
Carotid revascularization in asymptomatic patients:
when should we do revascularization
Vipul Gupta
Neurointerventional Surgery/Interventional neuroradiologyMedanta The -Medicity
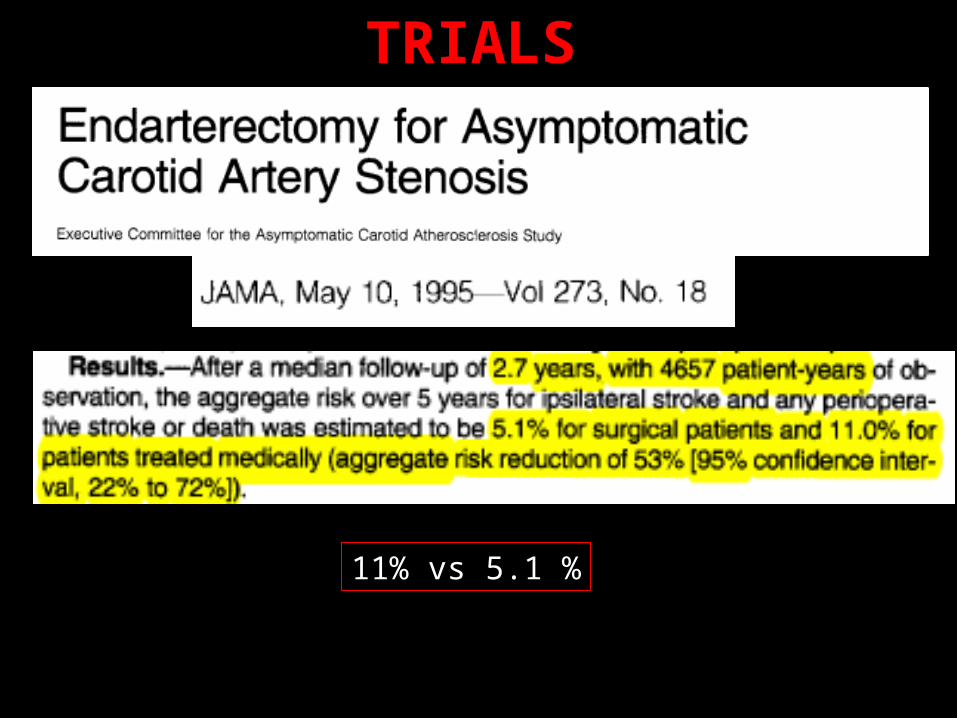
TRIALS
11% vs 5.1 %

Stroke 2013
Gain of 4.1% at 5 years and 4.6% at 10 years (13.4% vs 17.9%)

Against?•Medical therapy has improved significantly
Stroke 2009
In favour for intervention!
• Low complication rates of revascularization• Operator experience
• Technology
• Identification of high risk patients

It was -

Now -
1% risk
European society of vascular surgery, 2013Perirocedural risk (with in 30 days) stroke/MI/death – 1 %
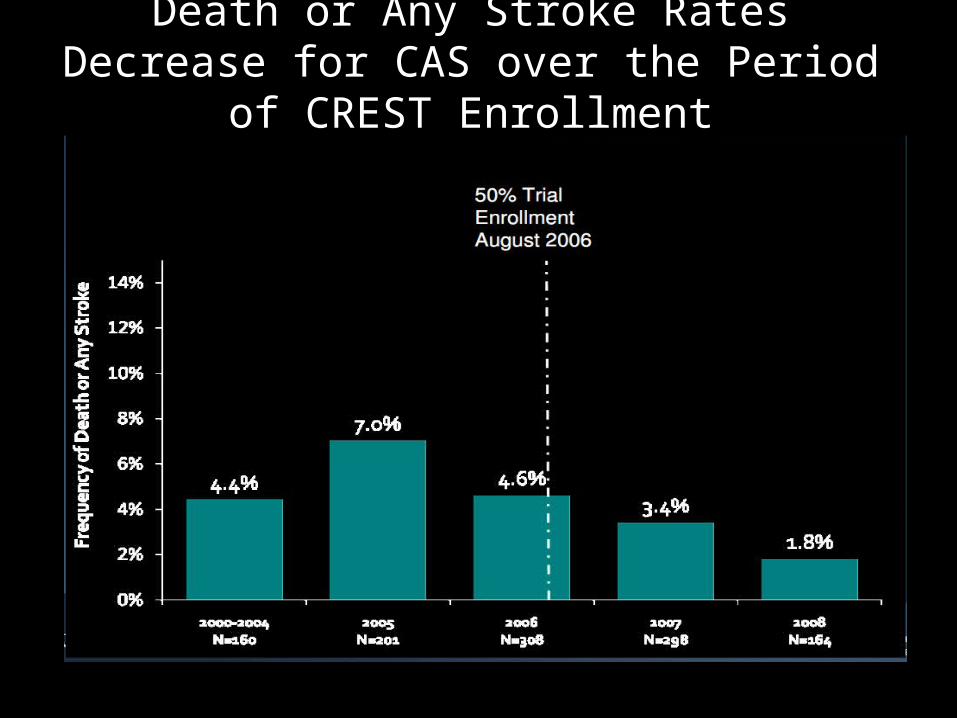
Death or Any Stroke Rates Decrease for CAS over the Period of CREST Enrollment

