
Changing pattern of malnutrition in Ethiopia
and lessons learnt
Ferew Lemma [PhD, MPH, MD, DLSHT&M]
Senior Advisor, Office of the MinisterMinistry of Health, ETHIOPIA

Outline
Changes in patterns of under-nutrition
Lessons Learnt
Way forward

Stunting Wasting Underweight0
10
20
30
40
50
60
70
58
12
41
51
12
33
44
10
29
40
9
25
2000 2005 2011 2013/4
WHO critical threshold
WHO critical threshold
Trends in Nutritional Status of Children under 5 in Ethiopia, 2000 - 2014
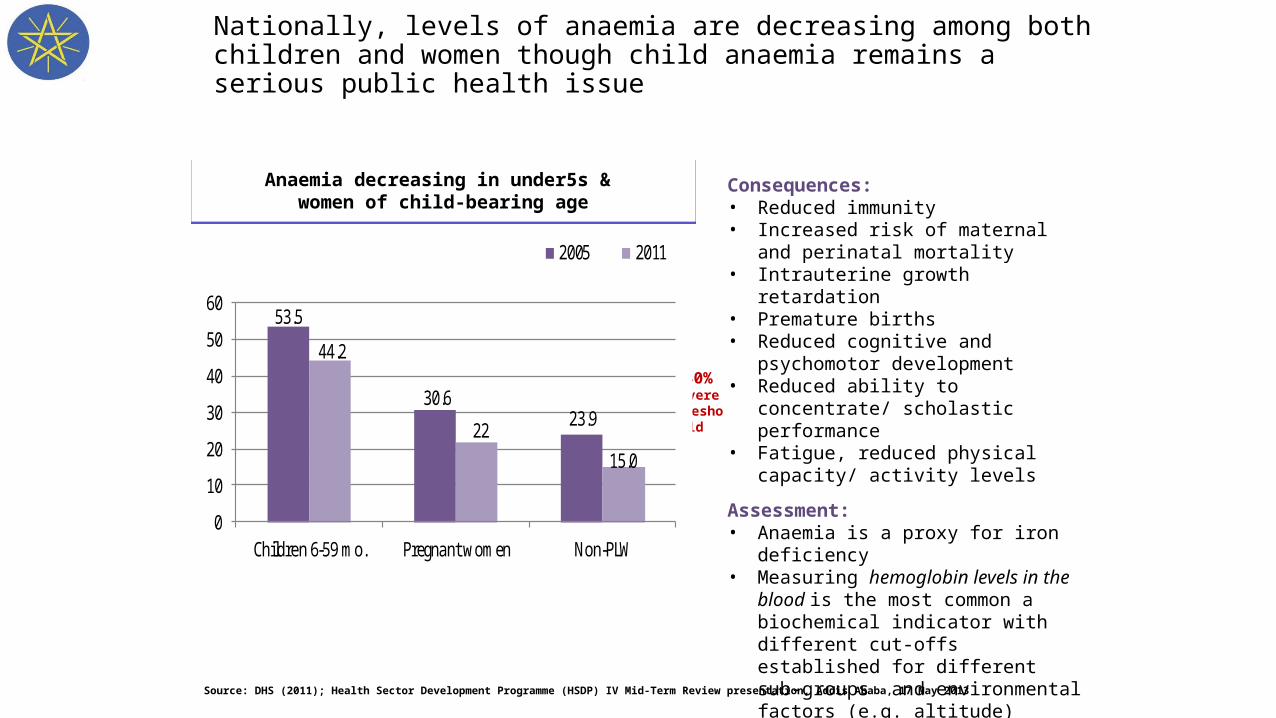
Nationally, levels of anaemia are decreasing among both children and women though child anaemia remains a serious public health issue
Anaemia decreasing in under5s & women of child-bearing age
Anaemia decreasing in under5s & women of child-bearing age
53.5
30.623.9
44.2
2215.0
0
10
20
30
40
50
60
Children 6-59 mo. Pregnant women Non-PLW
2005 2011
Source: DHS (2011); Health Sector Development Programme (HSDP) IV Mid-Term Review presentation, Addis Ababa, 17 May 2013
%
Consequences:• Reduced immunity • Increased risk of maternal and
perinatal mortality • Intrauterine growth retardation• Premature births• Reduced cognitive and psychomotor
development• Reduced ability to concentrate/
scholastic performance• Fatigue, reduced physical capacity/
activity levels
Assessment:• Anaemia is a proxy for iron deficiency • Measuring hemoglobin levels in the
blood is the most common a biochemical indicator with different cut-offs established for different sub-groups and environmental factors (e.g. altitude)
40%severe
threshold

