

Belang van cytogenetica bij CLL
Barbara Cauwelier
Voorjaarssymposium Hematologie 23.4.2016
FISH

Conventional karyotyping
Recurrent aberrations in CLL
Gahrton, Blood 1980
• Low mitotic index : only 40% aberrations >> 80% after B cell stimulation CpG-IL2
• sub-optimal quality of oncological metaphases
• Low sensitivity: 3/20 metaphases
• Low resolution (10 Mb) : del 13q > del 17p often missed
• Laborintensive (2-3 W)
• Expertise
• Whole genome
• Balanced / unbalanced translocations
• Cheap
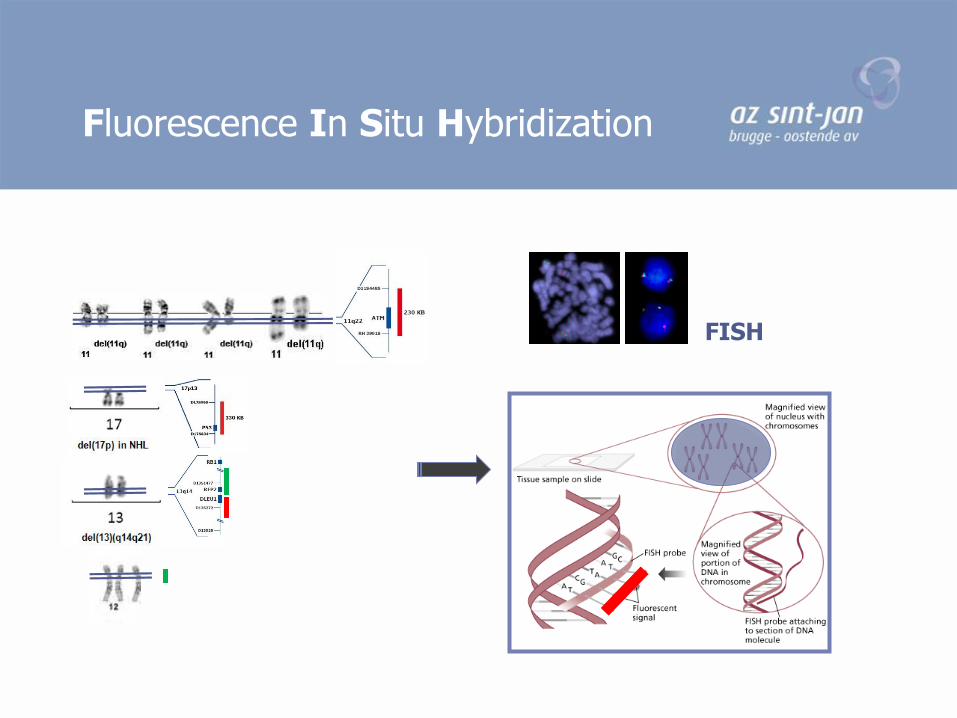
Fluorescence In Situ Hybridization
FISH

Cytogenetic prognostic markers of CLL
Interphase FISH ; 325 CLL
>80% aberrations 5 cytogenetic risk groups:
17p deletion (TP53) 7% 4%11q deletion (ATM) 18% 9%Trisomy 12 16% 12%Normal 18% 33%13q deletion (RB1) 55% 46%
clinical characteristics : •TP53 deletion: fludarabine resistence•Trisomy 12 : atypical morphology•ATM deletion: lymphadenopathy
Döhner et al N Engl J Med 2000Hernandez et al Haematologica, 2009
Interphase FISH ; 350 CLL

• No need for dividing cells (smears, imprints, FFPE)
• Higher sensitivity : 5/100
• Higher resolution : 100-200 kb vb del 13q/del 17p
• Fast (2d)
• Semi-quantitative
• Targeted :TP53,ATM,RB1,CEP12
• New translocations
• Expensive : € 20 per probe (€ 100 per patient)
• Not suited for MRD ; only at diagnosis/transformation
• Expertise interpretation/labourintensive
Fluorescence In Situ Hybridization

Comparative Genomic Hybridization on array
Array : slide imprinted with BAC (FISH) clones or oligonucleotides selected throughoutthe whole genome (or region of interest)
Hybridisation of tumor DNA vs normal DNA (Comparative)
High resolution *BAC clones: cfr FISH (100-200kb)
*oligonucleotides: 60 bp
* SNPs (single nucleotide) : aUPD
Array CGH
BAC aCGH
Oligo aCGH

