

Course: IDPT 5005Course: IDPT 5005School of Medicine, School of Medicine, UCDHSCUCDHSC
Urinary Tract Infections & Urinary Tract Infections & Tubulointerstitial Kidney Tubulointerstitial Kidney Diseases Diseases
Francisco G. La Rosa, MDFrancisco G. La Rosa, [email protected]@ucdenver.eduAssociate Professor, Department of PathologyAssociate Professor, Department of Pathology
University of Colorado Denver Health Sciences Programs, Denver, Colorado University of Colorado Denver Health Sciences Programs, Denver, Colorado 8004580045

Urinary TractUrinary Tract

ANATOMY OF THE KIDNEYANATOMY OF THE KIDNEY
1. Renal Vein 1. Renal Vein 2. Renal Artery 2. Renal Artery 3. Renal Calyx 3. Renal Calyx 4. Medullary Pyramid 4. Medullary Pyramid 5. Renal Cortex 5. Renal Cortex 6. Segmental Artery 6. Segmental Artery 7. Interlobar Artery 7. Interlobar Artery 8. Arcuate Artery 8. Arcuate Artery 9. Arcuate Vein 9. Arcuate Vein 10. Interlobar Vein 10. Interlobar Vein 11. Segmental Vein 11. Segmental Vein 12. Renal Column 12. Renal Column 13. Renal Papillae13. Renal Papillae (papillary or Bellini’s ducts)(papillary or Bellini’s ducts)
14. Renal Pelvis 14. Renal Pelvis 15. Ureter 15. Ureter

Kidney: Normal Kidney: Normal HistologyHistology

Kidney: Normal Kidney: Normal HistologyHistology

• CommonCommon• Mostly confined to lower GU tract (cystitis)Mostly confined to lower GU tract (cystitis)• May involve upper GU tract (pyelonephritis, May involve upper GU tract (pyelonephritis,
calculi)calculi)• Chronic pyelonephritisChronic pyelonephritis
−Associated with obstruction, VU-refluxAssociated with obstruction, VU-reflux−Chronic renal failureChronic renal failure−HypertensionHypertension
Urinary Tract Urinary Tract InfectionsInfections

Prevalence of bacteriuria in different age Prevalence of bacteriuria in different age groups:groups:
• Ascending infection – most commonAscending infection – most common− E. coliE. coli (~70%) – uropathogenic strains (~70%) – uropathogenic strains− Proteus, Pseudomonas, Klebsiella,Proteus, Pseudomonas, Klebsiella, etc. etc.
(recurrent, hospital acquired)(recurrent, hospital acquired)
• HematogenousHematogenous− Debilitated patientsDebilitated patients− Kidney injuryKidney injury− S. aureusS. aureus (catalase +), group A Strep, (catalase +), group A Strep,
opportunistic (immunocompromised)opportunistic (immunocompromised)− Clinical setting: septicemia, endocarditisClinical setting: septicemia, endocarditis
Urinary Tract Infections:Urinary Tract Infections:Routes of InfectionRoutes of Infection


Virulence FactorsVirulence Factors Host DefensesHost Defenses
Urinary Tract Infections:Urinary Tract Infections:PathogenesisPathogenesis

