

Clinical Case Discussion: Switching HIV Therapy
Pavel Khaykin, Frankfurt am Main
The Why and How of Switching in Virologic Suppression
Why
Simplify regimen
(pill number and frequency)
Tolerability
Comorbidity
Drug–drug and drug–food interactions
Pregnancy
Cost
How
Maintain viral suppression to avoid resistance
Need to consider
▪ Previous ART
▪ Previous resistance
▪ Likelihood of adherence
▪ Drug–drug or drug–food interactions
▪ Comorbid conditions
DHHS guidelines. March 2018.
Case 1: HIV and HCV infection
A 53-year-old man with HIV and HCV
▪ Origin: Portugal
▪ Injection heroin use (past); currently in OST
▪ eGFR: <10, End stage kidney disease, Hemodialysis
▪ HIV
‒ ED 2002
‒ CD4+ nadir 83 cells/mm3 and HIV RNA 11.580 copies/mL
‒ HLA-B*5701 negative
▪ HCV
‒ HCV genotype 3a infection with HCV RNA = 1.5 million IU/mL
‒ Liver elastography consistent with stage 3 fibrosis
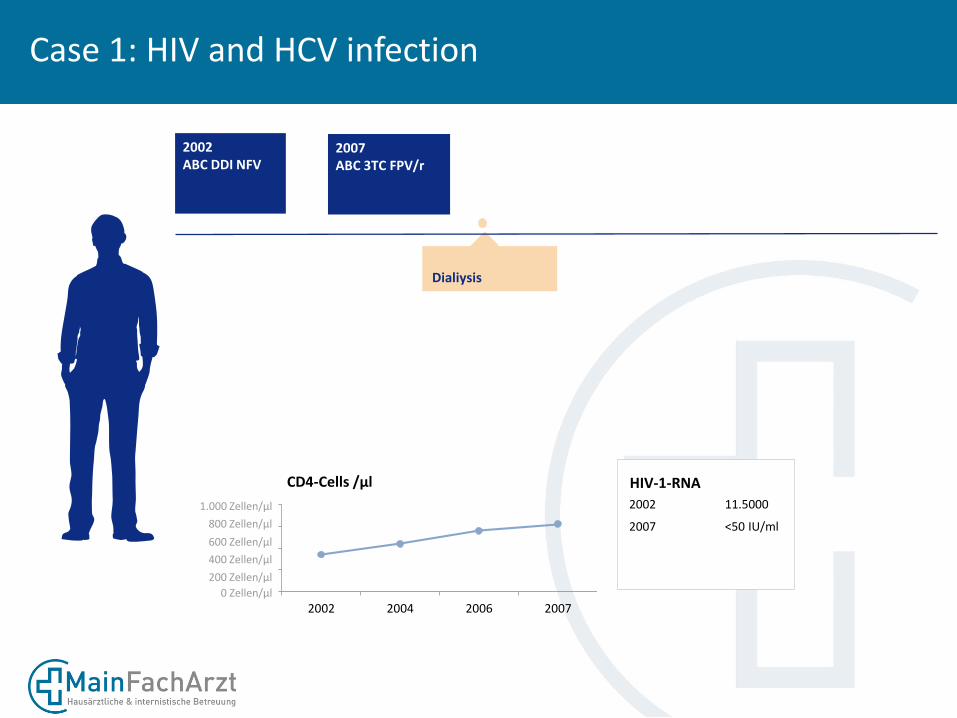
Dialiysis
2002ABC DDI NFV
2002 2004 2006 2007
CD4-Cells /µl HIV-1-RNA
2002 11.5000
2007 <50 IU/ml
1.000 Zellen/µl
800 Zellen/µl
600 Zellen/µl
400 Zellen/µl
200 Zellen/µl
0 Zellen/µl
2007 ABC 3TC FPV/r
Case 1: HIV and HCV infection

Case 1 HIV and HCV Infection
Dose Adjustment of ARVs for Impaired Renal Function
NRTI/NtRTI: Dose Adjustment or not recommended
NNRTI: No dose adjustment required
PI: No dose adjustment required

