
sid
e ho
spit
al
Cho
ice
of
pro
vid
er
in p
rim
ary/
am
bul
ato
ry c
are
GP
gat
ekee
pin
gP
aym
ent
of
phy
sici
ans
in p
rim
ary/
amb
ulat
ory
car
eP
aym
ent
of
hosp
ital
s (y
ear
intr
od
uced
)
Aus
tria
Sha
red
by c
entr
al
gove
rnm
ent,
nine
st
ate
gove
rnm
ents
an
d co
rpor
atis
t act
ors;
re
spon
sibi
lity
for
hosp
ital s
ecto
r m
ainl
y w
ith th
e fe
dera
l sta
tes
Office-basedprim
aryand
spec
ialis
t car
e ph
ysic
ians
; ou
tpat
ient
clin
ics
Yes
No
Ble
nded
sys
tem
of f
ee-f
or-s
ervi
ce
(FFS
) with
cap
itate
d el
emen
t for
bas
ic
serv
ices
; det
erm
ined
by
paym
ent
sche
mes
bas
ed o
n pu
blic
ser
vice
s or
priv
ate
law
and
sup
plem
ente
d by
bo
nusesdefinedbythestate
Per
form
ance
-or
ient
ed h
ospi
tal
financingsystem
(LK
F) (1
997)
Den
mar
kS
hare
d by
cen
tral
go
vern
men
t, re
gion
s an
d m
unic
ipal
ities
; re
gion
s an
d m
unic
ipal
ities
are
la
rgel
y re
spon
sibl
e fo
r or
gani
zing
hea
lth c
are
GP
s in
priv
ate
prac
tice
Yes,
with
in
specifiedlocalarea;
regi
stra
tion
with
GP
re
quire
d
Yes;
acc
ess
to s
peci
alis
t ca
re o
n re
ferr
al
only
exc
ept f
or
opht
halm
olog
ists
an
d de
ntis
ts
A c
ombi
natio
n of
cap
itatio
n pe
r pa
tient
and
FFS
, in
addi
tion
to
spec
ial f
ees
for
out-
of-h
ours
ser
vice
s,
tele
phon
e co
nsul
tatio
ns a
nd h
ome
visi
ts
Com
bina
tion
of
glob
al b
udge
t and
ac
tivity
-bas
ed
fund
ing
usin
g D
RG
s
Eng
land
Cen
tral
leve
l by
gov
ernm
ent
and
agen
cies
at
arm’slengthfrom
go
vern
men
t; lo
cal
orga
niza
tions
org
aniz
e he
alth
car
e de
liver
y
GP
s in
com
mun
ity-b
ased
pr
actic
es o
r he
alth
cen
tres
Withinspecified
smal
l are
a on
ly;
regi
stra
tion
with
GP
re
quire
d
Yes
Wei
ghte
d ca
pita
tion
base
d on
G
ener
al M
edic
al S
ervi
ces
cont
ract
, ne
gotia
ted
natio
nally
by
Dep
artm
ent
of H
ealth
with
NH
S E
mpl
oyer
s an
d G
P C
omm
ittee
of t
he B
ritis
h M
edic
al
Ass
ocia
tion;
plu
s el
emen
ts o
f FFS
an
d pe
rform
ance
-rel
ated
pay
men
t
Act
ivity
-bas
ed
paym
ent b
y re
sults
us
ing
heal
th
reso
urce
gro
ups
for
acut
e se
rvic
es
(200
3)
Est
onia
Con
cent
rate
d at
the
cent
ral l
evel
with
som
e in
volv
emen
t of l
ocal
au
thor
ities
esp
ecia
lly in
th
e ho
spita
l sec
tor
GP
s in
inde
pend
ent f
amily
pr
actic
e Ye
s; re
gist
ratio
n w
ith
GP
requ
ired
Yes;
dire
ct a
cces
s to
sel
ecte
d sp
ecia
lties
an
d fo
llow
-up
cons
ulta
tion
for
chro
nic
dise
ase
Com
bina
tion
of b
asic
allo
wan
ce,
capi
tatio
n fe
e, F
FS, w
ith a
dditi
onal
co
mpe
nsat
ion
for
thos
e pr
actic
ing
in
rem
ote
area
s; b
ased
on
nego
tiatio
ns
betw
een
SH
I and
Soc
iety
of F
amily
Physiciansforaperiodoffiveyears
DR
Gs
(200
4),
com
plem
ente
d by
pe
r di
em a
nd F
FS
paym
ents

27Access to health care services within and between countries of the European Union
Co
untr
yG
ove
rnan
ce o
f th
e p
ublic
hea
lth
syst
emP
rinc
iple
s o
f he
alth
car
e p
rovi
sio
n o
utsi
de
hosp
ital
Pay
men
t o
f p
rovi
der
sP
rovi
sio
n o
f p
rim
ary/
gen
eral
ist
and
sp
ecia
list
care
out
sid
e ho
spit
al
Cho
ice
of
pro
vid
er
in p
rim
ary/
am
bul
ato
ry c
are
GP
gat
ekee
pin
gP
aym
ent
of
phy
sici
ans
in p
rim
ary/
amb
ulat
ory
car
eP
aym
ent
of
hosp
ital
s (y
ear
intr
od
uced
)
Fran
ceTr
aditi
onal
ly
conc
entr
ated
at t
he
natio
nal l
evel
with
gr
adua
l dec
entr
aliz
atio
n of
(sel
ecte
d)
gove
rnan
ce fu
nctio
ns
to re
gion
al a
genc
ies
Office-basedprim
aryand
spec
ialis
t car
e ph
ysic
ians
Yes
Yes,
of a
sof
t typ
e (p
refe
rred
doc
tor
sche
me)
, with
strongfinancial
ince
ntiv
es fo
r pa
tient
s
FFS
; nat
iona
lly s
et c
over
age
of fe
es
base
d on
agr
eem
ents
bet
wee
n pr
ofes
sion
al o
rgan
izat
ions
and
SH
I ad
min
istr
atio
n; e
xtra
-billi
ng (c
once
rns
50%
of p
atie
nts)
; P4P
ele
men
t sin
ce
2009
bas
ed o
n in
divi
dual
con
trac
ts
betw
een
phys
icia
ns a
nd S
HI
DR
Gs
(pha
sed
in fr
om 2
004)
, su
pple
men
ted
by a
dditi
onal
pa
ymen
ts fo
r specificareas/
serv
ices
Ger
man
yS
hare
d by
cen
tral
go
vern
men
t, 16
sta
te
gove
rnm
ents
and
co
rpor
atis
t act
ors;
re
spon
sibi
lity
for
hosp
ital s
ecto
r m
ainl
y w
ith th
e fe
dera
l sta
tes
Office-basedprim
aryand
spec
ialis
t car
e ph
ysic
ians
Yes
Volu
ntar
y (G
P
cont
ract
s)
Com
bina
tion
of c
apita
tion
and
fee-
for
serv
ice
base
d on
cen
tral
ly n
egot
iate
d un
iform
val
ue s
cale
(EB
M) b
y th
e Fe
dera
l Ass
ocia
tion
of S
HI p
hysi
cian
s an
d th
e N
atio
nal A
ssoc
iatio
n of
SH
I Fu
nds
Ger
man
DR
Gs
(pha
sed
in fr
om
2003
)
Hun
gary
At c
entr
al le
vel b
y go
vern
men
t and
agenciesatarm
’s
leng
th fr
om g
over
nmen
t
Office-basedfamily
phys
icia
n; s
peci
alis
t ca
re in
pol
yclin
ics
and
disp
ensa
ries
Yes;
regi
stra
tion
with
fam
ily p
hysi
cian
re
quire
d
Yes,
in p
rinci
ple,
bu
t wid
e ra
nge
of
spec
ialis
t ser
vice
s ar
e ac
cess
ible
w
ithou
t ref
erra
l
Wei
ghte
d ca
pita
tion
plus
adj
ustm
ents
ba
sed
on p
rovi
der
char
acte
ristic
s
DR
Gs
(199
3);
outp
atie
nt
spec
ialis
t ser
vice
s on
a F
FS b
asis
Italy
Sha
red
by th
e ce
ntra
l go
vern
men
t and
the
20
regi
ons,
with
regi
ons
havi
ng e
xten
sive
au
tono
my
Office-basedGPs,typically
insolopractice;office-
base
d sp
ecia
lists
Yes;
regi
stra
tion
with
G
P re
quire
dYe
s; d
irect
ac
cess
to c
erta
in
spec
ialis
ts,
for
exam
ple
gyna
ecol
ogis
ts
Cap
itatio
n fe
e pl
us a
sha
re b
ased
on
par
ticip
atio
n in
pub
lic h
ealth
in
terv
entio
ns (v
acci
natio
n an
d sc
reen
ing)
, bas
ed o
n na
tiona
l co
ntra
ct a
nd re
gion
al a
gree
men
ts
DR
Gs
(199
5),
com
plem
ente
d by
cap
itatio
n or
gr
ants
for
sele
cted
se
rvic
es
Latv
iaC
once
ntra
ted
at
the
cent
ral l
evel
by
gove
rnm
ent a
nd
agenciesatarm
’s
leng
th fr
om g
over
nmen
t
Typi
cally
GP
in
inde
pend
ent p
ract
ice;
he
alth
cen
tres
Yes
Yes;
dire
ct
acce
ss to
cer
tain
sp
ecia
lists
Age
-wei
ghte
d ca
pita
tion
plus
fees
for
definedactivities,b
onuspayments
andfixedallowances
Cas
e-ba
sed
paym
ent,
per
diem
pl
us F
FS p
oint
s

28 Assessing chronic disease management in European health systems
Co
untr
yG
ove
rnan
ce o
f th
e p
ublic
hea
lth
syst
emP
rinc
iple
s o
f he
alth
car
e p
rovi
sio
n o
utsi
de
hosp
ital
Pay
men
t o
f p
rovi
der
sP
rovi
sio
n o
f p
rim
ary/
gen
eral
ist
and
sp
ecia
list
care
out
sid
e ho
spit
al
Cho
ice
of
pro
vid
er
in p
rim
ary/
am
bul
ato
ry c
are
GP
gat
ekee
pin
gP
aym
ent
of
phy
sici
ans
in p
rim
ary/
amb
ulat
ory
car
eP
aym
ent
of
hosp
ital
s (y
ear
intr
od
uced
)
Lith
uani
aC
once
ntra
ted
at th
e ce
ntra
l lev
elFa
mily
phy
sici
ans
in
inde
pend
ent p
ract
ice;
sp
ecia
list o
utpa
tient
car
e in
he
alth
cen
tres
Yes;
regi
stra
tion
with
GP
requ
ired
Yes
Age
-wei
ghte
d ca
pita
tion
plus
pa
ymen
t for
peo
ple
livin
g in
rur
al
area
s an
d in
cent
ive
paym
ents
for
cert
ain
liste
d se
rvic
es
Glo
bal b
udge
ts
plus
cas
e-ba
sed
paym
ent
The
Net
herla
nds
Sha
red
by fe
dera
l and
lo
cal a
utho
ritie
s an
d co
rpor
atis
t act
ors
GP
s in
gro
up p
ract
ices
Ye
s; re
gist
ratio
n w
ith G
P re
quire
dYe
s; a
cces
s to
sp
ecia
list c
are
on
refe
rral
onl
y
Com
bina
tion
of c
apita
tion
and
FFS
; m
axim
um re
mun
erat
ion
fees
for
GP
s ne
gotia
ted
betw
een
Nat
iona
l A
ssoc
iatio
n of
GP
s, H
ealth
Insu
rers
N
ethe
rland
s an
d M
inis
try
of H
ealth
, W
elfa
re a
nd S
port
Dia
gnos
is a
nd
trea
tmen
t co
mbi
natio
ns
DB
Cs
(200
5)
Sw
itzer
land
Sha
red
by th
e fe
dera
l an
d 26
can
tona
l go
vern
men
ts w
ith
the
cant
ons
havi
ng
exte
nsiv
e au
tono
my
Office-basedprim
aryand
spec
ialis
t car
e ph
ysic
ians
Yes
No,
exc
ept f
or
thos
e en
rolle
d in
m
anag
ed c
are
plan
s (1
2% o
f re
side
nts)
Inde
pend
ent h
ealth
car
e pr
ofes
sion
als
are
gene
rally
pai
d on
a F
FSs
basi
s;
som
e m
anag
ed c
are
plan
s op
erat
e ca
pita
tion
mod
els
Per
die
m p
lus
Sw
iss
DR
Gs
(from
200
9)
Sour
ces:
Ette
lt &
Nol
te (2
010)
, Ette
lt et
al.
(200
8); Th
omso
n, F
oubi
ster &
Mos
sialo
s (20
09);
the
auth
ors.
Not
es: G
P: g
ener
al p
ract
ition
er; F
FS: f
ee-fo
r-se
rvic
e; L
KF:
Lei
stung
sorie
ntie
rte
Kra
nken
ansta
ltenfi
nanz
ieru
ng (p
erfo
rman
ce-b
ased
fina
ncin
g); D
RG: d
iagn
osis-
rela
ted
grou
ps; N
HS:
nat
iona
l hea
lth se
rvic
e; S
HI:
statu
tory
hea
lth in
sura
nce;
P4P
: pay
-for-
perfo
rman
ce; E
BM: E
inhe
itlic
her B
ewer
tung
smaß
stab
(Uni
form
Ass
essm
ent S
cale
); D
BC: d
iagn
ose
beha
ndel
ing
com
bina
ties (
diag
nosis
and
trea
tmen
t com
bina
tions
).
Table
3.2
con
td

29Access to health care services within and between countries of the European Union
development of integrated care structures, linking the ambulatory care and hospital sectors (Busse & Riesberg, 2004). In Austria, the 2005 health reform led to the creation of a financial pool at the federal state level (reform pool) to promote coordination of and cooperation between ambulatory and hospital care (Hofmarcher & Rack, 2006). In England, the 2004 NHS Improvement Plan explicitly placed the care for those with chronic conditions at the centre of successive and ongoing reform efforts, emphasizing the need to strengthen the integration between providers and sectors (Nolte et al., 2015). This objective was also central to recent efforts in Hungary and Lithuania to strengthen chronic care (Gaal et al., 2015; Lai et al., 2015). Other reform efforts have aimed at supporting care coordination through the introduction and further development of nurse-led strategies in most countries reviewed here, although the degree to which relevant efforts have been implemented has varied, from nurses forming an integral part of primary care, such as in England and the Netherlands (Elissen et al., 2015; Nolte et al., 2015), or their deployment within defined areas of care delivery, such as in Austria, France and Germany (Chevreul et al., 2015; Erler, Fullerton & Nolte, 2015; Sönnichsen, Flamm & Nolte, 2015).
Several countries have introduced fundamental reforms which, although not necessarily implemented to specifically address chronic disease or indeed targeting the health care sector as such, have impacted on the ability of systems to develop an integrated policy response to the rising burden of chronic illness. Most notable are reforms of national administrative structures, as in Denmark and Italy (Frølich, Jacobsen & Knai, 2015; Ricciardi et al., 2015). For example, the 1992 Law 502 in Italy introduced the gradual decentralization of administrative and financial functions to regions and local authorities, which was further strengthened and expanded on by the 2001 constitutional reform and 2009 legislation stipulating fiscal autonomy of regional institutions. This has provided regions with the means to organize health care according to local need, but it has also meant that centrally planned policies tend to be fragmented and uncoordinated, resulting in considerable variation among (and within) regions. In Denmark, the 2007 administrative reform changed the way health care is funded and organized, with most responsibilities moved to regions while municipalities were made responsible for the cofinancing of health services. This sought to encourage municipalities to improve preventive services and so reduce use of hospital care, which is organized at the regional level.
Ideally, such reforms will pave the way for the development of a consistent and comprehensive policy response to chronic diseases, with elements of health promotion and primary prevention, early detection and treatment, to the management of co- and multimorbidities and complications to palliative

30 Assessing chronic disease management in European health systems
and end-of-life care. However, countries reviewed differ with regard to their vision for controlling and managing chronic disease, ranging from overarching strategies for chronic disease control, to specific policies addressing the various components along the care continuum, to a lack of explicit policy focus on chronic diseases altogether. Instead, the majority of countries considered here have implemented a range of policies targeting specific elements on the care continuum.
3.3 Overview of approaches to chronic disease management in 12 European countries
We reviewed some 50 approaches and groups of approaches to chronic disease management in 12 European countries. Given the highly selective nature of the types of approaches identified, we have refrained from attempting to quantify observed features, such as providing counts or proportions. Instead, we provide a narrative account of key observations, summarized in tabular format. Detailed information on each approach is included in the relevant country report presented in an accompanying volume to this book (Nolte & Knai, 2015).
Table 3.3 provides an overview of the type and aims of approaches that have been or are being implemented, the target populations addressed and the principal providers involved. Because the focus of this work has been specifically to identify and describe approaches that broadly seek to improve the care for those with chronic health problems, the stated aims of the various approaches typically have the improvement of the quality of care at their core. Frequently, approaches also consider some form of coordination or integration between providers or sectors as a further aim, alongside enhancing efficiency and, in some instances, reducing (hospital) use.
Importantly, the majority of approaches focus on care models for populations with defined conditions, most frequently targeting type 2 diabetes, followed by asthma/COPD, cardiovascular disease (mainly chronic heart failure, ischaemic heart disease, cardiovascular risk and stroke), cancer and mental health problems. However, several countries reviewed here are also implementing approaches with a broader focus, typically centring on older people. These tend to be available in selected regions only or are operated as pilot studies. Examples include the Integrated Care Pilot (ICP) programme and the Partnership for Older People Project (POPP) in England, the Coordinating Care for Older People programme (COPA) in Paris, France, selected integrated care contracts in Germany and the Care Coordination Pilot (CCP) in Hungary. Where care models have been implemented as a pilot, some have been adapted for implementation in other regions (for example, the COPA programme in

31Access to health care services within and between countries of the European Union
France) or are sustained beyond completion of the pilot phase (for example, selected POPP projects in England) (Table 3.3).
Three countries, Estonia, Latvia and Lithuania, have not (yet) established chronic disease management as a distinct concept (Lai & Knai, 2015; Lai, Knai & Taube, 2015; Lai et al., 2015). Instead, chronic care is seen to be embedded within the primary care system, which all three countries newly introduced in the 1990s, with the GP or family physician at the core. However, within this framework, these countries are implementing strategies specifically targeting (complex) chronic conditions.
Most approaches were introduced in the 2000s, with some in an ongoing process of implementation or pilot stage. Only a small number of service models described here date back to the 1990s or earlier; examples include an ambulatory after-care service for stroke in the State of Salzburg, Austria (1989), a stroke service in Delft, the Netherlands (1997), and the Delta physician network in Geneva, Switzerland (1992) (Table 3.3). This illustrates that chronic disease care has only relatively recently become the focus of health policy-makers, regulators, funders and other stakeholders, as noted in the introduction to this book. It also reflects the health care literature around approaches to, and models of care for chronic health problems, which has emerged from the mid-1990s onwards, largely evolving from accumulating evidence of the effectiveness of structured disease management in the USA (Nolte & McKee, 2008b). At the same time, it is important to recognize, as indicated here, that countries have experimented with new models of care well before the current chronic care debate, usually in the context of care for the frail older population at the interface between the cure and care sectors (shared care). Indeed, the Matador model of diabetes care described for the Maastricht region in the Netherlands has evolved from a shared care approach implemented in 1996 (Klein-Lankhorst & Spreeuwenberg, 2008).
As described in Table 3.3, the approaches implemented in the countries reviewed can be broadly categorized as care coordination, managed discharge, multidisciplinary team working, case management and nurse-led care. These distinctions do overlap, with case management and managed discharge frequently, although not always, led by (specialist) nurses, while care coordination and multidisciplinary team working tend to refer to a coordinated approach to providing care across different professions or disciplines, in some cases also involving different providers, for example, in the form of provider networks. Our simplified typology is largely driven by the principal coordinator or provider of patient care identified for each of the approaches described here. In most cases, this is the GP or family physician (DMPs in Austria and Germany; care groups in the Netherlands). Where multidisciplinary teams act

32 Assessing chronic disease management in European health systems
as principal coordinator, these are frequently led by a GP or other physicians, for example: selected integrated cure pilots in England; provider networks and local cancer networks in France; integrated cure contracts in Germany; treatment protocols and CCPs in Hungary; the “From On-Demand to Proactive Primary Care” programme in Tuscany, Italy; the DiaBaid diabetes care network and Delta physician network in Switzerland). Several countries also use nurse-led approaches, although it should be noted that these tend to be limited to a selected set of countries only, including England (nurse-led case management; selected integrated care pilots), Hungary (asthma and diabetes disease management), Italy IGEA diabetes care programme; Leonardo and Raffaello projects), and the Netherlands (Matador diabetes management programme; stroke service Delft).
Several countries have introduced enhanced roles for specialized nurses in a coordinating function or in case management, such as Denmark (integrated clinical pathways), the COPA coordination of professional care for the elderly programme and the ASALWW project in France, and Lithuania (case management pilot HIV/AIDS). The Sophia diabetes care programme in France uses trained nurses to lead on the main intervention to support patients; however, the patient’s GP remains the principal care coordinator. Similarly, the Kardiomobil home care for patients with chronic heart failure programme in Salzburg, Austria, involves a nurse-led intervention to support patient self-management of chronic heart failure. Although nurses act as the principal coordinators, they do so in collaboration with the patients’ GPs. Germany has introduced nurse-led projects based on the concept of a community nurse, with different formats being tested and implemented. The predominant model is that of a care assistant in family practice (for example, VerAH), with selected medical tasks delegated to the practice nurse but legally assigned and performed under the supervision of a GP.
A small number of approaches use care coordinators with a non-medical and non-nursing background. These approaches tend to focus on after-care, rehabilitation and general support schemes. Those involved include allied health professionals (for example, a team of therapists in the ambulatory after-care of stroke patients in Salzburg, Austria), social or hybrid (health and social care) workers (Partnership for Older People Project, England), volunteer organizations (Partnership for Older People Project, England) or skilled key workers (selected integrated care pilots, England). The care coordination/interface management programme in Styria, Austria, offered by the regional SHI fund, uses an employee of the fund as the principal coordinator for discharge management; similar approaches in other parts of Austria use nurses or social workers.

33Access to health care services within and between countries of the European Union
Table
3.3
Ove
rvie
w o
f app
roac
hes
to c
hron
ic d
isea
se m
anag
emen
t or
thei
r eq
uiva
lent
in 1
2 E
urop
ean
coun
trie
s
Nam
eA
im/g
ener
al d
escr
ipti
on
Typ
e o
f ap
pro
ach
Targ
et
po
pul
atio
nYe
ar
imp
lem
ente
dP
rinc
ipal
co
ord
inat
or
Pro
vid
ers
invo
lved
Aus
tria
‘Therapieaktiv’
dise
ase
man
agem
ent
prog
ram
me
To im
prov
e th
e qu
ality
of l
ife a
nd e
xten
d lif
e fo
r pe
ople
with
chr
onic
dis
ease
, to
plac
e th
e pa
tient
at t
he c
entr
e of
car
e an
d to
mak
e efficientuseofhealthcareresourcesandalso
redu
ce h
ospi
taliz
atio
ns
Car
e co
ordi
natio
nTy
pe 2
dia
bete
s pa
tient
s20
06D
MP
phy
sici
an
(GP
/fam
ily
phys
icia
n)
GP
s, s
peci
alis
ts,
diab
etes
adv
iser
s
Inte
grat
ed s
trok
e ca
re
Upp
er A
ustr
iaTo
impr
ove
care
for
patie
nts
with
str
oke
both
in
rela
tion
to a
cute
car
e an
d at
the
inte
rface
to
reha
bilit
atio
n
Man
aged
di
scha
rge
Str
oke
patie
nts
2005
GP
GP
s, s
peci
alis
ts in
/ou
tsid
e ho
spita
l, em
erge
ncy
serv
ices
, re
habi
litat
ion
Car
e co
ordi
natio
n/in
terfa
ce m
anag
emen
t S
tyria
To im
prov
e th
e co
ntin
uity
of c
are
follo
win
g di
scha
rge
from
hos
pita
l usi
ng a
car
e co
ordi
nato
r
Man
aged
di
scha
rge
Pat
ient
s in
ho
spita
l20
02–2
003
(p
ilot)
Car
e co
ordi
nato
r at
the
regi
onal
SH
I fu
nd
Car
e co
ordi
nato
r lia
ises
with
hos
pita
ls
and
GP
s
Am
bula
tory
afte
r-ca
re
of s
trok
e pa
tient
s,
Sal
zbur
g
To fa
cilit
ate
acce
ss to
spe
cial
ized
am
bula
tory
ca
re fo
r st
roke
pat
ient
s an
d th
ereb
y en
able
tim
ely
reha
bilit
atio
n an
d re
duce
hos
pita
l cos
ts
thro
ugh
early
dis
char
ge
Man
aged
pos
t-di
scha
rge
care
Str
oke
patie
nts
1989
Team
of t
hera
pist
s (n
euro
reha
bilit
atio
n te
am)
Occ
upat
iona
l, sp
eech
an
d ph
ysio
ther
apis
ts;
GP
s
Kar
diom
obil
– H
ome
care
for
patie
nts
with
ch
roni
c he
art f
ailu
re
To s
uppo
rt p
atie
nts
with
chr
onic
hea
rt fa
ilure
to
enh
ance
dis
ease
(sel
f)man
agem
ent,
redu
ce
hosp
ital (
re)a
dmis
sion
s an
d co
mpl
icat
ions
and
im
prov
e qu
ality
of l
ife
Nur
se-le
d ca
reC
hron
ic h
eart
fa
ilure
pat
ient
s20
04 (p
ilot)
Trai
ned
nurs
eG
Ps,
spe
cial
ists
, nu
rses
, hos
pita
ls,
hom
e ca
re s
ervi
ces
Den
mar
k
SIK
S p
roje
ct –
inte
grat
ed e
ffort
for
peop
le li
ving
with
ch
roni
c di
seas
e
To s
uppo
rt p
eopl
e w
ith c
hron
ic c
ondi
tions
(C
OP
D, t
ype
2 di
abet
es, c
hron
ic h
eart
failu
re,
IHD
, bal
ance
pro
blem
s) th
roug
h co
ordi
nate
d re
habi
litat
ion
Car
e co
ordi
natio
n Ty
pe 2
dia
bete
s,
asth
ma/
CO
PD
, chr
onic
he
art f
ailu
re,
IHD
, bal
ance
pr
oble
ms
amon
g ol
der p
eopl
e
2005
Mul
tidis
cipl
inar
y te
am a
t hea
lth c
are
cent
re/h
ospi
tal
(det
erm
ined
by
sev
erity
of
cond
ition
)
GP
s, s
peci
alis
ts
in h
ospi
tal,
(spe
cial
ist)
nurs
es,
phys
ioth
erap
ists
, di
etiti
ans
in h
ospi
tal
and
com
mun
ity
serv
ices

34 Assessing chronic disease management in European health systems
Nam
eA
im/g
ener
al d
escr
ipti
on
Typ
e o
f ap
pro
ach
Targ
et
po
pul
atio
nYe
ar
imp
lem
ente
dP
rinc
ipal
co
ord
inat
or
Pro
vid
ers
invo
lved
Den
mar
k co
ntd
Reg
iona
l dis
ease
m
anag
emen
t pr
ogra
mm
es
A c
ombi
ned,
inte
rdis
cipl
inar
y, in
ters
ecto
ral
andcoordinatedeffortforaspecificchronic
cond
ition
that
ens
ures
the
use
of e
vide
nce-
base
d re
com
men
datio
ns, a
pre
cise
de
scrip
tion
of ta
sks
and
coor
dina
tion
of a
nd
com
mun
icat
ion
betw
een
all p
artie
s in
volv
ed
Car
e co
ordi
natio
n Ty
pe 2
dia
bete
s,
CO
PD
, CV
D,
dem
entia
, m
uscu
losk
elet
al
diso
rder
s,
depr
essi
on,
schi
zoph
reni
a,
canc
er
2009
, ong
oing
D
MP
GP
GP
s, m
unic
ipal
hea
lth
care
cen
tre,
hos
pita
l sp
ecia
lists
Inte
grat
ed c
linic
al
path
way
sTo
ens
ure
fast
and
opt
imal
trea
tmen
t and
m
anag
emen
t of p
atie
nts
with
can
cer/
hear
t di
seas
e
Car
e co
ordi
natio
nH
eart
dis
ease
, ca
ncer
pat
ient
s20
08 (c
ance
r),
2010
(hea
rt
dise
ase)
Car
e (p
athw
ay)
coor
dina
tor
(spe
cial
ist n
urse
)
GP
s, s
peci
alis
ts,
nurs
es, h
ospi
tals
, m
ultid
isci
plin
ary
team
s
Eng
land
Cas
e m
anag
emen
t/co
mm
unity
mat
ron
To e
nabl
e in
tens
ive,
hom
e-ba
sed
case
m
anag
emen
t for
old
er p
eopl
e at
ris
k of
ho
spita
lizat
ion
and
othe
r hi
gh-in
tens
ity s
ervi
ce
user
s
Cas
e m
anag
emen
tO
lder
peo
ple
at r
isk
of
hosp
italiz
atio
n
2004
Spe
cial
ist n
urse
GP
s, s
peci
alis
ts,
nurs
es, h
ospi
tals
, co
mm
unity
car
e an
d so
cial
car
e se
rvic
es
Qua
lity
and
outc
omes
fra
mew
ork
(QO
F)To
mak
e th
e G
P p
rofe
ssio
n m
ore
attr
activ
e,
redu
ce th
e w
ide
varia
tion
in p
aym
ents
to
prac
tices
, fai
rly li
nk re
war
d to
wor
kloa
d, a
nd
help
redu
ce h
ealth
ineq
ualit
ies
GP
-led
syst
emG
ener
alis
t20
04G
PG
Ps,
nur
ses,
ph
arm
acis
ts,
spec
ialis
ts
Par
tner
ship
s fo
r ol
der
peop
le p
roje
ct (P
OP
P)
Toprovideperson‐centredandintegrated
serv
ices
for
olde
r pe
ople
, enc
oura
ge
inve
stm
ent i
n ca
re a
ppro
ache
s th
at p
rom
ote
heal
th, w
ell-b
eing
and
inde
pend
ence
, and
pr
even
t/de
lay
the
need
for
high
er in
tens
ity o
r in
stitu
tiona
l car
e
Inte
grat
ed
care
/pro
vide
r ne
twor
ks/c
ase
man
agem
ent/
man
aged
di
scha
rge
Old
er p
eopl
e (>
65
yea
rs)
2005
–201
0Va
ried:
m
ultid
isci
plin
ary
team
(hea
lth
and
soci
al c
are)
; so
cial
or
hybr
id
wor
ker;
vol
unte
er
orga
niza
tion
GP
s, h
ospi
tals
, nu
rses
, com
mun
ity
serv
ices
, soc
ial
care
, oth
er p
ublic
an
d vo
lunt
ary
and
com
mun
ity
orga
niza
tions
Table
3.3
con
td

