

1
Chronic Inflammatory Disease: An Introduction
Developed by Mike Crowe, PharmD, MBA, CSP, FMPA &
Alissa Johnson, PharmD CandidatePresented by
Mike Crowe , PharmD, MBA, CSP, FMPA
Speaker Disclosure
Michael Crowe has nothing to disclose.

2
Objectives
1. Summarize available treatments for the chronic inflammatory diseases (CIDs) rheumatoid arthritis (RA), plaque psoriasis, and Crohn’s disease.
2. Describe the etiology of CIDs.
3. Outline the pathophysiology of CIDs.
4. Explain the pharmacologic approach to treating CIDs.
3
Chronic Inflammatory Diseases (CIDs)
4
3
Immunology Introduction
Rheumatoid Arthritis
Inflammatory Bowel Disease
Psoriasis
5
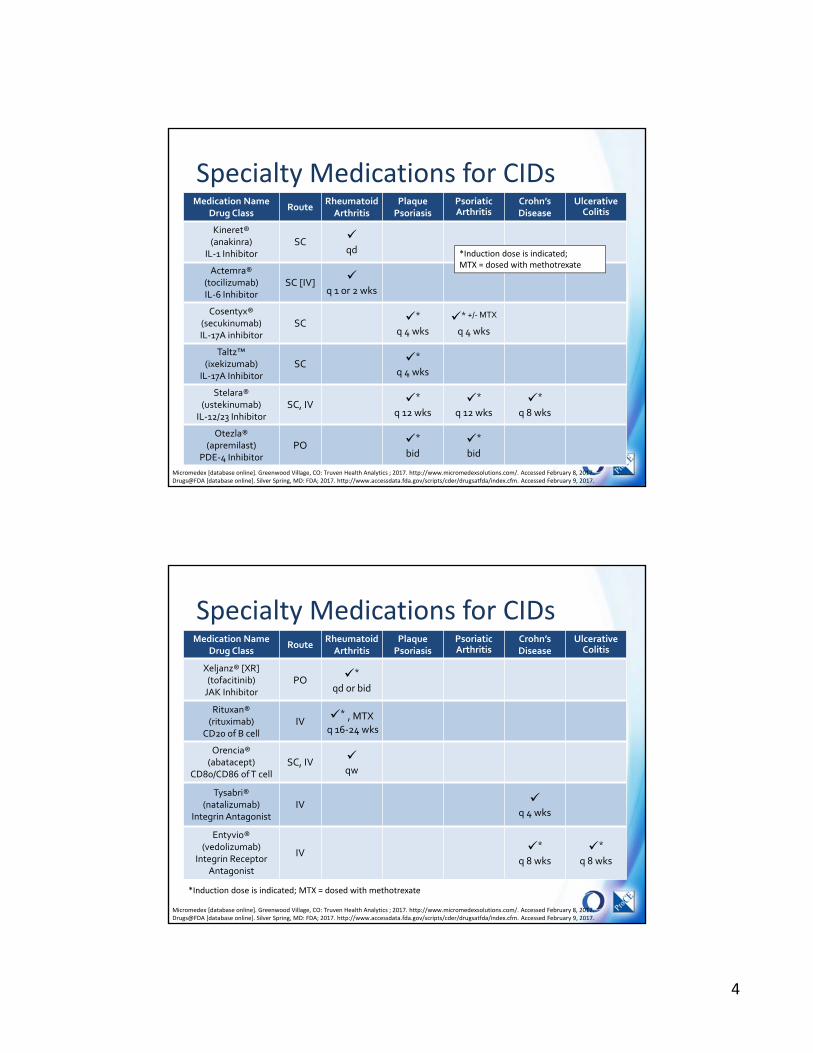
Tumor Necrosis Factor (TNF)‐α InhibitorsMedication Name
Drug ClassRoute
Rheumatoid Arthritis
Plaque Psoriasis
Psoriatic Arthritis
Crohn’s Disease
Ulcerative Colitis
Remicade® (infliximab)
TNFα InhibitorIV
*, MTX
q 4‐8 wks*
q 8 wks*
q 8 wks*
q 8 wks*
q 8 wks
Enbrel® (etanercept)
TNFα InhibitorSC
q week*
q week
q week
Humira®(adalimumab)TNFα Inhibitor
SC
q 1 or 2 wks*
qowqow
*
qow*
qow
Simponi® [AriaTM] (golimumab)TNFα Inhibitor
SC [IV] [*], MTX
q 4 [8] wks
q 4 wks
*
q 4 wks
Cimzia®(certolizumab pegol)
TNFα InhibitorSC *
q 2 or 4 wks*
qow*
q 4 wks
Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 8, 2017. Drugs@FDA [database online]. Silver Spring, MD: FDA; 2017. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm. Accessed February 9, 2017.
