

Barbara Deller, CNM, MPH Mary Ellen Stanton, CNM. MSN,
FACNM
October 27, 2006
Saving Mothers: Evidence and Issues
2
Purpose of this Session
Take a look at….
• Progress towards maternal survival
• New Evidence
• Issue & Discussion
3
“A woman who is pregnant has one foot in the grave”
. . . Local Proverb, Chad

4
The Lifetime Risk of Maternal Death in some places in the world it is staggering
1:94
1:16
1:2,800
1:160
Source: WHO, UNICEF and UNFPA. Maternal Mortality in 2000; Lancet Neonatal Survival Series, 2005
The chance of a woman dying as a result of pregnancy is 150 x greater in sub-Saharan Africa than it is in the United States
5
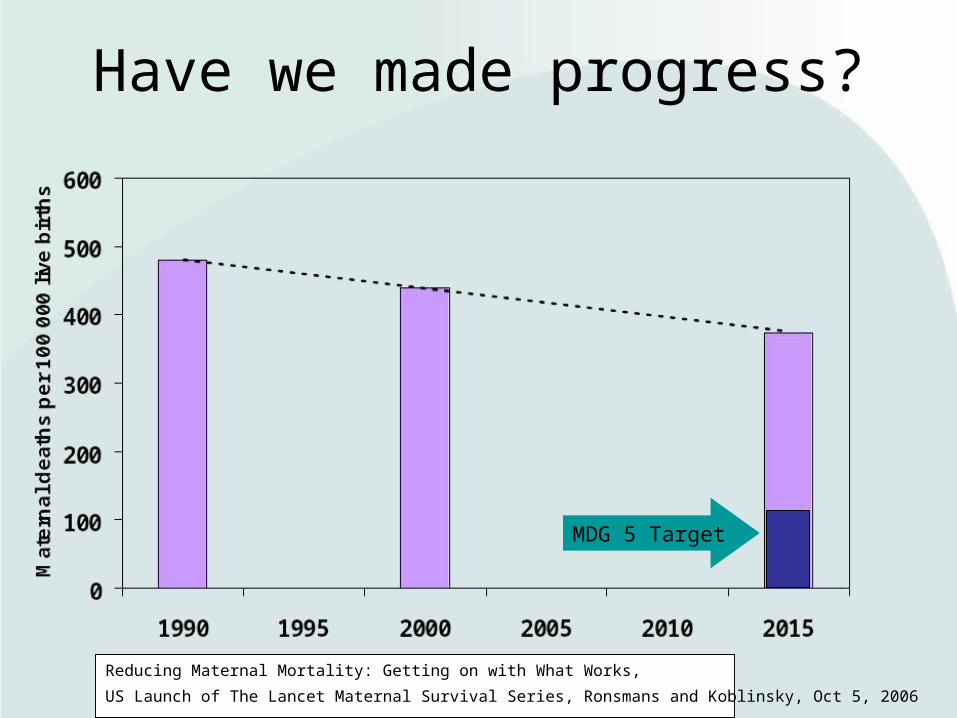
Have we made progress?
MDG 5 Target
Reducing Maternal Mortality: Getting on with What Works,
US Launch of The Lancet Maternal Survival Series, Ronsmans and Koblinsky, Oct 5, 2006
6
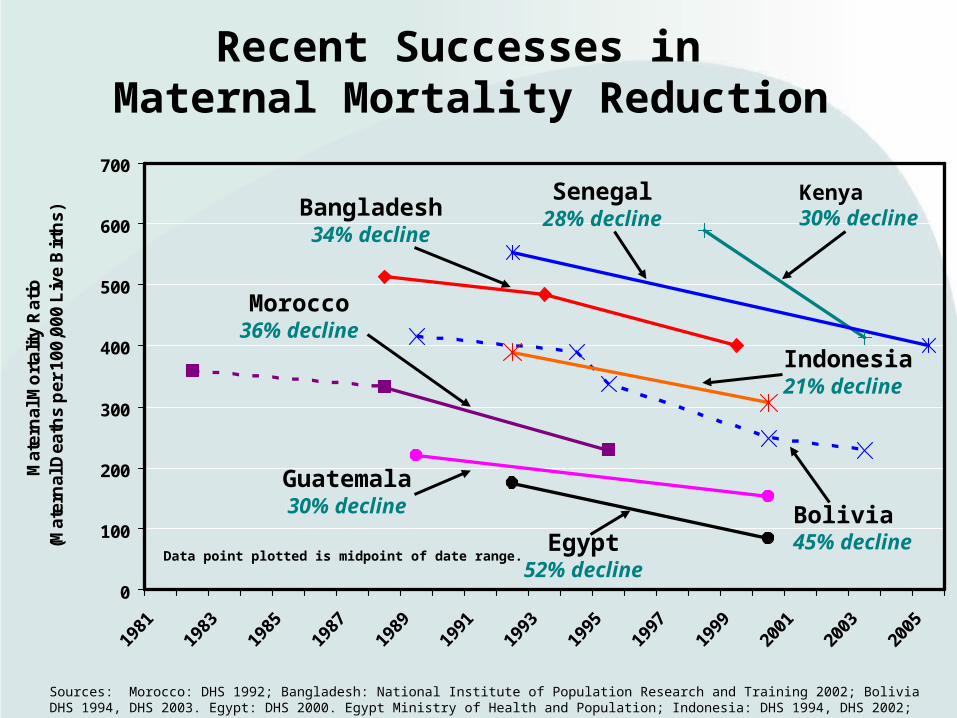
Recent Successes in Maternal Mortality Reduction
0
100
200
300
400
500
600
700
1981
1983
1985
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
Ma
tern
al M
ort
alit
y R
ati
o
(Ma
tern
al D
ea
ths
pe
r 1
00
,00
0 L
ive
Bir
ths
)
Morocco36% decline
Egypt52% decline
Bangladesh34% decline
Sources: Morocco: DHS 1992; Bangladesh: National Institute of Population Research and Training 2002; Bolivia DHS 1994, DHS 2003. Egypt: DHS 2000. Egypt Ministry of Health and Population; Indonesia: DHS 1994, DHS 2002; Guatemala: Duarte et al. 2003; Kenya DHS 1998, DHS 2003; Senegal DHS 1992, DHS 2005.
Data point plotted is midpoint of date range.
Indonesia21% decline
Bolivia45% decline
Guatemala30% decline
Kenya30% decline
Senegal28% decline