35Access to health care services within and between countries of the European Union
Nam
eA
im/g
ener
al d
escr
ipti
on
Typ
e o
f ap
pro
ach
Targ
et
po
pul
atio
nYe
ar
imp
lem
ente
dP
rinc
ipal
co
ord
inat
or
Pro
vid
ers
invo
lved
Eng
land
con
td
Inte
grat
ed c
are
pilo
t pr
ogra
mm
eTo
impr
ove
the
qual
ity o
f car
e an
d ou
tcom
es
for
patie
nts,
enh
ance
par
tner
ship
s on
car
e provisionandmakemoreefficientuseof
scar
ce re
sour
ces
Inte
grat
ed
care
/pro
vide
r ne
twor
ks/c
ase
man
agem
ent/
man
aged
di
scha
rge
Gen
eral
ist a
nd
disease-specific
(for
exam
ple,
di
abet
es, C
OP
D,
dem
entia
)
2009
–201
1Va
ried:
GP
-le
d ca
re;
mul
tidis
cipl
inar
y te
am w
orki
ng;
nurs
e-le
d ca
se
man
agem
ent;
skille
d ke
y w
orke
r-le
d ca
re
coor
dina
tion
GP
s, h
ospi
tals
, nu
rses
, allie
d he
alth
pr
ofes
sion
als,
co
mm
unity
ser
vice
s,
soci
al c
are,
oth
er
publ
ic a
nd v
olun
tary
se
rvic
es
Est
onia
Qua
lity
man
agem
ent i
n pr
imar
y he
alth
car
eC
hron
ic d
isea
se m
anag
emen
t as
a co
ncep
t no
t est
ablis
hed
but i
ndire
ctly
em
bedd
ed in
the
over
all s
truc
ture
and
org
aniz
atio
n of
the
heal
th
care
sys
tem
GP
-led
care
Type
2 d
iabe
tes,
ca
rdio
vasc
ular
di
seas
e (c
hron
ic
hear
t fai
lure
, IH
D)
2003
(c
ompl
etio
n of
G
P s
yste
m)
GP
GP
s, s
peci
alis
ts,
nurs
es, a
llied
heal
th
prof
essi
onal
s (fo
r ex
ampl
e,
phys
ioth
erap
ists
), so
cial
car
e
Chr
onic
dis
ease
m
anag
emen
t at t
he
prim
ary/
seco
ndar
y ca
re
inte
rface
Chr
onic
dis
ease
man
agem
ent a
s a
conc
ept
not e
stab
lishe
d bu
t ind
irect
ly e
mbe
dded
in th
e ov
eral
l str
uctu
re a
nd o
rgan
izat
ion
of th
e he
alth
ca
re s
yste
m
Spe
cial
ist-
led
care
Mul
tiple
sc
lero
sis,
Parkinson’s
dise
ase,
sc
hizo
phre
nia,
C
OP
D
Vario
usS
peci
alis
t (ce
ntre
); co
mor
bidi
ties
man
aged
by
GP
in
coor
dina
tion
with
sp
ecia
list
GP
s, s
peci
alis
ts,
nurs
es, a
llied
heal
th
prof
essi
onal
s,
hosp
itals
, soc
ial c
are,
sp
ecia
list c
entr
es
(mul
tiple
scl
eros
is)
Fran
ceP
rovi
der
netw
orks
For
exam
ple,
dia
bete
s ne
twor
ks: R
EV
ES
DIA
BTo
impr
ove
the
qual
ity o
f car
e fo
r pe
ople
with
ty
pe 2
dia
bete
sM
ultid
isci
plin
ary
team
Ty
pe 2
dia
bete
s20
01P
athw
ay
coor
dina
tor:
GP
or
nurs
e
GP
s, s
peci
alis
ts,
nurs
es, a
llied
heal
th
prof
essi
onal
s (d
ietit
ians
, the
rapi
sts)
, ho
spita
ls, l
abor
ator
ies

36 Assessing chronic disease management in European health systems
Nam
eA
im/g
ener
al d
escr
ipti
on
Typ
e o
f ap
pro
ach
Targ
et
po
pul
atio
nYe
ar
imp
lem
ente
dP
rinc
ipal
co
ord
inat
or
Pro
vid
ers
invo
lved
Fran
ce c
ontd
Pro
vide
r ne
twor
ksFo
r ex
ampl
e,
Coo
rdin
atio
n of
pr
ofes
sion
al c
are
for
the
elde
rly (C
OPA
)
To b
ette
r in
tegr
ate
serv
ice
prov
isio
n be
twee
n he
alth
and
soc
ial c
are;
to re
duce
inap
prop
riate
he
alth
car
e us
e, in
clud
ing
emer
genc
y de
part
men
t and
hos
pita
l use
; to
prev
ent l
ong-
term
nur
sing
hom
e in
stitu
tiona
lizat
ion
Cas
e m
anag
emen
tFr
ail o
lder
peo
ple
(> 6
5 ye
ars)
2006
Spe
cial
ist n
urse
as
case
man
ager
GP
s, s
peci
alis
ts,
nurs
es, h
ospi
tals
, allie
d he
alth
pro
fess
iona
ls
(psy
chol
ogis
ts,
ther
apis
ts),
soci
al
serv
ices
Spe
cific
pro
gram
mes
Sop
hia
diab
etes
an
d as
thm
a ca
re
prog
ram
me
(by
SH
I)
Toim
proveself-managem
ent,efficiencyand
qual
ity o
f dia
betic
car
e; n
atio
nwid
eC
are
coor
dina
tion
Type
1 a
nd 2
di
abet
es, a
sthm
a20
08
(dia
bete
s),
2014
(ast
hma)
GP,
in c
olla
bora
tion
with
nur
seG
Ps,
nur
ses
Hea
lth A
ctio
n by
Tea
ms
of S
elf-
Em
ploy
ed
Hea
lth P
rofe
ssio
nals
(A
SA
LEE
)
To im
prov
e he
alth
car
e qu
ality
by
dele
gatin
g se
lect
ed ta
sks
to n
urse
s N
urse
-led
care
Dia
bete
s, C
VD
2004
–200
7Tr
aine
d nu
rse
GP
s, n
urse
s
Hos
pita
l dis
char
ge
prog
ram
me
for
hear
t fa
ilure
pat
ient
s (P
RA
DO
)
Ada
pt a
nd im
prov
e fo
llow
-up
care
afte
r ho
spita
l dis
char
geC
are
coor
dina
tion/
man
aged
di
scha
rge
Pat
ient
s ho
spita
lized
for
hear
t fai
lure
2013
Dis
char
ge m
anag
erG
Ps,
car
diol
ogis
ts,
nurs
es
Specificpayment
base
d on
pub
lic h
ealth
ob
ject
ives
(RO
SP
)
Rew
ard
achi
evem
ent o
f obj
ectiv
es in
the
fieldsofprevention,chronicdiseasecareand
pres
crip
tion
Phy
sici
an-le
d sy
stem
GP
s an
d sp
ecia
list
phys
icia
ns
2009
(pilo
t: C
AP
I) 20
12 (f
ull
roll-
out)
Phy
sici
anG
Ps
and
spec
ialis
t ph
ysic
ians
Mea
sure
s in
the
2003
–200
7 C
ance
r P
lan
Pro
toco
l for
dis
ease
co
mm
unic
atio
n an
d pr
omot
ion
of s
hare
d de
cisi
on-m
akin
g (Dispo
sitifd’annonce)
To im
prov
e th
e or
gani
zatio
n of
pro
cess
es
and
com
pete
ncie
s in
dis
cuss
ing
a ca
ncer
di
agno
sis,
and
pro
mot
ing
shar
ed d
ecis
ion-
mak
ing
betw
een
prof
essi
onal
s, p
atie
nts
and
thei
r ca
rers
Car
e pr
otoc
olC
ance
r20
04S
peci
alis
tG
Ps,
spe
cial
ists
, nu
rses
, allie
d he
alth
pr
ofes
sion
als
(for
exam
ple,
psy
chol
ogis
ts),
soci
al w
orke
rs
Table
3.3
con
td

37Access to health care services within and between countries of the European Union
Nam
eA
im/g
ener
al d
escr
ipti
on
Typ
e o
f ap
pro
ach
Targ
et
po
pul
atio
nYe
ar
imp
lem
ente
dP
rinc
ipal
co
ord
inat
or
Pro
vid
ers
invo
lved
Fran
ce c
ontd
Mea
sure
s in
the
2003
–200
7 C
ance
r P
lan
cont
dM
ultid
isci
plin
ary
team
m
eetin
g (R
CP
)To
pro
mot
e th
e sy
stem
atic
use
of a
m
ultid
isci
plin
ary
team
in th
e de
velo
pmen
t of
the
Can
cer
Car
e pl
an s
o as
to im
prov
e th
e qu
ality
of c
ance
r di
agno
sis,
trea
tmen
t and
su
ppor
t
Mul
tidis
cipl
inar
y te
amC
ance
r20
04M
édec
in r
éfér
ent
(doctor’sreferral,
frequ
ently
sur
geon
)
Spe
cial
ists
, hos
pita
ls;
mul
tidis
cipl
inar
y te
am
com
pris
es a
s m
inim
um
surg
eon,
rad
iolo
gist
an
d on
colo
gist
Reg
iona
l can
cer
netw
orks
To c
oord
inat
e al
l rel
evan
t act
ors
and
leve
ls
of c
are
in th
e m
anag
emen
t of c
ance
r, an
d to
gu
aran
tee
qual
ity a
nd e
quity
of c
are
acro
ss a
ll re
gion
s
Car
e co
ordi
natio
n/pr
ovid
er
netw
ork
Can
cer
2004
As
in R
CP
Spe
cial
ists
, nur
ses,
ph
arm
acis
ts, h
ospi
tals
Loca
l can
cer
or lo
cal
mul
tiple
pat
holo
gy
netw
orks
To fa
cilit
ate
the
loca
l man
agem
ent a
nd
mon
itorin
g of
can
cer
patie
nts
thro
ugh
bett
er
inte
grat
ion
of G
Ps
into
net
wor
ks o
f can
cer c
are
Car
e co
ordi
natio
nC
ance
r20
04G
PG
Ps,
spe
cial
ists
, nu
rses
, allie
d he
alth
pr
ofes
sion
als,
ph
arm
acis
ts, h
ospi
tals
, so
cial
wor
kers
Ger
man
y
Dis
ease
man
agem
ent
prog
ram
mes
Org
aniz
atio
nal a
ppro
ach
to m
edic
al c
are
that
invo
lves
the
coor
dina
ted
trea
tmen
t and
ca
re o
f pat
ient
s w
ith c
hron
ic d
isea
se a
cros
s bo
unda
ries
betw
een
indi
vidu
al p
rovi
ders
on
thebasisofscientificandupto
dateevidence
Car
e co
ordi
natio
n Ty
pe 1
and
2
diab
etes
, IH
D
(+ h
eart
failu
re),
brea
st c
ance
r, as
thm
a/C
OP
D
2002
DM
P p
hysi
cian
GP
s, s
peci
alis
ts,
hosp
itals
GP
con
trac
tsTo
impr
ove
the
coor
dina
tion
of c
are
and
stre
ngth
en th
e ro
le o
f prim
ary
care
in th
e G
erm
an h
ealth
sys
tem
Car
e co
ordi
natio
nG
ener
alis
t (so
me
cont
ract
s ta
rget
th
e ov
er 6
5s)
2004
GP
/fam
ily p
hysi
cian
GP
s, n
urse
s
Inte
grat
ed c
are:
Hea
lthy
Kin
zigt
alToestablishmoreefficientandorganized
heal
th c
are
for
the
resi
dent
s of
the
Kin
zigt
al
area
Car
e co
ordi
natio
n G
ener
alis
t 20
05C
are
coor
dina
tor
(phy
sici
an/
psyc
hoth
erap
ist)
GP
s, s
peci
alis
ts,
psyc
hoth
erap
ists
,ho
spita
ls, p
harm
acis
ts,
allie
d he
alth
pro
fess
iona
ls;co
ordi
nate
d by
man
agem
ent
orga
niza
tion

38 Assessing chronic disease management in European health systems
Nam
eA
im/g
ener
al d
escr
ipti
on
Typ
e o
f ap
pro
ach
Targ
et
po
pul
atio
nYe
ar
imp
lem
ente
dP
rinc
ipal
co
ord
inat
or
Pro
vid
ers
invo
lved
Ger
man
y co
ntd
Com
mun
ity n
urse
s:
care
ass
ista
nt in
fam
ily
prac
tice
(for
exam
ple,
Ve
rAH
)
To s
uppo
rt G
P s
ervi
ces
in u
nder
serv
ed a
reas
Nur
se-le
d ca
re
Gen
eral
ist
(alth
ough
ty
pica
lly ta
rget
ing
the
over
65s
)
2005
Pra
ctic
e as
sist
ant
GP,
pra
ctic
e as
sist
ant
Hun
gary
Trea
tmen
t (an
d financing)protocols
To c
ontr
ol c
osts
of t
reat
men
t, su
ch a
s th
ose
for
expe
nsiv
e dr
ugs
in th
e ca
se o
f can
cer
care
Use
of
trea
tmen
t gu
idel
ines
Ast
hma/
CO
PD
, C
VD
(hea
rt
failu
re, I
HD
, st
roke
), ca
ncer
2005
(can
cer)
Varie
s by
dis
ease
(fo
r ex
ampl
e, G
P
for
hype
rten
sion
; sp
ecia
list f
or
canc
er)
GP
s, s
peci
alis
ts,
nurs
es, h
ospi
tals
, sp
ecia
list c
entr
es
(can
cer
disp
ensa
ry,
pulm
onar
y di
spen
sary
)
Car
e co
ordi
natio
n pi
lot
(CC
P)
To in
cent
iviz
e pr
ovid
ers
to ta
ke re
spon
sibi
lity
for
the
spec
trum
of s
ervi
ces
(prim
ary
to te
rtia
ry
care)foranenrolledpo
pulationinadefined
area
Car
e co
ordi
natio
n G
ener
alis
t19
98/9
9–20
08C
are
coor
dina
tion
orga
niza
tion:
GP
s/
grou
ps o
f GP
s,
poly
clin
ic o
r hos
pita
l
GP
s, s
peci
alis
ts,
nurs
es, a
llied
heal
th
prof
essi
onal
s,
hosp
itals
, pha
rmac
ists
Mul
tifun
ctio
nal
com
mun
ity c
entr
esToim
proveefficiencyinthehealthcaresystem
th
roug
h be
tter
qua
lity
of c
are
at lo
wer
cos
tsM
ultid
isci
plin
ary
team
sG
ener
alis
tO
ngoi
ngC
omm
unity
cen
tre
GP
s, s
peci
alis
ts,
nurs
es, p
harm
acis
ts,
soci
al c
are
Ast
hma
dise
ase
man
age-
men
t pro
gram
me
To e
nhan
ce th
e qu
ality
of a
sthm
a ca
re
Nur
se-le
d ca
reA
sthm
a20
04S
peci
alis
t (as
thm
a)
nurs
eN
urse
s, s
peci
alis
ts,
disp
ensa
ries
Dia
bete
s ca
re
man
agem
ent
prog
ram
me
To im
prov
e th
e ca
re o
f pat
ient
s w
ith ty
pe 2
di
abet
es th
roug
h a
rang
e of
mea
sure
s, w
ith
nurs
e-le
d ca
re a
t its
cor
e
Nur
se-le
d ca
reTy
pe 2
dia
bete
sVa
rious
D
iabe
tes
spec
ialis
t (p
hysi
cian
, nur
se)
Spe
cial
ists
, nur
ses,
ho
spita
ls, s
peci
alis
t di
abet
es o
utpa
tient
uni
ts
Italy
Dia
bete
s in
tegr
atio
n,
man
agem
ent a
nd
assi
stan
ce (I
GE
A)
Nat
iona
l str
ateg
y to
sup
port
the
impl
emen
tatio
n of
dis
ease
man
agem
ent f
or
type
2 d
iabe
tes
at th
e re
gion
al le
vel
Mul
tidis
cipl
inar
y te
am a
nd c
ase
man
agem
ent
Type
2 d
iabe
tes
2006
Mul
tidis
cipl
inar
y te
am/n
urse
(cas
e m
anag
emen
t)
GP
s, s
peci
alis
ts,
nurs
es, a
llied
heal
th
prof
essi
onal
s (fo
r ex
ampl
e, d
ietit
ian,
ps
ycho
logi
st),
hosp
itals
Table
3.3
con
td

39Access to health care services within and between countries of the European Union
Nam
eA
im/g
ener
al d
escr
ipti
on
Typ
e o
f ap
pro
ach
Targ
et
po
pul
atio
nYe
ar
imp
lem
ente
dP
rinc
ipal
co
ord
inat
or
Pro
vid
ers
invo
lved
Italy
con
td“F
rom
On-
Dem
and
to
Pro
activ
e P
rimar
y C
are”
pr
ogra
mm
e, T
usca
ny
A th
ree-
year
str
ateg
y to
war
ds th
e de
velo
pmen
t of
a n
ew o
rgan
izat
iona
l app
roac
h to
hea
lth
care
that
em
phas
izes
pro
activ
e pa
tient
car
e
Mul
tidis
cipl
inar
y te
am
Hyp
erte
nsio
n,
diab
etes
, chr
onic
he
art f
ailu
re,
CO
PD
, str
oke
2009
Mul
ti-pr
ofes
sion
al
team
s (m
odul
e) (G
P
lead
, com
mun
ity
heal
th d
octo
r, sp
ecia
list n
urse
)
GP
s, s
peci
alis
ts,
nurs
es, a
llied
heal
th
prof
essi
onal
s (fo
r ex
ampl
e, d
ietit
ian,
ps
ycho
logi
st),
soci
al
serv
ices
Leon
ardo
pilo
t pro
ject
, P
uglia
To im
prov
e th
e qu
ality
and
effe
ctiv
enes
s of
he
alth
car
e fo
r th
ose
with
chr
onic
con
ditio
ns
and
to fa
cilit
ate
syst
emat
ic in
tegr
atio
n in
to th
e ex
istin
g or
gani
zatio
nal f
ram
ewor
k se
t by
loca
l he
alth
age
ncie
s
Nur
se-le
d ca
re
Type
1 a
nd 2
di
abet
es, c
hron
ic
hear
t fai
lure
, hig
h ca
rdio
vasc
ular
ris
k
2004
–200
7S
peci
alis
t nur
seG
Ps,
nur
ses,
sp
ecia
lists
Raf
fael
lo p
roje
ct,
Mar
che
and
Abr
uzzo
Res
earc
h pr
ojec
t to
asse
ss th
e ef
fect
iven
ess
of a
n in
nova
tive
mod
el o
f pat
ient
car
e fo
r th
e pr
even
tion
of c
ardi
ovas
cula
r di
seas
e on
the
basi
s of
dis
ease
and
car
e m
anag
emen
t in
gene
ral p
ract
ice
Nur
se-le
d ca
re
Type
1 a
nd
2 di
abet
es,
card
iova
scul
ar
risk
2007
Spe
cial
ist n
urse
GP
s, n
urse
s
Latv
ia
Gen
eral
prim
ary
heal
th
care
sys
tem
Not
app
licab
leN
ot a
pplic
able
Gen
eral
ist
1996
–199
8 (p
rimar
y he
alth
ca
re re
form
)
GP
GPs,doctor’s
assi
stan
t (fe
ldsh
er),
nurs
e, m
idw
ife,
dentist,dentist’s
assi
stan
t, de
ntal
nu
rse
and
dent
al
hygi
ene
spec
ialis
t
Lith
uani
a
Impr
ovin
g in
ters
ecto
ral
colla
bora
tion
To im
prov
e co
llabo
ratio
n be
twee
n he
alth
and
so
cial
car
eC
ase
man
agem
ent
(pilo
t)
Gen
eral
ist a
nd
disease-specific
(dia
bete
s, C
VD
, ca
ncer
, chr
onic
re
nal f
ailu
re, m
ultip
le
scler
osis,
dep
ress
ion,
H
IV/A
IDS
)
From
200
4 N
urse
GP
s, s
peci
alis
ts,
prov
ider
s of
ed
ucat
iona
l and
soc
ial
serv
ices

40 Assessing chronic disease management in European health systems
Nam
eA
im/g
ener
al d
escr
ipti
on
Typ
e o
f ap
pro
ach
Targ
et
po
pul
atio
nYe
ar
imp
lem
ente
dP
rinc
ipal
co
ord
inat
or
Pro
vid
ers
invo
lved
Lith
uani
a co
ntd
Clin
ical
gui
delin
esTo
con
trol
med
icat
ion
cost
s; to
impr
ove
colla
bora
tion
betw
een
prim
ary
and
seco
ndar
y ca
re
Use
of c
linic
al
guid
elin
esD
iabe
tes,
CV
D,
brea
st c
ance
r, ch
roni
c re
nal
failu
re, m
ultip
le
scle
rosi
s,
depr
essi
on; h
igh-
inte
nsity
use
rs
From
200
2G
P/s
peci
alis
t (d
epen
ding
on
heal
th p
robl
em)
GP
s, s
peci
alis
ts,
nurs
es, a
llied
heal
th
prof
essi
onal
s,
hosp
itals
Net
herla
nds
Mat
ador
DM
P/
Maa
stric
ht-H
euve
lland
Bui
lds
on a
pilo
t sch
eme
esta
blis
hed
in 1
996,
w
hich
use
d sp
ecia
lized
dia
bete
s nu
rses
to
redu
ce th
e nu
mbe
r of p
atie
nts
seen
by
med
ical
sp
ecia
lists
in o
utpa
tient
car
e
Mul
tidis
cipl
inar
y te
amTy
pe 2
dia
bete
s20
00–2
006
Cor
e te
am o
f G
P, s
peci
alis
t di
abet
es n
urse
and
en
docr
inol
ogis
t
GP
s, s
peci
alis
ts,
nurs
es, h
ospi
tals
Prim
ary
care
gro
up Z
iO
(Maa
stric
ht-H
euve
lland
)Th
e pr
imar
y ca
re g
roup
des
crib
es th
e w
hole
co
ntin
uum
of c
are
for
diab
etes
pat
ient
s an
d is
financedonthebasisofthebundledpaym
ent
syst
em
Car
e co
ordi
natio
n Ty
pe 2
dia
bete
s (m
ore
rece
ntly
al
so a
sthm
a/C
OP
D,
card
iova
scul
ar
dise
ase)
From
200
7G
PG
Ps,
spe
cial
ists
, nu
rses
, allie
d he
alth
pr
ofes
sion
als,
ho
spita
ls
Str
oke
serv
ice
Del
ftE
volv
ed fr
om a
pilo
t pro
ject
for
impr
ovin
g st
roke
car
e in
itiat
ed in
199
7 an
d fu
nded
by
the
Net
herla
nds
Inst
itute
for
Hea
lth R
esea
rch
and
Dev
elop
men
t
Mul
tidis
cipl
inar
y te
am
Str
oke
1997
(pilo
t)S
hare
d ca
re n
urse
GP
s, s
peci
alis
ts,
nurs
es, h
ospi
tals
, al
lied
heal
th
prof
essi
onal
s, n
ursi
ng
hom
es, r
ehab
ilitat
ion
cent
res,
hom
e ca
re
orga
niza
tion
Nat
iona
l car
e st
anda
rd
for
vasc
ular
ris
k m
anag
emen
t
Des
crib
es th
e m
inim
um re
quire
men
ts fo
r ap
prop
riate
, pat
ient
-cen
tred
car
e al
ong
the
care
con
tinuu
m fr
om p
reve
ntio
n an
d ea
rly
dete
ctio
n to
trea
tmen
t and
reha
bilit
atio
n (th
ere
are
sim
ilar
stan
dard
s fo
r di
abet
es a
nd a
sthm
a/C
OP
D)
Mul
tidis
cipl
inar
y te
amVa
scul
ar r
isk
From
201
0C
entr
al c
areg
iver
(d
eter
min
ed b
y pr
ogra
mm
e)
GP
s, s
peci
alis
ts,
nurs
es, h
ospi
tals
, al
lied
heal
th
prof
essi
onal
s,
mun
icip
al h
ealth
se
rvic
es, p
harm
acis
ts,
reha
bilit
atio
n se
rvic
es
Table
3.3
con
td

41Access to health care services within and between countries of the European Union
Nam
eA
im/g
ener
al d
escr
ipti
on
Typ
e o
f ap
pro
ach
Targ
et
po
pul
atio
nYe
ar
imp
lem
ente
dP
rinc
ipal
co
ord
inat
or
Pro
vid
ers
invo
lved
Sw
itzer
land
Dia
Bai
d di
abet
es c
are
netw
ork
Dev
elop
ed fr
om a
n in
vent
ory
of th
e ne
eds
of d
iabe
tic p
atie
nts
in th
e re
gion
of N
yon–
Mor
ges,
Can
ton
de V
aud
and
the
crea
tion
of
a w
orki
ng g
roup
of h
ealth
car
e st
akeh
olde
rs
invo
lved
in d
iabe
tes
care
Mul
tidis
cipl
inar
y te
amTy
pe 1
and
2
diab
etes
2004
End
ocrin
olog
ist–
diab
etol
ogis
tS
peci
alis
ts, n
urse
s,
allie
d he
alth
pr
ofes
sion
als
(die
titia
n, p
odol
ogis
t)
Bre
ast c
ance
r cl
inic
al
path
way
, Lau
sann
e U
nive
rsity
Hos
pita
l and
La
usan
ne U
nive
rsity
Toim
provethequalityandefficiencyofhealth
care
Mul
tidis
cipl
inar
y te
amB
reas
t can
cer
2008
–200
9H
ospi
tal (
onco
logy
)S
peci
alis
ts, n
urse
s,
allie
d he
alth
pr
ofes
sion
als
(phy
siot
hera
pist
s,
psyc
holo
gist
s), s
ocia
l w
orke
rs
Del
ta p
hysi
cian
ne
twor
k, G
enev
aP
hysi
cian
net
wor
ks fo
rm p
art o
f the
se
rvic
e st
ruct
ure
in a
mbu
lato
ry c
are;
Del
ta
was
con
ceiv
ed a
s an
HM
O a
nd in
200
4 tr
ansf
orm
ed in
to a
phy
sici
an n
etw
ork
Man
aged
car
eG
ener
alis
t; D
MP
s fo
r di
abet
es,
hear
t fai
lure
and
as
thm
a un
der
deve
lopm
ent
1992
Prim
ary
care
ph
ysic
ians
/GP
sP
rimar
y ca
re
phys
icia
ns,
phar
mac
ists
, ps
ycho
logi
sts
Sour
ces:
Austr
ia: S
önni
chse
n, F
lam
m &
Nol
te (2
015)
; Den
mar
k: F
rølic
h, Ja
cobs
en &
Kna
i (20
15);
Engl
and:
Nol
te e
t al.
(201
5); E
stoni
a: L
ai &
Kna
i (20
15);
Fran
ce: C
hevr
eul e
t al.
(201
5); G
erm
any:
Erle
r, Fu
llert
on &
Nol
te (2
015)
; Hun
gary
: Gaa
l et a
l. (2
015)
; Ita
ly: R
icci
ardi
et a
l. (2
015)
; Lith
uani
a: L
ai e
t al.
(201
5); L
atvi
a: L
ai, K
nai &
Tau
be (2
015)
; the
Net
herla
nds:
Eliss
en e
t al.
(201
5); S
witz
erla
nd: P
eytre
man
n-Br
idev
aux
et a
l. (2
015)
.

42 Assessing chronic disease management in European health systems
3.4 Financing, distribution and uptake of approaches to chronic disease management
The majority of approaches reviewed are funded within the public health care system, frequently supplemented by additional resources made available through (time-limited) funds earmarked for care coordination and integration initiatives, for example: reform pool projects in Austria, such as the Therapie aktiv diabetes management programme; regional diabetes management programme in Denmark; the quality management framework for diabetes and chronic CVD care in Estonia; the FIQCS intervention fund for quality and care coordination in France to support provider networks; integrated care contracts in Germany; and the ministry of mealth ‘special programmes’ fund in Italy (Table 3.4). In several cases, additional funding has provided a one-off start-up grant to support project implementation; examples include the two major pilot programmes in England (Partnership for Older People Projects; integrated care contracts) and, until 2009, integrated care contracts in Germany. There are examples of additional funding provided by the pharmaceutical industry, including, in Hungary, the asthma disease management and diabetes care programmes, and in Italy, the Leonardo and Raffaello diabetes disease and care management projects.
Several approaches use financial incentives, usually targeted at physicians. These typically involve additional reimbursement for documentation, patient enrolment or regular assessment (for example, the DMPs in Austria and Germany; the Sophia diabetes and asthma care programme in France) or for quality improvement activities (quality management in primary health care in Hungary; GP contracts in Germany; the Delta physician network in Switzerland). Selected approaches also involve elements of pay-for-performance or financial risk sharing of providers. Examples include the CCP in Hungary; “From On-Demand to Proactive Primary Care” programme in Tuscany, Italy; the Leonardo project in Puglia, Italy; and the primary care group/bundled payment systems in the Netherlands.
Given that most of the approaches reviewed here are funded within the statutory system, patient access is typically granted in line with access to usual care. Indeed, the majority of approaches are free of charge. Only a small number require co- or full payment by patients to enable access, for example, ambulatory after-care for stroke patients in Salzburg, Austria (with exemption from co-payments for those on low incomes). Some approaches offer explicit incentives for patients to participate. These typically include exemption from co-payments for usual care services they would otherwise have to pay for (for example, provider networks in France).

