

Disease State Primer: Rheumatoid Arthritis
Q1 2012: Pre-EULAR

2
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on rheumatoid arthritis?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is rheumatoid arthritis?
• Presentation, diagnosis, classification
• Epidemiology by geography and patient segment
• Current care paradigm and clinical evidence
• Emerging care paradigm
10 • 11 - 12
• 13 - 14
• 15
• 16 – 27
• 28
III. Clinical Development Pipeline • Disease mechanism overview
• Clinical development pipeline mapping
• JAK Inhibitors
• Syk Inhibitors
• c-Kit Inhibitors
• Anti-Baff antibodies
• Other mechanisms
29 • 30 - 32
• 33 – 38
• 39 – 45
• 46 - 48
• 49 - 50
• 51 - 52
• 53 – 71
IV. Commercial Landscape • Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
72 • 73 – 78
• 79
• 80 – 81
• 82 – 90
V. Appendix • Table of Acronyms
• More about Lumleian
91 • 92 – 93
• 94 – 96

3
Lumleian offers the requisite scale and depth of life science expertise required for our client’s
most critical investment decisions; We offer universal information and real time knowledge.
• Data Mining
- Regulatory filings
- Scientific literature
- Patent filings
- Company filings
and press releases
• Secondary Data
- Industry pipelines
- Wall Street analysis
- US TRx, pricing,
promotional spend
• Primary Research
- Key opinion leaders
- Practicing physicians
- Reimbursement
Expertise Based
Teams
• Experience
- Academic faculty
- Bio-pharmaceutical
- Equity research
- Strategy consulting
• Expertise
- 30+ clinicians
and Ph.D. scientists
• Analytics
- 5 Ph.D. economists
and statisticians
Universal
Information
Real-Time
Knowledge
• Disease State Primers
- Disease overview
and care paradigm
- Clinical development pipeline
- Commercial landscape
• Functional Drill Downs
- In licensing assessments
- Early and late stage
- Preliminary due dilligence
- Real-time clinical data
• Proprietary Analytics
- Asset valuation
- Epidemiologic forecasts
- Industry benchmarks
• Drug Development
and commercial
- Patient segment valuations
- Promotional response models
• Healthcare professional
and direct to consumer
• Academic and
Research Institutions
- Portfolio optimization
• Early stage
- Out licensing strategy
• Asset valuation
• Transaction support
• Royalty monetization
• Bio-pharmaceutical Companies
- Asset valuation
- Clinical strategy
- In licensing strategy
• Early and late stage
- Portfolio optimization
• Early and late stage
- Preliminary due dilligence
• Life Science Investors
- Asset valuation
- Clinical strategy
- In licensing strategy
Life Science
Client Base
Decision
Support

4
Notes: 1These are a representative sub-set of the publicly available data sources
To ensure real-time knowledge, across disease states, our team of 30+ clinicians and Ph.D.
scientists maintain a comprehensive knowledge management platform, leveraging novel data
mining technology and proprietary analytics.
Data Mining
and Analytics
• Company presentations
• Earnings announcements
• Equity research coverage
• Investor relations transcripts
• Clinical trials
• Conference presentations
• Gene ontology
• Industry pipeline databases
• NIH grants
• Scientific literature & citations
• Business development transactions
• Venture capital investments
• Disease profiles
• Industry publications
• Sales and Rx data
• Treatment algorithms
• Advisory committee transcripts
• FDA and EMA filings
Scientific
& Clinical:
Financial:
Academic
Tech Transfer:
Competitive
Landscape:
• Early stage technologies
• Intellectual property filings
Business
Development:
Regulatory:
• Leverage data mining
technology to access
novel data sources
• Standardize, collate,
and link data sources
• Execute Lumleian’s
proprietary analytical
models
Universe of Public
Information1
• 30+ clinicians and
Ph.D. scientists
- Focused by area
of expertise
• 5 Ph.D. economists
and statisticians
Expert Validation
and Decision Support

5
Our efficient platform and our expertise based teams enable us to both deliver the highest
quality product and tailor our offer, to specific client needs: either custom decision support or
more standardized research and analytics, e.g. disease state primers.
Decision
Support
• Clinical strategy
• Portfolio optimization
- Pre-Clinical
- Clinical
• Transaction support
- In licensing
- Out licensing Disease
State Primers
Proprietary
Analytics
• Asset valuation
• Epidemiologic forecasts
• Industry benchmarks
- Commercial
- Clinical Development
• Patient segment
valuations
• Promotional
response models
- Healthcare professional
- Direct to consumer
• Royalty monetization
Functional
Drill Downs
• Real-time clinical
data
- Trial strategies
- Results
• In licensing
assessments
- Pre-clinical
- Clinical
• Preliminary
due dilligence
- Scientific
- Clinical
- Commercial
• Disease overview
and care paradigm
• Clinical development
pipeline
• Commercial
landscape Customized
Standardized

6
What information is included in a disease state primer?
• Lumleian’s objective and fact based perspective on the relative attractiveness of investing in a given disease state
• Disease overview and care paradigm - Etiology, Diagnosis and patient segmentation, Global epidemiology, Treatment algorithm, Clinical evidence, Emerging care paradigm
• Clinical Development Pipeline - Validated industry pipeline for all assets in clinical development, Select mechanism of action profiles, trial designs and evidence
• Commercial landscape - Global, US, EU, Japan market and brand revenue, Pipeline forecasts, US growth decomposition, Promotional spend and messaging
What disease states are planned for 2012? • Autoimmune: Inflammatory Bowel Disease, Lupus, Multiple Sclerosis, Psoriasis, Rheumatoid Arthritis
• Cardiovascular: Hyperlipidemia
• Central Nervous System: Alzheimer’s Disease, Depression, Pain, Schizophrenia
• Endocrine: Type II Diabetes, Obesity
• Infectious Disease: Gram Negative Bacteria, Hepatitis C Virus
• Oncology: Breast, Colorectal, Leukemia(s), Lung, Lymphoma(s), Melanoma, Ovarian, Pancreatic, Prostate
• Pulmonary: Chronic Obstructive Pulmonary Disease, Idiopathic Pulmonary Fibrosis
Can we create custom disease state primers for customers? • Yes, based on the expertise of our team of 30+ clinicians and Ph.D. scientists, 5 Ph.D. economists and statisticians we can create a
sustome primer in appoximately 3 to 4 weeks
• We can supplement the primers with deeper analysis to help customers reach a deeper understanding of critical issues e.g. KOL
interviews, Financial Models, Survey Conduction and Analysis, Pre-Clinical Asset Assessment
• We are also developing deep drills by function, e.g. Discovery, Clinical development, Business development, Commercial
Why did we create our disease state primers? • We were frustrated by having to repeatedly validate, standardize, and collate pipeline and commercial data
• Portfolio optimization requires a standard framework to compare “apples to apples” investment decisions across disease states
• Our primers began as a training tool; We require every decision scientist create one from scratch before supporting clients
What is a Lumleian’s disease state primer?

7
Executive Summary: Rheumatoid Arthritis
• The global
Disease
Overview and
Care Paradigm
• Rheumatoid arthritis is a chronic, debilitating, systemic inflammatory condition, with multiple serious comorbidities
including cardiovascular disease, increased risk of infections, malignancies, and osteoporosis ‐ Rheumatoid arthritis is a heterogeneous disease in which response to treatment varies dramatically by patient
• Remission rates remain sub-optimal despite aggressive therapy early in disease progression: ‐ DMARDs, non-biologic first then biologics, are the backbone for therapy with novel biologics reserved for later treatment lines
‐ Methotrexate is the most common non-biologic DMARD in 1st line mono-therapy and the base for most combination therapies
‐ Anti-TNFα’s are the cornerstone biologics used in 2nd line, as mono-therapy or commonly in combination with methotrexate
• After inadequate response, 3-6 months per recent 2012 ACR guidelines, switching to a successive anti-TNFα’s is standard
• 50% of patients stop responding to a particular DMARD after five years creating substantial unmet need later in treatment
‐ Novel biologics are used 3rd line: Orencia (T Cell Costimulation Inhibitor), Actemra (IL-6 Inhibitor), and Rituxan (B Cell Inhibitor)
Clinical
Development
Pipeline
• Substantial primary need exists for agents which offer an alternative for patients who do not respond to anti-TNFα therapy
‐ ACR50 response is achieved in ~2/3 of patients, leaving ~1/3 of patients without an effective long-term treatment strategy ‐ Secondary unmet needs include providing: (1) Additional benefits such as prevention of bone erosion or cardio-protection,
and (2) An oral formulation as an alternative to sub-cutaneous and intravenous agents
• As of May 2012, Lumleian validated 82 assets in clinical development, nearly all of which focus on chronic symptom
management and cessation of structural damage
• The late stage pipeline is crowded with multiple mechanisms, including: Cytokine inhibition (TNF, IL-6), Kinase inhibition
(JAK, Syk, P38 MAPK, c-Kit CD117), B Cell inhibition (BAFF, CD-20), and T Cell inhibition (CD4, CD23) ‐ FDA precedent suggests novel mechanisms will initially be approved in later lines of treatment where they will compete for
class and asset differentiation in the eyes of payors and physicians
• Most pipeline activity is focused on the development of kinase inhibitors: ‐ Excitement exists for Pfizer’s Tofacitinib, the first oral treatment with anti-TNFα like efficacy
‐ In May 2011 an FDA advisory committee voted 8-2 in favor of approval and its PDUFA decision is set for August 2012
‐ Tofacitinib approval will most likely be in 3rd line without an inhibition of structural damage claim and with dose titration
‐ Other kinase targets have not fared so well and in particular the relative lack of efficacy of p38 MAPK was surprising
• Oral Syk Inhibitors are promising; In addition to offering impressive inflammation control, they also slow bone resorption
Commercial
Landscape
• Global ’11 brand revenue for RA was ~$14.7B and is forecast to grow by ~4.5% to ~$18.3B between ’12 and ’15 ‐ Modest growth in pipeline biologics is expected short term supported by recent ACR guidelines reinforcing anti-TNFα’s
‐ Other approved biologic classes will gain 2nd line share based on sub-cutaneous formulations and Humira head-to-head trials
‐ Novel drug classes will likely be restricted to 3rd line by regulators and will all have to compete for differentiation • Precedent exist based on Actemra’s approval in January 2010 and concerns raised at Tofacitinib’s advisory committee in May 2012
‐ Payor pressure will be acute, as evidence by recent NICE guidelines for Orencia, and bio-similars will stunt growth in Europe • An EMA decision on bio-similar Remicade is expected in ~12 months with Enbrel and Humira in clinical development
• Promotion costs are substantial and may be a deterrent for less differentiated agents - In December 2011 US marketing/sales monthly costs exceeded $40M: $17.5 on Healthcare professional s and $32.6M in DTC
- Perhaps indicative of this challenge, Simponi and Cimzia the 4th and 5th anti-TNFα’s to market have reduced promotional spend
consistently throughout 2011; Actemra, which has a label restricted to 3rd line patients, is also reducing promotional spend

8
What are the key questions for 2012?
Key
Questions
• Commercial Opportunity - What will be the impact of Pfizer terminating its co-promote arrangement for Humira in 2012?
- What will be the impact of the JAK Inhibitors, and other orals on the treatment paradigm, given Tofacitinib,
the first JAK inhibitor is likely to be approved in August ’12 in 3rd line without a structural inhibition claim? • In which line of treatment is Tofacitinib likely to be indicated at launch, given safety concerns and FDA precedent
for initially approving novel mechanisms in later lines of treatment and then staggering approvals to earlier lines?
• What will be the impact of a likely label without an inhibition of progression of structural damage claim?
• How will payors perceive Tofacitinib based on its launch label, will they perceive it to be a driver of treatment cost
or perceive it as having potential to reduce treatment cost, by reducing anti-TNFα cycling?
• What will be the rate of uptake of orals in the market by rheumatologists and potentially primary care?
- What will be the impact of anti-TNFα therapy head-to-head studies by incumbent biologics, e.g. AMPLE and ADACTA?
- Will late stage biologics provide sufficient clinical advantage over incumbents to merit moving up in the treatment
paradigm? How long will it take for the FDA, ACR/EULAR and rheumatologists to gain comfort with their safety profiles?
- Will payors be willing to pay for novel pipeline agents given the size of the commercial market, $14.7B globally?
- How will the loss of European patent exclusivity for entrenched incumbents Remicade (2014), Enbrel (2015),
and Humira (2018) impact EU revenue considering that the EMA has already approved 14 bio-similars? • How will downward pricing pressure, caused by the entry of bio-similars, affect the opportunity of, and point
of entry in the treatment paradigm for future innovative approaches?
- How will the US’s Biologics Price Competition and Innovation Act impact the commercial landscape of biologics
in the US considering patent expiry for Enbrel (2014), Humira (2016), Remicade (2018)?
• Clinical Development and Regulatory Risk - Will regulators gain comfort approving agents in earlier treatment lines or will they continue to stage approvals?
- How will efficacy and safety requirements impact the point of entry in the treatment paradigm for novel therapies?
- Will more emphasis be placed on achieving ACR50 and ACR70 endpoints versus ACR20?
- Post Tofacitinib, how will pipeline assets overcome placebo challenges in short-term structural progression studies?
Lumleian’s
Perspective
• ACR50 response is achieved in fewer than 2/3 patients, leaving at least 1/3 of the most seriously affected patients with
rheumatoid arthritis without an effective long-term treatment strategy; acute need exists in later treatment lines
• This represents an attractive long-term opportunity for companies with novel therapies that can navigate regulatory
approval and payor reimbursements, and provide patients and clinicians with demonstrable efficacy/safety benefit ‐ Incumbent anti-TNFα’s will continue to dominate the market in the short term with slow but steady uptake of new MoAs
‐ Once oral agents demonstrate long-term safety and efficacy equivalent to current SoC, they will likely challenge anti-TNFα’s
the cornerstone of RA treatment after 1st line methotrexate; this will be slow over 3-5 years; novel biologics are a wild card
• Early diagnostic and prognostic markers are needed to ensure that appropriate treatment is initiated early and to identify
inadequate responders in earlier lines of treatment, for example ACR20 and power-doppler ultrasonography

9
0
1
2
3
4
5
Level of Unmet Need Likelihood of Technical Success Regulatory Impetus Commerical Attractiveness Required Investment
The attractiveness of investing in late stage clinical development is mechanistic specific based on
likelihood of technical success; appropriately the regulatory environment is highly conservative
dictating slow uptake; with high unmet RA is very commercially attractive for the right asset.
Average
RA: Relative Attractiveness of Greenfield Investment in Late Stage Clinical Development
High
Low
Required
Investment
Phase III Investment
• 500-1000 patients, with
2-3 Phase III trials minimum
• 6 month to 2 year length ‐ Safety extensions mandatory
• Costs increase dramatically
for active comparator trial
Commercial Spend
• Total category advertising
was ~$40M in Dec ’11 ($5M
per major brand) - $17.5M on health care
professionals
- $32.6M on consumers
Phase IV Investment
• New MoA requires long term
safety studies
• Active comparator studies
vs. anti-TNFα for 2nd line ‐ Studies: AMPLE, ADACTA
• Additional indications
beyond RA are standard
Level of
Unmet Need
Clinical Unmet Need
• Need exists in Anti-TNFα
inadequate responders
• Safety is a universal
concern for all lines
of treatment
Global Epidemiology
• 1.5M US prevalence ’11
• 3.3M EU prevalence ’11
Disease Burden
• ~$20B in tangible costs
• 33% patients stop work
within 2 years
Not a Cause of Mortality
• Mortality is increased in
RA patients, mainly due
to CV causes
Commercial
Attractiveness
Market Size
• WW ~$14.7B
• US ~$7.8B
Global Epidemiology
• 1.5M US prevalence ’11
• Declining diagnosis rates
Expansion Opportunities
• 2nd line of treatment
versus Anti-TNFα’s
Generic Penetration
• Generic methotrexate
dominates 1st line
• Bio-similars are certain
in EU and likely in US ‐ Rituxan EU (Aug ‘13)
‐ Remicade EU (Aug ‘14)
‐ Enbrel EU (Oct ‘15)
Competitive Launches
• 7 regulatory review/
Phase III drugs in pipeline
• Tofacitinib Q3/Q4 2012
Likelihood of
Technical Success
Unknown Etiology
• Combination of genetic
and environmental factors
Many Late Stage Failures
• AZD5672 (AZN); CEP-37247
(Cephalon); dnaJP1
(Adeona); Doramapimod (BI);
GLPG-0259 (Galapagos);
Maraviroc (PFE);
PF-05212368 (PFE);
MLN1202 (Millenium);
MLN3897 (Millenium);
RG4934 (Roche),
Pamapimod (Roche);
Scio-323; Scio-469 (Scios);
VX-702, VX-745 (VRTX)
Statistical Challenges
• Placebo radiography
challenges
• ACR endpoints well validated
Target Patient Populations
• Treatment naïve; MTX
failure; anti-TNFα failure
Regulatory
Environment
Regulatory Pathway
• High unmet need in 2nd
and 3rd lines of treatment
• Clear and established
regulatory pathway
Historical Precedents
• In Nov ‘98 Enbrel
• In Aug ‘98 Remicade ‐ Nov ‘99 in RA
• In Dec ‘02 Humira
• In Dec ‘05 Orencia
• In Nov ‘97 Rituxan ‐ Feb ‘06 in RA
• In Apr ‘09 Simponi
• In April ‘08 Cimzia ‐ May ‘09 in RA
• In Jan ‘10 Actemra
Safety Concerns
• Acute safety concerns
have led regulators to
initially restrict agents
to later treatment lines
Advocacy
• Arthritis Foundation
Highly
MoA specific
Well defined regulatory pathway,
but conservative labeling

10
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on rheumatoid arthritis?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is rheumatoid arthritis?
• Presentation, diagnosis, classification
• Epidemiology by geography and patient segment
• Current care paradigm and clinical evidence
• Emerging care paradigm
10 • 11 - 12
• 13 - 14
• 15
• 16 – 27
• 28
III. Clinical Development Pipeline • Disease mechanism overview
• Clinical development pipeline mapping
• JAK Inhibitors
• Syk Inhibitors
• c-Kit Inhibitors
• Anti-Baff antibodies
• Other mechanisms
29 • 30 - 32
• 33 – 38
• 39 – 45
• 46 - 48
• 49 - 50
• 51 - 52
• 53 – 71
IV. Commercial Landscape • Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
72 • 73 – 78
• 79
• 80 – 81
• 82 – 90
V. Appendix • Table of Acronyms
• More about Lumleian
91 • 92 – 93
• 94 – 96

11
Sources: 1Lajas C et al. Costs and Predictors of Costs in Rheumatoid Arthritis: A Prevalence-Based Study. Arthritis Rheum 2003;49: 64-70; 2Verstappen SMM
et al. Working status among Dutch patients with rheumatoid arthritis: work disability and working conditions. Rheumatology 2005; 44: 202- 206
Executive Summary: Disease Overview and Care Paradigm
• The global
What is
Rheumatoid
Arthritis?
• Rheumatoid arthritis is a chronic, debilitating, inflammatory condition, with a number of serious comorbidities
including cardiovascular disease, increased rate of infections, malignancies and osteoporosis - Rheumatoid arthritis affects about 1% of adults in industrialized countries and nearly three times as many women as men
- Onset commonly occurs between the ages of 30 and 60
• Rheumatoid arthritis has no known cause, but likely results from a combination of genetic and environmental factors - Non-modifiable risk factors include gender, aging, and genetics
- Modifiable risk factors include smoking, reproductive hormonal exposures, and periodontal disease (gingivitis)
What is the
disease burden?
• In 2011 estimated prevalence was ~1.5 M in the United States and ~3.3M in Europe - Prevalence has declined in the United States over the past decade and the annual incidence is estimated to be ~114K cases
• Rheumatoid arthritis is not a direct cause of mortality, although it increases the overall mortality ratio by 1.3 to 3,
primarily due to infections, malignancies and increased cardiovascular events
• Rheumatoid arthritis represents substantial financial burden in both tangible and intangible costs for patients,
employers and payors, private and particularly public: ‐ In the US the disease is estimated to cost $19.3B (tangible costs only) and $39.2B (with intangible costs) in ‘05 dollars
‐ Average annual cost to patients is estimated at $8,000 to $13,0001
‐ Cost to employers includes decreased productivity and absenteeism; this reduces tax revenue for public payors
• ~1/3 of patients stop work within two years and ~2/3 of patients are unable to work 15 years post onset
• ~40% of patients change their working conditions within 4 years2, as defined by reduced hours and/or pace of work
What is today’s
care paradigm?
• Under the current standard of care, treatment goals are symptom control and inhibition of structural damage
• Treatment of rheumatoid arthritis is driven by ACR/EULAR guidelines with DMARDs as the backbone of therapy ‐ Methotrexate is used as 1st line in naïve patients, anti-TNFα’s are used successively in 2nd line, and novel biologics are used 3rd
‐ Substantial unmet need exists in 3rd line for patients not responding to anti-TNFα’s and in 2nd line to reduce anti-TNFα cycling
• ~50% of patients stop responding to a particular DMARD after five years creating substantial unmet need later in treatment
What is the
emerging care
paradigm?
• For the foreseeable future methotrexate will remain the dominant choice for treatment naïve patients and the-
leading anti-TNFα’s (Humira, Enbrel, and Remicade) will continue to dominate 2nd line treatment
• Currently approved novel biologics (Orencia and Actemra) and once monthly anti-TNFα ‘s (Cimzia) are conducting
head-to-head trials in 2nd line; premised on superiority these will gain more traction with anti-TNFα naïve patients
• FDA precedent suggests that novel pipeline agents will be initially approved for 3rd line patients; over time once
safety has been validated in clinical practice they will receive label expansions to earlier lines of treatment
• Despite approval of new mechanisms and formulations FDA labels and ACR/EULAR guidelines will set a slow
timetable for new product uptake in earlier treatment lines; these guidelines will be effectively enforced by payors

12
No Yes (Women)
What is Rheumatoid Arthritis?
Description
• Rheumatoid arthritis is the most common systemic autoimmune disease, and is
characterized by chronic inflammation of the joints that can damage cartilage,
tendons and bone, lead to joint deformity and disability, and affect internal organs
- Rheumatoid arthritis affects about 1% of adults in industrialized countries, nearly
three times as many women as men, with common age of onset between 30 and 60
- Common co-morbidities include: cardiovascular disease, increased rate of infection,
lymphoproliferative malignancy, osteoporosis, psoriasis, and peptic ulcers
Etiology
• Rheumatoid arthritis has no known causes but likely results from a combination of
genetic and environmental factors
- The strongest genetic associations have been found with HLA class II DRB1*0401
and DRB1*0404 alleles and the PTPN22 gene
• Gender, aging, and genetics are non-modifiable primary risk factors
• Smoking, the highest modifiable risk factor, increases onset risk by 1.3 to 2.4 times
Symptom
Progression
• Symptoms vary widely between patients, from inactive to severe
• The hallmark symptom is synovitis, the inflammation of the lining of the joints
(synovium) that causes pain, stiffness and swelling, and potential irreversible damage
to the cartilage and bone leading to loss of function ‐ Synovitis usually affects the fingers and toes in the early stage, but can spread to the
knees, wrists, ankles, neck, shoulders, elbows, and even the jaw
‐ Joints are usually affected in a symmetrical pattern
• Systemic symptoms include flu symptoms (fatigue, malaise, loss of appetite, and
muscle aches), pleural effusion, pericardial effusion, vasculitis, anemia, nerve
entrapment, and eye dryness or inflammation (Sjögren’s syndrome)
Disease
Burden
• Rheumatoid arthritis has a standardized overall mortality ratio of 1.3 to 3 versus the
population, mainly due to increased rates of infection, malignancies, and CV risk
• Rheumatoid arthritis is a significant public health problem, and cost between $19.3B
(tangible costs) and $39.2B (with intangible costs included) in ‘05 dollars in the US - Employers and patients bear the majority of cost burden in lost productivity/wages
• Cost burden: Employers (33%); Patients (28%), Government (20%); Caregivers (19%)
- Intangible costs included quality of life deterioration ($10.3B) and mortality ($9.6B)
2. Is RA a primary cause of mortality?
7. Where is RA treated, commonly?
Yes No
Out
Patient
Inpatient
Hospital
Long
Term
Care
Symptom
Relief
Disease
Treatment
Disease
Cure
3. Is RA an acute or chronic disease?
Acute Chronic
6. Which specialties treat RA, commonly?
5. What is RA’ s treatment goal?
8. Who pays for RA care (Rx), commonly?
3rd party Cash Medicare
PCP Rheumatology
4. Is RA a communicable disease?
Yes No
1. Is RA’s etiology well understood?
Yes No
9. Does RA impact a special population?

