

George Sgouros PhD
Russell H Morgan Dept of Radiology amp Radiological Science
Johns Hopkins University School of Medicine
Baltimore MD
Dosimetry in Clinical Trial
Design Making the case
Disclosures
Consultant Bayer Roche
Scientific Advisory Board Orano Med
Founder Radiopharmaceutical Imaging and
Dosimetry (Rapid) LLC
Current cancer therapies
5-year survival by stageSite localized distant
Breast 99 30
Colorectal 90 14
Lung 56 5
Ovary 93 29
Pancreas 32 3
prostate 100 30SEERCancergov
Current cancer therapies
bull Chemotherapy- Kill rapidly proliferating cells
After the cancer has spreadmetastasized
bull Targeted Biologic Therapy (hormonal Tx)- Inhibit signaling pathways that tumor cells are addicted
to (ie rely on to maintain cancer phenotype)
bull Immunotherapy- Overcome immune tolerance to cancer
bull Radiopharmaceutical Therapy- Kill targeted cells by localized radiation delivery
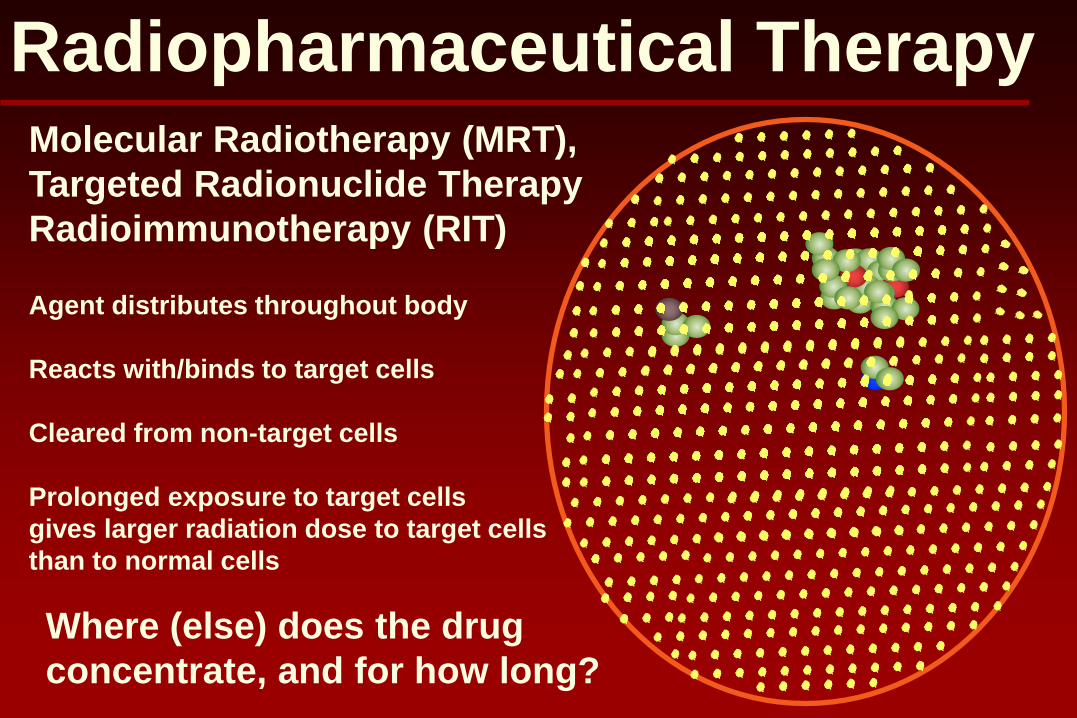
Radiopharmaceutical TherapyMolecular Radiotherapy (MRT)
Targeted Radionuclide Therapy
Radioimmunotherapy (RIT)
Agent distributes throughout body
Reacts withbinds to target cells
Cleared from non-target cells
Prolonged exposure to target cells
gives larger radiation dose to target cells
than to normal cells
Where (else) does the drug
concentrate and for how long
Radiopharmaceutical therapy
bull RPT provides targeted delivery of radiation
bull Not susceptible to resistance mechanism seen in
chemotherapy
bull Kills target cells vs inhibiting growthsurvival
pathways precludes adaptation
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Guide escalation protocols and plan treatment
Radiopharmaceutical therapy
RPT agent Company Indication131I-radioiodine Jubilant Draximage Thyroid cancer131I-MIBG Progenics Adrenergic+ tumors212Pb-trastuzumab
OranoMed HER2+ tumors
212Pb-PRIT OranoMedRoche Undisclosed212Pb-antisomatostatin
OranoMedRadiomedix Somatostatin+ tumors
212Pb-aTEM1 OranoMedMorphotek TEM1+ tumors212Pb-aCD37 OranoMedNordicNanovector Leukemia131I-aCD45 Actinium Pharmaceuticals BM xplant prep225Ac-aCD33 Actinium Pharmaceuticals Leukemia90Y-microspheres VarianSirtex Hepatic malignancies90Y-microspheres BTG Hepatic malignancies
Radiopharmaceutical therapy
RPT agent Company Indication
Lutathera (177Lu) NovartisAAA Somatostatin+ tumors177Lu-aPSMA-R2 NovartisAAA Prostate tumor neovasc177Lu-NeoBOMB1 NovartisAAA Bombesin+ tumors177Lu-PSMA-617 Endocyte Prostate tumor neovascXofigo (223Ra) Bayer Bone metsHER2-TTC (227Th) Bayer HER2+ tumorsPSMA-TTC (227Th) Bayer Prostate tumor neovascMSLN-TTC (227Th) Bayer Mesothelin+ tumorsaCD22-TTC (227Th) Bayer LymphomaFPX-01 (225Ac) JampJFusion Pharma NSCLC pan-cancer target
Radiopharmaceutical therapy
bull 21 RPTs (abridged list)
bull 5 commercially availableFDA approved- 131I thyroid malignancies
- Xofigo (223Ra) castration resistant prostate cancer bone mets
- Lutathera (177Lu) somatostatin+ tumors
- Sirtex (90Y) hepatic malignancies
- Therapsheres (90Y) hepatic malignancies
bull 3 beta-emitters ndash 131I 177Lu 90Y
bull 4 alpha-emitters ndash 225Ac 227Th 212Pb212Bi 223Ra
DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Disclosures
Consultant Bayer Roche
Scientific Advisory Board Orano Med
Founder Radiopharmaceutical Imaging and
Dosimetry (Rapid) LLC
Current cancer therapies
5-year survival by stageSite localized distant
Breast 99 30
Colorectal 90 14
Lung 56 5
Ovary 93 29
Pancreas 32 3
prostate 100 30SEERCancergov
Current cancer therapies
bull Chemotherapy- Kill rapidly proliferating cells
After the cancer has spreadmetastasized
