بسم هللا الرحمن الرحيم

Dr. Ahmed Abdallah Eisawy
MBBS M.Sc MD


CT diagnosis of the abnormal bowel wall
• Computed tomography demonstrates intestinal wall abnormalities that can be analyzed by
categorizing attenuation changes in the intestinal wall into five patterns

ATTENUATION WITH NO CONTRAST
circumferential thickening of sigmoid colon (arrow). Attenuation of bowel wall is homogeneous. Without IV contrast material, further characterization is not possible
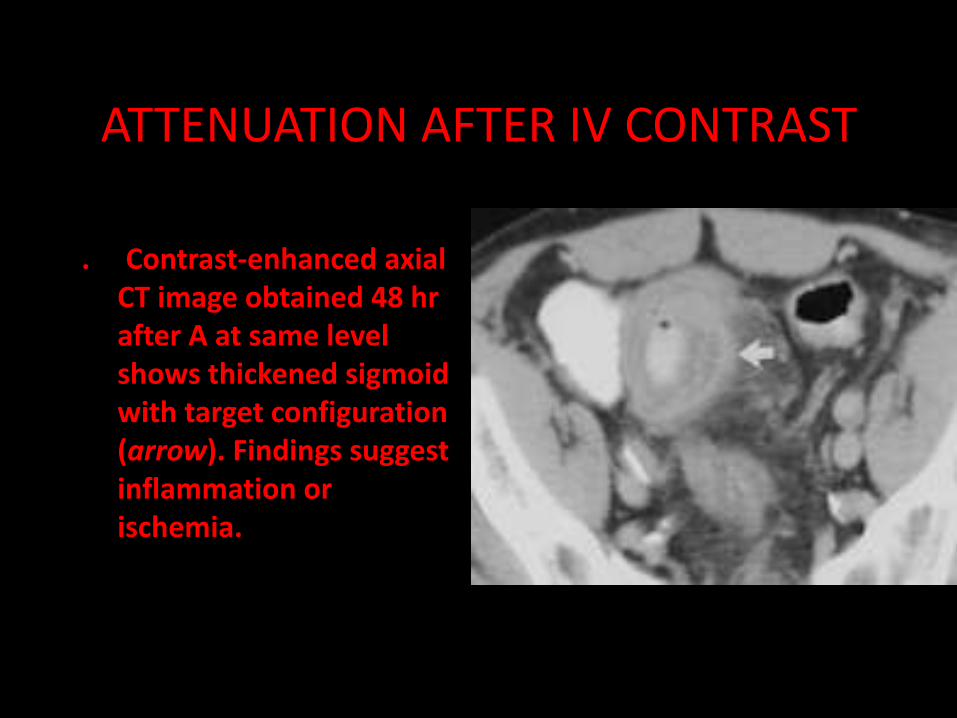
ATTENUATION AFTER IV CONTRAST
. Contrast-enhanced axial CT image obtained 48 hr after A at same level shows thickened sigmoid with target configuration (arrow). Findings suggest inflammation or ischemia.

Homogeneous Attenuation
• (gray and white attenuation)
• The differential diagnosis of a thickened bowel wall that shows homogenous attenuation on CT includes submucosal hemorrhage or hematoma, infarcted bowel, neoplasm, chronic Crohn's disease, radiation injury, and pseudothickening related to incomplete distention and residual fluid
Heterogenous(stratified) patteren
(water halo sign+fat halo sign+black attenuation)
(inflammation and ischemia)
pneumatosis may present as a striated
pattern of attenuation
Heterogenous(mixed) attenuation
• The final category of attenuation pattern in thickened bowel

.1- Gray attenuation
It is defined as a thickened bowel wall that shows little enhancement and whose
homogeneous Attenuation is comparable with that of enhanced muscle
Common diagnosis: It is the least specific of the five attenuation categories and is common inboth benign and malignant intestinal wall lesions

Morphologic criteria aiding interpretation of CT scans in intestinal diseases

2-The white pattern
• It represents avid uniform contrast enhancement of the thickened bowel wall that is equal to or greater than that of venous opacification in the same scan
• Common diagnosis: idiopathic inflammatory bowel disease , vascular disorders(bowel ischemia),bowel wall haematoma
• Uncommon diagnosis: Malignancy

3-water halo sign
• It indicates stratification within a thickened bowel wall. The lower attenuation layer of the water halo sign is believed to represent edema
The double halo sign consists of an inner low-attenuation (edema) ring surrounded by an outer higher attenuation ring.
• Common diagnosis: IBD, vascular disorders, infectious diseases and radiation damage