6
*Induction dose is indicated; MTX = dosed with methotrexate
4
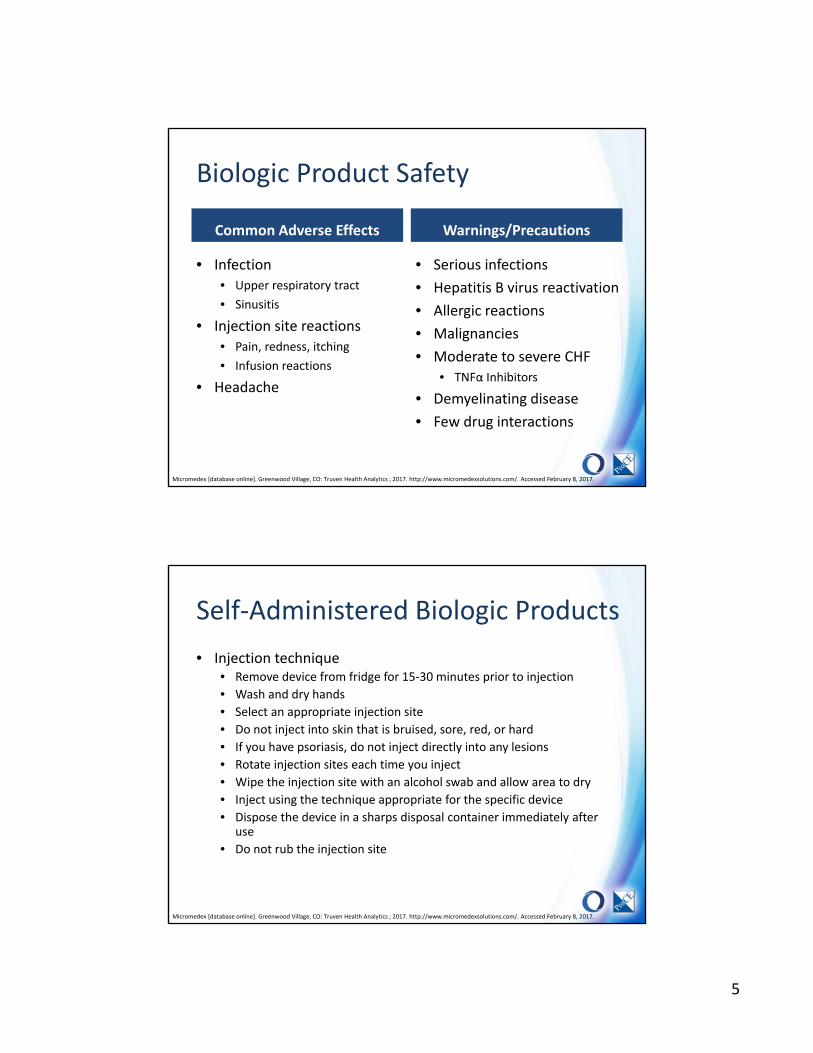
Specialty Medications for CIDsMedication Name
Drug ClassRoute
Rheumatoid Arthritis
Plaque Psoriasis
Psoriatic Arthritis
Crohn’s Disease
Ulcerative Colitis
Kineret® (anakinra)
IL‐1 InhibitorSC
qd
Actemra® (tocilizumab)IL‐6 Inhibitor
SC [IV]
q 1 or 2 wks
Cosentyx® (secukinumab)IL‐17A inhibitor
SC *
q 4 wks* +/‐MTX
q 4 wks
Taltz™ (ixekizumab)
IL‐17A InhibitorSC *
q 4 wks
Stelara® (ustekinumab)
IL‐12/23 InhibitorSC, IV *
q 12 wks*
q 12 wks*
q 8 wks
Otezla® (apremilast)
PDE‐4 InhibitorPO *
bid*
bid
Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 8, 2017. Drugs@FDA [database online]. Silver Spring, MD: FDA; 2017. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm. Accessed February 9, 2017.
*Induction dose is indicated; MTX = dosed with methotrexate
Specialty Medications for CIDsMedication Name
Drug ClassRoute
Rheumatoid Arthritis
Plaque Psoriasis
Psoriatic Arthritis
Crohn’s Disease
Ulcerative Colitis
Xeljanz® [XR](tofacitinib)JAK Inhibitor
PO *
qd or bid
Rituxan® (rituximab)
CD20 of B cellIV
* , MTX
q 16‐24 wks
Orencia® (abatacept)
CD80/CD86 of T cellSC, IV
qw
Tysabri® (natalizumab)
Integrin AntagonistIV
q 4 wks
Entyvio® (vedolizumab)
Integrin Receptor Antagonist
IV *
q 8 wks*
q 8 wks
Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 8, 2017. Drugs@FDA [database online]. Silver Spring, MD: FDA; 2017. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm. Accessed February 9, 2017.
*Induction dose is indicated; MTX = dosed with methotrexate
5
Biologic Product Safety
Common Adverse Effects
• Infection • Upper respiratory tract
• Sinusitis
• Injection site reactions• Pain, redness, itching
• Infusion reactions
• Headache
Warnings/Precautions
• Serious infections
• Hepatitis B virus reactivation
• Allergic reactions
• Malignancies
• Moderate to severe CHF• TNFα Inhibitors
• Demyelinating disease
• Few drug interactions
Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 8, 2017.
Self‐Administered Biologic Products
• Injection technique • Remove device from fridge for 15‐30 minutes prior to injection
• Wash and dry hands
• Select an appropriate injection site
• Do not inject into skin that is bruised, sore, red, or hard
• If you have psoriasis, do not inject directly into any lesions
• Rotate injection sites each time you inject
• Wipe the injection site with an alcohol swab and allow area to dry
• Inject using the technique appropriate for the specific device
• Dispose the device in a sharps disposal container immediately after use
• Do not rub the injection site
Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 8, 2017.

6
Biologic Product Counseling Points
• Storage
• Avoid live vaccines during treatment
• Notify physician of signs/symptoms of the following:
• Infection
• Hypersensitivity
• Hepatitis B reactivation
• Heart failure
• Demyelination
• Malignancy
• Expectations 11
Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 8, 2017.
RHEUMATOID ARTHRITIS
Chronic Inflammatory Disease
7
Rheumatoid Arthritis
• Chronic autoimmune disorder of the joints
• Symmetrical presentation
• Painful inflammation
• Joint deformity
• 1.3 million affected in US
• Women > Men (3:1)
• Races equally affected
Singh JA, et al. American College of Rheumatology. Arthritis Care & Research. 2015;68(1):1‐25. Wahl K, Schuna AA. Rheumatoid Arthritis. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10e. New York, NY: McGraw‐Hill; 2017.