Dialysis
2002ABC DDI NFV
2002 2007 2010 2018
CD4-Cells /µl HIV-1-RNA
2002 11.5000
2018 <20 IU/ml
2007 <50 IU/ml
2010 <20 IU/ml
1.000 Zellen/µl
800 Zellen/µl
600 Zellen/µl
400 Zellen/µl
200 Zellen/µl
0 Zellen/µl
2007 ABC 3TC FPV/r
2010LPV/r SQV
Case 1: HIV and HCV infection
HCV Tx
20818 ARV?
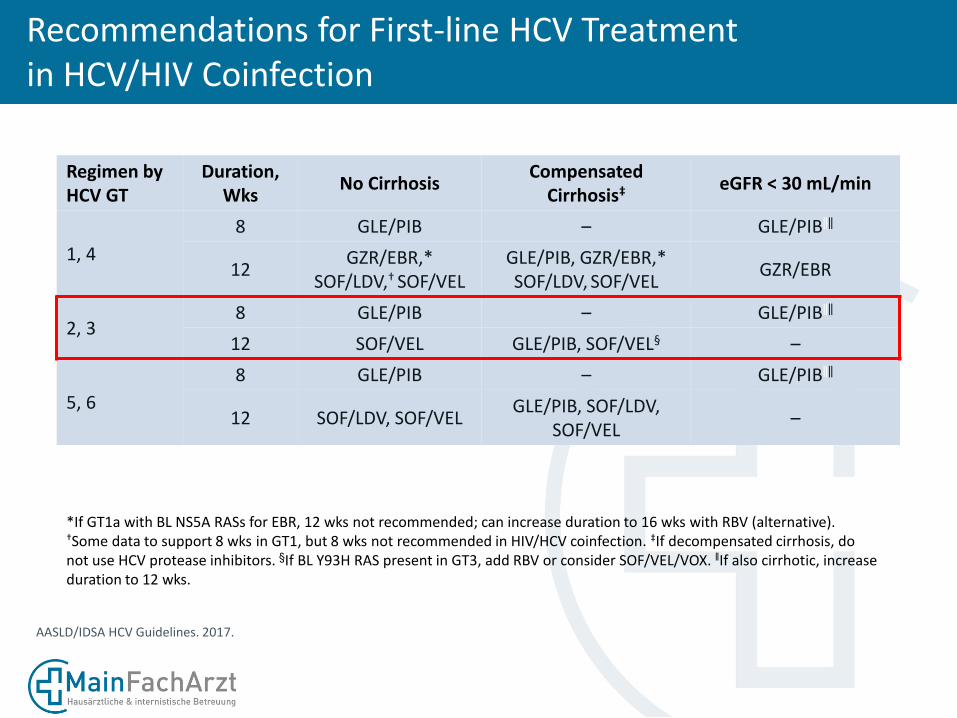
Recommendations for First-line HCV Treatment in HCV/HIV Coinfection
Regimen by HCV GT
Duration, Wks
No CirrhosisCompensated
Cirrhosis‡eGFR < 30 mL/min
1, 4
8 GLE/PIB – GLE/PIB‖‖
12GZR/EBR,*
SOF/LDV,† SOF/VELGLE/PIB, GZR/EBR,*SOF/LDV, SOF/VEL
GZR/EBR
2, 38 GLE/PIB – GLE/PIB‖‖
12 SOF/VEL GLE/PIB, SOF/VEL§ –
5, 6
8 GLE/PIB – GLE/PIB‖‖
12 SOF/LDV, SOF/VELGLE/PIB, SOF/LDV,
SOF/VEL–
AASLD/IDSA HCV Guidelines. 2017.
*If GT1a with BL NS5A RASs for EBR, 12 wks not recommended; can increase duration to 16 wks with RBV (alternative). †Some data to support 8 wks in GT1, but 8 wks not recommended in HIV/HCV coinfection. ‡If decompensated cirrhosis, do not use HCV protease inhibitors. §If BL Y93H RAS present in GT3, add RBV or consider SOF/VEL/VOX. ‖If also cirrhotic, increase duration to 12 wks.