7
Progress in reducing maternal mortality
• Globally1
– essentially no change via estimates since 1990– > 500,000 deaths annually– MMR 400/100,000 live births (US 17)– 2005 estimates not yet available
• In specific countries2 – Wide variability– Other surveys show good progress in some
countries– Overall lack of progress in sub-Saharan Africa
Source: 1 WHO Maternal Mortality in 200: Estimates Developed by WHO, UNICEF, UNFPA 2 Demographic and Health Surveys, Macro Int.

8
The Poor Are Hardest Hit
Source: C Ronsmans and Koblinsky, presentation at US Launch of The Lancet’s Maternal Survival Series, 5 Oct 06, Washington, DC
0
100
200
300
400
500
600
700
800
900
Tanzania 1996 Indonesia 2002 Peru 2000
Mate
rnal m
ort
alit
y r
atio
Poorest 20% Richest 20%
9
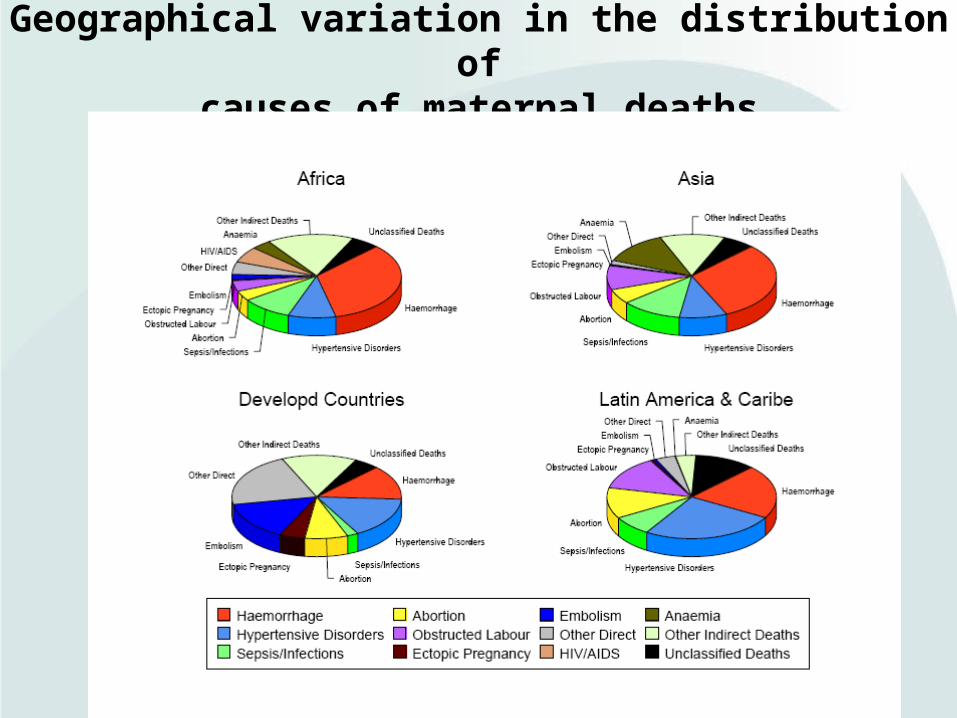
Geographical variation in the distribution ofcauses of maternal deaths