13
Note: *Presence of blood rheumatic factor and citrulline antibodies, erythrocyte sedimentation rate, and levels of C-reactive protein
Currently, rheumatoid arthritis is diagnosed by the rheumatologist, who provides the backbone
of treatment, based on physical examination and serology results*; primary care physicians and
nurse educators help patients with daily management; other specialists support complications.
Diagnosis (Current)
• Patients commonly present with symmetrical joint stiffness,
swelling, pain, redness and warmth, usually in the fingers and
toes in the early stage
Referral Pathway (Current)
• Primary Care Physician: first point of contact; referral to
rheumatologist and patient managers
• Nurse Educator: registered nurse with special training and
background in education and caring for patients on daily
management
• Physical therapist: helps patient to improve joint function
• Occupational therapist: instructs patient to protect joints,
minimize pain, and conserve energy while performing
everyday tasks
• Dietician: established diet to reduce inflammation and weight
• Rheumatologist:
- Specialized training and experience in diagnosis and
pharmacological treatment of RA and related conditions
- Rheumatologists also refer patients to other specialists
for the treatments of complications
• Other Specialists:
- Podiatrist: trained to treat foot-related pain, deformity,
and decreased motion caused by rheumatoid arthritis
- Orthopedic surgeon: specialized in treating bones, joints,
muscles, and tendons and perform procedures such as joint
injections and joint replacement
Diagnosis and Referral Pathway (Current)
Key:
Specialists for complications
Chronic management
Patient
Primary Care
Physician
Nurse Educator
Lifestyle Program
Rheumato- logist
Specialist
(Podiatrist,
Surgeon)
1
2
3

14
The American College of Rheumatology (ACR) recommends that assessment of disease activity
involve combined estimation of six different disease activity scores based on joint examination,
pain assessment, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) blood levels.
Note: 1Each instrument has advantages and disadvantages and has been used interchangeably; 2Erythrocyte Sedimentation Rate; 3 C-Reactive
Protein; 4Visual Analog Scale (measurement of pain)
Source: Saag KG et al. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying
antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum 2008;59:762-784
Disease Activity Score1 Criteria Score Range Low Moderate High
• DAS28: Disease Activity
Score in 28 joints
• Joint exam,
ESR2/CRP3, VAS4 • 0-9.4 • ≤3.2 • >3.2 and ≤5.1 • >5.1
• SDAI: Simplified Disease
Activity Index
• Joint exam, CRP, VAS • 0.1-86.0
• ≤11 • >11 and ≤26 • >26
• CDAI: Clinical Disease
Activity Index
• Joint exam, VAS
• 0-76.0 • ≤10 • >10 and ≤22 • >22
• RADI: Rheumatoid
Arthritis Disease Activity
Index
• Self-report of joint
pain • 0-10
• <2.2 • ≥2.2 and ≤4.9 • >4.9
• PAS: Patient Activity
Index
• Self-report of global
health • 0-10 • <1.9 • ≥1.9 and ≤5.3 • >5.3
• RAPID: Routine
Assessment Patient
Index Data
• Self-report of global
health • 0-30 • <6 • ≥6 and ≤12 • >12

15
Source: Tobon et al. The environment, geo-epidemiology, and autoimmune disease: rheumatoid arthritis. Autoimmune Rev 2010;35:10-14; Myasoedova E
et al. Is the incidence of rheumatoid arthritis rising? Results from Olmsted County, Minnesota, 1955-2007. Arthritis Rheum. 2010 June ; 62(6): 1576–
1582; Bax M et al., Genetics of rheumatoid arthritis: what have we learned? Immunogenetics 2011;63:459-465
Rheumatoid arthritis incidence and prevalence rates are higher in North America and in Northern
Europe than in Southern Europe and other countries; For reasons that are unclear US incidence,
based on rheumatoid arthritis diagnosis rates, has declined over the past decade.
Moderate
2011 Prevalent Cases (M)
• Genetics: Contributes 50-60% to the risk of developing RA ‐ The genes most strongly associated are HLA-DRB1, which
contributes by 30-50% to the risk of developing RA, and PTPN22
‐ Additional genes include TRAF1-C5, TNFAIP3, STAT4, PADI4,
CTLA-4, IL2/IL21, CD28, PRDM1, and CD2/CD58
• Gender: The female-to-male ratio in RA patients is 3:1
• Age: The peak age of onset is the 5th decade
• Smoking: The strongest environmental risk factor, especially
in rheumatoid factor (RF)+ men and heavy smokers
• Socioeconomic factors: Affect the course and outcome of
RA but are not believed to influence the risk of developing RA
• Hormones: Several lines of evidences suggest that estrogens
are a risk factor associated with RA
• Ethnicity: Some ethnic and racial groups at higher risk than
others to develop RA, including Pima Indians
• Infections: The role of several infectious agents as initiating
factors of RA is controversial
• Diet: The Mediterranean diet may protect from rheumatoid
arthritis
Primary Risk Factors Secondary Risk Factors
1.5
3.3
0.5
0
2
4
US EU Japan
2011 Incidence: Total New Cases (K)
117
185
23
0
100
200
US EU JP
Prevalence
Rate: 0.50% 0.40%
Incidence Rate:
(Cases per 100K
person per year) 38 24 18 0.44%

16
Diagnosis (Current)
• Diagnosis is based on physical examination and blood tests and
a definitive rheumatoid arthritis diagnosis is confirmed by:
‐ Blood autoantibodies: Rheumatic factor and citrulline antibodies
‐ Abnormal acute-phase response: Abnormal ESR and C-reactive protein
• X-rays are used to monitor disease progression in the joints
Treatment (Current)
• Updated ACR treatment recommendations (2012), include: ‐ Reiterating DMARDs as backbone of care
• Omits specific role for glucocorticoids and NSAIDs
‐ Shortening the treatment response window to 3-6 months
• 1st Line: Initiate treatment with non-biologic DMARDs - Use as mono-therapy or in dual/triple combination therapy:
• Methotrexate (MTX), Hydroxychloroquine (HCQ)
• Leflunomide (LEF), Minocycline, Sulfasalazine
- Add MTX, HCQ, or LEF if inadequate response after 3 months
- Switch to a non-MTX non-biologic DMARD after a year to minimize
hepatoxicity risk, for example Leflunomide
• 2nd line: Switch to anti-TNFα - Add or switch to an anti-TNFα if inadequate response
after 3-6 months; repeat anti-TNFα cycling as necessary
• 3rd line: Switch to novel biologic - Switch to Orencia, Actemra, or Rituxan if inadequate
response to multiple anti-TNFα’s
- Kineret has less attractive efficacy/safety profile
• Monitor disease progression as defined by: ‐ Tender and swollen joint counts, CRP level, and patient global
assessment of ≤1 each or a simplified DAS of ≤3.3
‐ Joint X-rays to monitor disease progression and structural damage
Source: Saag KG et al. American College of Rheumatology 2008 recommendations for the use of non-biologic and biologic disease-modifying anti-rheumatic
drugs in rheumatoid arthritis. Arthritis Rheum 2008;59:762-784; Singh JA et al. 2012 update of the 2008 American College of Rheumatology
recommendations for the use of disease-modifying anti-rheumatic drugs and biologic agents in the treatment of rheumatoid arthritis. Arthritis Care Res
2012;5:625-639; Smolen JS et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying
anti-rheumatic drugs. Ann Rheum Dis 2010;69:964-975
A well established standard of care exists to treat rheumatoid arthritis: (1) Non-biologic DMARDs
are used 1st line, (2) Anti-TNFα’s are used successively in 2nd line, (3) Novel biologics are reserved
for 3rd line; Substantial unmet need exists in 3rd line for patients not responding to anti-TNFα’s.
Diagnosis:
Low Activity
with Good Prognosis
Low with Poor Prognosis
or Moderate/High Activity
Physical Examination
Blood Test
Add / Switch
NB DMARD monotherapy
Anti-TNFα
Other Anti-TNFα
Novel Biologic
Switch
Methotrexate or
NB DMARD Combination
NB DMARDs
Switch Anti-TNFα
or Novel
Biologic
Add /Switch
Anti-TNFα or Novel Biologic
Switch Switch
Switch
Stratification:
1st line:
2nd line:
3rd line:

17
Note: *Selective NSAIDs are generally considered less toxic than nonselective NSAIDs for the gastrointestinal mucosa, but there is still some
controversy. **Celebrex is the only COX-2 inhibitor approved in the US following the withdrawal of Vioxx (rofecoxib) and Bextra (valdecoxib),
which were associated with an increased risk of heart attack and stroke
Source: Product prescription information; Company press release
Dosing
Safety
Mechanism
of Action
Efficacy
Brands
Generics
• Synthetic analogues to steroid
hormones that bind to the
glucocorticoid receptor ‐ Up-regulate anti-inflammatory
proteins, and down-regulate pro-
inflammatory proteins
• Oral, or injection into the joint
Glucocorticoids
• Reduces pain and swelling as a
low-dose “bridge therapy” when
initiating DMARDs, or short-term
high-dose therapy in some patients
• Swelling/edema
• Easy bruising
• Mood swings, insomnia, euphoria
• Risk of infection
• Decadron (dexamethasone)
• Medrol (methylprednisolone)
• Deltason (prednisone)
• Orasone (prednisone)
• Meticorten (prednisone)
• Celestone (betamethasone)
• Aristopan (triamcinolone)
• Yes
• Inhibit COX-2 selectively versus
COX-1, which is constitutively
expressed in the gastrointestinal
tract, blood platelets, and blood
vessels
• Oral
Selective NSAIDs*
• Liver toxicity
• Kidney toxicity
• Ringing in the ears
• Increased cardiovascular risk
• Celebrex (celecoxib)**
• Yes
Despite omission from the ACR’s updated treatment guidelines (2012), glucocorticoids and
non-steroidal anti-inflammatory drugs are commonly prescribed for short-term symptom relief;
clinicians prescribe these judiciously, most often as a bridge therapy when initiating DMARDs.
• Inhibit both cyclooxygenase (COX)
enzyme isoforms COX-1 and COX-2,
thereby inhibiting the production
of prostaglandins
• Oral
Nonselective NSAIDs
• Dyspepsia, peptic ulcer disease
• Liver toxicity
• Kidney toxicity
• Ringing in the ears
• Aspirin
• Advil (ibuprofen)
• Motrin (ibuprofen)
• Nuprin (ibuprofen)
• Aleve (naproxen)
• Voltaren (diclofenac sodium)
• Yes
• Reduce pain and swelling at low
dose, and fully treat inflammation
at higher doses
• Reduce pain and swelling at low
dose, and fully treat inflammation
at higher doses

18
Source: Product prescription information; Company press release
Dosing
Safety
Mechanism
of Action
Efficacy
Brands
Generic
• Mechanism of action
in RA is unknown ‐ Antimetabolite that
inhibits dihydrofolic
acid reductase
• QW Oral
Methotrexate
• Efficacious for
prolonged treatment ‐ 35-57% ACR20
at 6 months
• Teratogenic action
• Hepatotoxicity
• Myelosuppression
• Aplastic anemia
GI disorders with
NSAIDs
• Lung disease
• Severe skin reactions
• Rheumatrex
• Trexall
• Folex
• Yes
• Prevents expansion of
activated lymphocytes ‐ Inhibits pyrimidine
synthesis by inhibiting
dihydroorotate
dehydrogenase
• QD Oral
Leflunomide
• Teratogenic action
• Hepatotoxicity
• Myelosuppression
• Infections
• Anemia, bleeding
• Lung disease
• Arava
• Yes
• Mechanism of action
in RA is unknown ‐ Inhibits lysosomal
acidic proteases,
causing a diminished
proteolysis
‐ Antimalarial
• QD oral
Hydroxychloroquine
• Eye toxicity
• Plaquenil
• Yes
• Broad spectrum
tetracycline antibiotic ‐ Decreases production
of leukotriene and
prostaglandin
‐ Increases IL-10
production
• BID oral
Minocycline
• Drug reaction with
eosinophilia and
systemic symptoms
(DRESS)
• Thyroid cancer
• Minocin
• Dynacin
• Yes
• Activates liver enzyme
AMPK, which suppresses
hepatic gluconeogenesis
• Also increases Insulin
sensitivity
• BID oral
Sulfasalazine
• Hypersensitivity
• Allergic reaction
• Mild GI symptoms
• Azulfidine
• Yes
• Efficacious for
prolonged treatment ‐ 41-49% of ACR20
at 6 months
• Efficacious for
prolonged treatment
• Efficacious for
prolonged treatment ‐ 35-45% of ACR20
at 6 months
• Efficacious for
prolonged treatment
Generic non-biologic DMARDs, alone or in combination, are the standard of care in 1st line
patients who are treatment naïve; unfortunately only a third to half of patients treated with
methotrexate achieve ACR20 necessitating adding or switching to an anti-TNFα.

19
Source: Product prescription information; Company press release; Comparative effectiveness of drug therapy for rheumatoid arthritis and psoriatic
arthritis in adults (Agency for Healthcare Research and Quality, Rockville, MD, Nov. 2007)
Methotrexate is the is the most commonly prescribed 1st line DMARD, despite hepatoxicity risks
and frequent liver function tests; in year one more patients treated with methotrexate achieve
ACR20 than leflunomide patients; thereafter leflunomide is as effective with less toxicity.
Non-biologic DMARDs
Methotrexate Leflunomide
Sponsor • Pharmacia and Upjohn (Folex)
• Deva Pharmaceuticals (Rheumatrex)
• Treva Pharmaceuticals (Trexall)
• Sanofi
Formulation • Tablet (2.5 mg) • Tablet (10, 20, or 100 mg)
Dosing • Oral: QW • Oral: QD with loading dose
Indications • Treatment of adult patients with all RA durations
and for all degrees of disease activity, irrespective
of poor prognosis – 10-25 mg weekly orally
• Treatment of adult patients with all RA durations
and for all degrees of disease activity, irrespective
of poor prognosis – 10-20 mg daily orally
Adverse Events
• Liver toxicities (15%)
‐ Requires quarterly liver function tests (15%)
• Nausea/vomiting (10%)
• Stomatitis (3-10%)
• Thrombocytopenia (3-10%)
• Diarrhea (17%)
• Respiratory infection (15%)
• Hair loss (10%)
• Rash (10%)
Lumleian
Commentary
• Methotrexate is the most commonly prescribed DMARD based on its demonstrated 1st year efficacy, 35-57%
ACR20 at 6 months, despite significant hepatoxicity risks ‐ Studies indicate that more than 50% of patients who take methotrexate continue on therapy for more than
three years, which is longer than for any other DMARD
‐ More patients meet the ACR20 improvement criteria at year one with methotrexate than with leflunomide,
but statistical difference is lost after two years
• There is no difference between methotrexate and leflunomide in radiographic outcomes over two years

20
Source: Product prescription information; Company press release; Comparative effectiveness of drug therapy for rheumatoid arthritis and psoriatic
arthritis in adults (Agency for Healthcare Research and Quality, Rockville, MD, Nov. 2007)
Non-biologic DMARDs
Hydroxychloroquine Minocycline Sulfasalazine
Sponsor • Sanofi (Plaquenil) • Triax (Minocin)
• Medicis (Dynacin)
• Pfizer (Azulfidine)
Formulation • Tablet (200 mg) • Capsule (50, 100 mg) • Tablet (500 mg)
Dosing • Oral: QD • Oral: BID • Oral: BID
Indications • Mono-therapy recommended for
patients without poor prognosis
features, with low disease activity,
and with disease duration ≤24 months – 400 to 600 mg daily (induction)
– 200 to 400 mg daily (maintenance)
• Mono-therapy recommended for
patients without poor prognosis
features, with low disease
activity, and with short disease
duration – 200 mg initially
– 100 mg every 12 hours thereafter
• Mono-therapy recommended for
patients with all RA durations and
for all degrees of disease activity,
irrespective of poor prognosis – 2 to 3 grams per day in a twice
daily doing regimen
Adverse Events
• CNS reactions
• Neuromuscular reactions
• Ocular reactions
• Dermatologic reactions
• Hematologic reactions
• Gastrointestinal reactions
• Allergic reactions
• Diarrhea
• Dizziness
• Drowsiness
• Indigestion
• Lightheadedness
• Loss of appetite
• Nausea
• Headache
• Hypersensitivity reaction
• Photosensitivity
• Serum sickness-like syndrome
Lumleian
Commentary
• Sulfasalazine mono-therapy is less efficacious at 2 years (ACR20 and ACR50) than Leflunomide mono-therapy
Other non-methotrexate DMARDs play second fiddle to methotrexate and leflunomide; prolonged
use of hydroxychloroquine is associated with a decrease in cardiovascular disease, which is an
acute concern for rheumatoid arthritis patients who are at higher risk than the overall population.

21
Note: *An ACR20 response is defined as a 20% reduction in the number of swollen and tender joints, and a 20% reduction in 3 out of 5 other parameters
Biologic DMARDs, most commonly used as 2nd line therapy, have revolutionized the treatment of
RA underlining the key roles of T Cells, B Cells, and cytokines in disease pathogenesis; anti-TNFα’s
are the cornerstone of biologic DMARD treatment and capture ~90% of biologic market share.
Source: Product prescription information; Company press release
Dosing
Safety
Mechanism
of Action
Efficacy
Brands
Generic
• Block interaction of
TNFa with its
receptors, which
affects TNFa role in
inflammation and
joint destruction
• QW, QM IV or sub-c
Anti-TNFa’s
• 45 to 76% ACR20*
over 3 to 6 months
• Risk of serious
infections, including
TB reactivation, and
malignancies,
including lymphoma
• Humira (adalimumab)
• Remicade (infliximab)
• Enbrel (entanercept)
• Cimzia (certolizumab)
• Simponi (golimumab)
• No
• CTLA-4Ig fusion
protein: blocks CD80
and CD86 interactions
with CD28, which
inhibits T Cell
activation and
proliferation
• QM IV or QW sub-c
T Cell
Costimulation
Inhibitor
• 67.9% ACR20*
at 6 months
• Risk of serious
infections and
malignancies ‐ Increased with
concomitant
anti-TNFα usage
• Orencia (abatacept)
• No
• Rituxan (rituximab)
• Induces B Cell lysis by
binding to CD20,
inhibits B Cell-driven
inflammation,
autoantibody
formation, and
cytokine release
• Every 24 weeks IV
B Cell
Inhibitor
• 65 to 76% of ACR20*
at 6 months
• Risk of fatal infusion
reactions, severe
mucocutaneous
reactions, and
progressive multifocal
leukoencephalopathy
• No
• Inhibits IL-6-mediated
signaling via binding
to IL-6 receptors,
which inhibits IL-6
pro-inflammatory
actions
• QM IV
IL-6
Inhibitor
• 50 to 70% of ACR20*
at 6 months
• Risk of serious
infections
• Actemra (tocilizumab)
• No
• Blocks interaction of
IL-1 with its receptor.
which inhibits IL-1-
mediated cartilage
degradation, bone
resorption, and other
activities
• QD sub-c
IL-1
Inhibitor
• Risk of serious
infections
• Kineret (anakinra)
• No
• 38 to 43% of ACR20*
at 6 months
Key:
3rd line
(primarily)
2nd line
(primarily)

22
Source: Product prescription information; Company press release; Comparative effectiveness of drug therapy for rheumatoid arthritis and psoriatic
arthritis in adults (Agency for Healthcare Research and Quality, Rockville, MD, Nov. 2007)
Anti-TNFα’s
Humira (adalimumab) Enbrel (entanercept) Remicade (infliximab)
Sponsor • Abbott • Amgen/Pfizer • Johnson and Johnson/Merck
Formulation
• Pre-filled syringe / pen (40 mg) • Pre-filled syringe (50 or 25 mg)
• Lyophilized powder (25 mg)
• Lyophilized powder (100 mg)
Dosing • Subcutaneous: QW • Subcutaneous: QW • Intravenous: Q8W
Mono-therapy • Yes • Yes • No
Combination
therapy
• Yes with methotrexate • Yes with methotrexate • Yes with methotrexate
Indications • In adult patients with moderately to
severely active rheumatoid arthritis: ‐ Reducing signs and symptoms
‐ Inducing major clinical response
‐ Improving physical function
‐ Inhibiting the progression of
structural damage
• In adult patients with moderately to
severely active rheumatoid arthritis: ‐ Reducing signs and symptoms
‐ Inducing major clinical response
‐ Improving physical function
‐ Inhibiting the progression of
structural damage
• In adult patients with moderately to
severely active rheumatoid arthritis: ‐ Reducing signs and symptoms
‐ Inducing major clinical response
‐ Improving physical function
‐ Inhibiting the progression of
structural damage
Adverse
Events
• Injection site reaction (20%)
• Upper respiratory tract infection (17%)
• Headache (12%)
• Rash (12%)
• Sinusitis (11%)
• Infection (27%)
• Upper respiratory tract infection (17%)
• Injection site reaction (15%)
• Non-upper respiratory infection (12%)
• Upper respiratory tract infection (32%)
• Nausea (21%)
• Headache (18%)
• Sinusitis (14%)
Lumleian
Commentary • Clinical studies show no differences in ACR20 and ACR50 response rates among the three leading anti-TNFα’s
• In clinical practice Remicade is favored less for private patients but is the standard of care for Medicare patients ‐ It is perceived as less convenient, absent a sub-cutaneous formulation, and lacks a mono-therapy indication
• Anti-TNFα’s in combination with methotrexate are more efficacious than either anti-TNFα or methotrexate mono-therapy
Sub-cutaneous Humira and Enbrel lead the anti-TNFα’s with private payors; Remicade is used
mainly in Medicare - it is an intravenous formulation and lacks a mono-therapy indication; as a
class the Anti-TNFα’s recently received a black box serious infection/tuberculosis warning.

