

1lineVirginia Health Information 2008
Creating the Hybrid Database and Overview of Cardiac Care
Michael Pine, M.D., M.B.A.Michael Pine and Associates, Inc
Ramesh K. Shukla, PhDVirginia Commonwealth University

2lineVirginia Health Information 2008
Overview
Background
Empirical evidence
Pilot implementation

3lineVirginia Health Information 2008
Data for Monitoring Clinical Performance
Administrative Data – from Centers for Medicare and Medical Services (CMS) to Agency for Healthcare Research and Quality (AHRQ), VHI and HealthGrades.com
Clinical Data – from APACHE, PHC4 and Health Quality Choice to Specialty Society Registries (e.g., STS, ACC)

4lineVirginia Health Information 2008
Administrative Data v Clinical Data
Data serves as the basis for public reporting, pay-for-performance, and quality improvement initiatives
Must balance the need for data to enhance current risk-adjusted measurement of clinical performance and the cost of data collection

5lineVirginia Health Information 2008
Relative Ease of Data Collection
Standard Administrative
Numerical Laboratory
Vital Signs
Other Clinical DataManual
Automated
Dat
a C
olle
ctio
n
Administrative Data
Clinical Data

6lineVirginia Health Information 2008
Enhancing administrative Data
Present-on-Admission Coding – from Mayo, SPARCS, and OSHPD to the UB-04 and CMS
Numerical Laboratory Data – from MPA to AHRQ
New Hybrid Databases – AHRQ Pilot Projects

7lineVirginia Health Information 2008
Hybrid Database
Standard Administrative
Numerical Laboratory
Vital Signs
Other Clinical Data
Present-on-AdmissionAdministrative Data
Clinical Data
Hybrid Data

8lineVirginia Health Information 2008
Efficient Use of Clinical Data
Hemoglobin FEV1
Albumin Mental Status
Cost to CollectHighLow
Analytic Power
Low
High

9lineVirginia Health Information 2008
Benefits of Enhanced Administrative Data
Better distinguishes between comorbidities and complications
Adds objective findings to more subjective diagnostic designations
Provides finer definition of progression of disease and underlying pathophysiology than does diagnostic codes

10lineVirginia Health Information 2008
Lab Value and Gradation of Risk
CHF
MI
Sepsis
Distribution of Albumin Levels and Mortality Rates17.0
10.4
6.8
4.33.1
2.62.1
1.8 1.5 1.2 1.2 1.42.42.7
3.0
3.33.4 3.6 3.7 3.9
4.0 4.34.5
10.0
0
2
4
6
8
10
12
14
16
18
5 10 20 30 40 50 60 70 80 90 95 100
Percentile Cutoff
Mor
talit
y %
0
2
4
6
8
10
12
Lab
Valu
e C
utof
f
Mortality Rate Albumin in gm/dl

11lineVirginia Health Information 2008
Percentile Cutoff
Mor
talit
y % 16.8
19.5
18.1
12.5
9.8
8.27.8 7.9 8.5
10.7
13.9
20.6
19.0
26.129.2
33.1
35.137.1 39.1
42.145.1
50.1
61.5
75.5
0
5
10
15
20
25
1 5 10 20 30 40 50 60 70 80 90 950
10
20
30
40
50
60
70
80
Lab
Valu
e C
utof
f
Mortality Rate pCO2 Arterial mmHg
Distribution of pCO2 Levels and Mortality Rates
Complex Relation of Lab Value and Risk

12lineVirginia Health Information 2008
AHRQ Inpatient Quality Indicators (Mortality)
Medical Conditions – Acute Myocardial Infarction; Cerebrovascular Accident; Congestive Heart Failure; Gastrointestinal Hemorrhage; Pneumonia
Surgical Procedures – Abdominal Aortic Aneurysm Repair; Coronary Artery Bypass Graft Surgery; Craniotomy

13lineVirginia Health Information 2008
AHRQ Patient Safety Indicators (Complications)
Elective Surgical Procedures
Complications – Physiologic / Metabolic Abnormalities; Pulmonary Embolus / Deep Vein Thrombosis; Sepsis; Respiratory Failure

14lineVirginia Health Information 2008
Data Used in Administrative Models
Age and Sex
Principal Diagnosis
Secondary diagnoses only infrequently acquired during hospitalization
Selected surgical procedures

15lineVirginia Health Information 2008
Data Used in HYBRID Models
All data used in administrative models
Additional secondary diagnoses when clinical data establish that they were present on admission
Numerical laboratory data (e.g., creatinine, white blood cell count) generally available in electronic form

16lineVirginia Health Information 2008
Data Used in CLINICAL Models
All data used in HYBRID models
Vital signs and laboratory data not in HYBRID models (e.g., blood culture results)
Key clinical findings abstracted from medical records (e.g., immunocompromised)
Composite clinical scores (e.g., ASA Class)