bull Targeted Biologic Therapy (hormonal Tx)- Inhibit signaling pathways that tumor cells are addicted
to (ie rely on to maintain cancer phenotype)
bull Immunotherapy- Overcome immune tolerance to cancer
bull Radiopharmaceutical Therapy- Kill targeted cells by localized radiation delivery
Radiopharmaceutical TherapyMolecular Radiotherapy (MRT)
Targeted Radionuclide Therapy
Radioimmunotherapy (RIT)
Agent distributes throughout body
Reacts withbinds to target cells
Cleared from non-target cells
Prolonged exposure to target cells
gives larger radiation dose to target cells
than to normal cells
Where (else) does the drug
concentrate and for how long
Radiopharmaceutical therapy
bull RPT provides targeted delivery of radiation
bull Not susceptible to resistance mechanism seen in
chemotherapy
bull Kills target cells vs inhibiting growthsurvival
pathways precludes adaptation
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Guide escalation protocols and plan treatment
Radiopharmaceutical therapy
RPT agent Company Indication131I-radioiodine Jubilant Draximage Thyroid cancer131I-MIBG Progenics Adrenergic+ tumors212Pb-trastuzumab
OranoMed HER2+ tumors
212Pb-PRIT OranoMedRoche Undisclosed212Pb-antisomatostatin
OranoMedRadiomedix Somatostatin+ tumors
212Pb-aTEM1 OranoMedMorphotek TEM1+ tumors212Pb-aCD37 OranoMedNordicNanovector Leukemia131I-aCD45 Actinium Pharmaceuticals BM xplant prep225Ac-aCD33 Actinium Pharmaceuticals Leukemia90Y-microspheres VarianSirtex Hepatic malignancies90Y-microspheres BTG Hepatic malignancies
Radiopharmaceutical therapy
RPT agent Company Indication
Lutathera (177Lu) NovartisAAA Somatostatin+ tumors177Lu-aPSMA-R2 NovartisAAA Prostate tumor neovasc177Lu-NeoBOMB1 NovartisAAA Bombesin+ tumors177Lu-PSMA-617 Endocyte Prostate tumor neovascXofigo (223Ra) Bayer Bone metsHER2-TTC (227Th) Bayer HER2+ tumorsPSMA-TTC (227Th) Bayer Prostate tumor neovascMSLN-TTC (227Th) Bayer Mesothelin+ tumorsaCD22-TTC (227Th) Bayer LymphomaFPX-01 (225Ac) JampJFusion Pharma NSCLC pan-cancer target
Radiopharmaceutical therapy
bull 21 RPTs (abridged list)
bull 5 commercially availableFDA approved- 131I thyroid malignancies
- Xofigo (223Ra) castration resistant prostate cancer bone mets
- Lutathera (177Lu) somatostatin+ tumors
- Sirtex (90Y) hepatic malignancies
- Therapsheres (90Y) hepatic malignancies
bull 3 beta-emitters ndash 131I 177Lu 90Y
bull 4 alpha-emitters ndash 225Ac 227Th 212Pb212Bi 223Ra
DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Current cancer therapies
5-year survival by stageSite localized distant
Breast 99 30
Colorectal 90 14
Lung 56 5
Ovary 93 29
Pancreas 32 3
prostate 100 30SEERCancergov
Current cancer therapies
bull Chemotherapy- Kill rapidly proliferating cells
After the cancer has spreadmetastasized
bull Targeted Biologic Therapy (hormonal Tx)- Inhibit signaling pathways that tumor cells are addicted
to (ie rely on to maintain cancer phenotype)
bull Immunotherapy- Overcome immune tolerance to cancer
bull Radiopharmaceutical Therapy- Kill targeted cells by localized radiation delivery
Radiopharmaceutical TherapyMolecular Radiotherapy (MRT)
Targeted Radionuclide Therapy
Radioimmunotherapy (RIT)
Agent distributes throughout body
Reacts withbinds to target cells
Cleared from non-target cells
Prolonged exposure to target cells
gives larger radiation dose to target cells
than to normal cells
Where (else) does the drug
concentrate and for how long
Radiopharmaceutical therapy
bull RPT provides targeted delivery of radiation
bull Not susceptible to resistance mechanism seen in