23
Cimzia and Simponi offer once monthly sub-cutaneous dosing; as the 4th and 5th anti-TNFα’s to
market they account for ~10% market share; clinicians question duration of effect and head-to-
head trials are ongoing; in July 2011 the FDA rejected a “structural” indication for Simponi.
Anti-TNFα’s
Cimzia (certolizumab pegol) Simponi (golimumab)
Sponsor • UCB • Johnson and Johnson/Merck
Formulation • Single-use pre-filled syringe (200 mg) • Single-use pre-filled syringe (50 mg)
Dosing • Subcutaneous: QOW (QM maintenance) ‐ 400 mg (twice 200 mg) at weeks 1, 2, and 4,
followed by 200 mg every other week
‐ For maintenance 400mg every 4 weeks can be
considered
• Subcutaneous: QM ‐ With methotrexate, 50 mg once a month
Indications • Treatment of adults with moderately to severely
active RA ‐ Reducing signs and symptoms
‐ Inducing major clinical response
‐ Improving physical function
‐ Inhibiting the progression of structural damage
• In combination with methotrexate, treatment of adults
with moderately to severely active rheumatoid arthritis ‐ Reducing signs and symptoms
‐ Inducing major clinical response
‐ Improving physical function
Adverse Events
• Upper respiratory tract infection (6%)
• Headache (5%)
• Hypertension (5%)
• Nasopharyngitis (5%)
• Upper respiratory tract infection (16%)
• Injection site reaction (6%)
• Viral infection (5%)
• Hypertension (3%)
Lumleian
Commentary
• Both Cimzia and Simponi offer more convenient dosing and greater flexibility ‐ Cimzia offers flexible dosing options and a rapid onset (1 to 2 weeks in some patients)
‐ Simponi has similar efficacy and safety as Humira and Enbrel, and can be administered less frequently than other
anti-TNFα’s (once monthly for maintenance)
• Clinically physicians question whether the longer acting effect may taper off towards the end of the month ‐ Cimzia is currently conducting the EXXELERATE trial, which is a head-to-head trial versus Humira to assess the impact
of early responder treatment after 12 weeks
Source: Product prescription information; Company press release

24
Orencia, a CTLA4-immunoglobulin fusion protein, is the market leading non anti-TNFα biologic
based on its relatively attractive safety profile and recent subcutaneous formulation; head-to-
head data versus Humira in combination with methotrexate is scheduled for release in June ‘12.
T Cell Costimulation Inhibitor
Orencia (abatacept)
Sponsor • Bristol-Myers Squibb
Formulation • Lyophilized powder (250 mg) ‐ Intravenous dosing regimen: 30-min IV infusion (500-1000 mg per body weight ) followed by IV infusion at 2 and 4 weeks
and every 4 weeks thereafter, alone or with concomitant DMARDs other than anti-TNF
• Single-dose prefilled syringe (125 mg/ml) ‐ Subcutaneous dosing regimen: 30-min IV infusion (500-1000 mg per body weight) followed by 125 mg within a day,
and 125 mg once weekly thereafter, alone or with concomitant DMARDs other than anti-TNF
Dosing • Intravenous: QM
• Subcutaneous: QW
Indications • In adult patients with moderately to severely active rheumatoid arthritis: ‐ Reducing signs and symptoms
‐ Inducing major clinical response
‐ Improving physical function
‐ Inhibiting the progression of structural damage
Adverse Events
• Headache (18%)
• Nasopharyngitis (12%)
• Dizziness (9%)
• Cough (8%)
Lumleian
Commentary
• Orencia does not have a black box warning for tuberculosis (a confirmatory test is not required), and is not
contra-indicated in patients with congestive heart failure, unlike the anti-TNFα’s ‐ Safety issues include increased risk of infections, increased COPD flares, and a contra-indication in cancer patients
• Orencia has achieved ~70% ACR20 at 6 month in anti-TNFα inadequate response patients
• To effectively compete in earlier lines of treatment versus the anti-TNFα’s Orencia will release data, in June
‘12, from its head to head trial (AMPLE) versus Humira in combination with methotrexate
Source: Product prescription information; Company press release

25
Actemra, an IL-6 inhibitor, is disadvantaged versus Orencia as it is only approved in 3rd line for
patients refractory to anti-TNFα’s and is an intravenous formulation; Actemra’s recent phase IV
data showed superiority in 2nd line versus Humira; a sub-cutaneous formulation is being pursued.
Interleukin-6 Inhibitor
Actemra (tocilizumab)
Sponsor • Roche/Chugai
Formulation • Single-use vial (80, 200 or 400 mg)
Dosing • Intravenous: QM ‐ 60-min IV infusion once every 4 weeks, 8-12 mg/kg, alone or in combination with methotrexate, but not in combination
with any biologic DMARD
Indications • Treatment of adult patient with moderately to severely active RA who have had an inadequate response to
one or more anti-TNF agent ‐ Reducing signs and symptoms
‐ Inducing major clinical response
‐ Improving physical function
‐ Inhibiting the progression of structural damage
Adverse Events
• Upper respiratory tract infection (6-8%)
• Headache (5-7%)
• Hypertension (4-6%)
• Nasopharyngitis (4-7%)
Lumleian
Commentary • Actemra appears to be as efficacious as the anti-TNFα’s but has been constrained by: (1) The FDA granting only a
3rd line indication, a 2nd line expansion is anticipated with more safety data, and (2) An intravenous formulation
• Top line data from the ADACTA phase IV trial indicated that Actemra mono-therapy achieved superiority to
Humira mono-therapy on its primary end-point (DAS28) and all secondary end-points (ACR20, ACR50, ACR70) ‐ ADACTA compared mono-therapies and Humira with methotrexate is more efficacious than Humira mono-therapy
‐ Further the majority of clinical usage is combination therapy with methotrexate
• The FDA approved Actemra as a 3rd line agent, despite having compelling 2nd line data and a strong majority vote for approval
‐ This may set precedent for other novel pipeline agents seeking approval; in their briefing the FDA stressed the number of
recently approved agents and the need to trade the relative unmet need in later lines versus safety concerns
Source: Product prescription information; Company press release

26
Rituxan, an anti-CD20 antibody, offers strong efficacy, but is used as a last resort versus Orencia
and Actemra; it has a relatively high rate of injection site infections and patients treated with
Rituxan are at increased risk for potentially fatal viral infections of the white brain matter.
B Cell Inhibitor
Rituxan (rituximab)
Sponsor • Biogen Idec/Roche
Formulation • Single-use solution vial (100 or 500 mg)
Dosing • Intravenous ‐ With methotrexate, two 1,000 mg intravenous infusions separated by 2 weeks (one course) every 24 weeks or
based on clinical evaluation, but not sooner than every 16 weeks
Indications • In combination with methotrexate, treatment of adult patient with moderately to severely active rheumatoid
arthritis who have had an inadequate response to one or more anti-TNF agent ‐ Combination therapy with methotrexate has been shown to yield greater response rates over 2 years (ACR20, ACR50)
than Rituxan mono-therapy
Adverse Events
• Infusion reaction (32% within 24 hours following first infusion)
‐ 11% within 24 hours following second infusion
• Hypertension (8%)
• Nausea (8%)
• Upper respiratory tract infection (7%)
• Arthralgia (6%)
Lumleian
Commentary • Rituxan has demonstrated strong efficacy in 3rd line patients: 65 to 76% of ACR20 at 6 months
• Safety issues include a relatively high risk of infusion reactions and progressive multiple focal
leukoencephalopathy (PML) infection ‐ PML, is a rare viral disease characterized by progressive inflammation of white brain matter; it is commonly fatal
Source: Product prescription information; Company press release; Comparative effectiveness of drug therapy for rheumatoid arthritis and psoriatic
arthritis in adults (Agency for Healthcare Research and Quality, Rockville, MD, Nov. 2007)

27
Kineret, an IL-1 inhibitor, is rarely used to treat rheumatoid arthritis; nearly three out of four
patients experience an injection site infection; Kineret is thought to be less efficacious than
Rituxan in 3rd line anti-TNFα inadequate response patients yielding 38-43% ACR20 at 6 months.
Interleukin-1 Inhibitor
Kineret (anakinra)
Sponsor • Biovitrum
Formulation • Single-use prefilled syringe (100 mg)
Dosing • Subcutaneous: QD ‐ 100 mg daily, or every other day for patients with renal insufficiency
Indications • Treatment of adult patient with moderately to severely active RA who have had an inadequate response
to one or more anti-TNF agent ‐ Reducing signs and symptoms
‐ Inhibiting the progression of structural damage
Adverse Events
• Injection site reaction (71%)
• Worsening of RA (19%)
• Upper respiratory infections (14%)
• Headache (12%)
Lumleian
Commentary
• Although it is effective in other auto-inflammatory diseases, Kineret has only demonstrated moderate
effectiveness in rheumatoid arthritis, achieving 38-43% ACR at 6 months in anti-TNFα inadequate responders ‐ In comparison Rituxan has demonstrated strong efficacy in 3rd line patients: 65 to 76% of ACR20 at 6 months,
albeit not in head-to-head trials
Source: Product prescription information; Company press release; Kalliolias GD and Liossis SN, Expert Opin Investig Drugs 2008;17:349-59

28
Source: Geriag DM et al. EULAR recommendations for terminology and research in individuals at risk of rheumatoid arthritis: report from the Study
Group for Risk Factors for Rheumatoid Arthritis. Ann Rheum Dis 2011 doi:10.1136; Lindstrom T and Robinson WH. Biomarkers for rheumatoid
arthritis: making it personal. Scand J Clin Lab Invest 2010;70:79-84; Duroux-Richard I et al. miRNAs and rheumatoid arthritis – promising novel
biomarkers. Swiss Med Weekly;2011:w13175
Near term Lumleian sees slow but deliberate evolution of the treatment paradigm to include
novel mechanisms, starting in 3rd line and moving forward; long term Lumleian foresees a
progression toward more personalized care based on genetic and proteomic biomarkers.
• Additional risk factors and biomarkers are needed for (1) early diagnosis, (2) assessment and prediction
of disease severity, (3) selection of therapy, and (4) monitoring response to therapy: ‐ Risk factors and biomarkers will likely enable clinicians to identify patients at risk of developing clinical rheumatoid arthritis
‐ Biomarkers will likely allow clinicians to predict the state of progression of joint destruction and the development
of extra-articular manifestations, potentially allowing for a more aggressive approach in susceptible patients
‐ Therapy is still conducted on a trial-and-error basis prognostic biomarkers will likely improve therapy selection
• Proteomic and genetic biomarkers are being pursued but are quite far from clinical practice ‐ Proteomic biomarkers will likely be more valuable, but their development presents technical challenges
‐ Genetic biomarkers are useful as risk factors, but changes in genetic sequence does not always translate into changes
in gene expression and protein activity, which limits their clinical application
• Several candidate biomarkers have been recently described: - Anti-mutated citrullinated vimentin (MCV) might allow better diagnosis than anti-cyclic citrullinated peptides (CCPs)
- Genotypes of follate enzymes may predict which patients will develop adverse side effects in response to methotrexate
- A biomarker signature of 13 auto-antibodies and 11 cytokines has been shown to predict patients’ response to anti-TNFα’s
- An IFN signature was shown to predict patients’ response to rituximab treatment
- Several microRNAs (miRNAs) were found to be up-regulated in rheumatoid arthritis, and may become valuable biomarkers
• For the foreseeable future methotrexate will remain the dominant choice for treatment naïve patients and
the-leading anti-TNFα’s (Humira, Enbrel, and Remicade) will continue to dominate 2nd line treatment
• Currently approved novel biologics (Orencia and Actemra) and once monthly anti-TNFα ‘s (Cimzia) are conducting
head-to-head trials in 2nd line; premised on superiority these will gain more traction with anti-TNFα naïve patients
• FDA precedent suggests that novel pipeline agents will be initially approved for 3rd line patients; over time once
safety has been validated in clinical practice they will receive label expansions to earlier lines of treatment
• Despite approval of new mechanisms and formulations the FDA label, ACR/EULAR guidelines will set the timetable
for new product uptake in earlier treatment lines; these guidelines will be effectively enforced by payors
• Once oral agents demonstrate long-term safety and efficacy equivalent to current SoC, they will likely challenge
anti-TNFα’s the cornerstone of treatment after 1st line methotrexate ; this will be slow over 3-5 years
Future
Diagnosis
(Long Term)
Future
Treatment
(Near Term)

29
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on rheumatoid arthritis?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is rheumatoid arthritis?
• Presentation, diagnosis, classification
• Epidemiology by geography and patient segment
• Current care paradigm and clinical evidence
• Emerging care paradigm
10 • 11 - 12
• 13 - 14
• 15
• 16 – 27
• 28
III. Clinical Development Pipeline • Disease mechanism overview
• Clinical development pipeline mapping
• JAK Inhibitors
• Syk Inhibitors
• c-Kit Inhibitors
• Anti-Baff antibodies
• Other mechanisms
29 • 30 - 32
• 33 – 38
• 39 – 45
• 46 - 48
• 49 - 50
• 51 - 52
• 53 – 71
IV. Commercial Landscape • Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
72 • 73 – 78
• 79
• 80 – 81
• 82 – 90
V. Appendix • Table of Acronyms
• More about Lumleian
91 • 92 – 93
• 94 – 96

30
Executive Summary: Clinical Development Pipeline
What is in the
industry’s
clinical
development
pipeline?
• Most pipeline therapies in development focus on managing chronic symptoms and inhibiting structural damage,
similar to marketed agents
• Patient’s heterogeneous response to treatment remains a key development challenge, as highlighted by recent
pipeline failures: - AZD5672 (AZN); CEP-37247 (Cephalon); dnaJP1 (Adeona); Doramapimod (BIPI); GLPG-0259 (Galapagos); Maraviroc, PF-05212368
(PFE); MLN1202, MLN3897 (Millenium); RG4934, Pamapimod (Roche); Scio-323, Scio-469 (Scios); VX-702, VX-745 (VRTX)
• The overwhelming majority of drugs in development target the immune system including cytokines and chemokines
(TNFa,IL-6, CCR1), cell signaling (JAK, p38 MAPK, Syk), B Cell modulators (CD20, BAFF, CD19), and T Cell
modulators (CD4, CD28/80, CD3, CTLA4)
• The pipeline is very crowded and Lumleian validated 82 assets in ‘active’ clinical development ‐ 7 in US Regulatory/Phase III, 44 in Phase II, and 31 in Phase I
• Once approved US regulatory precedent suggests, Actemra, the initial label will restrict usage to later lines of
therapy, where unmet need is greatest; Subsequent label extensions expand usage to earlier treatment lines
What is the
evidence for
late stage
assets?
• Kinase Inhibitors: Although numerous kinase Inhibitors have failed in clinical trials, evidence suggests
that moving higher in the signaling cascade may provide efficacy with a more tolerable safety profile
‐ Nine JAK Inhibitors targeting various combinations of isoform subtypes are in development • Pfizer’s Tofacitinib will likely be the first orally available kinase inhibitor approved for RA; Most likely approved in 3rd line;
The FDA Arthritis Advisory Committee meeting on May 9th voted 8:2 in favor of approval and the PDUFA date is set for August 2012
• Phase IIb trial data for Baricitinib (Incyte/LLY) is anticipated at EUALR in June; Incyte CEO, Paul Friedman, suggests
that Phase III trials are expected to begin in 2012 but Lilly has not made a statement of public commitment
‐ Oral Syk Inhibitors are promising; In addition to offering impressive inflammation control, they also slow bone
resorption by osteoclasts; Three Syk Inhibitors are in development • Fostamatinib (AZN/Rigel) is leading the field with 6 month Phase III data anticipated in Q2 2012
• Cytokine Inhibitors: Anti-Il6 is a proven MoA in rheumatoid arthritis; Actemra was FDA approved in 2010, but
currently garners only modest market share and is only indicated for 3rd line patients ‐ Other late stage assets including Sarilumab (Regeneron/SNY) will need to offer clear clinical differentiation
• B Cell modulators: A number of B Cell modulators are currently in development ‐ Rituxan, the first drug to selectively target CD20 positive B Cells, is being eyed by generic manufacturers Spectrum and Teva
• Other anti-CD20 agents Ofatumumab (GSK/Genmab), Veltuzumab (Immunomedics/Takeda) and SBI-087 (Emergent Biosolutions/PFE)
will need to offer clear clinical differentiation
‐ Similarly Lilly’s anti-BAFF antibody, Tabalumab, which shares the same MoA (B Cell depletion) will need to offer clear clinical
advantage over anti-CD20 antibodies • GSK/ HGSI’s rheumatoid arthritis program for Belimumab was terminated by decision of the sponsor (unrelated to safety)

31
Sources: McInnes IB and Schett G. Cytokines in the pathogenesis of rheumatoid arthritis. Nat Rev Immunol 2007;7:429-442; Schaper F. Institute of Biology,
Otto von Guericke University Magdeburg, Germany
New therapeutics for RA are directed at a myriad of cellular and intracellular targets including
antibodies against pro-inflammatory cytokines, chemokines, adhesion molecules, T Cells, B Cells,
and small molecules targeting kinases and transcription factors involved in cell signaling.
B Cell Inhibitors: • Anti-CD20
• Anti-CD19
• Anti-BAFF
T Cell Inhibitors: • Anti-CD4
• Anti-CD3
• CTLA4-Ig
Cytokine Inhibitors: • Anti-RANKL
• Anti-IL-17
Macrophage Inhibitors
Cytokine Inhibitors: • Anti-TNF
• Anti-IL-1
• Anti-IL-6
Cytokine Inhibitors: • Anti-M-CSF
Adhesion Inhibitors: • Anti-VLA-1
• Anti-VAP-1
• Anti-chemokine
JAK Inhibitors
PI3K Inhibitors
STAT3/NFkB
Inhibitors
NFkB Inhibitors
PPARg Inhibitors
p38MAPK
Inhibitors
Cell Signaling Inhibitors:

32
Clear consensus exists on the need for new therapies based on the moderate rates of remission
achieved by approved biologics; it is also clear regulators will treat new therapies cautiously;
It is very unclear how the many alternative pipeline mechanisms will be utilized in practice.
Key
Unknowns
• Development of new drugs targeting specific pathways or cell subsets is motivated by the low rate of
remission achieved by RA patients, the lack of uniform response to biologics, and the association of
biologics with concerning adverse events, such as infections and risk of malignancies
• Regulatory precedent suggests novel therapies will initially be approved in 3rd line patients with
supplementary label expansions to early lines of treatment; this is consistent with unmet needs
Source: Lipsky PE. Are new agents needed to treat RA? Nat Rev 2009;5:521-522
• The combination of novel drugs and biomarker guidance will likely improve remission rates,
drug safety, and treatment cost
• That said it is very unclear which therapies will emerge as viable competitors to anti-TNFα’s in 2nd line
or if any will be viable alternatives to generic methotrexate in 1st line for treatment naïve patients
• Clinical pipelines are dominated by biologics targeting cytokines, chemokines, B Cells and T Cells, and
by small molecules targeting protein kinases
- Anti-BAFF antibody (Tabalumab)
- Anti-IL-17 antibodies (Ixekizumab, Secukinumab)
- Anti-GM-CSF (Mavrilimumab, MOR-103, MT-203, MORAb-022)
- Anti-CCR1 (BMS-817399, CCX354-C)
- Anti-CXCL10 (MDX-1100)
- Anti-RANKL antibodies (Prolia, ALX-0141)
- JAK Inhibitors (Tofacitinib, Baricitinib, GLPG0634, ASP 015K)
- Syk Inhibitors (Fostamatinib, GS-9973, PRT062607)
- c-Kit Inhibitors (Masitinib, PLX-3397)
• Development of biomarkers will likely inform treatment selection for future patients
- New genetic and proteomic risk factors/biomarkers will likely help to identify patients at risk to develop RA
- Prognosis biomarkers will likely inform on disease progression of the disease, and guide treatment intensity
- Biomarkers will likely enable selection of the most suitable MoA to individual patients or subsets of patients
Emerging
Consensus

33
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations, pipeline presentations, analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight; Clinical Trials.gov; CenterWatch
In RA the late stage pipeline is crowded with cytokine Inhibitors dominating: TNF, IL-6, IL-17 and
GM-CSF are the main targets; second come kinase Inhibitors with the most advanced targeting
the JAK family; B Cells, T Cells and the complement are also important targets. (1 of 2)
RA Pipeline: Recent History
• Follow on assets abound ‐ 5 follow-on anti-TNFα’s are in development,
although 5 are currently on-market
‐ Similarly, 7 anti-IL-6 agents are in development,
following Actemra which was approved in Jan 2010
• p38 MAPK Inhibitors have not held their promises ‐ ~9 assets were discontinued in Phase II due to lack of
efficacy or safety concerns
‐ These showed only transient CRP decreases
• Chemokine receptor Inhibitors have also had
mixed clinical results: 3 CCR1 Inhibitors and
3 CCR5 Inhibitors have been discontinued ‐ CCR1 may be a better target than CCR5 in RA due to its
role in monocyte migration
‐ One CCR1 inhibitor showed no efficacy over placebo in
a clinical trial, but CCR1 remains an acceptable target
‐ A possible hurdle is ineffective dosing, leading to
inappropriate level of receptor occupancy at all times
RA Pipeline: Upcoming Catalysts
• Tofacitinib (JAK inhibitor) PDUFA in August 2012
• Fostamatinib (Syk inhibitor)
• Prolia (Anti-RANKL)
• Tabalumab (Anti-BAFF) - Since the main effect of anti-BAFF agents is B Cell
depletion, it remains to be seen their relative
advantage versus anti-CD20 antibodies, e.g. Rituxan
• Iguratimod (COX-2, IL-1, IL-6, IL-8, and TNF)
• Anti-IL-17antibodies
Rheumatoid Arthritis Pipeline: Current (N=82)
Mechanism of Action US Reg/
Phase III (N=7)
Phase II
(N=44)
Phase I
(N=31)
Cyto
kin
e
Inhib
itio
n
( N
=30)
TNF Family
Inhibition
(N=9)
Anti-TNFα (N=5) 4 1
Other (N=4) 2 2
Interleukin
Inhibition
(N=12)
Anti-IL-6 (N=7) 1 5 1
Other (N=5) 4 1
CSF Inhibition (N=5) 2 3
Chemokine
Inhibition
(N=3)
CCR1 Antagonists (N=2) 2
Anti-CXCL10 (N=1) 1
Others
(N=1) Unclear Mechanisms
1
Cell S
ignaling Inhib
itio
n
(N=22)
Kinase
Inhibition
(N=17)
JAK Inhibitors (N=9) 1 7 1
p38 MAPK Inhibitors (N=3) 2 1
Syk Inhibitors (N=3) 1 2
c-Kit Inhibitors (N=2) 1 1
NFkB Inhibitors (N=2) 2
TLR Inhibition (N=1) 1
Phosphodiesterase 4 Inhibitors (N=2) 2

34
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations, pipeline presentations, analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight; Clinical Trials.gov; CenterWatch
Rheumatoid Arthritis Pipeline: Current (N=82)
Mechanism of Action US Reg/
Phase III
(N=7)
Phase II
(N=44)
Phase I
(N=31)
B Cell Inhibition
(N=8)
Anti-CD20 (N=5) 1 2 2
Anti-BAFF (N=1) 1
Anti-CD19 (N=2) 2
T Cell Inhibition
(N=4)
Anti-CD4 (N=1) 1
Anti-CD28/CD80 (N=1) 1
Anti-CD3 (N=1) 1
CTLA4-Ig Fusion Protein (N=1) 1
Complement Inhibition (N=2) 1 1
Adhesion Inhibition (N=2) 2
Innunogenic Peptides (N=2) 2
NK Cell Modulation (N=1) 1
Others (N=12) 8 4
In RA the late stage pipeline is crowded with cytokine Inhibitors dominating: TNF, IL-6, IL-17 and
GM-CSF are the main targets; second come kinase Inhibitors with the most advanced targeting
the JAK family; B Cells, T Cells and the complement are also important targets. (2 of 2)
RA Pipeline: Recent History
• Follow on assets abound ‐ 5 follow-on anti-TNFα’s are in development,
although 5 are currently on-market
‐ Similarly, 7 anti-IL-6 agents are in development,
following Actemra which was approved in Jan 2010
• p38 MAPK Inhibitors have not held their promises ‐ ~9 assets were discontinued in Phase II due to lack of
efficacy or safety concerns
‐ These showed only transient CRP decreases
• Chemokine receptor Inhibitors have also had
mixed clinical results: 3 CCR1 Inhibitors and 3 CCR5
Inhibitors have been discontinued ‐ CCR1 may be a better target than CCR5 in RA due to its
role in monocyte migration
‐ One CCR1 inhibitor showed no efficacy over placebo in
a clinical trial, but CCR1 remains an acceptable target
‐ A possible hurdle is ineffective dosing, leading to
inappropriate level of receptor occupancy at all times
RA Pipeline: Upcoming Catalysts
• Tofacitinib (JAK inhibitor) PDUFA in August 2012
• Fostamatinib (Syk inhibitor)
• Prolia (Anti-RANKL)
• Tabalumab (Anti-BAFF) - Since the main effect of anti-BAFF agents is B Cell
depletion, it remains to be seen their relative
advantage versus anti-CD20 antibodies, e.g. Rituxan
• Iguratimod (COX-2, IL-1, IL-6, IL-8, and TNF)
• Anti-IL-17antibodies

