

Neonatal/Pediatric Palliative Care
Carole Kenner, PhD, RN, FAANCarol Kuser Loser Dean/Professor

I have nothing to declare
Conflict of Interest

ObjectivesIdentify gaps in palliative care for neonatal/children/families.Describe the role of health professionals in providing palliative care.Discuss communication strategies to promote palliative care.

My Palliative Care JourneyStudent Rotation on Pediatric Oncology UnitInstructor and Staff Nurse on Unit with
Children with CancerNeonatal Intensive CareNICU DesignFamily-Centered Developmental CareNeonatal/Pediatric ELNECOK Attorney General’s Task Force On End-of-
Life/Palliative CareNational Perinatal Association (NPA) Project

The National Perinatal Association Identified Gaps In Family Centered CareOne aspect was perinatal/neonatal palliative
care.While this project focused on
perinatal/neonatal-much is applicable to pediatric
Gaps

Next Few Slides are from the NPA Project

Interdisciplinary Recommendations for
Psychosocial Support of NICU Parents
Workgroup Convened by the National Perinatal Association
Members from these OrganizationsAcademy of Neonatal Nursing National Perinatal Association
Perinatal Section of American Academy of Pediatrics
National Premature Infant Health Coalition
Association of Women’s Health, Obstetric and Neonatal Nurses
Nurse Family Partnership
Council of International Neonatal Nurses Oklahoma Infant Alliance
Healthy Mothers, Healthy Babies Postpartum Support International
March of Dimes Preeclampsia Foundation
National Association of Neonatal Nurses Society of Maternal Fetal Medicine
National Association of Neonatal Therapists
Society of Pediatric Psychology
National Association of Pediatric Nurse Practitioners
Special Care/Special Kids
National Association of Perinatal Social Workers
Transcultural Nursing Association

Participating Parent Support Organizations

Corporate and Foundation Sponsors
The Rosemary Kennedy Trust

Parent Support Sponsors
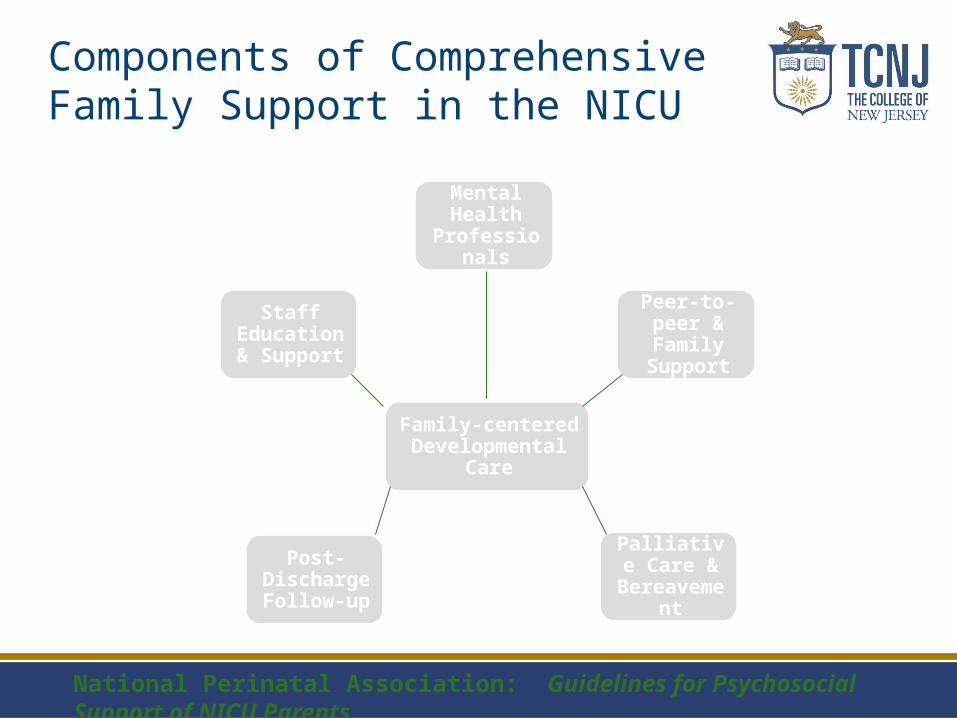
Components of Comprehensive Family Support in the NICU
Mental Health
Professionals
Peer-to-peer & Family Support
Palliative Care &
Bereavement
Post-Discharge Follow-up
Staff Education &
Support
Family-centered Developmental Care
National Perinatal Association: Guidelines for Psychosocial Support of NICU Parents

