
12/17/2020
1
CLINICAL PROBLEM SOLVING IN RHEUMATOLOGY
AJCHARA KOOLVISOOTDIVISION OF RHEUMATOLOGY, DEPARTMENT OF MEDICINE
SIRIRAJ HOSPITAL
• Behavior
• Respect
• Positive
• Tolerant
Attitudes
• Intellectual
• Communicative
• Interpersonal
• Reasoning
Skill
• Facts
• Concepts
• Understanding
Knowledge
Competency
Attitude Skill Knowledge
• Hx +++ +++ ++
• PE ++ +++ ++
• Ix + +++ +++
• Discussion + +++ +++
หวัขอ้หลกั รายละเอยีด ระดบั 1 ระดบั 2 ระดบี 3
ความรูพ้ ื�นฐานของ
อายรุศาสตร์
Basic pharmacology
Physiologic change
Immune response
Anatomy and function
โรคหรอืภาวะทาง
อายรุศาสตร์
Hyperuricemia
Gout
OA
RA
SLE
Glomerular dis in CNTD
Osteoporosis
Polyarthritis
Frozen shoulder
Pseudogout
Monoarthritis
Septic arthritis
SSc, PM/DM, MCTD
Vasculitis
DLE
AVN
Osteomyelitis
Myofascial pain &
Fibromyalgia
Sjogren’s
Takayasu’s & GCA
Behcet’s
Reactive arthritis
Palindromic rheumatism
EN
Acute rheumatic fever
Osteomalacia
Specific disease & Pregnancy
หตัถการ/การแปลผลทาง
หอ้งปฏบิตักิาร
Arthrocentesis
Synovial fluid analysis
Joint & soft tissue injection
Bone & joint radiography
ANA, APL, RF
Complement
BMD
บรูณาการ 1. Communication skill2. Professionalism
3. System-based
practice
4. Practice-based
learning &
improvement
5. Medical education
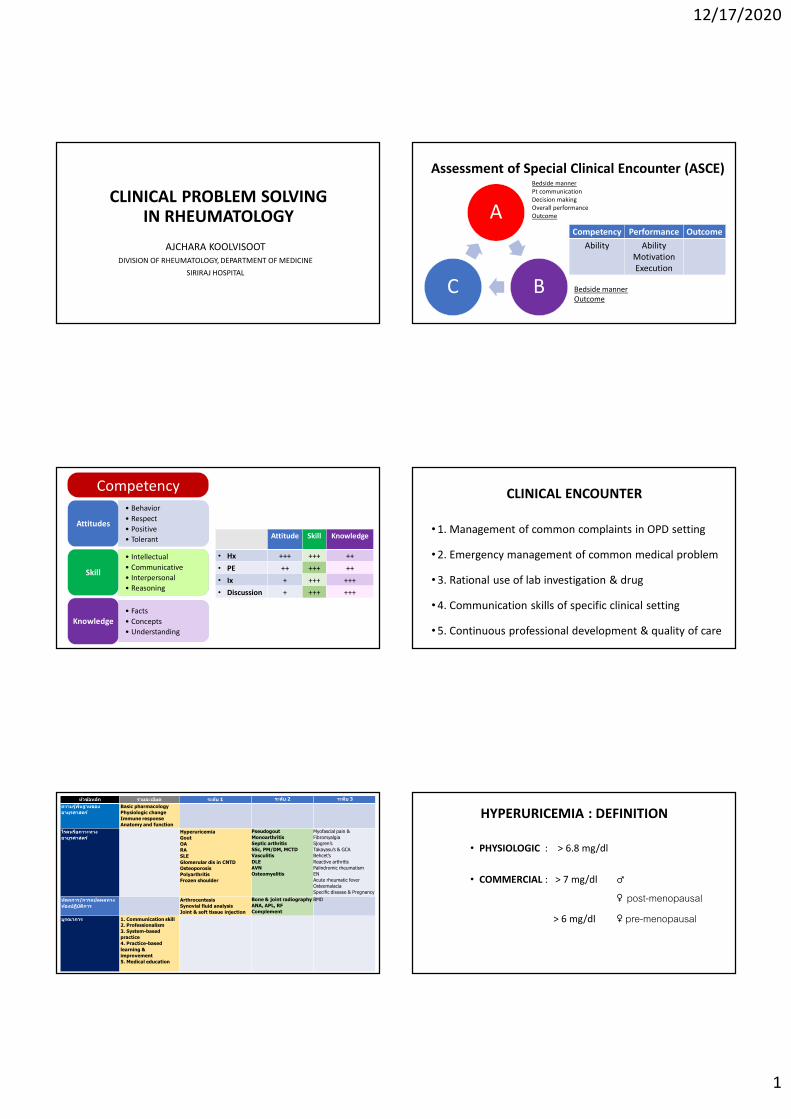
Assessment of Special Clinical Encounter (ASCE)
A
BC
Competency Performance Outcome
Ability AbilityMotivationExecution
Bedside mannerPt communicationDecision makingOverall performanceOutcome
Bedside mannerOutcome
CLINICAL ENCOUNTER
• 1. Management of common complaints in OPD setting
• 2. Emergency management of common medical problem
• 3. Rational use of lab investigation & drug
• 4. Communication skills of specific clinical setting
• 5. Continuous professional development & quality of care
HYPERURICEMIA : DEFINITION
• PHYSIOLOGIC : > 6.8 mg/dl
• COMMERCIAL : > 7 mg/dl ♂
♀ post-menopausal
> 6 mg/dl ♀ pre-menopausal
12/17/2020
2
RISK FACTOR
DRUGS :DiureticsLow dose ASAPyrazinamide, EthambutolCalcineurin inhibitors ( Cyclosporine, Tacrolimus)
DIETARY FACTORS :Purine-rich food ( red meat, seafood)
Alcohol ( beer, spirits)Sugar sweetened beverage
GENETIC FACTORS :GenderEthnicityGenetic variants of urate
transporter
OTHER :Increasing ageMenopause BMIHypertensionDyslipidemiaChronic kidney diseaseSmoking
HYPERURICEMIA
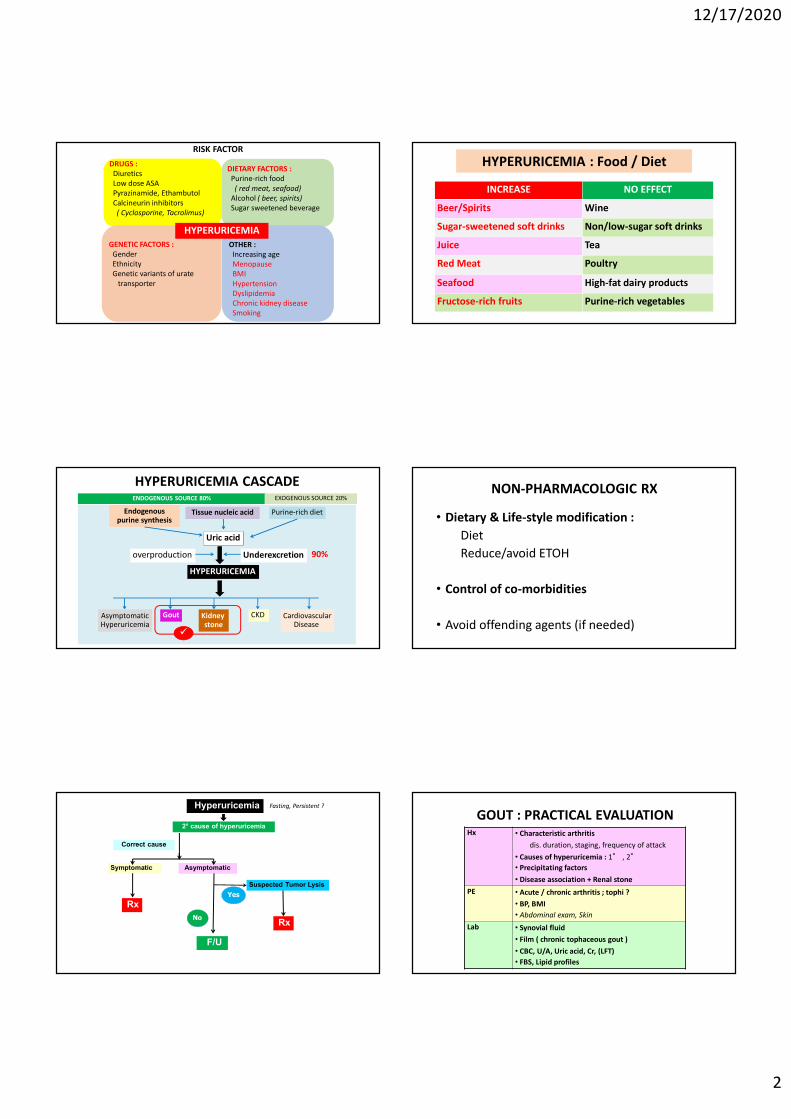
HYPERURICEMIA CASCADE
Uric acid
HYPERURICEMIA
Endogenous purine synthesis
Purine-rich dietTissue nucleic acid
Underexcretionoverproduction
AsymptomaticHyperuricemia
Gout Kidney stone
CKD CardiovascularDisease
ENDOGENOUS SOURCE 80% EXOGENOUS SOURCE 20%
90%
Hyperuricemia
2° cause of hyperuricemia
Symptomatic Asymptomatic
F/U
Suspected Tumor Lysis
Rx
Rx
Correct cause
Yes
No
Fasting, Persistent ?