35
Nota Bene: In this graph only, assets are double counted, in
the case of co-development partners
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations, pipeline presentations, analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight; Clinical Trials.gov; CenterWatch
As of Q1 Lumleian validated 82 assets in ‘active’ clinical development for RA: 7 in US
Regulatory/Phase III, 44 in Phase II, and 31 in Phase I; the leading sponsors are: Pfizer (5),
Bristol-Myers Squibb (5), GlaxoSmithKline (4), Ablynx (4), Novo Nordisk (4), and Eli Lilly (3).
Rheumatoid Arthritis Assets in ‘Active’ Clinical Development
Phase III (N=5) Phase II (N=44) Phase I (N=31) US Regulatory/Phase IV (N=2)
0
1
2
3
4
5
6
Pfi
zer
Bri
stol-
Myers
Squib
b
Gla
xoSm
ithKline
Ably
nx
Novo N
ord
isk
Eli L
illy
Eis
ai
Ast
raZeneca
Celg
ene
Chels
ea T
hera
peuti
cs
Am
gen
Ast
ellas
Em
erg
ent
Bio
solu
tions
Roche
AB S
cie
nce
Genm
ab
Regenero
n
Rig
el
Sanofi
Abbott
Acti
ve B
iote
ch
Am
bit
Bio
medic
al D
iagnost
ics
Bio
test
Can-F
ite
cBio
Cephalo
n
Chem
oCentr
yx
Csl
Gala
pagos
Gle
nm
ark
Pharm
a.
Imm
unom
edic
s
Incyte
Johnso
n &
Johnso
n
Lexic
on P
harm
a.
Logic
al Pharm
a.
MediG
ene
Mit
subis
hi Tanabe
Morp
hosy
s
Neovacs
Novart
is
Nuon P
harm
a.
Pir
am
al Lif
e S
cie
nces
Pro
cte
r &
Gam
ble
Synta
Pharm
aceuti
cals
UCB P
harm
aceuti
cals
Vert
ex P
harm
a.
YM
Bio
scie
nces
Oth
ers
(N
=22)

36
Cytokine Inhibitors account for the majority of pipeline assets; they target: TNF, IL-6, IL-17,
GM-CSF, M-CSF, lymphotoxin a, RANKL, IL-1, IL-13, IL-20, IL-21, IL-12/IL-23, and oncostatin M.
RA Pipeline: Current (N=82)
Mechanism of Action US Regulatory/Phase III
(N=7)
Phase II
(N=44)
Phase I
(N=31)
Cyto
kin
e
Inhib
itio
n (
N=30)
TNF Family
Inhibition
(N=9)
Anti-TNF (N=5)
• Ozoraluzimab (PFE/Ablynx) • CEP-37247 (Cephalon) • TNFα Kinoid (Biomedical
Diagnostics/ Neovacs) • Tinefcon (Piramal Life Sciences)
• PF-05230905 (Ablynx/ PFE)
Infliximab Biosimilar (N=1) • Infliximab Biosimilar (Celltrion/Lg
Life Sciences Ltd/Nippon Kayaku)
Anti-Lymphotoxin a (N=1) • RG-7416 (Roche)
Anti-RANKL (N=2) • Prolia (AMGN) • ALX-0141 (Ablynx)
Interleukin
Inhibition
(N=12)
Anti-IL-6 (N=7)
• Sarilumab (Regeneron/SNY)
• BMS-945429 (BMY) • Olokizumab (UCB Pharma) • PF-04236921 (PFE) • Sirukumab (GSK) • ALX-0061 (Ablynx)
• SA 237 (Roche/Chugai)
Anti-IL-17 (N=2) • Ixekizumab (LLY) • Secukinumab (NVS)
Anti-IL-20 (N=1) • NN8226 (NVO)
Anti-IL-21 (N=1) • NN8828 (NVO)
Anti-IL-12/IL-23 (N=1) • Apilimod Mesylate (Synta
Pharmaceuticals)
CSF
Inhibition
(N=5)
Anti-GM-CSF (N=4) • Mavrilimumab (AZN/CSL Ltd) • MOR-103 (Morphosys AG)
• MT-203 (Takeda) • MORab-022 (Eisai)
Anti-M-CSF (N=1) • PLX-5622 (Plexxikon)
Chemokine
Inhibition
(N=3)
CCR1 antagonists (N=2) • BMS-817399 (BMY) • CCX354 (Chemocentryx/ GSK)
Anti-CXCL10 (N=1) • MDX 1100 (BMY)
Other
(N=1) Unclear mechanism (N=1)
• Iguratimod/T-164 (Eisai)

37
RA Pipeline: Current (N=82)
Mechanism of Action US Regulatory/Phase III
(N=7)
Phase II
(N=44)
Phase I
(N=12)
Cell S
ignaling Inhib
itio
n (
N=21)
Kinase
Inhibition
(N=16)
JAK Inhibitors (N=8)
• Tofacitinib (PFE) • Baricitinib (Incyte/ LLY) • VX-509 (VRTX) • ASP 015K (Astellas) • GLPG0634 (Galapagos/ ABT) • AC430 (Ambit) • CYT387 (YM BioScience)
• SB1578 (S*Bio)
p38 MAPK Inhibitors (N=3) • BMS-582949 (BMY) • PG-760564 (PG)
• UR-13870 (Palau)
Syk Inhibitors (N=3) • Fostamatinib (AZN/Rigel) • GS-9973 (GILD)
• PRT062607 (BIIB/Portola)
c-Kit Inhibitors (N=2) • Masitinib (AB Science) • PLX-3397 (Plexxikon)
Transcription
Factors (N=2) NFkB Inhibitors (N=2)
• Triolex (Harbor Biosciences) • VGX-1027 (Inovio Pharmaceuticals)
TLR Inhibitor (N=1) • XToll (CBio Ltd)
Phosphodiesterase 4 Inhibitors (N=2) • Apremilast (CELG)
• Revamilast (Glenmark)
B C
ell Inhib
itors
(N=8)
Anti-CD20 Monoclonal Antibodies (N=5) • Ofatumumab (GSK /Genmab)
• Veltuzumab (Immunomedics/Takeda) • SBI-087 (S*Bio/ PFE)
• TL 011/ Rituxan biosimilar (Teva
Pharmaceuticals) • TX-RAD (TxCell)
Anti-BAFF Monoclonal Antibodies (N=1) • Tabalumab (LLY)
Anti-CD19 Monoclonal Antibody (N=2) • MDX 1342 (BMY)
• AMG729 (AMGN)
T C
ell Inhib
itors
(N
=4)
Anti-CD4 Monoclonal Antibodies (N=1) • Tregalizumab (Biotest AG)
CD28/CD80 Inhibitor (Small Molecule) (N=1) • RhuDex (MediGene/Active Biotech
AB)
Anti-CD3 Monoclonal Antibody (N=1) • Otelexizumab (GSK)
CTLA4-Ig Fusion Protein (N=1) • ASP 2408 (Astellas/ Maxygen/Perseid
Therapeutics)
B Cell Inhibitors include: anti-CD20, anti-BAFF, and anti-CD19 monoclonal antibodies, as well as
Iguratimod, whose MoA is undefined; T Cell Inhibitors include: anti-CD4 and anti-CD3 monoclonal
antibodies and Inhibitors of the CD28/CD80 interaction.

38
Mechanism of Action US Reg. / Phase III (N=7) Phase II (N=44) Phase I (N=31)
Complement Inhibitors (N=2) • MP-435 (Mitsubishi Tanabe)
• NN8209 (NVO)
Adhesion Molecule Inhibitors (N=2)
• BTT-1023 (Biotie) • SAN-300 (Santarus)
Innunogenic Peptides (N=2) • ARG301 (Argentis)
• Org39141 (Organon)
NK Cell Inhibitors (N=1) • NN8765 (NVO)
Other (N=12)
• PDA001 (CELG)
• CF101 (Can-Fite)
• LX2931 (Lexicon Pharmaceuticals)
• LT-NS001(Logical Therapeutics)
• RWJ-445380 (JNJ)
• NU3450 (Nuon Therapeutics)
• CH-1504 (Chelsea Therapeutics)
• CH-4051 (Chelsea Therapeutics)
• RPI-78 (Nutra Pharma)
• LAS-186323 (Almirall)
• RX-10001 (Resolvyx)
• MK50 (Mika Pharma)
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations, pipeline
presentations, analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight; Clinical Trials.gov; CenterWatch
A substantial number of early stage assets are pursuing more novel targets; Complement
Inhibitors target C5aR.

39
Sources: Goreschi K et al. Modulation of innate and adaptive immune responses by Tofacitinib (CP-690,550). J Immunol 2011;186:4234-4243.
JAK Inhibitors hold promise as an effective treatment for RA and have the potential to transform
the current SoC by providing once daily oral therapy; Within the JAK inhibitor class mechanistic
differences exist, but clinical relevance of JAK subtypes is still to be determined.
Physiology • Janus kinases (JAKs) bind to the intracellular portion of
some cell surface cytokine receptors
• Upon binding of the cytokine to its receptor, JAK is
activated and phosphorylates tyrosine motifs on the
receptor, creating binding sites for the Signal
Transducer and Activator of Transcription (STAT)
protein
• STAT is phosphorylated and translocated to the nucleus,
where it binds to DNA and promotes
gene transcription - In RA patients, the JAK-STAT pathway is over-stimulated by
some pro-inflammatory cytokines, including interleukins,
and GM-CSF
Hypothesized
Mechanism
• Tofacitinib inhibits both JAK3 and JAK1, which results in
the inhibition of IL-4-dependent Th2 cell
differentiation, expression of the IL-23 receptor and the
Th17 cytokines IL-17A, IL-17F, and IL-22 upon
stimulation with IL-6 and IL-23, activation of STAT1,
induction of T-bet, and subsequent generation of Th1
cells - JAK2 is crucial to red blood cell maturation; inhibition of
the enzyme results in anemia
- This might raise safety issues for the JAK1/JAK2 Inhibitors
- Some research suggests that JAK3 fails to mediate signaling
without active JAK1, though the reverse is not true
- If the data translates into the clinic, this may disadvantage
agents which are primarily JAK3 specific
Phase III • Tofacitinib (Pfizer): JAK3/JAK1
Phase II • Baricitinib (Incyte/Eli Lilly): JAK1/JAK2 • VX-509 (Vertex Pharmaceuticals): JAK3 • ASP 015K (Astellas): JAK3 • GLPG0634 (Galapagos/ Abbott): JAK1 • AC430 (Ambit): JAK2 • CYT387 (YM Biosciences): JAK1/ JAK2
Phase I • SB1578 (S*Bio): JAK2
Pipeline

40
Tofacitinib (Pfizer) is the most advanced JAK inhibitor having received a 8:2 vote in favor of
approval by the FDA Arthritis Advisory Committee meeting; 3rd line approval without a
“structural” claim is most likely; the August 2012 PDUFA will dictate near-term opportunity.
Clinical Results (Phase III: ORAL SOLO, ORAL SEQUEL)
Efficacy: • In ORAL SOLO, Tofacitinib showed a dose responsive and statistically significant improvements in ACR20/50/70 and
HAQ-DI scores compared to placebo at both doses, and in DAS28-4(ESR) at the 10 mg dose only
• In ORAL SEQUEL, the improvements in ACR20/50/70, DAS28-4(ESR), and HAQ-DI seen in the first 3 months were
maintained for the duration of the 24 months – ACR20s were 73.1-80.9%, ACR50s 47.0-57.4%, and ACR70s 24.3-35.0%
Safety: • A total of 2611 AEs were reported with the most common being infections, gastrointestinal disorders, and
musculoskeletal and connective tissue disorders; the most frequent class of SAEs was infections
• Several safety laboratory parameters were negatively influenced: total cholesterol, LDL, serum creatinine, AST,
ALT, and neutrophil count
Lumleian
Commentary:
• Tofacitinib will likely be initially approved as a 3rd line agent in anti-TNFα/Biologic IR patients without an
“Inhibition of progression of structural damage” claim and potentially also with titrated dosing
Phase III Program (ORAL SOLO; Completed) Phase II/III Program (ORAL SEQUEL, Completed)
Patient Segment: • Moderate to severe RA with inadequate prior response
to at least one DMARD
• Moderate to severe RA (rollover from prior Phase II or III
study)
Studies: • Single, double-blind, monotherapy (N=611) • Single, open-label, extension monotherapy (N=1070)
Comparator: • Placebo • Placebo
Dosing: • 5 mg or 10 mg twice a day, orally • 5 mg or 10 mg twice a day, orally
Duration: • 6 months • 24 months
Primary End-Points: • ACR20, mean change in HAQ-DI, and DAS28-
4(ESR)<2.6, all at 3 months
• Laboratory AEs and safety reports at 1, 2, and 3 months,
and each 3 months afterwards
Secondary End-Points:
• ACR50/70 and change in DAS 28 at 3 months • ACR20/50/70, DAS28-4(ESR) and HAQ-DI scores at 1, 2,
and 3 months, and each 3 months afterwards
Sources: Company press releases

41
Clinical Results (Phase III: ORAL SYNC, ORAL SCAN)
Efficacy: • ORAL SYNC met its primary efficacy endpoints
• In ORAL SCAN, ACR20 was improved at both doses at 6 months, but structural disease progression (measured as
change from baseline in mTSS) was only improved at the 10 mg dose at 6 months
Safety: • In ORAL SYNC, AE/SAE rates were similar with Tofacitinib and placebo at 3 months, but higher with Tofacitinib than
with placebo from 3-6 months; discontinuation rates were higher with Tofacitinib versus placebo from 3-6 months;
most frequent class of AEs were infections; in the Tofacitinib group there were 4 opportunistic infections, and 4
deaths, one of which was related to the study drug
• In ORAL SCAN, most frequent AEs were mild to moderate infections; the SAE rate was higher with Tofacitinib from 0-
3 months, and similar to placebo from months 3-6; there were 6 deaths, 4 on Tofacitinib 5 mg, 1 on Tofacitinib 10
mg, and 1 on placebo; increases in LDL, HDL, and serum creatinine, and decrease in neutrophil countswere observed
in the Tofacitinib groups
Lumleian
Commentary:
• Tofacitinib’s efficacy profile is viewed as similar to that of anti-TNFs, and its safety profile is viewed as comparable
to modestly worse to that of anti-TNFs
• Across Phase III, the frequency of serious adverse infection events is higher in the Tofacitinib groups than in the
Humira or placebo groups; there is some concerns about potential long-term side-effects, particularly cardiovascular
Phase III Program (ORAL SYNC; Completed) Phase III Program (ORAL SCAN; Completed)
Patient Segment: • Moderate to severe RA with inadequate prior response
to at least one DMARD
• Moderate to severe RA with inadequate prior response to
at least one DMARD
Studies: • Single, double-blind, monotherapy (N=792) • Single, double-blind, monotherapy (N=797)
Comparator: • Placebo (Background: MTX) • Placebo (Background: MTX)
Dosing: • 5 mg or 10 mg twice a day, orally • 5 mg or 10 mg twice a day, orally
Duration: • 6 months • 6 months
Primary End-Points: • HAQ-DI at 3 months
• ACR20 and DAS28-4(ESR)<2.6 at 6 months
• ACR20 at 6 months
• Structural disease progression at 6 months: radiographic
progression (total sharp score, mTSS), and erosions
Tofacitinib induces a decrease in IL-6, IL-8, MMP3, IL-17, and IFN, and an increase in IL-1; The
Phase III program includes the ORAL SOLO, ORAL SEQUEL, ORAL SYNC, ORAL SCAN, ORAL
STANDARD, and ORAL STEP studies.
Sources: Company press releases

42
Clinical Results (Phase III: ORAL STANDARD, ORAL STEP)
Efficacy: • In ORAL STANDARD, Tofacitinib showed statistically significant improvements in ACR20/50/70, HAQ-DI, and DAS28-
4(ESR) at both doses compared to placebo; these improvements were similar to those observed with Humira (NOTE:
Humira dosed once weekly has been shown to be more effective than dosed every other week)
• In ORAL STEP, Tofacitinib showed statistically significant improvements in ACR20/50/70, HAQ-DI, and DAS28-4(ESR)
at both doses compared to placebo
Safety: • In ORAL STANDARD, the frequencies of total AEs were similar in all treatment groups
• In ORAL STEP, the frequencies of total AEs were similar in the Tofacitinib and placebo groups
Lumleian
Commentary:
• Tofacitinib’s efficacy profile is viewed as similar to that of anti-TNFs, and its safety profile is viewed as comparable
to modestly worse to that of anti-TNFs
• Across Phase III, the frequency of serious adverse infection events is higher in the Tofacitinib groups than in the
Humira or placebo groups; there is some concerns about potential long-term side-effects, particularly cardiovascular
Phase III Program (ORAL STANDARD;
Completed)
Phase III Program (ORAL STEP, Completed)
Patient Segment: • Moderate to severe RA with inadequate prior response
to at least one DMARD
• Moderate to severe RA patients on a stable dose of MTX
and prior TNF inhibitor failure
Studies: • Randomized, double-blind, (N=717) • Randomized, double-blind, (N=399)
Comparator: • Humira (40 mg, SQ, Q2W)
• Placebo
• Placebo (background: MTX)
Dosing: • 5 mg or 10 mg twice a day, orally • 5 mg or 10 mg twice a day, orally
Duration: • 6 months • 6 months
Primary End-Points: • HAQ-DI at 3 months
• ACR20 and DAS28-4(ESR)<2.6 at 6 months
• Laboratory AEs and safety reports at 1, 2, and 3 months,
and each 3 months afterwards
Tofacitinib was shown in the Oral Standard trial to be comparable to Abbott’s Humira in treating
rheumatoid arthritis, but was associated with a higher rate of serious adverse events.
Sources: Company press releases

43
Baricitinib (Lilly/Incycte) is an oral small molecule that inhibits JAK1/JAK2 with critical 3 month
data from the Phase II trial anticipated to be released at EULAR in June, and 6 month data at
ACR in November 2012.
Clinical Results (Phase IIa)
Efficacy: • ACR20/50/70 were achieved in 59%/35%/16% of Baricitinib-treated patients vs. 32%/13%/3% of placebo-treated
patients at 3 months, and ACR20/50/70 rates incrementally increased to 72%/44%/30% at 6 months
Safety: • AEs were predominantly mild and moderate with rates similar to those observed on placebo
Lumleian
Commentary:
• Baricitinib has a level of efficacy similar to that of other biologics
• Safety might be a concern with longer-term dosing, particularly because of dose-related decreases in mean Hb,
increases in LDL levels, and several cases of uncomplicated Herpes Zoster infection
Phase IIa Program (Completed) Phase IIb Program (Ongoing)
Patient Segment: • Moderate to severe RA with inadequate prior response
to DMARDs, including biologic DMARDs
• Moderate to severe RA patients on background MTX
therapy
Studies: • Randomized, double-blind, placebo-controlled (N=125) • Randomized, double-blind, placebo-controlled (N=270)
Comparator: • Placebo • Placebo
Dosing: • 4, 7, and 10 mg once daily, orally • 4 mg and 8 mg, once or twice daily, orally
Duration: • 6 months • 12 weeks, then a 12-week extension, then an optional 52-
week open-label extension, and a 28-day follow up
Primary End-Points: • ACR20 response rates at 3 months
• Safety and tolerability as measured by AEs, vital signs,
clinical laboratory tests, and ECGs at 3 months
• ACR20 response rates at 12 weeks
Secondary End-Points:
• ACR20/50/70/90 response rates at 6 months
• Safety and tolerability as measured by AEs, vital signs,
clinical laboratory tests, and ECGs at 6 months
• ACR20/50/70/90 response rates at 2, 4, 8, 12, 14, 16, 20,
and 24 weeks; mean CRP, HAQ-DI, and DAS28 at 12 and
24 weeks; additional pain and stiffness criteria
Sources: Company press releases

44
VX-509 (VRTX) is a JAK3 inhibitor that has provided efficacy proof-of-concept, a Phase IIb study
in combination with methotrexate expected to begin in 1H 2012.
Clinical Results (Phase IIa)
Efficacy: • The study met its two primary endpoints, defined as a statistically significant improvement in the proportion of
people who achieved at least an ACR20, and a statistically significant improvement from baseline in DAS28
• For the two highest dose groups, statistically significant improvements in ACR20/50/70 and DAS28 responses were
observed over placebo, and >1/3 of patients in these groups achieved clinical remission (DAS28 remission)
Safety: • At least 80% of patients in VX-509 treatment group vs. 68% in the placebo group completed the 12-week treatment
course; most frequent class of AEs was infections (17% VX-509, 17% placebo); most frequent individual AEs were
nausea (6% VX-509, 0% placebo), ALT increase (4% VX-509, 5% placebo), and headache (4% VX-509, 5% placebo)
• Dose-related low-grade HDL and LDL increases were observed in VX-509-treated patients
• SAEs occurred in 2% of placebo-treated patients vs. 0%, 2%, 13%, and 5% of VX-509-treated patients in the 25, 50,
100, and 150 mg groups, respectively; in the 100 mg dose group, one patient died of a hemorrhagic stroke, reported
as unrelated to VX-509, and one patient died of pneumonia
Lumleian
Commentary:
• The data provide proof-of-concept for VX-509’s efficacy, but the safety profile remains in question
• A 6-month Phase IIb study of VX-509 in combination with MTX is expected to begin in early 2012
Phase IIa Program (Completed)
Patient Segment: • Moderate to severe RA with inadequate prior response to at least one non-biologic DMARD
Studies: • Randomized, double-blind, placebo-controlled Phase II (N=204)
Comparator: • Placebo
Dosing: • 25, 50, 100, or 150 mg twice a day, orally
Duration: • 12 weeks
Primary End-Points: • ACR20 response rates, change from baseline in DAS28 at 12 weeks
Secondary End-Points:
• ACR50/70 rates, moderate to good EULAR response rates, and magnitude of improvement in ACR response at 12
weeks, and PK and PD at 6 weeks
Sources: Company press releases

45
In February this year, Galapagos licensed GLPG0634, a JAK1 inhibitor, to Abbott for $150M
upfront, with the potential for significant milestone payments; ACR20 results were impressive.
Clinical Results (Phase II)
Efficacy: • GLPG0634 achieved the primary endpoint of significant improvement in the signs and symptoms of RA; overall,
ACR20/50/70 were achieved by 83%/42%/21% of GLPG0634-treated patients vs. 30%/8%/0% of placebo-treated
patients; half of treated patients went into remission or showed a low disease activity
• GLPG0634 also showed impressive results in DAS28 scores, and CRP levels
Safety: • A GLPG0634 was well-tolerated, with all patients completing the trial and no safety signals reported; no anemia or
increases in lipids (LDL or cholesterol) were observed in this trial although there were modest decreases in platelets
and neutrophils; no SAEs were reported in patients receiving GLPG0634
Lumleian
Commentary:
• The long-term efficacy and safety remain to be established
• ACR20 response rates re impressive
Phase II Program (Completed)
Patient Segment: • Active RA despite methotrexate treatment
Studies: • Randomized, double-blind, placebo-controlled Phase II (N=36)
Comparator: • Placebo
Dosing: • 100 mg twice a day, or 200 mg once a day, orally
Duration: • 4 weeks
Primary End-Points: • ACR20 response rates at 4 weeks
Secondary End-
Points:
• ACR20/50/70 response rates, time to response, and DAS28 score at every visit as a measure of efficacy
• Number of patients with AEs, abnormal lab tests, vital signs, and ECG as a measure of safety and tolerability
• Plasma levels of GLPG0634 as a measure of PK, and levels of immune- and inflammation-related parameters in blood
as a measure of PD
Sources: Company press releases

46
Sources: Yazici Y and Regens AL. Promising new treatments for rheumatoid arthritis. Bull NYU Hosp Jt Dis 2011;69:233-237; Braselmann S et al. R406, an
orally available spleen tyrosine kinase inhibitor blocks Fc receptor signaling and reduces immune complex-mediated inflammation. J Pharmacol Exp Ther
2006; 319:998-1008
Syk Inhibitors may provide a double benefit in RA treatment by not only controlling inflammation,
but also by slowing bone resorption by osteoclasts; Clinical results are promising in attractive
earlier treatment lines; Biogen Idec licensed Portola’s PRT062607 for $36M upfront.
Physiology • Syk is a cytoplasmic tyrosine kinase involved in
signaling and in the activation of Fcg receptors (FcRg)
on macrophages, neutrophils, and mast cells; Syk binds
to immunoreceptor tyrosine-based activation motifs
(ITAMs) located in the cytoplasmic tail of FcRg; this
leads to up-regulation of TNFa, IL-6 and matrix
metaloproteinases (MMPs) - In RA patients, autoantibodies and immune complexes
engage and activate FcR signaling in macrophages,
neutrophils, dendritic cells, and mast cells
Hypothesized
Mechanism
• Blocks the FcR signaling pathway - Syk Inhibitors potently inhibit immunoglobulin (Ig)E- and
IgG-mediated activation of Fc receptor signaling; It inhibits
the ITAM-dependent signaling by the Fc receptor
complexes in macrophages, neutrophils and mast cells,
and the ITAM-dependent signaling from the B Cell receptor
Phase III • Fostamatinib (AstraZeneca/Rigel Pharmaceuticals)
Phase I • GS-9973 (Gilead Sciences) • PRT062607 (Biogen Idec/Portola Pharmaceuticals)
Pipeline

