

Notes compiled for Pediatrics
Dermatology (Med I, Block 6, DM)

Contents
Class number Class name Type Department Instructor
DM003 Acne L DM Dr. J Keddy-Grant
DM007 Dermatologic Infection L DM Dr. S Silver
DM008 Dermatitis L DM Dr. M Wiseman
7/22/2009
1
Acne Vulgaris and Related Conditions
By Jill Keddy-Grant M.D., FRCPC
Acne Vulgaris
–Common disease of the pilosebaceous unit
–Usually seen in adolescents
–Can be seen at any age
–Due to the rise in androgens
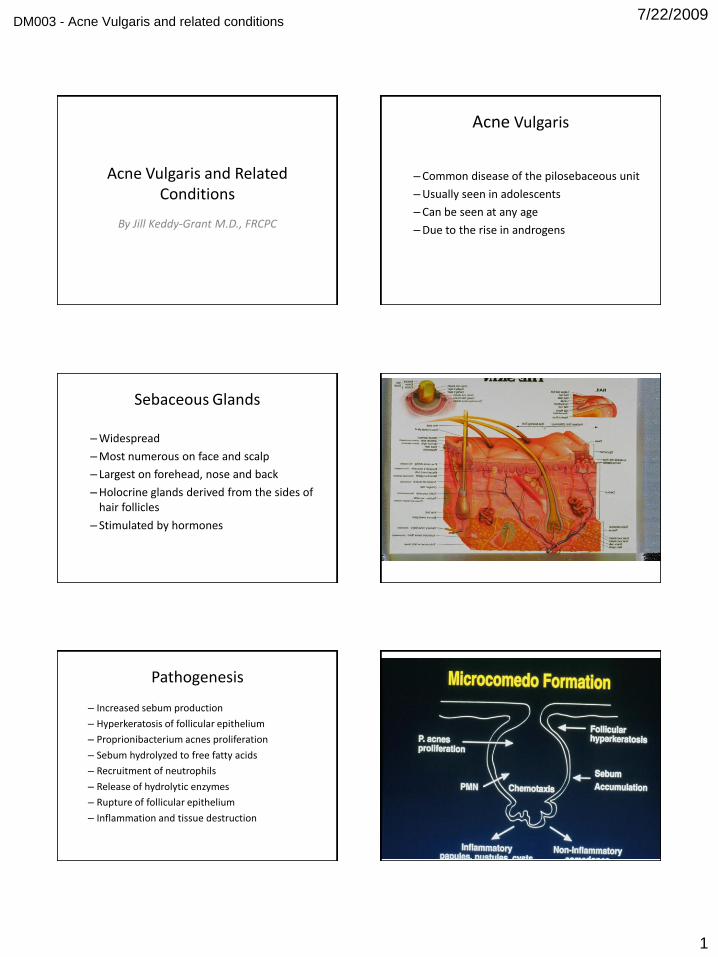
Sebaceous Glands
–Widespread
–Most numerous on face and scalp
– Largest on forehead, nose and back
–Holocrine glands derived from the sides of hair follicles
– Stimulated by hormones
Pathogenesis
– Increased sebum production
– Hyperkeratosis of follicular epithelium
– Proprionibacterium acnes proliferation
– Sebum hydrolyzed to free fatty acids
– Recruitment of neutrophils
– Release of hydrolytic enzymes
– Rupture of follicular epithelium
– Inflammation and tissue destruction
DM003 - Acne Vulgaris and related conditions

7/22/2009
2
Exacerbating Factors
• Cosmetics
• Increased androgens
• Friction
• Stress
• Drugs
• Oils
Clinical Lesions - Closed Comedone
• Skin colored papule
• Non-inflammatory
• 1-2 mm
Clinical Lesions - Open Comedone
• Papule with central black core
• Non-inflammatory
• 1-2 mm
Clinical Lesions -Inflammatory Papules
• Red
• Follicular
• Papules
• Small or large

7/22/2009
3
Clinical Lesions - Pustules
• Follicular
• Papules
• Red with white center
Clinical Lesions - Inflammatory Nodules
• Deeper lesions
• Red
• 5 mm
Clinical Lesions - Acne Cysts
• Inflammatory nodules
• Central fluctuation

