

1
HYPOFRACTIONATION AND DRUGS:OPPORTUNITIES AND CHALLENGES
Branislav Jeremic, MD, PhD
Professor and Head
Division of Radiation Oncology
Stellenbosch University and TygerbergHospital
Cape Town
South Africa

2
CONFLICT OF INTEREST
NONE TO DECLARE

Fakulteit Geneeskunde en Gesondheidswetenskappe
Faculty of Medicine and Health Sciences
RADIOTHERAPY AND DRUGSEXPLOITABLE MECHANISMS
1. SPATIAL CO-OPERATION
2. INDEPENDENT CELL KILL
3. PROTECTION OF NORMAL TISSUES
4. ENHANCEMENT OF TUMOUR RESPONSE
____________________________________________________
____
Steel & Peckham, 1979
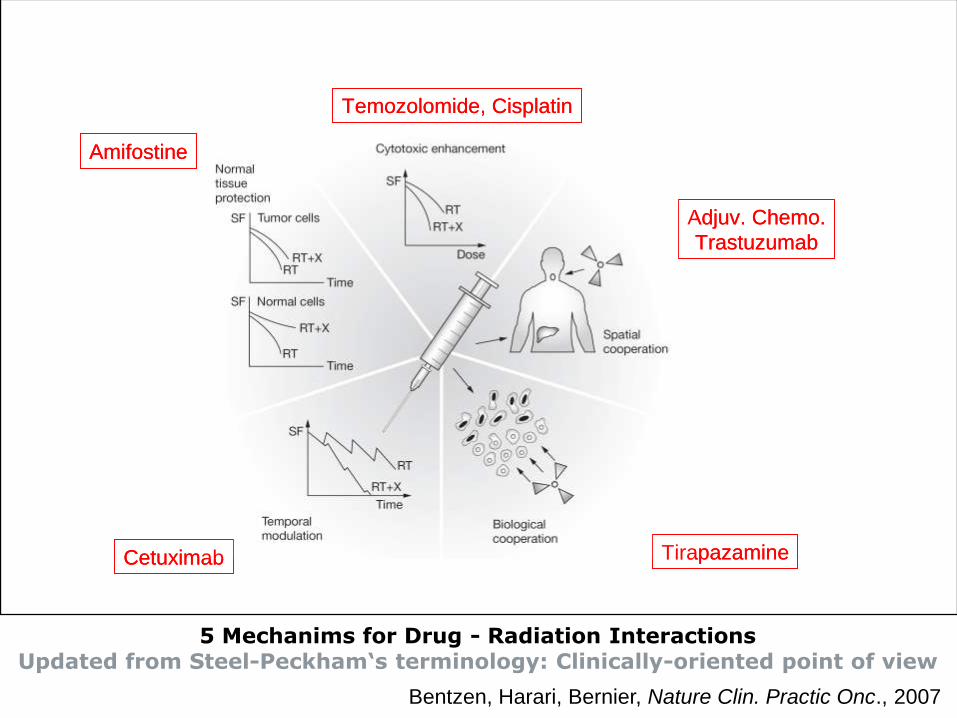
Tirapazamine
Temozolomide, Cisplatin
Amifostine
Cetuximab
Adjuv. Chemo.
Trastuzumab
Tirapazamine
Temozolomide, Cisplatin
Amifostine
Cetuximab
Adjuv. Chemo.
Trastuzumab
5 Mechanims for Drug - Radiation InteractionsUpdated from Steel-Peckham‘s terminology: Clinically-oriented point of view
Bentzen, Harari, Bernier, Nature Clin. Practic Onc., 2007

5
DOSE/FRACTIONATION
• Majority of studies with conventional fractionation
• Hypofractionation (HypoFx) mostly used in palliation
• LQ warning about HypoFx (alone or with drugs)
• More HypoFx radical regimens in recent years
• HypoFx and drugs???