47
Fostamatinib, an orally active small molecule Spleen Tyrosine Kinase (Syk) inhibitor, is in Phase
III development for the treatment of moderate to severe RA; Although safe, this drug has not
proven to be effective in patients with an inadequate response to biologic DMARDs (TASKi3).
Clinical Results (Phase IIa and TASKi2)
Efficacy: • Fostamatinib met both primary and secondary end-points at the doses of 100 and 150 mg; ACR20/50/70 were
achieved by 72%/57%/40% of patients on 150 mg fostamatinib vs. 18%/9%/2% of patients on placebo
• In TASKi2, both fostamatinib doses met the primary and secondary end-points
Safety: • In the 150 mg fostamatinib group, 47% of patients had moderate to severe GI symptoms, 21% had neutropenia lasting
one month, and 6% had ALT elevations greater than 3x normal; based on this, Rigel has discontinued the
development of 150 mg twice daily; in the 100 mg fostamatinib group, 9% had moderate to severe GI symptoms, 11%
had neutropenia lasting one month, and 4% had moderate to severe hypertension
• In TASKi2, AEs included diarrhea, transient neutropenia, elevations in ALT, and increase in blood pressure that
required adjustments or initiation of blood pressure medication in 23% of patients on 100 mg fostamitinib and 18% of
patients on 150 fostamitinib vs. 7% of patients on placebo
Lumleian
Commentary:
• Fostamatinib shows robust efficacy, but there is concern with several safety signals including infection, diarrhea,
high blood pressure/hypertension, neutropenia, and elevation in liver enzymes; potential tumor risk with long-term
use due to the tumor suppressor activity of Syk might also require close monitoring
Phase II Program (Phase IIa, Completed) Phase IIb Program (TASKi2, Completed)
Patient Segment: • Moderate to severe RA patients • Moderate to severe RA patients failing to respond
to methotrexate
Studies: • Randomized, double-blind, (N=189) • Randomized, double-blind, (N=457)
Comparator: • Placebo (background: MTX) • Placebo (background: MTX)
Dosing: • 50, 100, or 150 mg twice a day, orally • 100 twice a day or 150 mg once a day, orally
Duration: • 12 weeks • 6 months
Primary End-Points: • ACR20 • ACR20 response rates at 6 months
Secondary End-Points:
• ACR50/70 and DAS28<2.6 • ACR50/70, DAS28-CRP, and DAS28-ESR at 6 months
• FACIT-fatigue and SF-36 from baseline to 6 months
• Safety: liver function, neutrophils, GI side-effects
Sources: Company press releases

48
Clinical Results (Phase IIb: TASKi3)
Efficacy: • In TASKi3, fostamatinib missed both the primary and secondary end-points, which was attributed to unusually high
placebo response rates, and lack of response of patients with elevated ESR and normal baseline CRP levels
Safety: • In TASKi3, most common AEs were infection,diarrhea, and hypertension; AEs such as neutropenia, GI AEs,
hypertension/high blood pressure, and elevations in liver enzymes required fostamatinib dose reductions
Lumleian
Commentary:
• Fostamatinib shows robust efficacy, but there is concern with several safety signals including infection, diarrhea,
high blood pressure/hypertension, neutropenia, and elevation in liver enzymes; potential tumor risk with long-term
use due to the tumor suppressor activity of Syk might also require close monitoring
Phase IIb Program (TASKi3, Completed) Phase III Program (OSKIRA-1, -2, -3, Ongoing)
Patient Segment: • Moderate to severe RA patients who have
failed at least one biologic
• Moderate to severe RA patients who are: - MTX inadequate responders (OSKIRA-1)
- DMARD inadequate responders (OSKIRA-2)
- on MTX and anti-TNF refractory (OSKIRA-3)
Studies: • Randomized, double-blind, (N=219) • Randomized, double-blind, (N=900, OSKIRA-1 and -2;
N=450, OSKIRA-3)
Comparator: • Placebo (background: non-biologic DMARD) • Placebo
Dosing: • 100 mg twice a day, orally • 100 mg twice a day and 150 mg once a day, orally
Duration: • 3 months • 6 months
Primary End-Points: • ACR20 response rates at 3 months • ACR20 (OSKIRA-1, -2, -3) and mTSS (OSKIRA-1) at 6 mo.
Secondary End-Points:
• ACR50/70, ACRn, DAS28-CRP, DAS28-ESR at 3 months
• FACIT-fatigue and SF-36 from baseline to 3 months
• Radiologic response (MRI) using the modified RAMRIS
scoring system of hands and wrists (baseline, Month 3)
• Safety: liver function, neutrophils, GI side-effects
Fostamatinib completed its Phase II program for the treatment of moderate to severe RA; it
included 3 trials: a Phase IIa study, TASKi2, and TASKi3; In TASKi3, fostamatinib missed both the
primary and secondary end-point which was attributed to unusually high placebo response rates.
Sources: Company press releases

49
Sources: Tebbib J et al. Masitinib in the treatment of active rheumatoid arthritis: results of a multicentre, open-label, dose-ranging, phase 2a study.
Arthritis Res Ther 2009;11:R9
The receptor tyrosine kinase c-Kit plays a major role in the survival and activation of mast cells
which both blocks TNF signaling and recruitment of other inflammatory cell types; a different
approach from current RA therapy with potential for synergistic efficacy with other products.
Physiology • c-Kit is a receptor tyrosine kinase whose ligand is the
stem cell factor (SCF); mast cells are the only
terminally differentiated hematopoietic cells that
express the c-Kit receptor
• c-Kit is also expressed in hematopoietic stem cells,
melanocytes, germ cells, and hematopoietic
progenitor cells including erythroblasts, myeloblasts,
and megakaryocytes
• Interaction of SCF with c-Kit promotes mast cell
adhesion, migration, proliferation, and survival
• Mast cells produce factors that regulate lymphocyte
migration, angiogenesis, inflammation, and cartilage
and bone destruction - In RA patients, the percentage of mast cells in the
synovium is increased, and mast cells are observed at the
cartilage-pannus junction, near blood vessels, and in areas
of fibrosis
Hypothesized
Mechanism
• Inhibits mast cell activation by preventing the c-
Kit/SCF interaction
Phase III • Masitinib (3AB Science)
Phase I • PLX-3397 (Plexxikon)
Pipeline

50
Orally available Masitinib targets mast cells via the inhibition of the tyrosine kinase c-Kit
(CD117) and lyn; AB’s go-to-market strategy for Masitinib was to first gain approval in animal
health for canine mast cell tumors; High AE rates and withdrawal rates are notable.
Clinical Results (Phase IIa)
Efficacy: • Improvement was observed in all efficacy endpoints, including ACR20/50/70 scores of 54%, 26% and 8%,
respectively, and a reduction in CRP level by greater than 50% for approximately half the population
• This improvement was sustainable throughout an extension phase (> 84 weeks) and was also independent
of initial DMARD resistance
Safety: • A relatively high patient withdrawal rate (37%) required the use of last observation carried forward (LOCF) data
imputation
• Incidence of AEs was high (95%), although the majority were mild or moderate in severity with a considerable
decline in frequency observed after 12 weeks of treatment; 2 nonfatal SAEs were reported
Lumleian
Commentary:
• Incidence of adverse events was high (95%), and 31% of patients withdrew before the 12-week endpoint due to AEs;
most AEs were mild or moderate; AEs included rash (30%), edema (26%), nausea (23%) and diarrhea (18.6%); in 21%
of patients, AEs were severe
Phase IIa Program (Completed) Phase IIb/III Program (Ongoing)
Patient Segment: • Active RA patients with inadequate response to at
least one DMARD, including MTX or anti-TNF
• Active RA patients with inadequate response to MTX, any
DMARD including at least one biologic drug if patients
previously failed MTX, or MTX in combination with any
DMARD including biologic drugs
Studies: • Randomized, open-labeled, (N=43) • Randomized, double-blind, (N=450)
Comparator: • MTX
Dosing: • 3 or 6 mg/kg once daily • 3 or 6 mg/kg once daily
Duration: • 3 months • 24 weeks with possible extension
Primary End-Points: • ACR20/50/70/90 at 12 weeks • ACR50 at 24 weeks
Secondary End-Points:
• DAS28, ACRn, and improvement of quality of life
assessed by SF12 at 12 weeks
Sources: Company press releases

51
Sources: Moisin I and Davidson A. BAFF: a local and systemic target in autoimmune diseases. Clin Exp Immunol 2009;158:155-63
IV delivered, anti-BAFF agents offer an alternative approach to B Cell depletion vs. Rituxan;
B Cell depletion is thought to restore immune tolerance and provide sustained benefit over 18+
months post treatment.
Physiology • The B Cell activating factor (BAFF) is a homotrimer of
the TNF superfamily expressed on the surface of
monocytes, dendritic cells, neutrophils, stromal cells,
activated T Cells, malignant B Cells, and epithelial cells ‐ Most of the expressed BAFF is cleaved and circulates
in a soluble form
• BAFF plays a key role in B Cell survival, maturation, and
activation through its interaction with its receptors
TACI, BAFF-R, and BCMA - In RA patients, serum levels of BAFF are increased
- Pathologic concentrations of BAFF are thought to overcome
the negative selection of autoreactive B Cells
in the periphery; autoreactive B Cells then survive and
produce self-reactive antibodies
Hypothesized
Mechanism
• Reduces the concentration of circulating BAFF through
interaction with BAFF - Targeting of BAFF in patients with RA results in prompt
depletion of transitional and naive B Cells, with sparing
of memory B Cells and plasma cells, and only modest
reductions in serum Ig levels
Pipeline
Phase III • Tabalumab (Eli Lilly)

52
Clinical Results (Phase II)
Efficacy: • Tabalumab met the primary end-point at all 3 doses: ACR20 was achieved in 69.7% of patients on 30 mg, 67.6% of
patients on 60 mg, and 63.6% of patients on 160 mg vs. 26.5% of patients on placebo
• B Cell (except memory B Cells) were partially depleted: CD20+ B Cell counts decreased by 33.3% (160 mg) vs. 18.3%
(placebo), and IgD+CD27- B Cell counts by 63.6% (160 mg) vs. 17.7% (placebo) at 24 weeks
Safety: • The nature and frequency of AEs were similar across groups; serious AEs were reported in 5 (4.9%) Tabalumab
treated patients and 3 (9.1%) placebo-treated patients; serious infection was reported in 1 (1.0%) Tabalumab
treated patient and 1 (3.0%) placebo-treated patient; IgM (but not IgG or IgA) levels decreased significantly more
in all Tabalumab groups combined than in the placebo group
Lumleian
Commentary:
• Clinical trials of Belimumab in RA were confirmed to be terminated in June 2011. This was cited as being the
sponsors decision, not related to safety.
Phase II Program (Completed) Phase III Program (Ongoing)
Patient Segment: • Patients with active RA despite ongoing MTX therapy • Anti-TNF refractory RA patients (FLEX V)
• RA patients on background DMARD or not (FLEX O)
• RA patients on background MTX (FLEV M)
Studies: • Randomized, double-blind, placebo-controlled, dose-
ranging Phase II (N=136)
• Randomized, double-blind, (FLEX V, O, M)
• Open-labeled, long-term safety and efficacy
Comparator: • Placebo (background: MTX) • Placebo (FLEX V, O, M)
Dosing: • 30, 60, 120 mg IV, every 3 weeks for a total of 3 doses • 90 mg every 2 weeks, or 120 mg every 4 weeks, IV
Duration: • 24 weeks • 24 weeks (FLEX V, O); 52 weeks blinded, then 48 weeks
unblinded (FLEX M); 240 weeks
Primary End-Points: • ACR20 response rates at 24 weeks • ACR20 (FLEX V, O, M), HAQ-DI and mTSS (FLEX M)
• Anti-LY2127399 antibodies, B Cells, Ig levels
Secondary End-Points: • Safety through evaluation of laboratory tests, vital signs
and ECG; PK through blood sample collections
• ACR50/70, DAS28, CRP, B Cells, Ig, antibodies, PK
Tabalumab is a fully human anti-BAFF monoclonal antibody that binds both surface and soluble
BAFF; In Phase III it currently remains the only anti-BAFF in development since GSK/ HGSI’s RA
program for Belimumab was terminated by decision of the sponsor (unrelated to safety).
Sources: Company press releases

53
RANKL is thought to be involved in immune activation of osteoclasts resulting in bone
resorption; anti-RANKL agents reduce the progression of bone erosion without affecting
markers of inflammatory disease activity; they do not reduce pain symptoms.
Physiology • Receptor activator of nuclear factor-kB (RANK) ligand
(RANKL), a protein that binds to RANK, is the primary
mediator of bone resorption
• RANKL/RANK interaction activates a cellular signaling
that mediates the differentiation, activation, and
survival of osteoclasts.
• Osteoprotegerin (OPG) provides an alternative binding
site for RANKL and acts as a decoy receptor by blocking
RANKL/RANK interaction
• When RANKL is bound and neutralized by OPG,
osteoclasts cannot form, function, or survive, and bone
resorption is inhibited. - Articular bone erosions by osteoclasts are a characteristic
feature of RA, and destruction of articular bone is
associated with significant morbidity and poor prognosis
Hypothesized
Mechanism
• Inhibits RANKL/RANK interaction by mimicking the
binding of OPG to RANKL
Pipeline
Phase II • Prolia (Abbott/Biotest)
Phase I • ALX-0141 (Ablynx)
Sources: Pettit AR et al. RANKL protein is expressed at the pannus–bone interface at sites of articular bone erosion in rheumatoid arthritis. Rheumatology
2006;45:1068–1076; Josse RG. The role of RANK/RANKL/OPG pathway in bone loss: new insights. Conference Report from the 2009 CGS Annual Scientific
Meeting: Satellite Symposium

54
Prolia is an anti-RANKL humanized monoclonal antibody that is targeting the bone
manifestations of RA; In Phase II trials it significantly reduced the increase in bone erosion
score, and modified sharp erosion score at both 6 months and 12 months versus placebo.
Clinical Results (Phase II)
Efficacy: • Prolia at both doses statistically significantly reduced the increase in bone erosion score, and modified sharp erosion
score at both 6 months and 12 months versus placebo
• Prolia did not impact joint space narrowing, or measures of RA activity
• Prolia has a rapid onset of action (12-24 hours), a durable effect (out to 4+ years), and is reversible upon
discontinuation of therapy
Safety: • Side effects were similar across the three arms
Lumleian
Commentary:
• Prolia is likely to decrease the degree of structural damage, but may have a limited impact on the progression of
erosion associated with inflammation, because it is not an immunosuppressant; It will likely be adjunctive
Phase II Program (Completed)
Patient Segment: • RA patients on MTX
Studies: • Randomized, double-blind, placebo-controlled Phase II (N=218)
Comparator: • Placebo
Dosing: • 60 mg or 180 mg every 6 months, SQ
Duration: • 1 year
Primary End-Points: • Change in baseline erosion score (MRI) at 6 months
Secondary End-
Points:
• AEs, laboratory analytes and anti-denosumab antibodies at 24 months
• Change in mTSS, radiographic erosion score (ES) and radiographic joint space narrowing score (JS) at 24 months
• Percent changes in lumbar spine, total hip and proximal femur bone mass density at 24 months
• Percent changes in bone (serum Type I C-terminal telopeptide of type I collagen (CTX) and procollagen type I N
propeptide (PINP)), and cartilage (urine Type II CTX/creatinine) markers at 24 months
Sources: Company press releases

55
Sources: Szekanecz Z et al. Chemokine and chemokine receptor blockade in arthritis, a prototype of immune-mediated inflammatory diseases.
Neth J Med 2011;69:356-66.
Once promising, the clinical targeting of the chemokine receptors CCR1 and CCR5 has been
disappointing; however, three chemokine-targeting assets are still being developed in Phase II:
two target CCR1, and one targets the chemokine CXCL10.
Physiology • Chemokines and their receptors can promote
leukocyte migration at sites of inflammation - In RA, leukocyte extravasation into the synovium occurs
through the vascular endothelium, via a process that
involves certain chemokines and their receptors
- CXCL10 is abundantly expressed in the sera, and synovial
fluid and tissues of RA patients; CXCL10 inhibits synovial
neovascularisation, and has a proinflammatory action
- CCR1 is a receptor for the chemokines CCL3, CCL5,
CCL7, CCL14, CCL15, and CCL16, which have been
implicated in the pathogenesis of RA
- In RA patients, CCR1-expressing monocytes and
macrophages are found at high levels in the synovium;
the C6 superagonists of CCR1 (activated highly potent
forms of certain CCR1 ligands) are detected at high
levels in synovial fluids; CCR1 may mediate osteoclast
formation
Hypothesized
Mechanism
• Inhibit leukocyte recruitment into the synovium
Potential
considerations
• 3 CCR1 Inhibitors and 3 CCR5 Inhibitors were
discontinued for lack of efficacy in RA, including
Pfizer’s HIV drug Maraviroc (CCR5 antagonist)
• CCR1 may be a better target than CCR5 in RA, due to
its role in monocyte migration
Pipeline
Phase II • BMS-817399 (Bristol-Myers Squibb)
• CCX354-C
(ChemoCentryx/GlaxoSmithKline)
• MDX-1100 (Bristol-Myers Squibb)

56
Clinical Results (Phase II)
Efficacy: • ACR20 response rate was significantly higher in MDX-1100 group than in placebo group (54% vs. 17%; P=0.0024)
• ACR50/70 response rates in MDX-1100 treatment group at Day 85 were not significantly different from placebo
Safety: • Overall, 51.4% of MDX-1100-treated patients and 30.3% of placebo-treated patients experienced at least 1 AE; no
drug-related serious AEs were reported
Lumleian
Commentary:
• MDX-1100 was well tolerated and demonstrated clinical activity in RA patients who had an inadequate response to MTX
• This is the first study to demonstrate clinical activity of a chemokine inhibitor in RA and supports the potential role of CXCL10 in
the immunopathogenesis of RA
Phase II Program (Completed)
Patient Segment: • Patients with active RA receiving MTX
Studies: • Randomized, double-blind, placebo-controlled Phase II (N=70)
Comparator: • Placebo
Dosing: • 10 mg/kg administered IV over 60 minutes every other week, in combination with MTX (10-25 mg weekly)
Duration: • 85 days
Primary End-Points: • ACR20 response rate at day 85
Secondary End-
Points:
• Safety and tolerability monitored by physical exam, laboratory tests, ECGs, chest X-ray, and AEs over 141 days
MDX-1100 is an anti-CXCL10 monoclonal antibody that has completed its Phase II Program; ACR20
response rate was moderate (54%) and ACR50/70 response rates were not statistically significant
versus placebo.
Sources: Company press releases; Yellin M et al. A phase II, randomized, double-blind, placebo-controlled study evaluating the efficacy and safety of MDX-
1100, a fully human anti-CXCL10 monoclonal antibody, in combination with methotrexate in patients with rheumatoid arthritis. Arthritis Rheum
2011;DOI: 10.1002/art.34330
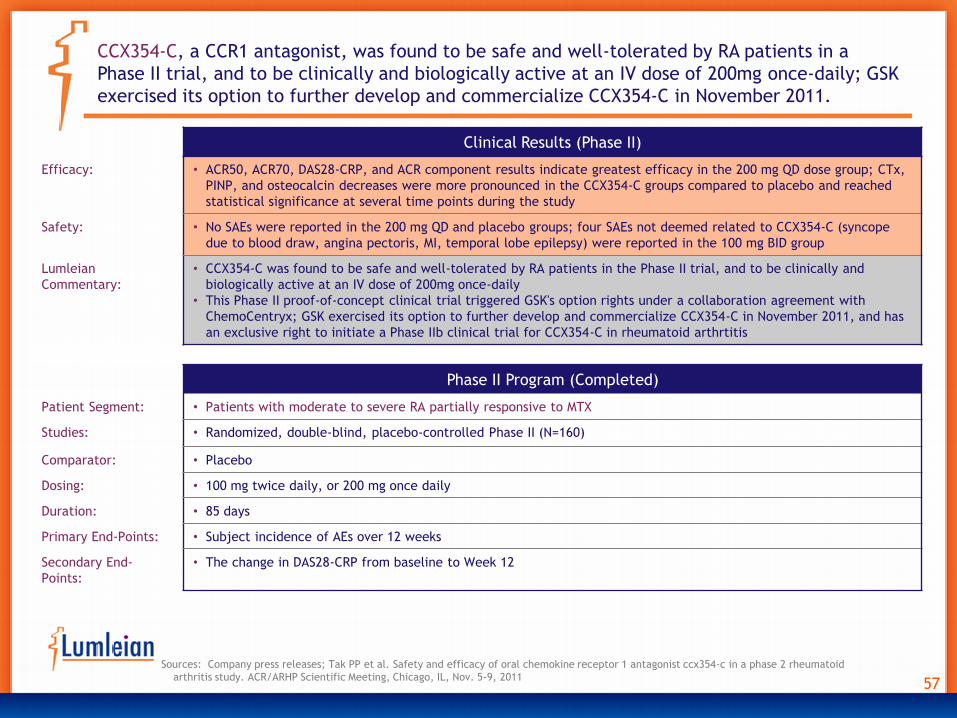
57
Clinical Results (Phase II)
Efficacy: • ACR50, ACR70, DAS28-CRP, and ACR component results indicate greatest efficacy in the 200 mg QD dose group; CTx,
PINP, and osteocalcin decreases were more pronounced in the CCX354-C groups compared to placebo and reached
statistical significance at several time points during the study
Safety: • No SAEs were reported in the 200 mg QD and placebo groups; four SAEs not deemed related to CCX354-C (syncope
due to blood draw, angina pectoris, MI, temporal lobe epilepsy) were reported in the 100 mg BID group
Lumleian
Commentary:
• CCX354-C was found to be safe and well-tolerated by RA patients in the Phase II trial, and to be clinically and
biologically active at an IV dose of 200mg once-daily
• This Phase II proof-of-concept clinical trial triggered GSK's option rights under a collaboration agreement with
ChemoCentryx; GSK exercised its option to further develop and commercialize CCX354-C in November 2011, and has
an exclusive right to initiate a Phase IIb clinical trial for CCX354-C in rheumatoid arthrtitis
Phase II Program (Completed)
Patient Segment: • Patients with moderate to severe RA partially responsive to MTX
Studies: • Randomized, double-blind, placebo-controlled Phase II (N=160)
Comparator: • Placebo
Dosing: • 100 mg twice daily, or 200 mg once daily
Duration: • 85 days
Primary End-Points: • Subject incidence of AEs over 12 weeks
Secondary End-
Points:
• The change in DAS28-CRP from baseline to Week 12
CCX354-C, a CCR1 antagonist, was found to be safe and well-tolerated by RA patients in a
Phase II trial, and to be clinically and biologically active at an IV dose of 200mg once-daily; GSK
exercised its option to further develop and commercialize CCX354-C in November 2011.
Sources: Company press releases; Tak PP et al. Safety and efficacy of oral chemokine receptor 1 antagonist ccx354-c in a phase 2 rheumatoid
arthritis study. ACR/ARHP Scientific Meeting, Chicago, IL, Nov. 5-9, 2011

