

ZVEI-Jahreskongress 2013
DRG-Systeme in EuropaDRG-Systeme in Europa
Dr. Alexander Geissler, Dipl.-Ing.
Department of Health Care Management (MiG)
Berlin University of Technology
European Observatory on Health Systems and Policies
WHO Collaborating Centre for Health Systems, Research and Management
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 1

Diagnosis-related Groups
Eine DRG ist eine Gruppe von Patienten mit ähnlichen klinischen Merkmalen, derenBehandlung zugleich einen vergleichbar hohen Ressourcenverbrauch aufweist.
DRG-Systeme sind medizinisch-ökonomische Patientenklassifikationssysteme, diePatienten jeweils genau einer Fallgruppe zuordnen.
Patienten-
Definition
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 2
Diagnosis-related Group (DRG)
Behandlungs-merkmale
(Prozeduren, Technologie, Kosten, etc.)
Patienten-merkmale
(Geschlecht, Alter,
Diagnosen, etc.)

Erlöse/Kosten Gesamtkosten
DRG-basierte Fallpauschalenerlöse
Erlössteigerung(z. B. durch Mengenausweitung,
Verhandlung von Zusatzentgelten)
Diagnosis-related Groups
DRG-basierte Fallpauschalen induzieren eine Yardstick-Competition. Krankenhäuser konkurrieren nicht direkt gegeneinander sondern gegen einen variablen und vorgegebenen Preis je DRG.
Anreize
Kurzlieger(Abschläge)
Langlieger(Zuschläge)
Obere Verweildauergrenze
Verweildauer
UntereVerweildauergrenze
Kostenreduktion ( z. B. durch Verringerung des Personal- und
Technologieeinsatzes)
Verringerung der Verweildauer
Normallieger
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 3

Land 19
80
19
85
19
90
19
95
20
00
20
05
20
10
Originärer Zweck Zweck in 2010
Deutschland Vergütung Vergütung
England Patientenklassifikation Vergütung
Estland Vergütung Vergütung
FinnlandTransparenz,
Benchmarking
Planung, Benchmarking,
Rechnungsstellung
Frankreich Transparenz Vergütung
Irland Budgetallokation Budgetallokation
Diagnosis-related GroupsZeitlinien
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 4
Irland Budgetallokation Budgetallokation
Niederlande Vergütung Vergütung
Österreich Budgetallokation Budgetallokation, Planung
Polen Vergütung Vergütung
Portugal Transparenz Budgetallokation
Schweden Vergütung Vergütung, Benchmarking
Spanien
(Katalonien)Vergütung Vergütung, Benchmarking
19
80
19
85
19
90
19
95
20
00
20
05
20
10
Einführung von DRGs
Nutzung von DRGs zur Krankenhausvergütung

Excluded costs(e.g. for infrastructure; in U.S. also physician services)
Payments for non-patient care activities(e.g. teaching, research, emergency availability)
Payments for patients not classified into DRG system(e.g. outpatients, day cases, psychiatry, rehabilitation)
Diagnosis-related GroupsBandbreite
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 5
DRG-based case payments,
DRG-based budget allocation(possibly adjusted for outliers, quality etc.)
(e.g. outpatients, day cases, psychiatry, rehabilitation)
Other types of payments for DRG-classified patients(e.g. global budgets, fee-for-service)
Additional payments for specific activities for DRG-classified patients (e.g. expensive drugs, innovations),
possibly listed in DRG catalogues

Original DRG system DRG systemDRG system DRG system
Diagnosis-related GroupsBandbreite
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 6
Psychiatry Day casesAcute
inpatient careOutpatient care Rehabilitation
Original
DRG
systems
DRG system(included in orseparate fromoriginal DRGs)
DRG system(included in orseparate fromoriginalDRGs)
DRG system(identical ordifferent to
original DRGs)
DRG system(included in orseparate fromoriginal DRGs)

DRG-Systembausteine
Patienten-
Datenerfassung
Preissetzung
Vergütung
• Demografische Daten• Klinische Daten• Kostendaten• Stichprobengröße,
Revisionsintervall
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 7
Patienten-
klassifikation
• Diagnosen• Prozeduren• Schweregrad• Revisionsintervall
• Relativ- bzw.
Kostengewichte• Basisraten• Preise/ Tarife • Durchschnittskosten
vs. „Best practice”• Revisionsintervall
• Leistungsbegrenzung
• Lang- und Kurzlieger• Hochkostenfälle• Qualität• Verhandlungen• Revisionsintervall
Import