43Access to health care services within and between countries of the European Union
Table
3.4
Fin
anci
ng, d
istr
ibut
ion
and
upta
ke o
f app
roac
hes
to c
hron
ic d
isea
se m
anag
emen
t or
thei
r eq
uiva
lent
in 1
2 E
urop
ean
coun
trie
s
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Aus
tria
‘The
rapi
e aktiv’d
isease
man
agem
ent
prog
ram
me
Reg
iona
l SH
I fun
d an
d fe
dera
l sta
te a
t abo
ut
50%
eac
h; p
rogr
amm
e de
velo
pmen
t fun
ded
by
regi
onal
SH
I fun
ds
Targ
eted
at D
MP
ph
ysic
ians
: pat
ient
si
gn-u
p an
d qu
arte
rly
fee
for
trea
tmen
t and
do
cum
enta
tion
Free
acc
ess
for
part
icip
atin
g pa
tient
s to
ed
ucat
ion
clas
ses
and
mat
eria
ls
Impl
emen
ted
in s
ix o
f nin
e st
ates
, inv
olvi
ng
abou
t 100
0 G
Ps
(201
4); t
hree
sta
tes
do n
ot
curr
ently
pro
vide
The
rapi
e ak
tiv b
ut o
ffer
diab
etes
edu
catio
n pr
ogra
mm
es
Abo
ut 3
9 50
0 pa
tient
s en
rolle
d inDMPacrossthefivestates
that
hav
e im
plem
ente
d Th
erap
ie
aktiv
(18%
of a
ll pe
ople
with
type
2
diab
etes
) (20
14)
Inte
grat
ed s
trok
e ca
re, U
pper
A
ustr
ia
Reg
iona
l SH
I fun
d U
pper
A
ustr
ia a
nd U
pper
Aus
tria
he
alth
fund
(50%
eac
h)
Notspecified
Not
app
licab
leIm
plem
ente
d ac
ross
Upp
er A
ustr
ia a
nd
invo
lvin
g al
l hos
pita
ls th
at p
rovi
de a
cute
st
roke
car
e, m
edic
al e
mer
genc
y se
rvic
es
and
thre
e re
habi
litat
ion
cent
res;
tran
sfer
red
into
rout
ine
care
from
the
end
of 2
010
Ther
e ar
e no
pub
lishe
d da
ta o
n th
e nu
mbe
r of
str
oke
patie
nts
whohavebenefitedfrom
the
prog
ram
me
so fa
r
Car
e co
ordi
natio
n/in
terfa
ce
man
agem
ent
Sty
ria
Reg
iona
l SH
I fun
d S
tyria
; Gra
z m
odel
als
o su
ppor
ted
by S
tyria
hea
lth
fund
(200
9)
Not
app
licab
leN
ot a
pplic
able
Intr
oduc
ed a
s pi
lot p
roje
ct in
one
loca
lity,
th
e ap
proa
ch w
as g
radu
ally
ext
ende
d ac
ross
Sty
ria; G
raz
mod
el to
be
tran
sfer
red
into
usu
al c
are
Ther
e ar
e no
pub
lishe
d da
ta o
n th
e nu
mbe
r of
pat
ient
s co
vere
d by
the
prog
ram
me
Am
bula
tory
afte
r-ca
re o
f str
oke
patie
nts,
Sal
zbur
g
Sal
zbur
g he
alth
fund
(9
5%) p
lus
3% p
atie
nt c
o-pa
ymen
t (de
duct
ible
for
hom
e vi
sit)
Not
app
licab
leN
ot a
pplic
able
Ser
vice
prin
cipa
lly a
cces
sibl
e to
all
stro
ke
patie
nts
acro
ss L
and
Sal
zbur
g; la
ck o
f th
erap
ists
in re
mot
e ar
eas
redu
ces
acce
ss
In 2
009,
the
serv
ice
cove
red
appr
oxim
atel
y 45
0 pa
tient
s w
ho
can
acce
ss s
ervi
ce o
n re
ferr
al
only
Kar
diom
obil
– H
ome
care
for
patie
nts
with
ch
roni
c he
art
failu
re
Reg
iona
l SH
I fun
d an
d La
nd S
alzb
urg
at a
bout
50
% e
ach
Not
app
licab
leN
ot a
pplic
able
Program
mecomprisesfivetrainednurses
oper
atin
g ac
ross
Lan
d S
alzb
urg
Acc
ess
to th
e se
rvic
e is
thro
ugh
refe
rral
; the
re a
re n
o pu
blis
hed
data
on
the
num
ber
of p
atie
nts
cove
red
Den
mar
k
SIK
S p
roje
ct –
In
tegr
ated
effo
rt
for
peop
le li
ving
w
ith c
hron
ic
dise
ase
Com
bina
tion
of u
sual
so
urce
s an
d go
vern
men
t gr
ant f
or 2
005–
2007
pr
ojec
t per
iod;
full
fund
ing
from
usu
al s
ourc
es fr
om
2007
Not
app
licab
leN
etw
orki
ng a
nd
peer
pre
ssur
e th
roug
h st
eerin
g co
mm
ittee
, pro
ject
gr
oup
and
wor
king
gr
oups
thro
ugho
ut
proj
ect p
erio
d
Impl
emen
ted
as a
pilo
t pro
ject
in th
e Ø
ster
bro
heal
th c
are
cent
re a
nd B
ispe
bjer
g ho
spita
l in
Cop
enha
gen
for
a pe
riod
of
thre
e ye
ars;
sub
sequ
ently
a p
art o
f DM
P
for
CO
PD
, typ
e 2
diab
etes
and
CV
D in
the
Cap
ital R
egio
n of
Den
mar
k
Dur
ing
2005
–200
7, a
bout
70
0 pa
tient
s pa
rtic
ipat
ed
in th
e S
IKS
pro
ject
; acc
ess
is th
roug
h re
ferr
al fo
llow
ing
diag
nosi
s (a
ppro
xim
atel
y 90
%
of p
artic
ipat
ing
phys
icia
ns re
fer
patie
nts
on)

44 Assessing chronic disease management in European health systems
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Den
mar
k co
ntd
Reg
iona
l dis
ease
m
anag
emen
t pr
ogra
mm
es
Cen
tral
gov
ernm
ent
fund
ing
pool
for
the
deve
lopm
ent o
f DM
Ps
of
DK
K 4
38 m
illion
dur
ing
2010
-201
2
Not
pla
nned
Notspecified
DM
Ps
for
CO
PD
and
type
2 d
iabe
tes,
CV
D,
dem
entia
and
mus
culo
skel
etal
dis
orde
rs
impl
emen
ted
in C
apita
l Reg
ion
(end
201
0);
DM
Ps
for
CO
PD
, typ
e 2
diab
etes
, CV
D,
depr
essi
on a
nd lo
wer
-bac
k pa
in d
evel
oped
in
the
Cen
tral
Den
mar
k R
egio
n; D
MP
s fo
r C
OP
D, t
ype
2 di
abet
es, C
VD
and
ske
leta
l di
sord
ers
deve
lope
d an
d, fr
om 2
010,
im
plem
ente
d in
sou
ther
n D
enm
ark;
DM
Ps
for
CO
PD
, typ
e 2
diab
etes
, dem
entia
, sc
hizo
phre
nia
and
back
pro
blem
s de
velo
ped
in R
egio
n Ze
elan
d
It is
ant
icip
ated
that
the
prog
ram
mes
will
cove
r al
l ta
rget
ed p
atie
nts
acro
ss th
e co
untr
y
Inte
grat
ed c
linic
al
path
way
sFu
nded
from
usu
al
sour
ces
(taxa
tion)
Not
app
licab
leNotspecified
As
a na
tiona
l pro
gram
me,
inte
grat
ed
clin
ical
pat
hway
s ar
e im
plem
ente
d ac
ross
D
enm
ark
It is
ant
icip
ated
that
the
inte
grat
ed c
linic
al p
athw
ays
will
cove
r ap
prox
imat
ely
40 0
00
CV
D p
atie
nts
per
year
and
all
canc
er p
atie
nts
Eng
land
Cas
e m
anag
emen
t/co
mm
unity
mat
ron
Fund
ed fr
om u
sual
so
urce
s w
ithin
the
NH
SN
oNotspecified
2004
pol
icy
fore
saw
impl
emen
tatio
n of
ca
se m
anag
emen
t and
app
oint
men
t of
3000
com
mun
ity m
atro
ns b
y al
l PC
Ts in
20
07; t
here
are
now
bet
wee
n 62
0 an
d 13
50 c
omm
unity
mat
rons
In p
rinci
ple,
all
NH
S p
atie
nts
in
Eng
land
sho
uld
have
acc
ess
to
com
mun
ity m
atro
n se
rvic
es
Qua
lity
and
outc
omes
fra
mew
ork
(QO
F)
Fund
ed fr
om u
sual
so
urce
s w
ithin
the
NH
SYe
s: a
war
d of
ac
hiev
emen
t po
ints
for
prac
tices
de
mon
stra
ting
that
they
hav
e m
et
seve
ral s
tage
s in
th
e m
anag
emen
t of
a g
iven
, usu
ally
ch
roni
c co
nditi
on, f
or
a pr
opor
tion
of th
e re
leva
nt p
opul
atio
n
Pee
r pr
essu
re:
perfo
rman
ce re
sults
ar
e pu
blis
hed
by
the
Hea
lth &
Soc
ial
Car
e In
form
atio
n C
entr
e
Volu
ntar
y fo
r G
P p
ract
ices
; mos
t pra
ctic
es
have
join
ed. C
urre
ntly,
mor
e th
an 8
000
prac
tices
hav
e si
gned
up
to th
e sc
hem
es,
cove
ring
som
e 54
milli
on p
eopl
e in
Eng
land
The
sche
me
initi
ally
app
lied
to
acro
ss th
e U
nite
d K
ingd
om a
nd
prin
cipa
lly c
over
s al
l pat
ient
s re
gist
ered
with
a g
iven
pra
ctic
e pa
rtic
ipat
ing
in th
e sc
hem
e; fr
om
2013
, QO
F ha
s di
ffere
d ac
ross
th
e fo
ur c
ount
ries
of th
e U
nite
d K
ingd
om
Table
3.4
con
td

45Access to health care services within and between countries of the European Union
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Eng
land
con
td
Par
tner
ship
for
olde
r pe
ople
pr
ojec
t (P
OP
P)
Ser
vice
s de
liver
ed b
y pi
lots
fund
ed fr
om u
sual
so
urce
s (h
ealth
ser
vice
s:
NH
S; s
ocia
l ser
vice
s: lo
cal
auth
oriti
es)
Gov
ernm
ent g
rant
to
supp
ort p
ilot s
et-u
pR
ecog
nitio
n as
a
gove
rnm
ent-
spon
sore
d pi
lot s
ite
PO
PP
ran
a to
tal o
f 146
pro
ject
s in
volv
ing
522
orga
niza
tions
incl
udin
g th
e po
lice
and
hous
ing
asso
ciat
ions
; 85%
of p
roje
cts
secu
red
fund
ing
beyo
nd th
e pi
lot p
hase
in
to u
sual
car
e
Aro
und
264
000
peop
le w
ere
cove
red
by th
e se
rvic
es p
rovi
ded
by p
roje
cts
Inte
grat
ed c
are
pilo
tsS
ervi
ces
deliv
ered
by
pilo
ts fu
nded
from
usu
al
sour
ces
(hea
lth s
ervi
ces:
N
HS
; soc
ial s
ervi
ces:
loca
l au
thor
ities
)
Gov
ernm
ent g
rant
to
supp
ort p
ilot s
et-u
p (g
rant
s of
bet
wee
n G
BP
600
000
and
GB
P3.
9 m
illion
per
si
te o
ver
two
year
s)
Rec
ogni
tion
as
a go
vern
men
t-sp
onso
red
pilo
t site
The
pilo
t pro
gram
me
invo
lved
16
Prim
ary
care
trus
tsP
opul
atio
n co
vera
ge o
f sch
emes
va
ried;
acc
ess
to s
ervi
ces
limite
d to
(tar
get)
popu
latio
ns in
pilo
t si
tes
Est
onia
Qua
lity
man
agem
ent i
n pr
imar
y he
alth
ca
re
Fund
ed fr
om u
sual
so
urce
s (E
HIF
); ad
ditio
nal
fund
ing
with
in q
ualit
y m
anag
emen
t fra
mew
ork
for
diab
etes
/CV
D c
are
Targ
eted
at G
P
prac
tices
with
in
qual
ity m
anag
emen
t fra
mew
ork
Net
wor
king
am
ong
prov
ider
sQ
ualit
y m
anag
emen
t fra
mew
ork
for
diab
etes
and
chr
onic
CV
D im
plem
ente
d ac
ross
Est
onia
and
cov
erin
g al
l GP
pr
actic
es
Prin
cipa
lly, a
ll pe
rson
s w
ith
diab
etes
/chr
onic
CV
D a
re
cove
red
by v
irtue
of S
HI;
acce
ss
to c
are
is fr
ee o
f cha
rge
Chr
onic
dis
ease
m
anag
emen
t at
the
prim
ary/
seco
ndar
y ca
re
inte
rface
Fund
ed fr
om u
sual
so
urce
s; a
dditi
onal
fundingforParkinson’s
asso
ciat
ion
for
patie
nt
educ
atio
n an
d su
ppor
t
Not
app
licab
leN
etw
orki
ng a
mon
g pr
ovid
ers
Impl
emen
ted
acro
ss E
ston
ia a
s pa
rt o
f us
ual c
are
Prin
cipa
lly, a
ll pe
rson
s w
ith
diag
nose
d di
seas
e co
vere
d by
vi
rtue
of S
HI;
acce
ss to
car
e is
fre
e of
cha
rge
Fran
ceP
rovi
der
netw
orks
Fo
r ex
ampl
e,
diab
etes
net
wor
ks:
RE
VE
SD
IAB
FIQ
CS
fund
est
ablis
hed
by 2
007
heal
th re
form
Fees
for
vario
us
prov
ider
s in
the
netw
ork,
for
exam
ple,
GP
s (a
nnua
l ass
essm
ent),
ed
ucat
ion,
die
titia
ns
Free
acc
ess
for
patie
nts
to c
erta
in
serv
ices
that
wou
ld
othe
rwis
e ha
ve
to p
ay fo
r (fo
r ex
ampl
e, fo
ot c
are)
RE
VE
SD
IAB
is b
ased
in th
ree
depa
rtm
ents
(d
épar
tmen
ts) i
n th
e P
aris
regi
on, i
nvol
ving
, in
200
7–20
08, a
roun
d 50
0 he
alth
pr
ofes
sion
als
in th
e E
sson
ne d
epar
tmen
t; O
vera
ll, in
200
7, th
ere
wer
e 72
dia
bete
s ne
twor
ks, i
nvol
ving
14
000
heal
th
prof
essi
onal
s
RE
VE
SD
IAB
is b
ased
in th
e P
aris
regi
on c
over
ing
abou
t 30
00 p
atie
nts
with
dia
bete
s;
over
all,
in 2
007,
aro
und
60 0
00
peop
le w
ith d
iabe
tes
wer
e en
rolle
d in
dia
bete
s ne
twor
ks
(app
roxi
mat
ely
2.5%
of d
iabe
tic
patie
nts
in F
ranc
e)

46 Assessing chronic disease management in European health systems
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Fran
ceP
rovi
der
netw
orks
con
tdFo
r ex
ampl
e,
Coo
rdin
atio
n of
pr
ofes
sion
al c
are
for
the
elde
rly
(CO
PA)
FIQ
CS
fund
est
ablis
hed
by th
e 20
07 h
ealth
refo
rmNotspecified
Notspecified
The
netw
ork
is e
stab
lishe
d in
one
dis
tric
t of
Par
is o
nly
and
in 2
007
invo
lved
79
out
of 2
00 p
rimar
y ca
re p
hysi
cian
s pr
actis
ing
in th
e ar
ea
By
the
end
of 2
007,
ap
prox
imat
ely
250
olde
r pe
ople
ha
d be
en re
ferr
ed to
CO
PA;
it is
bei
ng im
plem
ente
d in
ot
her
part
s of
Par
is a
nd th
ere
is in
tere
st in
oth
er re
gion
s of
Fr
ance
and
Bel
gium
als
o
Specificprogram
mes
Sop
hia
diab
etes
an
d as
thm
a ca
re
prog
ram
me
Fund
ed fr
om u
sual
so
urce
s (S
tatu
tory
hea
lth
insu
ranc
e (C
NA
M)
GP
s in
volv
ed a
re
paid
EU
R 6
6 pe
r pa
tient
per
yea
r
Pro
vide
s pa
tient
s w
ith fr
ee a
cces
s to
tele
phon
e-ba
sed
inte
rven
tion
by tr
aine
d nu
rse
follo
win
g en
rolm
ent
with
SH
I fun
d
Exp
erim
enta
l pha
se ta
rget
ed p
atie
nts
of 6
000
GP
s (6
.4%
of a
ll G
Ps)
in 1
0 de
part
men
ts; e
xpan
ded
in 2
010
to re
ach
17 5
00 G
Ps
in 1
9 de
part
men
ts; r
oll-o
ut
acro
ss F
ranc
e in
201
3
Exp
erim
enta
l pha
se a
imed
at
reac
hing
136
000
pat
ient
s w
ith d
iabe
tes;
by
the
end
of 2
010,
62
000
had
join
ed
(app
roxi
mat
ely
2.5%
of a
ll pe
ople
with
dia
bete
s)
Hea
lth A
ctio
n by
Te
ams
of S
elf-
Em
ploy
ed H
ealth
P
rofe
ssio
nals
(A
SA
LEE
)
UR
CA
M (r
egio
nal S
HI
fund
); us
ual s
ourc
esN
oP
rofe
ssio
nal
mot
ivat
ion
(pro
ject
w
as s
et u
p by
loca
l G
Ps)
ASALE
Eisanon-profitorganizationwhich,
as o
f 200
7, b
roug
ht to
geth
er 4
1 G
Ps
and
eigh
t nur
ses
in 1
8 G
P p
ract
ices
The
proj
ect c
over
ed a
roun
d 15
00 p
atie
nts
Hos
pita
l dis
char
ge
prog
ram
for
hear
t fa
ilure
pat
ient
s (P
RA
DO
)
Fund
ed fr
om u
sual
so
urce
s (S
tatu
tory
hea
lth
insu
ranc
e (C
NA
M)
GP
s au
thor
ized
to b
ill a
long
con
sulta
tion
for
coor
dina
tion
effo
rts
Ded
icat
ed tr
aini
ng
for
hom
e fo
llow
-up
by n
urse
s
Pilotp
haseinfivedepartm
ents
The
pilo
t pha
ses
conc
erns
an
estim
ated
60
000
patie
nts
per
year
Specificpayment
base
d on
pub
lic
heal
th o
bjec
tives
(R
OS
P)
Sta
tuto
ry h
ealth
insu
ranc
e (C
NA
M)
Yes:
add
ition
al
rem
uner
atio
n ta
kes
into
acc
ount
the
popu
latio
n si
ze a
nd
29 q
ualit
y in
dica
tors
w
ith in
term
edia
te
andfinaltargets
Phy
sici
ans
can
follo
w th
e ev
olut
ions
of t
heir
qual
ity in
dica
tors
on
a d
edic
ated
w
ebsi
te
Volu
ntar
y pa
rtic
ipat
ion
In 2
012,
mor
e th
an 7
5 00
0 ph
ysic
ians
par
ticip
ated
in th
e pr
ogra
mm
e, re
pres
entin
g a
maj
ority
of e
ligib
le G
Ps
Table
3.4
con
td

47Access to health care services within and between countries of the European Union
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Fran
ce c
ontd
Mea
sure
s of
the
2003
–200
7 C
ance
r P
lan
Pro
toco
l fo
r di
seas
e co
mm
unic
atio
n an
d pr
omot
ion
of
shar
ed d
ecis
ion-
mak
ing
(Dis
posi
tif
d’annonce)
Fund
ed fr
om re
gion
al
budg
ets
with
in M
IGA
C
envelope(specificbudget
tofinanceactivitiesof
publ
ic u
tility
) as
part
of
usu
al c
are
(hos
pita
l re
imbu
rsem
ent)
with
in S
HI
Som
e re
gion
s su
pple
men
t us
ual p
aym
ent t
o ph
ysic
ians
for
time
dedi
cate
d to
pat
ient
s w
ithin
dis
posi
tif
d’annonce
Net
wor
king
ha
s be
en m
ade
oblig
ator
y fo
r th
e m
anag
emen
t of
canc
er p
atie
nts
As
part
of t
he n
atio
nal C
ance
r P
lan,
pr
inci
pally
rolle
d ou
t acr
oss
the
coun
try
with
in th
e tim
e fra
me
of th
e 20
03–2
007
Can
cer
Pla
n; b
y 20
06, o
nly
half
of th
e fu
nds
set a
side
by
regi
ons
had
been
use
d fo
r th
is p
urpo
se a
nd a
cces
sibl
e to
all
new
ly
diag
nose
d ca
ncer
pat
ient
s
By
2007
, mor
e th
an 9
2 00
0 pa
tient
s ha
d be
en s
uppo
rted
th
roug
h a
dedi
cate
d di
spos
itif
d’annonce(app
roximately30%
of a
ll pa
tient
s ne
wly
dia
gnos
ed
with
can
cer);
app
roxi
mat
ely
23 0
00 h
ad re
ceiv
ed a
pe
rson
aliz
ed c
are
prog
ram
me
(PP
S) (
appr
oxim
atel
y 7%
of
patie
nts)
Mul
tidis
cipl
inar
y te
am m
eetin
g (R
CP
)
Fund
ed fr
om re
gion
al
budg
ets
with
in th
e M
IGA
C
envelope(specificbudget
tofinanceactivitiesof
publ
ic u
tility
) as
part
of
usu
al c
are
(hos
pita
l re
imbu
rsem
ent)
with
in S
HI
Notspecified
Notspecified
As
part
of t
he n
atio
nal C
ance
r P
lan,
pr
inci
pally
rolle
d ou
t acr
oss
the
coun
try
with
in ti
me
fram
e of
200
3–20
07 C
ance
r P
lan
and
acce
ssib
le to
all
new
ly d
iagn
osed
ca
ncer
pat
ient
s
By
2007
, app
roxi
mat
ely
500
000
RC
Ps
had
been
re
cord
ed w
hile
the
num
ber
of n
ewly
dia
gnos
ed c
ance
r pa
tient
s w
as 3
45 0
00 (p
artly
reflectingrepeatRCPforsome
patie
nts
pre/
post
-tre
atm
ent);
ap
prox
imat
ely
45%
of c
ance
r ca
ses
wer
e re
cord
ed b
y R
CP
s
Reg
iona
l can
cer
netw
orks
FIQ
CS
fund
est
ablis
hed
by 2
007
heal
th re
form
Notspecified
Net
wor
king
ha
s be
en m
ade
oblig
ator
y fo
r th
e m
anag
emen
t of
canc
er p
atie
nts;
po
ssib
ility
of
prov
ider
mon
itorin
g th
roug
h E
EP
As
part
of t
he n
atio
nal C
ance
r P
lan
rolle
d ou
t acr
oss
the
coun
try
with
in th
e tim
e fra
me
of th
e 20
03–2
007
Can
cer
Pla
n an
d ac
cess
ible
to a
ll ca
ncer
pat
ient
s
Not
kno
wn

48 Assessing chronic disease management in European health systems
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Fran
ceM
easu
res
of th
e 20
03–2
007
Can
cer
Pla
n co
ntd
Loca
l can
cer
or
loca
l mul
tiple
pa
thol
ogy
netw
orks
GP
s an
d nu
rses
fund
ed
from
usu
al s
ourc
es
with
in S
HI;
netw
orks
fu
nded
thro
ugh
FIQ
CS
es
tabl
ishe
d by
the
2007
he
alth
refo
rm
Phy
sici
ans:
pos
sibi
lity
to re
ceiv
e ad
ditio
nal
reim
burs
emen
t fo
r tim
e/ex
pert
ise
dedi
cate
d to
can
cer
patie
nts;
Pat
ient
s:
maybenefitfrom
financialsuppo
rt
for
hous
ehol
d as
sist
ance
Net
wor
king
ha
s be
en m
ade
oblig
ator
y fo
r th
e m
anag
emen
t of
canc
er p
atie
nts;
po
ssib
ility
of
prov
ider
mon
itorin
g th
roug
h E
EP
As
part
of t
he n
atio
nal C
ance
r P
lan,
pr
inci
pally
rolle
d ou
t acr
oss
the
coun
try
with
in th
e tim
e fra
me
of th
e 20
03–2
007
Can
cer
Pla
n an
d ac
cess
ible
to a
ll ca
ncer
pa
tient
s
Not
kno
wn
Ger
man
y
Dis
ease
m
anag
emen
t pr
ogra
mm
es
Fund
ed fr
om u
sual
so
urce
s (S
HI)
DM
P p
hysi
cian
s:
addi
tiona
l pay
men
t fo
r do
cum
enta
tion,
ed
ucat
ion
Free
acc
ess
for
part
icip
atin
g pa
tient
s to
ed
ucat
ion
clas
ses
and
mat
eria
ls;
phys
icia
ns: p
eer
pres
sure
; SH
I fun
ds
lega
lly re
quire
d to
of
fer
DM
P
DM
Ps
are
offe
red
by S
HI f
unds
acr
oss
Ger
man
y; in
201
3 th
ere
wer
e 17
00–1
800
DM
Ps
for
each
con
ditio
n; th
e nu
mbe
r of
par
ticip
atin
g ph
ysic
ians
var
ies,
ap
prox
imat
ely
65%
GP
s ac
t as
DM
P
phys
icia
n fo
r ty
pe 2
dia
bete
s (5
7% fo
r C
HD
)
By
the
end
of 2
013,
a to
tal
of 6
.4 m
illion
indi
vidu
als
wer
e en
rolle
d in
one
or
mor
e D
MP
s,
from
122
214
in b
reas
t can
cer
DM
P to
app
roxi
mat
ely
3.8
milli
on in
type
2 d
iabe
tes
DM
P
GP
con
trac
tsP
rinci
pally
from
usu
al
sour
ces
(SH
I) bu
t with
co
ntra
ct a
rran
gem
ents
perm
ittingflexible
GP
pay
men
t diff
eren
t fro
m u
sual
car
e G
P
reim
burs
emen
t
GP
s: a
dditi
onal
pa
ymen
t for
asp
ects
su
ch a
s qu
ality
im
prov
emen
t and
ra
tiona
l pre
scrib
ing.
P
atie
nts:
exe
mpt
ion
from
pra
ctic
e fe
e
GP
s: P
eer
pres
sure
in
som
e re
gion
s;
SH
I fun
ds le
gally
re
quire
d to
offe
r G
P
cont
ract
s
By
the
end
of 2
007,
55
GP
con
trac
ts h
ad
been
con
clud
ed w
ith G
P p
artic
ipat
ion
vary
ing
amon
g re
gion
s; m
ore
rece
nt d
ata
are
not d
ocum
ente
d
Pro
port
ion
of S
HI i
nsur
ed
peop
le e
nrol
led
varie
s be
twee
n 5.
9 m
illion
(8.5
% o
f all
SH
I in
sure
d) in
200
7 to
19%
in 2
010
Table
3.4
con
td