HYPERURICEMIA : Food / Diet
INCREASE NO EFFECT
Beer/Spirits Wine
Sugar-sweetened soft drinks Non/low-sugar soft drinks
Juice Tea
Red Meat Poultry
Seafood High-fat dairy products
Fructose-rich fruits Purine-rich vegetables
NON-PHARMACOLOGIC RX
• Dietary & Life-style modification :
Diet
Reduce/avoid ETOH
• Control of co-morbidities
• Avoid offending agents (if needed)
GOUT : PRACTICAL EVALUATIONHx • Characteristic arthritis
dis. duration, staging, frequency of attack
• Causes of hyperuricemia : 1° , 2°
• Precipitating factors
• Disease association + Renal stone
PE • Acute / chronic arthritis ; tophi ?
• BP, BMI
• Abdominal exam, Skin
Lab • Synovial fluid
• Film ( chronic tophaceous gout )
• CBC, U/A, Uric acid, Cr, (LFT)
• FBS, Lipid profiles
12/17/2020
3
13
Natural Hx of Gout
• Acute arthritis - self-limited 3-10 days
• Recurrent attack 62% - 1 y75% - 2 y89% - 5 y
GOUT : PRECIPITATING FACTORS
• Factors disturbing uric acid level
Alcohol
Diet
Medications
Factors decrease renal blood flow
• Trauma/ surgery
• Acute illness including infections
DIAGNOSIS
• Synovial fluid analysis
• Dramatic response to colchicine
• Hx intermittent arthritis of 1st MTP/Ankle + Uric
• Film - tophi
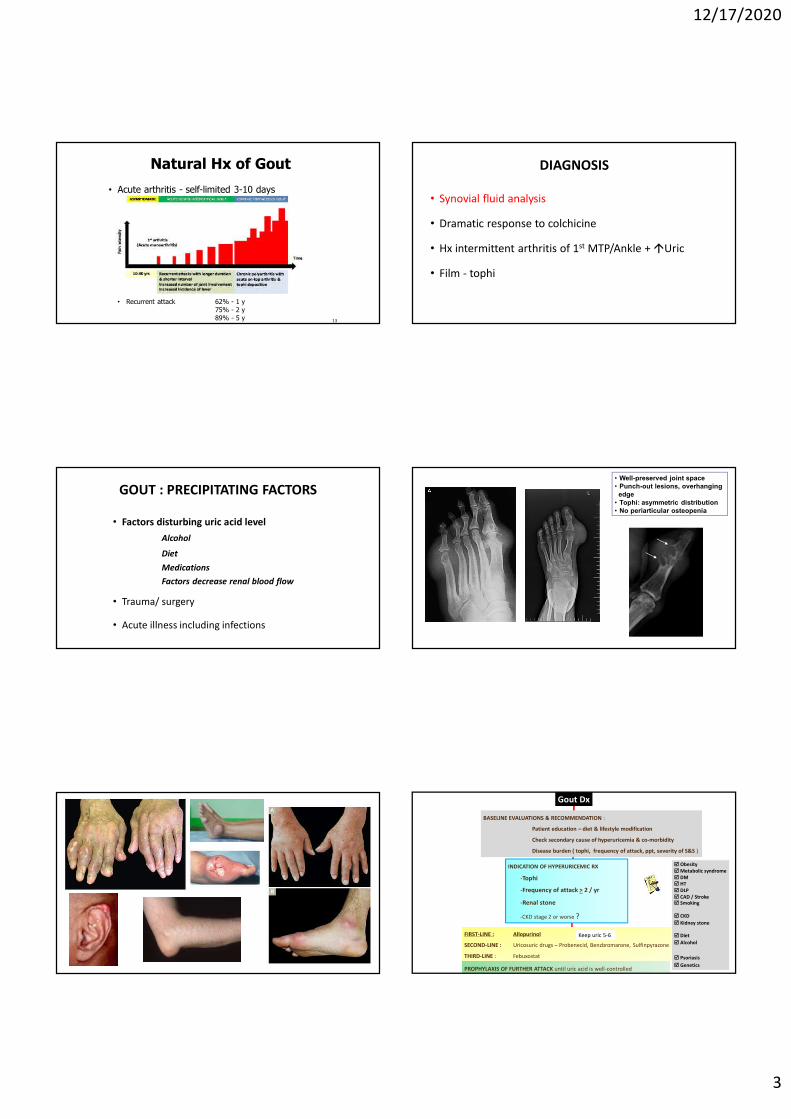
• Well-preserved joint space• Punch-out lesions, overhanging
edge• Tophi: asymmetric distribution• No periarticular osteopenia
Gout Dx
FIRST-LINE : Allopurinol
SECOND-LINE : Uricosuric drugs – Probenecid, Benzbromarone, Sulfinpyrazone
THIRD-LINE : Febuxostat
PROPHYLAXIS OF FURTHER ATTACK until uric acid is well-controlled
BASELINE EVALUATIONS & RECOMMENDATION :
Patient education – diet & lifestyle modification
Check secondary cause of hyperuricemia & co-morbidity
Disease burden ( tophi, frequency of attack, ppt, severity of S&S )
Obesity Metabolic syndrome DM HT DLP CAD / Stroke Smoking
CKD
Kidney stone
Diet
Alcohol
Psoriasis
Genetics
INDICATION OF HYPERURICEMIC RX
-Tophi
-Frequency of attack > 2 / yr
-Renal stone
-CKD stage 2 or worse ?