Patientenklassifikation
Kopiert, weiter- oder selbstentwickelt?
The great-grandfather
The grandfathers
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 8
The grandfathers
The fathers
Patientenklassifikation
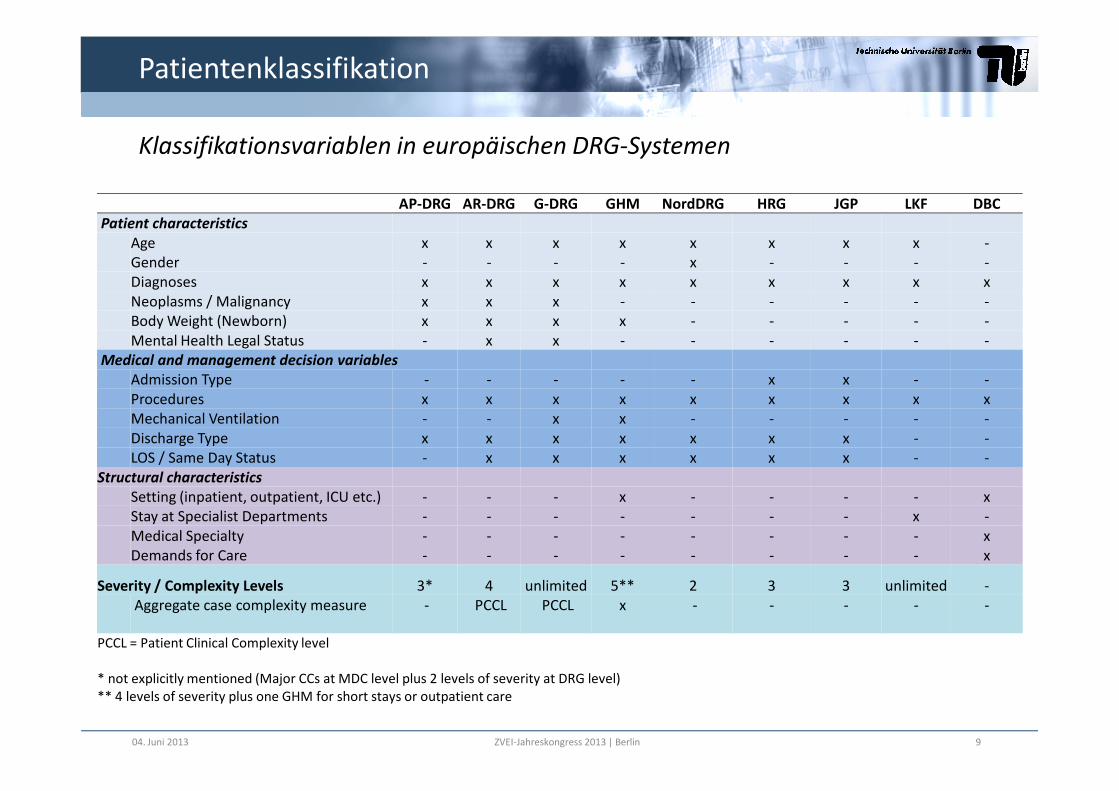
Klassifikationsvariablen in europäischen DRG-Systemen
AP-DRG AR-DRG G-DRG GHM NordDRG HRG JGP LKF DBC
Patient characteristics
Age x x x x x x x x -Gender - - - - x - - - -Diagnoses x x x x x x x x xNeoplasms / Malignancy x x x - - - - - -Body Weight (Newborn) x x x x - - - - -Mental Health Legal Status - x x - - - - - -
Medical and management decision variables
Admission Type - - - - - x x - -Procedures x x x x x x x x x
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 9
Procedures x x x x x x x x xMechanical Ventilation - - x x - - - - -Discharge Type x x x x x x x - -LOS / Same Day Status - x x x x x x - -
Structural characteristics
Setting (inpatient, outpatient, ICU etc.) - - - x - - - - xStay at Specialist Departments - - - - - - - x -Medical Specialty - - - - - - - - xDemands for Care - - - - - - - - x
Severity / Complexity Levels 3* 4 unlimited 5** 2 3 3 unlimited -Aggregate case complexity measure - PCCL PCCL x - - - - -
PCCL = Patient Clinical Complexity level
* not explicitly mentioned (Major CCs at MDC level plus 2 levels of severity at DRG level)** 4 levels of severity plus one GHM for short stays or outpatient care