7/22/2009
4
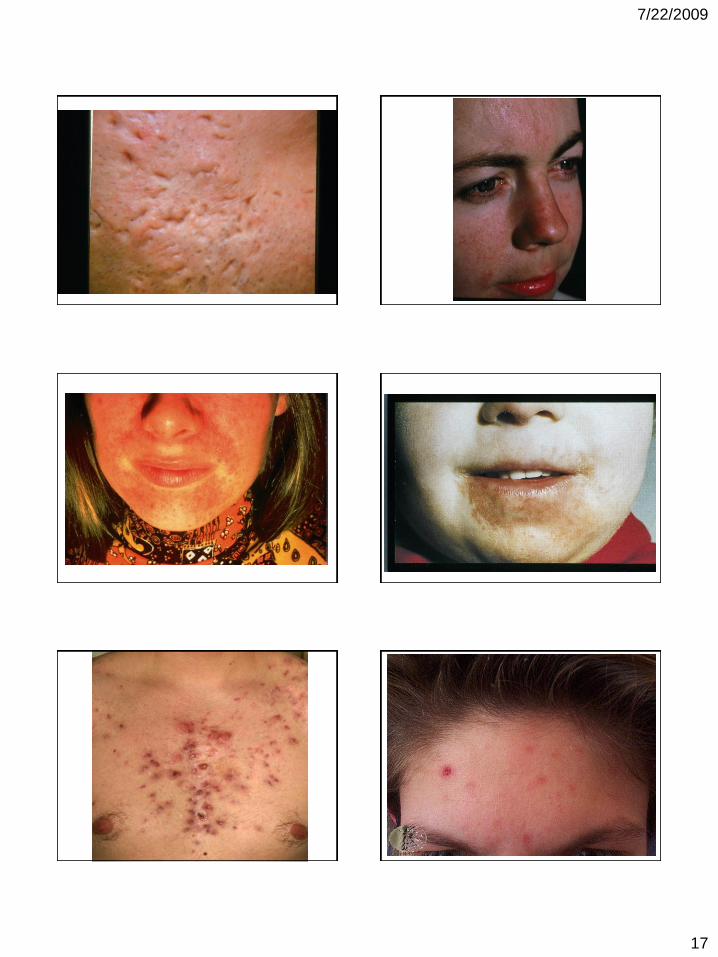
Clinical Lesions - After Acne Heals
• Postinflammatory hyperemia
• Postinflamatory hyperpigmentation
• Scars

7/22/2009
5
Clinical Assessment: History
• Duration
• Severity
• Past treatment
• Cleansing / makeup routine
• Menstrual history
• Past medical history
• Drugs
• Exacerbating factors
Clinical Assessment: Physical
• Lesions– Non inflammatory (closed and open comedones)
– Inflammatory (papules, pustules, cysts)
• Location and extent
• Complications– Excoriations
– Atrophic or hypertrophic scars
– Hyper or hypopigmentation
Clinical Assessment: Tests
• Culture – when gram neg. folliculitis suspected
• Hormone assay (free testosterone, DHEAS, LH, FSH)– Androgen excess
– Prepubertal acne
– Isotretinoin resistant acne
• Skin biopsy– Rarely done to exclude other diseases

7/22/2009
6
Treatment - Comedones
• Topical retinoids
• Salicylic acid
• Sulphur
• Alpha hydroxy acids
• Manual extraction
• Chemical peels
• Oral contraceptives
• Isotretinoin
Topical Retinoids
• Most effective comedolytic agent
• Normalizes follicular hyperkeratosis
• Maximum response in 3-6 months
• Adapalene, tretinoin, tazarotene
• Creams, gels, solutions
• Irritating
Other Comedolytic Agents
• Salicylic acid
– peeling agent
• Sulphur
– peeling agent
– dries papules and pustules
• Alpha hydroxy acids
– glycolic acid, lactic acid
– mild peeling agent
Treatment – Small Inflammatory Papules and Pustules
• Benzoyl peroxide
–2.5, 5 and 10%
• Topical antibiotics

7/22/2009
7
Benzoyl Peroxide
• Inhibits P. acnes proliferation
• Dries acne papules
• Irritating
• Allergenic
• Maximum response 8-12 weeks
Topical Antibiotics
• Clindamycin, erythromycin, sulpha, neomycin
• Inhibits P. acnes proliferation
• Usually well tolerated
• May develop bacterial resistance
• Maximum response 6 weeks
Combined Benzoyl Peroxide and Topical Antibiotics
• 1% Clindamycin or 1% Erythromycin
• 5% Benzoyl peroxide
• Prevents bacterial resistance
Treatment – Large Inflammatory Papules, Pustules, Nodules and Cysts
• Oral antibiotics
• Hormonal therapy
• Oral retinoids
• Blue light laser
• Intralesional steroids
• Cryotherapy
Oral Antibiotics
• Suppress P. acnes and bacterial lipases
• Inhibit neutrophil chemotaxis
• Maximum response in 6-12 weeks
• Standard course – 6 months