• Bacterial Adhesion: Pili (P or fimbria)Bacterial Adhesion: Pili (P or fimbria)• ““O” Antigens (certain strains more resistant)O” Antigens (certain strains more resistant)• Endotoxin (Endotoxin (↓ ureteric peristalsis)↓ ureteric peristalsis)
Virulence FactorsVirulence Factors
Host DefensesHost Defenses
Urinary Tract Infections:Urinary Tract Infections:PathogenesisPathogenesis
uropathogenuropathogenicic
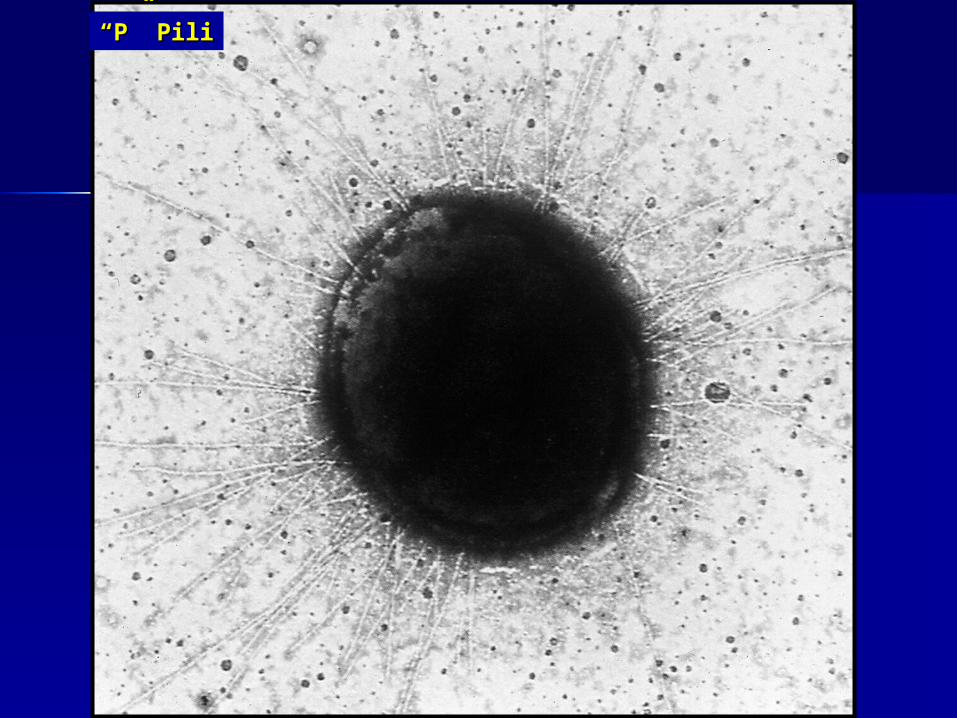
““P” PiliP” Pili

Cultured epithelial cellsCultured epithelial cells
+ + E. coliE. coli
DAPIDAPI4'-6-Diamidino-2-phenylindole4'-6-Diamidino-2-phenylindole
Fluorescein-labeledFluorescein-labeled““Anti-P” fimbriaAnti-P” fimbria
Bacterial AdhesionBacterial Adhesion

““O” AntigensO” Antigens(certain strains(certain strainsmore resistant)more resistant)

• Mechanical (Hydrokinetic)Mechanical (Hydrokinetic)• Chemical (Urine)Chemical (Urine)• ImmunologicalImmunological• CellularCellular
Virulence FactorsVirulence Factors
Host DefensesHost Defenses
Urinary Tract Infections:Urinary Tract Infections:PathogenesisPathogenesis

Urinary Tract Infections:Urinary Tract Infections:Pathogenesis – Host Pathogenesis – Host DefenseDefense
• Mechanical:Mechanical:– Bladder emptying/ urine flow– Ureteric peristalsis– Mucus
• Chemical:Chemical:– Prostatic secretions (antibacterial)– Urine osmolality, pH, Ammonia– Blood group Ag’s (P2<<P1)

Urinary Tract Infections:Urinary Tract Infections:Pathogenesis – Host Pathogenesis – Host DefenseDefense
• Immunological:Immunological:– Ig A– Complement
• Cellular:Cellular:– PMNs– Sheding urothelial cells

• Females > MalesFemales > Males− Short urethraShort urethra− Bacterial colonizationBacterial colonization− Urethral trauma (“honeymoon” cystitis)Urethral trauma (“honeymoon” cystitis)
• InstrumentationInstrumentation• Decreased urine flow / urine stasisDecreased urine flow / urine stasis
− Incomplete voidingIncomplete voiding− Urinary tract obstructionUrinary tract obstruction− DiverticulumDiverticulum− Neurogenic bladderNeurogenic bladder
• CalculiCalculi• Vesicoureteral refluxVesicoureteral reflux• Immune compromiseImmune compromise• Kidney / UT diseaseKidney / UT disease• PregnancyPregnancy
Urinary Tract Infections:Urinary Tract Infections:Pathogenesis – Predisposing Pathogenesis – Predisposing FactorsFactors