chemotherapy
bull Kills target cells vs inhibiting growthsurvival
pathways precludes adaptation
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Guide escalation protocols and plan treatment
Radiopharmaceutical therapy
RPT agent Company Indication131I-radioiodine Jubilant Draximage Thyroid cancer131I-MIBG Progenics Adrenergic+ tumors212Pb-trastuzumab
OranoMed HER2+ tumors
212Pb-PRIT OranoMedRoche Undisclosed212Pb-antisomatostatin
OranoMedRadiomedix Somatostatin+ tumors
212Pb-aTEM1 OranoMedMorphotek TEM1+ tumors212Pb-aCD37 OranoMedNordicNanovector Leukemia131I-aCD45 Actinium Pharmaceuticals BM xplant prep225Ac-aCD33 Actinium Pharmaceuticals Leukemia90Y-microspheres VarianSirtex Hepatic malignancies90Y-microspheres BTG Hepatic malignancies
Radiopharmaceutical therapy
RPT agent Company Indication
Lutathera (177Lu) NovartisAAA Somatostatin+ tumors177Lu-aPSMA-R2 NovartisAAA Prostate tumor neovasc177Lu-NeoBOMB1 NovartisAAA Bombesin+ tumors177Lu-PSMA-617 Endocyte Prostate tumor neovascXofigo (223Ra) Bayer Bone metsHER2-TTC (227Th) Bayer HER2+ tumorsPSMA-TTC (227Th) Bayer Prostate tumor neovascMSLN-TTC (227Th) Bayer Mesothelin+ tumorsaCD22-TTC (227Th) Bayer LymphomaFPX-01 (225Ac) JampJFusion Pharma NSCLC pan-cancer target
Radiopharmaceutical therapy
bull 21 RPTs (abridged list)
bull 5 commercially availableFDA approved- 131I thyroid malignancies
- Xofigo (223Ra) castration resistant prostate cancer bone mets
- Lutathera (177Lu) somatostatin+ tumors
- Sirtex (90Y) hepatic malignancies
- Therapsheres (90Y) hepatic malignancies
bull 3 beta-emitters ndash 131I 177Lu 90Y
bull 4 alpha-emitters ndash 225Ac 227Th 212Pb212Bi 223Ra
DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Current cancer therapies
bull Chemotherapy- Kill rapidly proliferating cells
After the cancer has spreadmetastasized
bull Targeted Biologic Therapy (hormonal Tx)- Inhibit signaling pathways that tumor cells are addicted
to (ie rely on to maintain cancer phenotype)
bull Immunotherapy- Overcome immune tolerance to cancer
bull Radiopharmaceutical Therapy- Kill targeted cells by localized radiation delivery
Radiopharmaceutical TherapyMolecular Radiotherapy (MRT)
Targeted Radionuclide Therapy
Radioimmunotherapy (RIT)
Agent distributes throughout body
Reacts withbinds to target cells
Cleared from non-target cells
Prolonged exposure to target cells
gives larger radiation dose to target cells
than to normal cells
Where (else) does the drug
concentrate and for how long
Radiopharmaceutical therapy
bull RPT provides targeted delivery of radiation
bull Not susceptible to resistance mechanism seen in
chemotherapy
bull Kills target cells vs inhibiting growthsurvival
pathways precludes adaptation
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Guide escalation protocols and plan treatment
Radiopharmaceutical therapy
RPT agent Company Indication131I-radioiodine Jubilant Draximage Thyroid cancer131I-MIBG Progenics Adrenergic+ tumors212Pb-trastuzumab
OranoMed HER2+ tumors
212Pb-PRIT OranoMedRoche Undisclosed212Pb-antisomatostatin
OranoMedRadiomedix Somatostatin+ tumors
212Pb-aTEM1 OranoMedMorphotek TEM1+ tumors212Pb-aCD37 OranoMedNordicNanovector Leukemia131I-aCD45 Actinium Pharmaceuticals BM xplant prep225Ac-aCD33 Actinium Pharmaceuticals Leukemia90Y-microspheres VarianSirtex Hepatic malignancies90Y-microspheres BTG Hepatic malignancies
Radiopharmaceutical therapy
RPT agent Company Indication