17lineVirginia Health Information 2008
Types of Data in CLINICAL IQI Models
Standard Administrative
Numerical Laboratory
Vital Signs andOther Clinical Data
Present-on-Admission15.6 data elements
11.1 data elements
Hybrid Data
9.0 data elements
18lineVirginia Health Information 2008
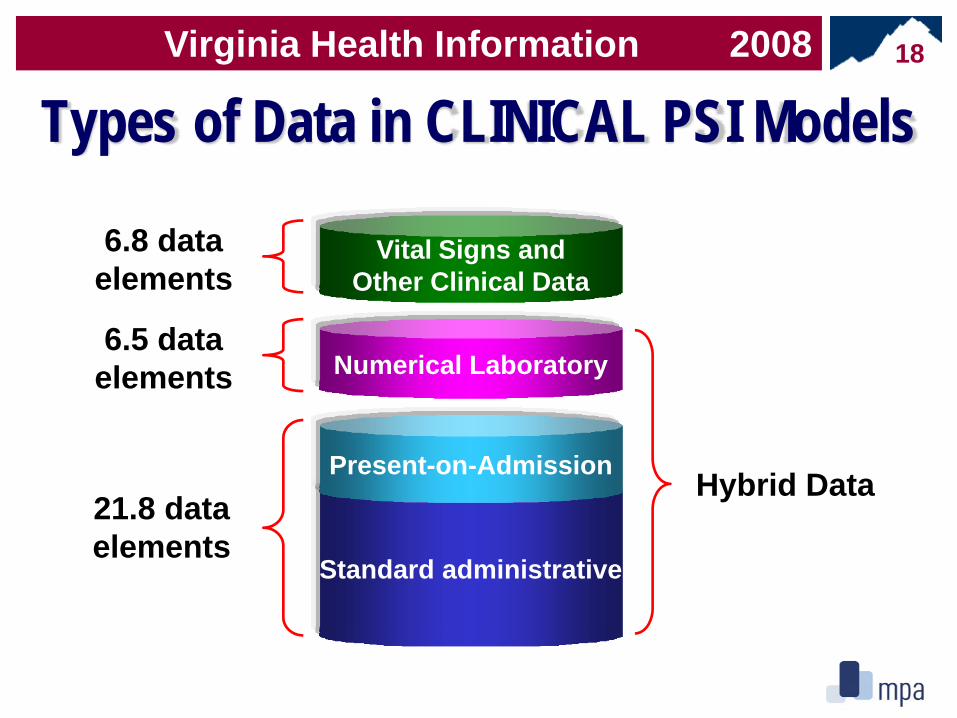
Types of Data in CLINICAL PSI Models
Standard administrative
Numerical Laboratory
Vital Signs andOther Clinical Data
Present-on-Admission21.8 data elements
6.5 data elements
Hybrid Data
6.8 data elements

19lineVirginia Health Information 2008
Bias Due to Suboptimal Risk-Adjustment
+ 2 Std Dev
Good Average Poor
- 2 Std Dev
Measured Performance
+ 0.5 Std Dev
Problematic Problematic
- 0.5 Std Dev
Bias
OK

20lineVirginia Health Information 2008
Bias Due to Suboptimal Data (IQIs)
0%
10%
20%
30%
40%
50%
60%
70%
0.5 1.0 1.5 2.0Upper Threshold for Bias in Standard Deviations
Perc
ent E
xcee
ding
Upp
erTh
resh
old
RAW CLAIMS HYBRID

21lineVirginia Health Information 2008
Recommended Chemistry Data• Aspartate Aminotransferase • Creatine Kinase MB• Albumin • Creatinine• Alkaline Phosphatase • Glucose• Amylase • Lactic Acid • Bicarbonate • Potassium• Bilirubin (Total) • Pro-B Natriuretic Protein• B Natriuretic Peptide • Sodium• Calcium • Troponin I• C-Reactive Protein • Troponin T• Creatine Kinase • Urea Nitrogen

22lineVirginia Health Information 2008
Other Recommended Lab DataBlood Gas Hematology
• Arterial O2 Saturation • Hemoglobin• Arterial pCO2 • International Normalized Ratio• Arterial pH • Neutrophil Bands• Arterial pO2 • Partial Thromboplastin Time• Base Excess • Platelet Count• Bicarbonate • Prothrombin Time• FIO2 (if electronic) • White Blood Count
23lineVirginia Health Information 2008
Enhancing VHI Public Reports of Hospital Performance –
Productivity, Efficiency and Quality Indicators
Ramesh K. Shukla, PhDProfessor and Director
Williamson InstituteDepartment of Health AdministrationVirginia Commonwealth University
24lineVirginia Health Information 2008
Existing Cardiac Care Volume, Mortality and Readmissions
• Open process of development and extensive testing
• Developed by VHI, Ramesh Shukla, Ph.D and extensive provider input
• Severity adjusted to level the playing field
• Based on patient level data• First published in 2002

25lineVirginia Health Information 2008
Enhancing VHI Cardiac Care Information
• Incorporate Lab and POA data into Cardiac Care dataset
• Develop and test model- does new data better explain variation?
• Share results with participating hospitals

26lineVirginia Health Information 2008
Present ModelPLD Data
Analyses APR‐DRGEstimating Expected Mortality
Estimating Actual
Mortality Rates
Mortality Ratio

27lineVirginia Health Information 2008
New & Enhanced ModelPLD
POA
APR-DRG Classification
Estimating Expected Mortality
Estimating Actual
Mortality Rates
MortalityRatio

28lineVirginia Health Information 2008
Model Research Base VHI/WIApproach
APR-DRG Base Model 3M Approach – tested for validity by the Williamson Institute
Cardiology Reports –Medical Cardiology, Invasive Cardiology and Open Heart after Validation by the WI
POA Model –APR-DRG with POA
Pine, et al using Diagnoses codes and POA – not tested with APR-DRG (C=.78)
POA Model will be tested by VHI/WI using APR-DRG and POA Diagnostic Codes
Lab Model –APR-DRG with POA & Lab
Same as above(C=.84)
Lab Model will be tested by VHI/WI using APR-DRG, POA Diagnostic Codes and Lab data
Clinical Model –APR-DRG with POA, Lab And Vital Signs
Same as above(C= .88)
Clinical Model will be tested by VHI/WI using APR-DRG, POA, Lab Data and Vital Signs







