

Chest Wall Trauma
Jonathan MessingMSN, ACNP‐BC, CCRN, TCRN

Disclosures
• None

Objectives
• Describe chest wall trauma and concomitant injuries
• Compare and Contrast Standards of Care with Novel Pharmacologic Therapies
• Identify Indications, Advantages, and Disadvantages of Surgical Fixation of Fractured Ribs
Successful Completion
• To successfully complete this course, participants must attend the entire event and complete/submit the evaluation at the end of the session.
• Society of Trauma Nurses is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation.

What is the chest wall?
• Ribs• Clavicles• Sternum• Scapula
Form & Function

Protecting Important Structures
• Heart• Aorta and its branches• Pulmonary Artery• Vena Cava• Lungs• Trachea• Bronchi• Esophagus• Diaphragm

Epidemiology
Blunt Penetrating
Energy
Rib Fractures
BlastBlast
ShearShear
CompressionCompression

Lethal Injuries
AirwayAirway
O2/VentO2/Vent
HemorrhageHemorrhageCardiac FailureCardiac Failure
Cardiac TamponadeCardiac
Tamponade
Concomitant Injuries
• Simple pneumothorax• Tension Pneumothorax• Blunt cardiac injury• Pulmonary contusion• Aortic transection• Tracheobronchial injury• Livers Laceration• Kidney Laceration
• Hemothorax• Open pneumothorax• Traumatic Chylothorax• Cardiac Tamponade• Cardiac laceration• Ruptured diaphragm • Splenic Laceration
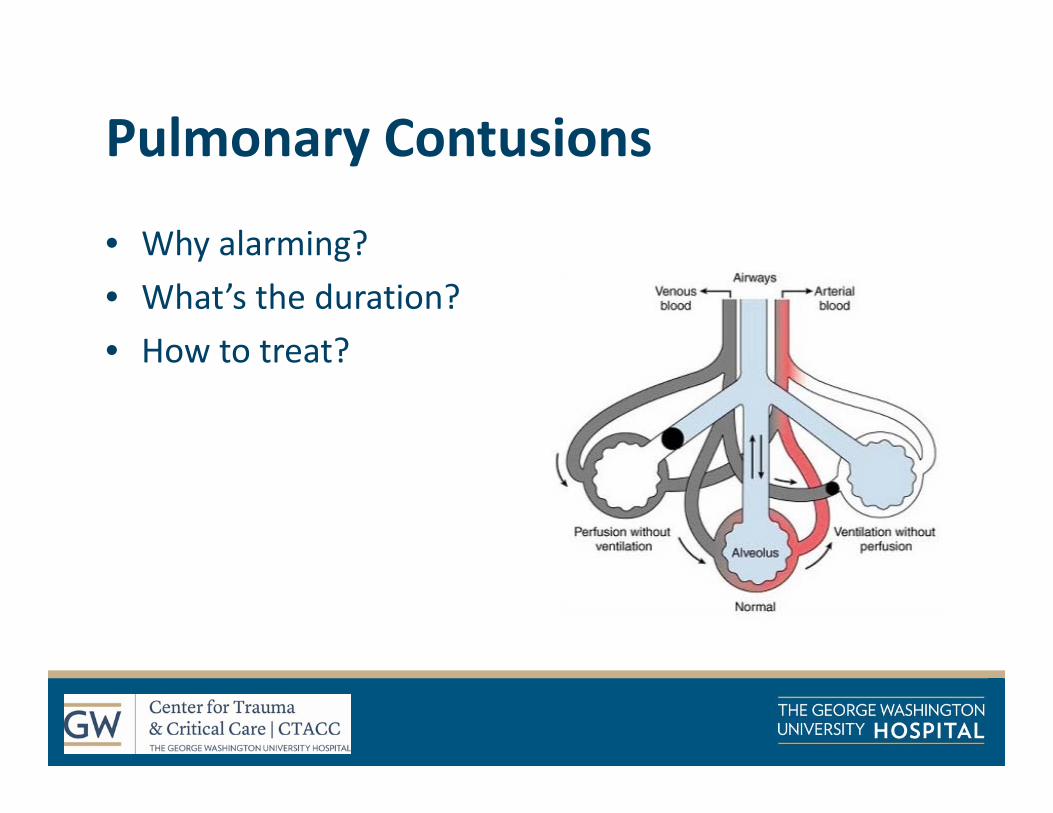
Pulmonary Contusions
• Why alarming?• What’s the duration?• How to treat?

