
17th November 2011
Audit of Impact of NICE guidelines for Ovarian Cancer
Helen LostyRoyal United Hospital Bath

17th November 2011
Background to Audit
• Ovarian cancer• Ca125 in ovarian cancer• Cancer strategy• Scope and brief for guidelines• Guideline algorithm

17th November 2011
Methodology of Audit
• Requesting of Ca 125 in primary care• Analytical method• Methodology of audit

17th November 2011
Results of audit
Background
Image reproduced by kind permission of Dr Sue Barter
• Ovarian cancer is a challenge to diagnose because of the non-specific nature of symptoms and signs – “silent killer”
• Most women are diagnosed with advanced disease (stages II– IV)

Epidemiology
• Ovarian cancer is the 5th most common cancer in women in the UK
• Over 6700 new cases are diagnosed each year, accounting for approximately 1 in 20 cases of cancer in women
• Around 4300 women die from ovarian cancer each year in the UK, representing 6% of all cancer deaths in women

Ca 125
• Known as the first and predominant ovarian tumour marker investigated
• Hybridoma defined tumour marker• High molecular weight glycoprotein
present in serum of women with primary epithelial ovarian cancer
• Not present on surface epithelial of normal ovaries

Ca 125 lack of specificity
Elevated in:• Benign gynaecology Endometriosis Fibroids Pelvic Inflammatory Disease
• Other peritoneal inflammation• Benign conditions Urinary retention Chronic renal failure Pancreatitis
• Cyclical variations in pre-menopausal age group• Other malignant disease – gastric and lung

Ca125 – lack of sensitiviry
• Ca 125 not raised in 30% of women with ovarian cancer – early stage disease

Ca125 diagnostic efficiency
• Sensitivity and specificity
Ca 125 U/mL Sensitivity % Specificity %
65 and greater 79 82
150 69 93
190 63 95
Cancer Strategy
• National awareness and Early Diagnosis Initiative NAEDI 2008
• Improving outcomes – save 5,000 lives through earlier diagnosis
• Cancer and general practice - GP’s in the driving seat
• Increase access for GP’s to diagnostic tests - imaging

Ovarian cancer
• Ovarian cancer – 29% present through emergency route which is always associated with poorer outcome
• Increase the number of women accessing the correct treatment pathway earlier.

Ovarian cancerImplementing NICE guidance
April 2011
NICE clinical guideline 122
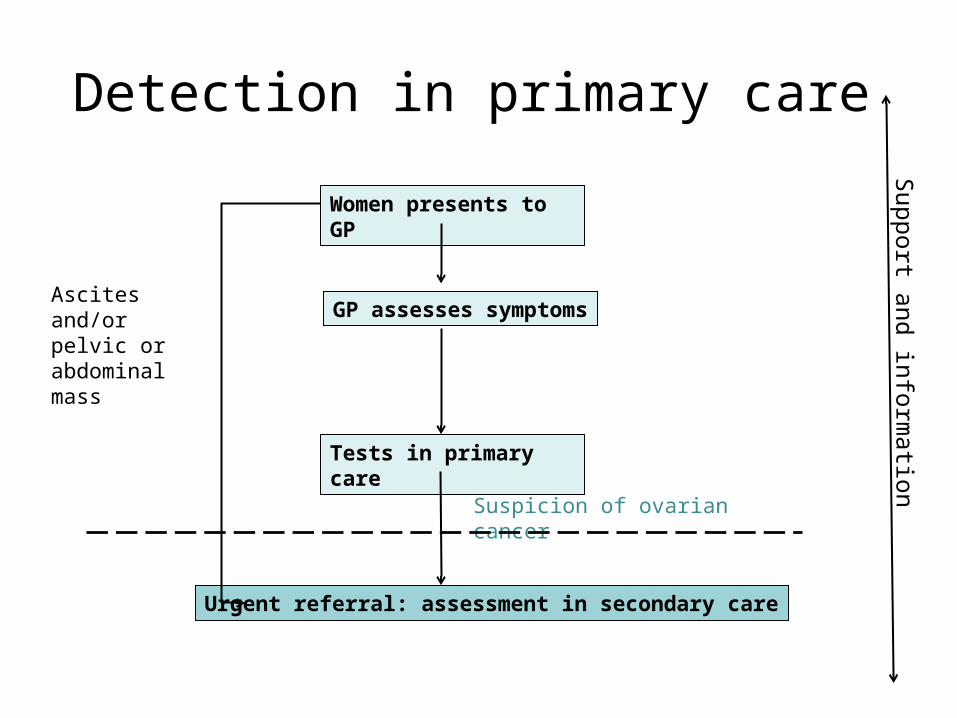
Detection in primary care
Women presents to GP
GP assesses symptoms
Tests in primary care
Urgent referral: assessment in secondary care
Suspicion of ovarian cancer
Ascites and/or pelvic or abdominal mass
Support and inform
ation