• Whole genome
• High resolution
• Deletions/amplifications (incl cryptic or new)
• Unbalanced translocations
• Low quality DNA (FFPE)
• ‘Simple’ interpretation
• Balanced translocations
• Normal copy number variants (CNV)
• Tumorsize at least 20%
• No quantitative result
Molecular karyotyping

Detection rate of prognostic markers
by different cytogenetic techniques
Karyotype aCGH FISH
del (13)(q14) 3(17 missed :
0.6 Mb-16 Mb)
20 20
afwijkend mannelijk:
del(13)(q14.11q21.1)
del(13)(q14) aanwezig in
45% van de cellen 46,XY,del (13)(Q14Q21) (8)
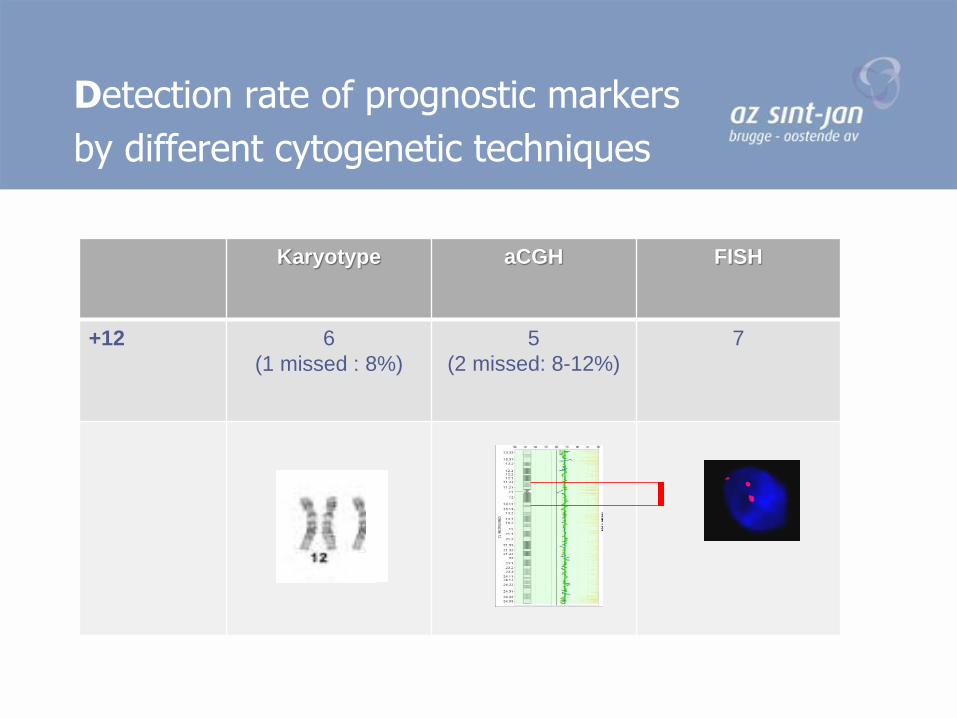
Karyotype aCGH FISH
+12 6
(1 missed : 8%)
5
(2 missed: 8-12%)
7
Detection rate of prognostic markers
by different cytogenetic techniques

Karyotype aCGH FISH
del (11)(q22) 3
(1 missed : 10%)
4 4
Detection rate of prognostic markers
by different cytogenetic techniques
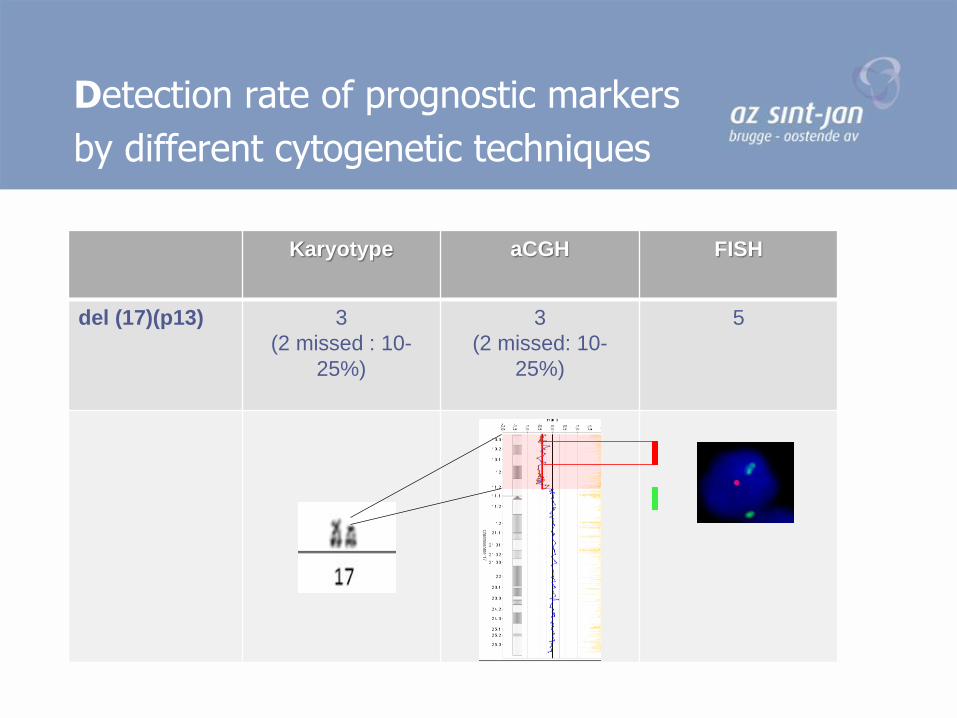
Karyotype aCGH FISH
del (17)(p13) 3
(2 missed : 10-
25%)
3
(2 missed: 10-
25%)
5
Detection rate of prognostic markers
by different cytogenetic techniques

