

Barcelona Clinic Liver Cancer (BCLC) staging for hepatocellular carcinoma.
Dr. Abhilash
Introduction
• Fifth most common neoplasm.
• Third most common cause of death.
• No universally accepted staging system.

Ideal staging system
• Predict treatment outcome.
• Aid selection for various treatment modalities.

Why not in HCC?
Prognosis is multifactorial.
1. Tumor related factors.
2. Anatomical extent.
3. Liver function.
4. Etiology.
5. Interaction between the above factors.

Prognostic factors in HCC
PATIENT FACTORS
• Performance status
• Quality of life score
• General medical condition
TUMOR FACTORS
• Number and size
• Histopathological grade
• DNA aneuploidy
• Vascular invasion
• Genotype• VEGF levels• Serum AFP
LIVER FACTORS
• Child Pugh Score
• MELD score• FIBROSIS score• Active
inflammation• Functional
hepatic reserve• GSA Rmax• PIVKA-II serum
levels
ETIOLOGY
• Alcohol• Hepatitis C• Hepatitis B
Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19:329–338

Staging systems
• Okuda stage
• French score
• CLIP score
• BCLC staging
• CUPI score
• TNM staging
• JIS score
• ER score.
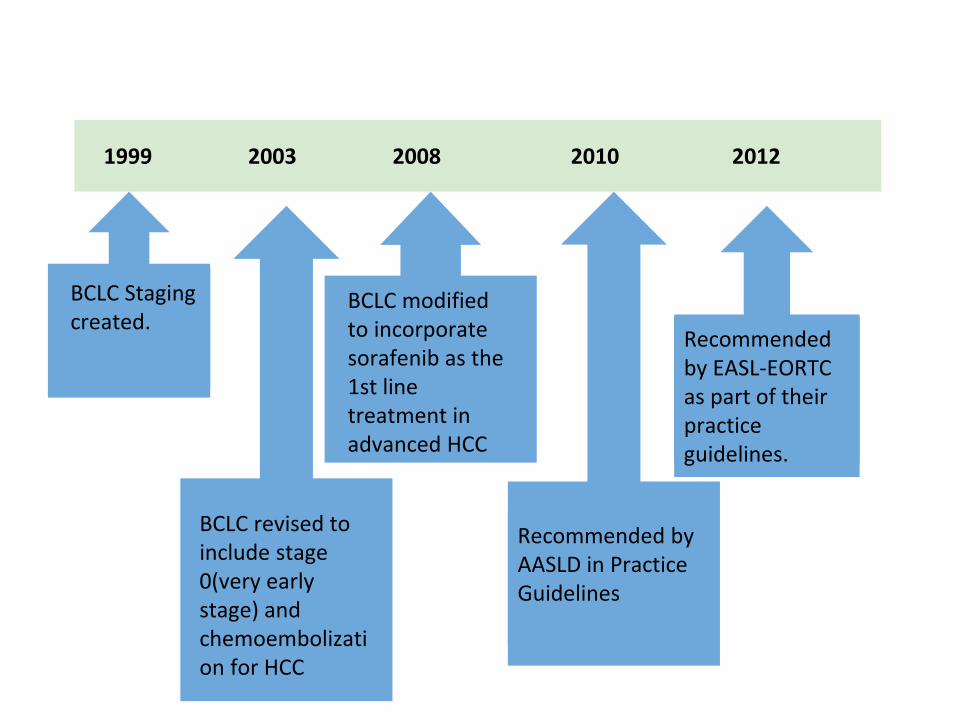
1999 2003 2008 2010 2012
BCLC Staging created.
BCLC revised to include stage 0(very early stage) and chemoembolization for HCC
BCLC modified to incorporate sorafenib as the 1st line treatment in advanced HCC
Recommended by AASLD in Practice Guidelines
Recommended by EASL-EORTC as part of their practice guidelines.
BCLCBased on several cohort studies and RCTs by the barcelona group.Has 5 stages - 0, A, B, C, D
Prognostic variables based on 1. Tumor factors (size, number, vascular invasion, N1, M1)2. Liver function (Child–Pugh’s) 3. Health status of the patient.(ECOG)
Treatment allocation variables -1. Bilirubin2. Portal hypertension3. Presence of symptoms-ECOG.
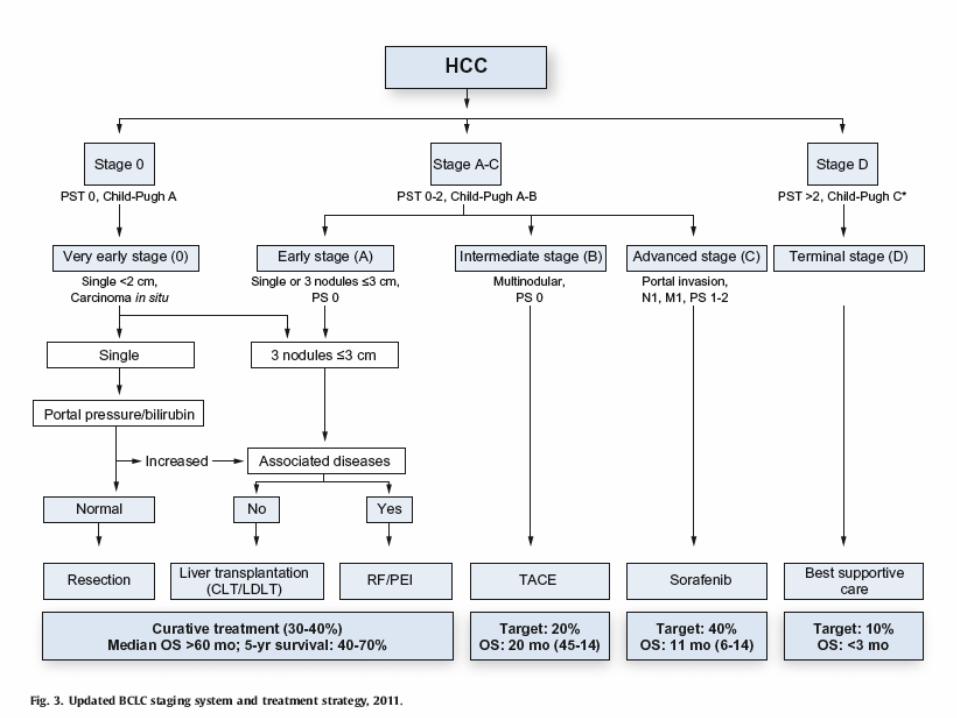