6
HypoFx issues – indirect
• RT and drugs given in lower doses – most effective
• Greatest RT-enhancement with drugs given
immediately before the RT fraction
• Dose-escalation may not be effective in RT + drugs
because cytotoxicity and radiosenzitization may be
mutually exclusive

7
HypoFx issues – direct
• Hypoxia expected to be significant with HypoFx RT
• Loss <3 logs of cell-kill when CF changed into HypoFx
• Hypoxia may have the largest negative effect on cell
survival after RT given with less than ca. 10 Fx
• Is LQ appropriate for high dose/Fx ?
(5 Gy, 10 Gy, 15-18 Gy)

8
HypoFx issues – direct
High dose/Fx may enhance cell killing
• Rapid endothelial cell apoptosis in tumour vessels
• Non-targeted pharmacodynamics effects mediated by
TNF-α, TRAIL, PAR-4, ceramide
(intratumoural bystander and abscopal effects)
• Increased host immune recognition of RT-induced
enhanced antigen presentation – enhance RT effects
• Better response of heterogenous tumours with
different cell populations whose clonal radiosensitivity
considerably differs

Impact of high-dose ablative RT on
tumor micro-environment components
9
Tumour cells
Cancer stem cells
T cells
B cell response
Endothelial cells
Hypoxic cells
Metastatic tumour killImmune activation
High-dose RT
Bystander/abscopal effects
Hypoxic cell damage Endothelial cell damage

10
TYPES OF HypoFx
EXTREME
1-5 fractions
dose/fx >10 Gy
MODERATE
6-15 fractions
dose/fx 5-10 Gy
MILD
15-25 fractions
dose/fx 2.5-5 Gy

11
HypoFx and DRUGSimportant issues
• SEQUEENCING
• DRUGS
• DOSAGES
• POTENTIAL ADVANTAGES
• POTENTIAL DISADVANTAGES
• POTENTIAL CLINICAL SITES

12
EXTREME HypoFX
1-5 Fx RT
SEQUENCING
• Likely not concurrent
• Neoadjuvant and/or adjuvant
• Duration of each
• Drugs will affect mostly subclinical disease
• Efficacy will depend on micrometastatic potential
• DM rates as guidance?

13
EXTREME HypoFX
1-5 Fx RT
DRUGS
• Chemo, hormonal, targeted
• Hypoxic cell sensitizers
• Opportunity for dublets and triplets
• Similarity with drug therapy alone

14
EXTREME HypoFX
1-5 Fx RT
DOSAGES
• Similar to drug therapy alone
• Dependent of efficacy and toxicity
• Dependent on the number of cycles
• Dependent on maintenance (or not)

15
EXTREME HypoFX
1-5 Fx RT
POTENTIAL ADVANTAGES
• Treat subclinical disease early
• Enable more cycles to be given
• Should not compromise RT delivery
• May enable non-cross resistance

16
EXTREME HypoFX
1-5 Fx RT
POTENTIAL DISADVANTAGES
• Local Tx (RT) starts late
• Risks of impaired local control
• Drugs may not be effective, yet toxic
• No influence on local control
• Too toxic if drugs given close to RT?

17
EXTREME HypoFX
1-5 Fx RT
POTENTIAL CLINICAL SITES
EARLY STAGE NSCLC
• Adjuvant and/or maintenance drugs
• Possibility of chemo and targeted
• Total of 4-6 cycles
• Hypoxic cell sensitizer given with RT?
• RT- and drug-related toxicity not to overlap


RTOG 0236:
SBRT in medical inoperable stage I NSCLC
Phase II, 2004-2006
55 inoperable patients,
peripheral T1-T2 NSCLC, <5 cm
54 Gy in 3 fxs over 1.5-2 weeks.
3 Year endpoints (Median f/u 2.9 years)
Tumor control – 98% (95%CI 84.3-99.7%)
LRC – 87% (95%CI 71-94.7%)
OS – 55.8 % (95%CI 41.6-67.9%)
Toxicity: Grade 3 (13%), Grade 4 (4%)

RTOG 0236:
SBRT in medical inoperable stage I NSCLC
(Timmerman et al: JAMA 303:1070, 2010)
Phase II, 2004-2006
55 inoperable patients,
peripheral T1-T2 NSCLC, <5 cm
54 Gy in 3 fxs over 1.5-2 weeks.
3 Year endpoints (Median f/u 2.9 years)
Tumor control – 98% (95%CI 84.3-99.7%)
LRC – 87% (95%CI 71-94.7%)
OS – 55.8 % (95%CI 41.6-67.9%)
Toxicity: Grade 3 (13%), Grade 4 (4%)

SBRT in stage I NSCLC1-yr, 2-yr OS rates: 93.0% and 78.2%
(Chang et al: ASTRO 2011)
MST = 60 mos
LC : 98.5% at 2yrs
LN: 8.5%
DM: 23.1%
No G 4/5 toxicity
G2 RP: 10.7%
G3 RP : 3.1%

21
MODERATE HypoFX
6-15 Fx RT
SEQUENCING
• Likely “limited” concurrent
• Neoadjuvant and/or adjuvant still predominate
• Duration of each
• Drugs will affect both T and N and M component
• LRC vs DM rates as guidance?