Case I – EMS call in
• 37 F• Motorcycle crash• Decreased breath sounds on right• Right knee deformity

Where to start?
• Stick to the basics

Primary Survey
• A – Speaking, in cervical collar• B – Right sided crepitus, chest wall instability• C – palpable left radial pulse, HR 90, SBP 110, sat 96% on 2L, no gross hemorrhage
• D – GCS 15, PERRL, MAE• E – Road rash

Secondary Survey
• Head• Neck• Chest• Abdomen/Pelvis• Extremities

Imaging
Imaging
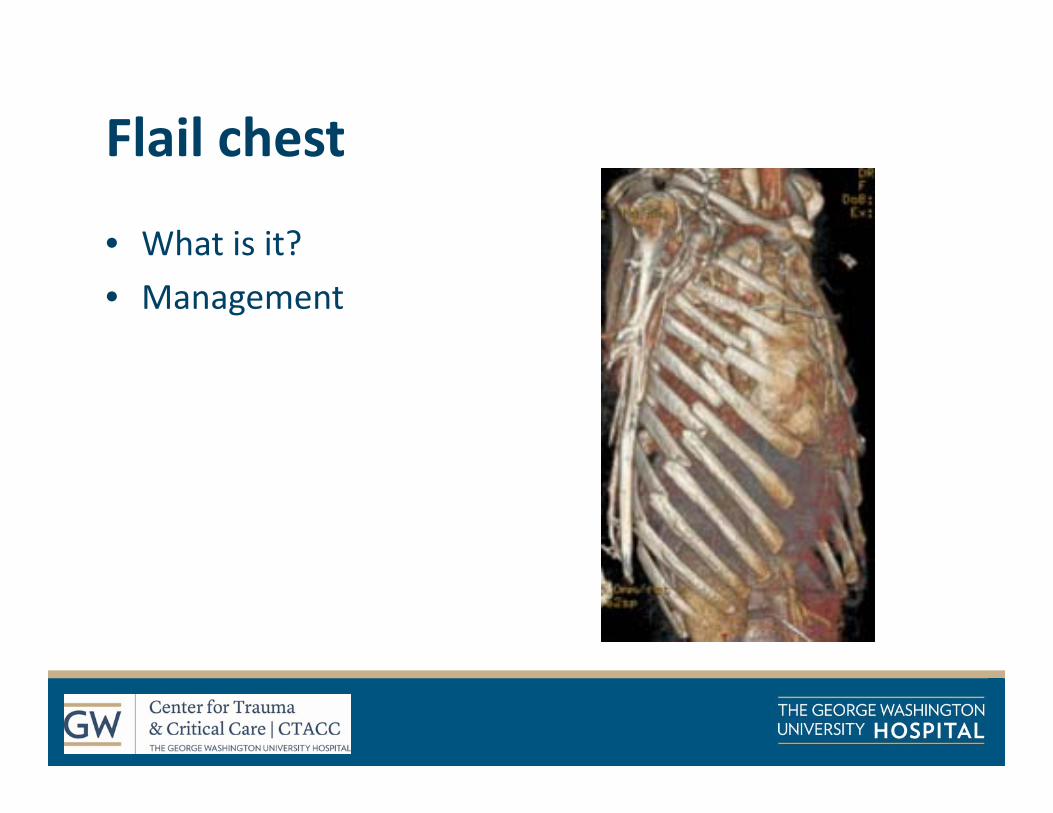
Flail chest
• What is it?• Management