Keep uric 5-6

12/17/2020
4
Suspected RA SUSPECTED GOUT
Disease Ask : pain/swelling – intermittent mono chron polyjt location & tophi
precipitating factors esp. ETOHfrequency of attack / yearfamilial Hxdrug – esp HCTZ, CSA
Inspect & palpate : jt involvement & deformitytophi – 1st MTP, lateral malleolus,
olecranon, ear pinnaROM
Complication of disease CTS
Disease association Common - HT, DM, DLP, CADObesity, Metabolic syndromeSmoking
Renal stoneothers - Psoriasis, ADPKD
HLA-B*5801 : USA/Eupropean Guideline
Khanna D, Fitzgerald JD, Khanna PP, et al. 2012
• HLA-B*5801 testing prior to Allopurinol Rx should be
in selected patient subpopulations (evidence A)
Thais
Hans Chinese
Koreans with stage 3 or worse CKD
96.6 (24.4-381)
79.3 (41.5-151.4)
Somkrua R,Eickman EE, Saokaew S, Lohitnavy M, Chaiyakunapruk N. BMC Med Genetics 2011
ALLOPURINOL HYPERSENSITIVITY
• (1) AmerJ Med 76:47,1984; (2) J Am AcadDermatol1:365,1979; (3) Arthritis Rheum 29:82,1986; (4) Proc Natl AcadSciUSA 102: 4134, 2005; (5) Ann Pharmacother27:33,1993; (6) South Med J 72:1361, 1979; (7) Arch IntMed 134:553, 1974; (8) J ClinRheumatol11:129, 2005; (9) J Rheumatol33: 1646, 2006; (10) Ann Rheum Dis 60: 981,2001
RISK FACTOR Reference
Recent initiation 1,2,3,4
Renal impairment 1,2,4,5,6,7
Diuretic Rx 1,2,5,6,7
HLA-B*5801 4
Allopurinol dose +ve 1,2,5,8
Allopurinol dose -ve 4,9,10
HLA-B*5801
• Warning – Risk vs Benefit
•High risk group :
Renal impairment 48.4%
Diuretic Rx
Ramasamy SN, Korb-Wells CS, Kannangara RW, et al. 2013
Mostly occur in 6-8 wks
คณะกรรมการหลกัประกนัสขุภาพแหง่ชาต ิประกาศสทิธปิระโยชนเ์พิ�มเตมิ (9 ธค 2563)
• 1. การผา่ตัดปลกูถา่ยตับในผูป่้วยโรคตับแข็งระยะกลางและระยะทา้ย
• 2. การตรวจยนี HLA-B*5801
• 3. Extracoporeal membrane oxygenator (ECMO) ในการรักษาภาวะหัวใจและ/หรอื
ปอดทํางานลม้เหลวเฉียบพลัน
• 4. การคัดกรองและวนิจิฉัยวัณโรคดว้ยการทํา CXR ในกลุม่เสี�ยง และ การตรวจ
molecular assay ไดแ้ก่ real-time PCR, TB-LAMP & LPA
+ เห็นชอบการใชก้ญัชาใน ผป 4 กลุม่โรค : มะเร็ง, Parkinson, migraine & epilepsy
12/17/2020
5
Thai Rheum Guideline
Hypouricemic Rx
CrCl >60
CrCl 30-60
ProbenecidSulfinpyrazoneBenzbromarone
Benzbromarone
AllopurinolCrCl <30
No stone +ve stone
1st line
2nd line
URICOSURIC : When ?
• Condition : No renal stone
Mild-mod renal impairment
• Treatment initiation :
Second-line
Allopurinol hypersensitivity
Allopurinol contraindication
Combination Rx
Hyperuricemic Rx
• 1st Line Allopurinol
• 2nd Line Probenecid
Benzbromarone
Sulfinpyrazone
• 3rd Line Febuxostat
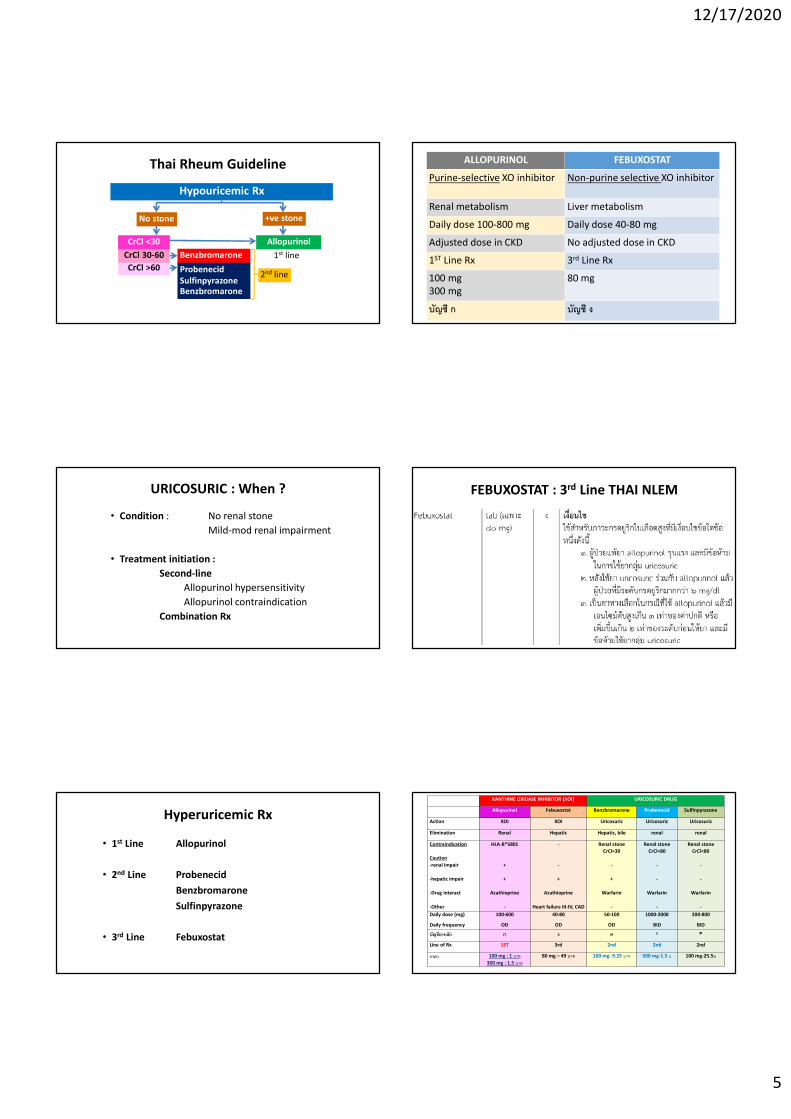
ALLOPURINOL FEBUXOSTAT
Purine-selective XO inhibitor Non-purine selective XO inhibitor
Renal metabolism Liver metabolism
Daily dose 100-800 mg Daily dose 40-80 mg
Adjusted dose in CKD No adjusted dose in CKD
1ST Line Rx 3rd Line Rx
100 mg300 mg
80 mg
บัญชี ก บัญชี ง
FEBUXOSTAT : 3rd Line THAI NLEM
XANTHINE OXIDASE INHIBITOR (XOI) URICOSURIC DRUG
Allopurinol Febuxostat Benzbromarone Probenecid Sulfinpyrazone
Action XOI XOI Uricosuric Uricosuric Uricosuric
Elimination Renal Hepatic Hepatic, bile renal renal
Contraindication
Caution
-renal impair
-hepatic impair
-Drug interact
-Other
HLA-B*5801
+
+
Azathioprine
-
-
-
+
Azathioprine
Heart failure III-IV, CAD
Renal stone
CrCl<30
-
+
Warfarin
-
Renal stone
CrCl<80
-
-
Warfarin
-
Renal stone
CrCl<80
-
-
Warfarin
-
Daily dose (mg)
Daily frequency
100-600
OD
40-80
OD
50-100
OD
1000-2000
BID
200-800
BID
บัญชียาหลกั ก ง ค ก
Line of Rx 1ST 3rd 2nd 2nd 2nd
ราคา 100 mg : 1 บาท
300 mg : 1.5 บาท
80 mg – 49 บาท 100 mg- 9.25 บาท 500 mg-1.5 บ 100 mg-25.5บ
12/17/2020
6
PATIENT EDUCATION
• Basic knowledge of disease
• Diet : Avoid ETOH
↓ Purine-rich diet
( NO total restriction )
Normal diet if well-controlled uric level
• Good compliance of medication – long-term Rx
• Avoid massage / hot pack in acute arthritis
NSAIDs : FDA RECOMMENDATION
• In established CV disease
cNSAIDs & Coxibs SHOULD NOT BE USED
• In CV risk group
cNSAIDs esp. Naproxen is recommended > Coxibs
with patient-warning
If no NSAIDs indication, give ALTERNATIVE drug
Low dose – short duration
มคีวามจาํเป็นตอ้งใช ้NSAIDs ?
ประเมนิ CVS Risk
ไมม่ ีRisk ม ีRisk
ประเมนิ GI Risk ประเมนิ GI Risk
No/Low Risk No/Low Risk High RiskHigh Risk Mod RiskMod Risk
C-NSAID C-NSAID+PPICoxib
Coxib+ PPI
Naproxen Naproxen + PPI
Non-NSAID
OA : RISK FACTORS
Major joint trauma*
Repetitive stress/jt overload*
Obesity*
Quadriceps weakness*
Prior inflam joint dis.