Lutathera (177Lu) NovartisAAA Somatostatin+ tumors177Lu-aPSMA-R2 NovartisAAA Prostate tumor neovasc177Lu-NeoBOMB1 NovartisAAA Bombesin+ tumors177Lu-PSMA-617 Endocyte Prostate tumor neovascXofigo (223Ra) Bayer Bone metsHER2-TTC (227Th) Bayer HER2+ tumorsPSMA-TTC (227Th) Bayer Prostate tumor neovascMSLN-TTC (227Th) Bayer Mesothelin+ tumorsaCD22-TTC (227Th) Bayer LymphomaFPX-01 (225Ac) JampJFusion Pharma NSCLC pan-cancer target
Radiopharmaceutical therapy
bull 21 RPTs (abridged list)
bull 5 commercially availableFDA approved- 131I thyroid malignancies
- Xofigo (223Ra) castration resistant prostate cancer bone mets
- Lutathera (177Lu) somatostatin+ tumors
- Sirtex (90Y) hepatic malignancies
- Therapsheres (90Y) hepatic malignancies
bull 3 beta-emitters ndash 131I 177Lu 90Y
bull 4 alpha-emitters ndash 225Ac 227Th 212Pb212Bi 223Ra
DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko
Radiopharmaceutical TherapyMolecular Radiotherapy (MRT)
Targeted Radionuclide Therapy
Radioimmunotherapy (RIT)
Agent distributes throughout body
Reacts withbinds to target cells
Cleared from non-target cells
Prolonged exposure to target cells
gives larger radiation dose to target cells
than to normal cells
Where (else) does the drug
concentrate and for how long
Radiopharmaceutical therapy
bull RPT provides targeted delivery of radiation
bull Not susceptible to resistance mechanism seen in
chemotherapy
bull Kills target cells vs inhibiting growthsurvival
pathways precludes adaptation
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Guide escalation protocols and plan treatment
Radiopharmaceutical therapy
RPT agent Company Indication131I-radioiodine Jubilant Draximage Thyroid cancer131I-MIBG Progenics Adrenergic+ tumors212Pb-trastuzumab
OranoMed HER2+ tumors
212Pb-PRIT OranoMedRoche Undisclosed212Pb-antisomatostatin
OranoMedRadiomedix Somatostatin+ tumors
212Pb-aTEM1 OranoMedMorphotek TEM1+ tumors212Pb-aCD37 OranoMedNordicNanovector Leukemia131I-aCD45 Actinium Pharmaceuticals BM xplant prep225Ac-aCD33 Actinium Pharmaceuticals Leukemia90Y-microspheres VarianSirtex Hepatic malignancies90Y-microspheres BTG Hepatic malignancies
Radiopharmaceutical therapy
RPT agent Company Indication
Lutathera (177Lu) NovartisAAA Somatostatin+ tumors177Lu-aPSMA-R2 NovartisAAA Prostate tumor neovasc177Lu-NeoBOMB1 NovartisAAA Bombesin+ tumors177Lu-PSMA-617 Endocyte Prostate tumor neovascXofigo (223Ra) Bayer Bone metsHER2-TTC (227Th) Bayer HER2+ tumorsPSMA-TTC (227Th) Bayer Prostate tumor neovascMSLN-TTC (227Th) Bayer Mesothelin+ tumorsaCD22-TTC (227Th) Bayer LymphomaFPX-01 (225Ac) JampJFusion Pharma NSCLC pan-cancer target
Radiopharmaceutical therapy
bull 21 RPTs (abridged list)
bull 5 commercially availableFDA approved- 131I thyroid malignancies
- Xofigo (223Ra) castration resistant prostate cancer bone mets
- Lutathera (177Lu) somatostatin+ tumors
- Sirtex (90Y) hepatic malignancies
- Therapsheres (90Y) hepatic malignancies
bull 3 beta-emitters ndash 131I 177Lu 90Y
bull 4 alpha-emitters ndash 225Ac 227Th 212Pb212Bi 223Ra
DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Radiopharmaceutical therapy
bull RPT provides targeted delivery of radiation
bull Not susceptible to resistance mechanism seen in
chemotherapy
bull Kills target cells vs inhibiting growthsurvival
pathways precludes adaptation
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Guide escalation protocols and plan treatment
Radiopharmaceutical therapy
RPT agent Company Indication131I-radioiodine Jubilant Draximage Thyroid cancer131I-MIBG Progenics Adrenergic+ tumors212Pb-trastuzumab
OranoMed HER2+ tumors
212Pb-PRIT OranoMedRoche Undisclosed212Pb-antisomatostatin