4-Fat halo sign
• The pattern of the fat halo sign refers to a 3-layered target sign of thickened bowel in which the middle or sub-mucosal later has a fatty attenuation.
• In the "target" sign, inner and outer layers of high attenuation surround a central area of decreased (edema) attenuation These signs are best visualized during the late arterial and early portal venous phases of IV contrast material enhancement On unenhanced or delayed (>2 min) IV contrast—enhanced CT, these signs may not be visualized. The high attenuation present with these signs is related to hyperemia
If measured in Hounsfield units, it will largely below -10HU and can be distinguished from the grayer tone of the water halo sign
• Diagnosis: Idiopathic inflammatory bowel disease . Fat target sign is more common in ulcerative colitis than Crohn's disease

• Target" sign in 37-year-old man with history of acute Crohn's
disease. Contrast-enhanced axial CT image shows marked circumferential thickening of terminal ileum. Target appearance is present, with enhancement of mucosa (short arrow) and outer enhancement of muscular layer (long arrow) surrounding low-attenuation edematous submucosa (arrowhead

• A notable exception to this accepted general rule (target sign = inflammation) is the rare occurrence of this sign in infiltrating scirrhous carcinoma of the stomach and colon Rigidity (after attempted air insufflation),

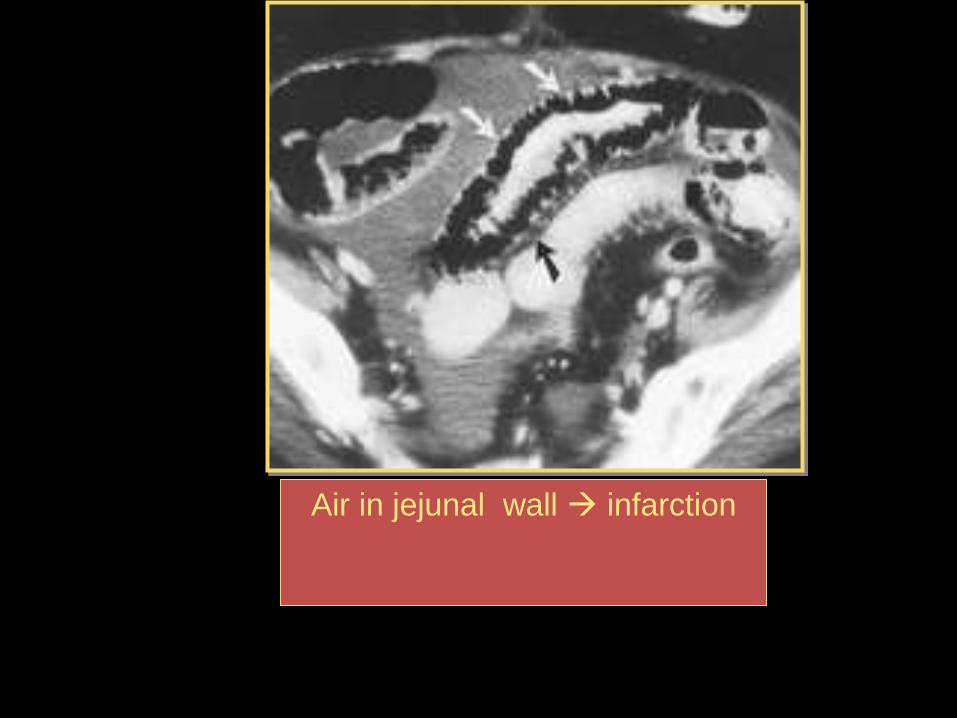
5- Black attenuation
• It is the equivalent of pneumatosis. Any process of injury of the bowel wall that is accompanied by a break
• in the mucosa can introduce intramural gas
• Common diagnosis: Ischemia, infection and trauma
• Pitfalls: confusing intramural gas with intraluminal gas

Combination of attenuation patterns
• A single disease, like IBD, may simultaneously demonstrate different attenuation patterns in
• contiguous segments of the bowel. Analysis of each segment of affected small or large intestine is judged by its separate category

• Heterogeneous low-attenuation enhancement in mucinous adenocarcinoma with irregular circumferential bowel wall thickening in 64-year-old man with abdominal pain. Contrast-enhanced axial CT image of splenic flexure shows irregular wall thickening (arrows) with heterogeneous areas of low attenuation in colon wall (arrowhead). Large mucinous adenocarcinoma was found at surgery

Gray
attenuation
White
attenuation
Black attenuation
Water halo sign
Fat halo sign
Benign & malignant
Hematoma
& ischemia
Infectious
radiation
IBD

Degree of Bowel Wall Thickening
• In general, benign conditions result in bowel wall thickening of less than 2 cm, whereas wall thickening greater than 3 cm is usually present in neoplastic conditions

Mild Thickening
• In cases of mild bowel wall thickening, a non-neoplastic (inflammatory or infectious) condition is usually present.