49Access to health care services within and between countries of the European Union
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Ger
man
y co
ntd
Inte
grat
ed c
are:
H
ealth
y K
inzi
gtal
Prin
cipa
lly fu
nded
fro
m u
sual
sou
rces
(S
HI)
but w
ith c
ontr
act
arra
ngem
ents
per
mitt
ing
flexiblereimbursem
ent;
star
t-up
fund
s (ti
me-
limite
d to
end
of 2
008)
Phy
sici
an
reim
burs
emen
t in
volv
es p
ay-f
or-
perfo
rman
ce (P
4P)
elem
ent
Phy
sici
ans:
ne
twor
king
; pa
tient
s: a
cces
s to
free
che
ck-
ups,
pre
vent
ion/
trea
tmen
t pla
ns,
case
con
fere
nces
w
ith s
peci
alis
ts,
etc.
By
the
end
of 2
008,
app
roxi
mat
ely
6400
in
tegr
ated
car
e co
ntra
cts
had
been
co
nclu
ded;
con
tent
and
sco
pe v
arie
s w
idel
y an
d th
eir
num
ber
has
stag
nate
d si
nce;
Hea
lthy
Kin
zigt
al in
volv
es o
ver
90
prov
ider
s (5
2% o
f all
prov
ider
s in
the
regi
on
in 2
013)
By
the
end
of 2
008,
ap
prox
imat
ely
4 m
illion
SH
I m
embe
rs w
ere
enro
lled
with
an
inte
grat
ed c
are
cont
ract
(a
ppro
xim
atel
y 6%
of a
ll S
HI
insu
red)
; Hea
lthy
Kin
zigt
al
cove
rs o
ver
9000
peo
ple
(30%
of
the
rele
vant
SH
I mem
bers
in
the
regi
on) (
2013
)
Com
mun
ity
nurs
es: c
are
assi
stan
t in
fam
ily
prac
tice
(Ver
AH
)
Prin
cipa
lly fu
nded
from
us
ual s
ourc
es (S
HI)
with
in
GP
con
trac
ts
GP
s: s
ervi
ces
prov
ided
by
prac
tice
assi
stan
ts
reim
burs
able
thro
ugh
SH
I
Pra
ctic
e as
sist
ant:
prof
essi
onal
de
velo
pmen
t
Inco
rpor
ated
in s
elec
ted
GP
mod
els,
see
ab
ove
Inco
rpor
ated
in s
elec
ted
GP
m
odel
s, s
ee a
bove
Hun
gary
Trea
tmen
t (andfinancing)
prot
ocol
s
Fund
ed fr
om u
sual
so
urce
s (S
HI)
No
Notspecified
As
part
of t
he m
ain
syst
em, c
over
age,
in
prin
cipl
e, is
100
%. I
n pr
actic
e, th
e ad
here
nce
to tr
eatm
ent p
roto
cols
is r
arel
y au
dite
d
In p
rinci
ple,
all
diag
nose
d pa
tient
s sh
ould
be
cove
red
by
trea
tmen
t pro
toco
ls; a
cces
s is
lik
ely
to v
ary
acro
ss re
gion
s,
reflectinginequalitiesinoverall
acce
ss to
car
e
Car
e co
ordi
natio
n pi
lot
Prin
cipa
lly fu
nded
from
us
ual s
ourc
es (S
HI);
ad
ditio
nal f
undi
ng fo
r ad
min
istr
ativ
e co
sts
and
prev
entio
n pr
ogra
mm
es
(cap
itatio
n fo
r ca
re
coor
dina
tor)
Phy
sici
ans:
ris
k sh
arin
g w
ith s
avin
gs
achi
eved
at e
nd
offinancialyear
redi
strib
uted
to
prov
ider
s
Pro
vide
rs:
peer
pre
ssur
e;
netw
orki
ng
The
CC
P g
radu
ally
exp
ande
d fro
m n
ine
care
coo
rdin
ator
s in
199
9 to
16
care
co
ordi
nato
rs in
200
5 w
hen
1500
GP
pr
actic
es p
artic
ipat
ed; e
stab
lishe
d in
the
Vere
segy
ház
regi
on, t
he C
CP
was
clo
sed
dow
n in
200
8
Gra
dual
exp
ansi
on o
f the
pr
ojec
t cov
erin
g 16
0 00
0 re
side
nts
in th
e re
gion
of
Vere
segy
ház
in 1
999
to 2
milli
on
in 2
005

50 Assessing chronic disease management in European health systems
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Hun
gary
con
tdM
ultif
unct
iona
l co
mm
unity
ce
ntre
s
Prin
cipa
lly fu
nded
fro
m u
sual
sou
rces
; in
frast
ruct
ure
inve
stm
ents
fro
m E
urop
ean
Uni
on
fund
s; a
dditi
onal
fund
ing
from
loca
l gov
ernm
ent
dete
rmin
ed b
y se
rvic
es
prov
ided
Notspecified
Notspecified
Pro
gram
me
impl
emen
tatio
n is
ong
oing
; it i
s an
ticip
ated
that
50–
60 c
entr
es/p
roje
cts
will
be e
stab
lishe
d
Cen
tres
are
not
yet
in o
pera
tion;
it
is a
ntic
ipat
ed th
at 3
0–35
%
of s
mal
l reg
ions
, and
thei
r re
side
nts,
will
be c
over
ed b
y th
e pr
ogra
mm
e
Ast
hma
dise
ase
man
agem
ent
prog
ram
me
Prin
cipa
lly fu
nded
from
us
ual s
ourc
es w
ith n
urse
tr
aini
ng a
nd p
aym
ent a
s w
ell a
s eq
uipm
ent (
for
exam
ple,
spi
rom
eter
for
patie
nts)
and
prin
ted
mat
eria
ls fu
nded
by
pha
rmac
eutic
al
com
pani
es
Nur
se p
aym
ent
is c
over
ed b
y ph
arm
aceu
tical
co
mpa
nies
Notspecified
The
prog
ram
me
has
evol
ved
into
a fo
rmal
na
tiona
l net
wor
k of
ast
hma
nurs
es. B
y Ja
nuar
y 20
10, t
here
wer
e ar
ound
850
tr
aine
d as
thm
a nu
rses
acr
oss
Hun
gary
; th
e nu
mbe
r of
pul
mon
ary
disp
ensa
ries
is
arou
nd 1
60 (2
007)
Pre
cise
dat
a on
pop
ulat
ion
cove
rage
are
lack
ing;
in th
eory
th
e co
vera
ge s
houl
d be
100
%
Dia
bete
s ca
re
man
agem
ent
prog
ram
me
Prin
cipa
lly fu
nded
fro
m u
sual
sou
rces
w
ith p
harm
aceu
tical
an
d m
edic
al d
evic
es
com
pani
es c
over
ing
extr
a co
sts
incl
udin
g pa
ymen
t to
doct
ors
and
nurs
es, e
quip
men
t and
op
erat
iona
l cos
ts
Dia
bete
s sp
ecia
list
paym
ents
cov
ered
by
pha
rmac
eutic
al/
devi
ce c
ompa
nies
Notspecified
Ext
ent t
o w
hich
pro
gram
me
has
been
im
plem
ente
d by
spe
cial
ist d
iabe
tes
outp
atie
nt u
nits
is n
ot w
ell u
nder
stoo
d; in
20
08, t
here
wer
e 17
6 sp
ecia
list d
iabe
tes
units
, inc
ludi
ng 4
1 in
Bud
apes
t
App
roxi
mat
ely
20 0
00
patie
nts
with
type
2 d
iabe
tes
in B
udap
est a
re c
over
ed b
y ap
prox
imat
ely
40 s
peci
alis
t di
abet
es o
utpa
tient
uni
ts; n
ot
all u
nits
pro
vide
all
prog
ram
me
com
pone
nts
Italy
Inte
grat
ion,
m
anag
emen
t and
as
sist
ance
for
diab
etes
(IG
EA
)
Fund
ed fr
om u
sual
so
urce
s (S
SN
), co
mpl
emen
ted
by
natio
nal a
nd re
gion
al
fund
s ea
rmar
ked
for
prev
entio
n
Use
of i
ncen
tives
for
GP
s to
par
ticip
ate
varie
s am
ong
regi
ons
Phy
sici
ans:
ne
twor
king
, in
form
atio
n sh
arin
g, a
cces
s to
gu
idel
ines
, pee
r pr
essu
re
Impl
emen
tatio
n at
regi
onal
leve
l has
be
en a
gra
dual
pro
cess
; 35%
of G
P
prac
tices
in P
iedm
ont p
artic
ipat
e (2
009)
; as
a g
over
nmen
t-sp
onso
red
prog
ram
me
invo
lvem
ent o
f all
GP
s an
ticip
ated
Bec
ause
of g
radu
al
impl
emen
tatio
n of
the
prog
ram
me,
pat
ient
enr
olm
ent
is o
ngoi
ng; t
here
are
no
prec
ise
figuresontheprop
ortionofthe
popu
latio
n co
vere
d by
IGE
A
Table
3.4
con
td

51Access to health care services within and between countries of the European Union
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Italy
con
td“F
rom
On-
Dem
and
to
Pro
activ
e P
rimar
y C
are”
pro
gram
me,
Tu
scan
y
Fund
ed fr
om u
sual
so
urce
s (S
SN
) with
re
gion
al re
gula
tion
stip
ulat
ing
allo
catio
n of
reso
urce
s to
pro
ject
im
plem
enta
tion
of E
UR
8
883
000
over
of t
hree
ye
ars
GP
s: in
cent
ive
paym
ent d
epen
ding
on
leve
l of
invo
lvem
ent (
team
le
ad; p
artic
ipan
t) an
d ag
ains
t per
form
ance
(P
4P)
GP
: pro
gram
me
supp
orte
d by
Tuscany’sGP
asso
ciat
ion,
th
us c
reat
ing
peer
pre
ssur
e to
pa
rtic
ipat
e
Two-
stag
e im
plem
enta
tion:
initi
al p
hase
in
201
0 in
volv
ed th
e es
tabl
ishm
ent o
f ap
prox
imat
ely
50 m
odul
es w
ith a
dditi
on o
f m
odul
es o
ngoi
ng; f
urth
er im
plem
enta
tion
ongo
ing
App
roxi
mat
ely
50 m
odul
es
cove
r ap
prox
imat
ely
500
000
resi
dent
s; in
itial
ly ta
rget
ing
diab
etes
and
hea
rt fa
ilure
; ot
her
cond
ition
s to
be
adde
d;
expe
cted
cov
erag
e w
ith fu
ll im
plem
enta
tion:
1.1
milli
on w
ith
chro
nic
dise
ase
in T
usca
ny
Leon
ardo
pilo
t pr
ojec
t, P
uglia
Fund
ed jo
intly
by
regi
onal
fund
s, M
inis
try
of H
ealth
Spe
cial
P
rogr
amm
es fu
nd,
loca
l hea
lth s
yste
m a
nd
PfizerItaly(contributing
Info
rmaC
are™
sof
twar
e)
GP
s: lu
mp
sum
at
pro
ject
sta
rt,
to in
cent
iviz
e pa
rtic
ipat
ion,
plu
s va
riabl
e pa
ymen
t at
the
end,
bas
ed o
n pe
rform
ance
Notspecified
Tota
l of 8
5 G
Ps
in P
uglia
regi
on
(app
roxi
mat
ely
2.5%
of G
Ps
prac
tisin
g in
th
e re
gion
), w
orki
ng w
ith s
ome
30 c
are
man
ager
s
Pro
ject
cov
ered
just
und
er 1
160
patie
nts
for
a pr
ojec
t dur
atio
n of
18
mon
ths
at th
e Le
cce
AS
L
Raf
fael
lo p
roje
ct,
Mar
che
and
Abr
uzzo
Join
tly fu
nded
by
regi
onal
fu
nds
allo
cate
d to
hea
lth
care
; add
ition
al fu
nds
by
Min
istr
y of
Hea
lth S
peci
al
Pro
gram
mes
fund
and
cofinancingbyPfizerItaly
Fina
ncia
l inc
entiv
es
for
GP
s pa
rtic
ipat
ing
in th
e pr
ojec
t (no
t furtherspecified)
Notspecified
The
rese
arch
pro
ject
invo
lves
16
clus
ters
of
GP
s pa
rtic
ipat
ing
in th
e ex
perim
enta
l arm
of
the
stud
y
The
rese
arch
pro
ject
is li
mite
d toadefinedgroupofpatients
recr
uite
d fo
r pa
rtic
ipat
ion,
a
tota
l of 9
00 p
atie
nts
in th
e re
gion
s of
Mar
che
and
Abr
uzzo
Latv
ia
Gen
eral
prim
ary
heal
th c
are
syst
emFu
nded
from
usu
al
sour
ces
(taxa
tion)
Notspecified
Notspecified
Chr
onic
dis
ease
man
agem
ent e
mbe
dded
w
ithin
prim
ary
care
and
as
such
invo
lves
al
l GP
s; a
201
0 ev
alua
tion
of th
e pr
imar
y ca
re s
yste
m fo
und
low
leve
ls o
f qua
lity
of c
hron
ic c
are
as a
sses
sed
by re
gula
r ex
amin
atio
n of
pat
ient
s w
ith ty
pe 2
di
abet
es (2
5% o
f all
GP
s) o
r as
thm
a (5
%)
Chr
onic
dis
ease
man
agem
ent
embe
dded
with
in p
rimar
y ca
re a
nd th
eref
ore
cove
ring
virt
ually
the
entir
e po
pula
tion;
severefinancialpressures
have
, how
ever
, mea
nt th
at
appr
oxim
atel
y 45
% o
f the
po
pula
tion
cann
ot a
cces
s se
rvic
es b
ecau
se o
f req
uire
d co
-pay
men
ts (2
008)

52 Assessing chronic disease management in European health systems
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Lith
uani
a
Impr
ovin
g in
ters
ecto
ral
colla
bora
tion
Fund
ed fr
om u
sual
so
urce
s (S
HI),
soc
ial
care
fund
ed b
y lo
cal
gove
rnm
ent;
plan
s to
intr
oduc
e m
ore
coordinatedfinancing
of m
ultid
isci
plin
ary
team
ac
tiviti
es
Pat
ient
s: in
cent
ive
to re
mai
n in
the
com
mun
ity r
athe
r th
an b
ecom
ing
inst
itutio
naliz
ed
Notspecified
Prin
cipa
lly im
plem
ente
d in
all
60
mun
icip
aliti
es o
f Lith
uani
aP
reci
se d
ata
on p
opul
atio
n co
vera
ge a
re la
ckin
g; a
cces
s to
cas
e m
anag
emen
t var
ies
by c
ondi
tion
and
likel
y ac
ross
m
unic
ipal
ities
Clin
ical
gui
delin
esFu
nded
from
usu
al
sour
ces
(SH
I)G
Ps:
add
ition
al
paym
ent,
for
exam
ple,
for
confirm
ationofearly
diag
nose
d ca
ses
(for
exam
ple,
can
cer)
and
cert
ain
prio
ritiz
ed
serv
ices
Notspecified
In p
rinci
ple,
clin
ical
gui
delin
es s
houl
d be
im
plem
ente
d ac
ross
hea
lth s
ervi
ces
in
Lith
uani
a; p
reci
se d
ata
are
not a
vaila
ble
In p
rinci
ple,
all
diag
nose
d pa
tient
s sh
ould
be
cove
red
by
care
pla
ns b
ased
on
clin
ical
gu
idel
ines
Net
herla
nds
Mat
ador
DM
P/
Maa
stric
ht–
Heu
vella
nd
Usu
al s
ourc
es fo
r pr
ovid
ers
incl
udin
g G
Ps,
sp
ecia
lists
, die
titia
ns a
nd
othe
r he
alth
pro
fess
iona
ls;
spec
ialis
t dia
bete
s nu
rses
fu
nded
und
er p
revi
ous
Gen
eral
Exc
eptio
nal
Med
ical
Exp
ense
s A
ct
Notspecified
Notspecified
In 2
006,
a to
tal o
f 63
of 9
0 G
Ps
(70%
) in
the
Maa
stric
ht re
gion
par
ticip
ated
in th
e M
atad
or p
rogr
amm
e
In 2
006,
abo
ut 3
000
patie
nts
with
dia
bete
s in
the
Maa
stric
ht
regi
on w
ere
cove
red
by th
e M
atad
or p
rogr
amm
e
Prim
ary
care
gro
up
ZiO
(Maa
stric
ht–
Heu
vella
nd)
Fund
ed fr
om u
sual
so
urce
s (m
anda
tory
in
sura
nce)
, prin
cipa
l co
ntra
ctor
is th
e he
alth
in
sure
r C
oöpe
ratie
VG
Z on
the
basi
s of
a b
undl
ed
paym
ent c
ontr
act
Phy
sici
ans:
bun
dled
paym
entfordefined
pack
age
of c
are.
In
sure
r: to
neg
otia
te
low
pric
e fo
r ca
re
chai
n
Pre
senc
e of
an
acad
emic
hos
pita
l; profilingofZiOas
dire
ctor
of r
egio
nal
prim
ary
care
sec
tor
All
regi
onal
GP
s ar
e m
embe
rs o
f ZiO
H
euve
lland
and
as
such
par
ticip
ate
in th
e di
abet
es c
are
prog
ram
me
(just
und
er 9
0 G
Ps
by th
e en
d of
200
9); t
here
wer
e 97
ca
re g
roup
s in
Mar
ch 2
010
with
bun
dled
pa
ymen
t con
trac
t with
a h
ealth
insu
rer,
mos
tly fo
r di
abet
es c
are
By
the
end
of 2
009,
the
prog
ram
me
cove
red
som
e 76
00 p
atie
nts
with
type
2
diab
etes
in th
e M
aast
richt
–H
euve
lland
regi
on
Table
3.4
con
td

53Access to health care services within and between countries of the European Union
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Net
herla
nds
cont
dS
trok
e se
rvic
e D
elft
Fund
ed fr
om u
sual
so
urce
s: b
asic
hea
lth
insu
ranc
e (G
P a
nd
hosp
ital s
ervi
ces)
; AW
BZ
(for
exam
ple,
reha
bilit
atio
n ce
ntre
; nur
sing
hom
e) a
nd
WM
O (h
ome
care
); sh
ared
ca
re n
urse
is fu
nded
by
all
thre
e sc
hem
es
Notspecified
Notspecified
Follo
win
g th
e ex
perie
nces
of p
ilots
, the
go
vern
men
t act
ivel
y pr
omot
ed fu
rthe
r im
plem
enta
tion
thro
ugh
brea
kthr
ough
pr
ojec
ts a
nd b
ench
mar
king
of s
trok
e se
rvic
es; a
s re
sult,
by
2003
, eac
h re
gion
ha
d de
velo
ped
at le
ast o
ne s
trok
e se
rvic
e (a
tota
l of 6
9 in
200
3)
Pre
cise
num
ber
of p
atie
nts
rece
ivin
g ca
re w
ithin
str
oke
serv
ices
not
kno
wn;
how
ever
, ac
cord
ing
to th
e D
utch
H
eart
Fou
ndat
ion,
the
69
stro
ke s
ervi
ces
pres
ent i
n th
e N
ethe
rland
s si
nce
2003
are
di
strib
uted
to a
leve
l tha
t sho
uld
sufficientlycoverallstroke
patie
nts
(aro
und
191
000
in
2007
)
Nat
iona
l car
e st
anda
rd fo
r va
scul
ar r
isk
man
agem
ent
Fund
ed fr
om u
sual
so
urce
s (m
anda
tory
in
sura
nce)
on
the
basi
s of
a b
undl
ed p
aym
ent
cont
ract
Phy
sici
ans:
bun
dled
paym
entfordefined
pack
age
of c
are.
In
sure
r: to
neg
otia
te
low
pric
e fo
r ca
re
chai
n
Notspecified
Com
pare
d w
ith d
iabe
tes,
ther
e ar
e re
lativ
ely
few
car
e gr
oups
for
the
prov
isio
n of
vas
cula
r ris
k m
anag
emen
t; of
55
care
gr
oups
sur
veye
d in
ear
ly 2
010,
two
had
a bu
ndle
d pa
ymen
t con
trac
t in
plac
e fo
r va
scul
ar r
isk
man
agem
ent,
whe
reas
17
wer
e pr
epar
ing
to c
ontr
act
Pre
cise
num
ber
of p
atie
nts
rece
ivin
g ca
re w
ithin
vas
cula
r ris
k m
anag
emen
t not
kno
wn;
lim
ited
to th
ose
rece
ivin
g se
rvic
es th
roug
h th
e th
ree
esta
blis
hed
stan
dard
s
Sw
itzer
land
Dia
Bai
d di
abet
es
care
net
wor
kFu
nded
by
the
Can
ton
of V
aud
(app
roxi
mat
ely
50%
) and
from
car
e ac
tiviti
es c
harg
ed to
the
patie
nts
and
reim
burs
ed
by th
eir
heal
th in
sure
rs
(app
roxi
mat
ely
50%
)
No
Notspecified
Join
tly r
un b
y th
e A
ssoc
iatio
n de
s ré
seau
x desoinsdelaCôte(oneofthefivecare
netw
orks
ope
ratin
g in
the
Can
ton
of V
aud)
an
d tw
o re
gion
al h
ospi
tals
Dia
Bai
d w
as to
cov
er 3
0% o
f th
e es
timat
ed p
opul
atio
n w
ith
diab
etes
in th
e N
yon–
Mor
ges
regi
on (a
ppro
xim
atel
y 60
00).
By
2009
, 720
pat
ient
s (1
2%) h
ad
been
reac
hed
(app
roxi
mat
ely
100–
150
new
pat
ient
s pe
r ye
ar)
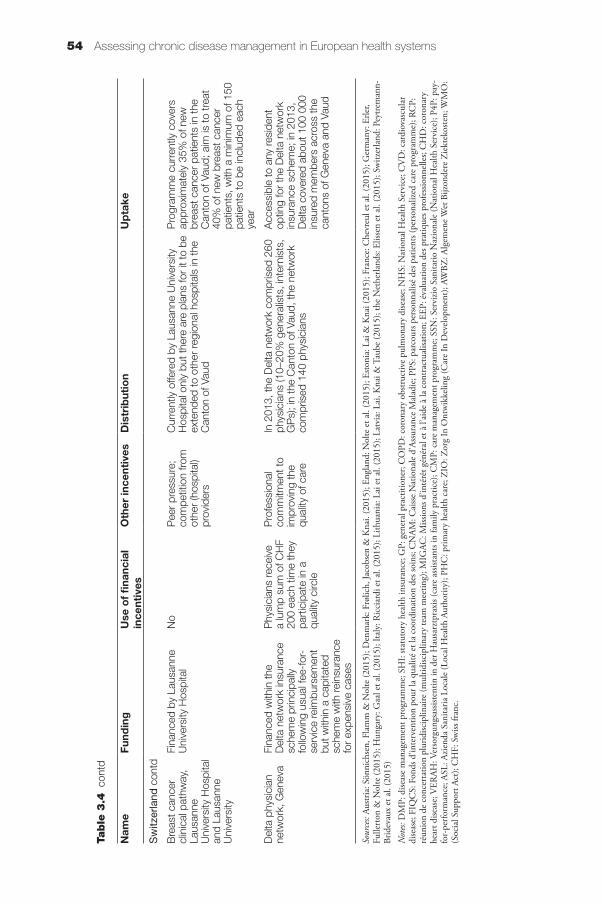
54 Assessing chronic disease management in European health systems
Nam
eFu
ndin
gU
se o
f fi
nanc
ial
ince
ntiv
esO
ther
ince
ntiv
esD
istr
ibut
ion
Up
take
Sw
itzer
land
con
td
Bre
ast c
ance
r cl
inic
al p
athw
ay,
Laus
anne
U
nive
rsity
Hos
pita
l an
d La
usan
ne
Uni
vers
ity
Fina
nced
by
Laus
anne
U
nive
rsity
Hos
pita
lN
oP
eer
pres
sure
; co
mpe
titio
n fro
m
othe
r (h
ospi
tal)
prov
ider
s
Cur
rent
ly o
ffere
d by
Lau
sann
e U
nive
rsity
H
ospi
tal o
nly
but t
here
are
pla
ns fo
r it
to b
e ex
tend
ed to
oth
er re
gion
al h
ospi
tals
in th
e C
anto
n of
Vau
d
Pro
gram
me
curr
ently
cov
ers
appr
oxim
atel
y 35
% o
f new
br
east
can
cer
patie
nts
in th
e C
anto
n of
Vau
d; a
im is
to tr
eat
40%
of n
ew b
reas
t can
cer
patie
nts,
with
a m
inim
um o
f 150
pa
tient
s to
be
incl
uded
eac
h ye
ar
Del
ta p
hysi
cian
ne
twor
k, G
enev
aFi
nanc
ed w
ithin
the
Del
ta n
etw
ork
insu
ranc
e sc
hem
e pr
inci
pally
fo
llow
ing
usua
l fee
-for
-se
rvic
e re
imbu
rsem
ent
but w
ithin
a c
apita
ted
sche
me
with
rein
sura
nce
for
expe
nsiv
e ca
ses
Phy
sici
ans
rece
ive
a lu
mp
sum
of C
HF
200
each
tim
e th
ey
part
icip
ate
in a
qu
ality
circ
le
Pro
fess
iona
l co
mm
itmen
t to
impr
ovin
g th
e qu
ality
of c
are
In 2
013,
the
Del
ta n
etw
ork
com
pris
ed 2
60
phys
icia
ns (1
0–20
% g
ener
alis
ts, i
nter
nist
s,
GP
s); i
n th
e C
anto
n of
Vau
d, th
e ne
twor
k co
mpr
ised
140
phy
sici
ans
Acc
essi
ble
to a
ny re
side
nt
optin
g fo
r th
e D
elta
net
wor
k in
sura
nce
sche
me;
in 2
013,
D
elta
cov
ered
abo
ut 1
00 0
00
insu
red
mem
bers
acr
oss
the
cant
ons
of G
enev
a an
d Va
ud
Sour
ces:
Austr
ia: S
önni
chse
n, F
lam
m &
Nol
te (2
015)
; Den
mar
k: F
rølic
h, Ja
cobs
en &
Kna
i. (2
015)
; Eng
land
: Nol
te e
t al.
(201
5); E
stoni
a: L
ai &
Kna
i (20
15);
Fran
ce: C
hevr
eul e
t al.
(201
5); G
erm
any:
Erle
r, Fu
llert
on &
Nol
te (2
015)
; Hun
gary
: Gaa
l et a
l. (2
015)
; Ita
ly: R
icci
ardi
et a
l. (2
015)
; Lith
uani
a: L
ai e
t al.
(201
5); L
atvi
a: L
ai, K
nai &
Tau
be (2
015)
; the
Net
herla
nds:
Eliss
en e
t al.
(201
5); S
witz
erla
nd: P
eytre
man
n-Br
idev
aux
et a
l. (2
015)
Not
es: D
MP:
dise
ase
man
agem
ent p
rogr
amm
e; S
HI:
statu
tory
hea
lth in
sura
nce;
GP:
gen
eral
pra
ctiti
oner
; CO
PD: c
oron
ary
obstr
uctiv
e pu
lmon
ary
dise
ase;
NH
S: N
atio
nal H
ealth
Ser
vice
; CV
D: c
ardi
ovas
cula
r di
seas
e; F
IQC
S: F
onds
d’in
terv
entio
n po
ur la
qua
lité
et la
coo
rdin
atio
n de
s soi
ns; C
NAM
: Cai
sse
Nat
iona
le d
’Ass
uran
ce M
alad
ie; P
PS: p
arco
urs p
erso
nnal
isé d
es p
atie
nts (
pers
onal
ized
care
pro
gram
me)
; RC
P:
réun
ion
de c
once
rtat
ion
plur
idisc
iplin
aire
(mul
tidisc
iplin
ary
team
mee
ting)
; MIG
AC: M
issio
ns d
’inté
rêt g
énér
al e
t à l’
aide
à la
con
trac
tual
isatio
n; E
EP: é
valu
atio
n de
s pra
tique
s pro
fess
ionn
elle
s; C
HD
: cor
onar
y he
art d
iseas
e; V
ERAH
: Ver
sorg
ungs
assis
tent
in in
der
Hau
sarz
tpra
xis (
care
ass
istan
ts in
fam
ily p
ract
ice)
; CM
P: c
are
man
agem
ent p
rogr
amm
e; S
SN: S
ervi
zio S
anita
rio N
azio
nale
(Nat
iona
l Hea
lth S
ervi
ce);
P4P:
pay
-fo
r-pe
rform
ance
; ASL
: Azie
nda
Sani
taria
Loc
ale
(Loc
al H
ealth
Aut
horit
y); P
HC
: prim
ary
heal
th c
are;
ZIO
: Zor
g In
Ont
wik
kelin
g (C
are
In D
evel
opm
ent);
AW
BZ: A
lgem
ene W
et B
ijzon
dere
Zie
ktek
oste
n; W
MO
: (S
ocia
l Sup
port
Act
); C
HF:
Sw
iss fr
anc.
Table
3.4
con
td

55Access to health care services within and between countries of the European Union
A number of approaches have been implemented at national level; these include: the care management programme and the Quality and Outcomes Framework in England; quality management in primary health care and management at the primary/secondary care interface in Estonia; disease management programmes in Germany; treatment (and financing) protocols in Hungary; and the improving intersectoral collaboration programme in Lithuania. Several approaches have been implemented at the regional level but are being (gradually) rolled out towards countrywide coverage. These have frequently, although not always, evolved from pilot or experimental projects. Examples include: the diabetes disease management programmes in Austria; the Sophia diabetes and asthma care programme and cancer networks in France; the asthma disease management programme and (possibly) the diabetes care programme in Hungary; the IGEA diabetes disease management programme in Italy; and care groups and standards as well as stroke services in the Netherlands. In Denmark, the regional DMPs and integrated clinical pathways are expected to cover the entire resident population in due course. Some approaches are fairly localized but are being considered for implementation elsewhere, such as the previously described COPA in Paris.
3.5 Components of chronic disease management
As noted in the Introduction, data collection on approaches to chronic disease management in Europe has sought to examine the extent to which these make use of the four components considered key to providing high-quality care for those with chronic health problems as identified by the chronic care model. These components are:
• self-management support
• delivery system design
• decision support
• clinical information systems.
For each of the approaches reviewed, Table 3.5 provides an overview of the nature and scope of these four interacting components. We find that the large majority provides some form of patient self-management support, although the level of support offered varies considerably, for example, involving the provision of information material, such as through brochures (for example, Integrated stroke care Upper Austria; Delta physician network, Switzerland), routine assessment of clinical indicators (for example, clinical guidelines in Lithuania) or access to coaching and face-to-face or telephone follow-up (for example, the Raffaello project, Italy), lifestyle intervention training (for example, the