What is concerning here?
• How can a rib fracture kill you?
Bergeron 2003

Bulger 2000

Holcomb 2003

Why does this matter?
Jones et al. Am J Surg 2011; 202: 598‐604

Treatment
MedicalMedical
SurgicalSurgical
NursingNursing
RecoveryRecovery

Placement
• Laws of The House of God
V. Placement comes first
‐ Samuel Shem
Brasel 2016
Medical Management
Pain ControlPain ControlMVMV
FluidsFluids

Pain in trauma
TransductionTransduction TransmissionTransmission PerceptionPerception ModulationModulation

Pain• Opioids
– Morphine– Hydromorphone– Fentanyl
• Route– IV, PO, etc.– PCA
• With/without basal• AACA
• Non‐opioids– Regional blocks– Ketamine– Acetaminophen– NSAIDs, COX‐2 inhibitors– Gabapentin– Alpha‐2 agonists– Muscle relaxants– Transdermal Lidocaine– Non‐pharmacologic
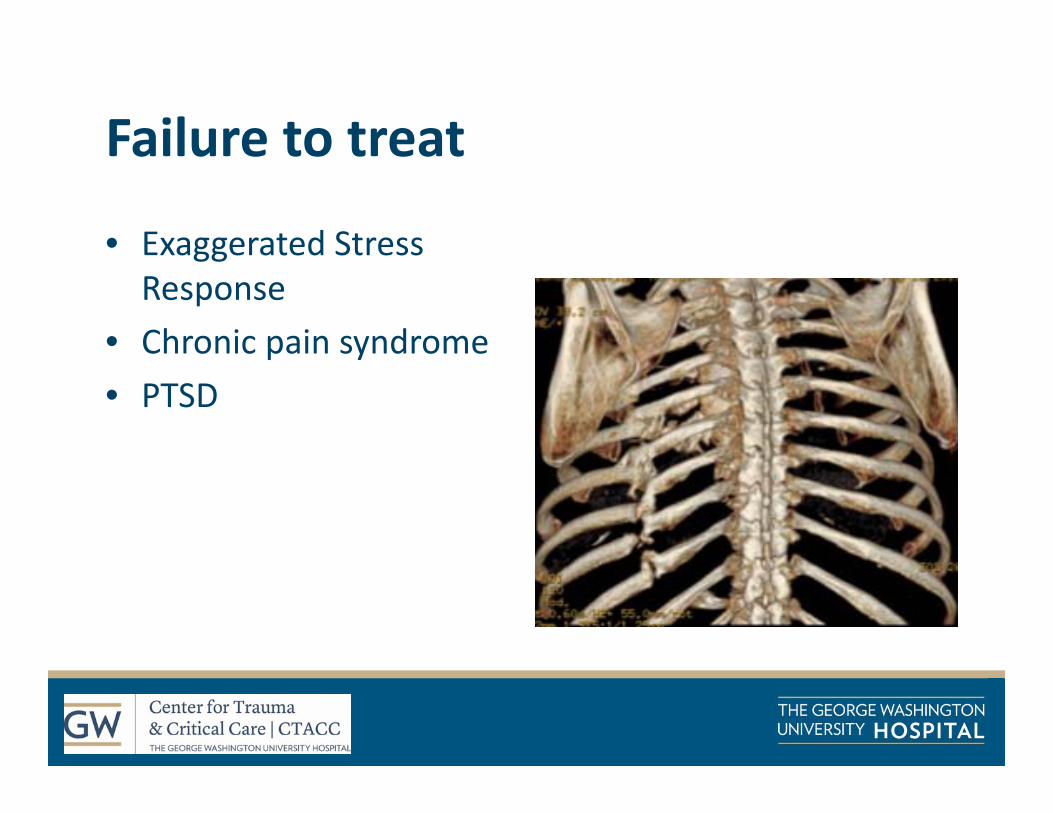
Failure to treat
• Exaggerated Stress Response
• Chronic pain syndrome• PTSD

Where to start
• Depends on the patient

Non‐opioids
Acetaminophen
Advantages
Disadvantages

Non‐opioidsNSAIDs
Advantages
Disadvantages
COX‐2 Inhibitors

Opioids
Advantages• Rapid• Effective• Numerous routes• Inexpensive
Limitations• Respiratory• CNS• GI• Heme• Derm• GU
Opioids
OpioidsOpioids
MorphineMorphine
HydromorphoneHydromorphone
FentanylFentanyl