10
Leading Causes of Maternal Death
Cause of death Developed countries
Africa Asia Latin America/ Caribbean
Hemorrhage 13% 34% 31% 21%
Hypertensive disorders
16% 9% 9% 26%
Sepsis/infections
2% 10% 12% 8%
Abortion 8% 4% 8% 12%
Obstructed labor
0% 4% 9% 13%
Anemia 0% 4% 13% 0%
HIV/AIDS 0% 6% 0% 0%Source: Khan et al, WHO analysis of causes of maternal death: a systematic review, The Lancet, March 28, 2006 -- % rounded; not included on this table: ectopic pregnancy, embolism, other direct causes, other indirect causes, unclassified deaths
11
Because Maternal Mortality is “relatively rare,”
Severe acute maternal morbidity (SAMM)
may be important in measuring progress• SAMM—”near miss”--“A very ill pregnant or
recently delivered woman who would have died had it not been that luck and good care was on her side” — differs from complications
• Systematic review -- 30 reports --prevalence– Disease-specific (e.g. eclampsia) 0.80% - 8.23%– Management specific (e.g. hysterectomy) 0.01%-2.99%– Organ system dysfunction/failure—0.38%-1.09%
• Inverse trend in prevalence with development status of the country
• Need better definitions before uptakeSource: reported in Say, WHO systematic review of maternal morbidity and mortality, Reproductive Health, 2004
12
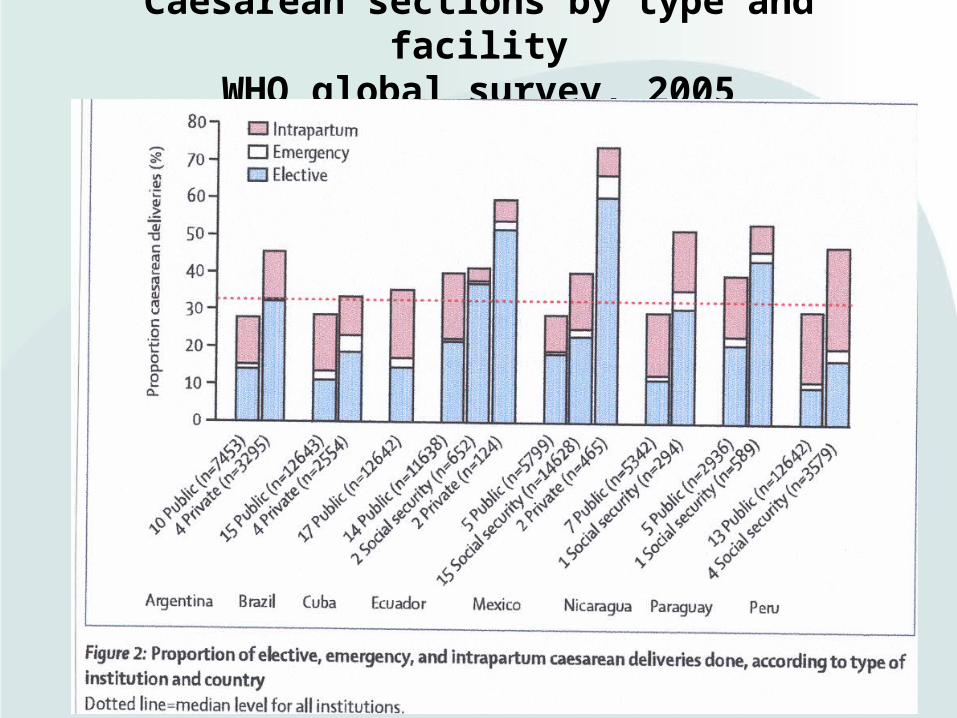
Caesarean sections by type and facility
WHO global survey, 2005
13
WHO Global Survey, 2005 -- Latin America
Caesarean Rates and Pregnancy Outcomes
• Median C/S rate 33%, 51% in private hospitals• C/S rate was positively associated with
– Increase in a severe maternal morbidity and mortality (index)
– Postnatal tx with antibiotics– Fetal death and neonatal mortality and morbidity– C/S did not improve perinatal outcomes
• Preterm delivery rates and neonatal mortality rose at rates of C/S between 10 and 20%
• Limitations included: – 3 of 11 countries (Haiti, USA, Paraguay) and 3 selected
institutions originally selected did not participate– Limited standardization of diagnoses
Source: Villar, et al. Caesarean delivery rates and pregnancy outcomes: 2005 Global Survey…in Latin America, 2006.
14
CHALLENGE
We do know a lot about what interventions
workbut. . . we still face
manyissues in programmingto bring life-savinginterventions tochildbearing women toreduce maternalmortality
15
In the developing world where 50% of births occur in home. . .
. . . what strategy should we invest in for maximum reduction in maternal mortality?
• Bring skilled care to mothers at home• Bring misoprostol (and other
evidence-based home care) to homes where there is no skilled care
• Bring mothers to skilled care
16
Skilled care at home
• Women’s choice
• Success in UK, Denmark, Malaysia
• Inefficient
• Requires links to EmOC
• Quality uncertain/supervision difficult