56 Assessing chronic disease management in European health systems
Matador diabetes disease management programme, the Netherlands) and counselling techniques (for example, National care standard for vascular risk management, the Netherlands). Most approaches involve patients in the development of a care or treatment plan and goal setting, and provide regular assessment of patient needs and problems. The extent to which these support mechanisms are implemented in practice is, however, often unclear.
In the majority of cases, self-management support is provided by health professionals including physicians (for example, diabetes disease management programmes in Austria and Germany; chronic disease management at the primary/secondary care interface in Estonia), or, more frequently, trained nurses (for example, selected integrate care pilots in England; quality management in primary care in Estonia; the Sophia diabetes and asthma care programme and provider networks in France; Care Coordination Pilot, asthma disease and diabetes care management programmes in Hungary; IGEA, Leonardo and Raffaello projects in Italy; care groups and stroke services in the Netherlands; the breast cancer clinical pathway in Lausanne, Switzerland). Self-management support provided by others including lay groups appears uncommon; examples include selected projects implemented within the Partnership for Older People Project set-up in England.
Most approaches reviewed here involve some form of delivery system design, but as with self-management support the nature and scope of related strategies varies. Common elements include a clear definition of roles, the development of (individualized) care or treatment pathways and patient follow-up. Several approaches use case-finding or risk stratification (for example, care coordination/interface management Styria, Austria; Partnership for Older People Project and integrated care pilots, England; France; selected integrated care contracts, Germany; Care Coordination Pilot, Hungary; Raffaello project, Italy; care groups, the Netherlands). These approaches also tend to involve case management, or indeed constitute dedicated case management approaches, such as within the Partnership for Older People Project and integrated care pilots in England; the COPA Coordinates of professional care for the Elderly in France; and the improving intersectoral collaboration approach in Lithuania, with case management elements also incorporated within selected GP contracts in Germany; the Care Coordination Pilot in Hungary; the “From On-Demand to Proactive Primary Care” programme in Tuscany, Italy; and the Matador diabetes disease management programme in the Netherlands.
These strategies are commonly supported by decision support tools, such as guidelines and protocols, developed at organizational, regional, national or international level with some strategies also incorporating training in translating national or regional guidelines to the local level, as, for example,

57Access to health care services within and between countries of the European Union
Table
3.5
C
ompo
nent
s of
chr
onic
dis
ease
man
agem
ent u
sed
in 1
2 E
urop
ean
coun
trie
s
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Aus
tria
‘Therapie’
aktiv
dis
ease
m
anag
emen
t pr
ogra
mm
e
Edu
catio
n th
roug
h gr
oup
inst
ruct
ion;
invo
lvem
ent i
n go
al
sett
ing
and
timel
ines
, with
agr
eed
targ
ets
sign
ed jo
intly
; reg
ular
follo
w-
up
Pat
ient
man
agem
ent t
hrou
gh
coor
dina
ting
phys
icia
n w
ith
cond
ition
s fo
r re
ferr
al b
etw
een
leve
ls o
f car
e; re
gula
r pa
tient
fo
llow
-up
(in p
erso
n)
Car
e pa
thw
ays
deve
lope
d by
th
e A
ustr
ian
Soc
iety
of D
iabe
tes
(ÖD
G);
man
dato
ry p
rovi
der
trai
ning
pr
ogra
mm
es fo
r D
MP
phy
sici
ans;
an
nual
adv
ance
d tr
aini
ng s
essi
ons
and
qual
ity c
ircle
s
Sta
ndar
dize
d do
cum
enta
tion
of c
linic
al
and
diag
nost
ic m
easu
res
and
trea
tmen
t; na
tionw
ide
mon
itorin
g is
pla
nned
, but
re
gula
r fe
edba
ck re
port
s to
par
ticip
atin
g ph
ysic
ians
hav
e ye
t to
be e
stab
lishe
d
Inte
grat
ed s
trok
e ca
re U
pper
A
ustr
ia
Info
rmat
ion
(str
oke
awar
enes
s ca
mpa
igns
, bro
chur
es d
istr
ibut
ed
in G
P p
ract
ices
and
hos
pita
ls,
dedi
cate
d w
ebsi
te, t
arge
ted
lect
ures
)
Dev
elop
men
t of i
nteg
rate
d ca
re
path
way
s; re
gula
r (p
eer
grou
p)
meetings;d
efinedrolesfor
part
icip
atin
g pr
ovid
ers
Pra
ctic
e gu
idel
ines
(for
exa
mpl
e,
stro
ke c
heck
list f
or G
Ps)
; de
velo
pmen
t of i
nteg
rate
d ca
re
path
way
s ba
sed
on e
vide
nce-
base
d gu
idel
ines
Com
mon
dat
a w
areh
ouse
that
com
pile
s in
form
atio
n on
str
oke
patie
nts
colle
cted
by
par
ticip
atin
g or
gani
zatio
ns; p
rovi
der
feed
back
to m
onito
r an
d im
prov
e pr
oces
ses
and
outc
omes
Car
e co
ordi
natio
n/in
terfa
ce
man
agem
ent
Sty
ria
Invo
lvem
ent o
f pat
ient
s an
d th
eir
care
give
rs in
pla
nnin
g of
dis
char
ge
and
subs
eque
nt c
are
arra
ngem
ents
in
clud
ing
info
rmat
ion
and
prac
tical
as
sist
ance
, suc
h as
arr
ange
men
t of
devi
ces
and
serv
ices
Car
e co
ordi
nato
r ac
ts a
s ke
y co
ntac
t for
the
patie
nt, h
ospi
tal
andthepatient’sGP;regular
mee
tings
of t
he c
oord
inat
or w
ith
prov
ider
s ou
tsid
e ho
spita
l; ca
se-
finding
Che
cklis
t to
iden
tify
patie
nts
requ
iring
sup
port
by
the
care
m
anag
er; u
se o
f the
BR
AS
S in
dex
inGrazforcase-finding
Notspecified
Am
bula
tory
afte
r-ca
re o
f str
oke
patie
nts,
Sal
zbur
g
Acc
ess
to te
am o
f occ
upat
iona
l th
erap
ists
, spe
ech
ther
apis
ts a
nd
phys
ioth
erap
ists
in o
ne-t
o-on
e an
d gr
oup
sett
ings
; soc
ial a
ctiv
ities
; in
form
atio
n th
roug
h ev
ents
Team
of t
hera
pist
s le
d by
sen
ior
ther
apis
t and
phy
sici
an in
eac
h di
stric
t act
ing
as p
rogr
amm
e le
ad; r
egul
ar te
am m
eetin
gs a
nd
mee
tings
of p
roje
ct le
ader
s
Con
tinui
ng e
duca
tion
and
trai
ning
of
ther
apis
ts; a
cces
s fo
r th
erap
ists
to
mon
thly
gro
up s
uper
visi
on
mee
tings
Notspecified
Kar
diom
obil
– H
ome
care
for
patie
nts
with
ch
roni
c he
art
failu
re
Edu
catio
n ab
out t
he d
isea
se,
inst
ruct
ion
in s
elf-
mon
itorin
g an
d in
han
dlin
g em
erge
ncy
situ
atio
ns
by tr
aine
d nu
rse;
follo
w-u
p as
sess
men
t of p
atie
nt s
elf-
man
agem
ent c
ompe
tenc
es a
nd
need
s
Sup
port
of p
atie
nts
alon
g definedprotocolofthree
hom
e vi
sits
by
trai
ned
nurs
e;
nurs
e al
so a
cts
as k
ey p
oint
of
cont
act f
or p
atie
nts
and
as c
are
coor
dina
tor
in c
olla
bora
tion
with
G
P a
nd s
peci
alis
t out
patie
nt
clin
ic
Con
tinui
ng e
duca
tion
for
Kar
diom
obil
nurs
es o
n as
pect
s of
med
icat
ion,
qua
lity
assu
ranc
e,
com
mun
icat
ion
with
clin
icia
ns,
Iinfo
rmat
ion
tech
nolg
y
Not
inte
gral
par
t of t
he p
rogr
amm
e; p
lans
to
impl
emen
t an
elec
tron
ic in
form
atio
n sy
stem
that
allo
ws
for
the
shar
ing
of
patie
nt d
ata
with
in th
e pr
ogra
mm
e

58 Assessing chronic disease management in European health systems
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Den
mar
k
SIK
S p
roje
ct –
inte
grat
ed e
ffort
fo
r pe
ople
livi
ng
with
chr
onic
di
seas
e
Edu
catio
n an
d re
gula
r do
cum
enta
tion
of s
elf-
man
agem
ent
need
s an
d ac
tiviti
es; i
nvol
vem
ent i
n de
velo
ping
indi
vidu
aliz
ed tr
eatm
ent
plan
s an
d go
al s
ettin
g; a
cces
s to
phy
sica
l exe
rcis
e in
terv
entio
n;
info
rmat
ion
Cleardefinitionofro
lesand
task
s of
par
ticip
atin
g he
alth
pr
ofes
sion
als;
mul
tidis
cipl
inar
y te
am s
uppo
rts
the
deliv
ery
of re
habi
litat
ion;
regu
lar
patie
nt fo
llow
-up;
regu
lar
inte
rorg
aniz
atio
nal m
eetin
gs
Evi
denc
e-ba
sed
clin
ical
gui
delin
es
deve
lope
d by
SIK
S w
orki
ng
grou
ps; r
egul
ar p
rovi
der
educ
atio
n an
d tr
aini
ng
Mon
itorin
g of
pra
ctic
e te
am p
erfo
rman
ce;
syst
emat
ic c
olle
ctio
n of
clin
ical
and
ot
her
data
; use
of m
unic
ipal
IT p
latfo
rm
Sun
dhed
spor
tal;
prov
ider
s m
ay o
pera
te
thei
r ow
n da
taba
se
Reg
iona
l dis
ease
m
amag
emen
t pr
ogra
mm
es
(gen
eric
mod
el
as p
ropo
sed
in
2008
by
the
then
N
atio
nal B
oard
of
Hea
lth)
Structured(disease-specificand
gene
ral)
educ
atio
n; in
form
atio
n;
invo
lvem
ent i
n de
velo
ping
car
e tr
eatm
ent p
lan
and
goal
set
ting
incl
udin
g ag
reei
ng ti
mel
ine
and
met
hods
for
eval
uatio
n of
goa
ls;
regu
lar
asse
ssm
ent a
nd fo
llow
-up
of p
robl
ems
and
need
s
Clearlydefinedroles
of p
artic
ipat
ing
heal
th
prof
essi
onal
s; d
evel
opm
ent o
f in
divi
dual
ized
inte
grat
ed c
are
plan
s; G
P is
prin
cipa
l car
e co
ordi
nato
r w
ith s
uppo
rt b
y sp
ecia
list a
nd b
y ca
se m
anag
er
(usu
ally
spe
cial
ist n
urse
) for
co
mpl
ex p
atie
nts;
regu
lar
follo
w-
up
Clin
ical
gui
delin
es d
evel
oped
by
a w
orki
ng g
roup
and
bas
ed o
n na
tiona
l and
inte
rnat
iona
l clin
ical
gu
idel
ines
; pro
vide
r tr
aini
ng in
re
leva
nt d
isci
plin
es o
f chr
onic
di
seas
e, in
clud
ing
lifes
tyle
in
terv
entio
ns, s
elf-
man
agem
ent
supp
ort a
nd in
edu
catio
n co
mpe
tenc
ies
and
mot
ivat
ion
tech
niqu
es
Nat
iona
l adm
inis
trat
ive
regi
ster
s an
d cl
inic
al q
ualit
y da
taba
ses
allo
w fo
r da
ta
shar
ing
and
com
mun
icat
ion,
as
wel
l as
con
sist
ent d
ata
colle
ctio
n; q
ualit
y m
onito
ring
acco
rdin
g to
the
Dan
ish
Qua
lity
Mod
el (D
DK
M) a
nd th
e N
atio
nal
Indi
cato
r S
yste
m
Inte
grat
ed c
linic
al
path
way
sNotspecified
Cleardefinitionofresponsibilities
(dia
gnos
is, t
reat
men
t, re
habi
litat
ion)
; dev
elop
men
t of
indi
vidu
aliz
ed c
are
plan
s;
desi
gnat
ed c
are
coor
dina
tor;
re
gula
r fo
llow
-up
with
inte
rval
s de
pend
ing
on c
ondi
tion
Nat
iona
l clin
ical
gui
delin
esFr
om 2
012,
the
Sta
te S
erum
Inst
itute
(S
SI)
coor
dina
tes
the
Nat
iona
l Pat
ient
R
egis
try
and
the
Can
cer
Reg
iste
r;
establishedspecificcodesforthe
mon
itorin
g of
the
inte
grat
ed c
linic
al
path
way
s, w
ith re
port
ing
mad
e m
anda
tory
for
Dan
ish
hosp
itals
from
O
ctob
er 2
012.
Sim
ilar
code
s w
ere
also
est
ablis
hed
for
inte
grat
ed c
linic
al
path
way
s fo
r he
art d
isea
se; r
epor
ting
of
thes
e be
cam
e m
anda
tory
in J
uly
2013
Table
3.5
co
ntd

59Access to health care services within and between countries of the European Union
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Eng
land
Com
mun
ity
mat
ron
Edu
catio
n pr
ovid
ed b
y sp
ecia
list
nurs
e; in
volv
emen
t in
deve
lopm
ent
of c
are
plan
and
goa
ls; r
egul
ar
asse
ssm
ent a
nd d
ocum
enta
tion
of
need
s an
d ac
tiviti
es
Cleardefinitionofro
leswith
spec
ialis
t nur
se a
s ca
se
man
ager
, coo
rdin
atin
g w
ith
GP,
com
mun
ity a
nd s
ocia
l ca
re s
ervi
ces;
med
icin
es
managem
ent;case-findingusing
stan
dard
ized
ris
k as
sess
men
t
Trai
ning
of n
urse
s w
ithin
nat
iona
l co
mpe
tenc
y fra
mew
orks
and
gu
idan
ce
Mayincludeuseofriskstratification
tool
s to
iden
tify
patie
nts
at r
isk
of
reho
spita
lizat
ion;
ava
ilabi
lity
of IT
sup
port
/in
form
atio
n sh
arin
g va
riabl
e ac
ross
co
mm
issi
ners
Qua
lity
and
outc
omes
fra
mew
ork
n/a
Varie
s at
pra
ctic
e le
vel;
may
in
clud
e re
gula
r st
aff m
eetin
gs,
patie
nt fo
llow
-up
(usu
ally
by
phon
e or
pos
t), a
nd m
edic
ines
m
anag
emen
t
Use
of c
linic
al g
uide
lines
and
tr
aini
ng o
f pra
ctic
e nu
rses
on
the
basi
s of
indi
vidu
al le
arni
ng p
lans
Aut
omat
ed m
echa
nism
for
the
colle
ctio
n of
dat
a fo
r cl
inic
al q
ualit
y in
dica
tors
from
G
P e
lect
roni
c m
edic
al re
cord
s, in
clud
ing
dise
ase
regi
stra
tion
and
perfo
rman
ce
mon
itorin
g, th
roug
h na
tiona
l IT
syst
em;
data
ext
ract
s ar
e ac
cess
ible
to th
e H
ealth
an
d S
ocia
l Car
e In
form
atio
n C
entr
e to
su
ppor
t pub
licat
ion
Par
tner
ship
for
olde
r pe
ople
pr
ojec
t (P
OP
P)
Varie
d: in
volv
emen
t of o
lder
peo
ple
in p
roje
ct d
evel
opm
ent,
oper
atio
n an
d ev
alua
tion;
pee
r su
ppor
t, in
clud
ing
EE
P; s
taff
and
volu
ntee
rs
actin
g as
“na
viga
tors
” to
hel
ping
ol
der
peop
le th
roug
h th
e sy
stem
; fo
llow
-up;
exp
ert c
arer
pro
gram
me;
Varie
d: c
omm
unity
-bas
ed m
ulti-
agen
cy te
ams;
dev
elop
men
t of
inte
grat
ed c
are
path
way
s;
mul
tidis
cipl
inar
y he
alth
and
so
cial
car
e te
ams;
des
igna
ted
role
s, in
clud
ing
com
mun
ity
mat
rons
and
cas
e w
orke
rs
(soc
ial/“
hybr
id”
wor
kers
); ca
se-
finding;regularfollow-up
Varie
d: h
ealth
or
soci
al c
are
staf
f tr
aini
ng; v
olun
teer
trai
ning
; ski
ll sh
arin
g an
d tr
aini
ng; a
cces
s to
sp
ecia
list e
xper
tise
Varie
d: in
tegr
ated
IT s
yste
ms
conn
ectin
g pr
imar
y an
d se
cond
ary
care
, or
prim
ary
and
soci
al/c
omm
unity
car
e; u
se o
f telehealthtechnologyandcase-finding
softw
are;
use
of w
irele
ss te
chno
logy
for
mob
ile u
nits
IInte
grat
ed c
are
pilo
tsVa
ried:
pat
ient
edu
catio
n an
d pr
ovis
ion
of s
elf-
man
agem
ent t
ools
by
sen
ior
nurs
es; t
rain
ing
in s
elf-
man
agem
ent o
f med
icin
es
Varie
d: d
evel
opm
ent o
f car
e pa
thw
ays;
man
aged
dis
char
ge;
case
man
agem
ent,
led
by
seni
or/s
peci
alis
t nur
ses;
use
of
inte
grat
ed c
omm
unity
team
s pr
ovid
ing
a si
ngle
poi
nt o
f ac
cess
for
patie
nts
Varie
d: h
ealth
or
soci
al c
are
prof
essi
onal
trai
ning
, par
ticul
arly
re
gard
ing
gene
ric s
kills
that
en
able
mor
e ef
fect
ive
wor
k on
m
ultid
isci
plin
ary
team
s or
in a
ra
pid-
resp
onse
cap
acity
; acc
ess
to s
peci
alis
t exp
ertis
e
Varied:case-findingsoftware;afewsites
aim
ed to
est
ablis
h a
sing
le in
tegr
ated
IT
sys
tem
for
prim
ary
and
com
mun
ity
care
, whi
le o
ther
s m
ake
use
of te
leca
re
serv
ices
and
rem
ote
heal
th m
onito
ring

60 Assessing chronic disease management in European health systems
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Est
onia
Qua
lity
man
agem
ent i
n pr
imar
y he
alth
ca
re
Edu
catio
n pr
ovid
ed b
y G
P/f
amily
nu
rse;
invo
lvem
ent i
n de
velo
pmen
t of
car
e pl
an; r
egul
ar a
sses
smen
t an
d fo
llow
-up;
add
ition
al s
uppo
rt
by h
ome
care
nur
se o
r so
cial
w
orke
r w
here
nec
essa
ry
Case-finding;d
evelop
ment
of in
divi
dual
ized
car
e an
d tr
eatm
ent p
lans
; rou
tine
follo
w-
up
Evi
denc
e-ba
sed
diag
nosi
s,
trea
tmen
t and
dis
ease
m
anag
emen
t gui
delin
es; p
rovi
der
educ
atio
n as
par
t of c
ontin
uing
pr
ofes
sion
al d
evel
opm
ent i
n pr
imar
y an
d sp
ecia
list c
are;
qua
lity
man
agem
ent a
ctiv
ities
GP
pra
ctic
e in
form
atio
n sy
stem
ac
cord
ing
to m
anda
tory
gui
delin
es
incl
udin
g el
ectr
onic
med
ical
reco
rds,
bo
okin
g an
d re
min
der
syst
ems;
IT
syst
em li
nked
to c
ount
ryw
ide
patie
nt
and
trea
tmen
t sys
tem
of a
ll he
alth
car
e pr
ovid
ers
(ava
ilabl
e on
line
from
200
9)
Chr
onic
dis
ease
m
anag
emen
t at
the
prim
ary/
seco
ndar
y ca
re
inte
rface
Edu
catio
n (s
peci
alis
t); in
volv
emen
t in
dev
elop
men
t of c
are
plan
; re
gula
r as
sess
men
t and
follo
w-u
p;
men
torin
g/pe
er s
uppo
rt th
roug
h pa
tient
ass
ocia
tions
(for
exa
mpl
e,
multiplesclerosis,P
arkinson’s
dise
ase)
; sup
port
at h
ome
by n
urse
or
soc
ial w
orke
r w
here
nec
essa
ry
Case-finding;d
evelop
ment
of in
divi
dual
ized
car
e an
d tr
eatm
ent p
lans
; rou
tine
follo
w-
up
Evi
denc
e-ba
sed
diag
nosi
s,
trea
tmen
t and
dis
ease
m
anag
emen
t gui
delin
es; p
rovi
der
educ
atio
n as
par
t of c
ontin
uing
pr
ofes
sion
al d
evel
opm
ent i
n pr
imar
y an
d sp
ecia
list c
are
GP
pra
ctic
e in
form
atio
n sy
stem
ac
cord
ing
to m
anda
tory
gui
delin
es
incl
udin
g el
ectr
onic
med
ical
reco
rds,
bo
okin
g an
d re
min
der
syst
ems;
IT
syst
em li
nked
to c
ount
ryw
ide
patie
nt
and
trea
tmen
t sys
tem
of a
ll he
alth
car
e pr
ovid
ers
(ava
ilabl
e on
line
from
200
9)
Fran
ceP
rovi
der
netw
orks
Fo
r ex
ampl
e,
(dia
bete
s ne
twor
ks):
RE
VE
SD
IAB
Info
rmat
ion
and
educ
atio
n (fo
r ex
ampl
e, d
iet);
coa
chin
g by
nu
rses
; inv
olve
men
t in
deve
lopi
ng
trea
tmen
t pla
n to
war
ds a
form
al
agre
emen
t bet
wee
n pa
tient
and
ne
twor
k; re
gula
r as
sess
men
t and
fo
llow
-up
incl
udin
g pa
tient
logb
ook
com
plet
ed w
ith d
octo
r co
nsul
ted
Cleardefinitionofro
les
of m
ultid
isci
plin
ary
heal
th
care
team
; dev
elop
men
t of
indi
vidu
aliz
ed c
are
plan
by
core
te
am; d
iscu
ssio
n fo
rum
and
qu
ality
circ
les;
regu
lar
follo
w-u
p
Evi
denc
e-ba
sed
guid
elin
es a
nd
care
pro
toco
ls; p
rovi
der
trai
ning
w
ithin
con
tinuo
us m
edic
al
educ
atio
n
Sha
red
info
rmat
ion
syst
em in
volv
ing
a da
taba
se c
olle
ctin
g ro
utin
e cl
inic
al
indi
cato
rs a
nd u
sed
for
eval
uatio
n an
d qu
ality
con
trol
; pat
ient
-hel
d ca
re fo
lder
to
sup
port
mon
itorin
g; s
ome
syst
ems
oper
ate
rem
inde
r fu
nctio
ns; G
Ps
do n
ot
have
rout
ine
acce
ss to
cen
tral
ized
pat
ient
in
form
atio
n
Coo
rdin
atio
n of
pr
ofes
sion
al c
are
for
the
Eld
erly
(C
OPA
)
Invo
lvem
ent i
n de
velo
ping
tr
eatm
ent p
lan
and
goal
set
ting
Clearlydefinedroleswith
trai
ned
nurs
e as
cas
e m
anag
er;
deve
lopm
ent o
f ind
ivid
ualiz
ed
care
pla
n; o
ccas
iona
l m
ultid
isci
plin
ary
team
mee
tings
(G
P, g
eria
tric
ian,
car
egiv
ers)
; case-finding
Pro
vide
r tr
aini
ng in
ger
iatr
ic
asse
ssm
ent (
Inte
rRA
I) to
info
rm
careplanandcase-finding
Dat
abas
e fo
r ev
alua
tion
and
docu
men
tatio
n; to
be
inte
grat
ed in
the
clin
ical
rout
ine
in th
e fu
ture
Table
3.5
co
ntd

61Access to health care services within and between countries of the European Union
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Fran
ce c
ontd
Spe
cific
pro
gram
mes
Sop
hia
diab
etes
an
d as
thm
a ca
re
prog
ram
me
(by
SH
I)
Adv
ice
and
info
rmat
ion
on s
elf-
man
agem
ent o
f dis
ease
and
he
alth
beh
avio
ur; f
acilit
atin
g co
mm
unic
atio
n w
ith h
ealth
pr
ofes
sion
als;
acc
ess
to d
edic
ated
pr
ogra
mm
e w
ebsi
te
Cleardefinitionofro
les:regular
indi
vidu
aliz
ed (n
eed-
base
d)
phon
e in
terv
entio
n by
trai
ned
nurs
e w
ith G
P re
mai
ning
car
e coordinator;stratificationof
patie
nts
acco
rdin
g to
ris
k to
det
erm
ine
frequ
ency
of
inte
rven
tion
Evi
denc
e-ba
sed
guid
elin
esRiskstratificationsoftw
are
Hea
lth A
ctio
n by
Te
ams
of S
elf-
empl
oyed
Hea
lth
Pro
fess
iona
ls
(AS
ALE
E)
Edu
catio
n ab
out d
isea
se p
rovi
ded
by tr
aine
d nu
rse
Clearlydefinedrolesforstaff
with
nur
ses
resp
onsi
ble
for
scre
enin
g fo
r co
gniti
ve p
robl
ems
and
card
iova
scul
ar r
isk
fact
ors
in in
divi
dual
s ov
er 7
5 ye
ars
Notspecified
Rem
inde
r sy
stem
s on
pat
ient
not
es a
nd
mon
itorin
g sy
stem
s
Hos
pita
l di
scha
rge
prog
ram
for
hear
t fa
ilure
pat
ient
s (P
RA
DO
)
Wee
kly
hom
e vi
sit b
y nu
rse
durin
g tw
o m
onth
s to
del
iver
pat
ient
ed
ucat
ion;
sup
port
bro
chur
es fo
r pa
tient
s
Org
aniz
atio
n an
d co
ordi
natio
n of
follo
w-u
p co
nsul
tatio
ns b
y th
e di
scha
rge
man
ager
Car
e al
gorit
hms
for
the
part
icip
atin
g he
alth
pro
fess
iona
lsP
aper
-bas
ed lo
gboo
k fo
r th
e pa
tient
, co
ntai
ning
phy
siol
ogic
al in
form
atio
n to
be
shar
ed a
mon
g al
l hea
lth p
rofe
ssio
nals
Specificpayment
base
d on
pub
lic
heal
th o
bjec
tives
(R
OS
P)
Not
app
licab
leN
ot a
pplic
able
Ince
ntiv
es fo
r se
t-up
of
pres
crip
tion
aid
softw
are;
(ind
irect
) ad
here
nce
to g
uide
lines
via
the
qual
ity in
dica
tors
for
rem
uner
atio
n
Ince
ntiv
es fo
r in
frast
ruct
ure
rela
ted
to e
lect
roni
c pa
tient
reco
rd a
nd d
ata
tran
smis
sion
(mos
tly w
ith S
HI)
Mea
sure
s of
the
2003
–200
7 C
ance
r P
lan
Pro
toco
l fo
r di
seas
e co
mm
unic
atio
n an
d pr
omot
ion
of
shar
ed d
ecis
ion-
mak
ing
(Dis
posi
tif
d’annonce)
Acc
ess
to d
edic
ated
tim
e in
form
ing
abou
t the
illn
ess
and
supp
ort;
invo
lvem
ent i
n de
cisi
on-m
akin
g;
acce
ss to
psy
chol
ogic
al a
nd s
ocia
l su
ppor
t; re
gula
r as
sess
men
t of
patie
nt n
eeds
; fol
low
-up
Rolesofstaffareclearlydefined
with
sup
port
pro
vide
d by
nur
se,
psyc
holo
gist
or
soci
al w
orke
r;
pers
onal
ized
follo
w-u
p
Nat
iona
l rec
omm
enda
tions
on
patie
nt c
omm
unic
atio
n de
velo
ped
by th
e H
AS
/INC
a
Sys
tem
s ha
ve b
een
esta
blis
hed
to
enab
le s
harin
g of
can
cer
patie
nt re
cord
s (D
ossi
er c
omm
uniq
uant
en
canc
érol
ogie
); ho
wev
er, i
mpl
emen
tatio
n ha
s va
ried
acro
ss re
gion
s

62 Assessing chronic disease management in European health systems
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Fran
ceM
easu
res
of th
e 20
03–2
007
Can
cer
Pla
n co
ntd
Mul
tidis
cipl
inar
y te
am m
eetin
g (R
CP
)
As
impl
emen
ted
with
in d
ispo
sitif
d’annonce
Dev
elop
men
t of i
ndiv
idua
lized
ca
re p
lans
(PP
S);
staf
f rol
es a
re
clearlydefinedwithmédecin
refe
rent
(ref
errin
g do
ctor
) pr
epar
ing
draf
t tre
atm
ent p
lan
for
disc
ussi
on w
ith te
am; w
eekl
y te
am m
eetin
gs fo
r ea
ch c
ance
r sp
ecia
lity
and
ever
y tw
o w
eeks
to
dis
cuss
indi
vidu
al c
ance
r pa
tient
s
Reg
iona
l gui
delin
es/
reco
mm
enda
tions
on
canc
er
prac
tice
base
d on
nat
iona
l re
com
men
datio
ns is
sued
by
HA
S/
INC
a
Sys
tem
s ha
ve b
een
esta
blis
hed
to
enab
le s
harin
g of
can
cer
patie
nt re
cord
s (D
ossi
er c
omm
uniq
uant
en
canc
érol
ogie
); ho
wev
er, i
mpl
emen
tatio
n ha
s va
ried
acro
ss re
gion
s
Reg
iona
l can
cer
netw
orks
As
impl
emen
ted
with
in d
ispo
sitif
d’annonce
As
impl
emen
ted
with
in R
CP
; in
addi
tion:
regu
lar
(mon
thly,
six
-m
onth
ly) m
eetin
gs o
f pro
vide
rs
in th
e fo
rm o
f wor
ksho
ps fo
r ea
ch g
roup
of s
peci
altie
s of
regi
onal
impo
rtan
ce, f
or
exam
ple,
var
iatio
n in
pra
ctic
e,
regi
onal
gui
delin
es
As
impl
emen
ted
with
in R
CP
Sys
tem
s ha
ve b
een
esta
blis
hed
to
enab
le s
harin
g of
can
cer
patie
nt re
cord
s (D
ossi
er c
omm
uniq
uant
en
canc
érol
ogie
); ho
wev
er, i
mpl
emen
tatio
n ha
s va
ried
acro
ss re
gion
s
Loca
l can
cer
or
loca
l mul
tiple
pa
thol
ogy
netw
orks
As
impl
emen
ted
with
in d
ispo
sitif
d’annonce
Par
ticip
atio
n of
GP
s in
m
ultid
isci
plin
ary
cons
ulta
tion;
de
velo
pmen
t of m
onito
ring
plan
by
GP
cov
erin
g ep
isod
es
betw
een
hosp
italiz
atio
ns,
trea
tmen
t at h
ome
and
mon
itorin
g af
ter-
care
As
impl
emen
ted
with
in R
CP
with
an
ele
men
t of p
rovi
der
educ
atio
n at
loca
l lev
el (G
Ps,
hom
e ca
re
nurs
es) a
s m
eans
to im
plem
ent
regi
onal
gui
delin
es; a
cces
s to
sp
ecia
list e
xper
tise
in h
ospi
tal
Acc
ess
of G
Ps
to e
lect
roni
c pa
tient
re
cord
s of
par
ticip
atin
g pa
tient
s
Table
3.5
co
ntd