Personally Controlled Analgesia
PCA• Saves time• Empowers patients• Provides data
AACA• Improves pain control• Saves time• Prevents higher doses
Ketamine
Category?• General anesthetic
Mechanism? Pd? Pk?• NMDA receptor antagonist• Onset: 30 seconds when IV• Duration: 5‐10 mins IV• Metabolized Hepatically

Ketamine
Adverse Reactions?• Emergence Reaction
Contraindications?• Schizophrenia• Age < 3 months• Elevated ICP?

Other options
• Transdermal Lidocaine• Lidocaine Infusions• Skeletal Muscle Relaxants• TENS

Regional blocks
Karamakar 2003

Thoracic Epidural Anesthesia
Pros• Ease of placement• Effective• Can include personally
controlled component
Cons• Hemodynamics• Coagulopathy limitations• Sympathectomy• Mobility impairment

Paravertebral Nerve Blockade
• What are they?• Advantages?• Complications?• Nursing concerns

Intercostal Nerve Blocks
• Single injection vscontinuous
• Can be tedious• Not limited by anticoagulation
Truitt 2011
Interpleural
‐ Blocks multiple dermatomes
‐ Can be lost via chest tubes

Non‐pharmacologic
• Heat• Ice• Reiki Therapy• Physical and Occupational Therapy• Repositioning• Distraction

Nursing ImplicationsNursing
Implications
Incentive SpirometryIncentive Spirometry
Out of bedOut of bed
PT/OTPT/OT
Chest PTChest PT
TheravestTheravest
TCDBTCDB

Back to our patient…
• Right ribs 3‐12 fractured• Flail chest• Pneumothorax
Case I ‐Management
• Paravertebrals• fPCA• Celecoxib• Ketamine• And…

Failure of medical management
Chen 2014; Chapman 2016

Scoring systems
Chen 2014

Chest Trauma Scoring System
Chen 2014

RibScore
6 or more rib fx 1 pointBilateral rib fx 1 pointFlail chest 1 point3 or more bicortical fx 1 point1st rib fx 1 point1 or more fx in each of 3 anatomic areas 1 point

Predicting failure
• IS• Deep breathing• Coughing• Speaking• Mobility

Surgical Fixation
• Why?• Benefits

Indications
Sarani 2015

Contraindications
Pulmonary Contusions?Pulmonary Contusions?
Severe Injuries?Severe Injuries? Instability?Instability?
Acute Resp. Failure?
Acute Resp. Failure? Infection?Infection?

What do we know so far?
• Review of studies for rib plating

Slobogean 2013

Pieracci 2016

Lengths of stay
Kocher 2016; Majercik 2014

Reduced infection

EAST PMG

Case I ‐ Rib Plating
• Hospital Day 2• Ribs 5‐9 plated through an 8 cm transverse thoracic incision
• Procedure time 1 hour 45 minutes• Extubated same day

Case I ‐ Post‐op Imaging

Post‐op care
• Chest tube?• Pain control!• Ambulation

Case II
• 71M Ped Struck• Polytrauma
• Ketamine infusion• AACA hydromorphone• Gabapentin• Transdermal lidoderm• Lidocaine infusion• Paravertebral blockade