Marked Thickening
• INFLAMMATION,INFECTION:With severe infections of the colon, the wall may become markedly thickened by edematous haustral folds (up to 2 cm or even greater
• On CT, the finding of barium trapped between these folds is known as the "accordion" sign
• NEOPLASM: Small-bowel lymphoma rarely obstructs the lumen, and it often presents as a markedly thickened segment ranging from 1.5 to 7 cm (mean, 2.6 cm)
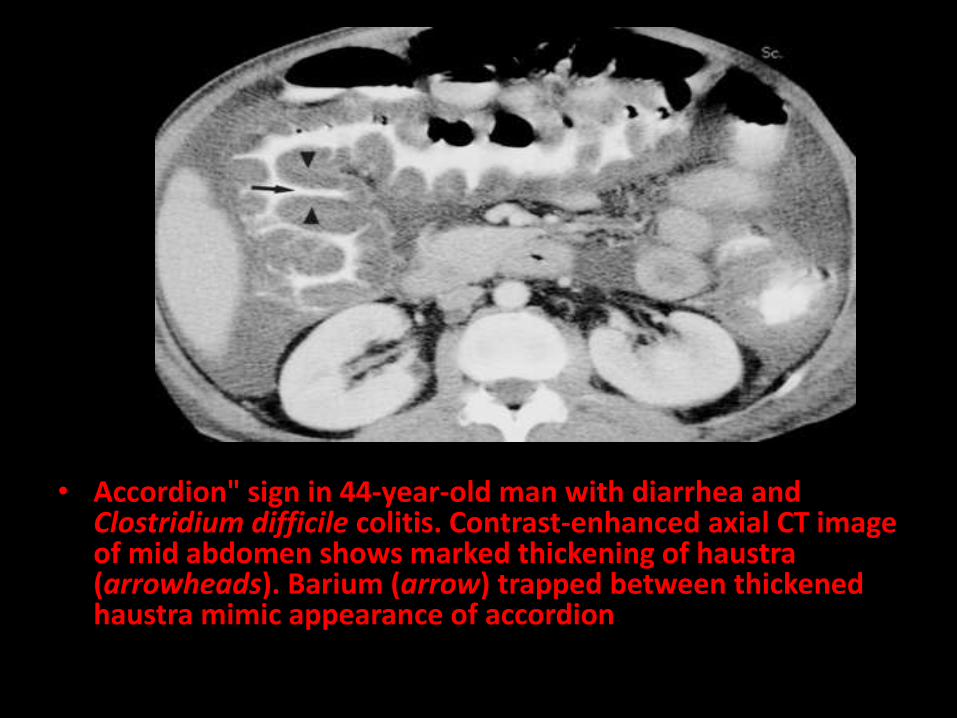
• Accordion" sign in 44-year-old man with diarrhea and Clostridium difficile colitis. Contrast-enhanced axial CT image of mid abdomen shows marked thickening of haustra (arrowheads). Barium (arrow) trapped between thickened haustra mimic appearance of accordion

Lymphoma Variants
Widespread thickening of SI wall
Narrowing + irregular thickening of folds

• Exophytic intestinal mass in 84-year-old man with bowel obstruction.
Contrast enhanced axial CT image shows large bulky exophytic mass extending from jejunum with heterogeneous attenuation (white arrows). Small bubble of gas is present in mass (black arrow), suggesting fistula in
bowel. Surgery revealed malignant gastrointestinal stromal tumor

CT
Non-specific bowel
wall thickening

Malrotation. Abdominal CT scan shows the superior mesenteric vein
(+) lying anterior to the superior mesenteric artery. The superior
mesenteric vein normally lies on the right side of the superior
mesenteric artery; in malrotation, it lies either in front or on the left
side

Coronal and axial CT showing low density clearly delineated mass in
duodenum/jejunum. Low intensity of the mass on MR T1 fat sat. Macroscopic image of
lipoma.

Intraluminal lipoma.

Small bowel lipoma (black arrow).

Schwannoma of the stomach.

Extra-luminal jejunal leiomyomas.

Small bowel leiomyoma.