58
Sources: Burmester GR et al. Mavrilimumab, a human monoclonal antibody targeting GM-CSF receptor-α, in subjects with rheumatoid arthritis: a
randomised, double-blind, placebo-controlled, phase I, first-in-human study. Ann Rheum Dis 2011;70:1542-1549
Targeting of the GM-CSF/GM-CSFR interaction is a novel strategy in treating rheumatoid
arthritis; the leading agent, AstraZeneca’s mavrilimumab, has achieved positive interim
phase II results with an attractive safety profile.
Physiology • Granulocyte-macrophage colony-stimulating factor
(GM-CSF) is a soluble cytokine that binds to GM-CSFR;
GM-CSF/GM-CSFR interaction promotes the generation,
survival, and activation of neutrophils, eosinophils,
and macrophages, and regulates numerous functions of
mature tissue macrophages: cell adhesion, expression
of pathogen recognition receptors, expression of the
proinflammatory cytokines TNFa, IL-6, IL-12, IL-18,
MCP-1 and M-CSF; phagocytosis, and microbial killing;
GM-CSF is also critical in maintaining the ability of
pulmonary alveolar macrophages to clearsurfactant
lipid and proteins from the lung surface - In RA patients, levels of GM-CSF and GM-CSFR are
increased in the synovial fluid and plasma
- Administration of recombinant GM-CSF to Felty’s syndrome
patients can induce arthritic flares
Hypothesized
Mechanism
• Suppresses macrophage activity by blocking the
interaction between GM-CSF and GM-CSFR - Mavrilimumab was well tolerated and showed efficacy in
RA patients, and there were few safety signals
- Main adverse events associated with mavrilimumab were a
decrease in carbon monoxide diffusing capacity,
nasopharyngitis, and upper respiratory infections
- MOR-103 (Phase II) and MT-203 and MORAb-022 (Phase I)
are monoclonal antibodies directed against GM-CSF
Pipeline
Phase II • Mavrilimumab (AstraZeneca/Csl Ltd.) • MOR-103 (Morphosys AG)
Phase I
• MORAb-022 (Eisai) • MT-203 (Takeda)

59
Clinical Results (Phase II)
Efficacy: • 55.7% of mavrilimumab subjects met the primary endpoint vs. 34.7% in the combined placebo group (P=0.003)
• The 100 mg mavrilimumab group showed significant improvement compared with placebo in the primary (P=0.001),
and secondary endpoints (P<0.05)
• The onset of response generally occurred within 2 wks
Safety: • AEs were generally mild or moderate in intensity; the most common AEs were decrease in carbon monoxide
diffusing capacity (placebo 5.1%; mavrilimumab 11.9%), nasopharyngitis (placebo 2.5%; mavrilimumab 6.3%) and
upper respiratory tract infections (placebo 5.1%; mavrilimumab 3.8%); no significant hypersensitivity reactions,
serious or opportunistic infections, or changes in pulmonary parameters were reported; SAEs were reported in 1.3%
of placebo-treated and 1.9% of mavrilimumab-treated subjects, and were not treatment related
Phase II Program (Ongoing)
Patient Segment: • Patients with moderate to severe RA
Studies: • Randomized, double-blind, placebo-controled Phase II (N=233)
Comparator: • Placebo
Dosing: • 10, 30, 50, or 100 mg every other week, SQ
Duration: • 12 weeks
Primary End-Points: • DAS28-CRP decrease ≥1.2 from baseline at 12 weeks
Secondary End-Points: • DAS28-CRP remission, ACR20/50/70, and HAQ-DI
Mavrilimumab is an anti-GM-CSFR monoclonal antibody; positive intermediate results of an
ongoing Phase II trial were reported in November 2011.
Sources: Company press releases

60
Sources: Genovese M et al. s . One Year Efficacy And Safety Results Of A Phase Ii Trial Of Secukinumab In Patients With Rheumatoid Arthritis. Arthritis
Rheum 2011;63 Suppl10:401; Genovese M et al. Ixekizumab, a humanized anti–interleukin-17 monoclonal antibody, in the treatment of patients with
rheumatoid arthritis. Arthritis Rheum 2010;62:929-939
Two anti-IL-17 monoclonal antibodies are being developed, currently in Phase II; they both show
efficacy and limited safety concerns in rheumatoid arthritis patients.
Physiology • IL-17 is a proinflammatory cytokine produced primarily
by CD4+ T helper (Th) 17 cells; IL-17 provides immunity
to bacteria, fungi, and some other pathogens through
generation and reruitment of neutrophils - In RA patients, serum and synovial fluid levels of IL-17 are
elevated; RA synovial tissue explants produce biologically
active IL-17; a subset of infiltrating T Cells expressing IL-
17 has been identified in RA synovium
- IL-17 could contribute to the pathogenesis of RA in synergy
with TNFa and IL-1b, and independently from these
cytokines
Hypothesized
Mechanism
• Neutralizes the biologic effects of IL-17 - Secukinumab showed efficacy in active RA patients on MTX
over a 24-week period and a safety profile comparable to
placebo in a Phase IIb trial
- Ixekizumab was tolerated and showed efficacy in RA
patients over a 10-week period; there were few safety
signals, although leukopenia and neutropenia would
require monitoring in future trials
- Amgen had completed a Phase II trial to assess the efficacy
of the IL-17 antibody AMG-827 in RA subjects with
inadequate response to MTX, but announced in April 2011
that it was stopping that clinical program
Pipeline
Phase II • Ixekizumab (Eli Lilly)
• Secukinumab/AIN457 (Novartis)

61
Clinical Results (Phase II)
Efficacy: • ACR20 responder rates at Week 16 were higher with secukinumab 75mg, 150mg and 300mg (47%, 47% and 54%,
respectively) versus placebo (36%) but did not reach statistical significance
• Responders on secukinumab maintained their ACR20 response from Week 24 to 52; improvement in ACR20 response
rates at weeks 24 and 52 were seen in patients who remained on secukinumab 150mg for the entire study; through
Week 52, responders who remained on secukinumab 150mg had further improvement in ACR50/70
• Non-responders did not gain much additional efficacy benefit after dose escalation as assessed by ACR20/50/70 and
DAS28-CRP
Safety: • AE rates were similar at Week 20 and Week 52 (60-70%); most AEs were mild to moderate in severity and did not lead
to study discontinuation (6.9%); the rate of infections was 31.9% overall; 9.7% of SAEs were reported including 6 cases
of serious infections without dose relationship; there were 3 malignancies and no deaths up to Week 52
Phase II Program (Completed) Phase III Program (Ongoing)
Patient Segment: • Patients with active RA despite ongoing MTX therapy • RA patients refractory or intolerant to anti-TNF
Studies: • Randomized, double-blind, placebo-controlled, dose-
ranging Phase II (N =237)
• Randomized, double-blind, Phase III (FLEX V, O, M)
• Open-labeled, long-term safety and efficacy (Phase
IIIb)
Comparator: • Placebo (background: MTX) • Placebo
• Abatacept (CTLA4-Ig)
Dosing: • 25, 75, 150, or 300 mg once a month, SQ • 75 or 150 mg once a month, SQ
Duration: • 52 weeks; doses escalated in non-responders at Week 20 • 24 weeks
Primary End-
Points:
• ACR20 response rates at 16 weeks • ACR20 (vs. placebo) at 24 weeks
Secondary End-
Points:
• ACR20/50/70 and DAS28-CRP at 52 weeks • ACR20 (vs. atabacept) at 24 weeks; ACR70 (vs.
placebo) at 52 weeks; HAQ-DI (vs. placebo) at 52
weeks; HAQ-DI (vs. atabacept) at 52 weeks
Secukinumab is anti-IL-17 monoclonal antibody that has completed its Phase II Program and
entered a Phase III Program; ACR20 rates at week 16 were higher than placebo but did not
attain statistical significance.
Sources: Company press releases; Genovese MC et al. One year efficacy and safety results of a Phase II trial of Secukinumab in patients with
rheumatoid arthritis. Arthritis Rheum 2011;63 Suppl 10:401

62
Clinical Results (Phase II)
Efficacy: • Meaningful differences vs. placebo were seen at Week 12 for ACR20 in bDMARD-naïve patients receiving 30, 80, or
180 mg Ixekizumab, and in TNF-IR patients receiving 80 or 180 mg Ixekizumab
• CRP values showed a rapid drop with nadir values at 1 week after the first injection
• Significant differences vs. placebo were observed for other clinical measures in both populations at Week 12
Safety: • The frequency of AEs through Week 12 was similar across treatment arms in both populations (range: 45-64%)
• Infections were more frequent in Ixekizumab arms than in placebo arm in bDMARD-naïve (25 vs. 19%) and TNF-IR
patients (27 vs. 23%)
• In bDMARD-naive patients, SAEs occurred in 1.9% of placebo-treated and 3.4% of Ixekizumab-treated patients with 1
serious infection-related event in a patient receiving 80 mg Ixekizumab
• In the TNF-IR population, SAEs occurred in 1.6% of placebo-treated and 9.7% of Ixekizumab-treated patients, and
serious infections occurred in 3.2% of Ixekizumab-treated patients
Lumleian
Commentary:
• If Lilly advances Ixekizumab to phase III it would likely be its third asset targeted to later treatment lines
Phase II Program (Completed)
Patient Segment: • RA patients who are naïve to biologic therapy (bDMARD-naïve), or inadequate responders to TNF Inhibitors (TNF-IR)
Studies: • Randomized, double-blind, placebo-controlled Phase II (N=448)
Comparator: • Placebo
Dosing: • 3, 10, 30, 80, or 180 mg at 0, 1, 2, 4, 6, 8, and 10 weeks, SQ
Duration: • 12 weeks
Primary End-Points: • Determine the dose-response relationship of Ixekizumab in bDMARD naïve pts at Week 12, based on logistic
regression of the ACR20 response rate
Secondary End-
Points:
• Additional safety and efficacy evaluations in the two populations at Week 12
Ixekizumab is an anti-Il17 monoclonal antibody that has completed its Phase II program and
achieved its primary end-point; Lilly has not publicly commented on its advancement to phase III.
Sources: Company press releases; Genovese MC et al. A Phase 2 study of multiple subcutaneous doses of Ixekizumab, an anti-IL-17 monoclonal antibody, in
patients with rheumatoid arthritis in two populations: naïve to biologic therapy or inadequate responders to tumor necrosis factor alpha Inhibitors.
ACR/ARHP Meeting, Chicago, IL, Nov. 5-9, 2011

63
Sources: Simmonds RE and Foxwell BM.. NF-kB and its relevance to arthritis and inflammation. Rheumatology 2008;47:584–590; Hara M et al.
Efficacy and safety of iguratimod compared with placebo and salazosulfapyridine in active rheumatoid arthritis: a controlled, multicenter,
double-blind, parallel-group study.. Mod Rheumatol 2007;17:1-9; Hara M et al.. s Long-term safety study of iguratimod in patients with
rheumatoid arthritis. Mod Rheumatol 2007;17:10-16; Lü LJ et al. Safety and efficacy of T-614 in the treatment of patients with active
rheumatoid arthritis: a double blind, randomized, placebo-controlled and multicenter trial. Chin Med J 2008;121:615-619
Iguratimod is a small molecule compound with anti-inflammatory and immunomodulatory actions.
Physiology • The transcription factor nuclear factor kB (NF-kB)
regulates many aspects of cellular activity in response
to stress and injury, especially the inflammatory
response via induction of IL-1, TNF-a, and the adhesion
molecules E-selectin, VCAM-1, and ICAM-1
• NF-kB consists out of homo- and hetero-dimers of
different subunits: p50, p52, p65, RelB, and c-Rel; NF-
kB dimers are sequestered in the cytosol of
unstimulated cells via non-covalent interaction with
the inhibitor protein IkB; upon phosphorylation, IkB is
degraded, and NF-kB enters the nucleus and binds to
DNA to induce gene expression - In the synovial cells of patients with RA, NF-kB activation
results in the transactivation of multiple genes that
contribute to the inflammatory phenotype, including TNF-
α from macrophages, matrix metalloproteinases from
synovial fibroblasts, and chemokines that recruit immune
cells to the inflamed pannus
Hypothesized
Mechanism
• Multiple mechanisms, including inhibition of NF-kB - Iguratimod inhibits the production of immunoglobulins and
various inflammatory cytokines via suppression of NF-kB
activation without blocking NF-kB inhibitor a (IkBa)
degradation
- Iguratimod also has an anabolic effect on bone metabolism
via stimulation of osteoblastic differentiation and
inhibition of osteoclastogenesis
- Iguratimod has been SFDA-approved in China, and is
undergoing Phase IV trials for re-filing in Japan
Phase IV • Iguratimod (Eisai)
Pipeline

64
Sources: Branger J et al. Anti-inflammatory effects of a p38 mitogen-activated protein kinase inhibitor during human endotoxemia. J Immunol
2002;168:4070–4077.
Three p38 MAP kinase Inhibitors are in the pipeline, but their future is uncertain as several p38
MAP kinase Inhibitors have already been discontinued for lack of efficacy in patients with RA.
Physiology • p38 mitogen-activated (MAP) kinases are responsive
to stress stimuli, such as cytokines, growth factors,
ultraviolet, irradiation, heat shock, and osmotic
shock, and are involved in cell differentiation and
apoptosis - In RA patients, abnormal activation of p38 MAPK to
prevent Fas-mediated apoptosis may represent a
common survival mechanism of RA synovial T Cells
contributing to persistent inflammation of affected
synovium
Hypothesized
Mechanism
• Inhibition of the p38 MAP kinase pathway leading to
inhibition of cytokines and adhesion molecules, and
decrease in CRP release
Potential
considerations
• BMS-582949, an oral dual-action p38 kinase inhibitor,
is a more promising asset than are most other p38
kinase Inhibitors - in a Phase I study, BMS-582949 significantly increased
the proportion of ACR20, DAS28, and HAQ-DI responders
in patients with active RA who had an inadequate
response to MTX
• The long list of failed or terminated p38MAP kinase
Inhibitors in RA includes: - doramapimod, VX-745, VX-702, AMG-548, Scio-323, Scio-
469, pamapimod and ARRY-797
Phase II • BMS-582949 (Bristol-Myers Squibb) • PG-760564 (Procter & Gamble)
Phase I • UR-13870 (Palau Pharmaceuticals)
Pipeline

65
Sources: Vergunst CE et al. Blocking the receptor for C5a in patients with rheumatoid arthritis does not reduce synovial inflammation.
Rheumatology 2007;46:1773–1778
A novel approach targeting the complement system in RA, anti-C5aR agents competitively bind
the C5a receptor which is expressed on activated immune cells, thereby blocking the action of
C5a from guiding inflammatory cells into tissue.
Physiology • All three pathways of complement lead to
formation of C5 convertase, which cleaves C5 into
C5a and C5b
• Whereas C5b is incorporated into the membrane-
attack complex, C5a exerts a predominant pro-
inflammatory activity through interactions with the
classical G-protein coupled receptor C5aR (CD88) as
well as with the non-G protein coupled receptor
C5L2, expressed on various immune and non-
immune cells
• C5a serves as a strong chemotactic factor CD88+
monocytes and neutrophils - In RA patients, monocytes and neutrophils are abundant
in the joints, and C5a is found in the synovium in levels
high enough to induce CD88+ cell chemotaxis
Hypothesized
Mechanism
• Inhibits C5a proinflammatory action by blocking the
C5aR receptor
Potential
Considerations
• MP-435 is being evaluated in combination with MTX
in a Phase II study in RA patients
• NN8209 was evaluated in a Phase I study, and RA
patients are being recruited for a Phase II study
• Cephalon’s anti-C5aR antagonist PMX53 was
discontinued after failing to show efficacy in RA
patients in a Phase II study
• Another C5aR antagonist, CCX168, is being
developed by Chemocentryx for use in vasculitis
Pipeline
Phase II • MP-435 (Mitsubishi Tanabe)
Phase I • NN8209 (Novo Nordisk)

66
Sources: Crilly A et al. Phosphodiesterase 4 (PDE4) regulation of proinflammattory cytokine and chemokine release from rheumatoid synovial
membrane. Ann Rheum Dis 2011;70:1130-1137
Orally available PDE4 Inhibitors reduce TNFα production and therefore provide a potential
alternative to approved, injectable, anti-TNF biologics; two oral phosphodiesterase-4 Inhibitors
are in Phase II.
Physiology • PDE4 is the major cyclic AMP (cAMP)-metabolizing
enzyme found in inflammatory and immune cells
Hypothesized
Mechanism
• Inhibition of PDE4-mediated cAMP metabolism,
leading to the inhibition of multiple cytokines
(TNFa, IL-12, IL-2, IFN-g, IL-5, IL-8), leukotriene B4,
and the adhesion molecule Mac-1 (CD18/CD11b)
Potential
considerations
• Apremilast is in Phase II (recruiting stage) in patients
with rheumatoid arthritis
• Revamilast is in Phase II (recruiting stage) in patients
with rheumatoid arthritis who are taking
methotrexate
Pipeline
Phase II • Apremilast (Celgene Corp.) • Revamilast (Glenmark Pharmaceuticals)

67
Sources: Söderström K et al. Natural killer cells trigger osteoclastogenesis and bone destruction in arthritis. Proc Natl Acad Sci USA
2010;107:13028-13033; Andersson AK et al. Blockade of NKG2D ameliorates disease in mice with collagen-induced arthritis: a potential
pathogenic role in chronic inflammatory arthritis. Arthritis Rheum 2011;63:2617-2629; Park KS et al. Inhibitory NKG2A and activating NKG2D
and NKG2C natural killer cell receptor genes: susceptibility for rheumatoid arthritis. Tissue Antigens 2008:72:342-346
Assets from Novo Nordisk targeting natural killer (NK) cells constitute a new therapeutic
strategy for RA.
Physiology • Natural killer (NK) cells mediate the clearance of virus-
infected, aberrant, or transformed cells
• NK cells also release cytokines and growth factors that
might influence the initiation and development of
immune responses by T and B Cells
• The inhibitory NKG2A and activating NKG2D NK cell
receptors are expressed on subsets on NK cells and T
Cells; they might contribute to chronic inflammation
and destruction of bone and cartilage in RA - NK cells can be detected in the inflamed synovial tissue at
an early stage of RA, and they constitute up to 20% of all
lymphocytes in the synovial fluid of patients with
established RA
- Such NK cells express NKG2A, RANKL and M-CSF, and are
frequently associated with CD14+ monocytes; expression of
NKG2D was also detected on RA synovial cells
Hypothesized
Mechanism
• Modulate NK cell function via blockade of either NKG2D
or NKG2A
Potential
considerations
• The safety and tolerability of anti-NKG2A antibody
NN8765 in RA patients are currently under evaluation in
a Phase I study
• The anti-NKG2D antibody NN8555 program has been
terminated in RA, and is now only focusing on Crohn’s
Phase I • NN8765 (Novo Nordisk)
Pipeline

68
Sources: Gendron S et al. α1β1 integrin and interleukin-7 receptor up-regulate the expression of RANKL in human T Cells and enhance their
osteoclastogenic function. Immunology 2008;125:359–369
Two adhesion molecule Inhibitors are in the early stage of clinical development, though two
integrin Inhibitors have been discontinued after Phase II trials; Cell adhesion molecules play a
key role in the migration, retention and proliferation of activated T Cells and monocytes.
Physiology • Integrins modulate cell adhesion via interaction with
their primary ligands, vascular cell adhesion
molecule (VCAM) and mucosal addressin cell
adhesion molecule (MAdCAM), expressed in the
affected tissue; very late activation antigen-1 (VLA-
1, or a1b1) is a collagen receptor located on T Cells
• Vascular adhesion protein-1 (VAP-1) is required for
leukocyte rolling and transmigration through the
endothelium - In RA patients, activation of both α1β1 integrin (VLA-1)
and IL-7R enhance the ability of CD4+ T Cells to induce
the formation of osteoclasts from human monocytes via
synergic increase in RANKL production
Hypothesized
Mechanism
• Inhibit the recruitment of lymphocytes into the
synovium
Potential
considerations
• The anti-a4 integrin TYSABRI (Biogen Idec), and the
anti-aVb3 integrin Vitaxin (MedImmune) were both
discontinued in Phase II
• BTT-1023 showed encouraging efficacy and safety in
early clinical studies in RA. In April 2012, Biotie and
Seikagaku agreed to terminate their License
Agreement for BTT-1023
• The safety, tolerability, pharmacokinetics, and
pharmacodynamics of a single dose of SAN-300 is
being investigated in about 60 subjects, including
healthy controls and RA patients in a Phase I study
Pipeline
Phase I • BTT-1023 (Biotie Therapies)
• SAN-300 (Santarus)

69
Sources: Sources: Simmonds RE and Foxwell BM.. NF-kB and its relevance to arthritis and inflammation. Rheumatology 2008;47:584–590
NF-κB is involved in many aspects of RA pathology, including inflammation, development of T
helper 1 responses, activation, abnormal apoptosis and proliferation of RA fibroblast-like
synovial cells, and differentiation and activation of bone resorbing activity of osteoclasts.
Physiology • The transcription factor nuclear factor kB (NF-kB)
regulates many aspects of cellular activity in response
to stress and injury, especially the inflammatory
response via induction of IL-1, TNF-a, and the
adhesion molecules E-selectin, VCAM-1, and ICAM-1
• NF-kB consists out of homo- and hetero-dimers of
different subunits: p50, p52, p65, RelB, and c-Rel
• NF-kB dimers are sequestered in the cytosol of
unstimulated cells via non-covalent interaction with
the inhibitor protein IkB; upon phosphorylation, IkB is
degraded, and NF-kB enters the nucleus and binds to
DNA to induce gene expression. - In the synovial cells of patients with RA, NF-kB activation
results in the transactivation of multiple genes that
contribute to the inflammatory phenotype, including TNF-
α from macrophages, matrix metalloproteinases from
synovial fibroblasts, and chemokines that recruit immune
cells to the inflamed pannus
Hypothesized
Mechanism
• Inhibition of NFkB and p38 MAP kinase pathways,
leading to the inhibition of multiple cytokines
Potential
considerations
• A Phase I trial has been completed to evaluate the
safety, tolerance, pharmacokinetics, and activity of
Triolex (HE3286) in RA patients taking MTX ‐ Triolex was found to be safe and well tolerated, and no
drug-drug interactions were observed
‐ Triolex is also being investigated in Phase II for use in type
2 diabetes, in Phase I for use in ulcerative colitis, and in
preclinical stage for use in cystic fibrosis and Parkinson’s
disease
• A Phase I safety and pharmacokinetic study of VGX-
1027 in healthy subjects has been completed
Pipeline
Phase I • Triolex (Harbor Bioscience) • VGX-1027 (Inovio Pharmaceuticals)

70
Sources: van Eden W. XToll, a recombinant chaperonin 10 as an anti-inflammatory immunomodulator. Curr Opin Investig Drugs 2008;9:523-533;
O’Neill LA. Primer: Toll-like receptor signaling pathways--what do rheumatologists need to know? Nat Clin Pract Rheumatol 2008;4:319-327
One asset targeting the Toll-like receptor (TLR) pathway remains in Phase II; XToll is a
recombinant chaperonin 10; IMO-3100, a TLR7/TLR9 inhibitor, is no longer in trials for RA.
Physiology • Toll-like receptors (TLRs) play a key role in innate
immunity; they are pattern recognition receptors
that recognize structurally conserved microbial
molecules; TLR7 and 9 are expressed on monocytes,
macrophages, plasmatoid DCs, and B Cells; TLRs are
potent activators of proinflammatory cytokines, such
as TNFa and IL-6, and of metalloproteinases - In RA patients, immune complexes containing host-
derived nucleic acids have been shown to induce
inflammatory responses mediated through TLR7 and 9;
the expressions of TLR2, 3, 4, and 7 are increased in the
rheumatoid synovium; synovial fibrobalsts of RA patients
constitutively express TLR1-6
Hypothesized
Mechanism
• Inhibition of TLR signaling
Potential
Considerations
• IMO-3100 (Idera) is no longer being pursued in RA. A
Phase II trial in psoriasis was initiated in April 2012
• XToll is a recombinant chaperonin 10 (heat-shock
protein 10), a mitonchondrial protein that inhibits
TLRs; XToll was investigated for safety and efficacy
in 155 patients with moderate to severe RA despite
MTX treatment in a Phase IIa trial; XToll was found to
be safe and well-tolerated; improvement in ACR20 in
RA patients failed to reach statistical significance;
however, a statistically significant effect was
observed in several secondary efficacy parameters
Pipeline
Phase II • XToll (CBio Ltd.)