PatientenklassifikationUnterschiede in der Patientenklassifikation
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 10
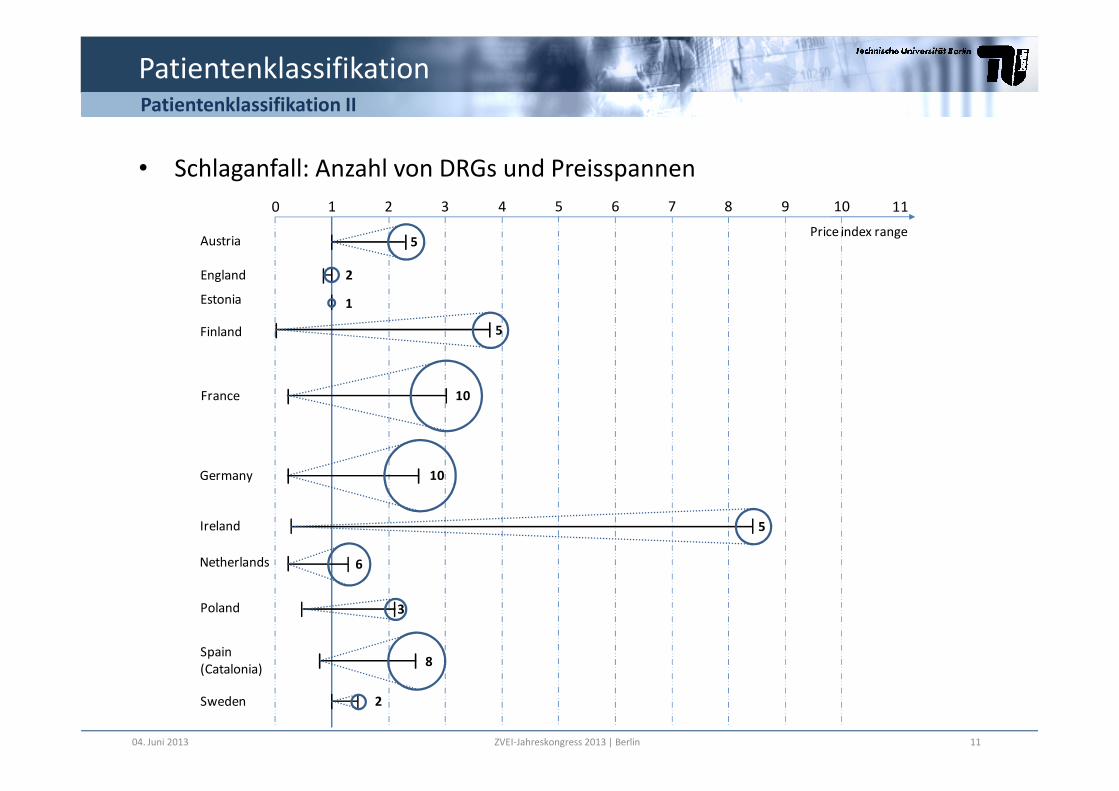
PatientenklassifikationPatientenklassifikation II
• Schlaganfall: Anzahl von DRGs und Preisspannen
1 2 3 4
Austria
England
0
5
Estonia
Finland
France
Price index range
2
5
5 6 7 8 9 10 11
10
1
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 11
6
Poland
Germany 10
France
Ireland
Spain(Catalonia)
Sweden
Netherlands
10
5
8
2
3

Patientenklassifikation
LandSystem
(Herkunft)
Diagnose-
klassifikationProzedurklassifikation
Anzahl
Gruppen
in 2008
MDC/
Kapitel
Deutschland G-DRG (AR-DRG) ICD-10-GM OPS (Operationen- und Prozedurenschlüssel) 1200 26
EnglandHRG (selbst
entwickelt)ICD-10
OPCS (Classification of Surgical Operations and
Procedures)1389 23
EstlandNordDRG (HCFA-
DRG)ICD-10 NCSP (Nomesco Classification of Surgical Procedures) 794 28
FinnlandNordDRG (HCFA-
DRG)ICD-10-FI NCSP-FI (Finnische NCSP-Adaption) 794 28
Frankreich GHM (HCFA-DRG) CIM-10 CCAM (Classification Commune des Actes Médicaux) 2297 28
Diagnosen und Prozeduren
Frankreich GHM (HCFA-DRG) CIM-10 CCAM (Classification Commune des Actes Médicaux) 2297 28
Irland AR-DRG ICD-10-AM ACHI (Australian Classification of Health Interventions) 665 24
NiederlandeDBC (selbst
entwickelt)ICD-10 Elektronische DBC Typeringslijst ~30 000 -
ÖsterreichLKF (selbst
entwickelt)
ICD-10-
BMSG-2001Leistungskatalog 979 -
Polen JGP (HRG) ICD-10 ICD-9-CM 518 16
Portugal AP-DRG ICD-9-CM ICD-9-CM 679 25
Spanien AP-DRG ICD-9-CM ICD-9-CM 679 25
SchwedenNordDRG (HCFA-
DRG)ICD-10-SE
KVÅ-Klassifikation av vårdåtgärder (Schwedische NCSP-
Adaption)794 28
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 12
Quasi-Standard Kein Standard verfügbar