Benign hamartomatous polyps.
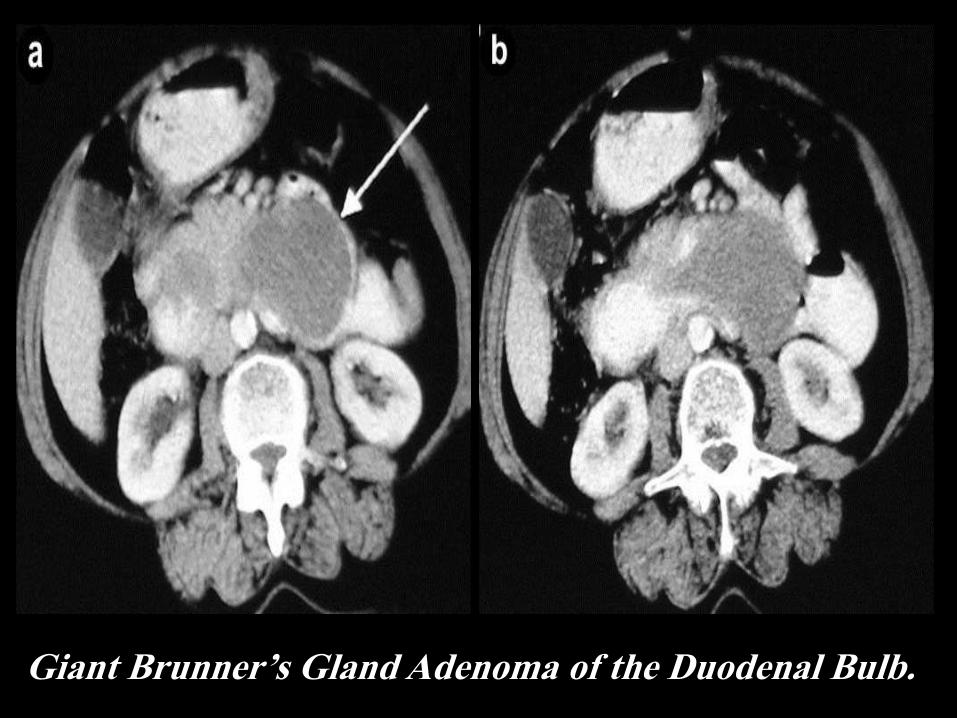
Giant Brunner’s Gland Adenoma of the Duodenal Bulb.

Barium study showing a well-defined lobular large adenoma.

Jejunal adenoma.

Axial CT shows large clearly delineated mesenterial
mass compressing the IVC, PA proven desmoid tumor

Small hemangioma.

Adenocarcinoma of the small bowel.
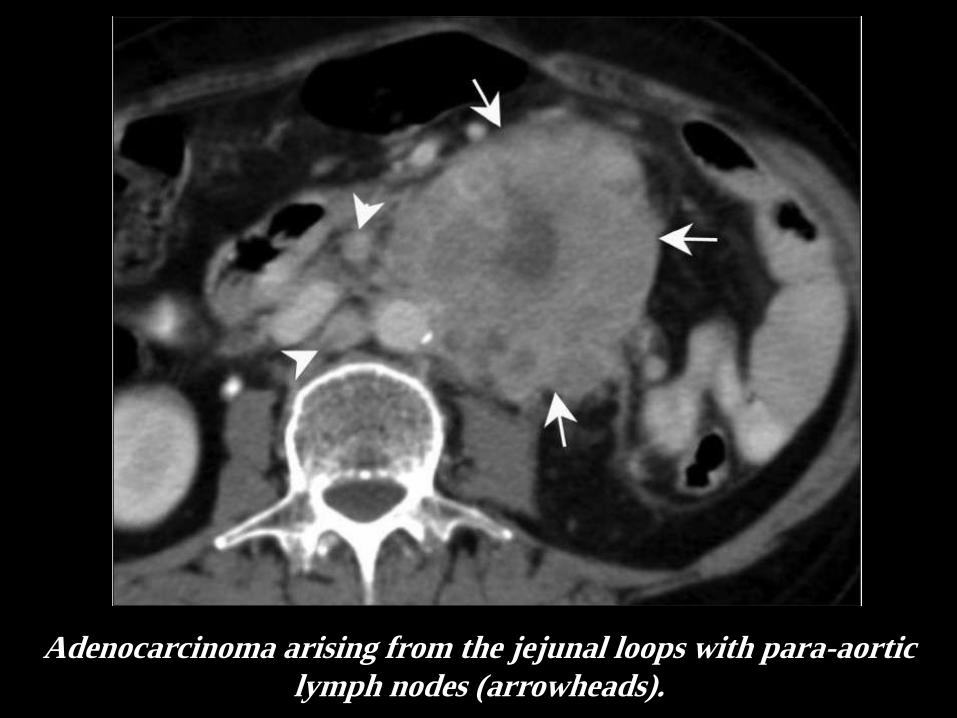
Adenocarcinoma arising from the jejunal loops with para-aortic
lymph nodes (arrowheads).

Adenocarcinoma of the ileum Adenocarcinoma of the Jejunum.