Metabolic /endocrine dis.
• Age
• Race/Genetic factors
• Female gender
• Congenital defects
* Potentially modifiable
Suspected RA SUSPECTED OA
Disease Ask : pain with activitylocation ( localized/generalized )risk factor – * modifiable risk factor
familial Hx
Inspect : jt involvement ( 1º/2º)inflammation / effusion deformity :
finger - Bouchard’s & Heberden’shand - “squaring” appearanceknee - varus / valgus ( standing )spine - kyphoscoliosis
Palpate : bony enlargementKnee - crepitus, effusion, stability, quad wasting Spine – muscle spasm, tenderness
ROM
Complication SLRT, Nerve root compression (spine)
Disease association Comorbidity
OA : Classification
Primary ( Idiopathic )
• Localized
Hand
Feet
Hip
Spine
Others
• Generalized : > 3 areas
Secondary
• Congenital
• Trauma
• Metabolic
• Endocrine
• Calcium deposition dis.
• Neuropathic
• Others
12/17/2020
7
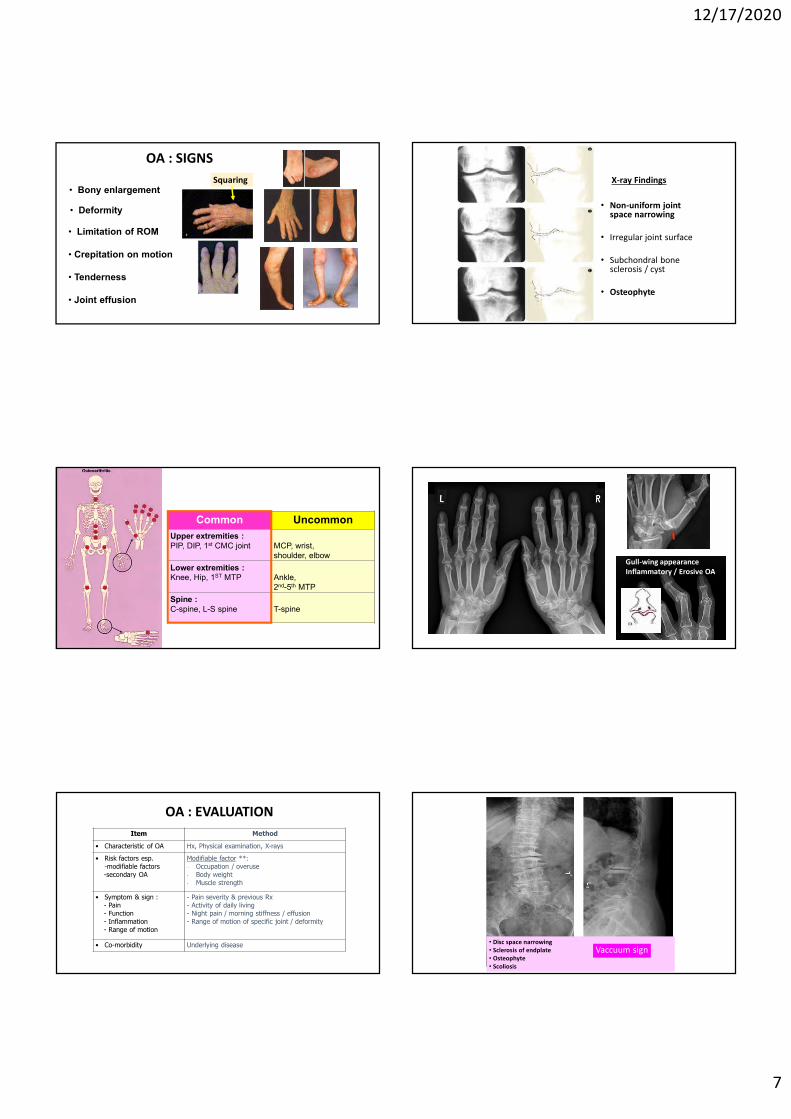
OA : SIGNS
• Limitation of ROM
• Crepitation on motion
• Tenderness
• Joint effusion
ValgusVarus
• Bony enlargement
• Deformity
Squaring
Location in OA
Common Uncommon
Upper extremities :PIP, DIP, 1st CMC joint MCP, wrist,
shoulder, elbow
Lower extremities :Knee, Hip, 1ST MTP Ankle,
2nd-5th MTP
Spine :C-spine, L-S spine T-spine
OA : EVALUATION
Item Method
• Characteristic of OA Hx, Physical examination, X-rays
• Risk factors esp. -modifiable factors-secondary OA
Modifiable factor **:- Occupation / overuse- Body weight - Muscle strength
• Symptom & sign :- Pain- Function- Inflammation- Range of motion
- Pain severity & previous Rx- Activity of daily living - Night pain / morning stiffness / effusion- Range of motion of specific joint / deformity
• Co-morbidity Underlying disease
X-ray Findings
• Non-uniform joint space narrowing
• Irregular joint surface
• Subchondral bone sclerosis / cyst
• Osteophyte
Gull-wing appearanceInflammatory / Erosive OA
• Disc space narrowing• Sclerosis of endplate• Osteophyte• Scoliosis
Vaccuum sign
12/17/2020
8
VACUUM SIGN
• Linear radiolucent defect, typical central gas collection
• Nitrogen gas accumulations in annular & nuclear degen fissure
• Indicative of ADVANCED DISC DEGENERATION
OSTEOARTHRITIS
• Non-pharmacologic Rx : Patient education, correct modifiable risk factor
• Pharmacologic Rx :Symptom-modifying :
1st line – Acetaminophen 2nd line – NSAID/Coxib (อายุ <75, ไม่มขีอ้หา้ม)
Topical NSAID3rd line – Tramadol
+/- IA Steroid if effusionStructural-modifying : ?