Articular Presentation
• Pain/tenderness
• Swelling
• Morning stiffness
• Walking difficulties
• Joint deformity
Hands Wrists
Elbows Shoulders
Knees Ankles
14Singh JA, et al. American College of Rheumatology. Arthritis Care & Research. 2015;68(1):1‐25. Wahl K, Schuna AA. Rheumatoid Arthritis. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10e. New York, NY: McGraw‐Hill; 2017.

8
Pathophysiology
Immune System Fails to Recognize
Self
Increased Inflammatory Response
Inflammation of Synovial Tissues
Cartilage and Bone Erosion
15Singh JA, et al. American College of Rheumatology. Arthritis Care & Research. 2015;68(1):1‐25.
Symptomatic Therapies
Non‐Steroidal Anti‐Inflammatory Drugs
(NSAIDs)Corticosteroids
Disease Modifying Antirheumatic Drugs (DMARDs)
Traditional DMARDs Biologics
Rheumatoid Arthritis Treatment Options
Singh JA, et al. American College of Rheumatology. Arthritis Care & Research. 2015;68(1):1‐25.

9
DMARD monotherapy^
Combo DMARD tx (double/triple tx)‡^ orAnti‐TNF +/‐MTX^ or
Non‐TNF Biologic +/‐MTX^
LOW Disease Activity
MODERATE or HIGHDisease Activity
DMARD = disease modifying antirheumatic drug (includes hydroxychloroquine [HCQ], leflunomide [LEF], methotrexate [MTX], and sulfasalazine [SSZ])Anti‐TNF = anti–tumor necrosis factor (TNFα inhibitor)# Treatment target should ideally be low disease activity or remission^ Consider adding short‐term glucocorticoids (defined as <3 months) for RA disease flares‡ Combina on DMARD therapy with 2 DMARDs, which is most commonly MTX based, with some excep ons (e.g., MTX + HCQ, MTX + LEF, MTX + sulfasalazine, and sulfasalazine + HCQ), and triple therapy (MTX + HCQ + sulfasalazine)
American College of Rheumatology Guidelines
17
Treat to Target#
Another Anti‐TNF +/‐MTX^ orAnother Non‐TNF Biologic +/‐MTX^ or
Tofacitinib +/‐MTX
Singh JA, et al. American College of Rheumatology. Arthritis Care & Research. 2015;68(1):1‐25. Adapted from Figures 3 and 5.
Counseling
Avoid pregnancy (women/partners) X X
Take with food X X
Hydrate and report renal toxicity X X
Urine/skin discoloration may occur X
Report vision changes X
May cause photosensitivity X X
Report rashes immediately X X
Hepatic toxicity X X X
GI toxicity X X
Hematologic toxicity X X X
MTX LEF SSZ HCQ
Traditional DMARD Counseling
18Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics; 2017. http://www.micromedexsolutions.com/. Accessed February 9, 2017.
10
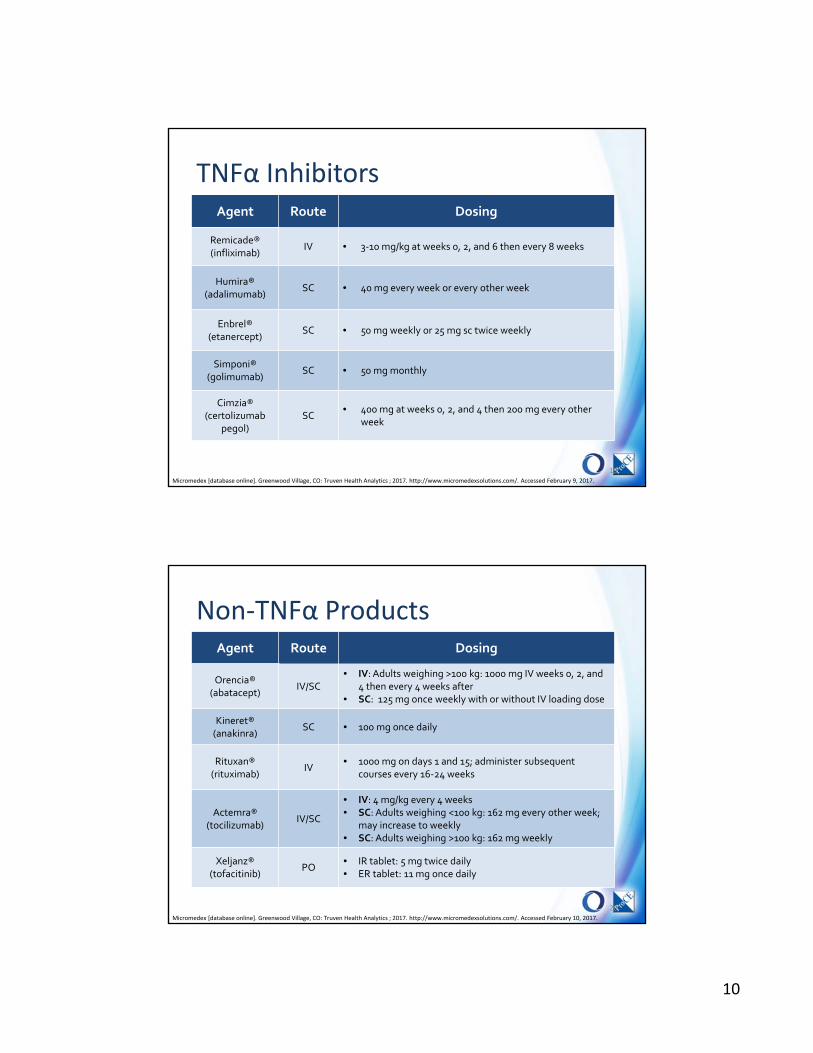
TNFα Inhibitors
19
Agent Route Dosing
Remicade®(infliximab)
IV • 3‐10 mg/kg at weeks 0, 2, and 6 then every 8 weeks
Humira®(adalimumab)
SC • 40 mg every week or every other week
Enbrel®(etanercept)
SC • 50 mg weekly or 25 mg sc twice weekly
Simponi®(golimumab)
SC • 50 mg monthly
Cimzia®(certolizumab
pegol)SC
• 400 mg at weeks 0, 2, and 4 then 200 mg every other week
Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 9, 2017.