Axial CT. Thick walled jejunal mass with dilated
lumen, PA: adenocarcinoma
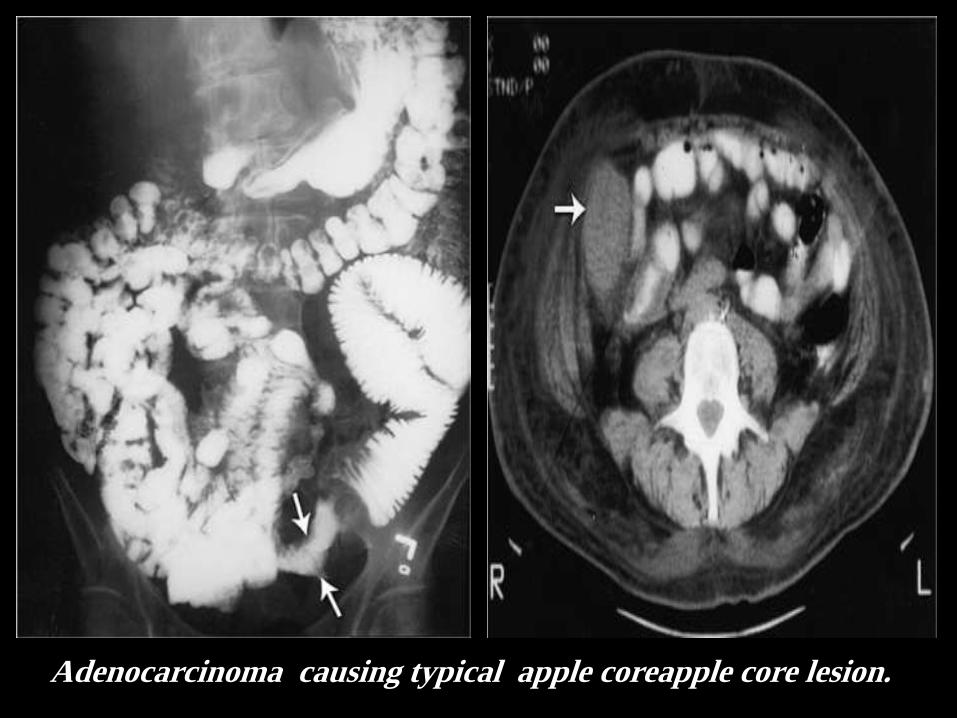
Adenocarcinoma causing typical apple coreapple core lesion.