Death or Major Stroke Rates in CASDecrease for Symptomatic Patients

How to select?Identify high risk patients
•Plaque morphology
•MES
•Progression
•Silent infarcts
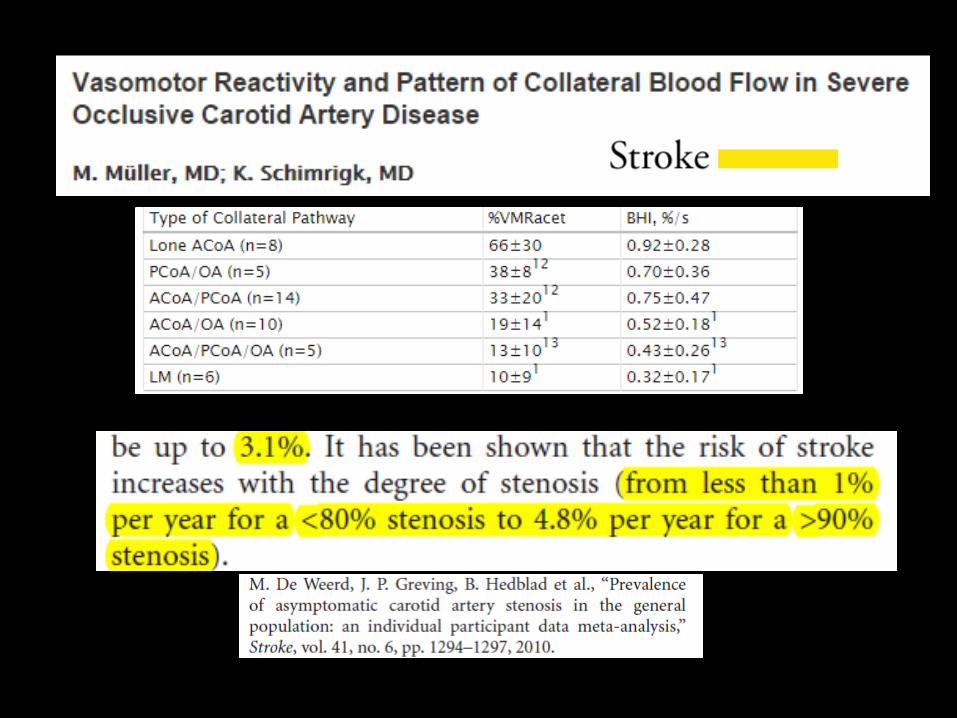
•Hemodynamic (VMR, degree of stenosis)

• Consecutive patients
• > 60% stenosis on doppler
• TCD – 2 MES in 1 hour
• 3D US – Ulcer detection