Case II
• 0200 noted to have two episodes of seizure activity
• Head CT normal

Local Anesthetic Systemic Toxicity
Prodromal Symptoms
SeizuresLOCAgitation
CNSCNSHR changesEctopyST segment changes
Hypo/Hypertension
CVCV
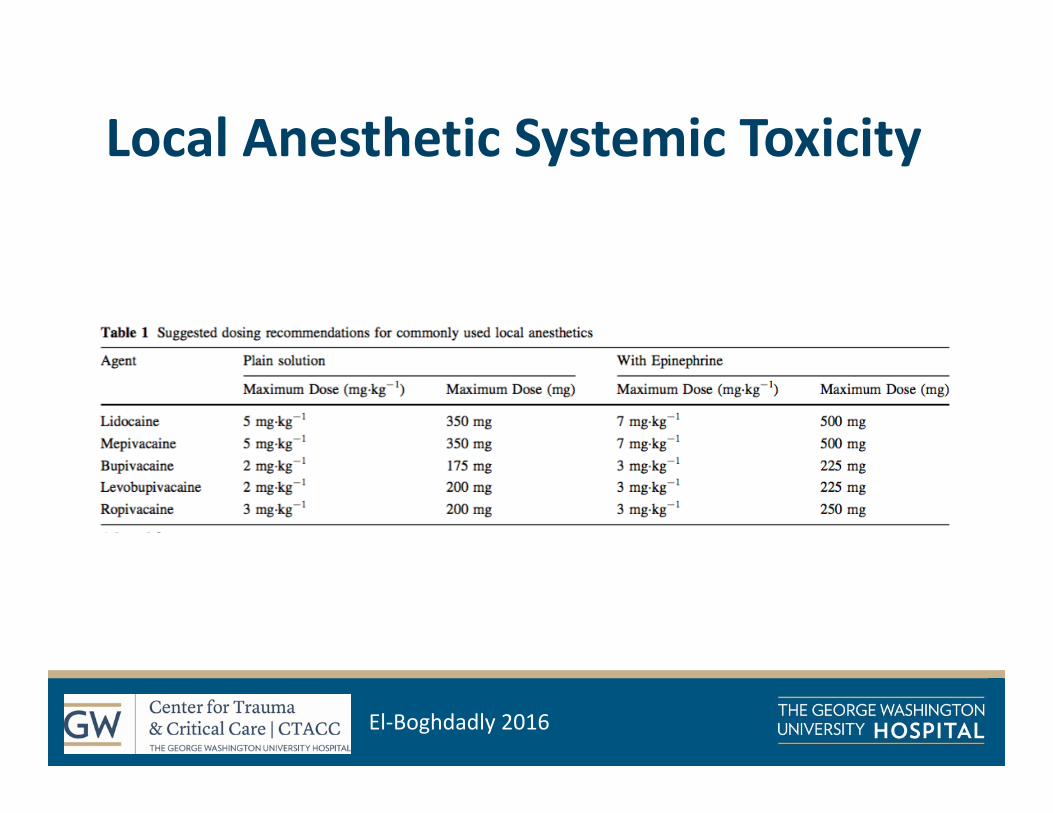
Local Anesthetic Systemic Toxicity
El‐Boghdadly 2016