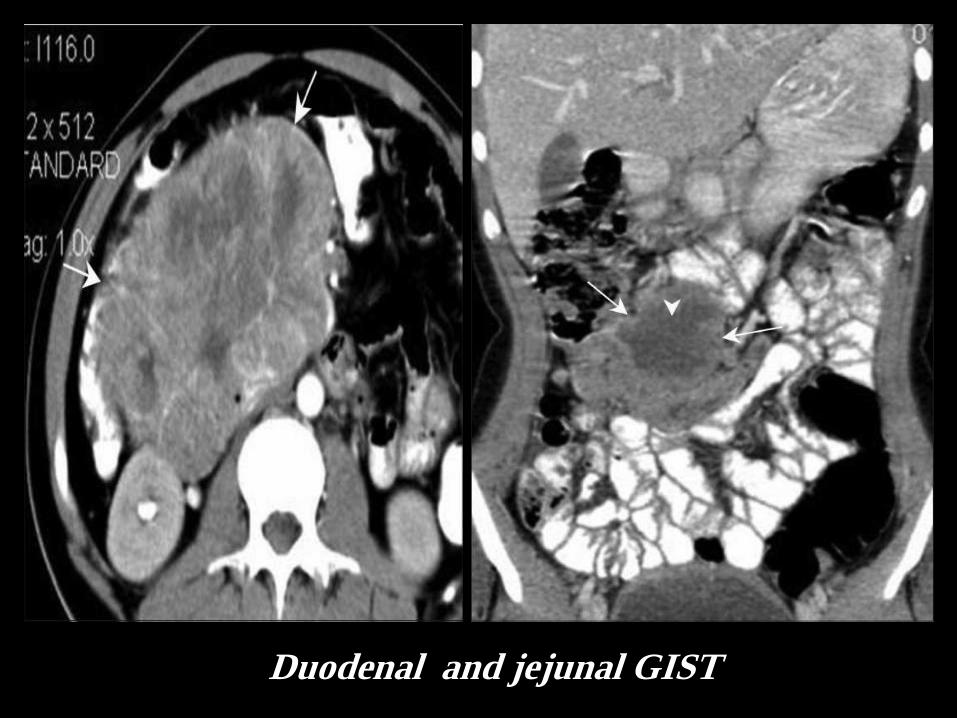
Duodenal and jejunal GIST
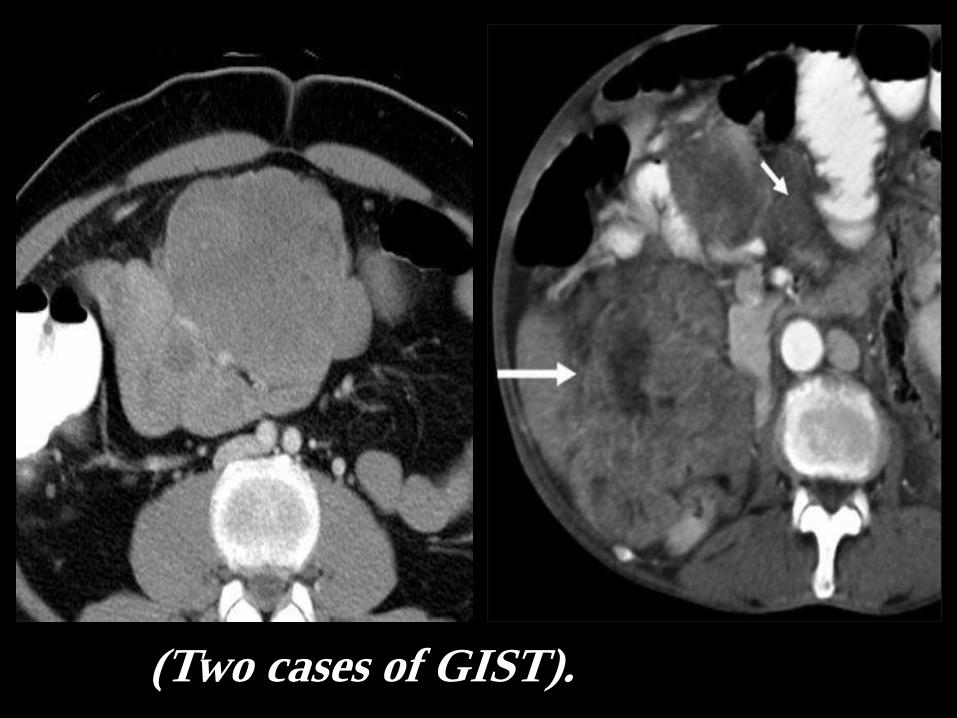
(Two cases of GIST).
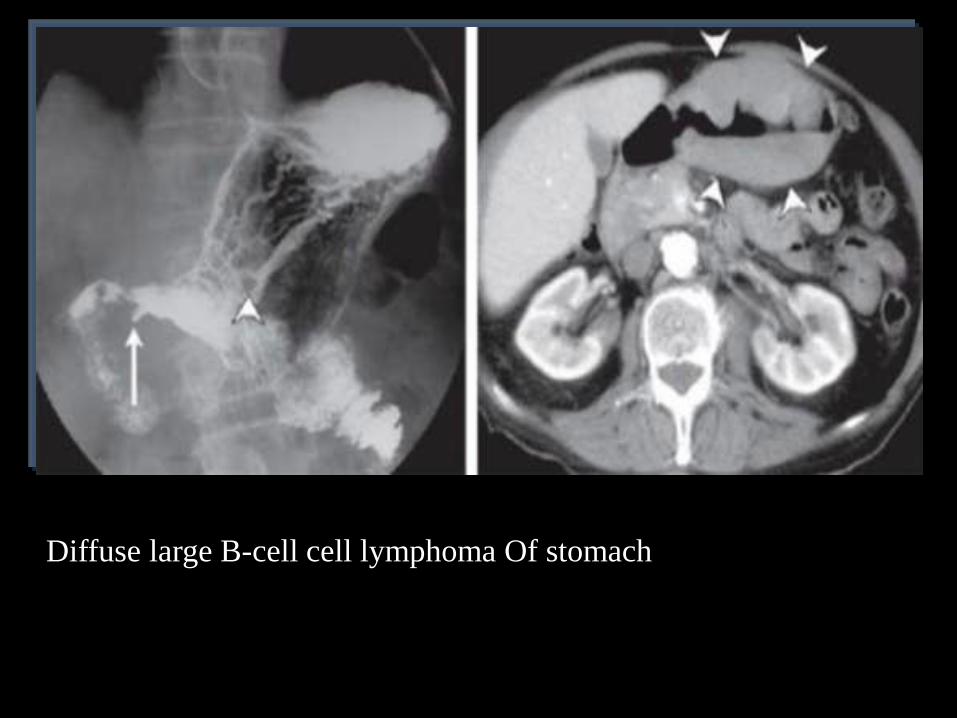
Diffuse large B-cell cell lymphoma Of stomach