63Access to health care services within and between countries of the European Union
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Ger
man
y
Dis
ease
m
anag
emen
t pr
ogra
mm
es
Edu
catio
n pr
ogra
mm
e in
gro
up
sess
ions
; inv
olve
men
t in
agre
eing
tr
eatm
ent g
oals
; reg
ular
follo
w-u
p,
with
pat
ient
rem
inde
rs fo
r m
isse
d se
ssio
ns; s
ome
SH
I fun
ds a
lso
offe
r te
leph
one
serv
ices
to fu
rthe
r su
ppor
t the
ir m
embe
rs p
artic
ipat
ing
in D
MP
s
Coo
rdin
atio
n of
thre
e ca
re
levelsaccordingto
specified
cond
ition
s fo
r re
ferr
al b
etw
een
leve
ls o
f car
e; re
gula
r pa
tient
fo
llow
-up
Evi
denc
e-ba
sed
guid
elin
es a
s de
velo
ped
by th
e G
erm
an N
etw
ork
for
Evi
denc
e-ba
sed
Med
icin
e an
d InstituteforQualityandEfficiency
in H
ealth
Car
e; p
artic
ipat
ing
physicianshavetomeetd
efined
trai
ning
sta
ndar
ds a
nd m
ay h
ave
to a
tten
d fu
rthe
r tr
aini
ng; f
urth
er
trai
ning
or
qual
ity c
ircle
s on
a
regu
lar
basi
s
Sta
ndar
dize
d el
ectr
onic
doc
umen
tatio
n oftreatm
ent,patient’sconditionandtest
resu
lts, m
edic
atio
n re
gim
e an
d ag
reed
tr
eatm
ent g
oals
; cen
tral
dat
a an
alys
is
to p
rodu
ce q
ualit
y re
port
s. a
nd p
rovi
der
feed
back
on
perfo
rman
ce a
nd fo
r be
nchm
arki
ng
GP
con
trac
tsA
nnua
l che
ck-u
ps; a
dvic
e on
pre
vent
ive
mea
sure
s an
d in
form
atio
n; a
sses
smen
t of
card
iova
scul
ar r
isk
fact
ors
(arr
iba
softw
are)
sup
port
s sh
ared
dec
isio
n-m
akin
g on
trea
tmen
t opt
ions
GP
act
s as
gat
ekee
per
to s
peci
alis
t car
e; c
ase
managem
entledbyqualified
nurs
es/p
ract
ice
assi
stan
ts is
en
cour
aged
Trea
tmen
t gui
delin
es b
y as
soci
atio
n of
fam
ily p
hysi
cian
s;
requ
irem
ent t
o pa
rtic
ipat
e in
(c
ontin
uous
) pro
fess
iona
l tra
inin
g,
sele
cted
DM
Ps
and
in a
t lea
st fo
ur
qual
ity c
ircle
s pe
r ye
ar; t
rain
ing
in p
sych
osom
atic
med
icin
e an
d re
habi
litat
ion
care
(Opt
iona
l) us
e of
ele
ctro
nic
med
ical
re
cord
(pat
ient
pas
spor
t); e
xter
nally
cr
eate
d fe
edba
ck re
port
s fo
r ph
ysic
ians
; re
quire
men
t to
impl
emen
t a q
ualit
y m
anag
emen
t sys
tem
Inte
grat
ed c
are/
Hea
lthy
Kin
zigt
alR
egul
ar c
heck
-ups
and
ris
k as
sess
men
ts; i
nvol
vem
ent i
n th
e de
velo
pmen
t of i
ndiv
idua
l tr
eatm
ent/
prev
entio
n pl
ans
and
goal
set
ting;
repr
esen
tatio
n th
roug
h pa
tient
adv
isor
y bo
ard
and
a pa
tient
om
buds
man
Clearlydefinedroleswith
identifiedcarecoordinators;
inte
grat
ed p
rovi
der
netw
ork
and
desi
gnat
ed m
anag
emen
t or
gani
zatio
n re
spon
sibl
e fo
r pr
ovid
er c
oord
inat
ion;
cas
e-finding
Trea
tmen
t gui
delin
es fo
r ov
er 1
5 di
seas
es; p
rovi
ders
and
exp
erts
fro
m th
e pa
rtic
ipat
ing
SH
I fun
ds
colla
bora
te in
wor
king
gro
ups
to d
evel
op g
uide
lines
and
car
e pa
thw
ays
Qua
lity
man
agem
ent s
yste
m a
nd
elec
tron
ic p
atie
nt re
cord
s; re
gula
r an
alys
is o
f pat
ient
dat
a us
ing
pred
ictiv
e m
odel
ling
to id
entif
y hi
gh-c
ost r
isks
Com
mun
ity
nurs
es: c
are
assi
stan
t in
fam
ily
prac
tice
(Ver
AH
)
Acc
ess
to tr
aine
d ca
se m
anag
ers
Del
egat
ion
of ta
sks
to p
ract
ice
assi
stan
ts a
nd p
erfo
rmed
un
der
the
supe
rvis
ion
of th
e G
P; u
sual
ly fo
rms
part
of G
P
cont
ract
Par
t of G
P c
ontr
act a
s de
scrib
ed
abov
e un
der
GP
con
trac
tsP
art o
f GP
con
trac
t as
desc
ribed
abo
ve

64 Assessing chronic disease management in European health systems
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Hun
gary
Trea
tmen
t (andfinancing)
prot
ocol
s
Info
rmat
ion
mat
eria
l on
canc
er,
hype
rten
sion
and
oth
er C
VD
; sel
f-m
anag
emen
t sup
port
by
patie
nt
asso
ciat
ions
and
by
heal
th c
are
staf
f pre
disc
harg
e fo
r ho
spita
lized
pa
tient
s (c
ance
r, C
VD
)
Not
app
licab
leU
se o
f tre
atm
ent g
uide
lines
/pr
otoc
ols
deve
lope
d by
pr
ofes
sion
al a
ssoc
iatio
ns o
n th
e ba
sis
of b
est a
vaila
ble
evid
ence
w
ith v
aria
tion
in q
ualit
y of
gu
idel
ines
; pro
vide
r ed
ucat
ion
for
som
e co
nditi
ons,
org
aniz
ed a
t th
e na
tiona
l lev
el a
nd fr
eque
ntly
su
ppor
ted
by p
harm
aceu
tical
co
mpa
nies
Nat
iona
l dis
ease
regi
strie
s ar
e in
pla
ce fo
r ca
ncer
, ast
hma/
CO
PD
, car
diov
ascu
lar
dise
ase
Car
e co
ordi
natio
n pi
lot
Edu
catio
n by
spe
cial
ized
nur
ses;
in
volv
emen
t in
deve
lopi
ng
trea
tmen
t pla
n an
d go
al s
ettin
g;
acce
ss to
sel
f-m
anag
emen
t too
ls;
regu
lar
asse
ssm
ent o
f pro
blem
s/ac
com
plis
hmen
ts
Car
e co
ordi
natio
n or
gani
zatio
n re
spon
sibl
e fo
r ca
re d
eliv
ery
to a
n en
rolle
d po
pula
tion;
re
gula
r m
eetin
gs o
f pro
vide
rs;
med
icin
es m
anag
emen
t; case-findingandfollow-up;
case
man
agem
ent;
syst
emat
ic
scre
enin
g
Use
of l
ocal
car
e pa
thw
ays
and
of e
vide
nce-
base
d gu
idel
ines
de
velo
ped
by c
are
coor
dina
tion
orga
niza
tion
and
disc
usse
d w
ith
loca
l pro
vide
rs
NIH
FA d
atab
ase
on h
ealth
car
e us
e to
ana
lyse
pro
vide
r pe
rform
ance
and
feedback;createpatientprofilesto
id
entif
y ne
ed
Mul
tifun
ctio
nal
com
mun
ity
cent
res
Pat
ient
edu
catio
n m
ay b
e pr
ovid
edC
omm
unity
cen
tre
inte
grat
es
prim
ary,
spe
cial
ist c
are
and
soci
al c
are;
dev
elop
men
t and
us
e of
inte
grat
ed c
are
path
way
s
Not
app
licab
leIm
plem
enta
tion
of in
tegr
ated
info
rmat
ion
syst
em is
a re
quire
men
t
Ast
hma
dise
ase
man
agem
ent
prog
ram
me
Pat
ient
edu
catio
n on
ast
hma;
ac
cess
to s
elf-
mon
itorin
g to
ols;
in
volv
emen
t in
trea
tmen
t pla
n,
goal
set
ting,
dec
isio
n-m
akin
g;
regu
lar
asse
ssm
ent o
f pro
blem
s/ac
com
plis
hmen
ts
Asthm
anurseispatient’sfirst
poin
t of c
onta
ct, a
nd c
ase
man
ager
; reg
ular
sta
ff m
eetin
gs;
resp
onsi
bilit
y of
all
care
de
cisi
ons
rem
ain
with
trea
ting
phys
icia
n
Use
of t
reat
men
t pla
ns b
ased
on
evid
ence
-bas
ed g
uide
lines
and
tr
aini
ng o
f pro
vide
rs, i
n pa
rtic
ular
as
thm
a nu
rse
Use
of a
nat
iona
l reg
istr
y of
ast
hma
patie
nts
mai
ntai
ned
by N
atio
nal
Kor
ányi
Inst
itute
of T
uber
culo
sis
and
Pul
mon
olog
y; n
urse
s ke
ep d
etai
led
reco
rds
of e
ach
patie
nt
Table
3.5
co
ntd

65Access to health care services within and between countries of the European Union
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Hun
gary
con
tdD
iabe
tes
care
m
anag
emen
t pr
ogra
mm
e
Edu
catio
n pr
ovid
ed b
y a
diab
etes
nu
rse;
acc
ess
to s
elf-
mon
itorin
g de
vice
s (g
luco
met
er);
regu
lar
follo
w-u
p to
rout
inel
y as
sess
pr
oble
ms
and
acco
mpl
ishm
ents
, bo
th in
per
son
and
by te
leph
one
Cleardefinitionofro
lesofhealth
care
sta
ff; re
gula
r st
aff m
eetin
gs
to d
iscu
ss p
robl
emat
ic c
ases
; re
gula
r fo
llow
-up
of p
atie
nts;
us
e of
dis
char
ge s
ocia
l nur
ses
who
coo
rdin
ate
soci
al s
uppo
rt
(cas
h an
d in
kin
d)
Evi
denc
e-ba
sed
trea
tmen
t gu
idel
ines
dev
elop
ed a
nd re
gula
rly
upda
ted
by th
e H
unga
rian
Dia
bete
s A
ssoc
iatio
n an
d th
e tr
aini
ng o
f hea
lth c
are
staf
f, in
pa
rtic
ular
spe
cial
ist d
iabe
tes
nurs
es
Pla
nned
; str
ateg
ies
envi
sage
d in
clud
e re
min
der
syst
ems,
ele
ctro
nic
book
ing
syst
em a
nd p
rovi
der
feed
back
Italy
Inte
grat
ion,
m
anag
emen
t and
as
sist
ance
for
diab
etes
(IG
EA
)
Str
uctu
red
diab
etes
edu
catio
n by
trai
ned
staf
f (sp
ecia
lists
, nu
rses
, GP
s); i
nvol
vem
ent i
n de
velo
ping
car
e pl
an; a
cces
s to
se
lf-m
anag
emen
t too
ls; r
outin
e as
sess
men
ts o
f pro
blem
s an
d ac
com
plis
hmen
ts
Use
of i
nteg
rate
d ca
re
path
way
s; s
peci
alis
t nur
se
deve
lops
indi
vidu
aliz
ed
care
or
trea
tmen
t pla
ns;
team
com
posi
tion
varie
s in
ac
cord
ance
with
indi
vidu
al
patient’sneeds
Evi
denc
e-ba
sed
guid
elin
es fo
r th
e m
anag
emen
t of t
ype
2 di
abet
es
and
two-
stag
e pr
ovid
er tr
aini
ng:
trai
ning
-the
-tra
iner
s st
age
at
natio
nal a
nd re
gion
al le
vel a
nd
indi
vidu
al p
rovi
der
educ
atio
n w
ith fe
edba
ck fo
r pr
ogra
mm
e im
prov
emen
t
Reg
istr
ies
of p
atie
nts
with
dia
bete
s en
rolle
d in
the
prog
ram
me
alth
ough
fo
rmat
var
ies
by re
gion
; doc
umen
t “T
he in
form
atio
n sy
stem
” se
ts o
ut
the
prin
cipl
es fo
r th
e de
velo
pmen
t of
info
rmat
ion
syst
ems
“Fro
m O
n-D
eman
d to
P
roac
tive
Prim
ary
Car
e”
prog
ram
me,
Tu
scan
y
Edu
catio
n an
d co
unse
lling;
in
stru
ctio
n in
sel
f-m
onito
ring
activ
ities
; inv
olve
men
t in
deve
lopi
ng
and
cons
ent t
o ca
re p
lan;
regu
lar
asse
ssm
ents
of p
robl
ems
and
need
s; s
uppo
rt b
y so
cial
wor
kers
w
here
nee
ded
Clin
ical
pat
hway
s de
liver
ed
by G
P-le
d te
ams;
per
iodi
c m
eetin
gs w
ith c
omm
unity
he
alth
doc
tor
at th
e lo
cal
heal
th a
utho
rity
(AS
L); s
taff
rolesclearlydefinedincluding
flowcharts;staffnurseforcase
man
agem
ent a
nd c
ouns
ellin
g
Evi
denc
e-ba
sed
guid
elin
es to
in
form
clin
ical
pat
hway
s an
d co
mpr
ehen
sive
pro
gram
me
of
peer
edu
catio
n fo
r al
l pro
fess
iona
ls
invo
lved
and
sin
gle
grou
ps o
f professionalsonspecificissues;
acce
ss to
spe
cial
ist e
xper
tise;
nu
rse
trai
ning
Dat
abas
es o
n en
rolle
d pa
tient
s to
m
onito
r pe
rform
ance
of p
ract
ice
team
in
regu
lar
mee
tings
; inf
orm
atio
n sh
arin
g am
ong
team
mem
bers
thro
ugh
lead
GP
s el
ectr
onic
sys
tem
; ele
ctro
nic
book
ing
syst
em in
pla
ce
Leon
ardo
pilo
t pr
ojec
t, P
uglia
Edu
catio
n ba
sed
on th
e ei
ght
prioritiesapproachdefinedbyLorig
& H
olm
an; s
yste
mat
ic a
sses
smen
t of
pat
ient
nee
ds (i
n pe
rson
/by
tele
phon
e) a
nd fo
llow
-up
Car
e m
anag
er w
orks
with
GP
todeliverindividualpatient’s
care
pla
n; s
taff
role
s ar
e cl
early
defined;regularstaffmeetings;
flowchartsdescribeactivitiesset
out i
n th
e ca
re p
lan;
med
icin
es
man
agem
ent
Evi
denc
e-ba
sed
prin
cipl
es o
f ca
re m
anag
emen
t and
sco
ring
syst
ems
and
trai
ning
of s
taff
(car
e m
anag
ers
in c
ouns
ellin
g an
d co
mm
unic
atio
n te
chni
ques
; GP
s in
us
e of
the
prog
ram
me
softw
are)
; sp
ecia
list e
xper
tise
is a
vaila
ble
whe
re re
quire
d
Sof
twar
e, In
form
aCar
e™: r
emin
ders
for
prov
ider
s; d
ata
colle
ctio
n fo
r per
form
ance
as
sess
men
t; co
ntin
uous
mon
itorin
g of
pr
ogre
ss; i
nfor
mat
ion
shar
ing.
Ele
ctro
nic
book
ing
syst
em in
pla
ce

66 Assessing chronic disease management in European health systems
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Italy
Raf
fael
lo p
roje
ct,
Mar
che
and
Abr
uzzo
Par
ticip
atio
n in
dev
isin
g ca
re p
lan
and
deci
sion
-mak
ing;
acc
ess
to
coac
hing
and
follo
w-u
p ac
tiviti
es
bytelephone,doctor’soffice
orpatient’shom
e;accessto
info
rmat
ion
mat
eria
l on
dise
ase,
se
rvic
es a
vaila
bilit
y an
d lif
esty
le
Car
e m
anag
er w
orks
with
GP
todeliverindividualpatient’s
care
pla
n; s
taff
role
s ar
e cl
early
defined;useofcase-finding
thro
ugh
mea
sure
s of
prim
ary
prev
entio
n
Pro
vide
r ed
ucat
ion
(trai
ning
-the
-tr
aine
rs a
nd in
divi
dual
pro
vide
r tr
aini
ng fo
r G
Ps
and
care
m
anag
ers)
; acc
ess
to s
peci
alis
t ex
pert
ise
and
expe
rienc
e is
m
entio
ned,
but
spe
cial
ists
do
not
play
an
activ
e ro
le in
the
team
; pr
eim
plem
enta
tion
sim
ulat
ion
to
asse
ss im
pact
of p
ropo
sed
care
st
rate
gy o
n ex
istin
g or
gani
zatio
n
Sof
twar
e de
velo
ped
for
care
man
ager
s:
regu
lar
rem
inde
rs fo
r G
Ps
on s
ched
uled
te
sts
and
appo
intm
ents
; com
mun
icat
ion
betw
een
patie
nt a
nd s
taff
mem
bers
; en
sure
adh
eren
ce to
evi
denc
e-ba
sed
guid
elin
es; e
valu
atio
n of
clin
ical
out
com
es
Latv
ia
Gen
eral
prim
ary
heal
th c
are
syst
em
Notspecified
Pla
ns to
sec
ond
nurs
es to
w
ork
with
GP
in c
hron
ic
care
; edu
catio
n ab
out s
elf-
man
agem
ent;
heal
th p
rom
otio
n an
d di
seas
e pr
even
tion;
de
velo
pmen
t of h
ome
heal
th
care
Qua
lity
crite
ria fo
r ge
nera
l practitionersaredefinedbylaw;
thes
e in
clud
e in
dica
tors
on
the
perio
dic
asse
ssm
ent o
f pat
ient
s w
ith c
ondi
tions
suc
h as
ast
hma
or
diab
etes
Notspecified
Lith
uani
a
Impr
ovin
g in
ters
ecto
ral
colla
bora
tion
Rou
tine
asse
ssm
ent o
f pro
blem
s an
d ac
com
plis
hmen
ts; a
cces
s to
ps
ycho
soci
al re
habi
litat
ion
serv
ices
in
som
e ca
ses
(men
tal h
ealth
)
Case-findingbynurse;case
man
agem
ent p
ilot (
HIV
/AID
S,
som
e m
enta
l hea
lth p
robl
ems)
Acc
ess
to s
peci
alis
t exp
ertis
eN
ot d
ocum
ente
d
Clin
ical
gui
delin
esR
outin
e as
sess
men
t of c
linic
al
indi
cato
rs
Dev
elop
men
t of i
ndiv
idua
lized
ca
re p
lans
com
mon
for
diab
etes
an
d de
pres
sion
, req
uire
d fo
r ca
rdio
vasc
ular
dis
ease
(Evi
denc
e-ba
sed)
clin
ical
gu
idel
ines
; pro
vide
r ed
ucat
ion
in
case
s (fo
r ex
ampl
e, d
epre
ssio
n)
with
sup
port
from
priv
ate
sect
or
(pha
rmac
eutic
al c
ompa
nies
); ac
cess
to s
peci
alis
t exp
ertis
e
Ele
ctro
nic
book
ing
syst
ems
pilo
ted;
pr
ovid
er fe
edba
ck o
n se
rvic
e de
liver
y th
roug
h da
taba
se h
eld
by te
rrito
rial
patie
nt fu
nd (S
VE
IDR
A)
Table
3.5
co
ntd

67Access to health care services within and between countries of the European Union
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Net
herla
nds
Mat
ador
dis
ease
m
anag
emen
t pr
ogra
mm
e
Acc
ess
to D
iabe
tes
Inte
ract
ive
Edu
catio
n P
rogr
amm
e (D
IEP
), co
mpr
isin
g lif
esty
le in
terv
entio
n tr
aini
ng c
ompo
nent
for
prov
ider
s to
en
gage
pat
ient
s in
the
deve
lopm
ent
of tr
eatm
ent p
lan
and
goal
s; D
IEP
w
ebsi
te; s
yste
mat
ic p
atie
nt fo
llow
-up
Stratificationofpatientsinto
thre
e le
vels
of c
are
inte
nsity
and
cl
inic
ians
(GP,
dia
bete
s sp
ecia
list
nurs
e, e
ndoc
rinol
ogis
t); s
taff
rolesclearlydefined;specialist
diab
etes
nur
se li
aiso
n be
twee
n ho
spita
l and
prim
ary
care
for
all p
atie
nts;
regu
lar
core
team
m
eetin
gs
Use
of M
atad
or p
roto
col;
acce
ss to
spe
cial
ist e
xper
tise
with
end
ocrin
olog
ist s
uper
visi
ng
spec
ialis
t dia
bete
s nu
rse
and
actin
g as
con
sulta
nt to
GP,
plu
s tr
aini
ng
Not
inte
grat
ed; d
ata
on p
atie
nt c
onta
cts
and
outc
omes
col
lect
ed o
n G
P a
nd
hosp
ital i
nfor
mat
ion
syst
ems
Prim
ary
care
gr
oup
ZiO
(M
aast
richt
–H
euve
lland
)
Reg
ular
che
ck-u
ps th
at in
clud
e ed
ucat
ion
on s
elf-
man
agem
ent
by p
ract
ice
nurs
es/s
peci
aliz
ed
diab
etes
nur
ses,
dep
endi
ng o
n th
e le
vel o
f nee
d
Stratificationofpatientsinto
four
regu
lar
mod
ules
plu
s tw
o m
odul
es fo
r (c
ompl
ex)
prob
lem
s; s
taff
role
s an
d responsibilitiesaredefined;G
P
over
sees
refe
rral
to s
econ
dary
ca
re a
nd e
nsur
es fo
llow
-up
Nationallydefinedstandardsfor
diab
etes
car
e an
d m
ultid
isci
plin
ary
care
pro
toco
l; re
ferr
al c
riter
ia
to o
ther
car
e pr
ovid
ers;
inte
rnis
t ac
ts a
s co
nsul
tant
to s
peci
aliz
ed
diab
etes
nur
se o
n pa
tient
s w
ith
(com
plex
) pro
blem
s
Disease-specificelectronicpatientrecord
(Med
ix) c
onta
ins
chec
k-up
and
refe
rral
s da
ta w
ithin
car
e pr
ogra
mm
e, a
llow
s fo
r in
form
atio
n sh
arin
g an
d au
tom
atiz
atio
n of
car
e pr
otoc
ols,
and
can
be
linke
d to
labo
rato
ry d
ata
and
func
tiona
l m
easu
rem
ents
Str
oke
serv
ice
Del
ftE
duca
tion
adap
ted
to th
e w
ishe
s an
d ne
eds
of in
divi
dual
pat
ient
s an
d th
eir
care
rs (v
erba
l or
writ
ten;
co
mm
unic
ated
in g
roup
mee
tings
al
tern
atin
g w
ith in
divi
dual
ses
sion
s or
thro
ugh
med
ia s
uch
as In
tern
et
or D
VD
)
Com
mon
ele
men
ts: h
ospi
tal
stro
ke u
nit;
spec
ialis
t m
ultid
isci
plin
ary
team
of
care
give
rs; p
roto
col-b
ased
ca
re; a
gree
men
ts a
bout
pat
ient
re
ferr
al; r
egul
ar m
ultid
isci
plin
ary
staf
f mee
tings
in th
e va
rious
se
ttin
gs; s
truc
ture
d fo
llow
-up
by s
peci
alis
t nur
ses
of s
trok
e pa
tient
s fo
llow
ing
disc
harg
e to
th
eir
hom
e
Sha
red
care
pro
toco
ls a
nd n
atio
nal
mul
tidis
cipl
inar
y ca
re fo
r st
roke
gu
idel
ine
deve
lope
d by
ove
r 70
pr
ofes
sion
als
and
repr
esen
ting
26 s
ocie
ties
or in
stitu
tions
dea
ling
with
str
oke
patie
nts;
spe
cial
sta
ff tr
aini
ng
Ele
ctro
nic
patie
nt re
cord
Por
tavi
ta
Str
oke
Ser
vice
: per
mits
doc
umen
tatio
n an
d sh
arin
g of
info
rmat
ion;
trac
king
an
d re
gist
erin
g of
med
icat
ions
; re
ques
ting,
pla
nnin
g an
d re
gist
erin
g of
(com
plem
entary)examinations;w
orkflow
su
ppor
t

68 Assessing chronic disease management in European health systems
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Net
herla
nds
cont
dN
atio
nal c
are
stan
dard
for
vasc
ular
ris
k m
anag
emen
t
Invo
lvem
ent i
n sh
ared
dec
isio
n-m
akin
g, d
evel
opm
ent o
f car
e pl
an a
nd g
oal s
ettin
g; a
cqui
re
self-
man
agem
ent c
ompe
tenc
ies
thro
ugh
task
-orie
nted
co
mm
unic
atio
n; m
otiv
atio
nal
inte
rvie
win
g; o
r em
otio
nal-o
rient
ed
com
mun
icat
ion
Definedstagedprocess;staff
role
s an
d re
spon
sibi
litie
s cl
early
defined;centralcaregiverisfirst
poin
t of c
onta
ct a
nd c
oord
inat
or
of c
are,
is tr
aine
d in
vas
cula
r ris
k m
anag
emen
t and
ski
lled
in
supp
ortin
g se
lf-m
anag
emen
t an
d ov
erse
es re
ferr
als
Mul
tidis
cipl
inar
y ca
re s
tand
ard
for
vasc
ular
ris
k m
anag
emen
t; if
nece
ssar
y, e
xper
ts c
an b
e co
nsul
ted
IT s
yste
ms
are
used
to re
gist
er, s
hare
and
in
terp
ret p
atie
nt d
ata
as p
art o
f vas
cula
r ris
k m
anag
emen
t, bo
th a
t ind
ivid
ual a
nd
grou
p le
vel
Sw
itzer
land
Dia
Bai
d di
abet
es
care
net
wor
kIn
form
atio
n m
ater
ial;
cust
omiz
ed
face
-to-
face
sel
f-m
anag
emen
t ed
ucat
ion
and
follo
w-u
p; re
gula
r as
sess
men
t of p
robl
ems
and
need
s; in
volv
emen
t in
goal
set
ting
and
deve
lopi
ng a
trea
tmen
t pla
n
Cleardefinitionofstaffrolesand
task
s; m
onth
ly te
am m
eetin
gs
and
wee
kly
coor
dina
tion
mee
tings
; dev
elop
men
t of c
are
plan
s; s
ched
uled
pat
ient
follo
w-
up in
clud
ing
tele
phon
e co
ntac
t at
leas
t onc
e a
year
Car
e pr
otoc
ols
are
deve
lope
d ac
cord
ing
to in
tern
atio
nal a
nd
Sw
iss
guid
elin
es; s
peci
alis
t ph
ysic
ians
are
invo
lved
in th
e pr
ogra
mm
e
Sha
red
elec
tron
ic m
edic
al re
cord
pe
rmitt
ing
(rest
ricte
d) in
form
atio
n sh
arin
g am
ong
heal
th p
rofe
ssio
nals
(cus
tom
ized
ac
cess
); in
clud
es a
n el
ectr
onic
boo
king
sy
stem
Bre
ast c
ance
r cl
inic
al p
athw
ay,
Laus
anne
U
nive
rsity
H
ospi
tal a
nd
Laus
anne
U
nive
rsity
Writ
ten
info
rmat
ion;
regu
lar
reassessmento
fthepatient’s
situ
atio
n; s
hare
d de
cisi
on-m
akin
g;
supp
ort b
y tr
aine
d nu
rses
and
so
cial
wor
kers
; pos
sibl
e ac
cess
to
peer
sup
port
gro
ups
Det
aile
d de
scrip
tion
of c
linic
al
path
way
; reg
ular
mee
tings
with
st
aff a
nd p
roje
ct le
ads;
pla
nned
, pr
edet
erm
ined
and
str
uctu
red
face
-to-
face
con
sulta
tions
; re
gula
r as
sess
men
ts o
f pat
hway
im
plem
enta
tion
Ada
pted
(int
er)n
atio
nal g
uide
lines
; pr
ovid
er e
duca
tion
of p
hysi
cian
s an
d nu
rses
invo
lved
in th
e pr
ogra
mm
e; h
ospi
tal s
peci
alis
ts
are
entir
ely
inte
grat
ed in
the
prog
ram
me;
furt
her
supp
ort
thro
ugh
writ
ten
docu
men
tatio
n de
tailin
g ca
re p
athw
ay
Dat
abas
e an
d bi
oban
k; p
rovi
ders
fe
edba
ck o
n de
lays
, num
ber
of n
ew
case
s pe
r m
onth
, vol
ume
of re
oper
atio
n,
or fr
eque
ncy
of a
giv
en s
urge
on a
ctin
g as
mai
n op
erat
or in
rela
tion
to th
e to
tal
num
ber
of b
reas
t can
cer
oper
atio
ns
Table
3.5
co
ntd

69Access to health care services within and between countries of the European Union
Nam
eS
elf-
man
agem
ent
sup
po
rtD
eliv
ery
syst
em d
esig
nD
ecis
ion
sup
po
rtC
linic
al in
form
atio
n sy
stem
s
Net
herla
nds
cont
d
Del
ta p
hysi
cian
ne
twor
k, G
enev
aR
egul
ar in
form
atio
n (tw
o in
form
atio
n le
tter
s pe
r ye
ar),
deta
iling
prov
isio
ns fo
r ac
cess
to
hea
lth p
rom
otio
n an
d di
seas
e pr
even
tion
cons
ulta
tions
and
ac
tiviti
es; w
ebsi
te
Prim
ary
care
phy
sici
ans
act a
s ga
teke
eper
s to
spe
cial
ist c
are;
ch
roni
c di
seas
e m
anag
emen
t fo
r di
abet
es, h
eart
failu
re a
nd
asth
ma
unde
r de
velo
pmen
t
Org
aniz
atio
n of
regu
lar
qual
ity
circ
les
for
all p
hysi
cian
s pa
rtic
ipat
ing
in th
e ne
twor
k
Notspecified
Sour
ces:
Austr
ia: S
önni
chse
n, F
lam
m &
Nol
te (2
015)
; Den
mar
k: F
rølic
h, Ja
cobs
en &
Kna
i (20
15);
Engl
and:
Nol
te e
t al.
(201
5); E
stoni
a: L
ai &
Kna
i (20
15g)
; Fra
nce:
Che
vreu
l et
al. (
2015
); G
erm
any:
Erle
r, Fu
llert
on &
Nol
te (2
015)
; Hun
gary
: Gaa
l et a
l. (2
015)
; Ita
ly: R
icci
ardi
et a
l. (2
015)
; Lith
uani
a: L
ai e
t al.
(201
5); L
atvi
a: L
ai, K
nai &
Tau
be (2
015)
; the
N
ethe
rland
s: El
issen
et a
l. (2
015)
; Sw
itzer
land
: Pey
trem
ann-
Brid
evau
x et
al.
(201
5).
Not
es: D
MP:
dise
ase
man
agem
ent p
rogr
amm
e; G
P: g
ener
al p
ract
ition
er; B
RAS
S: B
layl
ock
Risk
Ass
essm
ent S
cree
ning
Sco
re; I
T: in
form
atio
n te
chno
logy
; EEP
: éva
luat
ion
des p
ratiq
ues
prof
essio
nnel
les (
eval
uatio
n of
pro
fess
iona
l pra
ctic
e); S
HI:
statu
tory
hea
lth in
sura
nce;
HAS
: Hau
te A
utor
ité d
e Sa
nté
(Nat
iona
l Aut
horit
y fo
r Hea
lth);
INC
a: In
stitu
t Nat
iona
l Du
Can
cer
(Nat
iona
l Can
cer I
nstit
ute)
; RC
P: re
unio
n de
con
cert
atio
n pl
urid
iscip
linai
re (m
ultid
iscip
linar
y te
am m
eetin
g); C
VD
: car
diov
ascu
lar d
iseas
e; C
OPD
: cor
onar
y ob
struc
tive
pulm
onar
y di
seas
e; N
IHFA
: Nat
iona
l Hea
lth In
sura
nce
Fund
Adm
inist
ratio
n; H
IV: h
uman
imm
unod
efici
ency
viru
s; AI
DS:
acq
uire
d im
mun
odefi
cien
cy sy
ndro
me;
DIE
P: D
iabe
tes I
nter
activ
e Ed
ucat
ion
Prog
ram
me;
ZiO
: Zor
g In
Ont
wik
kelin
g (C
are
In D
evel
opm
ent);
DV
D: d
igita
l ver
satil
e di
sc.