(อายุ >75, มขีอ้หา้ม)
< 3 g/day< 650 mg/dose
Surgery : 1. Pain out of control 2. Deformity
Patient Education
• Basic knowledge of disease
• Correct modifying factor :
Weight control
↓ Joint burden
Muscle strengthening
Suspected RA SUSPECTED RA
Disease Ask : pain/swellingmorning stiffnessfunction
Inspect : joint inflam, subluxation, deformityskin – vasculitiseye – episcleritis/scleritisLungs - ILD
Palpate : synovial thickening & fluidnodulesplenomegalylymph node
ROM
Complication of disease Extensor tendon ruptureCTSC1-2 subluxation
Disease association Sjogren’sOther CNT diseaseCo-morbidity
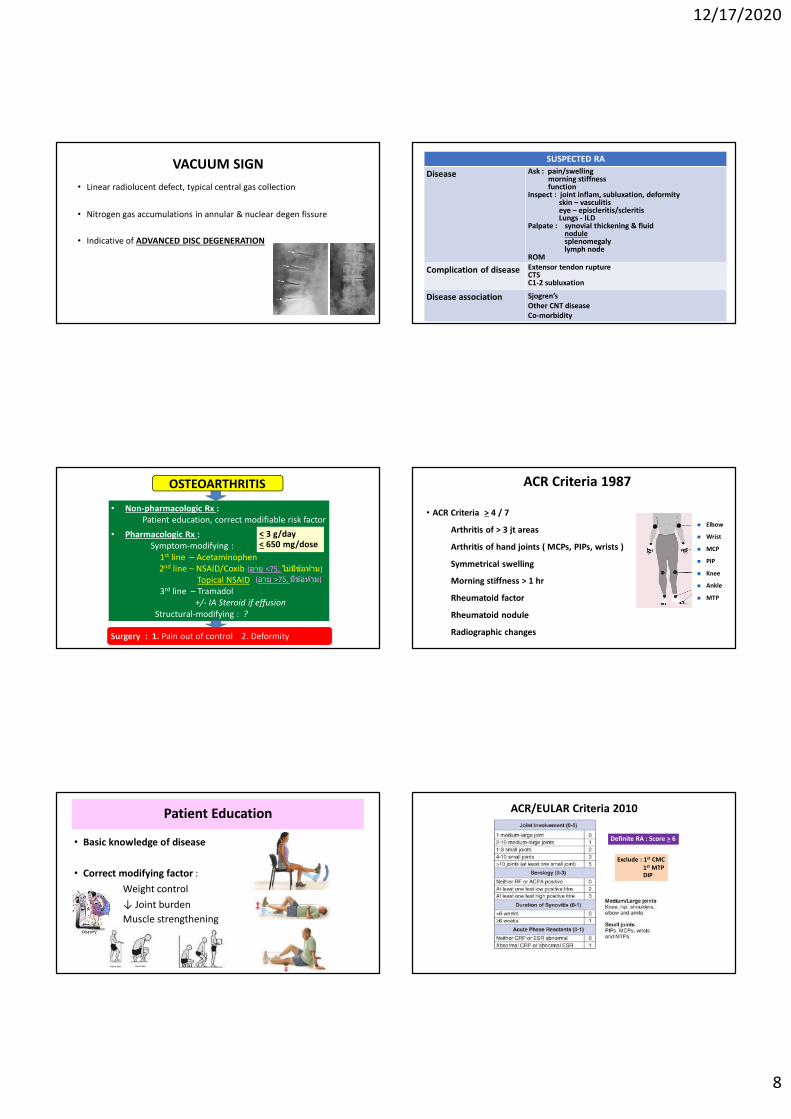
ACR Criteria 1987
• ACR Criteria > 4 / 7
Arthritis of > 3 jt areas
Arthritis of hand joints ( MCPs, PIPs, wrists )
Symmetrical swelling
Morning stiffness > 1 hr
Rheumatoid factor
Rheumatoid nodule
Radiographic changes
> 6 weeks
Elbow
Wrist
MCP
PIP
Knee
Ankle
MTP
ACR/EULAR Criteria 2010
Definite RA : Score > 6
Exclude : 1st CMC1st MTPDIP
12/17/2020
9
Subcutaneous nodule
Subluxation of metatarsal bone
L : Lateral 2 Lumbricoids
O : Opponen pollicis
A : Abductor pollicis brevis
F : Flexor pollicis brevis
CARPAL TUNNEL SYNDROME
TINEL’S TEST PHALEN’S TEST
Sensitivity 67% Specificity 68%
Sensitivity 85% Specificity 89%
COMMON COMPLICATIONS
• Cervical spine subluxation : C1-C2Extension Flexion
• Atlanto-dental interval (ADI) > 3 mm
• Subaxial subluxation
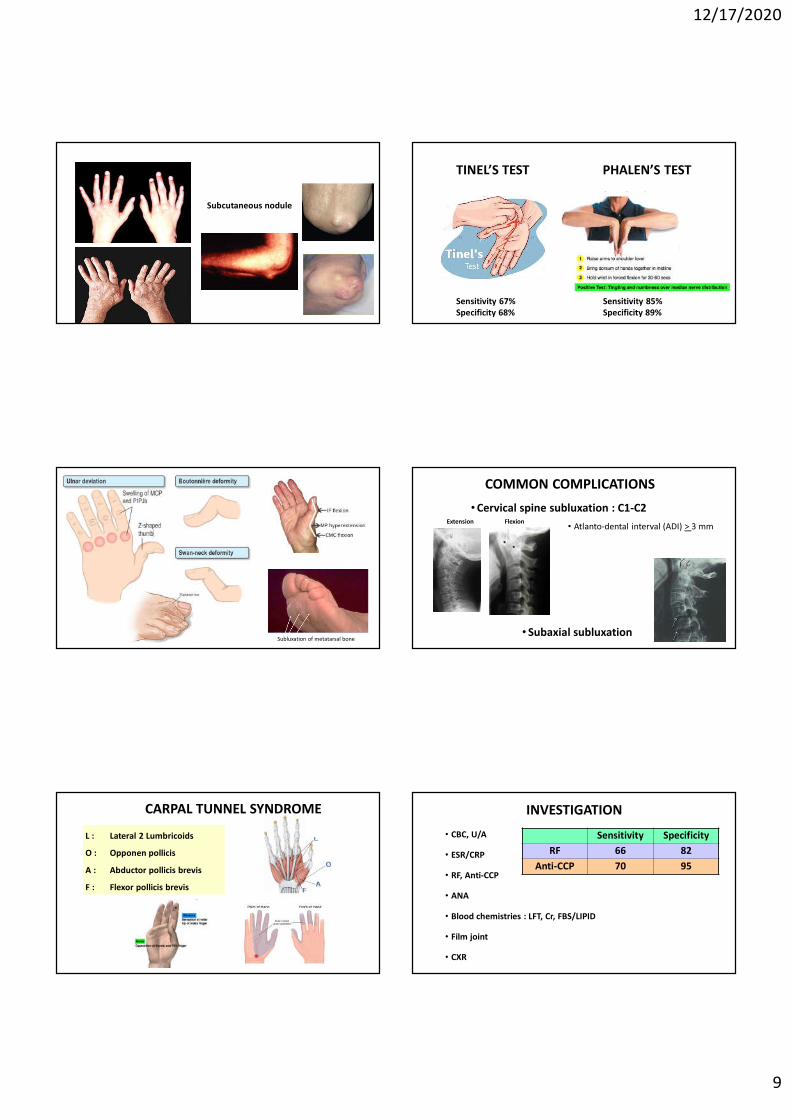
INVESTIGATION
• CBC, U/A
• ESR/CRP
• RF, Anti-CCP
• ANA
• Blood chemistries : LFT, Cr, FBS/LIPID
• Film joint
• CXR
Sensitivity Specificity
RF 66 82
Anti-CCP 70 95
12/17/2020
10
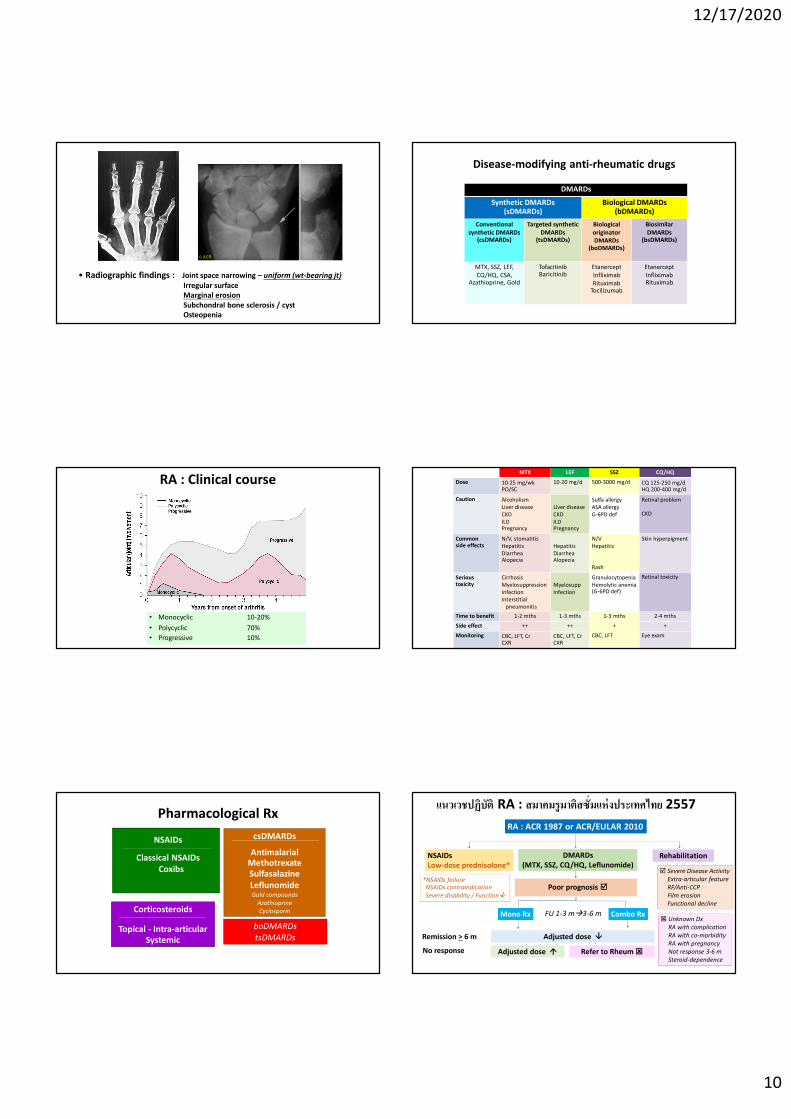
• Radiographic findings : Joint space narrowing – uniform (wt-bearing jt)Irregular surfaceMarginal erosionSubchondral bone sclerosis / cystOsteopenia
RA : Clinical course
• Monocyclic 10-20%
• Polycyclic 70%
• Progressive 10%
Pharmacological Rx
NSAIDs
Classical NSAIDsCoxibs
csDMARDs
AntimalarialMethotrexateSulfasalazineLeflunomideGold compounds
AzathioprineCyclosporinCorticosteroids
Topical - Intra-articularSystemic
boDMARDstsDMARDs
Disease-modifying anti-rheumatic drugs
DMARDs
Synthetic DMARDs(sDMARDs)
Biological DMARDs(bDMARDs)
Conventional synthetic DMARDs
(csDMARDs)
Targeted synthetic DMARDs
(tsDMARDs)
Biological originator DMARDs
(boDMARDs)
Biosimilar DMARDs
(bsDMARDs)
MTX, SSZ, LEF, CQ/HQ, CSA,