Non‐TNFα Products
20
Agent Route Dosing
Orencia®(abatacept)
IV/SC• IV: Adults weighing >100 kg: 1000 mg IV weeks 0, 2, and
4 then every 4 weeks after• SC: 125 mg once weekly with or without IV loading dose
Kineret®(anakinra)
SC • 100 mg once daily
Rituxan®(rituximab)
IV• 1000 mg on days 1 and 15; administer subsequent
courses every 16‐24 weeks
Actemra®(tocilizumab)
IV/SC
• IV: 4 mg/kg every 4 weeks • SC: Adults weighing <100 kg: 162 mg every other week;
may increase to weekly• SC: Adults weighing >100 kg: 162 mg weekly
Xeljanz®(tofacitinib)
PO• IR tablet: 5 mg twice daily• ER tablet: 11 mg once daily
Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 10, 2017.

11
Health Assessment Questionnaire II (HAQ‐II)
• 10‐item validated questionnaire
• Common tool for measuring functioning status in rheumatology
• Looks at difficulty of completing common activities of daily living
Routine Assessment of Patient Index Data (RAPID) 3
• Validated patient questionnaire
• Uses the multidimensional HAQ (MD‐HAQ)
Patient Activity Scale (PAS)
• Validated patient questionnaire
• Includes the HAQ‐II
RA Treatment Goals and Efficacy Evaluation
21Singh JA, et al. American College of Rheumatology. Arthritis Care & Research. 2015;68(1):1‐25.
Menter A, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 1. J Am Acad Dermatol. 2008;58:826‐50
PSORIASISChronic Inflammatory Disease

12
Psoriasis (PsO)
• Chronic, inflammatory, autoimmune disease of skin
• Hallmark sign is plaques
• Irritating, painful, emotionally debilitating
• Concurrent joint involvement
• Psoriatic arthritis (PsA)
• 7.4 million affected in US (~2% of population)
• Genders equally affected
• Prevalence difference by race
• Onset typically 15‐35 years of age
Rachakonda TD, Schupp CW, Armstrong AW. Psoriasis prevalence among adults in the United States. J Am Acad Dermatol. 2014;70(3):512‐516. Menter A, Gottlieb A, Feldman S, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 1: overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol. 2008;58(5):826‐50.
Pathphysiology
Inappropriate autoreactive
T-cell activation
Release of growth factors and
inflammatory cytokines
Increased rate of skin cell
proliferation
The skin cell cycle is shortened almost 10-fold, from an average of 311 hours to just 36 hours.
Tsuruta D. NF‐ĸB links keratinocytes and lymphocytes in the pathogenesis of psoriasis. Recent Pat Inflamm Allergy Drug Discov. 2009;3(1):40‐48. Nickoloff BJ, Nestle FO. Recent insight into the immunopathogenesis of psoriasis provide new therapeutic opportunities. J Clin Invest. 2004;113(12):1664–1675.
24
13
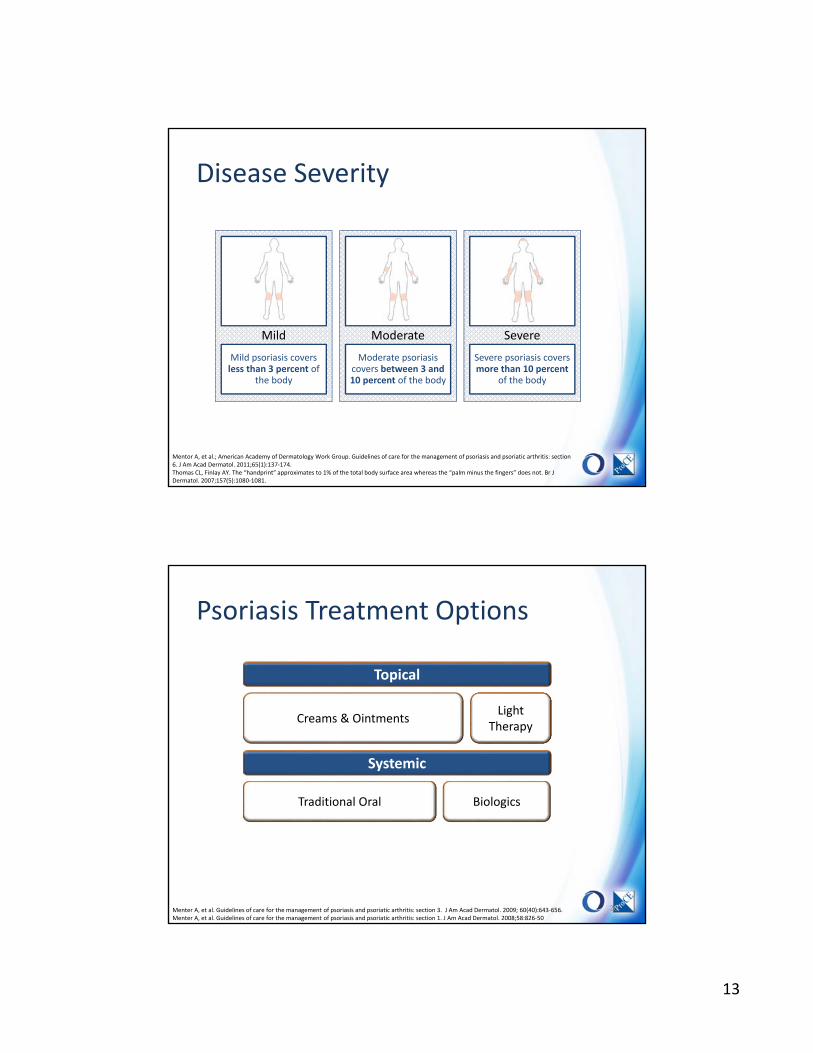
Disease Severity
Mild psoriasis covers less than 3 percent of
the body
Mild
Moderate psoriasis covers between 3 and 10 percent of the body
Moderate
Severe psoriasis covers more than 10 percent
of the body
Severe
Mentor A, et al.; American Academy of Dermatology Work Group. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. J Am Acad Dermatol. 2011;65(1):137‐174. Thomas CL, Finlay AY. The “handprint” approximates to 1% of the total body surface area whereas the “palm minus the fingers” does not. Br J Dermatol. 2007;157(5):1080‐1081.