Recommendation for End-Stage Renal Disease
7
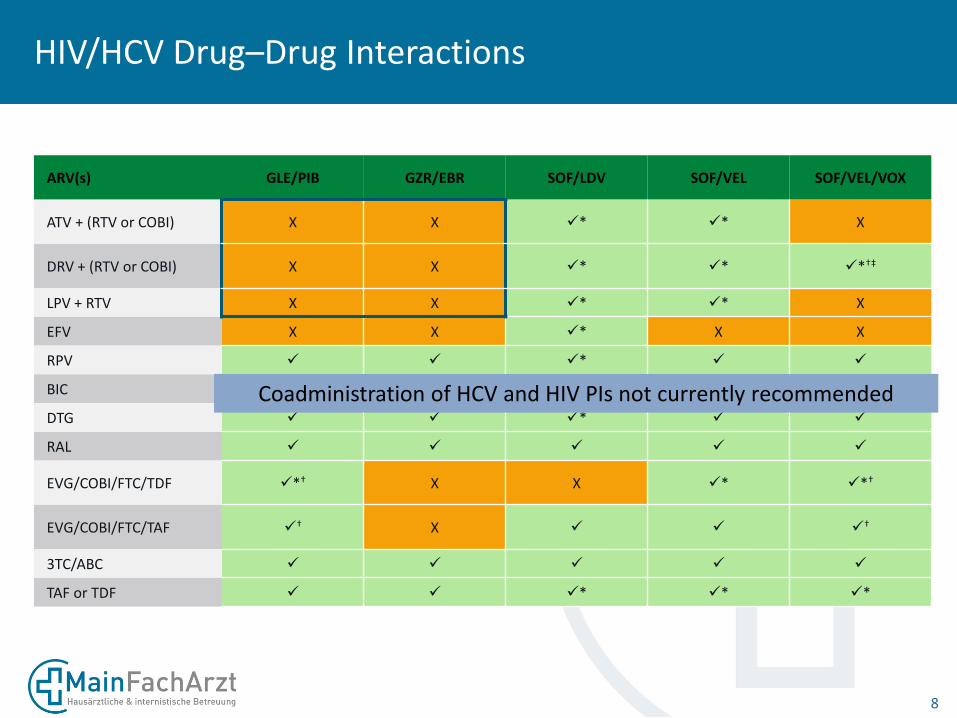
HIV/HCV Drug–Drug Interactions
8
ARV(s) GLE/PIB GZR/EBR SOF/LDV SOF/VEL SOF/VEL/VOX
ATV + (RTV or COBI) X X ✓* ✓* X
DRV + (RTV or COBI) X X ✓* ✓* ✓*†‡
LPV + RTV X X ✓* ✓* X
EFV X X ✓* X X
RPV ✓ ✓ ✓* ✓ ✓
BIC ‒§ ‒§✓
† ✓†
✓†
DTG ✓ ✓ ✓* ✓ ✓
RAL ✓ ✓ ✓ ✓ ✓
EVG/COBI/FTC/TDF ✓*† X X ✓* ✓*†
EVG/COBI/FTC/TAF ✓† X ✓ ✓ ✓
†
3TC/ABC ✓ ✓ ✓ ✓ ✓
TAF or TDF ✓ ✓ ✓* ✓* ✓*
Coadministration of HCV and HIV PIs not currently recommended

Case 1 HIV and HCV Coinfection
Dose Adjustment of ARVs for Impaired Renal Function
NRTI/NtRTI: Dose Adjustment or not recommended
NNRTI: No dose adjustment required
PI: No dose adjustment required but not with HCV PI
INSTI: No dose adjustment required
DTG RPV
Principles of ART Regimen Switching in Virologically Suppressed Patients
• Review ART history for previous intolerance or HIV virologic failure
• Review HIV resistance test results
• If previous HIV resistance uncertain, consider a switch only if new regimen likely to maintain suppression of resistant virus
• In patients with HBV/HIV coinfection, continue ARVs active against HBV (even if not needed for HIV suppression)
• Check HIV-1 RNA during first 3 mos after switch to ensure suppression