BCLC STAGES
Stage 0 -
• Very early HCC
• Single tumor < 2 cm in diameter
• Without vascular invasion or satellites
• ECOG-0
• Child-Pugh Class A
• 5-10 % detected in this stage.

STAGE A
• Early HCC
• single tumor > 2cm
OR
3 nodules <3 cm diameter.
• ECOG-0
• Child Pugh class A or B
STAGE B
Multinodular tumors
Asymptomatic
Poor candidates for resection.
STAGE C
• Advanced HCC
• Symptomatic tumors
• ECOG 1-2
• Macrovascular invasion
• Extrahepatic spread

STAGE D
• End stage HCC
• Symptomatic tumors
• Tumor related disability ECOG 3-4


Stage migration
• For treatment allocation.
• All patients do not fulfil all the criterias of a particular stage.
• Provide next most suitable option.

Surgical resection
First line treatment option for
• solitary tumors with well preserved liver function.
• Multifocal tumors meeting Milan criteria ( less than or equal to 3 nodules less than or equal to 3 cm)
In case of recurrence re-assess patient with BCLC.

Liver transplantation
First line treatment option for
• single tumors less than 5 cm with liver dysfunction
• tumors adhering to Milan criteria not suitable for resection.
Five year survival - 70%
Neo-adjuvant therapy can be considered if waiting list exceeds 6 months.

Local ablation
1. Radiofrequency ablation.
2. Percutaneous ethanol injection.
• Standard of care for BCLC 0-A not suitable for surgery.
• In BCLC 0 and tumors less than 2 cm -complete response in 90%.
TACE
BCLC stage B
• Multinodular asymptomatic tumors without vascular invasion or extrahepatic spread.
• Most widely used primary therapy for unresectableHCC.
• Rationale - strong cytotoxic and ischemic effect
• Delays tumor progression and macrovascularinvasion.
• Increases mean survival from 16 months to 20 months.

Sorafenib
Indications
• Child Pugh Class A
• BCLC stage C
• tumors progressing on loco-regional therapies.
Oral multi-tyrosine kinase inhibitor.
Only drug with survival benefit in HCC.

Stage D
Pallitative support
• Pain
• Nutrition
• Psychological support.


References
I. Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19:329–338
II. ASSLD Practice guideline 2010
III. EASL–EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma, Journal of Hepatology, Volume 56, Issue 4, April 2012