17
Effective interventions at home without SBA
• Evidence of some effective interventions related to significant maternal complications that don’t require SBA (Lancet does not agree)– Oral misoprostol– Iron supplementation
• TBA meta analysis did not show effectiveness in reducing maternal mortality
• If trained de novo—huge investment
• Supervision and logistics difficult
Lancet advocates pragmatism

18
Oral misoprostolRural India, 2006
• 1620 women, placebo-controlled trial• Misoprostol: oral, stable, positive safety
profile—can be used in the absence of a skilled birth attendant
• Misoprostol associated with– Reduction in PPH (12% to 6.4%; p<0.0001)– Reduction in acute severe PPH (1.2% to 0.2%;
p<0.0001)– Decrease in mean PP blood loss (262.3 to 214.3ml;
p<0.0001)– Transitory chills and fever
Source: Derman, et al, Oral misoprostol in preventing postpartum hemorrhage in resource-poor communities: A randomized controlled trial, The Lancet, Oct. 7, 2006.
19
SBA at the facility(includes EmOC or link)
• Can maintain normality (vs hospital)
• Can provide robust interventions
• Promotes 24/7• Scale-up team
model can be 10x solo practitioners
• No RCTs• Does not ensure
quality—studies document– Negligence– Iatrogenic
complications– Abuse
20
Strategy Proposed in The Lancet:Team of skilled birth attendants in health
center
• Care during delivery is the priority
• All women should be able to deliver in health centres, with midwives working in teams
• Target the women in greatest need: poor and rural women in sub-Saharan Africa and South Asia
Reducing Maternal Mortality: Getting on with What Works, US Launch of The Lancet Maternal Survival Series, Ronsmans and Koblinsky, Oct 5, 2006
21
Considerations• Design programming approach based upon MMR, cause of
death, current availability and cadres of providers
• Can chose more than one approach—keeping in mind that everything costs
• Plan for scale to achieve public health impact
• Phasing strategies
• Different approaches with massive deprivation and marginal exclusion
• Lancet: Need a new era of strategic thinking to address stagnation:
Vision Funds Human resources Track progress

22
Our Pearls
• The chance of a woman dying as a result of pregnancy is 150 times greater in Sub-Saharan Africa than in the U.S. This is the health indicator with the greatest disparity between the developed and the developing work.
• Postpartum hemorrhage (PPH) is, by far, the biggest maternal killed, responsible for greater than 30% of maternal deaths in Asia and Africa. PPH is preventable.
23
“ Women are not dying because of diseases we cannot treat . . .
. . . they are dying because societies have yet to make the decision that their lives are worth saving ”
. . . . Mahmoud Fathalla