71
Sources: Company press releases; 3rd party equity research reports; Bio-Pharma Insight; Clinical Trials.gov; Centerwatch
Several additional assets have generated Phase III or Phase II data; Regeneron/Sanofi’s
Sarilumab, which is in phase III trials, achieved 72% ACR20 at week 12.
Mechanism of Action Phase Efficacy Data Safety Data
Sarilumab
(Regeneron/
Sanofi)
• Anti-IL-6Ra
monoclonal
antibody
III • Sarilumab in combination with MTX
demonstrated efficacy: ACR20
response at Wk 12 was significantly
greater with 150 mg QW sarilumab
(72.0%) than with placebo (46.2%)
• The most common treatment
emergent AEs reported by patients in
the treatment arms were infections
(non-serious) 12-26%, neutropenia 0-
20%, and ALT increase 0-6%
Ozoralizumab
(Pfizer/Ablynx)
• Anti-TNF-a
nanobody
II • 80 mg every 4 weeks statistically
significantly improved ACR20
responses over placebo at Week 16
• Improvements of clinical scores,
DAS28, ACR50, ACR70 and EULAR
response at Week 16
• No dose limiting toxicities were
observed, and the AEs and SAEs that
occurred did not show a clinically
significant increase on increased
dosing
Apilimod
(Synta Pharma)
• IL-12/IL-23
transcription
inhibitor
II • No significant difference was found
between apilimod and placebo
• Headache and nausea were reported
with apilimod 180 mg BID for 8
weeks
LX2931
(Lexicon
Pharma)
• Sphingosine 1-
phosphate (S1P)
lyase inhibitor
II • The 150 mg dose did not show a
statistically significant benefit vs.
placebo on ACR20 response
• However, a pooled analysis of the
placebo plus low-dose cohorts (70
mg and 110 mg) vs. the 150 mg
cohort showed a statistically
significant benefit on ACR20
response
• LX2931 exhibited a favorable safety
profile at all three doses tested

72
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on rheumatoid arthritis?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is rheumatoid arthritis?
• Presentation, diagnosis, classification
• Epidemiology by geography and patient segment
• Current care paradigm and clinical evidence
• Emerging care paradigm
10 • 11 - 12
• 13 - 14
• 15
• 16 – 27
• 28
III. Clinical Development Pipeline • Disease mechanism overview
• Clinical development pipeline mapping
• JAK Inhibitors
• Syk Inhibitors
• c-Kit Inhibitors
• Anti-Baff antibodies
• Other mechanisms
29 • 30 - 32
• 33 – 38
• 39 – 45
• 46 - 48
• 49 - 50
• 51 - 52
• 53 – 71
IV. Commercial Landscape • Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
72 • 73 – 78
• 79
• 80 – 81
• 82 – 90
V. Appendix • Table of Acronyms
• More about Lumleian
91 • 92 – 93
• 94 – 96

73
How large is
the global
market and what
growth
is forecast?
• Global ’11 brand revenue for RA was ~$14.7B, steadily increasing throughout the last 3 years
• The market will continue its growth by ~4.5% to ~$18.3B between ’12 and ’15 as currently approved
biologics will continue to dominate rheumatoid arthritis treatment in the next 5 years - US: ‘11 brand revenue increased by ~12% to ~$6.3B, and is forecast to continue this trend to ~$6.8B in ’12, and
increase ~4.7% annually to ~$7.8B through ’15, driven by steady anti-TNFα growth and adoption of newer biologics
in 2nd line treatment based on head-to-head studies versus Humira and newer sub-cutaneous formulations • In Q4 ’11, Orencia showed strong 11% growth driven by its recently approved sub-cutaneous formulation
- EU: ’11 brand revenues were ~$5.0B which is forecast to grow ~4.6% annually between ’12 and ’15, with pipeline
drugs expected to capture limited market share; anti-TNFα bio-similars are anticipated
- JP: Japan’s ’11 brand revenue was ~$1.0B with pipeline drugs expected to accelerate growth through ’15
- RW: ‘11 brand revenue increased by ~33% to ~$2.4B reflecting biologic penetration over the past three years,
however total revenue growth is expected to slow and start to reverse by ’15 • Remicade and Enbrel are expected to lose market share to bio-similars, which are already available in some geographies
What are launch
forecasts?
• Wall Street consensus estimates forecast new product launches will expand the ’15 global market by
~$1.1B, driven largely by anticipated launches: ‐ 2012: Tofacitinib (PFE)
‐ 2013: Iguratimod (Eisai), Secukinumab (NVS)
‐ 2014: Fostamatinib (AZN/Rigel), Sarilumab (SNY), Tabalumab (LLY), Ixekizumab (LLY)
• Analyst forecasts are tempered by the: (1) Crowded competitive landscape, (2) High likelihood that
regulators will constrain launches to 3rd line, (3) Unclear future treatment paradigm, (4) Payor resistance
What trends
are driving the
US market?
• In Q4 ’11 US retail revenue increased ~18% compared to Q4 ’10, driven by a ~7.5% increase in days of
therapy, a ~4.3% increase in price per day, and a 6.4% increase in product mix; Rx volume gains are driven
by capture of Orencia’s sub-cutaneous formulation data at retail pharmacies - Mix: In the US, the prescription market for RA stayed relatively constant in the first 3 quarters in ’11; Humira,
Enbrel and Remicade accounted for ~70% market share; Orencia gained 5 market share, 5 percentage points, after
the approval of its sub-cutaneous formulation
- Promotion: In the three month period ending December ’11, healthcare professional (HCP) spend grew ~10% as
Humira increased its spend by 36% from the previous period; direct to consumer (DTC) spend has been dominated
by Enbrel and Humira, which account for 50%-85% share of DTC voice since April; Simponi and Cimzia, the 4th and
5th anti-TNFα’s to market, have steadily decreased promotional spend throughout 2011 indicating the challenge to
competing in this crowded market; Actemra, which has a restricted 3rd line label, is also reducing marketing spend
Executive Summary: Commercial Landscape

74
Sources: SDI (IMS) PDDA 2010
Methodologically to estimate Rx and revenues specific to rheumatoid arthritis, we pro-rate each drug’s total revenue and prescription volume, based on it percent use in rheumatoid arthritis versus other indications, as reported by physicians; we the use US mix as a global proxy.
54%
47%
44%
96%
64%
51%
6%
100%
0% 20% 40% 60% 80% 100%
Enbrel
Humira
Remicade
Orencia
Simponi
Cimzia
Rituxan
Actemra
Physician reported prescription mix by indication 2010 US
Rheumatoid
Arthritis
Other
Indications
Indication

75
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight
Global ’11 brand revenue for RA was ~$14.7B, steadily increasing throughout the last 3 years; The market is forecast to grow by ~4.5% to ~$18.3B between ’12 and ’15 as current biologics will continue to dominate rheumatoid arthritis treatment in the next 5 years.
’11 Sales ($B) ’10–’11A ’11-’12F ’12–’15F
CAGR
Global &
Pipeline $14.7 18.7% 9.5% 4.5%
US $6.3 11.6% 8.5% 4.7%
EU $5.0 17.3% 17.4% 1.8%
JP $1.0 31.5% 16.2% 26.3%
RW $2.4 39.0% 17.4% 1.8%
Recent and Anticipated New Product Launches - Global
• Roche’s Actemra (01/10)
• Eisai/Abbott’s Humira (07/11, JP)
• PFE’s Tofacitinib (’12)
• Eisai’s Iguratimod (’13 JP) ‐Simcere’s Iremod, approved China, 08/11)
• NVS‘s Secukinumab (’13)
• AZN/Rigel’s Fostamatinib (’14)
• SNY’s Sarilumab (’14)
• LLY’s Tabalumab (’14)
• LLY’s Ixekizumab (’14)
• LLY’s Baricitinib (’15)
Recent and Anticipated Line Extensions
• BMY’s Orencia (08/11, sub-cutaneous)
Recent and Anticipated Loss of Exclusivity
• US: Kineret (12/13), Enbrel (02/14), Rituxan (09/16), and
Humira (12/16)
• EU: Rituxan (08/13), Remicade (08/14), Enbrel EU (10/15)
RA’s Global Brand Revenue ($B)
Actual: Solid bars Consensus Wall Street Forecast: Hashed bars
$9.2
$12.4
$14.7 $16.1
$17.2 $18.0 $18.3
$0.0
$10.0
$20.0
09A 10A 11A 12F 13F 14F 15F
EU
US
JP
RW
Updated: 04/15/12
Pipeline
Notes: Branded sales excludes generic revenues; Pipeline includes: PFE’ s Tofacitinib (’12), Eisai’s Iguratimod (’13), NVS’ s Secukinumab (’13),
AZN/Rigel’ s Fostamatinib (’14), SNY’s Sarilumab (’14), LLY’s Tabalumab (’14), Ixekizumab (’14), Baricitinib (’15)

76
RA’s United States Yearly Brand Revenue ($B) 2011 RA’s United States Quarterly Brand Revenue ($B)
’11 Revenue
($B)
’10–’11A
’11-’12F
’12–’15F
CAGR
United States $6.3 11.6% 8.5% 4.7%
Humira $1.6 19.3% 8.7% 5.7%
Enbrel $1.9 4.7% 0.1% -3.6%
Remicade $1.4 5.7% -1.4% -15.7%
Orencia $0.6 12.4% 23.3% 10.6%
Actemra $0.2 71.4% 37.0% 14.0%
Simponi $0.2 21.8% 17.0% 12.8%
Cimzia $0.2 36.1% 75.7% 21.2%
Rituxan $0.3 2.3% 3.7% 3.0%
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight
Q4 Revenue
($B)
Q3A–Q2A
Q3A–Q4A
United States $1.69 2.3% 4.7%
Humira $0.50 8.4% 20.5%
Enbrel $0.48 -3.5% 2.0%
Remicade $0.34 4.8% -11.4%
Orencia $0.16 1.3% 11.0%
Actemra $0.06 5.9% 1.4%
Simponi $0.04 -3.3% 5.1%
Cimzia $0.05 -2.5% 14.3%
Rituxan $0.06 1.3% 0.2%
United States brand revenue increased by ~12% to ~$6.3B in ’11, and is forecast to continue this
trend’12, and increase ~4.7% annually to ~$7.8B through ’15, driven by steady anti-TNFα growth
and new drug launches; in Q4 ’11, Orencia grew by 11% based on its sub-cutaneous approval.
Actual: Solid bars Wall Street Consensus Forecast: Hashed bars Actual: Solid bars Wall Street Consensus Forecast: Hashed bars
$5.1 $5.6
$6.3 $6.8
$7.2 $7.5 $7.8
$0.0
$5.0
$10.0
09A 10A 11A 12F 13F 14F 15F
Thousa
nds
Updated: 04/15/12
$1.4
$1.6 $1.6 $1.7
$0.0
$1.0
$2.0
Q1A Q2A Q3A Q4A
Updated: 04/15/12
US
Pipeline
Notes: Branded sales excludes generic revenues; Pipeline includes: PFE’ s Tofacitinib (’12), Eisai’s Iguratimod (’13), NVS’ s Secukinumab (’13),
AZN/Rigel’ s Fostamatinib (’14), SNY’s Sarilumab (’14), LLY’s Tabalumab (’14), Ixekizumab (’14), Baricitinib (’15)

77
European Union ’11 brand revenues were ~$5.0B and are forecast to grow ~4.6% annually
between ’12 and ’15 with bio-similar competition offsetting launches; Japan’s ’11 brand
revenue was ~$1.0B with pipeline drugs expected to accelerate growth through ’15.
RA’s Japan Brand Revenue ($B)
RA’s European Union Brand Revenue ($B) ’11 Revenue
($B)
’10–’11A
’11-’12F
’12–’15F
CAGR
European
Union $5.0 17.3% 6.2% 4.2%
Humira $1.8 19.3% 8.7% 5.7%
Enbrel $1.3 6.0% -1.6% 4.1%
Remicade $1.3 5.7% -1.4% -15.7%
Orencia $0.2 62.4% 2.3% 10.3%
Actemra $0.2 186.3% 37.0% 14.0%
Simponi $0.1 237.7% 67.4% 29.7%
Cimzia $0.1 161.3% 59.8% 26.0%
Rituxan $0.1 13.2% 9.7% 1.9% Actual: Solid bars Wall Street Consensus Forecast: Hashed bars
Actual: Solid bars Wall Street Consensus Forecast: Hashed bars
Updated: 04/15/12
Updated: 04/15/12
EU
Pipeline
’11 Revenue
($B)
’10–’11A
’11-’12F
’12–’15F
CAGR
Japan $1.0 31.5% 16.2% 26.3%
Humira $0.1 88.7% 16.4% 28.6%
Enbrel $0.3 19.9% 5.8% 3.3%
Remicade $0.4 23.4% 6.1% 3.3%
Orencia $0.1 62.4% 2.3% 10.3%
Actemra $0.2 37.5% 21.4% 19.1%
Simponi $0.0 67.9%
Cimzia $0.0 79.4%
Rituxan $0.0 9.7% 47.4% 1.6%
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight
JP
Pipeline
$2.9
$4.2 $5.0
$5.3 $5.6 $5.9 $6.0
$0.0
$4.0
$8.0
09A 10A 11A 12F 13F 14F 15F
Thousa
nds
$0.5 $0.8
$1.0 $1.2
$1.5
$1.8
$2.4
$0.0
$1.5
$3.0
09A 10A 11A 12F 13F 14F 15F
Thousa
nds
Notes: Branded sales excludes generic revenues; Pipeline includes: PFE’ s Tofacitinib (’12), Eisai’s Iguratimod (’13), NVS’ s Secukinumab (’13),
AZN/Rigel’ s Fostamatinib (’14), SNY’s Sarilumab (’14), LLY’s Tabalumab (’14), Ixekizumab (’14), Baricitinib (’15)

78
Rest of world brand revenue increased by ~33% to ~$2.4B in ’11 with increasing biologic
penetration; However total revenue growth is expected to slow and start to reverse by ’15;
Remicade and Enbrel are expected to lose market share to bio-similars.
Sources: Lumleian estimates based on publicly available data from bio-pharmaceutical companies (financial statements, investor presentations,
analyst day transcripts); 3rd party equity research reports; Bio-Pharma Insight
RA’s Rest of World Brand Revenue ($B) ’11 Revenue
($B)
’10–’11A
’11-’12F
’12–’15F
CAGR
Rest of World $2.4 39.0% 17.4% 1.8%
Humira $0.4 41.4% 44.5% 16.0%
Enbrel $0.8 21.6% -1.1% -20.9%
Remicade $0.8 34.7% 4.7% -9.5%
Orencia $0.0 62.4% 2.3% 10.3%
Actemra $0.1 174.8% 91.2% -6.6%
Simponi $0.2 237.7% 60.2% 27.3%
Cimzia $0.0 400.0% 432.2% 41.1%
Rituxan $0.1 20.6% 17.9% -0.5% Actual: Solid bars Wall Street Consensus Forecast: Hashed bars
Updated: 04/15/12
RW
Pipeline
$0.7
$1.8
$2.4
$2.9 $3.1 $3.1 $3.0
$0.0
$2.0
$4.0
09A 10A 11A 12F 13F 14F 15F
Thousa
nds
Notes: Branded sales excludes generic revenues; Pipeline includes: PFE’ s Tofacitinib (’12), Eisai’s Iguratimod (’13), NVS’ s Secukinumab (’13),
AZN/Rigel’ s Fostamatinib (’14), SNY’s Sarilumab (’14), LLY’s Tabalumab (’14), Ixekizumab (’14), Baricitinib (’15)

79
$0.1 $0.2
$0.5
$1.1
$0.0
$0.6
$1.2
09A 10A 11A 12F 13F 14F 15F
Baricitinib
Tofacitinib
Secukinumab
Sarilumab
Ixekizumab
Iguratimod
Fostamatinib
Tabalumab
Notes: These forecasts are not representative of Lumleian’s viewpoint; Ad-hoc Lumleian develops its own forecasts for clients
based on its proprietary analytics and research
Global AZN’s Fostamatinib
Equity Research Forecasts ($B)
Global Pipeline Assets Wall Street Consensus Forecast ($B)
Sources: Consensus estimates based on publicly available equity research forecasts that have been updated in the past 12
months (since 02/15/11); Consensus estimate is the ‘straight line’ average with each bank’s forecast weighted equally
Wall Street consensus estimates forecast new product launches will increase the ’15 global market
by ~$1.1B, driven largely by anticipated launches for PFE’s Tofacitinib (’12), Eisai’s Iguratimod
(’13), NVS’ s Secukinumab (’13), AZN/Rigel’ s Fostamatinib (’14), SNY’s Sarilumab (’14), LLY’s
Tabalumab (’14), Ixekizumab (’14) and Baricitinib (’15).
Global LLY’s Ixekizumab
Equity Research Forecasts ($B)
$0.00
$0.10
$0.20
12F 13F 14F 15F
Thousa
nds
$0.00
$0.11
$0.22
12F 13F 14F 15F
Thousa
nds
Updated: 04/15/12
15F Consensus: $0.15B 15F Consensus: $0.98B
Wall Street Consensus Forecast: Hashed bars
Global PFE’s Tofacitinib
Equity Research Forecasts ($B)
$0.00
$0.40
$0.80
12F 13F 14F 15F
Thousa
nds
15F Consensus: $0.46B
(Adjusted for RA only)

80
0%
15%
30%
Sources: SDI (IMS) retail sales and prescription data
Notes: Revenues include both branded and generic products; YTD growth compares 2011 vs. 2010; QTD growth compares the 3months 10/11-12/11
vs. the 3 months 7/11-9/11; MTD compares the month 12/11 vs. the month 12/10
In Q4 ’11, US RA retail revenue increased ~18% compared to Q4 ’10, driven by a ~7.5% increase
in days of therapy, a ~4.3% increase in price per day, and a 6.4% increase in product mix; Rx
volume gains are driven by capture of Orencia’s sub-cutaneous formulation data at retail
pharmacies.
Decomposition of Q4’11 US RA’s Retail Revenue Growth (over Q4 ’10)
Updated: 04/15/12
Dec-11 vs. Dec-10 46.7% 2.5% 0.7% 49.8%
2011 vs. 2010 10.0% 5.7% 4.3% 20.1%
Days of
Therapy
Price per day
(Independent of Mix)
Product
Mix
Retail
Revenue
+7.5%
+4.3%
+6.4% +18.3%

81
0%
50%
100%
In the US, the prescription market for RA has been relatively constant for the first 3 quarters of
’11; Humira, Enbrel and Remicade accounted for ~70% market share; However, Orencia has steadily
gained share from 13% in Q3 to 18% in Q4 with the approval of it sub-cutaneous formulation.
Share
Share Change
(% points) Growth
Dec '11 1 mon 3 mon 12 mon QTD YTD
Total TRx 5.2% 3.4%
Humira 20.4% -0.2 -1.4 -1.9 -2.3% -1.1%
Enbrel 26.4% -0.7 -2.1 -4.4 -8.3% -7.2%
Remicade 20.6% 1.0 -1.3 -0.3 5.5% -2.2%
Orencia 18.1% -0.3 3.7 5.3 36.7% 22.7%
Actemra 1.3% 0.1 0.5 0.8 94.4% 75.3%
Simponi 4.4% -0.1 -0.3 -0.5 -3.9% 16.1%
Cimzia 4.5% 0.0 0.0 0.0 9.9% 25.1%
Rituxan 3.9% 0.2 1.0 1.1 53.8% 77.1%
Kineret 0.5% 0.0 -0.1 -0.1 -15.7% -5.9%
US RA’s Prescription Share (TRx)
Updated: 04/15/12
Humira
Enbrel
Remicade
Orencia
Cimzia
Simponi
Rituxan
Sources: SDI (IMS) Oncology Tracker data
Notes: Patient share includes both branded and generic products; Share Change compares the share for 12/11 vs. 1 month, 3
months, and 12 months ago; YTD growth compares the patient share for 2011 vs. the patient share for 2010; QTD growth

82
In the three month period ending December ’11, healthcare professional (HCP) spend grew ~14% as
Humira increased its spend by 36% from the previous period; direct to consumer (DTC) spend has
been dominated by Enbrel and Humira, which account for 50%-85% share of DTC voice since April.
$0
$30
$60
J F M A M J J A S O N D
$0
$10
$20
J F M A M J J A S O N D
Millions
DTC
HCP
$40.5M
(12/11)
$17.5M
(12/11)
$32.6M
(12/11)
2011 Total Promotional Spend ($M)
2011 Healthcare Professional Spend ($M) 2011 Direct to Consumer Spend ($M)
Updated: 04/15/12
Updated: 03/15/12 Updated: 03/15/12
Share of
Wallet
Growth
Rate
(Dec-11) 3MR
HCP 37.5% 14.3%
DTC 62.5% 8.1%
Share of
Voice
Growth
Rate
HCP (Dec-11) 3MR
Humira 35.3% 36.2%
Enbrel 18.8% -0.7%
Remicade 14.0% 35.9%
Orencia 7.5% 37.8%
Actemra 4.0% 17.5%
Simponi 1.8% -41.2%
Cimzia 10.2% -35.8%
Rituxan 2.8% -3.1%
NPS(RA) 5.5% 188.4%
Share of
Voice
Growth
Rate
DTC
(Dec-
11) 3MR
Humira 18.7% -37.6%
Enbrel 63.7% 70.4%
Orencia 11.0% 89.6%
Actemra 0.1% -36.2%
Simponi 0.0% 197.7%
Cimzia 1.5% -37.0%
NPS(RA) 4.9% -13.0%
$0
$20
$40
J F M A M J J A S O N D
Millions
Sources: SDI (IMS) Promotion Audits, Kantar Media Research 2010 - 2011
Note: Healthcare Professional (HCP) spend includes marketing to physicians, nurse practitioners, physician assistants through marketing & event
promotions, journals, and online promotions; Direct to Consumer (DTC) includes marketing channels in television, radio, newspapers,
magazines, outdoor advertisements, and internet; 3 month rolling (3MR) compares spend for the 3 months 8/11-10/11 vs. the 3 months 5/11-
7/11; The promotional spend for a certain drug covers all indications.

83
0
15
30
J F M A M J J A S O N D
2011 Total Promotional Spend ($M)
Share of
voice
HCP 14.5% 20.7% 21.3% 19.9% 21.0% 15.7% 13.6% 24.2% 26.4% 18.7% 18.2% 18.8%
DTC 26.8% 30.0% 30.1% 44.7% 37.5% 29.3% 23.7% 39.6% 34.2% 25.6% 63.9% 63.7%
Notes: Updated: 04/15/12; 3 month rolling (3MR) compares spend for the 3 months 8/11-10/11 vs. the 3 months 5/11-7/11; The promotional
spend for a certain drug covers all indications.
Sources: SDI Promotion Audits, Kantar Media Research
From the second half of ‘11, Humira’s promotional spend leaned towards DTC;
Humira messaging focuses on preventing joint damage.
HCP
$10.1M
Growth
Rate
(Dec-11) 3MR
HCP $5.4M 36.2%
DTC $4.7M -37.6%
DTC
5/11, 6/11, 10/11, 11/11 & 12/11 -
Help manage many threats.
Rheumatoid arthritis. Psoriatic
arthritis. Ankylosing spondylitis. One
Humira. HUMIRA
11/11 - Help stop joint damage before
it stops you. For many patients with
moderate to severe RA, Humira has
been proven to help relieve pain and
stop further joint damage. Receive
free RA Health Organizer and
Educational Series. www.humira.com
7/11 - Humira has been proven to help
prevent further joint damage while
reducing pain, stiffness, and swelling
in many patients with moderate to
severe RA. Send attached card in
today for a free RA educational series.
www.humira.com

84
0
10
20
30
J F M A M J J A S O N D
Total Promotional Spend ($M)
Share of
voice
HCP 14.5% 20.7% 21.3% 19.9% 21.0% 15.7% 13.6% 24.2% 26.4% 18.7% 18.2% 18.8%
DTC 26.8% 30.0% 30.1% 44.7% 37.5% 29.3% 23.7% 39.6% 34.2% 25.6% 63.9% 63.7%
Sources: SDI Promotion Audits, Kantar Media Research
Enbrel has been widely co-promoted with use for psoriatic arthritis in 2011;
Total promotional spend doubled that of Humira, for November and
December of 2011, with a DTC campaign emphasizing earlier treatment.
DTC
$19M
Growth
Rate
(Dec-11) 3MR
HCP $2.9M -0.7%
DTC $16.1M 70.4%
DTC
Notes: Updated: 04/15/12; 3 month rolling (3MR) compares spend for the 3 months 8/11-10/11 vs. the 3 months 5/11-7/11; The promotional
spend for a certain drug covers all indications.
10/11 - Do you have psoriasis and
joint pain? You may have psoriatic
arthritis. Enbrel is indicated for
reducing signs and symptoms in
adults 18 years or older with
chronic moderate to severe plaque
psoriasis and is taken by injection.
www.enbrel.com
5/11 - If you have psoriatic
arthritis or moderate to
severe rheumatoid arthritis
"Don't let joint pain keep
you from the things that
matter the most." At six
months, Enbrel was shown
to be effective in about
50% of psoriatic arthritis
patients. www.enbrel.com
HCP
10/11 - In patients with
moderate to severe
rheumatoid arthritis (RA).
You may be thinking
"Wait," but their joints may
be saying "Now". ENBREL
10/11 - In appropriate
patients with psoriatic
arthritis or moderate to severe
rheumatoid arthritis, consider
Enbrel "Now". ENBREL

85
0
2
4
J F M A M J J A S O N D
2011 Total Promotional Spend ($M)
Share of
voice
HCP 12.0% 6.2% 17.6% 14.4% 8.7% 20.4% 8.9% 8.4% 13.3% 13.6% 8.5% 14.0%
DTC 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
Remicade promotional spend focuses exclusively on HCP; messaging encourages use
with methotrexate to delay disease advancement versus symptom relief.
HCP
$2.1M
Growth
Rate
(Dec-11) 3MR
HCP $2.1M 35.9%
7/11 - How do you control
an aggressive disease? For
moderately to severely
active rheumatoid arthritis
an aggressive disease
demands aggressive
control. Remicade can help
hold back the progression
of RA. REMICADE
Sources: SDI Promotion Audits, Kantar Media Research;
Notes: Updated: 04/15/12; 3 month rolling (3MR) compares spend for the 3 months 8/11-10/11 vs. the 3 months 5/11-7/11; The
promotional spend for a certain drug covers all indications.