• Monotherapy with boosted PI or INSTI not recommended

11
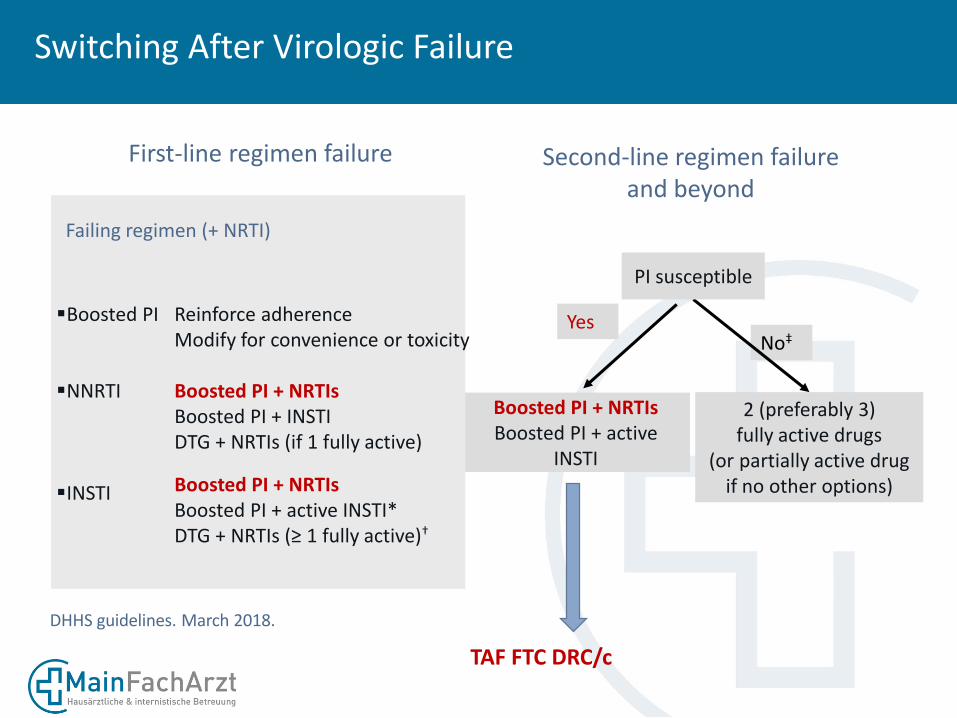
Switching After Virologic Failure

Switching After Virologic Failure
First-line regimen failure
Boosted PI + NRTIsBoosted PI + active
INSTI
Yes
2 (preferably 3)fully active drugs
(or partially active drug if no other options)
No‡
Second-line regimen failureand beyond
PI susceptible
Failing regimen (+ NRTI)
▪Boosted PI
▪NNRTI
▪INSTI
Reinforce adherenceModify convenience or toxicity
Boosted PI + NRTIsBoosted PI + INSTIDTG + NRTIs (if 1 fully active)
Boosted PI + NRTIsBoosted PI + active INSTI*DTG + NRTIs (≥ 1 fully active)†
DHHS guidelines. March 2018.
Slide credit: clinicaloptions.com
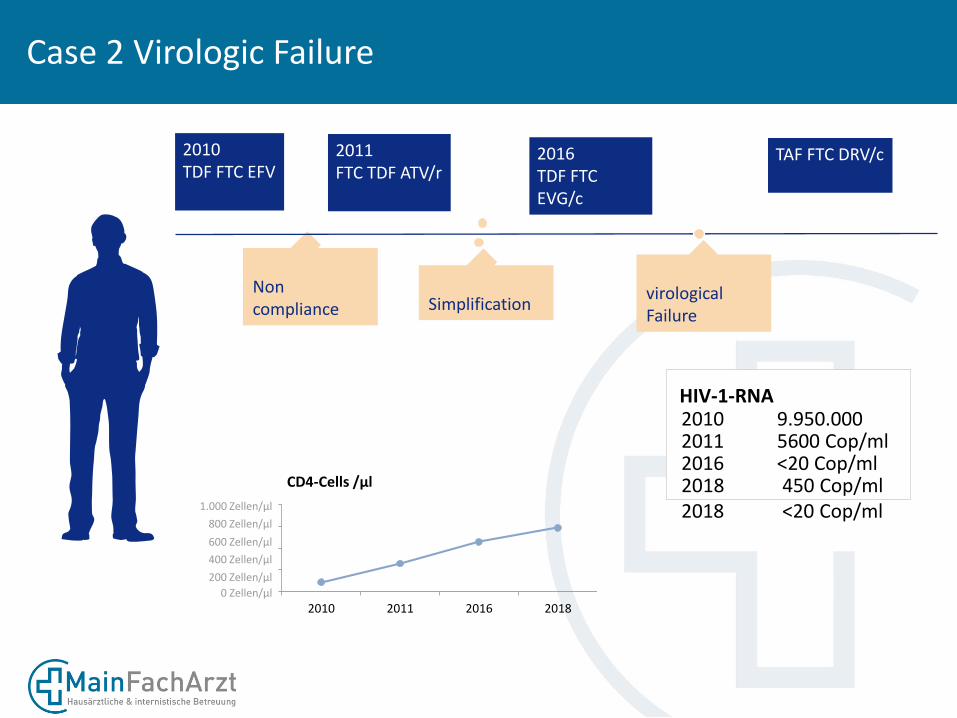
Case 2 Virologic Failure
A 40-year-old man with HIV
▪ Origin: Germany
▪ MSM
▪ No comorbidity
▪ HIV
‒ ED 2003
‒ First ART 2010
‒ CD4+ nadir 43 cells/mm3 and HIV RNA 9.950.000 copies/mL
‒ HLA-B*5701 negative

Case 2 Virologic Failure
Non compliance
2010TDF FTC EFV
2010 2011 2016 2018
CD4-Cells /µl
HIV-1-RNA2010 9.950.000
2018 450 Cop/ml
2011 5600 Cop/ml2016 <20 Cop/ml
1.000 Zellen/µl
800 Zellen/µl
600 Zellen/µl
400 Zellen/µl
200 Zellen/µl
0 Zellen/µl
2011FTC TDF ATV/r
2016TDF FTC EVG/c
Simplification
2018?