OranoMedRadiomedix Somatostatin+ tumors
212Pb-aTEM1 OranoMedMorphotek TEM1+ tumors212Pb-aCD37 OranoMedNordicNanovector Leukemia131I-aCD45 Actinium Pharmaceuticals BM xplant prep225Ac-aCD33 Actinium Pharmaceuticals Leukemia90Y-microspheres VarianSirtex Hepatic malignancies90Y-microspheres BTG Hepatic malignancies
Radiopharmaceutical therapy
RPT agent Company Indication
Lutathera (177Lu) NovartisAAA Somatostatin+ tumors177Lu-aPSMA-R2 NovartisAAA Prostate tumor neovasc177Lu-NeoBOMB1 NovartisAAA Bombesin+ tumors177Lu-PSMA-617 Endocyte Prostate tumor neovascXofigo (223Ra) Bayer Bone metsHER2-TTC (227Th) Bayer HER2+ tumorsPSMA-TTC (227Th) Bayer Prostate tumor neovascMSLN-TTC (227Th) Bayer Mesothelin+ tumorsaCD22-TTC (227Th) Bayer LymphomaFPX-01 (225Ac) JampJFusion Pharma NSCLC pan-cancer target
Radiopharmaceutical therapy
bull 21 RPTs (abridged list)
bull 5 commercially availableFDA approved- 131I thyroid malignancies
- Xofigo (223Ra) castration resistant prostate cancer bone mets
- Lutathera (177Lu) somatostatin+ tumors
- Sirtex (90Y) hepatic malignancies
- Therapsheres (90Y) hepatic malignancies
bull 3 beta-emitters ndash 131I 177Lu 90Y
bull 4 alpha-emitters ndash 225Ac 227Th 212Pb212Bi 223Ra
DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Radiopharmaceutical therapy
RPT agent Company Indication131I-radioiodine Jubilant Draximage Thyroid cancer131I-MIBG Progenics Adrenergic+ tumors212Pb-trastuzumab
OranoMed HER2+ tumors
212Pb-PRIT OranoMedRoche Undisclosed212Pb-antisomatostatin
OranoMedRadiomedix Somatostatin+ tumors
212Pb-aTEM1 OranoMedMorphotek TEM1+ tumors212Pb-aCD37 OranoMedNordicNanovector Leukemia131I-aCD45 Actinium Pharmaceuticals BM xplant prep225Ac-aCD33 Actinium Pharmaceuticals Leukemia90Y-microspheres VarianSirtex Hepatic malignancies90Y-microspheres BTG Hepatic malignancies
Radiopharmaceutical therapy
RPT agent Company Indication
Lutathera (177Lu) NovartisAAA Somatostatin+ tumors177Lu-aPSMA-R2 NovartisAAA Prostate tumor neovasc177Lu-NeoBOMB1 NovartisAAA Bombesin+ tumors177Lu-PSMA-617 Endocyte Prostate tumor neovascXofigo (223Ra) Bayer Bone metsHER2-TTC (227Th) Bayer HER2+ tumorsPSMA-TTC (227Th) Bayer Prostate tumor neovascMSLN-TTC (227Th) Bayer Mesothelin+ tumorsaCD22-TTC (227Th) Bayer LymphomaFPX-01 (225Ac) JampJFusion Pharma NSCLC pan-cancer target
Radiopharmaceutical therapy
bull 21 RPTs (abridged list)
bull 5 commercially availableFDA approved- 131I thyroid malignancies
- Xofigo (223Ra) castration resistant prostate cancer bone mets
- Lutathera (177Lu) somatostatin+ tumors
- Sirtex (90Y) hepatic malignancies
- Therapsheres (90Y) hepatic malignancies
bull 3 beta-emitters ndash 131I 177Lu 90Y
bull 4 alpha-emitters ndash 225Ac 227Th 212Pb212Bi 223Ra
DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Radiopharmaceutical therapy
RPT agent Company Indication
Lutathera (177Lu) NovartisAAA Somatostatin+ tumors177Lu-aPSMA-R2 NovartisAAA Prostate tumor neovasc177Lu-NeoBOMB1 NovartisAAA Bombesin+ tumors177Lu-PSMA-617 Endocyte Prostate tumor neovascXofigo (223Ra) Bayer Bone metsHER2-TTC (227Th) Bayer HER2+ tumorsPSMA-TTC (227Th) Bayer Prostate tumor neovascMSLN-TTC (227Th) Bayer Mesothelin+ tumorsaCD22-TTC (227Th) Bayer LymphomaFPX-01 (225Ac) JampJFusion Pharma NSCLC pan-cancer target
Radiopharmaceutical therapy
bull 21 RPTs (abridged list)
bull 5 commercially availableFDA approved- 131I thyroid malignancies
- Xofigo (223Ra) castration resistant prostate cancer bone mets
- Lutathera (177Lu) somatostatin+ tumors
- Sirtex (90Y) hepatic malignancies
- Therapsheres (90Y) hepatic malignancies