86
0
2
4
6
J F M A M J J A S O N D
2011 Total Promotional Spend ($M)
Share of
voice
HCP 1.6% 4.9% 3.9% 2.7% 6.9% 6.4% 5.3% 4.5% 6.6% 7.0% 5.2% 7.5%
DTC 11.6% 19.9% 11.1% 13.4% 11.4% 5.8% 3.2% 0.3% 15.3% 9.7% 12.9% 11.0%
Promotional spend for Orencia is heavily concentrated in DTC, given its more
convenient formulation, with an emphasis on aiding daily activities; HPC
promotional spend touted Orencia as a unique biologic solution for 1s line RA.
DTC
$3.9M Growth
Rate
(Dec-11) 3MR
HCP $1.1M 37.8%
DTC $2.8M 89.6%
DTC
HCP
9/11 & 2/12- We're
about to flatten what
you may think is a big
obstacle to prescribing
Orencia. Orencia is the
first and only RA
biologic to offer both IV
and SC formulations.
ORENCIA
7/11 - We're about
to shatter how you
may think about
prescribing Orencia
as a first biologic.
ORENCIA
4/11 - Do you have
trouble with everyday
activities? If your
current treatment isn't
helping enough, it may
be time for a change.
Orencia reduces signs
and symptoms in adults
with moderate to
severe RA. Complete
card for Orencia
information.
www.orencia.com
9/11 - I wanted to button my
shirt. I wanted to open a jar.
I wanted to pick up the
paper. Is RA getting in the
way of how you start your
day? Orencia helps reduce
signs and symptoms of
moderate to severe RA.
www.orencia.com 9/11 - Will today be an "I
Want" day or an "I Can" day?
10/11- Is RA getting in
the way of how you start
the day? I wanted...to
open a jar, to get out of
bed, to button my shirt,
to pick up the paper.
Change your "I want" to
"Oh, yes I can!"
www.orencia.com
Sources: SDI Promotion Audits, Kantar Media Research;
Notes: Updated: 04/15/12; 3 month rolling (3MR) compares spend for the 3 months 8/11-10/11 vs. the 3 months 5/11-7/11; The
promotional spend for a certain drug covers all indications.
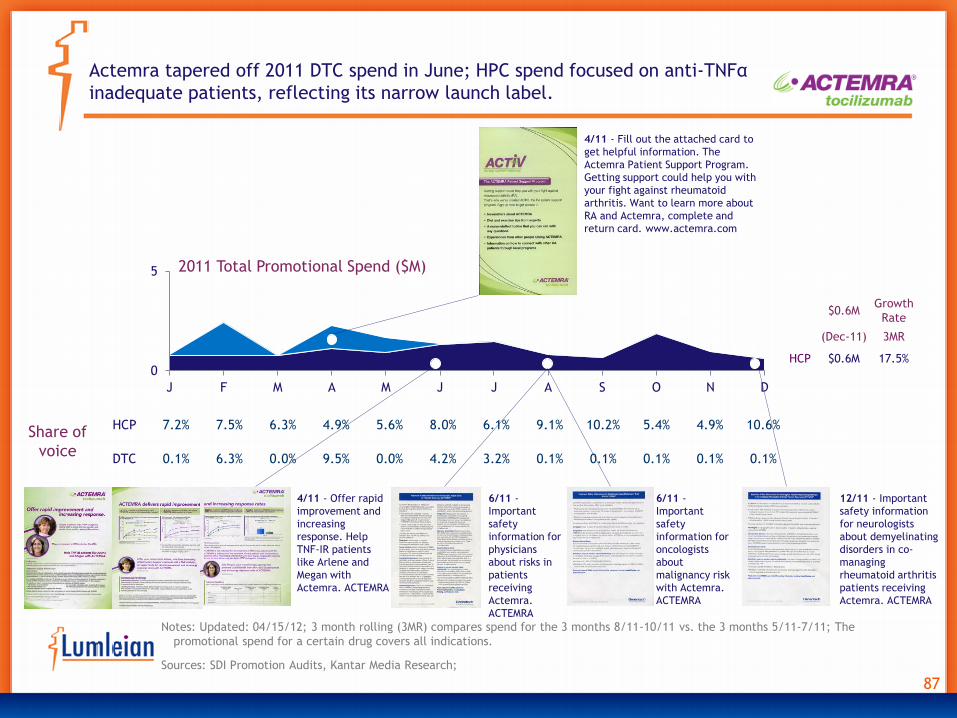
87
0
5
J F M A M J J A S O N D
2011 Total Promotional Spend ($M)
Share of
voice
HCP 7.2% 7.5% 6.3% 4.9% 5.6% 8.0% 6.1% 9.1% 10.2% 5.4% 4.9% 10.6%
DTC 0.1% 6.3% 0.0% 9.5% 0.0% 4.2% 3.2% 0.1% 0.1% 0.1% 0.1% 0.1%
Actemra tapered off 2011 DTC spend in June; HPC spend focused on anti-TNFα
inadequate patients, reflecting its narrow launch label.
$0.6M
Growth
Rate
(Dec-11) 3MR
HCP $0.6M 17.5% HCP
4/11 - Fill out the attached card to
get helpful information. The
Actemra Patient Support Program.
Getting support could help you with
your fight against rheumatoid
arthritis. Want to learn more about
RA and Actemra, complete and
return card. www.actemra.com
6/11 -
Important
safety
information for
physicians
about risks in
patients
receiving
Actemra.
ACTEMRA
4/11 - Offer rapid
improvement and
increasing
response. Help
TNF-IR patients
like Arlene and
Megan with
Actemra. ACTEMRA
12/11 - Important
safety information
for neurologists
about demyelinating
disorders in co-
managing
rheumatoid arthritis
patients receiving
Actemra. ACTEMRA
6/11 -
Important
safety
information for
oncologists
about
malignancy risk
with Actemra.
ACTEMRA
Sources: SDI Promotion Audits, Kantar Media Research;
Notes: Updated: 04/15/12; 3 month rolling (3MR) compares spend for the 3 months 8/11-10/11 vs. the 3 months 5/11-7/11; The
promotional spend for a certain drug covers all indications.

88
0
5
10
J F M A M J J A S O N D
2011 Total Promotional Spend ($M)
Share of
voice
HCP 11.7% 12.3% 11.6% 12.2% 13.5% 8.6% 17.5% 12.4% 7.6% 3.7% 7.7% 10.2%
DTC 21.9% 16.1% 19.0% 10.4% 12.0% 13.5% 5.3% 9.6% 8.8% 8.9% 2.8% 1.5%
From the second half of ‘11, Cimzia’s promotional spend has concentrated on DTC
advertising messaging rapid onset and its convenient sub-cutaneous formulation;
Cimzia has steadily decreased promotional spending throughout the year.
DTC
$1.9M
Growth
Rate
(Dec-11) 3MR
HCP $1.6M -35.8%
DTC $0.38M -37.0% HCP
3/11 & 6/11 & 7/11 - For treatment
of adults with moderate to severe
Rheumatoid Arthritis. Cimzia. RA
relief that can help you get better
grip on life. Reduces RA pain,
stiffness and fatigue in as little 1-2
weeks. Prefilled syringe for comfort.
www.cimzia.com
Sources: SDI Promotion Audits, Kantar Media Research;
Notes: Updated: 04/15/12; 3 month rolling (3MR) compares spend for the 3 months 8/11-10/11 vs. the 3 months 5/11-7/11; The
promotional spend for a certain drug covers all indications.

89
0
5
J F M A M J J A S O N D
2011 Total Promotional Spend ($M)
Share of
voice
HCP 6.9% 6.7% 3.1% 4.1% 2.1% 5.0% 4.0% 3.0% 11.3% 2.8% 4.8% 5.1%
DTC 3.5% 8.2% 9.4% 3.2% 10.5% 5.3% 9.7% 4.6% 0.0% 1.7% 0.0% 4.0%
Similarly Simponi promotional spend has also decreased throughout the year,
reflecting the challenge of competing in a market with five approved anti-TNFα’s.
DTC
$0.3M
Growth
Rate
(Dec-11) 3MR
HCP $0.3M -41.2%
HCP
3/11 - Simponi: A
once-monthly,
subcutaneous
(SC) anti-TNFα
agent.
Dependable
dosing with the
Smartject
Autoinjector.
SIMPONI
10/11- Why make starting a biologic a bigger step
than it has to be? SIMPONI
5/11- A full month of efficacy. For your patients with
moderately to severely active RA. Choose Simponi as their
first biologic. SIMPONI
Sources: SDI Promotion Audits, Kantar Media Research;
Notes: Updated: 04/15/12; 3 month rolling (3MR) compares spend for the 3 months 8/11-10/11 vs. the 3 months 5/11-7/11; The
promotional spend for a certain drug covers all indications.

90
0
1
2
3
4
J F M A M J J A S O N D
2011 Total Promotional Spend ($M) UCB PHARMA HCPPFIZER HCP ABBOTT PHARMA DTCABBOTT PHARMA HCP UNSPECIFIED COMP HCPBRISTOL-MYERS SQUIBB DTC BRISTOL-MYERS SQUIBB HCP
Share of
voice
HCP 4.2% 4.2% 9.2% 6.3% 4.2% 2.0% 5.7% 3.8% 1.4% 4.7% 6.5% 3.7%
DTC 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
NPS (Non-Product-Specific) promotional spend for RA peaked in October along with most other
drug-specific promotional campaigns; NPS HPC promotional spend was dominated by messaging
from Pfizer around the JAK pathways, preceding Tofacitinib’s anticipated launch in Q4.
BMS
10/11 -"Thirsty? Are you
going to try and open me
yourself? Or are you going
to ask someone for help?"
Is your RA still
challenging you?
www.realraliving.com
BMS
10/11 - Are you settling or
living? Mail this card to get
your free realRAliving
information kit.
www.realraliving.com
Abbott
7/11 - A little information can help make a big
decision. Return this card for your free
educational series. To help us better help you,
tell us more about yourself and your RA. Fill
out the form and receive information about RA
and a treatment option.
Pfizer
5/11, 6/11 -In rheumatoid
arthritis, there may be a
different path to take in
approaching cytokine
signaling. Explore an
intracellular approach. JAK
pathways in action.
Pfizer
9/11 - In rheumatoid
arthritis, JAK pathways
transmit signals that
drive inflammation.
Pfizer
7/11 – Explore a
different path to
cytokine signaling in
rheumatoid arthritis.
Sources: SDI Promotion Audits, Kantar Media Research
Notes: Updated: 04/15/12

91
Table of Contents
Slide Number
I. Introduction • Who is Lumleian and what is a disease state primer?
• What is our perspective on rheumatoid arthritis?
• 3 – 6
• 7 – 9
II. Disease Overview and Care Paradigm • What is rheumatoid arthritis?
• Presentation, diagnosis, classification
• Epidemiology by geography and patient segment
• Current care paradigm and clinical evidence
• Emerging care paradigm
10 • 11 - 12
• 13 - 14
• 15
• 16 – 27
• 28
III. Clinical Development Pipeline • Disease mechanism overview
• Clinical development pipeline mapping
• JAK Inhibitors
• Syk Inhibitors
• c-Kit Inhibitors
• Anti-Baff antibodies
• Other mechanisms
29 • 30 - 32
• 33 – 38
• 39 – 45
• 46 - 48
• 49 - 50
• 51 - 52
• 53 – 71
IV. Commercial Landscape • Global, US, EU, Japan market size and growth by brand
• Wall Street consensus forecasts for pipeline assets
• US growth decomposition: Rx volume, pricing, product mix
• US promotional spending, marketing mix and brand messaging
72 • 73 – 78
• 79
• 80 – 81
• 82 – 90
V. Appendix • Table of Acronyms
• More about Lumleian
91 • 92 – 93
• 94 – 96

92
Table of Acronyms (1 of 2)
ACE Angiotensin-converting enzyme
ACPA Anti-citrullinated protein antibody
ACR American College of Rheumatology
AE Adverse event
ALT Alanine aminotransferase
B Billions
BAFF B Cell-activating factor
BID Bis in die (twice daily)
bDMARD Biologic DMARD
CAMKII
Ca2+/calmodulin-dependent protein
kinase
CDAI Clinical disease activity index
COPD Chronic Obstructive Pulmonary Disease
COX Cyclooxygenase
CRP C-reactive protein
CTLA4 Cytotoxic T lymphocyte antigen 4
CTX
C-terminal telopeptide of type I
collagen
DAS Disease activity score
DHODH Dihydroorotate dehydrogenase
DMARD Disease-modifying antirheumatoid drug
DRESS
Drug reaction with eosinophilia and
systemic symptoms
ECG Electrocardiogram
ES Erosion score
ESR Erythrocyte sedimentation rate
EULAR European League Against Rheumatism
FACIT
Functional assessment of chronic illness
therapy
GI Gastrointestinal
GM-CSF
Granulocyte-macrophage colony-
stimulating factor
GSK GlaxoSmithKline
HAQ-DI
Health assessment questionnaire
disability index
HDL High density lipoprotein
HLA Human leukocyte antigen
IFN Interferon
Ig Immunoglobulin
IL Interleukin
ITAM
Immunoreceptor tyrosine-based
activation-motif
IV Intravenously
JAK Janus kinase
LDL Low density lipoprotein
LOCF Last observation carried forward
MAPK Mitogen-activated protein kinase
M-CSF Macrophage colony-stimulating factor
mg Milligram
miRNA microRNA
MMP Matrix metalloproteinase
MoA Mode of action
MRI Magnetic resonance imaging
mTSS Modified total sharp scores
MTX Methotrexate
NFkB Nuclear factor kappa B
NIAMS
National Institute of Arthritis and
Musculoskeletal and Skin Disease
NSAID Nonsteroidal antiinflammatory drug
OAM Once a month
OPG Osteoprotegerin
PAS Patient activity index
PCP Primary care physician
PD Pharmacodynamics
PDE4 Phosphodiesterase-4
PINP Procollagen type I N propeptide
PI3K Phosphoinositide 3-kinase
PK Pharmacokinetics
PML
Progressive multiple focal
leukoencephalopathy
PPAR
Peroxisome proliferator-activated
receptor

93
Table of Acronyms (2 of 2)
QD Quaque die (once daily)
QM Once a month
q8w Every eight weeks
QOD Every other day
QOW Every other week
QW Once weekly
RA Rheumatoid arthritis
RANK
Receptor activator of nuclear factor
kappa-B
RANKL
Receptor activator of nuclear factor
kappa-B ligand
RAPID Routine assessment patient index data
RF Rheumatoid factor
RN Registered nurse
SAE Serious adverse event
sub-c Subcutaneously
SCF Stem cell factor
SFDA Quarter To Date
SF-36 Once weekly
SF-36 Short form 36
SJC Swollen joint count
SQ Subcutaneously
STAT
Signal transducer and activator of
transcription
Syk Spleen tyrosine kinase
TB Tuberculosis
Th T helper
TJC Tender joint count
TLR Toll-like receptor
TNF Tumor necrosis factor
TNF-IR Inadequate responder to TNF Inhibitors
VAP-1 Vascular adhesion protein-1
VAS Visual analog scale
VLA-1 Very late activation antigen-1

94
• Frank Deane, Ph.D. is a Director of Decision Science and Founder of Lumleian. Frank has over ten years experience
working with life science companies and concurrently holds an appointment in the department of strategy at the
Carroll School of Management, Boston College, where he teaches ‘Strategic Issues in Pharma and Bio-Tech,’ to MBA
students. Prior to founding Lumleian, Frank was a director with Leerink Swann and a case team leader with Bain,
where he gained substantial operational experience growing and operating a diverse set of businesses. Frank
entered consulting after spending three years in the bio-pharmaceutical industry with Eli Lilly, supporting portfolio
optimization and business unit strategic planning. He began his career, as a quantitative risk analyst working at
BlackRock. Frank earned a Ph.D. in econometrics from the Krannert School of Management at Purdue University,
where his dissertation focused on applying game theory and statistical modeling to optimize pharmaceutical sales
and marketing resources. Frank has a bachelor of arts in economics from Princeton University.
As a leadership team, we designed Lumleian’s business model based on our collective
experience in: academic R&D, bio-pharmaceutical industry, equity research and strategy
consulting …
• Mark Hochstetler, MBA is a Director of Decision Science at Lumleian. Mark has over ten years experience working
with life science companies. Prior to joining Lumleian, Mark served as the CFO at OPK Biotech, which focuses on
developing oxygen therapeutics for the treatment of anemia, ischemia, and trauma. Before segueing to industry,
Mark spent 5 years as a strategy consultant and equity research analyst at Leerink Swann, where he covered:
Array, Arqule, Ariad, Celgene, Chelsea, Cougar, Cubist, Genentech, GTx, Hana, Idenix, InterMune, Kosan,
Millennium, MGI Pharma, Onyx, Poniard and Vertex. Mark earned an MBA from Duke University’s Fuqua School of
Business with a concentration in health sector management. Mark has a bachelor of arts in political science from
Stanford University.
• Sarah Haigh Molina, Ph.D. is a Manager of Decision Science at Lumleian, where she leads the Academia and Non-
profit practice. Sarah has over ten years experience working and researching in the life sciences. Prior to joining
Lumleian, Sarah was an Assistant Professor of Medicine at Boston University School of Medicine where she served
as the Director of High-throughput Screening. Before returning to academia, Sarah was US Operations Manager at
Molecular Cytomics. Sarah earned a Ph.D. in biology from York University, an MBA from Boston University with a
concentration in entrepreneurship, and a bachelors of science in biochemistry from Dundee University.

95
… Having lived the client experience, we know quality is paramount, and pioneered our
approach with quality and process efficiency as dual mantras.
• Jean Kung, M.Eng, MBA as Manager of Process Efficiency and Quality Control oversees day-to-day operations and
finances at Lumleian and has over five years experience working in the life sciences. Jean designed the process
by which Lumleian efficiently and effectively creates and quarterly updates its disease state primers and serves as
the final point of quality control. Prior to joining Lumleian, Jean served as a contract project manager to various
life science clients. Before entrepreneurship, Jean was a clinical research associate at Health Policy Associates
and a researcher at the Harris Orthopedic Biomaterials and Biomechanics Laboratory, Massachusetts General
Hospital. Jean earned a masters of science in biological engineering from Cornell University and an MBA in the
Health Sector Management Program from Boston University with a concentration in operations and technology
management. Jean has a bachelor of science and masters of engineering in biological engineering, also from
Cornell University.
• Morgen Caroll, MBA as Manager of the Customer Experience at Lumleian, aspires to provide Lumleian's clients with
superior care and service based on their particular needs. Morgen brings over five years life science experience
and has a background in Marketing, Sales, and Public Relations. Prior to joining Lumleian, Morgen worked at
GlaxoSmithKline, with responsibility for the company’s flagship cardiology and endocrinology products. At
GlaxoSmithKline, Morgen was a primary care and specialty care sales representative while serving as a liaison
between product management teams and field sales. As a representative, Morgen consistently ranked in the top
10% of GSK’s sales force, despite working in an inner city territory with significant access challenges. Prior to
entering the life sciences Morgen worked on the sales and marketing staff at Philadelphia Magazine and Food &
Wine Magazine. Morgen earned an MBA from the Villanova School of Business with a concentration in marketing,
and a bachelor of arts in English from Gettysburg College.
• Qingwei Sun, M.Eng., MS as a Decision Science Analyst oversees secondary data collection, synthesis and analysis
and designed analytical methodologies fundamental to Lumleian’s knowledge management platform. KM
database. Using meta-analysis method, he aggregates the clinical and commercial data required to generate
Lumleian’s disease state primers. His work has wide application in product development, portfolio management,
and investment strategy for both large pharmaceutical companies and emerging bio-techs. Qingwei, who is fluent
in Chinese and Japanese, leads our work with Asian clients. Qingwei joined Lumleian after obtaining a master of
science degree from Harvard School of Public Health. He earned both bachelor and master of engineering degrees
from Kyoto University, Japan, concentrating in materials science.

96
We recruit decision scientists explicitly for their expertise and relevant experience across
the gamut of major therapeutic areas and disease states.
• Whitney Amyot, Ph.D. as Decision Scientist focusing on infectious disease leverages her expertise in
scientific investigation and infectious disease to support primary and secondary research for strategic
decision making with biopharmaceutical clients and investors. She has more than ten years of experience in
scientific research, including positions at Atlanta’s Veteran Affairs hospital and in the pharmacology
department at Emory University School of Medicine. In her current role Whitney provides a broad knowledge
base to ensure Lumleian is up to date on current discovery and clinical trends. Whitney earned a Ph.D. in
Molecular Microbiology from Tufts University Sackler Graduate School of Biomedical Sciences where her
dissertation focused translocation in the becterium Legionella pneumophila. Whitney has a Bachelor of
Science degree in Biology from Emory University.
• Alice S. Kaanta, Ph.D. as Decision Scientist focusing on oncology is responsible for leading a team of decision
scientists in reviewing the scientific, clinical and regulatory landscape in numerous oncology indications.
Alice has over ten years of experience in scientific research, in both academia and industry, where her
primary focus has been on cancer research. Alice earned her Ph.D. in Biological and Biomedical Sciences
from Harvard University. At Harvard, Alice worked in the Brugge Lab studying the regulation of pro-
apoptotic Bcl-2 family member Bim in breast cancer progression and in the Neel lab where she identified and
characterized a novel multi-potent mammary progenitor with pregnancy-specific activity. Alice earned dual
bachelor of science degrees in Biology and Physics from the Massachusetts Institute of Technology.
• Olivier Morteau, Ph.D. is a Decision Scientist at Lumleian, where he focuses on the scientific, clinical, and
market developments of therapeutics for autoimmune and inflammatory diseases. Olivier has conducted
research in the field of inflammation and autoimmunity for over 10 years, as a postdoctoral scientist at the
University of North Carolina at Chapel Hill and at Children’s Hospital in Boston, and as a junior faculty at
Children’s Hospital, at the Cummings School of Veterinary Medicine at Tufts University, and at the University
of Oxford (UK). More recently, Olivier was a Senior Immunologist at ImmunoCore Ltd, and a Senior
Communications Scientist at Vertex Pharmaceuticals. Olivier earned a Ph.D. in Pharmacology from Paul
Sabatier University, in Toulouse (France).