70 Assessing chronic disease management in European health systems
within local cancer networks in France. Dedicated staff training tends to be common for those strategies that involve (the delegation of tasks to) non-medical professionals, such as nurses (for example, asthma disease management and diabetes care management programmes in Hungary; IGEA, Leonardo and Raffaello projects in Italy; breast cancer clinical pathway in Lausanne, Switzerland), practice assistants (for example, VerAH care assistant in family practice, Germany) or allied health professionals (for example, therapists in ambulatory after-care of stroke patients in Salzburg, Austria). Physicians acting as coordinators in Austria, Denmark, Germany and Italy are required to undergo additional training; in other settings, this is provided within the framework of continuing medical education (for example, Estonia, France, Hungary).
A number of approaches also provide training in the use of specific programmes designed to support case-finding (for example, care coordination/interface management Styria, Austria; COPA, Coordination & professional care for the Elderly, France). However, overall the use of clinical information systems tends to be the least developed strategy in most approaches. Exceptions include England and Estonia, with both employing standardized, electronic medical records and electronic booking and reminder systems throughout the primary care system.
3.6 Conclusions
In this chapter, we have reviewed the policy context for, and approaches to, chronic disease management in 12 European countries in place during 2009–2011. Countries have sought to create a regulatory and policy framework to respond to chronic disease during recent years. These generally aim to promote approaches that better integrate care and improve coordination between sectors and levels of care, but countries differ with regard to their vision towards controlling and managing chronic disease.
As noted earlier, our review did not attempt to present a comprehensive inventory of all approaches that are being implemented in a given country. Also, as we have focused on published evidence, it is likely that we have missed innovative approaches that are currently being developed or implemented. However, there are a number of general observations that we have identified.
3.6.1 The majority of approaches tend to focus on populations with defined conditions
The most frequently targeted conditions were type 2 diabetes, asthma/COPD, cardiovascular disease (chronic heart failure, IHD, stroke), cancer and mental

71Access to health care services within and between countries of the European Union
health problems. These conditions are typically targeted by means of structured disease management to enhance coordination, which are typically implemented at the national level, or, in decentralized systems, at regional level. There is wide variation in the nature and scope of approaches and the extent to which non-medical staff is involved in care delivery. Commonly, the GP or family physician tends to act as principal provider or “care coordinator”.
3.6.2 There is a trend towards strengthening the role of nurses in care delivery and coordination
The use of nurses in care delivery and coordination is common in systems that have a tradition in multidisciplinary team working (Nolte & McKee, 2008a). Examples include nurse-led clinics and nurse-led case management as established in countries such as England, Italy and the Netherlands. Conversely, the introduction of nurse-led approaches in primary care has remained challenging in systems where primary care is traditionally provided by doctors in solo practices with few support staff. However, there are moves in these countries towards enhanced functions of nurses in care coordination or case management, as, for example, in Denmark, France and Lithuania. Countries are also seeking to strengthen the role of nurses in providing patient self-management support or the delivery of selected medical tasks, although most often such tasks have remained under the supervision of the GP or family physician, such as in Austria, France and Germany.
3.6.3 Approaches that seek to reduce barriers between sectors remain less common
Many of the observed approaches seeking to enhance the care for people with chronic or long-term conditions tend to be implemented within existing organizational and governance structures without necessarily overcoming existing structural or sectoral boundaries. Such approaches may still be effective in enhancing coordination, through, for example, the use of structured referral pathways, but structural barriers between sectors remain, potentially impeding further progress in advancing service delivery towards one better suited to meet complex chronic care needs.
Approaches that seek to more specifically reduce or eliminate these structural or sectoral barriers were less common. Typically, such approaches would focus on managing the primary–secondary care or the secondary care–rehabilitation interface. Examples include some provider networks in France, a range of integrated care contracts in Germany, or the stroke service Delft in the Netherlands as one specific example of an integrated care service. Frequently,

72 Assessing chronic disease management in European health systems
although not always, approaches that perhaps challenge the established ways to service delivery by overcoming sectoral boundaries through, for example, new ways of contracting between funders and providers, were implemented as pilot projects, with the integrated care pilots and the Partnership for Older People Project, both in England, or the improving intersectoral collaboration pilot in Lithuania as examples. The SIKS project in Copenhagen, Denmark, provides an illustration of an integrated care ‘pilot’ that ended following completion of the project phase but that crucially informed policy development for coordinated care approaches across Denmark more widely.
3.6.4 The implementation of approaches frequently involves financial incentives
In a number of countries, the introduction of new approaches to enhance the care for people with chronic conditions involved additional funding in the form of start-up funding to support infrastructural development (for example, administrative structures). These can be targeted at payers, for example, municipalities in Denmark, integrated care pilots in England, or integrated care contracts in Germany, or, in some cases, support providers, such as in the case of provider networks in France.
Typically, however, new approaches would involve some form of financial incentive, most frequently targeted individual providers or physicians, such as within disease management programmes in Austria and Germany, GPs (diabetes care) in Denmark, provider networks in France, care groups in the Netherlands and Italy or GP practices in the England. Incentives for patients are also being used, but these are less common.
3.6.5 Levels of patient and clinician support vary
Patient access is typically granted in line with access to usual care. Many approaches are being implemented in selected geographical regions and may therefore potentially limit access to defined population groups. The majority of approaches provide some form of patient self-management support, although the level and scope of support offered varies. The use of clinical information systems for chronic disease management tends to be the least developed strategy in most approaches.

Chapter 4
Looking aheadEllen Nolte, Cécile Knai, Richard B. Saltman
Chronic disease as a core challenge to health care systems is now firmly on national and international agendas (United Nations General Assembly, 2011; Council of the European Union, 2013; World Health Organization, 2013). In Europe, chronic disease is the greatest challenge to the goal that the EU has set itself of contributing to the achievement of an increase by two years in the number of years spent by the EU population in good health (Council of the European Union, 2013). Achieving this ambition will require effective measures of disease prevention (Novotny, 2008), while also ensuring that those with established illness will be able to participate in society.
We have shown that while policy-makers in European health systems have recognized these challenges, and have acknowledged both the fiscal and social importance of more effectively addressing the requirements associated with chronic and long-term conditions, they often have had considerable difficulty translating this recognition into effective policy programmes (Nolte & McKee, 2008a).
There are several reasons for these continued translational difficulties, but the core challenge is that strategies that would address the complexity arising from the changing burden of disease sit at policy intersections between several different subsystems involving public health, health care and social care, and the wider regulatory framework within which these are embedded. The approaches implemented by countries described in Chapter 3 pursue a wide range of goals, often seeking to simultaneously:
• improve the quality of care and health outcomes for people with complex care needs;
• strengthen primary care and community services, and optimize their interface with secondary care;
• make more efficient use of scarce resources, and reduce spending on health services;

74 Assessing chronic disease management in European health systems
• empower people with chronic and long-term conditions to help define treatment and care modalities.
This list of objectives would be a tall order for any single set of policy innovations to achieve. It is especially difficult to attain where complex care needs created by people with multiple chronic conditions are concerned, the long-term nature of their requirements, alongside the complex set of interests and priorities of those involved in the delivery and financing of care services. These are likely to differ at the different tiers of the system, from the primary process of patient care and the organizational context, to the financing and policy context at system level, each with distinct rationales and perspectives concerning the delivery of health care (Plochg & Klazinga, 2002). Even where innovative approaches addressing the various objectives may be possible, the likelihood of their successful implementation will be determined, to a considerable degree, by the specific political, economic and cultural context within which they are being introduced.
This volume presents the current state of policy thinking across Europe about how to respond to this set of multiple policy objectives. By exploring different approaches in the studied countries, patterns can be identified and their innovative potential and likelihood of success, or indeed failure, noted. It is important to emphasize that strategies to address chronic disease are constantly evolving and this volume could, in the space available, only provide a brief illustration of the many approaches that are being tested and implemented in countries in Europe. It is likely that some approaches presented here will have experienced further modification, roll-out or indeed termination while new strategies will be in the process of implementation at the time of publication of this volume. Further, as we have noted previously, different systems are at different stages of the process and with different degrees of comprehensiveness (Nolte & McKee, 2008c), and evidence presented in this volume confirms this observation. It is against this background that our discussion of the main observations drawn from the presentation of findings has to be set.
4.1 Learning from existing approaches
Our review of approaches seeking to improve the care for those with chronic conditions in Europe found a tendency among countries to implement change within existing provider structures while models that aimed to reduce barriers between providers, institutions or sectors through service redesign were less common. Where such approaches have been implemented, these are likely to be in the form of pilot projects, or, where they form part of routine care, they tended to be confined to a particular locality or region.

75Looking ahead
One such example is the Gesundes Kinzigtal (Healthy Kinzigtal) model of integrated care in Germany (Hildebrandt et al., 2010). Introduced in 2006, the model is considered the only long-term public health and population-based integration approach in Germany. It uses an innovative shared health gain contract between a health care management company, involving a local physicians’ network, and two regional SHI funds in south-west Germany, alongside P4P elements and a share of the company’s profit on the basis of individual provider performance. The approach was associated with a proportionally smaller increase in health care expenditure compared to other regions in the same state, and a comparative saving of 17% of total costs during a four-year period between 2006 and 2010 (Hildebrandt, Schulte & Stunder, 2013).
The Healthy Kinzigtal service delivery model took advantage of start-up funding, a provision made possible by the government from 2004 to encourage selective contracting of SHI funds with individual providers towards the development of more integrated care (Erler, Fullerton & Nolte, 2015). This option created substantial activity, with some 6500 integrated care contracts concluded by 2008, covering a total of around 6% of patients insured under SHI (Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen, 2012). However, the number of integrated care contracts has remained stagnant since, coinciding with the discontinuation of start-up funding from 2009; for example, during 2008 and 2009, around 20% of contracts were terminated or not renewed because of funding discontinuation. Importantly, an assessment of the experience of integrated care contracts published in 2012 found that although a number of anticipated benefits from integrated care contracts had been met, such as improved patient satisfaction with care, or the ability to enter into selective contracts, others were not, such as cost savings and reduced service use (Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen, 2012). The Healthy Kinzigtal model did continue, however, and, as indicated previously, showed potential for cost savings. Although there are efforts to roll out this and other models of more integrated care across Germany, overall their uptake has remained slow.
The Healthy Kinzigtal example is not unique to Germany; indeed similar observations can be made for other countries that have examples of successful models of innovative delivery models but have thus far failed to roll out these models more widely (Curry & Ham, 2011). Where the wider diffusion of models has been possible, this typically required some modification of a given approach to enable take up, which might mean that innovative elements may have to be adapted. The Dutch primary care groups may serve as an example for the scaling up of a care model that was developed locally, and which served

76 Assessing chronic disease management in European health systems
to inform the development of a countrywide approach while retaining the core innovative features of the local model, the Matador disease management programme in Maastricht (Elissen et al., 2015).
Innovative components of the Matador model included: a team approach with the diabetes nurse linking primary and secondary care and taking on some of the tasks previously performed by doctors only; the use of protocols setting out the primary responsibilities for three subgroups of patients to a medical specialist (highly complex), a diabetes nurse (intermediate or stable) or the GP and a practice supporter (low complex) and support of self-management. The redesign of the model towards the one implemented in the form of diabetes care groups included a redefining of the role of the GP and of primary care in general, tasked with the primary responsibility for the subgroup of patients with intermediate to complex care needs. Further adaptations included employment by GPs of practice supporters, who may or may not have a nursing background. This implied a different role for the diabetes nurse, who became a consultant for primary care and a caregiver for patients with highly complex care needs. The wider uptake of the programme was further stimulated and facilitated by the introduction of bundled payments. In a similar vein, the SIKS (Integrated effort for people living with chronic disease) project in Copenhagen, Denmark, served to inform the development of disease management programmes for COPD, type 2 diabetes and CVD in the Capital Region of Denmark (Frølich, Jacobsen & Knai, 2015).
Against this background, it is apparent that, to elevate innovative models of service delivery that provide promising results to a level beyond pilot project or best practice, there is a crucial need for better understanding of specific local conditions that influence the implementation and sustainability of a given approach, so that identified processes can be translated to other contexts and settings. In the context of integrated care in particular, Goodwin (2013) highlighted the need to draw more firmly on implementation science that would enable evidence to be used to support health care policy and practice. It also seems necessary to better understand what Greenhalgh et al. (2004) have referred to as ‘system readiness’ for innovative approaches, that is, the steps that need to be taken to enable wider adoption of new care models. More fundamentally perhaps, there is a need to better understand existing approaches to service delivery to identify those components that present the greatest obstacles to the delivery of high-quality care and that are most likely to act as barriers to change. This issue was highlighted by Epstein and Sherwood (1996); they identified a number of factors for the successful implementation of chronic care management processes, noting that this would require understanding of:
• existing inefficiencies in health care delivery;

77Looking ahead
• disincentives for the patient or the provider to receive or deliver the highest quality care (such as access or cost);
• the relative cost–effectiveness of alternative treatments; and
• the success of different interventions in modifying individual behaviour (for example, adherence).
Lack of understanding of current context, structures and processes, and of the potential for change in the way services are being staffed and delivered to lead to improvement in patient outcomes, might result in the implementation of approaches that are, ultimately, ill-equipped to achieve the desired outcomes. Returning to the example of Germany, among the factors that Amelung, Hildebrandt and Wolf (2012) identified as important barriers to the wider uptake of more coordinated or integrated care approaches within the German health system, the lack of appropriate incentives for key actors to engage in the process was one such barrier. For example, they argued that, for health insurers, the risks to do so currently outweigh the benefits: innovative forms of care typically require investments, yet, stipulations require that where insurers exceed their income (that is, contributions from their members), they have to impose higher premiums on their members, which in turn may threaten their competitiveness in the insurance market. Thus, to encourage insurers to engage in integrated care approaches there may be a need to establish incentive structures that have the potential to better balance the risk–benefit ratio for insurers. Clearly, the specific enablers and barriers for the various actors in the system to engage in change will differ in different settings and it will be important to unpack these various factors in the specific context within which they operate.
In addition to the need to better understand the how and why a given approach works, and its potential for scaling up, there is also a need to better understand the differential impacts of new models of care and what works for whom. We have argued elsewhere how lack of evidence of improved outcomes (however conceptualized) of a given intervention might simply reflect that programme components were not suitable to lead to health improvement in the first place (Nolte et al., 2012b). Likewise, where evidence finds that a given care approach improves outcomes for a subgroup of participants only, this might indicate that the intervention was suboptimal or not sufficiently targeted at those who would benefit most. Indeed, as discussed in Chapter 2, existing research points to the value of targeted approaches to enhance outcomes of people with complex care needs, focusing on those who are most likely to benefit. For example, an evaluation of Dutch primary care groups found that diabetes patients with poorly controlled blood sugar levels saw notable improvements, but there

78 Assessing chronic disease management in European health systems
was little additional benefit for the majority of patients who were already adequately controlled (Elissen et al., 2012). Although these findings require further confirmation (Elissen et al., 2013a), similar observations were reported by a systematic review of diabetes care programmes (Pimouguet et al., 2011).
Likewise, the evaluation of a diabetes disease management programme in Salzburg, Austria, which was implemented as a cluster randomized controlled trial, found only small effects of the intervention on the primary outcome metabolic control (Flamm, Panisch & Sönnichsen, 2012). It concluded that the intervention approach might have taken insufficient account of patient self-management support. Informed by these findings, in a subsequent trial, the patient education module was enhanced through introducing peer support for diabetes patients in the same region (Sönnichsen, Flamm & Nolte, 2015). However, preliminary findings of that trial suggest that the enhanced programme did not significantly improve clinical outcomes, risk profile or quality of life in the intervention group after two years of follow-up (Johansson et al., 2014). Similar to the Dutch primary care groups described earlier, the authors attributed this absence of a significant effect to the observation that both intervention and control groups had already adequate metabolic control, so leaving little room for further substantial improvement.
Overall, these findings point to the need for a more systematic evaluation of new models of care as a means to inform the development of efficient and effective interventions to address the growing burden of chronic conditions in Europe and elsewhere. Evaluation may help identify where a given intervention is likely to lead to inequities in health care delivery. For example, where participation in a novel care approach relies on voluntary enrolment, this might lead to only those with higher health literacy actually benefiting from the programme (selection bias) (Craig et al., 2008). Furthermore, evaluation findings might also highlight issues around programme implementation; for example, where a given intervention is characterized by high drop-out rates of participants this might indicate problems with programme set-up, while also suggesting that the intervention might overall be ill-suited to the needs of the target population.
Arguably, interventions that address the needs of people with chronic conditions should be developed systematically, are based on the best available evidence and appropriate theory, and are tested using a phased approach to inform further development, alongside evaluation. However, as Craig et al. (2008) have pointed out, in practice, interventions emerge from various sources, which may include theory, but may also be based on weak evidence, depending on the drivers behind the intervention. However, even if models and programmes are informed by, say, political imperatives, there are programme design requirements about assessing performance and permitting mid-course corrections that are equally

79Looking ahead
Box 4.1ReportedbarrierstoevaluationinfiveEuropeancountries
In 2010, as part of the DISMEVAL project, we carried out a range of semi-structured
interviews with key informants from Austria, Denmark, France, Germany and the
Netherlands, who were involved in the decision-making process as it relates to various
aspects of chronic disease management in a given health care system context.
Interviews sought, among other things, to explore perceived barriers to developing,
implementing and evaluating chronic care approaches.
Focusing on evaluation, key informants highlighted a lack of overall interest in wanting
to know whether a given innovation does result in improvements in processes or
outcomes. This reluctance can be driven by a range of factors. For example, in
Germany, until recently, SHI funds (commonly referred to as sickness funds), which offer
structured disease management to their enrolled population, received additional funding
for every patient registered in a disease management programme (Erler, Fullerton
& Nolte, 2015). As a consequence, for those SHI funds that have a high proportion
of members with chronic disease, there may have been low interest in identifying
whether or not disease management works because of the risk of losing this additional
funding. Yet, conversely, for those SHI funds with a high proportion of relatively healthy
members,whobenefitedlessfromthefinancialincentive,proofofDMPeffectiveness
was equally undesirable:
There were clear political reasons. [...] So for some sickness funds it was a very
attractive idea to have DMPs because they had more chronic[ally] ill patients who are
eligible for those programmes. They earned a lot of money [from this system]. [...] Other
sickness funds [...] calculated that they would lose a lot of money because they had
not so [many registered] chronic[ally] ill patients. [...] And those sickness funds tried to
stop the programmes on a political basis.[...] This was a big battle. They wanted to stop
the connection of those DMPs to the RSA [risk structure compensation scheme], so
they had no interest in proof of success of those programmes. And this is a big political
issue (Germany).
Other informants from Germany highlighted a historical lack of interest among funders
in “what is done with their money” although this has changed over the years, with an
increasing “consensus about the necessity to have evaluation of the effectiveness of
money spent by the State or by the sickness funds”.
important if programme outcomes are to match expectations. Elsewhere, we have shown that countries can face considerable barriers to the systematic evaluation of new care models (see Box 4.1), reflecting, to considerable extent, lack of evaluation culture and related shortage of capacity as well as a reluctance of payers or providers to engage in evaluation (Knai et al., 2013).

80 Assessing chronic disease management in European health systems
4.1.1 Incorporating the patient perspective
A growing body of evidence points to the potential benefits of actively involving patients with chronic conditions in their own care (Wagner, 1998; Holman & Lorig, 2000). Supporting self-management has been associated with more appropriate use of health services and the potential to improve health outcomes, although the precise benefits will vary according to the conditions involved (Coulter, 2006; Rijken et al., 2008). The concept of active engagement has a
Box 4.1 contd
Several key informants also pointed to a perceived or real reluctance of providers in
supporting evaluation, for example, as a result of the additional administrative burden
this entails. There may be uncertainties about the range of relevant indicators and the
feasibility to collect them, alongside questions, among providers, about the validity of
metrics used for evaluation; such metrics were commonly perceived as not necessarily
representing the true quality of care provided. This notion was reported in several
countries, with interview participants noting that making available such data (for
example, to health insurers) may be interpreted by providers as a compromise on their
freedom of practice to the extent that this would likely involve subjecting their practice
to more external scrutiny:
[...] some doctors [say] that they don’t want to collect data because they are afraid
about the ‘big brother’ syndrome, [...] of being judged on their data. In Denmark there
are many small units of GPs: one-third of GPs are alone in their own practice and
therefore it is easier to blame them if the data are not good enough (Denmark).
This reluctance of physicians to disclose patient data and outcomes to payers and
otherstakeholdersmayalsoreflecttheimportancethatprovidersassigntotheir
professional independence. The underlying concern seems to be that if treatment and
outcomes are made transparent this might interfere with the doctor–patient relationship
and thus impact on patient care.
Against this background, respondents highlighted the need to engage clinicians in the
process more actively so as to come to a common understanding about the purpose of
the evaluation, and thereby strengthen support, as noted for Germany:
Ambulatory [care] physicians have a lot of work with these DMPs, about the evaluation.
They have to give a lot of information but this information is more or less used for
regulatory purposes [only] and is not a good feedback for the practices. For example,
they don’t know what happens to the patient, they have got very bulky reports. [...]
They are not very happy that they have to write a lot of data, a lot of work with that, and
the results of the evaluation are not quite transparent and usable. (Germany)
Source: Knai et al. (2013)

81Looking ahead
persuasive appeal, building on the notion of what Dieterich (2007) referred to as the “modern patient”, who has a legal or moral right to autonomy and self-determination and who can, with the appropriate knowledge and information, make decisions and help improve the system through making informed choices (Greenhalgh, 2009). However, as Bate and Robert (2006:307) observed “[i]n most countries, despite the longevity of the “patient involvement” concept, health care systems are still not putting patients first”. Indeed, as we have shown in Chapter 3 in relation to self-management support for people with chronic conditions, the implementation of such approaches in practice remains weak (Elissen et al., 2013b). Although patient support has moved beyond the mere distribution of information materials towards those that provide access to coaching, lifestyle intervention training and counselling techniques, as well as lay-led programmes, such as the Expert Patients Programme in England, the extent to which these support mechanisms reach wider groups of patients in practice is often unclear.
Experiences of the diabetes disease management programme in Salzburg, Austria, cited earlier point to the challenges of self-management support programmes in demonstrating evidence of effect on clinical outcomes (Johansson et al., 2014). Systematic reviews of self-management support interventions for people with chronic disease have pointed to some improvements in selected outcomes, such as self-efficacy (Foster et al., 2007), or moderate improvements in a range of symptoms such as pain, fatigue, health distress, as well as self-rated health and health-related quality of life, but these were often short-term only and their clinical relevance remains uncertain, as does their impact on service use (Franek, 2013; Kroon et al., 2014). There are many possible explanations for the apparent failure of self-management support programmes to lead to sustained improvement in outcomes; examples include that the length of the evaluation, typically of around 12 months, might be insufficient to demonstrate tangible change in health outcomes, or indeed, resource use (Nolte et al., 2012b). Reflecting on our discussion in the preceding section, it is also likely that programme design may have been inadequate to lead to the desired effect, because it was too narrowly focused and reliant on the clinical setting, and targeted those groups which were less likely to benefit.
An evaluation of the Dutch primary care groups provides further illustration of this point (Elissen et al., 2013b). It found that although Dutch guidelines for type 2 diabetes (care standard) stipulate that patients should play a central role in their care, the practice of diabetes care has remained highly paternalistic. Thus, in its current format, the care group motivates providers to deliver highly standardized care based on performance indicators as stipulated in the national diabetes care standard (Nederlandse Diabetes Federatie, 2007). These

82 Assessing chronic disease management in European health systems
indicators, which are monitored by health insurers, prescribe a defined intensity of service delivery, regardless of patients’ health, demographic or social status. Although frequent monitoring was shown to be especially useful for improving clinical values in poorly controlled diabetic patients, patients in relatively good health could be managed equally effectively in a less physician-guided way that emphasizes self-management. The authors thus argued that there was potential for a more tailored approach to disease management that proactively considers patient characteristics in determining care processes, including self-management support, benefiting a relatively healthy population of diabetic patients for whom intensive monitoring may be inappropriate (Elissen et al., 2012).
Importantly, however, there is a need for initiatives seeking to support people with chronic conditions to self-manage to account for the social and cultural context and norms within which they live (Greenhalgh, 2009). Chronic illness confronts patients with a spectrum of needs that requires them to alter their behaviour and engage in activities that promote physical and psychological well-being, to interact with health care providers and adhere to treatment regimens, to monitor their health status and make associated care decisions, and to manage the impact of the illness on physical, psychological and social functioning (Clark, 2003) This means that any intervention seeking to support people with chronic conditions to self-manage will have to consider their changing needs over time, in particular where they have multiple care needs. Thus, increasing responsibility taken by patients for self-management can create particular challenges for those with multiple conditions, as they may experience aggravation of one condition by treatment of another. For example, a patient with chronic respiratory disease may struggle to adhere to exercise programmes designed for their diabetes (Bayliss et al., 2003). Furthermore, as we have argued previously, patients vary in their preferences for care and the importance they place on health outcomes (Nolte & McKee, 2008a). While the ability of patients to develop individualized treatment plans will be of critical importance to aide effective care, this is unlikely to be sufficient when patients are not considered partners in a care process that is sensitive to the contexts within which people make decisions (Dubois, Singh & Jiwani, 2008).
Failure to take account of patient preferences may lead to suboptimal outcomes of an otherwise innovative service delivery model that seeks to enhance patient care. An illustrative example is that of the national integrated care pilot programme in England, which was carried out from 2009 through to 2011 as described in Chapter 3 (Nolte et al., 2015). A three-year evaluation of six of the 16 pilot sites that used intensive case management for older people at risk of emergency hospital admission, found that staff involved in the delivery of

83Looking ahead
the care believed that the quality of patient care had improved, while patients receiving care in the pilots reported that they found it significantly more difficult to see a doctor or nurse of their choice and felt less involved in the decisions about their care (Roland et al., 2012). Although it is difficult to say whether these perceptions were linked to the change in service delivery as such, this observation highlights that patients need to be consulted on what they actually need and how new delivery models are to be structured to be acceptable to patients and so more likely to be successful. Patient preferences, rather than expert determinations, will need to drive policy formulation.
This latter point is receiving increasing attention under the notion of “experience-based co-design”, which is being tested in patient safety initiatives (Bate & Robert, 2006). It goes beyond mere consultation using user views and perceptions collated through focus groups, patient surveys and other feedback mechanisms. Instead, it is conceived as a joint venture that involves users and professionals working together and throughout the change process as co-designers of a service, based on the experiences of patients (and professionals). This concept has been tested in the area of cancer care (Tsianakas et al., 2012), and may present a useful way forward for improving service design for people with chronic conditions.
4.2 Providing the (regulatory) context to enable innovation
We have previously noted that the policy context within which services are being designed and delivered will be crucial to encourage innovation (Nolte & McKee, 2008c). One area of tension we highlighted was the need to strike a balance, in a given country context, between centrally defined requirements and local autonomy. For example, the creation of a strict national regulatory framework for disease management in Germany has been viewed as beneficial in ensuring that disease management programmes meet an appropriate standard, but it has also been challenged on grounds that it might impede further improvements that take account of local circumstances (Siering, 2008). Tensions also arise in relation to weighing top-down versus bottom-up approaches. Actors operating at the different levels of the health care system are faced with different pressures and consequent priorities that are not necessarily compatible or may even be contradictory (Plochg & Klazinga, 2002). There are particular challenges for organizations that arise from policies initiated by health care reformers on the one hand and established ways of delivery, on the other, which are likely to result in a gap between policy intent and actual implementation (Ham, 2003). We have observed such tensions in our review of approaches to chronic disease management, highlighting the need to create a policy environment that

84 Assessing chronic disease management in European health systems
Box 4.2 Balancing the gap between policy intent and actual implementation: evidence from the DISMEVAL project
As part of the DISMEVAL project, we sought to further explore the barriers to
successful implementation of chronic care, and ways of overcoming these barriers, by
means of interviews with key informants in a range of countries. These revealed a range
of challenges, such as a perceived failure to integrate risk minimization and disease
prevention along the spectrum of care; the persistence of care fragmentation hindering
better coordination; and a lack of structures suitable to promote proactive engagement
with patients in the management of their own condition. Key informants further
discussed the challenge arising from a perceived mismatch between intent, at national
level, to enhance coordination and integration, and the ability at regional or local level to
translate these ambitions into practice.
For example, in Denmark, the 2007 administrative reform led to the reorganization
of regions and municipalities, giving municipalities more responsibility for health.
Specifically,thereformrequiredmunicipalitiestocontribute20%tohealthcare
funding so as to encourage them to increase preventive services and, ultimately,
reduce hospitalizations. However, it was reported that municipalities lacked a
coherent framework to guide them in their new tasks, as well as support to develop
competencies in health care. There was concern that many of the resulting projects
might not be sustainable and measureable:
[Following the administrative reform] the municipalities had a central place in [solving]
problems of the health care sector. The municipalities [have the responsibility] to create
new health centres [...] [designed to overcome] barriers to coordination [...] [However]
municipalities do not have the competence and knowledge about health care. And
there is no systematic development in this area; [...] it is dependent on learning from the
regional level. [...] [Moreover] the Regions got most of the [earmarked] 600 million DKK.
[...] We have ended up with a lot of different projects and I am not sure how they will
evaluate the projects and […] implement the best. (Denmark)
Such disjoint between intent, at national level, to enhance coordination and integration,
and ability at regional or local level to translate these ambitions into practice was also
reported by French participants. For example, the 2009 reform in France stipulated
that patient education should form a mandatory component of chronic illness care.
However, this stipulation was not accompanied by adequate resources to implement
relevant initiatives on the ground:
Funding for patient education has only got limited or ad hoc financing […] usually
allocated for one year, and then [once the funding runs out] it is always put into
provides the means for those who are asked to implement change to acquire the actual capacity and competence to do so to be critical for success (see Box 4.2).