bull 3 beta-emitters ndash 131I 177Lu 90Y
bull 4 alpha-emitters ndash 225Ac 227Th 212Pb212Bi 223Ra
DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Radiopharmaceutical therapy
bull 21 RPTs (abridged list)
bull 5 commercially availableFDA approved- 131I thyroid malignancies
- Xofigo (223Ra) castration resistant prostate cancer bone mets
- Lutathera (177Lu) somatostatin+ tumors
- Sirtex (90Y) hepatic malignancies
- Therapsheres (90Y) hepatic malignancies
bull 3 beta-emitters ndash 131I 177Lu 90Y
bull 4 alpha-emitters ndash 225Ac 227Th 212Pb212Bi 223Ra
DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

DNA
ele
ctr
on
sA
lph
a-
part
icle
Clustered ionizations from
low-energy electron
Delta-ray electron
Single ionization
-- high probability of damage when
alpha-particle hits DNA
(DTGoodhead CERRIE Workshop 2003)
Linear Energy Transfer (LET)
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko
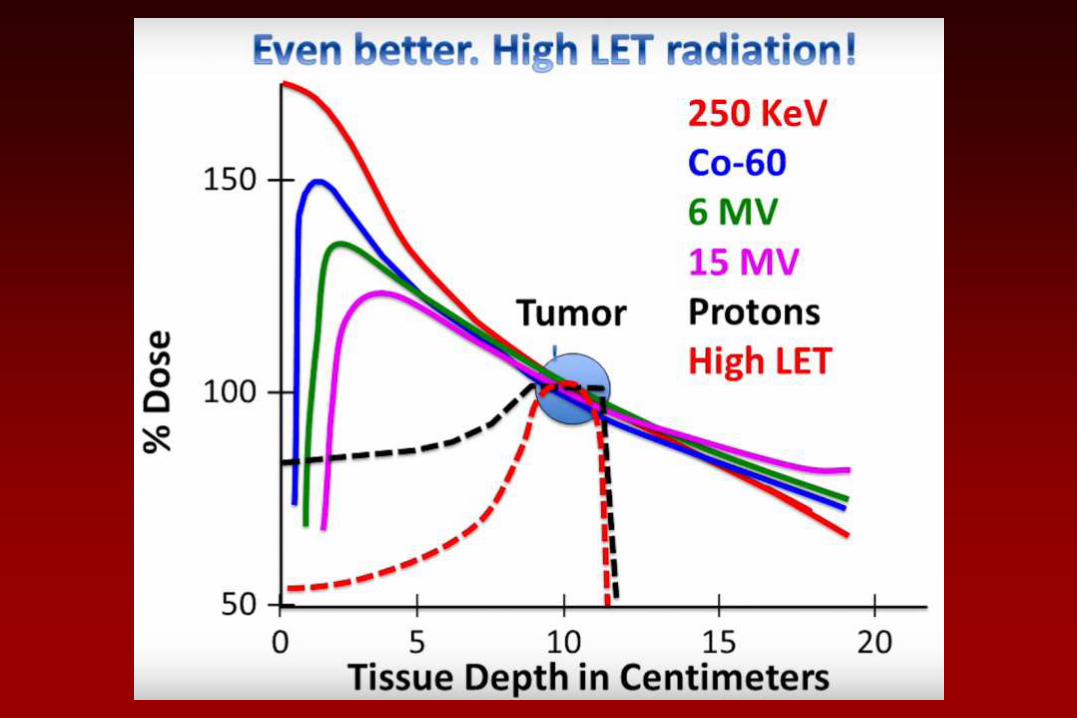
Tumor-response evaluation in αRPT
Kratochwil et al JNM 2016
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko
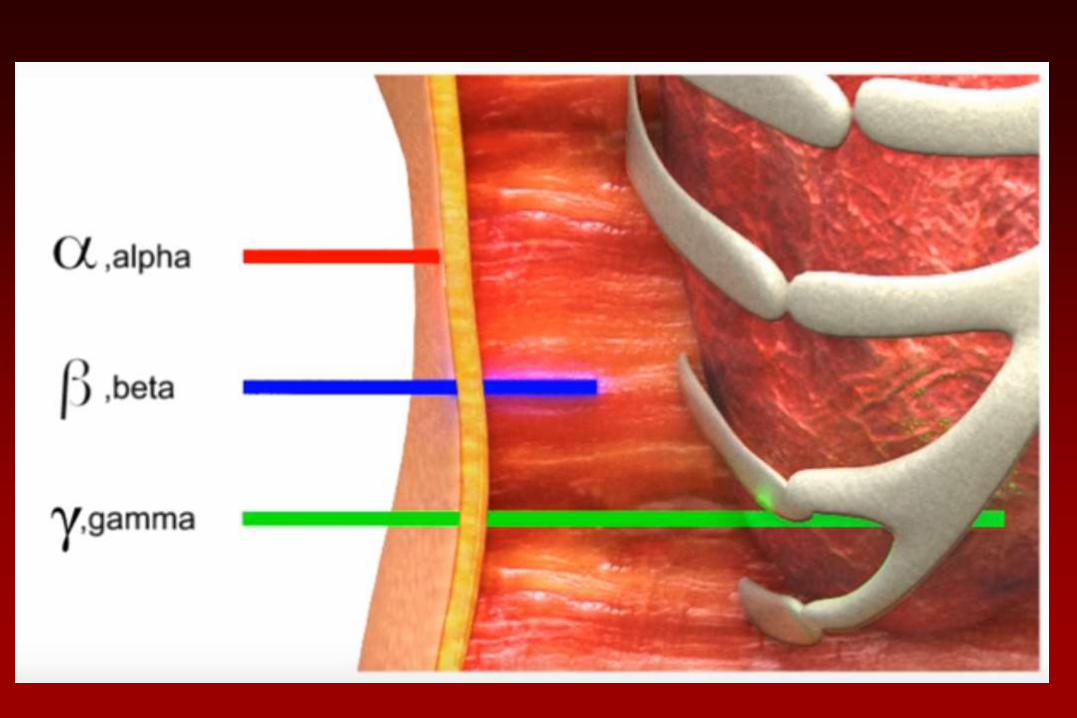
Tumor-response evaluation in RPT
Kratochwil et al JNM 2016
DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

DNA double-strand breaks
BT474 370kBq (10 uCi)213Bi-trastuzumab 1h
BT474 4Gy XRT
1h
bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

bull dose for cell kill w betas 3-7 x alphas in vitro
bull RBE influenced by- Biological end-point
- Reference radiation
- Dosimetry methodology
Relative Biological Effectiveness (RBE)
)(
)()(
xD
xDxRBE
t
r=x = biological effect
r = reference radiation
t = test radiation
Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Repair Radiosensitization and RBE
Song et al MCT 2013
Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Potential for increased toxicity
httpwwwemaeuropaeuemaindexjspcurl=pagesnews_and_eventsnews201807ne
ws_detail_002996jspampmid=WC0b01ac058004d5c1
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko
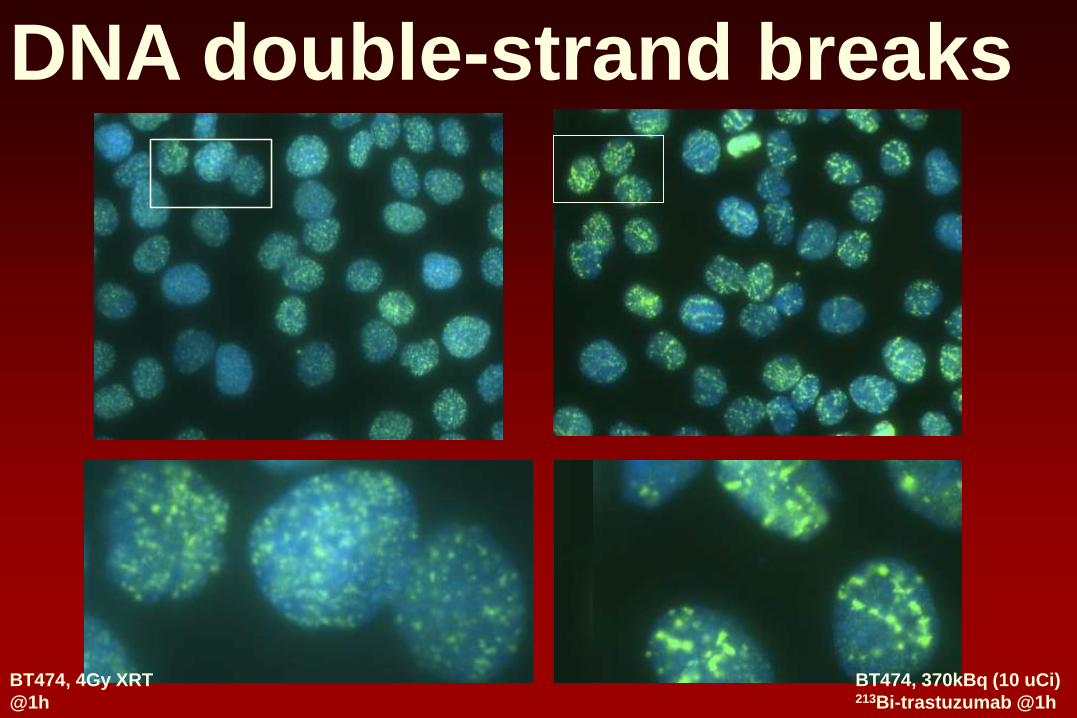
bull Early phase trials ndash opportunity to collect data
bull Donrsquot propose altering treatment
bull Show that dosimetry would have predicted toxicity or lack of efficacy
bull Assess patient variability
bull Apply rigorous consistent methods- 3 time-points 1st and last cycle
- Pre-therapy tracer study
- SPECTCT
bull Use collected data to validate simpler schemes
bull Be prepared to accept conclusions- Prior patient history dose-range can impact dose-response
relationship
PROVEDOSIMETRY IMPROVES TX
Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Biomarkers
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

bull Select patients most likely to respond
bull Avoid toxicity
bull Tumor biopsy
bull Serum sampling
bull Genetic and epigenetic marker analysis
bull Must be rigorously qualifiedvalidated retrospectively or in prospective studies
bull Standardized
bull Incorporated in the design of clinical trials
Dosimetry
bull
bull
bull Quantitative Imaging
bull Blood Counting
bull Dose Calculation
bull
bull
bull
Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Admin Activity (AA) vs Abs Dose
Wahl RL Semin Oncol lsquo03
Example of
patient
variability
Previously
demonstrated
that 75 cGy to
WB increases
RM toxicity
Is small fraction of patients that will be
undertreated worth the dosimetry effortcost
131I-anti-CD20 Ab NHL patients
Bexxar
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko
le 200 cGy
gt 200 cGy