7/22/2009
8
Oral Antibiotics - Adverse Effects:General
• Bacterial resistance
• Gram negative folliculitis
• Candidiasis
• Pseudomembranous colitis
Oral Antibiotics – Adverse Effects: Specific
• Tetracycline:• phototoxicity, teeth discoloration, GI upset
• Minocycline:• pigmentation, teeth discoloration, vertigo,
hypersensitivity sydrome
• Erythromycin:• GI upset
• Cotrimoxazole / trimethoprim:• rashes, bone marrow suppression
Oral Antibiotics - Dosage
• Tetracycline 500 mg BID
• Minocycline 100 mg BID
• Erythromycin 500 mg BID
• Septra DS 1 tab BID
Hormone Therapy
• Oral contraceptives– Tricyclen, Cyclen and Marvelon
– response takes 3 months
• Antiandrogens– Spironolactone – only for women
– cyproterone acetate (Diane 35)
– Response takes 6-12 months
Diane 35
• 35 ug of ethinyl estradiol
• 2 mg of cyproterone acetate
• Is a contraceptive but not marketed in Canada for this indication
• Indicated for women with acne
• Indicated for women with symptoms of hyperandrogenization
• Safety profile similar to other OC’s
Diane 35
• Reduces sebum production
–estrogen exerts a negative feedback on production of androgens
– cyproterone acetate has an antiandrogen effect on the sebaceous glands

7/22/2009
9
Oral Retinoids - Isotretinoin
• Decreases sebum production
• Normalizes follicular hyperkeratinization
• Decreases P. acnes
• Anti inflammatory and anti chemotactic effects
Isotretinoin - Benefits
• Most effective agent for treatment of acne
• Long term remissions or cures in the majority of patients
• Side effects are generally temporary and disappear when treatment is stopped
• Most patients improve after 1 or 2 courses
Isotretinoin - Indications
• Scarring acne
• Nodulocystic acne
• Acne unresponsive to conventional therapy
• Adult onset acne (>20 years)
• Persistent acne
• Severe psychological effects of acne
Isotretinoin – Side Effects
• Teratogenicity
• Mucocutaneous drying - 100%
• Arthralgias, myalgias – transient
• Headache – 10%, usually mild
• Eyes – decreased night vision, dry eyes (rarely persistent)
• Mood changes