High -grade B-cell lymphoma Of stomach

Aneurysmal diltation (arrow)of the
lumen of the terminal ilieum along
with mass effect (lymphoma)
SBFT show diffuse nodular
Fold thickening of most of the SB
(LYMPHOMA)



Small Bowel Lymphoma

Small Bowel Lymphoma.

Low-grade MALT lymphoma Of stomach

Diffuse B-cell cell lymphoma
Of stomach
Diffuse large B-cell cell
lymphoma Of stomach
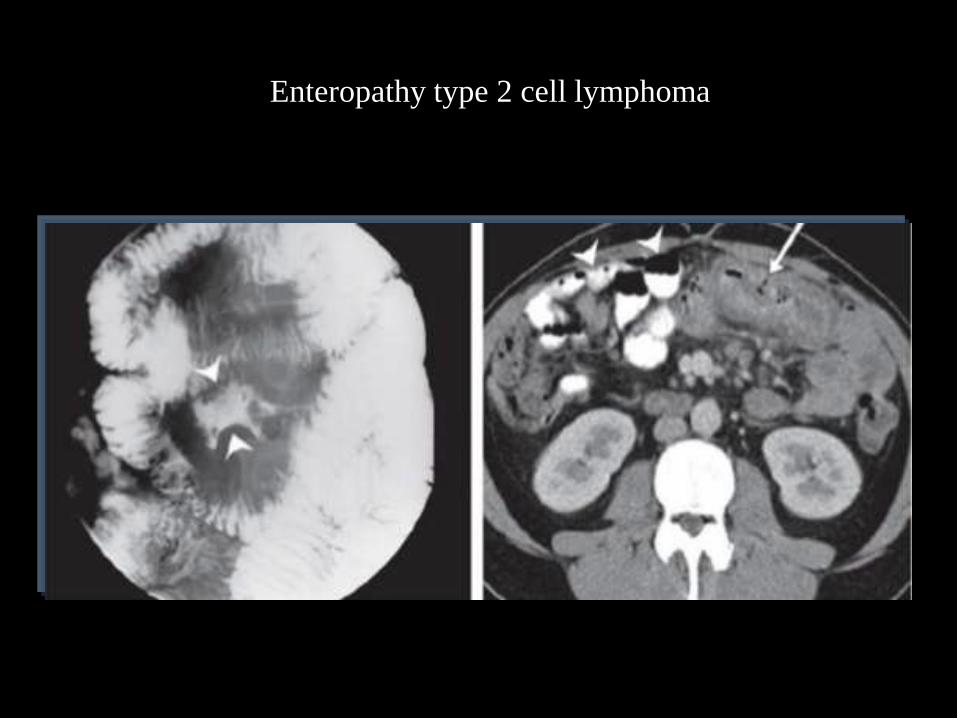
Enteropathy type 2 cell lymphoma

Burkett's lymphoma.

Leiomyosarcoma of small bowel.

Carcinoid tumour of the small bowel.

Carcinoid tumour of the small bowel and liver.

Axial CT. Speculated calcified mesenterial mass and dilated
small bowel loops, consistent with small bowel carcinoid.

Satellite mesenteric
mass although the
primary carcinoid
tumor.

Axial nonenhanced CT images and fused FDG-PET images. Two sites of
wall thickening in the small bowel with marked FDG uptake, in a
patient with metastasized melanoma

Axial and coronal CT of intussuscepting luminal mass
of small bowel on right side in patient with melanoma

Metastasis from carcinoma breast.


MRI polypoidal rectal tumor

Leiomyosarcoma of small bowel.

MRI
Thick bowel wall.
Engorged mysentery.

SBFT: Recurrent
SBO shows mucosal
edema and
stricturing of the
terminal ileum and the
caecum..

Coronal T1 fat sat and coronal T2 shows enhancing clearly delineated luminal
mass in the right upper quadrant, PA proven small bowel hemangioma.

Axial T2 images. Multifocal small bowel intussusceptions
in patient with Peutz Jeghers syndrome.

Homogenously
enhancing
polypoid lesions
(arrows) in Peutz
Jeghers syndrome

Axial T2 image. Unilocular benign mass with shouldering margins in the duodenum.

Virtual colonoscopy: value of 2D images.
(A) Large polypoid intraluminal filling defect on an endoluminal 3D
image. (B) The internal density of the mass is fatty on the two
dimensional image, pathognomonic of a benign lipoma

virtual CT colonoscopy versus CT. A. CT: axial: Missed polyp of the ileocaecal valve. The
lesion (arrow) can be misinterpreted as stool or prominent valve. B. CT colonoscopy: showed
well the polyp (arrow). The polyp was missed in fiberoptic colonoscopy (blind spot)

Fibreoptic VS virtual endoscopy
Better visualization of the entire colon, unlike
blind spots of fiberoptic colonoscopy