85Looking ahead
Fundamentally, however, it is important to come to an understanding as to whether approaches to better coordinate care for those with chronic conditions is to be considered as a series of interventions that, by implication, ought to be cost-effective and support financial sustainability. Alternatively care coordination and integration could be interpreted, and evaluated, as a complex strategy to innovate and implement long-lasting change in the way services in the health (and social care) sectors are being delivered and that involve multiple changes at multiple levels. Evidence presented here and elsewhere strongly points to the latter, and initiatives and strategies under way will require continuous evaluation over extended periods of time that will enable assessment of their impacts on both economic and health outcomes. This will mean investment in research alongside investment in the development and implementation of service reconfiguration initiatives to ensure that evaluation will inform service development, in particular if we are to generate appropriate conclusions about programme effectiveness and the application of findings to inform decision-making.
References
Adams SG et al. (2007). Systematic review of the chronic care model in chronic obstructive pulmonary disease prevention and management. Archives of Internal Medicine, 167(6):551–561.
Althaus F et al. (2011). Effectiveness of interventions targeting frequent users of emergency departments: a systematic review. Annals of Emergency Medicine 58(1):41–52.e42.
Box 4.2 contd
question. The law now says that patient education is mandatory. However where
the financing comes from is still not clear [...] The nursing profession is collectively in
agreement with [...] developing and implementing patient education programmes but
this is based on the assumption that they have money to do it and at the moment they
don’t. (France)
Furthermore, the creation in 2010 of regional health agencies was aimed at ensuring
that health care provision meets the needs of the population by improving coordination
between ambulatory and hospital care and between health and social care services.
Yet, respondents highlighted that this recent decentralization tended to result in unclear
responsibilities, further fragmented decision-making and disjointed care.
Source: Knai et al. (in press)
86 Assessing chronic disease management in European health systems
Amelung V, Hildebrandt H, Wolf S (2012). Integrated care in Germany-a stony but necessary road! International Journal of Integrated Care 12:e16.
Archer J et al. (2012). Collaborative care for depression and anxiety problems. Cochrane Database of Systematic Reviews, CD006525.
Aspin C et al. (2010). Health policy responses to rising rates of multi-morbid chronic illness in Australia and New Zealand. Australian and New Zeland Journal of Public Health, 34(4):386–393.
Barnett K et al. (2012). Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet, 380(9836):37–43.
Bate P, Robert G (2006). Experience-based design: from redesigning the system around the patient to co-designing services with the patient. Quality and Safety in Health Care, 15(5):307–310.
Bayliss EA et al. (2003). Descriptions of barriers to self-care by persons with comorbid chronic diseases. Annals of Family Medicine, 1(1):15–21.
Bodenheimer T (1999). Disease management—promises and pitfalls. New England Journal of Medicine, 340(15):1202–1205.
Brink-Huis A, van Achterberg T, Schoonhoven L (2008). Pain management: a review of organisation models with integrated processes for the management of pain in adult cancer patients. Journal of Clinical Nursing, 17(15):1986–2000.
Busse R, Mays N (2008). Paying for chronic disease care. In: Nolte E, McKee M, eds. Caring for people with chronic conditions: a health system perspective. Maidenhead, Open University Press:195–221.
Busse R, Riesberg A (2004). Health care systems in transition: Germany. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies.
Campbell H et al. (1998). Integrated care pathways. BMJ, 316(7125):133–137.
Chevreul K et al. (2015). France. In: Nolte E, Knai C, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Chiu WK, Newcomer R (2007). A systematic review of nurse-assisted case management to improve hospital discharge transition outcomes for the elderly. Professional Case Management, 12(6):330–336.

87Looking ahead
Clark NM (2003). Management of chronic disease by patients. Annual Review of Public Health, 24:289–313.
Coleman K et al. (2009). Untangling practice redesign from disease management: how do we best care for the chronically ill? Annual Review of Public Health, 30:385–408.
Coulter A (2006). The quality enhancing interventions project: patient-focused interventions. London, Health Foundation.
Council of the European Union (2013). Reflection process: innovative approaches for chronic diseases in public health and healthcare systems. Brussels, Council of the European Union.
Craig P et al. (2008). Developing and evaluating complex interventions: new guidance. London, Medical Research Council.
Curry N, Ham C (2011). Clinical and service integration: the route to improved outcomes. London, King’s Fund.
Danaei G et al. (2013). The global cardiovascular risk transition: associations of four metabolic risk factors with national income, urbanization, and Western diet in 1980 and 2008. Circulation, 127(14):1493–1502.
de Bruin SR et al. (2011). Impact of disease management programs on healthcare expenditures for patients with diabetes, depression, heart failure or chronic obstructive pulmonary disease: a systematic review of the literature. Health Policy, 101(2):105–121.
Department of Health (2004). Chronic disease management: a compendium of information. London, Department of Health.
Dieterich A (2007). The modern patient – threat or promise? Physicians’ perspectives on patients’ changing attributes. Patient Education and Counseling, 67(3):279–285.
Drewes H et al. (2012). The effectiveness of chronic care management for heart failure: meta-regression analyses to explain the heterogeneity in outcomes. Health Services Research, 47(5):1926–1959.
Dubois C-A, Singh D, Jiwani I (2008). The human resource challenge in chronic care. In: Nolte E, McKee M, eds. Caring for people with chronic conditions: a health system perspective. Maidenhead, Open University Press:143–171.
Egginton J et al. (2012). Care management for type 2 diabetes in the United States: a systematic review and meta-analyis. BMC Health Services Research, 12:72.

88 Assessing chronic disease management in European health systems
Elissen A et al. (2013a). Advancing current approaches to disease management evaluation: capitalizing on heterogeneity to understand what works and for whom. BMC Medical Research Methodology, 13:40.
Elissen A et al. (2013b). Is Europe putting theory into practice? A qualitative study of the level of self-management support in chronic care management approaches. BMC Health Services Research, 13:117.
Elissen A et al. (2015). The Netherlands. In: Nolte E, Knai C, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Elissen AM et al. (2012). Toward tailored disease management for type 2 diabetes. American Journal of Managed Care, 18(10):619–630.
Ellrodt G et al. (1997). Evidence-based disease management. JAMA, 278:1687–1692.
Epstein RS, Sherwood LM (1996). From outcomes research to disease management: a guide for the perplexed. Annals of Internal Medicine, 124(9):832–837.
Erler A, Fullerton B, Nolte E (2015). Germany. In: Nolte E, Knai C, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Ettelt S, Nolte E (2010). Funding intensive care: approaches in systems using diagnosis-related groups. Santa Monica, CA, Rand Corporation.
Ettelt S et al. (2008). Decision-making in health care: roles and responsibilities at local, regional and national level. London, London School of Hygiene & Tropical Medicine.
Finucane MM et al. (2011). National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet, 377(9765):557–567.
Flamm M, Panisch S, Sönnichsen A (2012). Evaluation of disease management in Austria. In: Nolte E, Hinrichs S, eds. DISMEVAL: developing and validating disease management evaluation methods for European healthcare systems: final report. Santa Monica, CA, RAND.

89Looking ahead
Foster G et al. (2007). Self-management education programmes by lay leaders for people with chronic conditions. Cochrane Database of Systematic Reviews, CD005108.
Franek J (2013). Self-management support interventions for persons with chronic disease: an evidence-based analysis. Ontario Health Technology Assessment Series, 13(9):1–60.
Frølich A, Jacobsen R, Knai C (2015). Denmark. In: Nolte E, Knai C, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Fullerton B, Nolte E, Erler A (2011). The quality of chronic care in Germany [in German]. Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen, 105(8):554–562.
Gaal P et al. (2015). Hungary. In: Nolte E, Knai C, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Geyman JP (2007). Disease management: panacea, another false hope, or something in between? Annals of Family Medicine, 5(3):257–260.
Gilbody S, Bower P, Whitty P (2006). Costs and consequences of enhanced primary care for depression: systematic review of randomised economic evaluations. British Journal of Psychiatry, 189:297–308.
Glasby J, Dickinson H, Peck E (2006). Guest editorial: partnership working in health and social care. Health & Social Care in the Community, 14(5):373–374.
Glasgow N et al. (2008). Australia. In: Nolte E, Knai C, McKee M, eds. Managing chronic conditions: experience in eight countries. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies:131–160.
Göhler A et al. (2006). A systematic meta-analysis of the efficacy and heterogeneity of disease management programs in congestive heart failure. Journal of Cardiac Failure, 12(7):554–567.
Gonseth J et al. (2004). The effectiveness of disease management programmes in reducing hospital re-admission in older patients with heart failure: a systematic review and meta-analysis of published reports. European Heart Journal, 25(18):1570–1595.

90 Assessing chronic disease management in European health systems
Goodwin N (2013). How do you build programmes of integrated care? The need to broaden our conceptual and empirical understanding. International Journal of Integrated Care, 13:e040.
Greenhalgh T (2009). Patient and public involvement in chronic illness: beyond the expert patient. BMJ, 338:b49.
Greenhalgh T et al. (2004). Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Quarterly, 82(4):581–629.
Gröne O, Garcia-Barbero M (2001). Integrated care: a position paper of the WHO European Office for Integrated Health Care Services. International Journal of Integrated Care, 1:e21.
Grumbach K (2003). Chronic illness, comorbidities, and the need for medical generalism. Annals of Family Medicine, 1(1):4–7.
Ham C (2003). Improving the performance of health services: the role of clinical leadership. Lancet, 361(9373):1978–1980.
Hildebrandt H, Schulte T, Stunder B (2013). Triple aim in Kinzigtal, Germany: improving population health, integrating health care and reducing costs of care – lessons for the UK? Journal of Integrated Care, 20(4):205–222.
Hildebrandt H et al. (2010). Gesundes Kinzigtal Integrated Care: improving population health by a shared health gain approach and a shared savings contract. International Journal of Integrated Care, 10:e046.
Hofmarcher MM, Rack HM (2006). Austria: health system review. Health Systems in Transition, 8(3):1–247.
Holman H, Lorig K (2000). Patients as partners in managing chronic disease. Partnership is a prerequisite for effective and efficient health care. BMJ, 320(7234):526–527.
Institute for Health Metrics and Evaluation (2013a). Global burden of disease cause patterns (http://www.healthmetricsandevaluation.org/gbd/visualizations/gbd-cause-patterns, accessed 4 December 2014).
Institute for Health Metrics and Evaluation (2013b). Global burden of disease: country profiles (http://www.healthmetricsandevaluation.org/gbd/country-profiles#g, accessed 4 December 2014).
Jacob V et al. (2012). Economics of collaborative care for management of depressive disorders: a community guide systematic review. American Journal of Preventive Medicine, 42(5):539–549.

91Looking ahead
Johansson T et al. (2014). Can a peer support intervention improve type 2 diabetes outcomes? Diabetes Voice, 59:60–63.
Klein-Lankhorst E, Spreeuwenberg C (2008). The Netherlands. In: Knai C, Nolte E, McKee M, eds. Managing chronic conditions: experience in eight countries. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies:97–114.
Knai C et al. (2013). Reported barriers to evaluation in chronic care: experiences in six European countries. Health Policy, 110(2–3):220–228.
Knai C et al. (in press). The underlying challenges of coordination of chronic care across Europe. International Journal of Care Coordination.
Knight K et al. (2005). A systematic review of diabetes disease management programs. American Journal of Managed Care, 11(4):242–250.
Kodner DL, Spreeuwenberg C (2002). Integrated care: meaning, logic, applications, and implications–a discussion paper. International Journal of Integrated Care, 2:e12.
Kroon FP et al. (2014). Self-management education programmes for osteoarthritis. Cochrane Database of Systematic Reviews, CD008963.
Krumholz HM et al. (2006). A taxonomy for disease management: a scientific statement from the American Heart Association Disease Management Taxonomy Writing Group. Circulation,114(13):1432–1445.
Lai T, Knai C (2015). Estonia. In: Knai C, Nolte E, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Lai T, Knai C, Taube M (2015). Latvia. In: Knai C, Nolte E, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Lai T et al. (2015). Lithuania. In: Knai C, Nolte E, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Langhorne P et al. (2005). Early supported discharge services for stroke patients: a meta-analysis of individual patients’ data. Lancet, 365(9458):501–506.

92 Assessing chronic disease management in European health systems
Lemmens K, Nieboer AP, Huijsman R (2009). A systematic review of integrated use of disease-management interventions in asthma and COPD. Respiratory Medicine, 103(5):670–691.
Leutz WN (1999). Five laws for integrating medical and social services: lessons from the United States and the United Kingdom. Milbank Quarterly, 77(1): 77–110.
Maciejewski ML, Chen SY, Au DH (2009). Adult asthma disease management: an analysis of studies, approaches, outcomes, and methods. Respiratory Care, 54(7):878–886.
Nederlandse Diabetes Federatie (2007). NDF Zorgstandaard. Transparantie en kwaliteit van diabeteszorg voor mensen met diabetes type 2.
Neumeyer-Gromen A et al. (2004). Disease management programs for depression: a systematic review and meta-analysis of randomized controlled trials. Medical Care, 42(12):1211–1221.
Nies H, Berman PC (eds.) (2004). Integrating services for older people: a resource book for managers. Dublin, European Health Management Association.
Nolte E (in press). Disease management. In: Busse R, Klazinga N, Røttingen J-A, eds. Improving quality in European health system: a comprehensive framework approach. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies.
Nolte E, Hinrichs S (eds.) (2012). DISMEVAL: developing and validating disease management evaluation methods for European healthcare systems: final report. Santa Monica, CA, RAND Corporation.
Nolte E, Knai C (eds.) (2015). Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies.
Nolte E, McKee M (eds.) (2008a). Caring for people with chronic conditions: a health system perspective. Maidenhead, Open University Press.
Nolte E, McKee M (2008b). Integration and chronic care: a review. In: Nolte E, McKee M, eds. Caring for people with chronic conditions: a health system perspective. Maidenhead, Open University Press:64–91.
Nolte E, McKee M (2008c). Making it happen. In: Nolte E, McKee M, eds. Caring for people with chronic conditions: a health system perspective. Maidenhead, Open University Press:222–244.

93Looking ahead
Nolte E, Pitchforth E (2014). What is the evidence on the economic impacts of integrated care? Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies.
Nolte E, Knai C, McKee M (eds.) (2008). Managing chronic conditions: experience in eight countries. Copenhagen, World Health Organization on behalf of the European Observatory on Health Systems and Policies.
Nolte E, McKee M, Knai C (2008). Managing chronic conditions: an introduction to the experience in eight countries. In: Nolte E, Cnai C, McKee M, eds. Managing chronic conditions: experience in eight countries. Copenhagen, World Health Organization on behalf of the European Observatory on Health Systems and Policies:1–14.
Nolte E et al. (2012a). Overcoming fragmentation in healthcare: chronic care in Austria, Germany and the Netherlands. Health Economics, Policy, and Law, 7(1):125–146.
Nolte E et al. (2012b). Evaluating chronic disease management: recommendations for funders and users. Santa Monica, CA, RAND Corporation.
Nolte E et al. (2015). England. In: Knai C, Nolte E, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Novotny T (2008). Preventing chronic disease: everybody’s business. In: Nolte E, McKee M, eds. Caring for people with chronic conditions: a health system perspective. Maidenhead, Open University Press:92–115.
Oeseburg B et al. (2009). Effects of case management for frail older people or those with chronic illness: a systematic review. Nursing Research, 58(3):201–210.
Ofman J et al. (2004). Does disease management improve clinical and economic outcomes in patients with chronic diseases? A systematic review. American Journal of Medicine, 117(3):182–192.
Ouwens M et al. (2005). Integrated care programmes for chronically ill patients: a review of systematic reviews. International Journal for Quality in Health Care, 17(2):141–146.
Øvretveit J (1998). Integrated care: models and issues. Goteborg, Nordic School of Public Health.

94 Assessing chronic disease management in European health systems
Øvretveit J (2009). Does improving quality save money? A review of evidence of which improvements to quality reduce costs to health service providers. London, Health Foundation.
Peytremann-Bridevaux I et al. (2008). Effectiveness of chronic obstructive pulmonary disease-management programs: systematic review and meta-analysis. American Journal of Medicine, 121(5):433–443.
Peytremann-Bridevaux I et al. (2015). Switzerland. In: Nolte E, Cnai C, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Phillips CO et al. (2004). Comprehensive discharge planning with postdischarge support for older patients with congestive heart failure: a meta-analysis. JAMA, 291(11):1358–1367.
Piette J, Richardson C, Valenstein M (2004). Addressing the needs of patients with multiple chronic illnesses: the case of diabetes and depression. American Journal of Managed Care, 10(2 Pt 2):152–162.
Pimouguet C et al. (2010). Dementia case management effectiveness on health care costs and resource utilization: a systematic review of randomized controlled trials. Journal of Nutrition, Health & Aging, 14(8):669–676.
Pimouguet C et al. (2011). Effectiveness of disease-management programs for improving diabetes care: a meta-analysis. Canadian Medical Association Journal, 183(2):E115–127.
Plochg T, Klazinga N (2002). Community-based integrated care: myth or must? International Journal for Quality in Health Care, 14(2):91–101.
Pomerleau J, Knai C, Nolte E (2008). The burden of chronic disease in Europe. In: Nolte E, McKee M, eds. Caring for people with chronic conditions: a health system perspective. Maidenhead, Open University Press:15–42.
Population Health Alliance (2014). PHM glossary: D. Disease management. (http://www.populationhealthalliance.org/research/phm-glossary/d.html, accessed 4 December 2014).
Powell Davies G et al. (2008). Coordinating primary health care: an analysis of the outcomes of a systematic review. Medical Journal of Australia, 188(8 Suppl):S65–68.
Ricciardi W et al. (2015). Italy. In: Nolte E, Cnai C, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen,

95Looking ahead
WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Rijken M et al. (2008). Supporting self-management. In: Nolte E, McKee M, eds. Caring for people with chronic conditions: a health system perspective. Maidenhead, Open University Press:116–142.
Rijken M et al. (2014). Chronic Disease Management Programmes: an adequate response to patients’ needs? Health Expectations, 17(5):608–621.
Roccaforte R et al. (2005). Effectiveness of comprehensive disease management programmes in improving clinical outcomes in heart failure patients. A meta-analysis. European Journal of Heart Failure, 7(7):1133–1144.
Roland M et al. (2012). Case management for at-risk elderly patients in the English integrated care pilots: observational study of staff and patient experience and secondary care utilisation. International Journal of Integrated Care, 12:e130.
Rothman AA, Wagner EH (2003). Chronic illness management: what is the role of primary care? Annals of Internal Medicine, 138(3):256–261.
Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen (2012). Wettbewerb an der Schnittstelle zwischen ambulanter und stationärer Gesundheitsversorgung. Bonn, Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen.
Savard LA, Thompson DR, Clark AM (2011). A meta-review of evidence on heart failure disease management programs: the challenges of describing and synthesizing evidence on complex interventions. Trials, 12:194.
Schoen C et al. (2007). Toward higher-performance health systems: adults’ health care experiences in seven countries. Health Affairs, 26:w717–734.
Shepperd S et al. (2008). Admission avoidance hospital at home. Cochrane Database of Systematic Reviews, CD007491.
Shortell SM, Gillies RR, Anderson DA (1994). The new world of managed care: creating organized delivery systems. Health Affairs, 13(5):46–64.
Siering U (2008). Germany. In: Knai C, Nolte E, McKee M, eds. Managing chronic conditions: experience in eight countries. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies:75–96.
Simoens S et al. (2011). Review of the cost-effectiveness of interventions to improve seamless care focusing on medication. International Journal of Clinical Pharmacy, 33(6):909–917.

96 Assessing chronic disease management in European health systems
Smith L, Newton R (2007). Systematic review of case management. Australian and New Zealand Journal of Psychiatry, 41(1):2–9.
Smith SM et al. (2012). Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database of Systematic Reviews, CD006560.
Sönnichsen A, Flamm M, Nolte E (2015). Austria. In: Knai C, Nolte E, eds. Assessing chronic disease management in European health systems. Country reports. Copenhagen, WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies (http://www.euro.who.int/en/about-us/partners/observatory/publications/studies).
Steffen S et al. (2009). Discharge planning in mental health care: a systematic review of the recent literature. Acta Psychiatrica Scandinavica, 120(1):1–9.
Steuten L et al. (2009). Identifying potentially cost effective chronic care programs for people with COPD. International Journal of Chronic Obstructive Pulmonary Disease, 4:87–100.
Suhrcke M, Fahey D, McKee M (2008). Economic aspects of chronic disease and chronic disease management. In: Nolte E, McKee M, eds. Caring for people with chronic conditions: a health system perspective. Maidenhead, Open University Press:43–63.
Suhrcke M et al. (2006). Chronic disease: an economic perspective. London, Oxford Health Alliance.
Takeda A et al. (2012). Clinical service organisation for heart failure. Cochrane Database of Systematic Reviews, CD002752.
Tappenden P et al. (2012). The clinical effectiveness and cost-effectiveness of home-based, nurse-led health promotion for older people: a systematic review. Health Technology Assessment, 16(20):1–72.
Thomson S, Foubister T, Mossialos E (2009). Financing health care in the European Union: challenges and policy responses. Copenhagen, World Health Organization on behalf of the European Observatory on Health Systems and Policies.
Thota AB et al. (2012). Collaborative care to improve the management of depressive disorders: a community guide systematic review and meta-analysis. American Journal of Preventive Medicine, 42(5):525–538.
TNS Opinion & Social (2007). Health in the European Union. Special Eurobarometer 272e. Brussels, European Commission.

97Looking ahead
Tsai AC et al. (2005). A meta-analysis of interventions to improve care for chronic illness. American Journal of Managed Care, 11(8):478–488.
Tsianakas V et al. (2012). Implementing patient-centred cancer care: using experience-based co-design to improve patient experience in breast and lung cancer services. Support Care Cancer, 20(11):2639–2647.
United Nations General Assembly (2011). Prevention and control of non-communicable diseases (http://www.un.org/en/ga/search/view_doc.asp?symbol=A/66/83&Lang=E, accessed 4 December 2014).
Unwin N, Epping Jordan J, Bonita R (2004). Rethinking the terms non-communicable disease and chronic disease. Journal of Epidemiology and Community Health, 58(9):801.
Van Cleave J, Gortmaker SL, Perrin JM (2010). Dynamics of obesity and chronic health conditions among children and youth. JAMA, 303(7):623–630.
van Steenbergen-Weijenburg KM et al. (2010). Cost-effectiveness of collaborative care for the treatment of major depressive disorder in primary care. A systematic review. BMC Health Services Research, 10:19.
Wagner EH (1998). Chronic disease management: what will it take to improve care for chronic illness? Effective Clinical Practice, 1(1):2–4.
Wagner EH et al. (1999). A survey of leading chronic disease management programs: are they consistent with the literature? Managed Care Quarterly, 7(3):56–66.
Wong FK, Chung LC (2006). Establishing a definition for a nurse-led clinic: structure, process, and outcome. Journal of Advanced Nursing, 53(3):358–369.
World Health Organization (2013). Global action plan for the prevention and control of NCDs 2013–2020. Geneva, World Health Organization.
World Health Organization (2014). Global health expenditure database: NHA indicators and tables (http://apps.who.int/nha/database, accessed 4 December 2014).
Yach D et al. (2004). The global burden of chronic diseases: overcoming impediments to prevention and control. JAMA, 291(21):2616–2622.

ISB
N 9
2890
5030
2
97
89
28
90
50
30
2
The rising burden of chronic illness, in particular the rapid increase in the number of people withmultiple health problems, is a challenge to health systems globally. Associated premature mortalityand reduced physical functioning, along with higher use of health services and related costs, areamong the key concerns faced by policy-makers and practitioners.
There is a clear need to redesign delivery systems in order to better meet the needs created bychronic conditions, moving from the traditional, acute and episodic model of care to one that bettercoordinates professionals and institutions and actively engages service users and their carers.Many countries have begun this process but it has been difficult to reach conclusions about thebest approach to take: care models are highly context-dependent and scientifically rigorous evaluations have been lacking.
Assessing chronic disease management in European health systems explores some of the key issues, ranging from interpreting the evidence base to assessing the policy context for, and approaches to, chronic disease management across Europe. Drawing on 12 detailed country reports(available in a second, online volume), the study provides insights into the range of care modelsand the people involved in delivering these; payment mechanisms and service user access; andchallenges faced by countries in the implementation and evaluation of these novel approaches.
This book builds on the findings of the DISMEVAL project (Developing and validating DISease Management EVALuation methods for European health care systems), led by RAND Europe andfunded under the European Union’s (EU) Seventh Framework Programme (FP7) (Agreement no. 223277).
The editors
Ellen Nolte, Hub Cordinator, European Observatory on Health Systems and Policies.
Cécile Knai, Senior Lecturer, London School of Hygiene & Tropical Medicine.
Richard B. Saltman, Professor of Health Policy and Management at the Rollins School of PublicHealth of Emory University in Atlanta and Associate Head of Research Policy at the EuropeanObservatory on Health Systems and Policies.
Observatory Studies Series No. 37
37
Obs
erva
tory
S
tudi
es S
erie
s
37Ed
ited
by
Elle
n N
olte
, Cé
cile
Kn
ai, R
ich
ard
B S
altm
an
AS
SES
SIN
G CH
RO
NIC D
ISEA
SE M
AN
AGEM
ENT IN
EUR
OPEA
N H
EALTH
SYSTEMS
Concepts and approaches
Assessing chronic disease management in European health systems
Edited by
Ellen Nolte
Cécile Knai
Richard B. Saltman
Cover_WHO_nr37_bis_Mise en page 1 5/02/15 15:39 Page 1