13q14 deletions :
55% of CLL, similar frequency in CLL-MBL (early event)
Isolated : Good prognosis
Array CGH Heterogeneous !
MDR: miR-15a and miR16-1 : tumor suppressor genes ; downregulation leads to increased BCL2 expression
Cytogenetic prognostic markers of CLL : What’s new ?
RB1
MDR: miR-15a and miR16-1
Y Pekarsky1and C M Croce1
Cell Death and Differentiation (2015)
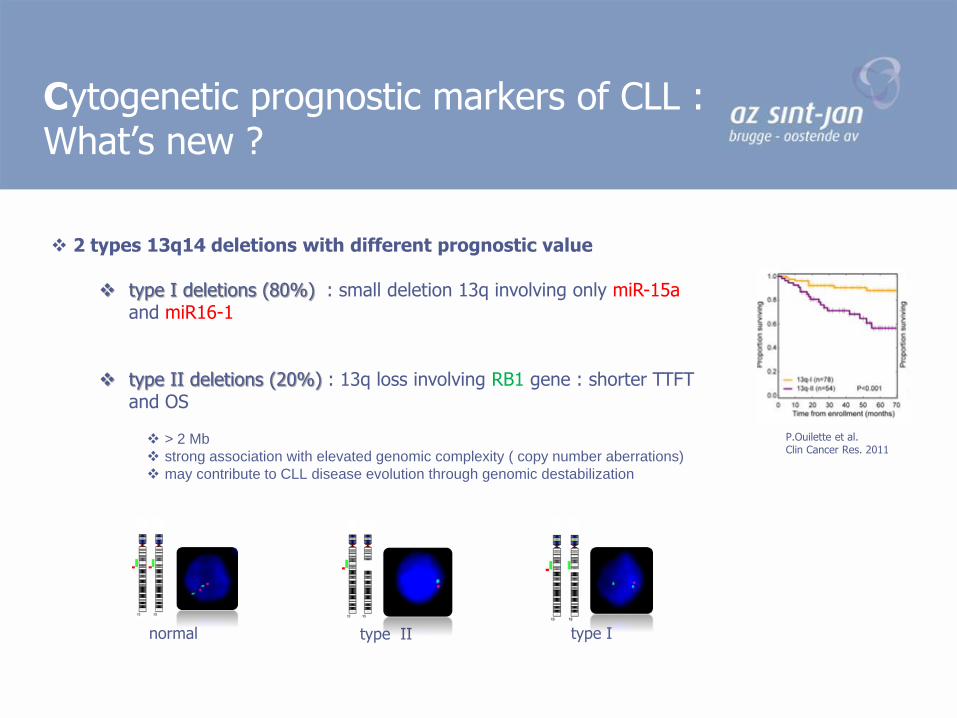
2 types 13q14 deletions with different prognostic value
type I deletions (80%) : small deletion 13q involving only miR-15aand miR16-1
type II deletions (20%) : 13q loss involving RB1 gene : shorter TTFT and OS
> 2 Mb
strong association with elevated genomic complexity ( copy number aberrations)
may contribute to CLL disease evolution through genomic destabilization
P.Ouilette et al. Clin Cancer Res. 2011
Cytogenetic prognostic markers of CLL : What’s new ?
normal type II type I