Topical
Creams & OintmentsLight
Therapy
Systemic
Traditional Oral Biologics
Psoriasis Treatment Options
26Menter A, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 3. J Am Acad Dermatol. 2009; 60(40):643‐656.Menter A, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 1. J Am Acad Dermatol. 2008;58:826‐50
14
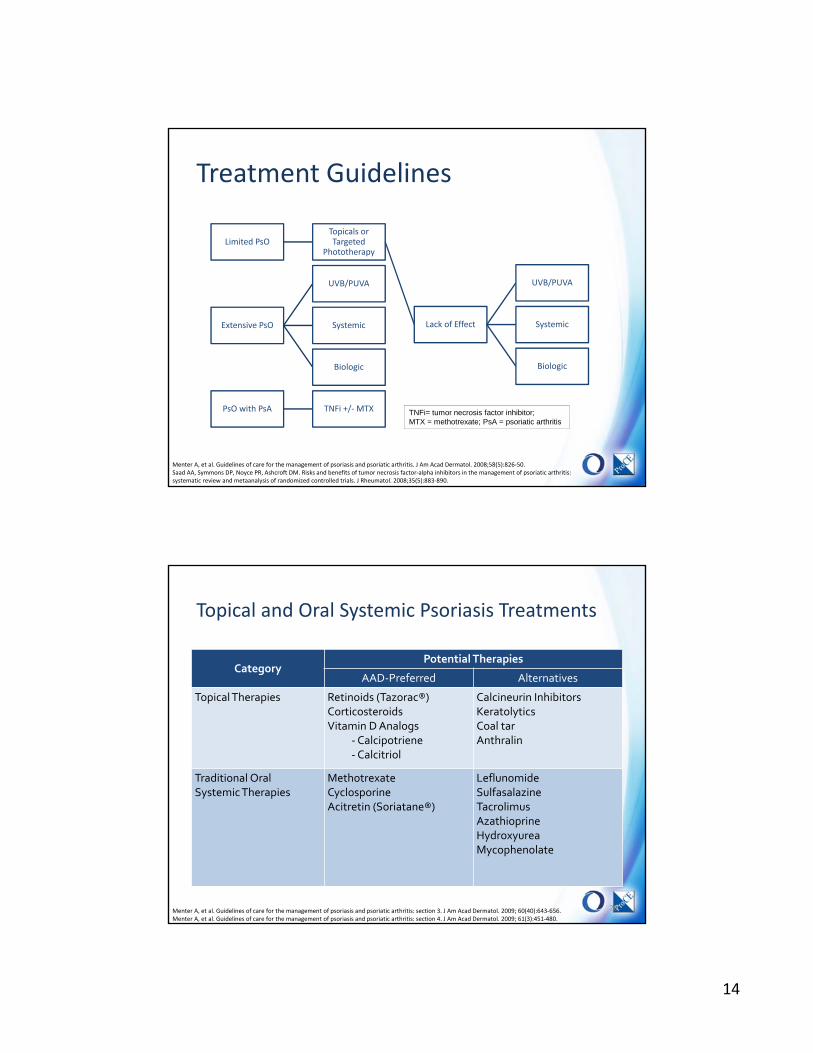
Treatment Guidelines
Menter A, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. J Am Acad Dermatol. 2008;58(5):826‐50. Saad AA, Symmons DP, Noyce PR, Ashcroft DM. Risks and benefits of tumor necrosis factor‐alpha inhibitors in the management of psoriatic arthritis: systematic review and metaanalysis of randomized controlled trials. J Rheumatol. 2008;35(5):883‐890.
Limited PsOTopicals or Targeted
Phototherapy
Lack of Effect
UVB/PUVA
Systemic
Biologic
Extensive PsO
UVB/PUVA
Systemic
Biologic
PsO with PsA TNFi +/‐MTX TNFi= tumor necrosis factor inhibitor; MTX = methotrexate; PsA = psoriatic arthritis
Topical and Oral Systemic Psoriasis Treatments
CategoryPotential Therapies
AAD‐Preferred Alternatives
Topical Therapies Retinoids (Tazorac®) Corticosteroids Vitamin D Analogs
‐Calcipotriene‐Calcitriol
Calcineurin Inhibitors KeratolyticsCoal tar Anthralin
Traditional Oral Systemic Therapies
MethotrexateCyclosporine Acitretin (Soriatane®)
LeflunomideSulfasalazine Tacrolimus Azathioprine Hydroxyurea Mycophenolate
28Menter A, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 3. J Am Acad Dermatol. 2009; 60(40):643‐656.Menter A, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 4. J Am Acad Dermatol. 2009; 61(3):451‐480.