22
MODERATE HypoFX
6-15 Fx RT
DRUGS
• Chemo, hormonal, targeted
• Less hypoxic cell sensitizers
• Opportunity for dublets and triplets
• Similarity with drug therapy alone

23
MODERATE HypoFX
6-15 Fx RT
DOSAGES
• Similar to drug therapy alone
• Dependent of efficacy and toxicity
• Concurrent part may be more toxic
• Dependent on the number of cycles
• Dependent on maintenance (or not)

24
MODERATE HypoFX
6-15 Fx RT
POTENTIAL ADVANTAGES
• Treat subclinical disease early
• As early as possible start concurrent part
• Should not compromise RT-drug delivery
• May enable non-cross resistance
• May require different drugs post-RT/drugs

25
MODERATE HypoFX
6-15 Fx RT
POTENTIAL DISADVANTAGES
• Local Tx (RT) starts late
• Risks of impaired local control
• Drugs may not be effective, yet toxic
• Too toxic if drugs given pre-, during and post-RT
26
MODERATE HypoFX
6-15 Fx RT
POTENTIAL CLINICAL SITES
PANCREAS, BREAST
• Adjuvant and/or concurrent and/or maintenance?
• Possibility of chemo and targeted
• Total of # cycles dependent on concurrent part
• RT- and drug-related toxicity not to overlap

27
MILD HypoFX
16 - 25 Fx RT
SEQUENCING
• Concurrent part predominates
• Neoadjuvant and/or adjuvant still possible
• Duration of each important
• Drugs will affect both T and N and M component
• LRC vs DM rates as guidance?

28
MILD HypoFX
16 - 25 Fx RT
DRUGS
• Chemo, hormonal, targeted
• Likely no hypoxic cell sensitizers
• Opportunity for dublets and triplets
• Similarity with drug therapy alone

29
MILD HypoFX
16 - 25 Fx RT
DOSAGES
• Similar to drug therapy alone
• Dependent of efficacy and toxicity
• Concurrent part may be more toxic
• Dependent on the number of cycles
• Dependent on maintenance (or not)

30
MILD HypoFX
16 - 25 Fx RT
POTENTIAL ADVANTAGES
• As early as possible start concurrent part
• Should not compromise RT-drug delivery
• May enable non-cross resistance
• May require different drugs post-RT/drugs

31
MILD HypoFX
16 - 25 Fx RT
POTENTIAL DISADVANTAGES
• Induction chemo may lead to impaired local control
• Induction hormones may do good
• Drugs may not be effective, yet toxic
• Too toxic if drugs given pre-, during and post-RT

32
MILD HypoFX
16 - 25 Fx RT
POTENTIAL CLINICAL SITES
BREAST, H&N, PROSTATE, LUNG
• Concurrent +/- adjuvant +/- maintenance?
• Possibility of chemo/hormonal and targeted
• Total of # cycles dependent on concurrent part
• RT- and drug-related toxicity not to overlap

33
HypoFX and DRUGSCONCLUSIONS
• RADIOBIOLOGICAL ASPECTS REMAIN UNCLEAR
• EXTREME HypoFx/DRUGS VIRTUALLY NOT PRACTICED
• PRACTICE IT AND DOCUMENT LATE TOXICITY
• MODERATE HypoFx/DRUGS WITH DIFFERENT OPPORTUNITY
• HIGH-DOSE PALLIATION AS POTENTIAL MODEL?
• MILD HypoFx/DRUGS ALREADY IN USE
• TOXICITY ACCEPTABLE, LONGER F/U MANDATORY!

Table Mountain - a view from Western Seaboard
Gracias!