J Nucl Med 2014 Jul55(7)1047-53 doi 102967jnumed113136044 Epub 2014 May 19Tumor-Absorbed Dose Predicts Progression-Free Survival Following (131)I-Tositumomab RadioimmunotherapyDewaraja YK1 Schipper MJ2 Shen J3 Smith LB4 Murgic J5 Savas H6 Youssef E6 Regan D6 Wilderman SJ7 Roberson PL2 Kaminski MS8 Avram AM6
Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors httpswwwnejmorgdoifull101056nejmoa1607427
by J Strosberg - 2017 - Cited by 376 - Related articles
12 Jan 2017 - Patients with advanced midgut neuroendocrine tumors who have had disease progression
during first-line somatostatin analogue therapy have limited therapeutic options This randomized controlled
trial evaluated the efficacy and safety of lutetium-177 (177Lu)ndashDotatate in patients
Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Red Marrow Dose vs Response Literature
Pla
tele
t Toxic
ity G
rade
(N = 109) (N = 57)
(N = 91) (N = 56)
OrsquoDonoghue et al CBR lsquo00
Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Red Marrow Dose vs Response MSKCC (N=36)
Pla
tele
t Toxic
ity G
rade
OrsquoDonoghue et al CBR lsquo00
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
Effect of Chemotherapy Mitomycin
0
1
2
3
4
0 100 200 300 400 500
RM dose (rad)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
0
1
2
3
4
0 50 100 150
WB dose (rad)
0
1
2
3
4
0 50 100 150
Admin ActviitySA (mCim2)
w mito
wo mito
00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

00
01
02
03
04
05
06
07
08
P-G
W-
DC
W-G
P-
DC
W-A
DC
W-T
TN
P-T
TN
P-A
DC
wo mytomycin
w mytomycin
RM Dose Correlation Coefficients (r)
mitomycin
mitomycin
Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Dosimetry 34
Dose Standard volume (Gy)
20 30 40
Cre
atinin
e c
leara
nce lossy
ear
( b
aselin
e)
0
20
40
60
Correlation between kidney dose (Gy)
and creatinine clearance lossyear ( baseline) N=18
Kidney volumes measured by CT
cortex (70)
Standard kidney volumes
Kidney dose CT volume (Gy)
0 10 20 30 40 50
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60
R=054p= 002
Importance of organ volume in self irradiation
UNIVERSITE CATHOLIQUE DE LOUVAINBarone et al JNM lsquo05
Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Dosimetry 35
Correlation between BED
and creatinine clearance lossyear
Biologic Effective Dose (Gy)
0 10 20 30 40 50 60
Cre
atin
ine c
leara
nce
lo
ssy
ear
( b
ase
line)
0
20
40
60R=093plt00001
UNIVERSITE CATHOLIQUE DE LOUVAIN
Barone R Borson-Chazot F Valkema R et al J Nucl Med 2005 Jan46 Suppl 199S-106S
Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Activity data
SPECT or PET
Anatomic data
CT (or MRI)
Input
Registration
VOIs definition
Generation of
data volumes
Processing Monte Carlo
Calculation
Activity
(xyzt)
Density
(xyz)
Composition
(xyz)
Output
Abs dose
rate (xyzt)
Processing
- Mean dose
- Isodose
-DVH
1 2 3 4
- BED (BVH)
- EUD
3D-RD Flowchart
MIRD Pamphlet 23 Quantitative SPECT for Patient-Specific
3-D Dosimetry in Radionuclide Therapy JNM 2012
153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

153Sm-EDTMP ndash Xbeam Therapy
Pediatric patient population153Sm emits bminus with a half-life
of 467 h and 103 keV
photon
Escalation protocols ndash patients
treated with 12 mCikg and
50 mCikg (myeloablative)
and imaged with planar
images for dosimetry
Median survival was 79 days ndash
2 patients (out of 14) had
longer survival times (990
and 1472 days)
Loeb et al Cancer rsquo09
Hobbs et al Phys Med Biol rsquo10
Loeb et al Cancer rsquo10
Senthamizhchelvan et al J Nucl Med rsquo11
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Absorbed Dose (21 Gy) EUD (6 Gy) threshold for PD vs SD