15
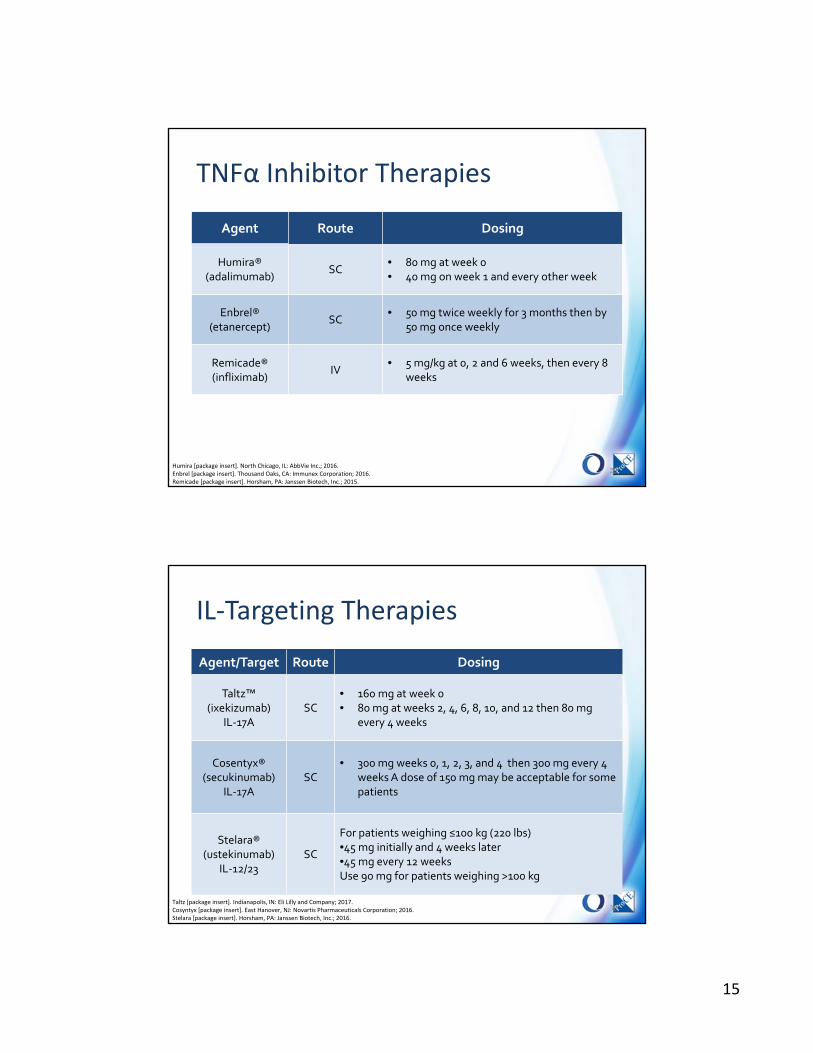
TNFα Inhibitor Therapies
Agent Route Dosing
Humira®(adalimumab)
SC• 80 mg at week 0 • 40 mg on week 1 and every other week
Enbrel®(etanercept)
SC• 50 mg twice weekly for 3 months then by
50 mg once weekly
Remicade®(infliximab)
IV• 5 mg/kg at 0, 2 and 6 weeks, then every 8
weeks
29Humira [package insert]. North Chicago, IL: AbbVie Inc.; 2016.Enbrel [package insert]. Thousand Oaks, CA: Immunex Corporation; 2016.Remicade [package insert]. Horsham, PA: Janssen Biotech, Inc.; 2015.
IL‐Targeting Therapies
Agent/Target Route Dosing
Taltz™(ixekizumab)
IL‐17ASC
• 160 mg at week 0• 80 mg at weeks 2, 4, 6, 8, 10, and 12 then 80 mg
every 4 weeks
Cosentyx®(secukinumab)
IL‐17ASC
• 300 mg weeks 0, 1, 2, 3, and 4 then 300 mg every 4 weeks A dose of 150 mg may be acceptable for some patients
Stelara®(ustekinumab)
IL‐12/23SC
For patients weighing ≤100 kg (220 lbs)•45 mg initially and 4 weeks later•45 mg every 12 weeks Use 90 mg for patients weighing >100 kg
30Taltz [package insert]. Indianapolis, IN: Eli Lilly and Company; 2017.Cosyntyx [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2016.Stelara [package insert]. Horsham, PA: Janssen Biotech, Inc.; 2016.