Case III
• 85 yo female presents after choking on food• CPR with ROSC and normal MS• Extubated• Injuries: flail sternum, bilateral rib fractures of 2‐8
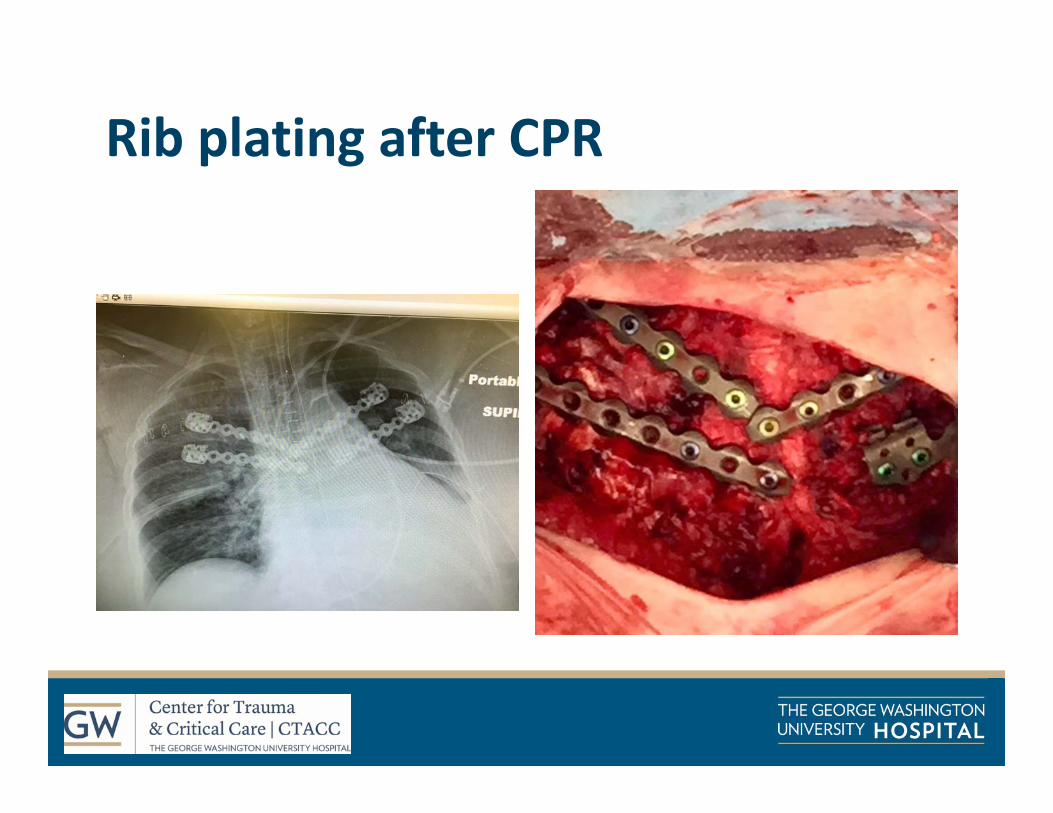
Rib plating after CPR

Take home messages
• Value the clinical exam• Advocate for our patients• Promote patient recovery• Provide multimodal pain therapy + regional blocks
• We need more data needed on SSRF, but early results promising

ReferencesBergeron E, Lavoie A, Clas D, et al. Elderly trauma patients with rib fractures are at a greater risk of death and pneumonia. J Trauma 2003; 54(3): 479‐85.
Brasel KJ, Moore EE, Albrecht RA, et al. Western Trauma Association critical decisions in trauma: management of rib fractures. J Trauma Acute Care Surg2016; 82(1): 200‐3.
Brown SD, Walters MR. Patients with rib fractures: use of incentive spirometry to guide care. J Trauma Nurs 2012; 19(2): 92‐3.
Bulger EM, Areneson MA, Mock CN, et al. Rib fractures in the elderly. J Trauma 2000; 48(6): 1040‐7.
Chapman BC, Herbert B, Rodil M, et al. Ribscore: a novel radiographic score based on fracture pattern that predicts pneumonia, respiratory failure, and tracheostomy. J Trauma Acute Care Surg 2016; 80(1): 95‐101.
Chen J, Jeremitsky E, Philp F, et al. A chest trauma scoring system to predict outcomes. Surgery 2014; 156(4): 988‐93.
Choi JJ, Lin E, Gadsden J. Regional anesthesia for trauma outside the operating theatre. Curr Opin Anaesthesiol 2013; 26(4): 495‐500.
Cooney MF, Czarnecki M, Dunwoody C, et al: American society for pain management nursing position statement with clinical practice guidelines: authorized agent controlled analgesia. Pain Manag Nurs 2013; 14(3): 176‐81.
Dickerson DM, Apfelbaum JF. Local anesthetic systemic toxicity. Aesthet Surg J 2014; 34(7): 1111‐9.
El‐Boghdadly K, Chin KJ. Local anesthestic systemic toxicity: continuing professional development. Can J Anaesth 2016; 63(3): 330‐49.