Azathioprine, Gold
TofacitinibBaricitinib
EtanerceptInfliximabRituximab
Tocilizumab
EtanerceptInfliximabRituximab
MTX LEF SSZ CQ/HQ
Dose 10-25 mg/wkPO/SC
10-20 mg/d 500-3000 mg/d CQ 125-250 mg/dHQ 200-400 mg/d
Caution AlcoholismLiver diseaseCKDILDPregnancy
Liver diseaseCKDILDPregnancy
Sulfa allergyASA allergyG-6PD def
Retinal problem
CKD
Common side effects
N/V, stomatitis Hepatitis DiarrheaAlopecia
HepatitisDiarrheaAlopecia
N/VHepatitis
Rash
Skin hyperpigment
Serious toxicity
CirrhosisMyelosuppressionInfectionInterstitial
pneumonitis
MyelosuppInfection
GranulocytopeniaHemolytic anemia (G-6PD def)
Retinal toxicity
Time to benefit 1-2 mths 1-3 mths 1-3 mths 2-4 mths
Side effect ++ ++ + +
Monitoring CBC, LFT, CrCXR
CBC, LFT, CrCXR
CBC, LFT Eye exam
แนวเวชปฏิบัติ RA : สมาคมรูมาติสซั�มแห่งประเทศไทย 2557
Poor prognosis
Mono Rx Combo Rx
RA : ACR 1987 or ACR/EULAR 2010
DMARDs (MTX, SSZ, CQ/HQ, Leflunomide)
NSAIDsLow-dose prednisolone*
Rehabilitation
*NSAIDs failure NSAIDs contraindication Severe disability / Function
Mono Rx Combo RxFU 1-3 m3-6 m
Remission > 6 m
Severe Disease ActivityExtra-articular featureRF/Anti-CCPFilm erosionFunctional decline
Adjusted dose
No response Adjusted dose Refer to Rheum
Unknown DxRA with complicationRA with co-morbidityRA with pregnancyNot response 3-6 mSteroid-dependence
12/17/2020
11
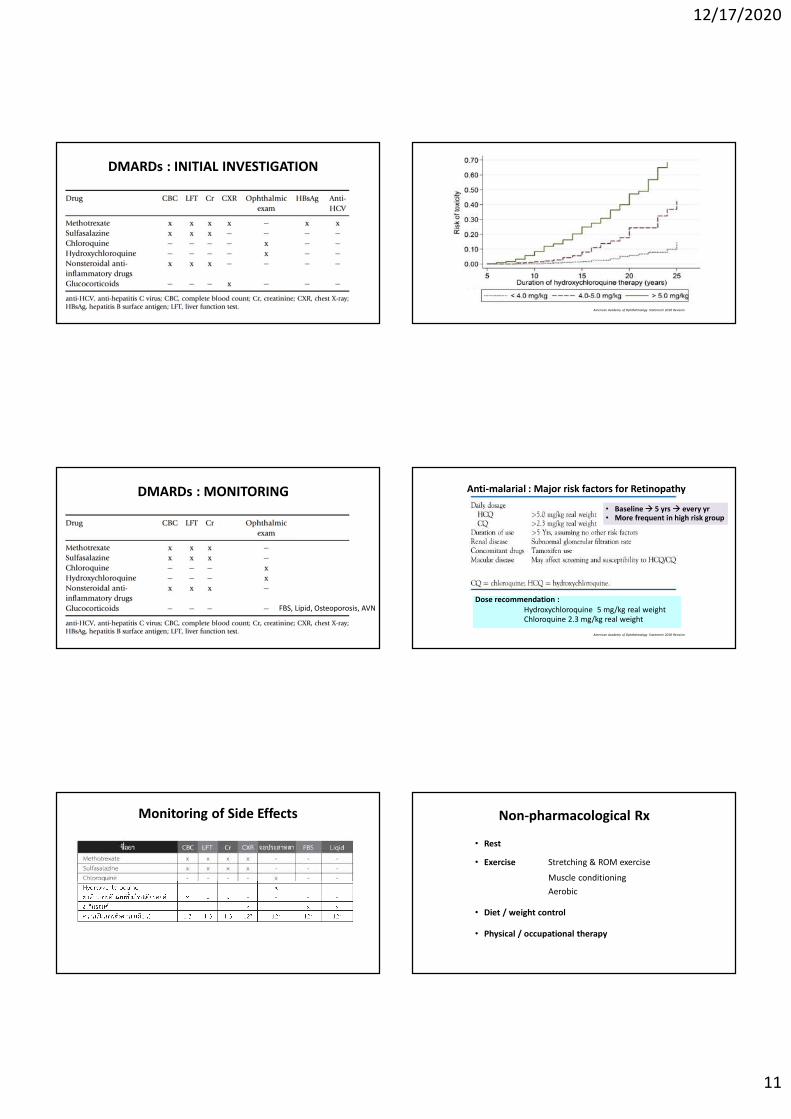
DMARDs : INITIAL INVESTIGATION
DMARDs : MONITORING
FBS, Lipid, Osteoporosis, AVN
Monitoring of Side Effects
American Academy of Ophthalmology Statement 2018 Revision
Anti-malarial : Major risk factors for Retinopathy
Dose recommendation :Hydroxychloroquine 5 mg/kg real weightChloroquine 2.3 mg/kg real weight
American Academy of Ophthalmology Statement 2018 Revision
• Baseline 5 yrs every yr• More frequent in high risk group
Non-pharmacological Rx
• Rest
• Exercise Stretching & ROM exercise
Muscle conditioning
Aerobic
• Diet / weight control
• Physical / occupational therapy
12/17/2020
12
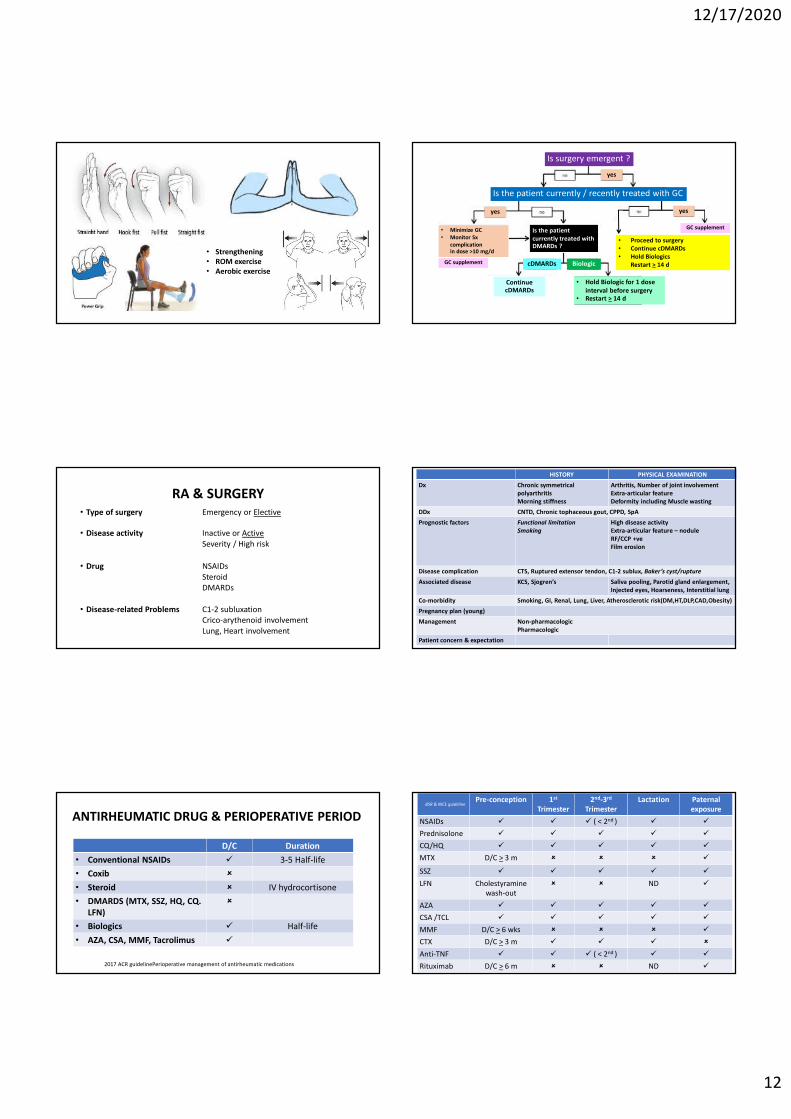
• Strengthening• ROM exercise• Aerobic exercise
RA & SURGERY• Type of surgery Emergency or Elective
• Disease activity Inactive or ActiveSeverity / High risk
• Drug NSAIDsSteroidDMARDs
• Disease-related Problems C1-2 subluxationCrico-arythenoid involvementLung, Heart involvement
D/C Duration
• Conventional NSAIDs 3-5 Half-life
• Coxib
• Steroid IV hydrocortisone