16
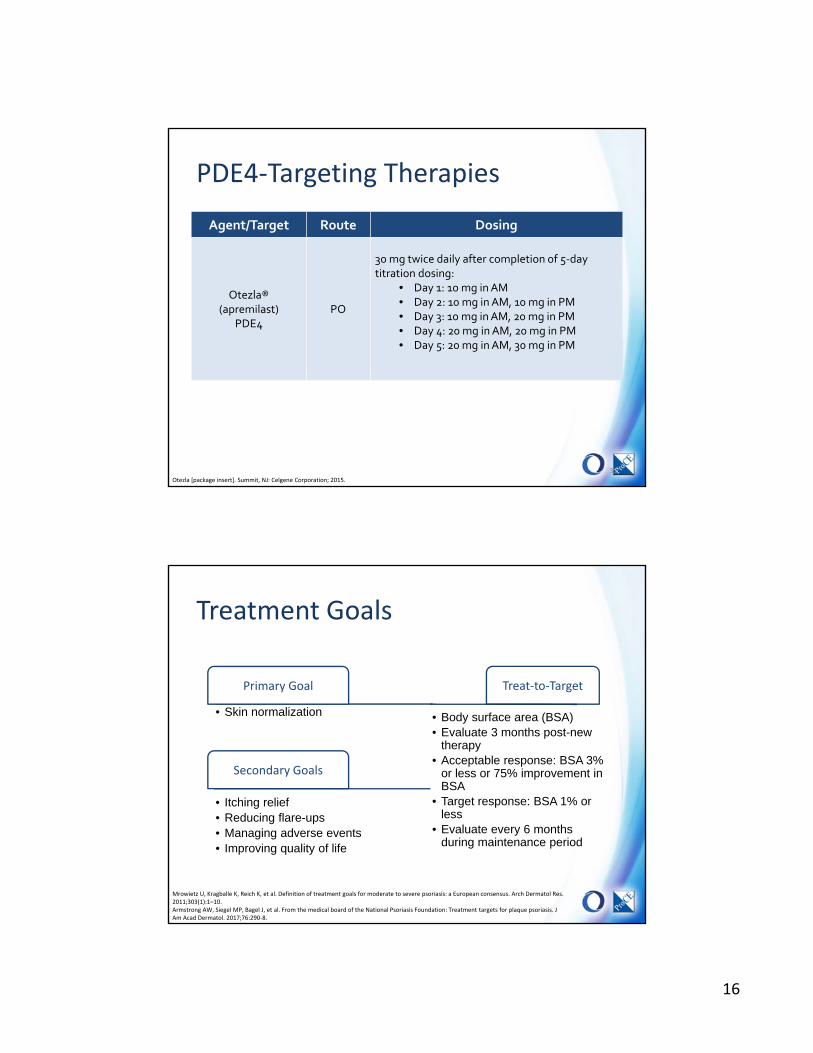
PDE4‐Targeting Therapies
Agent/Target Route Dosing
Otezla®(apremilast)
PDE4PO
30 mg twice daily after completion of 5‐daytitration dosing:
• Day 1: 10 mg in AM• Day 2: 10 mg in AM, 10 mg in PM• Day 3: 10 mg in AM, 20 mg in PM• Day 4: 20 mg in AM, 20 mg in PM• Day 5: 20 mg in AM, 30 mg in PM
31Otezla [package insert]. Summit, NJ: Celgene Corporation; 2015.
Treatment Goals
Primary Goal
• Skin normalization
Secondary Goals
• Itching relief• Reducing flare-ups• Managing adverse events• Improving quality of life
Mrowietz U, Kragballe K, Reich K, et al. Definition of treatment goals for moderate to severe psoriasis: a European consensus. Arch Dermatol Res. 2011;303(1):1–10.Armstrong AW, Siegel MP, Bagel J, et al. From the medical board of the National Psoriasis Foundation: Treatment targets for plaque psoriasis. J Am Acad Dermatol. 2017;76:290‐8.
Treat‐to‐Target
• Body surface area (BSA)• Evaluate 3 months post-new
therapy• Acceptable response: BSA 3%
or less or 75% improvement in BSA
• Target response: BSA 1% or less
• Evaluate every 6 months during maintenance period

17
INFLAMMATORY BOWEL DISEASES
Hemstreet BA. Chapter 41. In: DiPiro JT, et al. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw‐Hill; 2016.
Chronic Inflammatory Disease
Etiology
• Irritable bowel disease (IBD) most prevalent in Western Countries
• Crohn’s Disease (CD) Incidence
• 6 ‐ 15.5 cases per 100,000 persons/year
• Ulcerative colitis (UC) Incidence
• 1.2 ‐ 20 cases per 100,000 persons/year
• Males and females equally affected by IBD
• 20‐30% more women CD
• 60% more men UC
Hemstreet BA. Chapter 41. In: DiPiro JT, et al. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw‐Hill; 2016.

18
Presentation
• Malaise and fever
• Mild abdominal cramping
• Frequent small‐volume bowel movements
• Weight loss and malnutrition
• Hematochezia common with colonic involvement
Hemstreet BA. Chapter 41. In: DiPiro JT, et al. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw‐Hill; 2016.
Distinguishing Factors
Ulcerative Colitis (UC)
• Any part of GI tract
• Discontinuous lesions
• Transmural process – Fistulas
– Perforations
– Strictures
Crohn’s Disease (CD)
• Confined to rectum and colon
• Continuous lesions
• Mucosa and submucosaaffected
Hemstreet BA. Chapter 41. In: DiPiro JT, et al. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw‐Hill; 2016. Kornbluth A, et al. Ulcerative colitis practice guidelines in adults: American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol. 2010: 501‐23.