Palliative and Bereavement Care:
A Family-Centered Integrative
Approach
Recommendations for Palliative & Bereavement Care
1. All HCP that work with pregnant women, neonates and their families should receive education in palliative and bereavement care.
2. When intensive care will not be provided, a collaborative, interdisciplinary approach should be used to provide palliative and bereavement care to any family whose fetus or neonate is facing a life-limiting condition or imminent death.

Palliative & Bereavement, con’t
3. Neonatologists and NNPs should follow AAP guidelines when discussing with parents re whether to initiate or continue intensive care for a baby who may not survive. The best interests of the baby should be the guiding standard.
4. In cases of disagreements between parents and HCP re end-of-life decisions, a Bioethics consult should be obtained.

5. Parents who lose a baby should be offered:
a. Anticipatory guidance regarding the grieving process.
b. Participation in bereavement rituals.c. Psychosocial support for all members of the
family.d. Peer-to-peer support and/or referral to
community or internet support organizations.
e. Counseling re attempting another pregnancy.

More offerings…
f. Post-hospital follow-up including:
1) Individual contact by a staff member.2) Conference 4-6 weeks after baby’s death to review autopsy and other results that will help parents understand what happened.

Palliative & Bereavement, con’t
7. Palliative and bereavement care resources in the community should be available to anyone providing care to a neonate or family whether or not there is a palliative care program at a specific institution.
8. Hospitals should work with local organ donation organizations to determine whether specific babies are eligible and to assess if donation is right for a family.

Palliative & Bereavement, con’t
9. If a baby with a life-limiting condition survives to hospital discharge, parents should be offered practical and psychosocial support and/or referred to perinatal hospice. All of baby’s doctors should be involved in making and carrying out home care plans and providing follow-up support.
10.HCP providing palliative and/or bereavement care should receive psychosocial support and engage in self-care.
When losses are anticipated:
1. Parents should be offered an antenatal interdisciplinary conference to develop plans for birth, resuscitation, and palliative care if desired.
2. Parents should be encouraged to bond and to create memories with their baby during pregnancy.
3. Policies for palliative and bereavement care should be in place and easily accessible to all staff in every hospital.

So how many of these recommendations related to a child 1 year and older?
A Child’s Death
Pediatric NeedsThe child’s age will determine how we talk to
them about their illness/impending death.The parent’s wishes are important.
Sometimes they do not want the child to know how sick they are. Unfortunately the child usually do.Attempt to get both the child and parent to
realize they need to talk to each other.
End-of-Life Nursing Education Consortium (ELNEC)Modules to illustrate symptom management,
communication, resourceshttp://www.aacn.nche.edu/elnec
Neonatal/Pediatric ELNEC
The parent of a child versus a newborn has essentially the same needs.Clear communicationClear understanding of what is going to
happenIf they are taking their child home what are the
resources that they have available.What do they need to care for the child in the
home?A big challenge is that many hospice
organizations have few nurses who know pediatrics-still a small segment of patients/families they serve.
Parent Needs

Parents need follow up. The extended family may need to be included depending on the family’s wishes.
After the Death

Debriefing must be availableTalking through the experience is importantTaking time to process and reflect is
important
Care for the Health Professional

So what is the take home message?Communicate, communicate, communicateReally find out what the child and family
needs and individualize your approachMentor novice professionals in how to be less
fearful and more authentic in their care; and to admit when they do not know the answers
Recognize the impact we have on the family for the rest of their lives!
Take Home Message