Increases in stunting and wasting occurred in some regions from 2005 to 2011; Deterioration particularly pronounced in Afar
Change in stunting prevalence(in % points)
Change in stunting prevalence(in % points)
Not only did Affar have some of the highest stunting and wasting levels, it also had the 2nd largest increase in stunting (46.85%* to 50.2%) and
the largest increase in wasting (11.7%* to 19.5%) from 2005 to 2011 .*Note: Prevalence values for 2005 recalculated using 2006 WHO growth standards
Change in wasting prevalence(in % points)
Change in wasting prevalence(in % points)
Source: DHS (2011); DHS (2005); WHO Conversion tool from NCHS reference into estimates based on the WHO Child Growth Standards
IncreaseDecrease
0 5 5
IncreaseDecrease
05510 10+ 10+ 10+15+

In 2011, largest numbers of children with chronic (stunting) and acute (wasting) malnutrition found in the same four regions
Wasted children <5Wasted children <5
Source: DHS (2011); Ethiopia Census Report (2007); World Population Prospects, The 2010 Revision, Volume II (2011)
950,000 children
Stunted children <5 in 2011Stunted children <5 in 2011
4.6 million children
≥ 1 million
500,000-999,999
100,000-499,999
50,000-99,999
0-49,999
≥ 200,000
100,000-199,999
50,000-99,999
25,000-49,999
0-24,999

Lessons Learnt

Decisive Government commitment and leadership
8

9
60%
40%
Poorest Less poor
Poorest = 54% of population
Poorest = 20% of population
Population size
20%
2000 2011
Mean stunting prevalence
Stunting %
Stunting changes 2000-11From 2000-11 the % of the population estimated as poorest (using the same indicators) fell from 54% to 20%; the reduction in stunting was somewhat faster in the poorest group (15.0 vs13.8ppts). Mean stunting prevalences were 55.2% (2000) and 39.1% (2011).
Ethiopia data from DHSs, for children 0-59 months, national samples, 2000 and2011
58%
43%53%
38%
Poorest: those with unimproved water, roof, and toilet
Source: calculated from DHS 2000-11 data, Potts/Mason, Tulane SPHTM, 19 Feb 2015
Economic development reaching all

System Strengthening
Improving access to Primary Health CareHealth Extension Program 38,000 Health extension workers; Government salariedThroughout the country – 2 per village Provision of promotive, preventative & basic curative services
Improving access to Agriculture (services, technology) 60,000 Agriculture extension workers (3 per village) Technologies (fertilizers, improved seeds, etc)
Improved access to Education Primary Schools: from a thousand to over 32,000 Enrolment (primary) increased from 36% to 83% last 5 years
(23-80%)

Policies
Agriculture: DRM: Control of the impact of emergencies (droughts, etc.) on children and
women [CMAM sites hundreds to 14,000] Agriculture Growth Program; Productive safety net program, Livestock
Education: School Health and Nutrition Strategy school feeding program, de-worming and nutrition education
Industry: food fortification; private sector engagement
MoLSA: Social Protection policy
Dedicated nutrition unit/ focal person in the above sector offices

Overall and Specific Objectives for Mainstreaming Nutrition in AGP 2
SO 1: Improved production and productivity of diverse
foods
SO 4: Increase awareness about
nutrition
SO 6: Support research and dissemination of improved production
and post-harvest technologies
SO 5: Build capacity of staff about nutrition/ to
implement the NNP
SO 3: Improved income generating capacity of
women
Overall Objective:Improved Dietary
Consumption
SO 2: Improved post harvest handling and
food preparation, processing and
preservation

Main Challenges being addressed
Equity and quality Limited (local) evidence in nutrition – sensitive sectors; slow
engagement Information systems – accountability across sectors and
administrative levels Resources
Capacity to act at scale Tools: to guide professionals
Emergence of overweight/ obesity

“We have the means; we have the capacity to eliminate hunger from the face of the earth in our lifetime. We need only the will.”
John F. Kennedy, 1963

15AMESEGNALEHU!