DRG-Systembausteine
Patienten-
Datenerfassung
Preissetzung
Vergütung
• Demografische Daten• Klinische Daten• Kostendaten• Stichprobengröße,
Revisionsintervall
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 13
Patienten-
klassifikation
• Diagnosen• Prozeduren• Schweregrad• Revisionsintervall
• Relativ- bzw.
Kostengewichte• Basisraten• Preise/ Tarife • Durchschnittskosten
vs. „Best practice”• Revisionsintervall
• Leistungsbegrenzung
• Lang- und Kurzlieger• Hochkostenfälle• Qualität• Verhandlungen• Revisionsintervall
Import

DRGs have improved the cost accounting utilization and vice versa
Datenerfassung
Cost accounting
Required for self
developed DRG systems
Enables hospitals to detect sources
of resource consumption
Kostendaten
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 14
Hospital management
- Internal budget planning
- Benchmarking (within and across hospitals)
- Monitoring of service delivery
DRG system development
- Precise (fair) payment rate calculation
- Continuous system updates
- Transparency
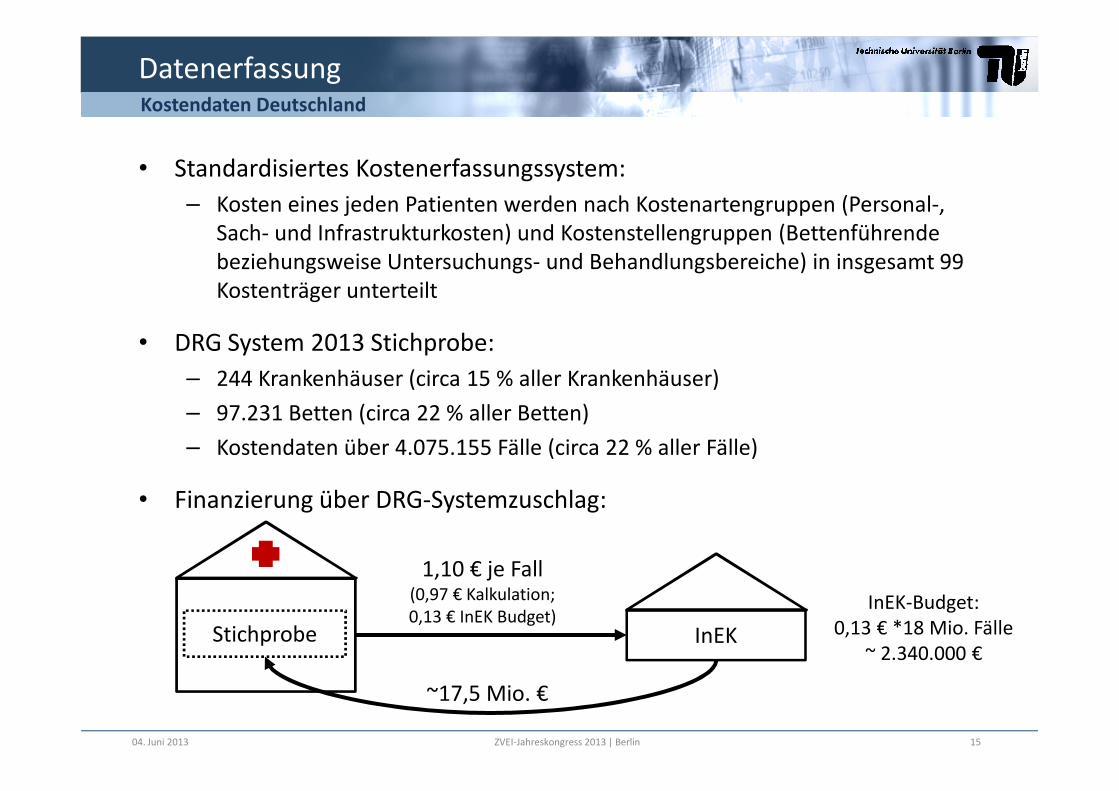
• Standardisiertes Kostenerfassungssystem:
– Kosten eines jeden Patienten werden nach Kostenartengruppen (Personal-, Sach- und Infrastrukturkosten) und Kostenstellengruppen (Bettenführende beziehungsweise Untersuchungs- und Behandlungsbereiche) in insgesamt 99 Kostenträger unterteilt
• DRG System 2013 Stichprobe:
– 244 Krankenhäuser (circa 15 % aller Krankenhäuser)
DatenerfassungKostendaten Deutschland
– 97.231 Betten (circa 22 % aller Betten)
– Kostendaten über 4.075.155 Fälle (circa 22 % aller Fälle)
• Finanzierung über DRG-Systemzuschlag:
InEKStichprobe
1,10 € je Fall(0,97 € Kalkulation; 0,13 € InEK Budget)
InEK-Budget:0,13 € *18 Mio. Fälle
~ 2.340.000 €
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 15
~17,5 Mio. €