• DMARDS (MTX, SSZ, HQ, CQ. LFN)
• Biologics Half-life
• AZA, CSA, MMF, Tacrolimus
ANTIRHEUMATIC DRUG & PERIOPERATIVE PERIOD
2017 ACR guidelinePerioperative management of antirheumatic medications
Is surgery emergent ?
Is the patient currently / recently treated with GC
GC supplement
• Proceed to surgery• Continue cDMARDs• Hold Biologics
Restart > 14 d
yes
yesyes
• Minimize GC • Monitor Sx
complication in dose >10 mg/d
GC supplement
Is the patient currently treated with DMARDs ?
BiologiccDMARDs
Continue cDMARDs
• Hold Biologic for 1 dose interval before surgery
• Restart > 14 d
HISTORY PHYSICAL EXAMINATION
Dx Chronic symmetrical polyarthritisMorning stiffness
Arthritis, Number of joint involvementExtra-articular featureDeformity including Muscle wasting
DDx CNTD, Chronic tophaceous gout, CPPD, SpA
Prognostic factors Functional limitationSmoking
High disease activityExtra-articular feature – noduleRF/CCP +veFilm erosion
Disease complication CTS, Ruptured extensor tendon, C1-2 sublux, Baker’s cyst/rupture
Associated disease KCS, Sjogren’s Saliva pooling, Parotid gland enlargement,Injected eyes, Hoarseness, Interstitial lung
Co-morbidity Smoking, GI, Renal, Lung, Liver, Atherosclerotic risk(DM,HT,DLP,CAD,Obesity)
Pregnancy plan (young)
Management Non-pharmacologicPharmacologic
Patient concern & expectation
Pre-conception 1st
Trimester2nd-3rd
TrimesterLactation Paternal
exposure
NSAIDs ( < 2nd )
Prednisolone
CQ/HQ
MTX D/C > 3 m
SSZ
LFN Cholestyramine wash-out
ND
AZA
CSA /TCL
MMF D/C > 6 wks
CTX D/C > 3 m
Anti-TNF ( < 2nd )
Rituximab D/C > 6 m ND
BSR & NICE guideline
12/17/2020
13
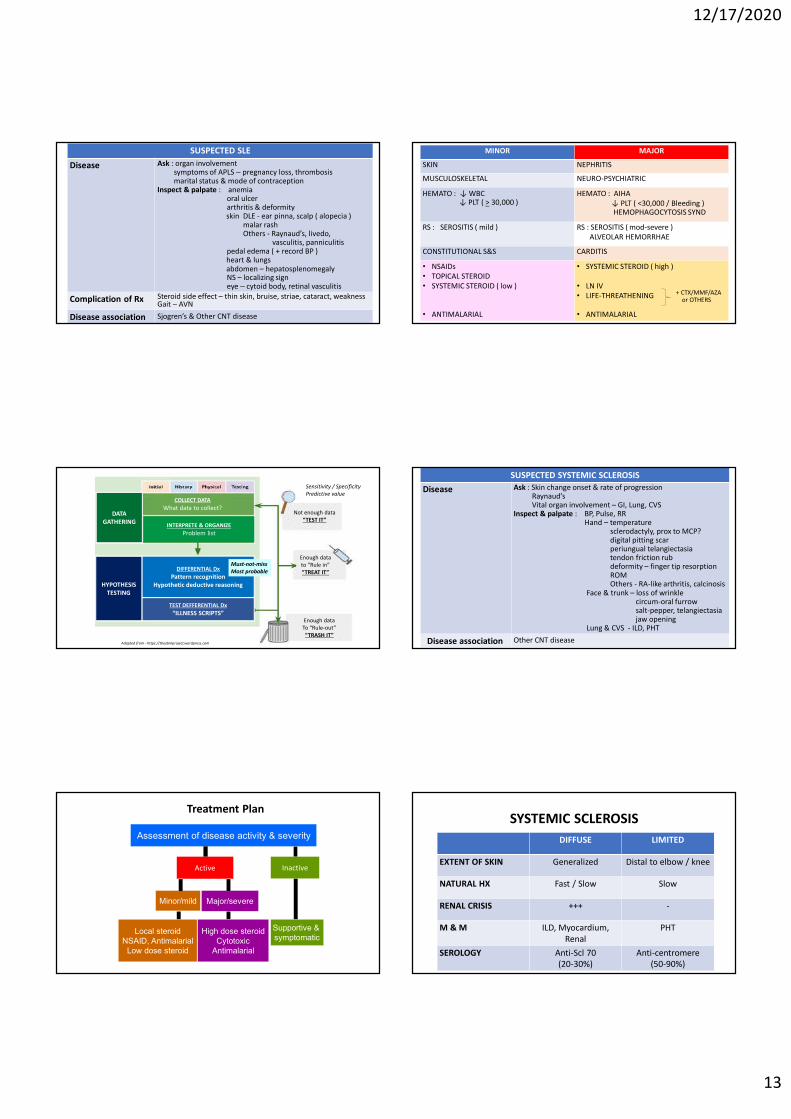
Suspected RA SUSPECTED SLE
Disease Ask : organ involvementsymptoms of APLS – pregnancy loss, thrombosismarital status & mode of contraception
Inspect & palpate : anemiaoral ulcerarthritis & deformityskin DLE - ear pinna, scalp ( alopecia )
malar rashOthers - Raynaud’s, livedo,
vasculitis, panniculitispedal edema ( + record BP )heart & lungsabdomen – hepatosplenomegalyNS – localizing signeye – cytoid body, retinal vasculitis
Complication of Rx Steroid side effect – thin skin, bruise, striae, cataract, weaknessGait – AVN
Disease association Sjogren’s & Other CNT disease
Not enough data“TEST IT”
Enough data to “Rule in”“TREAT IT”
Enough data To “Rule-out”“TRASH IT”
COLLECT DATA
What data to collect?