ReferencesGalvagno SM, Smith CE, Varon AJ, et al. Pain management for blunt thoracic trauma: a joint practice management guideline from the Eastern Association for the Surgery of Trauma and Trauma Anesthesiology Society. J Trauma Acute Care Surg 2016; 81(5): 936‐51.
Ho AM, Karmakar MK, Critchley LA. Acute pain management of patients with multiple rib fractures: a focus on regional techniques. Curr Opin Crit Care 2011; 17: 323‐7.
Holcomb JB, McMullin NR, Kozar RA, et al. Morbidity from rib fractures increases after age 45. J Am Coll Surg 2003; 196(4): 549‐555.
Jones KM, Reed RL, Luchette FA. Ribs or not the ribs: which influences mortality? Am J Surg 2011; 202(5): 598‐604.
Karamakar MK, Ho A. Acute pain management of patients with multiple rib fractures. J Trauma 2003; 54(3): 615‐25.
Kasotakis G, Hasenboehler EA, Streib EW, et al. Operative fixation of rib fractures after blunt trauma: a practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg 2016; ePub ahead of print.
Khandar SJ, Johnson SB, Calhoon JH. Overview of thoracic trauma in the united states. Thorac Surg Clin 2007.
Kiraly L, Schreiber M. Management of the crushed chest. Crit Care Med 2010; 38(9): s469‐77.
Kocher GJ, Sharafi S, Azenha LF, et al. Chest wall stabilization in ventilator‐dependent traumatic flail chest patients: who benefits. European Journal of Cardiothoracic Surgery 2016.
Laskowski K, Stirling A, McKay WP, et al. A systematic review of intravenous ketamine for postoperative analgesia. Can J Anesth 2011; 58: 911‐23.
Majercik S, Vijayakumar S, Olsen G, et al. Surgical stabilization of severe rib fractures decreases incidence of retained hemothorax and empyema. Am J Surg2015; 210(6): 1112‐7.

ReferencesMajercik S, Wilson E, Gardner S, et al. In‐hospital outcomes and costs of surgical stabilization versus nonoperative management of severe rib fractures. J Trauma Acute Care Surg 2014; 79(4): 533‐9.
McKay DR, Fawzy HF, McKay KM, et al. Are chest compressions safe for the patient reconstructed with sternal plates? Evaluating the safety of cardiopulmonary resuscitation using a human cadaveric model. J Cardiothoracic Surg 2010; 18.
Messing JA, Gall V, Sarani B. Successful management of severe flail chest via early operative intervention. J Trauma Nurs 2014; 21(2): 83‐5.
Oyler DR, Parli SE, Bernard AC, et al. Nonopioid management of acute pain associated with trauma: focus on pharmacologic options. J Trauma Acute Care Surg 2015; 79(3): 475‐83.
Patanwala AE, Martin JR, Erstad BL. Ketamine for analgosedation in the intensive care unit: a systematic review. J Intens Care Med 2015.
Pieracci FM, Lin Y, Rodil M, et al. A prospective, controlled clinical evaluation of surgical stabilization of severe rib fractures. J Trauma Acute Care Surg 2016; 80(2): 187‐94.
Pressley CM, Fry WR, Philp AS, et al. Predicting outcome of patients with chest wall injury. Am J Surg 2012; 204(6): 910‐3.
Rostas JW, Lively TB, Brevard SB, et al. Rib fractures and their association with solid organ injury: higher rib fractures have greater significance for solid organ injury screening. Am J Surg 2016.
Sammy IA, Chatha H, Lecky F, et al. Are first rib fractures a marker for other life‐threatening injuries in patients with major trauma? A cohort study of patients on the UK trauma audit and research network database. Emerg Med J 2017; ePub ahead of print.
Sarani B, Schulte L, Diaz J. Pitfalls associated with open reduction and internal fixation of fractured ribs. Int J Care Injured 2015; 46: 2335‐40.

ReferencesSlobogean GP, MacPherson CA, Sun T, et al. Surgical fixation vs nonoperative management of flail chest: a meta‐analysis. J Am Coll Surg 2013; 216(2): 302‐11.
Sullivan D, Lyons M, Montgomery R, et al. Exploring opioid‐sparing multimodal analgesia options in trauma: a nursing perspective. J Trauma Nurs 2016; 23(6): 361‐75.
Truitt MS, Murry J, Amos J, et al. Continuous intercostal nerve blockade for rib fractures: ready for primetime? J Trauma 2011; 71(6): 1548‐52.
Questions? [email protected]