ANGIOGRAPHY
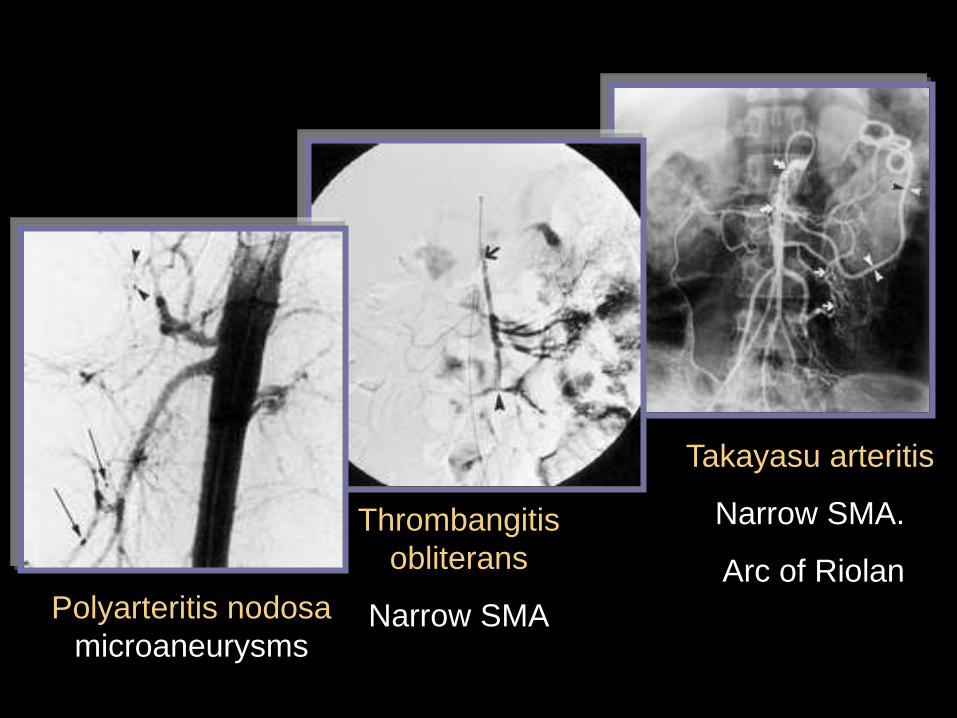
Takayasu arteritis
Narrow SMA.
Arc of Riolan
Thrombangitis
obliterans
Narrow SMA Polyarteritis nodosa
microaneurysms

Angiography
PAN: microaneurysms

NUCLEAR MEDICINE
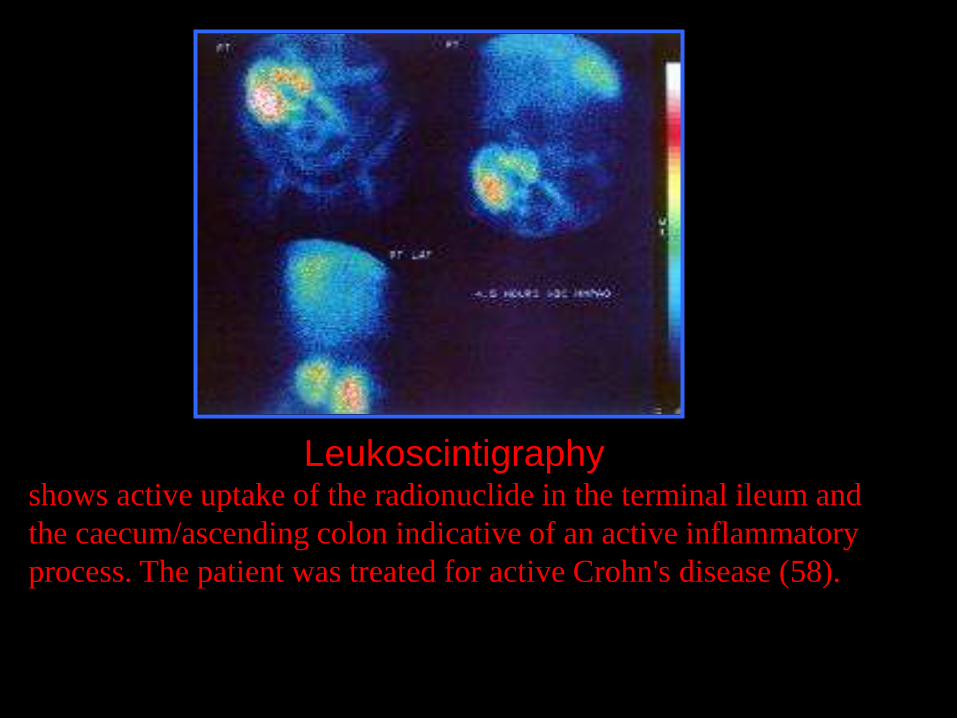
Leukoscintigraphy shows active uptake of the radionuclide in the terminal ileum and
the caecum/ascending colon indicative of an active inflammatory
process. The patient was treated for active Crohn's disease (58).

Tc- RBCs:
Obscure bleeding: small bowel carcinoidi
a case of repeated episodes of bleeding per rectum. The scan
shows extravasation of radiolabelled blood in a loop of ileum
(arrow). Intra-operative enteroscopy revealed ulcerating
Carcinoid (5mm in diameter) .

Plain radiographs: acute abdomen.
Ba studies: mucosal pattern.
CT: Screening: acute
Etiology: wall thickening
Extra-intestinal
Endoscopy, angio, isotopes: selected