7/22/2009
10
Isotretinoin – Side Effects
• Temporary elevation of triglycerides and cholesterol - 10 – 20%
– stop or reduce drug if TG > 800 mg/dl
• Transient mild elevation of liver enzymes –10%
Isotretinoin - Contraindications
• Absolute
– pregnancy (pregnancy prevention program)
• Relative
– history of depression
– hypertriglyceridemia / cholesterolemia
– pre – existing liver disease
Isotretinoin – Things to Avoid
• Tetracyclines
• Vitamin A supplements
• Alcohol
• Sun exposure
Isotretinoin - Dosage
• 0.5 mg/kg for the first 2 – 4 weeks
• 1 mg/kg for the next 4 – 5 months
• Total cumulative dose of 120 – 150 mg/kg
Isotretinoin - Monitoring
• Monthly follow up
• Baseline and monthly bloodwork
– pregnancy test
– liver function tests
– complete blood count
– cholesterol and triglyceride levels
7/22/2009
11
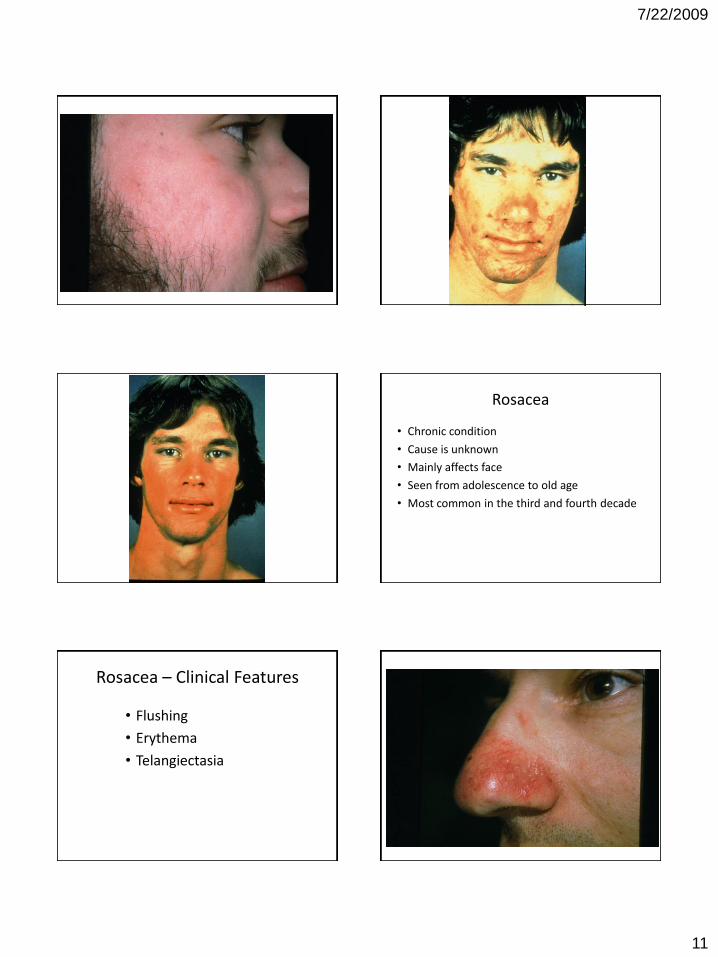
Rosacea
• Chronic condition
• Cause is unknown
• Mainly affects face
• Seen from adolescence to old age
• Most common in the third and fourth decade
Rosacea – Clinical Features
• Flushing
• Erythema
• Telangiectasia
7/22/2009
12
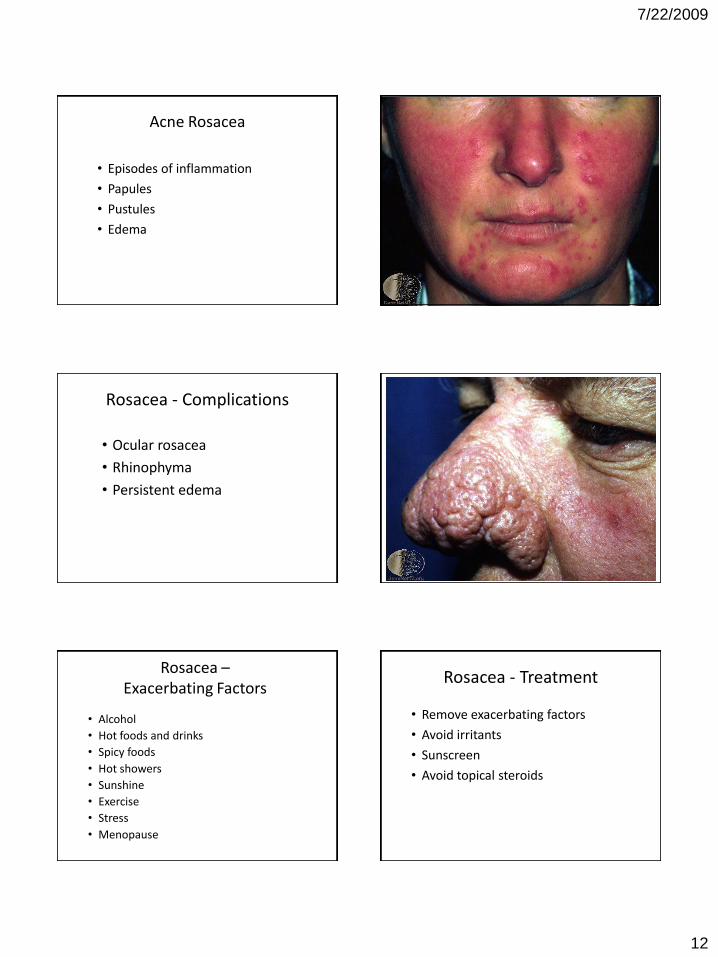
Acne Rosacea
• Episodes of inflammation
• Papules
• Pustules
• Edema
Rosacea - Complications
• Ocular rosacea
• Rhinophyma
• Persistent edema
Rosacea –Exacerbating Factors
• Alcohol
• Hot foods and drinks
• Spicy foods
• Hot showers
• Sunshine
• Exercise
• Stress
• Menopause
Rosacea - Treatment
• Remove exacerbating factors
• Avoid irritants
• Sunscreen
• Avoid topical steroids