Biallelic loss of 13q14 in 30% of 13q deleted CLLs (2013)
small type I deletions evolution of monoallelic 13q14 deletion : more aggressive ? no significant differences in clinical outcome by different studies
Higher percentage of 13q14 deleted nuclei : > 80 % deleted nuclei
overexpression of genes involved in proliferation ≈ % deleted nuclei Higher lymphocyte count, diffuse bone marrow infiltration significant shorter TTFT and OS than normal karyotype gene expression pattern similar to 11q- cases
Although heterogeneity of 13q deletion, studies that integrate molecular
and cytogenetic data keep 13q deletion as very low-risk group
Cytogenetic prognostic markers of CLL : What’s new ?
Hernandez et al Haematologica, 2009

Trisomy 12
Clonal driver mutation (early in CLL )
10-20% of CLL, 8-22% of MBL (both HC and LC-MBL)
Often unique cytogenetic aberration (40-60%)
Atypical morphology and immunophenotype
Atypical morphology : CLL with > 10% larger lymphocytes with cleft and folded nuclei, CLL-PL
Atypical immunophenotype : FMC7+, bright sIg expression, Catovsky score < 3/5
Diagnostic for (atypical) CLL : DD Mantle cell lymphoma
CLL with trisomy 12 : mostly catovsky score < 3/5 and CD200 – (cfr MCL), CCND1/BCL1 negative
Cytogenetic prognostic markers of CLL : What’s new ?

Trisomy 12
- Prognosis : First studies : agressive clinical coarse low - intermediate
• depending on the presence of concurrent mutations or deletions
• Patients with trisomy 12 in the absence of TP53, NOTCH1 or other mutations have similarsurvival than those with normal FISH findings
• Patients with trisomy 12 and NOTCH 1/ SF3B1 mutations have similar survival as del 11q22

Del 17p (TP53)
3-8% of CLL diagnosis; up to 30% in refractory CLL patiënts Highest risk category No response to standard treatment for CLL
(FC: fludarabine-cyclofosfamide) or FCR (FC+rituximab)
Percentage of 17p deleted nuclei prognostic important
cut-off : 20-25%
clone size has a negative impact on OS and response to treatment as a continious variable
Rare cryptic deletions 17p can be detected by aCGH
smaller than FISH probes
Additional mutations in TP53 non-deleted allele :
75% of del 17p, 5% in non del 17p Sanger sequencing/NGS Monoallelic inactivation of TP53 is enough for resistance to treatment and clonal selection
Delgado et al. BJH 2012
Del 11q (ATM)
10-15% of CLL diagnosis; 30% in refractory CLL
Large deletions (>20 Mb) including entire ATM gene
Clinically progressive disease , lymphadenopathy, shorter TTFT, lower treatment response following standard chemotherapy (FC)
Percentage of 11q deleted nuclei prognostic important
<25% 11q deleted nuclei experienced longer TTFT compared with patients with ≥25% 11q deleted nuclei and also showed better response to treatments
(Marasca et al, Hematolgical Oncology 2013)
Genetic mutations associated with higher percentage (>40%) of 11q deleted cells :
SF3B1, NOTCH1, TP53, BIRC3 (not for ATM)
(Hernandez et al, PLOS 2015)

Del 11q (ATM)
ATM deletions mostly include the BIRC3 gene
11q deleted CLL : 83% including BIRC3 gene ATM or BIRC3 responsible for worse prognosis ?
ATM mutation rather than BIRC3 deletion or mutation predicts reduced survival in 11q deleted CLL (Rose-Zerilli, Haematologica 2014)
Additional mutations in ATM in non-deleted allele :
31% ATM mutations in del 11q (ex 3-59, no hotspots)
5% BIRC3 mutations , mostly associated with BIRC3 deletion Monoallelic inactivation of ATM by eiter deletion or mutation is not enough for
impaired therapy response; biallelic ATM lesions as bad as TP53 alterations

Which cytogenetic test at CLL diagnosis/ evolution ?
Karyotyping aCGH FISH
Known
prognostic
factors
+12, del11q +12, del11q, del 13q, del17p
except for small clones ( < 20%)
+12, del11q, del 13q, del17p
(cut-off 5%)
Additional
findings
Chromosomal translocations :
27%
IgH, 13q14, other B-NHL
other genome loss or gain
detection of (novel)
cryptic aberrations (del17p)
Clinical
importance
Complex karyotype (> 3) or
unbalanced translocations :
13,6% poor prognosis (often
associated with del11q or del17p)
6q deletions (9 %): ?
2p gain (MYCN): up to 28% , risk
of transformation Richter, shorter
OS
8p+, 8q+ : 2-5% : shorter OS?
MYC : < 1% ; transformation;
poor prognosis
diagnosis
evolution