virologicalFailure
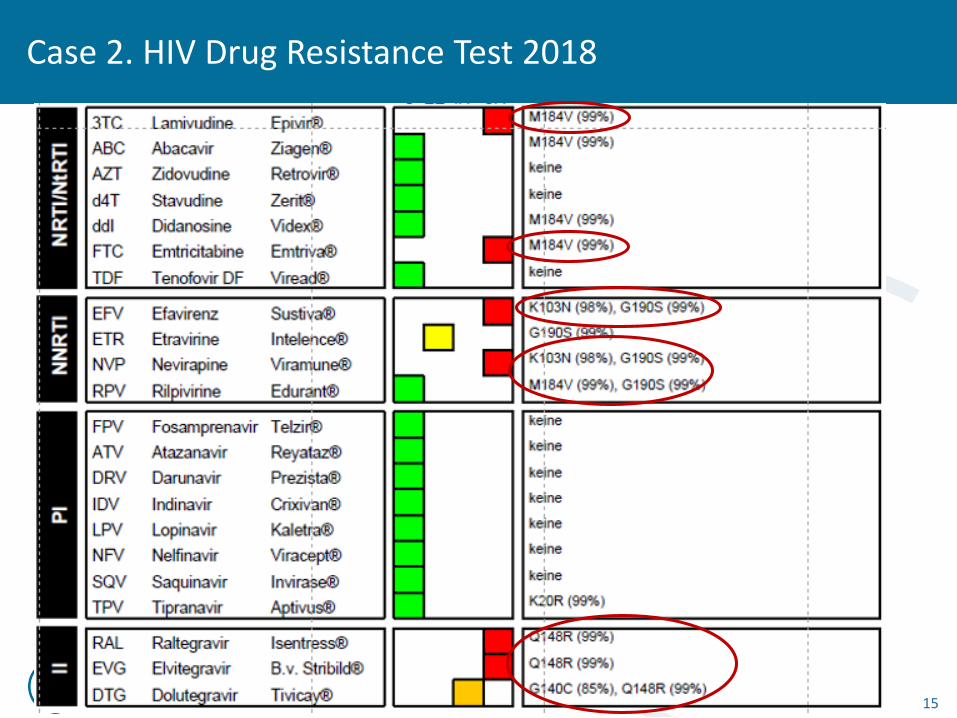
Case 2. HIV Drug Resistance Test 2018
15
Switching After Virologic Failure
First-line regimen failure
Boosted PI + NRTIsBoosted PI + active
INSTI
Yes
2 (preferably 3)fully active drugs
(or partially active drug if no other options)
No‡
Second-line regimen failureand beyond
PI susceptible
Failing regimen (+ NRTI)
▪Boosted PI
▪NNRTI
▪INSTI
Reinforce adherenceModify for convenience or toxicity
Boosted PI + NRTIsBoosted PI + INSTIDTG + NRTIs (if 1 fully active)
Boosted PI + NRTIsBoosted PI + active INSTI*DTG + NRTIs (≥ 1 fully active)†
DHHS guidelines. March 2018.
TAF FTC DRC/c
Case 2 Virologic Failure
Non compliance
2010TDF FTC EFV
2010 2011 2016 2018
CD4-Cells /µl
HIV-1-RNA2010 9.950.000
2018 450 Cop/ml2018 <20 Cop/ml
2011 5600 Cop/ml2016 <20 Cop/ml
1.000 Zellen/µl
800 Zellen/µl
600 Zellen/µl
400 Zellen/µl
200 Zellen/µl
0 Zellen/µl
2011FTC TDF ATV/r
2016TDF FTC EVG/c
Simplification
TAF FTC DRV/c
virologicalFailure