Cost- Element Groups
Lab
ou
rco
sts
of
the
ph
ysic
ian
sta
ff
Lab
ou
rco
sts
of
the
nu
rsin
g st
aff
Lab
ou
rco
sts
of
the
adm
inis
trat
ive
and
tech
nic
al s
taff
: Dru
g co
sts
: Dru
g co
sts
(in
div
idu
al c
ost
s/ a
ctu
alc
nsu
mti
on
)
: co
sts
of
imp
lan
ts a
nd
gra
fts
: Mat
eria
l co
sts
(wit
ho
ut
dru
gs,
imp
lan
ts a
nd
gra
fts)
: Mat
eria
l co
sts
(in
div
idu
al c
ost
s/
actu
al c
on
sum
pti
on
, wit
ho
ut
dru
gs,
imp
lan
ts/
graf
ts
: Med
ical
infr
astr
uct
ure
cost
s
: No
n-
med
ical
infr
astr
uct
ure
cost
s
Datenerfassung
Bottom-up microcosting
Example: DRG I03A
(Hip revision or replacement with cc)
Cost weight: 4,192
Kostendaten Deutschland Beispiel
1: L
abo
ur
2: L
abo
ur
3: L
abo
ur
tech
nic
al
4a: D
rug
4b: D
rug
cost
s (i
nd
ivid
ual
co
sts/
act
ual
c n
sum
tio
n
5: c
ost
s o
f im
pla
nts
an
d g
raft
s
6a: M
ater
ial c
ost
s (w
ith
ou
t d
rugs
,im
pla
nts
6b: M
ater
ial c
ost
s (i
nd
ivid
ual
co
sts/
ac
tual
im
pla
nts
7: M
edic
al
8: N
on
Labour Material Infrastructure Total
Co
st-
Ce
ntr
e G
rou
ps
01: Normal ward
Ho
spit
al
un
its
wit
h
be
ds
654 1744 80 156 41 ---- 131 19 371 1358 4554
02: Intensive care unit 152 360 10 45 11 ---- 60 1 64 179 881
03: Dialysis unit ---- ---- ---- ---- ---- ---- ---- ---- ---- ---- 0
04: Operating room
Dia
gn
ost
ic a
nd
tre
atm
en
t a
rea
s
623 ---- 401 23 32 1282 286 109 264 360 3380
05: Anaesthesia 356 ---- 236 30 2 85 5 50 112 875
06: Maternity room ---- ---- ---- ---- ---- ---- ---- ---- ---- ---- 0
07: Cardiac diagnostics/ therapy 2 ---- 2 ---- ---- ---- 1 2 1 1 8
08: Endoscopic diagnostics/ therapy 3 ---- 3 ---- 1 ---- 2 ---- 2 2 12
09: Radiology 46 ---- 67 1 ---- 2 14 41 24 45 240
10: Laboratories 18 ---- 110 6 339 ---- 75 82 12 50 694
11: Other diagnostic and therapeutic areas 36 2 271 1 ---- ---- 14 16 15 111 468
Total 1890 2106 1180 261 424 1283 669 276 803 2219 11 112
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 16