Patients were on maximal medical therapy
Relative risk = 11.7
Relative risk = 8.6
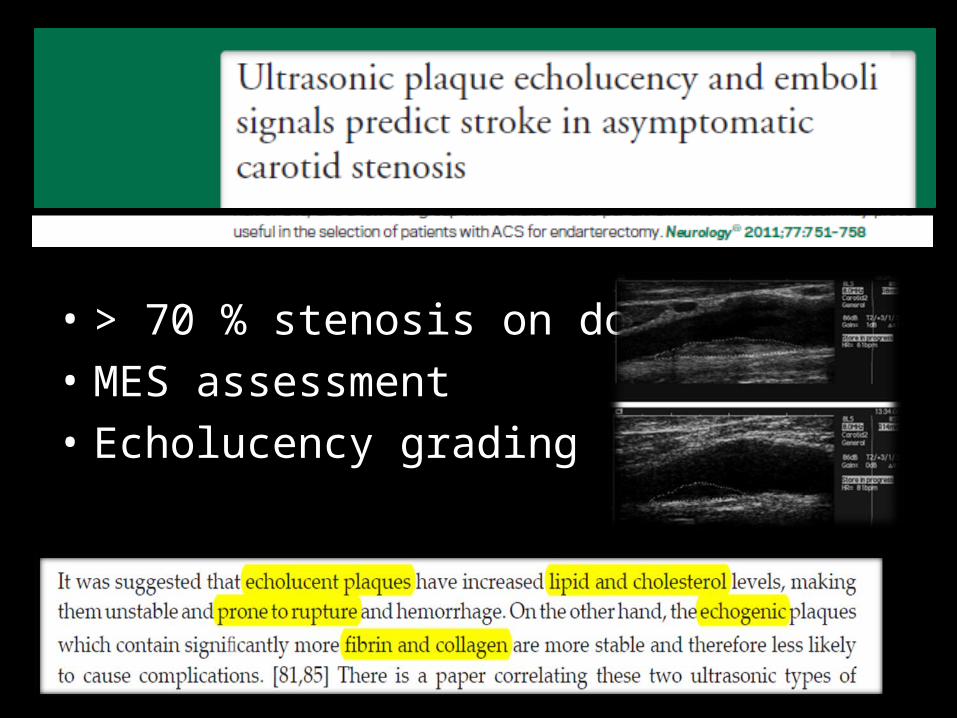
• > 70 % stenosis on doppler
• MES assessment
• Echolucency grading


Intra-plaque hemorrhage
HR – 2-3 fold increase

Microembolic signals
• Stroke : 10-18.5 % vs 1 %
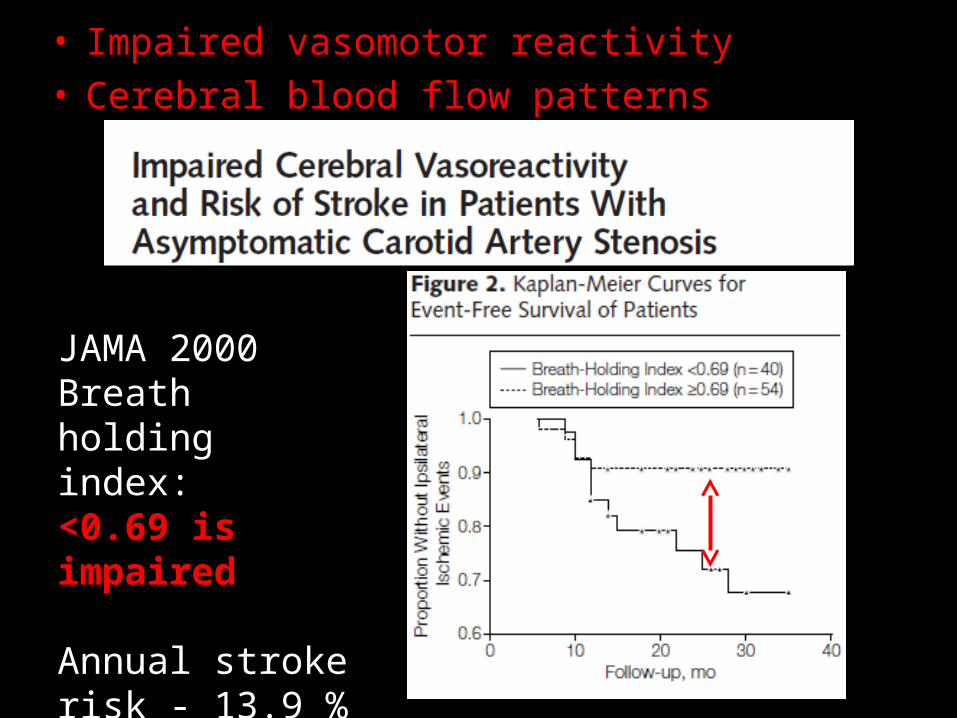
• Impaired vasomotor reactivity
• Cerebral blood flow patterns
JAMA 2000Breath holding index:<0.69 is impaired
Annual stroke risk - 13.9 % vs 4.1 %