p lt 005
Absorbed Dose EUD vs Response
Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Sm-135 osteosarcoma RPT
Srinivasan et al JNM rsquo12
Confirms PD vs SD results
Tumor Volume Reduction vs AD EUD
p lt 0031 p lt 0023
Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Combined modality Therapybull Osteogenic Sarcoma
bull XRT for inoperable tumors
bull XRT limited if close to spinal cord (SC)
bull Combine w 153Sm (RPT)
bull uarr tumor dose SC dose
bull Adjust for dose-rates ( )( )( )
RPT RPTdGF
RPT
D G DD
d
b
b
+ =
+
( )
2
0 0
2( ) ( ) ( )
T t
t w
RPT RPT
RPT
G T D t dt D w e dwD
minus minus= Hobbs et al IJROBP rsquo10
3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

3 Combined RPT-XRT
Ideandash XRT can deliver precise amounts of radiation to
regions of interest (ROIs) but limited by adjacent organ at risk (eg spinal cord)
ndash RPT highly conformal - delivers dose to all tumor sites including micro-metastases
How ndash The combination XRT with RPT requires accurate
3-D dose calculations to avoid toxicity and evaluate potential efficacy
ndash Deliver RPT (12 mCikg) and make 3D dose map in 3D-RD convert to external beam AD values and import into XRT software and include in treatment plan Hobbs et al IJROBP rsquo10
Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Protocol(a) 18F-MISO PETCT for baseline
b Stem cell collection for autologous transplant
c CT-sim used for both XRT and RPT treatment planning
d Low dose 153Sm-EDTMP (1 mCikg)
e SPECTCT imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
f High dose 153Sm-EDTMP determined by dosimetry (max 20 mCikg)
g High dose imaging at 4 24 and 48 h image reconstruction and dosimetry calculations
h Autologous stem cell transplant (recovery)
i IMRT plan add fusion of low + high dose maps
(j) 18F-MISO PETCT for treatment response
RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

RPT-XRT AD equivalence
AD from XRT fractionated
AD from RPT over time
What about biological equivalence
Use BED as a bridge
(Equivalent linear dose compared to the linear-quadratic absorbed dose with a repair term)
Equivalence depends on dose per fraction d
+= )(
1 i
ii
iii G
DDBED
b
+=
ii
ii
dDBED
b 1
( )2
)(2
+
+=
b
b iRPTRPT GDDEQD
RPT
XRT
Hobbs et al IJROBP rsquo10
Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Combined treatment
Xbeam and PTV
Xbeam and Sm-153
Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Conclusions
bull RPT dosimetry is the ideal biomarker
bull Mechanism of action is well understood
bull Needed measurements are known
bull Patient-specific dosimetry tools are available
bull Response data from radiotherapy
bull Can measure delivery of the therapeutic agent to
tumor targets and to normal organs
bull Calculate radiation dose to tumors normal organs
bull Guide escalation protocols and plan treatment
Need to overcome prior history- 2nd chance
Implement standardized validated activity
quantification and dosimetry methods in early
phase clinical trials to gather rigorous
evidence that dosimetry will improve patient
care
Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko

Acknowledgments
NIH
DOD
DOE
Rob Hobbs
Senthamil Srinivasan
Donika Plyku
Anders Josefsson
Sunju Park
Jessie Nedrow
Sanchita Roy
Alireza Karimian
Akhila Rao
Hong Song
Andy Prideaux
Yah-el Har-el
Mohana Lingappa
Karineh Shahverd
Kitiwat Khamwan
Eric Frey
Richard Wahl
Ivan Guan
Kevin Yeh
Sagar Ranka
Martin Pomper
Benjamin Tsui
James Fox
Yuchuan Wang
Hong Fan
Ron Mease
David Huso
Kathy Gabrielson
Zaver Bhujwalla
Barjor Gimi
VP Chacko