7/22/2009
13
Mild Acne Rosacea - Treatment
• Topical metronidazole
• Topical antibiotics – erythromycin, clindamycin, sulpha, neomycin
• Topical sulfur
Severe Acne Rosacea - Treatment
• Tetracyclines
• Erythromycin
• Metronidazole
• Sulpha
• Isotretinoin
Erythema of Rosacea -Treatment
• Camouflage
• Topical metronidazole
• Oral antibiotics
• Laser
7/22/2009
14
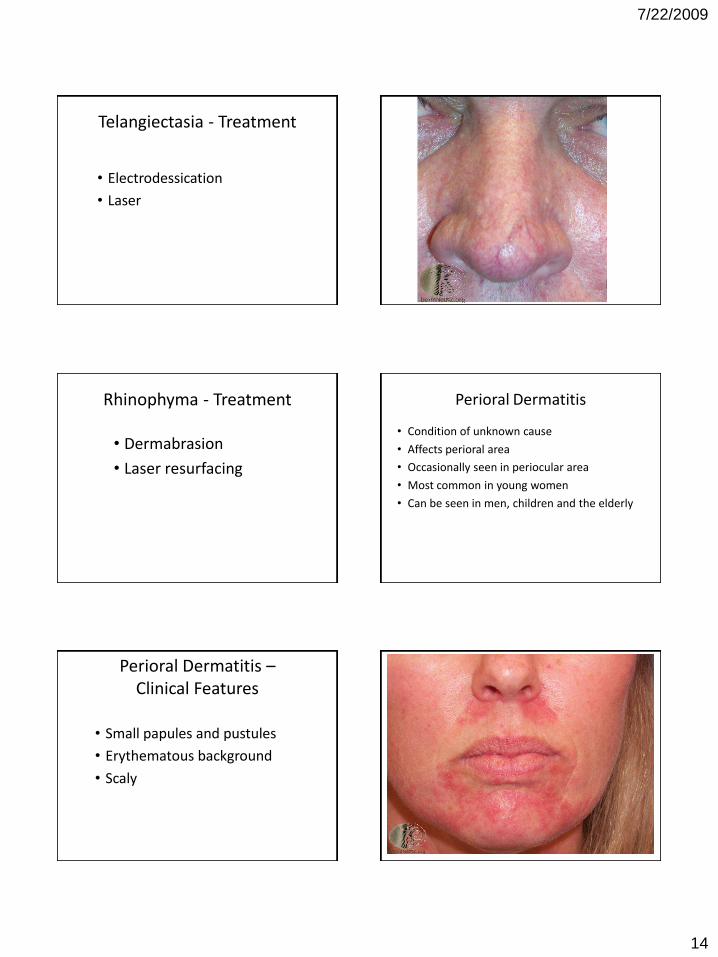
Telangiectasia - Treatment
• Electrodessication
• Laser
Rhinophyma - Treatment
• Dermabrasion
• Laser resurfacing
Perioral Dermatitis
• Condition of unknown cause
• Affects perioral area
• Occasionally seen in periocular area
• Most common in young women
• Can be seen in men, children and the elderly
Perioral Dermatitis –Clinical Features
• Small papules and pustules
• Erythematous background
• Scaly

7/22/2009
15
Perioral Dermatitis –Contributing Factors
• Fluorinated steroids
• Cosmetics – creamy cleansers and moisturizers
• Fluorinated toothpastes
• Hormones
• Stress
Perioral Dermatitis - Treatment
• Remove contributing factors
• Antibiotics for six weeks
– tetracycline
– minocycline
– erythromycin

7/22/2009
16
7/22/2009
17

7/22/2009
18

7/22/2009
1
Dermatologic Presentations of
Infectious Disease
Shane Silver MD FRCPC
Overview
Bacterial infections
Viral infections
Fungal infections
Infestations
BACTERIAL Impetigo
Staph or Strep
Group II phage Staph – strains 77 and 55
Exfoliative toxin A and B
ECTHYMA
• Neglected impetigo
• Diabetics, homeless
• Crusted erosions with erythema
• Treat as for Staph or strep
DM007 - Dermatologic Presentations of infectious disease

7/22/2009
2
Furuncle and Carbuncle
Furuncle is one abscess and a carbuncle is
many furuncles together
These are follicular based
Paronychia
Staphylococcal scalded skin
syndrome Toxin mediated – exfoliative toxin
Children less than 5 and renal failure patients
Constitutional symptoms, erythema in folded regions, desquamation, bullae and positive Nikolsky sign
Mortality 3% for children and 50% adults
Culture from bullae are negative
Treat with antistaphylococcal Abx and supportive therapy