• Covert bacteriuriaCovert bacteriuria
• Symptomatic UTI:Symptomatic UTI:− Reflective of level of Reflective of level of
infectioninfection− Recurrent infection in Recurrent infection in
males usually indicates males usually indicates UT diseaseUT disease
• Early childhood: Early childhood: − symptoms nonspecificsymptoms nonspecific− Irritability, convulsionsIrritability, convulsions
Urinary Tract Urinary Tract Infections:Infections:Clinical ManifestationsClinical Manifestations
SymptomsSymptoms



• RecurrenceRecurrence• Acute pyelonephritisAcute pyelonephritis• Renal/perinephric abscessRenal/perinephric abscess• Papillary necrosis (diabetes)Papillary necrosis (diabetes)• Staghorn calculi (Staghorn calculi (ProteusProteus))• Chronic pyelonephritis/renal scarringChronic pyelonephritis/renal scarring
Urinary Tract Urinary Tract Infections:Infections:ComplicationsComplications

Acute pyelonephritisAcute pyelonephritis

Acute pyelonephritisAcute pyelonephritis
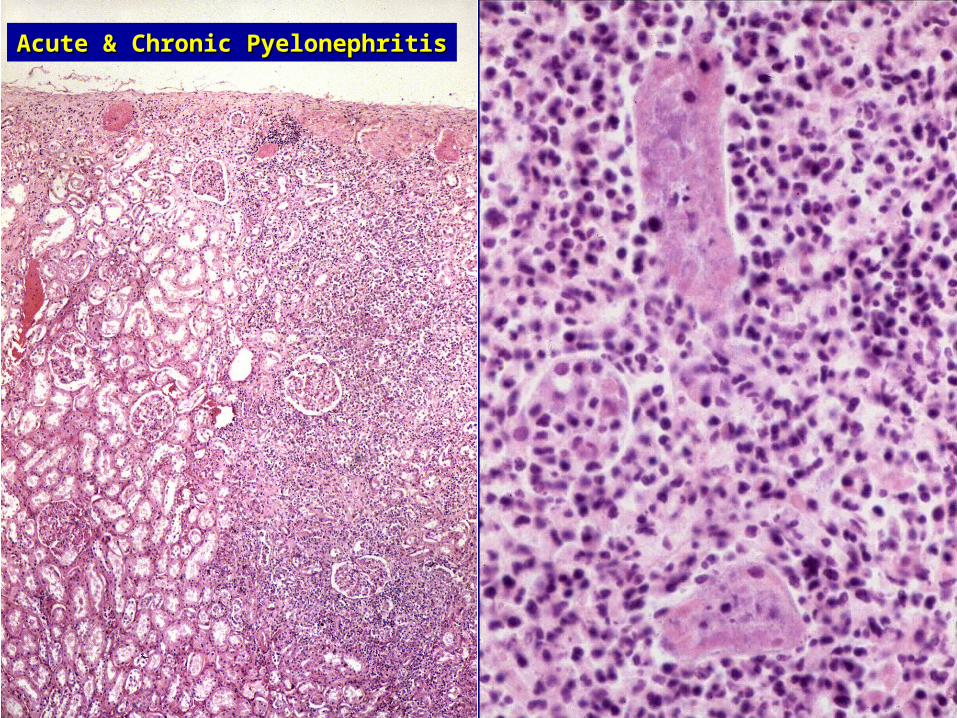
Acute & Chronic PyelonephritisAcute & Chronic Pyelonephritis

microabscessesmicroabscesses

PyonephrosisPyonephrosisNecrotizing papillitisNecrotizing papillitis

Staghorn calculusStaghorn calculus

Causes:Causes:
• Urinary tract obstructionUrinary tract obstruction
• Vesicoureteral reflux (VUR)Vesicoureteral reflux (VUR)
Urinary Tract Infections:Urinary Tract Infections:Chronic PyelonephritisChronic Pyelonephritis

• Obstruction predisposes to infectionObstruction predisposes to infection• Obstruction interferes with eradicationObstruction interferes with eradication• Obstruction predisposes to recurrenceObstruction predisposes to recurrence• Obstruction + InfectionObstruction + Infection
− ↑↑ pressurepressure
− inflammationinflammation− ischemiaischemia− direct injurydirect injury
Chronic Chronic pyelonephritispyelonephritis
Urinary Tract Urinary Tract Obstruction:Obstruction:Relationship with infectionRelationship with infection