Measure serum CA125
Ultrasound of abdomen and pelvis
Advise to return to GP if symptoms become more frequent and/or persistent
InvestigateRefer urgently
Assess carefully: are other clinical causes of
symptoms apparent?
Suggestive of ovarian cancer
35 IU/ml or greater
Normal
Less than 35 IU/ml
No
First tests in primary care
Yes

Why choice of Ca125
• Least expensive option as first test compared with ultrasound – access undeliverable or pelvic examination which is not specific enough
• Prevalence in primary care in symptomatic woman is only 0.23% ie if all symptomatic patients were referred then only 1:500 would have ovarian cancer.
• NB GP sees a patient with ovarian cancer every
5-6 years

Awareness of symptoms and signs: 1
• Refer the woman urgently if physical examination identifies ascites and/or a pelvic or abdominal mass (which is not obviously uterine fibroids)

Awareness of symptoms and signs: 2
– Carry out tests in primary care if a woman (especially if 50 or over) reports having any of the following symptoms on a persistent or frequent basis – particularly more than 12 times per month:– persistent abdominal distension (women often refer to this as ‘bloating’)– feeling full (early satiety) and/or loss of appetite– pelvic or abdominal pain– increased urinary urgency and/or frequency
Awareness of symptoms and signs: 3
• Consider carrying out tests in primary care if a woman reports unexplained weight loss, fatigue or changes in bowel habit
• Carry out appropriate tests for ovarian cancer in any woman of 50 or over who has experienced symptoms within the last 12 months that suggest irritable bowel syndrome (IBS)
• Advise any woman who is not suspected of having ovarian cancer to return to her GP if her symptoms become more frequent and/or persistent

NICE guidelines
• Awareness of symptoms• Facilitate improved detection in primary
care

Audit 1- On line requesting

Ca 125 methodology
• Monoclonal antibody – murine lymphocytes immunised with ovarian cancer cell line 433
• Sandwich IRMA• Most important tumour marker for
monitoring therapy and progress of patients with serous carcinoma
Audit
• Computer search of ICE for Ca125 requests from primary care
May to July 2011 vs May to July 2010
Itemised for each of 57 practices
Sole identifier was laboratory number
Results

1 20
50
100
150
200
250
300
350
400
450
500
2010
2011
146
429
Increase in test requests from primary care 2010 vs
2011

B2=169
Q=120
Z=130
G2=176
I=108
N1=149
Q1=154
Z1=1
66G=1
06
D2=171
L=114
T=123
X=128
M=115
X1=164
K=113
F1=1
40U=1
24Y=
129S=
122
A =100
D=103
P=119
A1=131
F=105
D1=134
Y1=1
65H=1
07N=1
160
5
10
15
20
25
30
Number of Ca 125 requests per practice 2010 compared with 2011
Series1Series2
57 prac-tices

1 20%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%Percentage of normal results in 2010 and 2011
Series1
70%
90%
2010
2011

Ca 125
• 10% greater than or equal to 35IU/ml• ie 45 requests • Clinical details abstracted from information
accompanying ICE request