7/22/2009
3
Staphylococcal infections
Impetigo
Ecthyma
Carbuncle/furuncle
Paronychia
Staphlococcal scalded skin syndrome
Folliculitis / sycocis barbae or lupoides
Staphylococcal infections
Felon
Botryomycosis
Staphylococcal toxic shock syndrome
RED syndrome
Recurrent toxin – mediated perineal
erythema
Streptococcal
Ecthyma
Impetigo
Blistering
Distal
Dactylitis
Scarlet fever
2-10yrs old
Exotoxins B and C
Inc 2-4 days
Pharyngitis and fever, constitutional sx
Enanthen: phaynx red, edema of tonsils, white then red strawberry tongue
Exanthem: H+N, circumoral sparing, sandpaper feel, pastias lines, desquamation when rash begins to fade, exanthem 4-5 days

7/22/2009
4
Associated with Streptococcus
Streptococcal Infections
Impetigo
Ecthyma
Blistering dactylitis
Erysipelas/cellulitis
Scarlet fever
Erythema nodosum
Guttate psoriasis
Vasculitis
Sweets syndrome (acute neutrophilic dermatosis)
endocarditis
Streptococcal Infections
Streptococcal intertrigo
Streptococcal toxic shock syndrome
Perianal streptococcal cellulitis
Necrotizing faciitis
Erythema multiforme

7/22/2009
5
Bacterial infections
Viral infections
Fungal infections
Infestations
Overview
Hand foot and Mouth
Cocksackie A 16 and enterovirus 71
Constitutional symptoms, including
abdominal, sore throat
Extensor surfaces most involved
Rarely encephalitis especially with
enterovirus strain
Erythema infectiosum
30-60% of adults are seropositive
If elderly 90%
Inc 4-14 days
No longer infectious by the time they
manifest symptoms
Aplastic crisis, arthritis, hydrops, chronic
anemia in immunocompromises (lysis)

7/22/2009
6
Herpes viruses

7/22/2009
7
TZANCK SMEAR
Herpes Simplex Virus
HSV1- oral “cold sores”, 10-20% of genital HSV
HSV-2 – Genitals (prevalence is 25%)
Incubation period is 3 – 7 days
Prodrome of lymphadenopathy and Constitutional symptoms, pain tenderness and burning at the site
Grouped vesicles on erythematous base > pustules > crusts
Diagnosis – culture, DFA, Tzanck smear, PCR, serology, western blot
Varicella

7/22/2009
8
Varicella
Chicken pox and shingles (zoster)
90% of children prior to age 10
Zoster is reactivation of varicella after
primary chicken pox
Zoster in 20% of adults and 50% of
immunocompromised
Varicella
Transmission
– Airborne droplets (primary varicella or diss
zoster, not with classic zoster)
– Direct contact of vesicular fluid (primary
varicella or any form of zoster)
Incubation period - 11-20 days
Varicella
Prodrome of fever, malaise, myalgia
Pruritic macules > papules > vesicles >
pustules > crusts
Dew drops on a rose petal
Lesions in all stages of development
Zoster has similar presentation but is
dermatomal
Varicella
Complication
– Bacterial infection, CNS complication, Reyes
syndrome, Pneumonia, keratitis, hepatitis
– Zoster – Ramsay – Hunt syndrome, bacterial
infx, scarring, keratitis, motor neuropathy,
postherpetic neuralgia(incidence inc with age)

7/22/2009
9
Varicella
Prevention
– Varicella zoster immunoglobulin within 96 hrs
of exposure
– Viravax- 96% conversion rate
Molluscum Contagiosum
Molluscum contagiosum
Treatment
– Most resolve on their own
– Liquid nitrogen, cantherone
curettage, aldara, tretinoin, silver nitrate sticks, tape
stripping
Warts
Verrucae vulgaris – common wart , hands
Verrucae plantaris – plantars wart, feet
Verrucae planus – flat wart, dorsal hands
and face
Condyloma acuminata – genital warts,
genitals and perianal

7/22/2009
10
Verrucae vulgaris Verrucae plantaris
Verrucae planus Condyloma acuminata
Treatment - Warts
Cryotherapy
Salicylic acid (over the counter preps)
Glutaraldehyde
Cantherone
Imiquimod
Bleomycin
Podophyllin
Excision
Laser
DPCP

7/22/2009
11
Overview
Bacterial infections
Viral infections
Fungal infections
Infestations
Median rhomboid glossitis
Erosio interdigitalis
blastomycetica Dermatophytes
Onychomycosis
Onychomycosis – dermatophyte, mold or
yeast
Tinea unguium- dermatophyte
Risk factors – older age, male,
immunosuppressed, DM, PVD, trauma,
concomitant nail disease