Progression of stenosis
21.7 % experienced an ipsilateral stroke
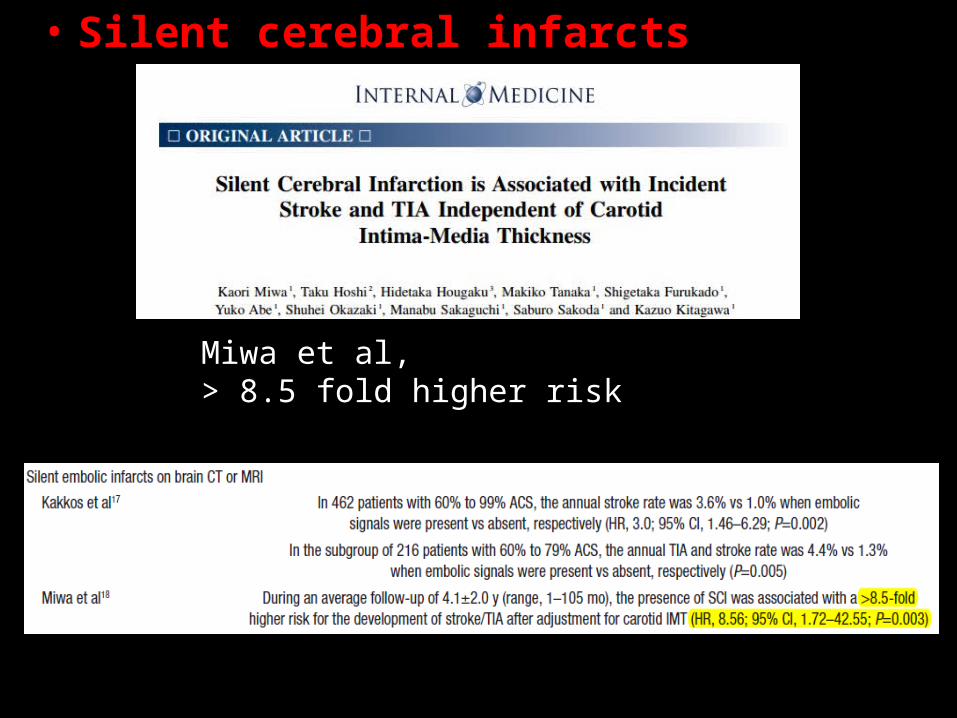
• Silent cerebral infarcts
Miwa et al, > 8.5 fold higher risk
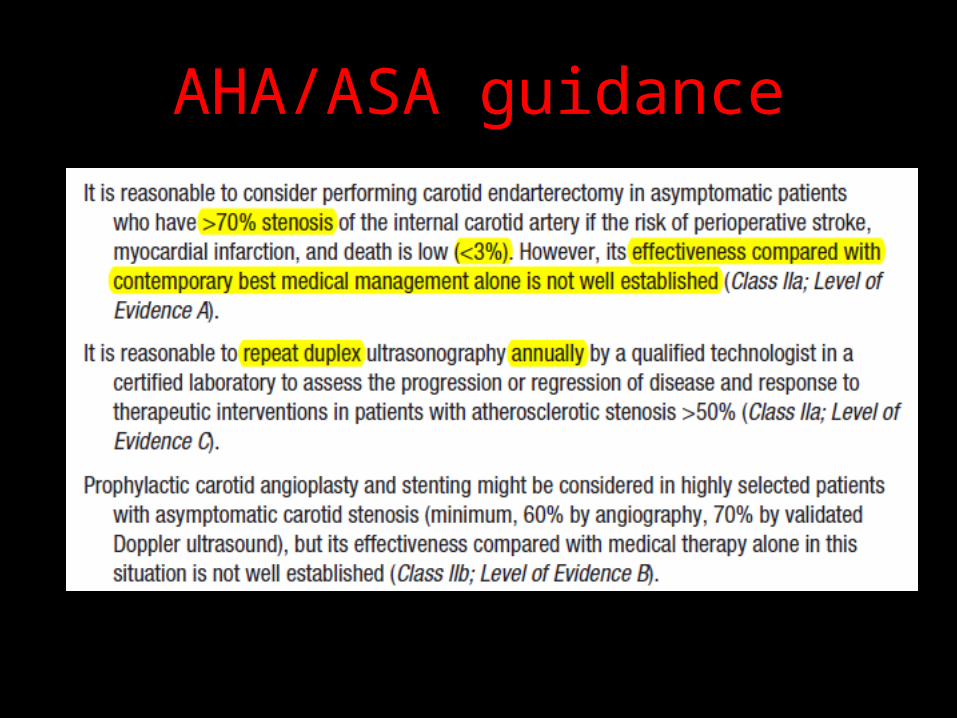
AHA/ASA guidance
• Microemboli• Plaque morphology• Vasomotor reactivity• Silent infarcts • Progression

65-M, Hypertensive
Thank you