19
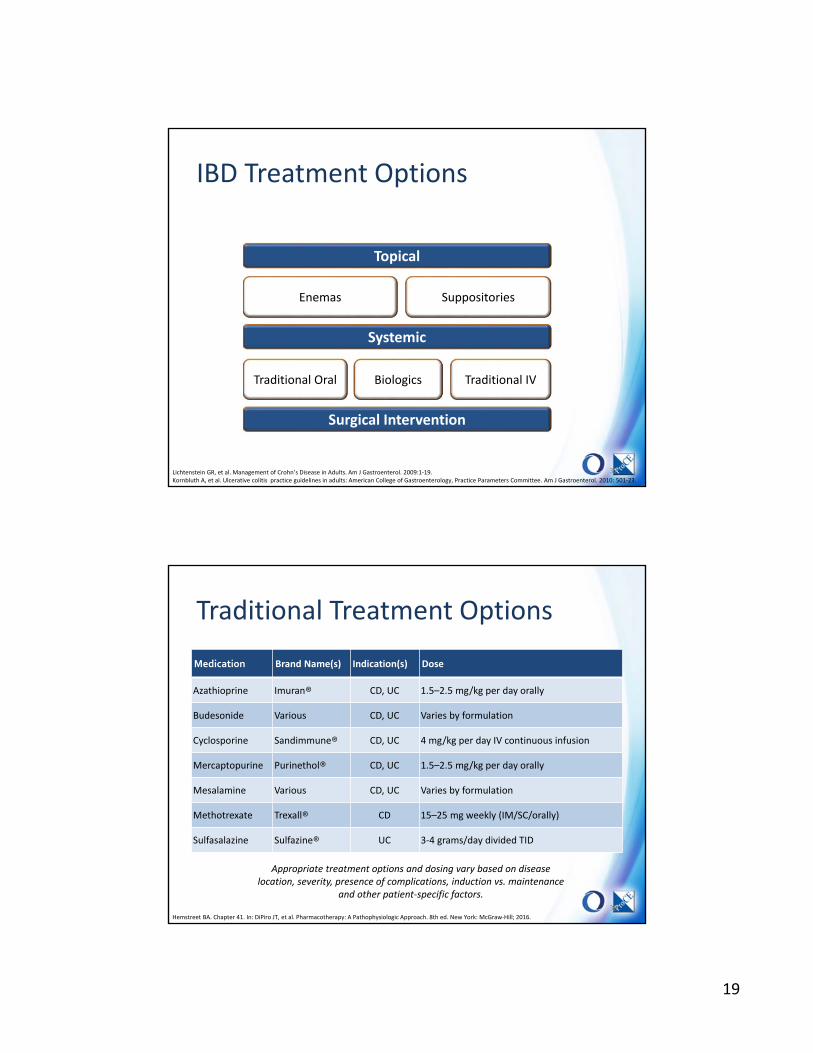
Topical
Enemas Suppositories
Systemic
Traditional Oral Biologics
IBD Treatment Options
37Lichtenstein GR, et al. Management of Crohn’s Disease in Adults. Am J Gastroenterol. 2009:1‐19.Kornbluth A, et al. Ulcerative colitis practice guidelines in adults: American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol. 2010: 501‐23.
Traditional IV
Surgical Intervention
Traditional Treatment Options
Medication Brand Name(s) Indication(s) Dose
Azathioprine Imuran® CD, UC 1.5–2.5 mg/kg per day orally
Budesonide Various CD, UC Varies by formulation
Cyclosporine Sandimmune® CD, UC 4 mg/kg per day IV continuous infusion
Mercaptopurine Purinethol® CD, UC 1.5–2.5 mg/kg per day orally
Mesalamine Various CD, UC Varies by formulation
Methotrexate Trexall® CD 15–25 mg weekly (IM/SC/orally)
Sulfasalazine Sulfazine® UC 3‐4 grams/day divided TID
38
Appropriate treatment options and dosing vary based on disease location, severity, presence of complications, induction vs. maintenance
and other patient‐specific factors.
Hemstreet BA. Chapter 41. In: DiPiro JT, et al. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw‐Hill; 2016.

20
TNFα Inhibitor Therapies
MedicationDrug Class
Route Dosing
Remicade® (infliximab)
TNFα InhibitorIV UC/CD: 5 mg/kg week 0, 2, and 6 then every 8 weeks
Humira®(adalimumab)TNFα Inhibitor
SCUC/CD: 160 mg on day 1, 80 mg at week 2, then 40 mg every other week
Simponi® (golimumab)TNFα Inhibitor
SCUC: 200 mg day 1, then 100mg two weeks later then every 4 weeks starting at week 6
Cimzia®(certolizumab
pegol)TNFα Inhibitor
SC CD: 400 mg at week 0, 2, 4, then every 4 weeks
39Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 10, 2017.
Non‐TNF Inhibitor Biologics
40
Medication
Drug ClassDosing Counseling Points
Tysabri®
(natalizumab)CD: 300 mg IV every 4 weeks
• Available only through the TOUCH™
Prescribing Program (REMS program)
• Has been linked to cases of PML
• Report signs/symptoms of infection
• Report signs/symptoms of hepatotoxicity
Stelara®
(ustekinumab)
CD: Induction: ≤55 kg: 260 mg IV,
56‐85 kg: 390 mg IV, >85 kg: 520 mg IV
Maintenance: 90 mg SC every 8 weeks
thereafter
• (Please refer to psoriasis section)
Entyvio®
(vedolizumab)
CD/UC: 300 mg IV at weeks 0, 2, 6 then
every 8 weeks thereafter
• Hypersensitivity reactions
• Has been linked to cases of PML
• Report signs/symptoms of infection
Micromedex [database online]. Greenwood Village, CO: Truven Health Analytics ; 2017. http://www.micromedexsolutions.com/. Accessed February 10, 2017. Kornbluth A, et al. Ulcerative colitis practice guidelines in adults: American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol. 2010: 501‐23.
21
IBD Treatment Goals and Efficacy Evaluation
• Goals of treatment
• Resolve inflammation and complications
• Alleviate systemic manifestations
• Maintain remission
• Measures of treatment effectiveness
• Crohn’s Disease Activity Index (CDAI)
• Harvey Bradshaw Index (HBI)
• Inflammatory Bowel Disease Questionnaire (IBDQ)
41Hemstreet BA. Chapter 41. In: DiPiro JT, et al. Pharmacotherapy: A Pathophysiologic Approach. 8th ed. New York: McGraw‐Hill; 2016.
Conclusion
• CIDs result from overactive or malfunctioning immune system
• Mild disease can usually be treated with non‐targeted, non‐specialty meds
• Moderate to severe disease often includes oral and/or biologic targeted therapies
– Symptom management
– Non‐curative