7/22/2009
12
Onychomycosis
Distal lateral subungual onychomycosis (DLSO)
– T. rubrum, T. mentagrophytes
White superficial onychomycosis (WSO)
– T. mentagrophytes
– Nail plate is with leukonychia
Proximal subungual onychomycosis
– T. rubrum
– Check for HIV
Onychomycosis
Other rare organisms:
– Scopulariopsis, Alternaria, Aspergillus,
Fusarium, Scytalidium, others
Diagnosis
– CULTURE
– Direct microscopy
Onychomycosis Treatment
Establish a diagnosis
Systemic agents
– Terbinafine – 12 wks for toenails, 6 wks for finger nail
(250mg od)
– Itraconazole – 200mg bid 1 week per month for 2
months for fingernails and 3 months for toenails
– Fluconazole – 150 mg per week until nail is clear
– Ciclopirox nail lacquer
Onychomycosis Treatment
Nail is NOT expected to be clear after finishing
the 3 month coarse
Side effects
– Terbinafine –Nausea, GI upset, Taste disturbance,
hepatic toxicity, leukopenia, rash, Drug interactions
CBC, AST, ALT monthly
– Itraconazole – Nausea, GI upset, Rash, Pruritus,
Hepatic toxicity, Drug interactions
Liver test monitoring controversial
Dermatophytes
Caused by 3 genera of species
– Trichophyton
– Microsporum
– Epidermophyton
These fungi attack keratinized tissue
Depending on location is the name given to the
condition
– Tinea pedis, Tinea capitis, Tinea corporis, Tinea
manuum, Tinea cruris, tinea faciei

7/22/2009
13
Dermatophytes
Clinical – annular papulosquamous lesion
with peripheral scale and central clearing
Diagnosis – KOH, Culture
Treatment – topical or systemic antifungals

7/22/2009
14
Tinea Capitis
Ectothrix vs Endothrix
M. canis most common world wide
T. Tonsurans most common in N. America
Inflammatory via Zoophilic organisms
Tinea Capitis
Clinical
– Non- inflammatory- Seborrheic dermatitis like
– Black dot
– Kerion
– Favus
Treatment
– Griseofulvin 20mg/kg x 8 weeks
– Terbinafine 3-6mg/kg/d for 2-4 weeks
– Itraconazole 3-5mg/kg/d for 4-6 weeks
– Fluconazole 6mg/kg/d x 20 days

7/22/2009
15
Overview
Bacterial infections
Viral infections
Fungal infections
Infestations
Scabies
Sarcoptes scabiei var. hominis
Incubation 2-6 weeks
Pruritus more severe at night
Distribution – hands, web spaces, wrists,
axillae, umbilicus, sparing face in adults
Papules with excoriations, characteristic
burrows, scrotal nodules
Scabies
Clothing needs to be washed and stored
All individuals in the house to be treated
whether they are pruritic or not (prevent
ping-ponging between pts)

7/22/2009
16

7/22/2009
1
Dermatitis
Marni C. Wiseman MD FRCPC
Assistant Professor, University of Manitoba
Director, Cutaneous Oncology,
CancerCare Manitoba
What is a dermatitis?
• Difficult to define:
- inflammation involving epidermis and
superficial dermis
- assoc pruritus
- ill-defined and erythematous
- range from:
- acute- vesicles/bullae, oozing
- subacute- crusts
- chronic- lichenification
Types of Dermatitis
• Atopic dermatitis
• Contact dermatitis
• Dyshidrotic eczema
• Nummular dermatitis
• Asteatotic dermatitis
• Lichen simplex chronicus
• Stasis dermatitis
Atopic Dermatitis
Pathophysiology
• Decreased barrier function
–Decreased epidermal lipids
(ceramide)
–Increased transepidermal water
loss
THERAPEUTIC STRATEGIES FOR THE MANAGEMENT OF ATOPIC DERMATITIS (AD):
A Case-Based CHE Program
Barrier function
breakdown in skin
with AD
• Keratinocytes become less tightly held together
• Vulnerable to external factors such as chemical solvents and water, which dissolve the natural protective barrier of the skin
Atopic
Dermatitis
DM008 - Dermatitis

7/22/2009
2
Epidemiology
• 10-20% of children, 17% of
Canadian
• 85% occur before the age of 5
• 30% persist into adulthood
• 50% in children with
asthma/allergic rhinitis
Physical Examination
Distribution
• Infants • face and scalp
• Crawling infant • Extensor surfaces of extremities, trunk, face, and
neck
• Older child• Wrists, ankles, antecubital fossae, popliteal
fossae, and neck
• Adult• May be limited to hands and feet
THERAPEUTIC STRATEGIES FOR THE MANAGEMENT OF ATOPIC DERMATITIS (AD):
A Case-Based CHE Program
Typical presentation in infants, children, adolescents, and adults
Illustration by Carlos Machado, M.D.