INTERPRETE & ORGANIZE
Problem list
Adapted from - https://theebmproject.wordpress.com
DIFFERENTIAL Dx
Pattern recognitionHypothetic deductive reasoning
TEST DEFFERENTIAL Dx
“ILLNESS SCRIPTS”
HYPOTHESIS TESTING
DATA GATHERING
Must-not-missMost probable
Sensitivity / Specificity Predictive value
Treatment Plan
Assessment of disease activity & severity
Active Inactive
Major/severeMinor/mild
Supportive & symptomatic
Local steroidNSAID, Antimalarial
Low dose steroid
High dose steroidCytotoxic
Antimalarial
MINOR MAJOR
SKIN NEPHRITIS
MUSCULOSKELETAL NEURO-PSYCHIATRIC
HEMATO : ↓ WBC↓ PLT ( > 30,000 )
HEMATO : AIHA↓ PLT ( <30,000 / Bleeding )HEMOPHAGOCYTOSIS SYND
RS : SEROSITIS ( mild ) RS : SEROSITIS ( mod-severe )ALVEOLAR HEMORRHAE
CONSTITUTIONAL S&S CARDITIS
• NSAIDs• TOPICAL STEROID• SYSTEMIC STEROID ( low )
• ANTIMALARIAL
• SYSTEMIC STEROID ( high )
• LN IV• LIFE-THREATHENING
• ANTIMALARIAL
+ CTX/MMF/AZAor OTHERS
Suspected RASUSPECTED SYSTEMIC SCLEROSIS
Disease Ask : Skin change onset & rate of progressionRaynaud’sVital organ involvement – GI, Lung, CVS
Inspect & palpate : BP, Pulse, RRHand – temperature
sclerodactyly, prox to MCP?digital pitting scarperiungual telangiectasiatendon friction rubdeformity – finger tip resorptionROMOthers - RA-like arthritis, calcinosis
Face & trunk – loss of wrinklecircum-oral furrowsalt-pepper, telangiectasiajaw opening
Lung & CVS - ILD, PHT
Disease association Other CNT disease
SYSTEMIC SCLEROSIS
DIFFUSE LIMITED
EXTENT OF SKIN Generalized Distal to elbow / knee
NATURAL HX Fast / Slow Slow
RENAL CRISIS +++ -
M & M ILD, Myocardium, Renal
PHT
SEROLOGY Anti-Scl 70 (20-30%)
Anti-centromere (50-90%)
12/17/2020
14
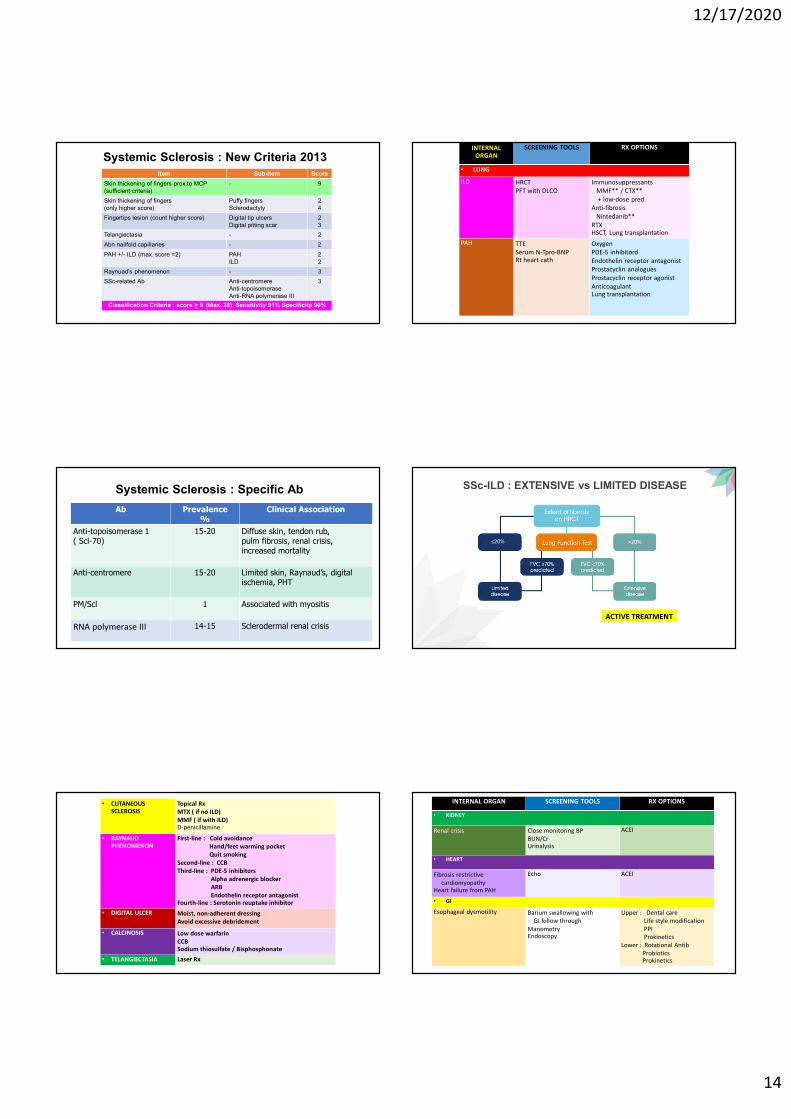
Systemic Sclerosis : New Criteria 2013Item Sub-Item Score
Skin thickening of fingers prox.to MCP (sufficient criteria)
- 9
Skin thickening of fingers (only higher score)
Puffy fingersSclerodactyly
24
Fingertips lesion (count higher score) Digital tip ulcersDigital pitting scar
23
Telangiectasia - 2
Abn nailfold capillaries - 2
PAH +/- ILD (max. score =2) PAHILD
22
Raynuad’s phenomenon - 3
SSc-related Ab Anti-centromereAnti-topoisomeraseAnti-RNA polymerase III
3
Classification Criteria : score > 9 (Max. 28) Sensitivity 91% Specificity 90%
Systemic Sclerosis : Specific Ab
Ab Prevalence %
Clinical Association
Anti-topoisomerase 1 ( Scl-70)
15-20 Diffuse skin, tendon rub, pulm fibrosis, renal crisis, increased mortality
Anti-centromere 15-20 Limited skin, Raynaud’s, digital ischemia, PHT
PM/Scl 1 Associated with myositis
RNA polymerase III 14-15 Sclerodermal renal crisis
• CUTANEOUS SCLEROSIS
Topical RxMTX ( if no ILD)MMF ( if with ILD)D-penicillamine
• RAYNAUD PHENOMENON
First-line : Cold avoidanceHand/feet warming pocketQuit smoking
Second-line : CCBThird-line : PDE-5 inhibitors
Alpha adrenergic blockerARBEndothelin receptor antagonist
Fourth-line : Serotonin reuptake inhibitor
• DIGITAL ULCER Moist, non-adherent dressingAvoid excessive debridement
• CALCINOSIS Low dose warfarinCCBSodium thiosulfate / Bisphosphonate
• TELANGIECTASIA Laser Rx
INTERNAL ORGAN
SCREENING TOOLS RX OPTIONS
• LUNG
ILD HRCTPFT with DLCO
ImmunosuppressantsMMF** / CTX** + low-dose pred
Anti-fibrosisNintedanib**
RTX HSCT, Lung transplantation
PAH TTESerum N-Tpro-BNPRt heart cath
OxygenPDE-5 inhibitordEndothelin receptor antagonistProstacyclin analoguesProstacyclin receptor agonistAnticoagulantLung transplantation
SSc-ILD : EXTENSIVE vs LIMITED DISEASE
<20% >20%
ACTIVE TREATMENT
INTERNAL ORGAN SCREENING TOOLS RX OPTIONS
• KIDNEY
Renal crisis Close monitoring BPBUN/CrUrinalysis
ACEI
• HEART
Fibrosis restrictive cardiomyopathy
Heart failure from PAH
Echo ACEI
• GI
Esophageal dysmotility Barium swallowing with GI follow through
ManometryEndoscopy
Upper : Dental careLife style modificationPPIProkinetics
Lower : Rotational AntibProbioticsProkinetics