• IntrinsicIntrinsic− Exophytic: tumors of UTExophytic: tumors of UT− CalculiCalculi− Sloughed necrotic papillaeSloughed necrotic papillae− Blood clotsBlood clots
• StrictureStricture• Urethral valvesUrethral valves• Extrinsic compressionExtrinsic compression
− Tumors (pelvic, retroperitoneal)Tumors (pelvic, retroperitoneal)− Retroperitoneal fibrosisRetroperitoneal fibrosis− HemorrhageHemorrhage− IatrogenicIatrogenic
• FunctionalFunctional− Neurologic diseaseNeurologic disease− DMDM
• IdiopathicIdiopathic
Causes of Urinary Tract Causes of Urinary Tract Obstruction:Obstruction:

• HydronephrosisHydronephrosis• InfectionInfection
− AcuteAcute− Recurrent / persistentRecurrent / persistent
• Chronic obstructive pyelonephritisChronic obstructive pyelonephritis• Renal failureRenal failure• HypertensionHypertension
Urinary Tract Urinary Tract Obstruction:Obstruction:ConsequencesConsequences

Urinary Tract Obstruction:Urinary Tract Obstruction:HydronephrosisHydronephrosis

Urinary Tract Obstruction:Urinary Tract Obstruction:HydronephrosisHydronephrosis

Vesicoureteral reflux (VUR)Vesicoureteral reflux (VUR)

• Primary− Congenital abnormality of VU anatomy
− Common in infants
− Decreases in freq & severity during childhood
− Usually mild
• Secondary− Congenital malformations
− Neurogenic bladder (paraplegia, spina bifida)
− Obstruction
− Older children, adults
Vesicoureteral reflux (VUR)Vesicoureteral reflux (VUR)


NormalNormal VURVUR

Vesicoureteral reflux Vesicoureteral reflux (VUR)(VUR)

• Severe, persistent reflux + infectionSevere, persistent reflux + infection− Allows organisms to access renal parenchymaAllows organisms to access renal parenchyma
• Renal scars directly over dilated calycesRenal scars directly over dilated calyces− More extensive at poles (compound vs. simple papillae)More extensive at poles (compound vs. simple papillae)− Often unilateral or unequal bilateralOften unilateral or unequal bilateral
Reflux NephropathyReflux Nephropathy::Chronic Non-obstructive PyelonephritisChronic Non-obstructive Pyelonephritis

Typical coarse scars of chronic pyelonephritis Typical coarse scars of chronic pyelonephritis associated with vesicoureteral reflux. The scars are associated with vesicoureteral reflux. The scars are
usually polar and are associated with underlying usually polar and are associated with underlying blunted calyces.blunted calyces.

Reflux NephropathyReflux Nephropathy

Reflux Nephropathy:Reflux Nephropathy:

Reflux Nephropathy:Reflux Nephropathy:Chronic Non-obstructive PyelonephritisChronic Non-obstructive Pyelonephritis
• Micro: Atrophy, “periglomerular Micro: Atrophy, “periglomerular fibrosis”fibrosis”
• Focal Segmental Glomerulosclerosis) Focal Segmental Glomerulosclerosis) (?)(?)
• Chronic renal failureChronic renal failure• HypertensionHypertension


Questions?Questions?

Disclaimer:Disclaimer:
The images and texts presented in this slide show are solely for The images and texts presented in this slide show are solely for educational purposes and not intended for commercial or pecuniary educational purposes and not intended for commercial or pecuniary benefit. The images have been obtained from Dr. La Rosa’s benefit. The images have been obtained from Dr. La Rosa’s personal collection, from text books used during the teaching of personal collection, from text books used during the teaching of this chapter, and from published articles and educational works. this chapter, and from published articles and educational works. Reproduction of these images can be done only for educational use.Reproduction of these images can be done only for educational use. Reference: USA Copyright Law, Section 110, “Limitations on Reference: USA Copyright Law, Section 110, “Limitations on exclusive rights: Exemption of certain performances and displays”).exclusive rights: Exemption of certain performances and displays”).[[Download] the USA Copyright Law version, October 2009.] the USA Copyright Law version, October 2009.