7/22/2009
3
Weeping, Oozing, and Fissuring

7/22/2009
4
Hand Dermatitis
Reprinted from J Am Acad Dermatol 2001;44(Suppl1) with permission from Mosby, Inc.
Erythema and Excoriation
Dennie-Morgan Folds
Keratosis Pilaris Hyperlinear Palms

7/22/2009
5
Pityriasis Alba in AD Xerosis
Atopic Dermatitis: Management
• General measures
• Moisturize and hydrate
• Antihistamines prn
• Antibiotics prn
• Anti-inflammatory therapy
• Support for parent
Fitzpatrick’s Dermatology in General Medicine, 1999
Treatment – General Measures
• Avoid irritants
• Loose fitting cotton clothing; avoid wool
• Daily Bath, 10 min.
• Gentle cleansers
• Petroleum jelly around mouth when eating irritating foods (tomatoes, oranges)
Moisturization
• VERY IMPORTANT!
• Aggressive and frequent
• The greasier the better
• 2 minute rule- daily bath- pat dry-apply emmolient within 10 minutes
Fitzpatrick’s Dermatology in General Medicine, 1999
Antihistamines
• Sedating antihistamines at night
• Do not restrain hands of children

7/22/2009
6
Antibiotics
• Systemic or topical- not routine
• Antibiotics should cover staph and strep
• Watch for HSV
• Routine swabs useless
• Topical corticosteroids (“steroids”)
• Topical immunomodulators (TIMS)
– Pimecrolimus (Elidel)
– Tacrolimus (Protopic)
• Systemic
– Methotrexate
– Prednisone
– Azathioprine, MMF
– Light (U VB, narrow band UVB, UVA1, PUVA)
– Cyclosporin
Anti-inflammatories
Treatment –Corticosteroids
• Topical steroids
–Ointment preferred
–Hydrocortisone 1% to face bid/tid
–Betamethasone Valerate .1 % to
body bid/tid
–Increase strength if needed
• Skin Atrophy
• Striae
• Acne
• Tachyphylaxis
• Allergy
• Eyes – Increased Intraocular Pressure
• Systemic Effects
Corticosteroids –
Common Side Effects
Corticosteroids Can Cause
Skin Atrophy & Striae

7/22/2009
7
Impetiginized Eczema
Eczema Herpeticum (HSV)Contact Dermatitis
Two types:
1. Allergic Contact Dermatitis
- Delayed Type Hypersensitivity (type IV)
- common causes- plants, nickel….
2. Irritant Contact Dermatitis
- direct damage to tissue
- causes- strong detergents, chemicals

7/22/2009
8
Contact Dermatitis
• The clue to contact dermatitis is the
distribution!!
• Treatment:
- avoid contact
- compresses
- moderate potent topical steroids (BMV)
- severe- two week course of prednisone
Dyshidrotic Eczema
(pompholyx)
• Pruritic pinpoint vesicles on sides of
fingers, toes, palms, soles
• Idiopathic
• Treatment- topical steroid ointment

7/22/2009
9
Nummular Eczema
• Pruritic ill-defines coin-like plaques
• Trunk and extremities
• Exacerbated in winter
• Treat as atopic dermatitis
Asteatotic Dermatitis
(Eczema craquele)
• Fine fissures with erythema
• Lower extremities- most common site
• Common in elderly
• Exacerbated in winter
• Treatment - ointments- vasaline
- steroid ointments

7/22/2009
10
Lichen Simplex Chronicus
• Chronic dermatitis due to repetitive rubbing
• Lichenified, hyperpigmented, ill-defined
• Ankle – most common site
• Difficult to treat
- superpotent topical steroid +/-occlusion (dermavate)
- educate patient
Stasis Dermatitis
• Dermatitis associated with venous disease and
stasis
• Lower extremity
• Assoc: venous ulcers, hyperpigmentation,
varicosities, pedal edema, lipodermatosclerosis
• Treatment - treat venous disease
- mild steroid ointments
(hydrocortisone)

7/22/2009
11
THE END
QUESTIONS????







![Non-dermatophyte onychomycosis · 2016. 1. 14. · gens of already diseased nails. The prevalence of non-dermatophyte molds as nail invaders ranges between 1.45% and 17.60% [3], The](https://static.documents.pub/doc/80x56/60d6204a3fc9a30f0a11bfaa/non-dermatophyte-onychomycosis-2016-1-14-gens-of-already-diseased-nails-the.jpg)