Datenerfassung
CountryPresence of mandatory
cost accounting system
Presence of national
costing guidelinesPresence of own cost data
Austria --- --- X
England X X X
Estonia --- --- X
Finland --- --- X
Kostendaten in Europa I
Finland --- --- X
France --- X X
Germany --- X X
Ireland --- X ---
Poland --- --- ---
Portugal X X ---
the Netherlands X X X
Spain/Catalonia --- --- ---
Sweden --- X X
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 17

Datenerfassung
Number (share) of cost collecting
hospitals
Overhead
allocation
Indirect cost
allocation
Direct cost
allocation
Data checks on
reported cost data
Austria20 reference hospitals (about 8% of
all hospitals)varying by hospital
varying by hospital
mainly grosscosting
regional authority, regularly
England all hospitals direct methodweighting statistics
top down microcosting
national authority, annually
Estoniahospitals contracted with the national
health insurance funddirect method
mainly mark-up percentage
mainly top down
microcosting
national authority, annually
Finland
5 reference hospitals meeting particular cost accounting standards
(about 30% of specialised care)direct method
weighting statistics
bottom up microcosting
no (responsibility of hospitals)
99 volunteering hospitals
Kostendaten in Europa II
France
99 volunteering hospitals participating in the hospital cost
database ENCC (about 13% of inpatient admissions)
step down method
weighting statistics
mainly top down
microcosting
regional authority, annually
Germany
about 225 volunteering hospitals meeting InEK cost accounting
standards (about 13% of all hospitals)
preferably step down method
weighting statistics
bottom up microcosting
national authority, annually
Netherlands
resource use: all hospitals; unit costs: 15-25 volunteering general hospitals
(about 24% of all hospitals)direct method
weighting statistics
bottom up microcosting
national authority, annually
Swedenhospitals with case costing systems (about 62% of inpatient admissions)
direct methodweighting statistics
bottom up microcosting
national and regional authority, annually
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 18
(Ireland, Poland, Portugal and Spain import DRG cost weights from abroad)

DRG-Systembausteine
Patienten-
Datenerfassung
Preissetzung
Vergütung
• Demografische Daten• Klinische Daten• Kostendaten• Stichprobengröße,
Revisionsintervall
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 19
Patienten-
klassifikation
• Diagnosen• Prozeduren• Schweregrad• Revisionsintervall
• Relativ- bzw.
Kostengewichte• Basisraten• Preise/ Tarife • Durchschnittskosten
vs. „Best practice”• Revisionsintervall
• Leistungsbegrenzung
• Lang- und Kurzlieger• Hochkostenfälle• Qualität• Verhandlungen• Revisionsintervall
Import

Preissetzung
• Relativgewichte:
– DRGs werden relativ zueinander gewichtet
– Relativgewicht*Basisrate = DRG-basierte Vergütung
– Starke Verwendung in Europa
– Adjustierung der Vergütung nur für alle DRGs gleichzeitig möglich
Relativgewichte vs. Tarife/Preise
• Tarife/Preise
– Direkte Preise durch Berechnung der Durchschnittskosten je DRG
– Tarife/Preise global oder für einzelne DRGs adjustierbar
– Eröffnet mehr Flexibilität für Preisverhandlungen
– Fördert Intransparenz
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 20

DRG-Systembausteine
Patienten-
Datenerfassung
Preissetzung
Vergütung
• Demografische Daten• Klinische Daten• Kostendaten• Stichprobengröße,
Revisionsintervall
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 21
Patienten-
klassifikation
• Diagnosen• Prozeduren• Schweregrad• Revisionsintervall
• Relativ- bzw.
Kostengewichte• Basisraten• Preise/ Tarife • Durchschnittskosten
vs. „Best practice”• Revisionsintervall
• Leistungsbegrenzung
• Lang- und Kurzlieger• Hochkostenfälle• Qualität• Verhandlungen• Revisionsintervall
Import
Vergütung
• Vergütung in Deutschland bisher rein ökonomisch getrieben
• Ergebnisqualität wird trotz zahlreicher Qualitätsinitiativen nicht berücksichtigt
• Andere europäische Länder nicht deutlich weiter
Diskussion
• Vorreiter USA: „present on admission marker“
• Frage: Vergütungsadjustierung vs. „voting by feet“
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 22

Vielen Dank fürIhre Aufmerksamkeit!
23
Ihre Aufmerksamkeit!
Alle Folien und mehr Material auf:www.mig.tu-berlin.de
undwww.eurodrg.eu
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin
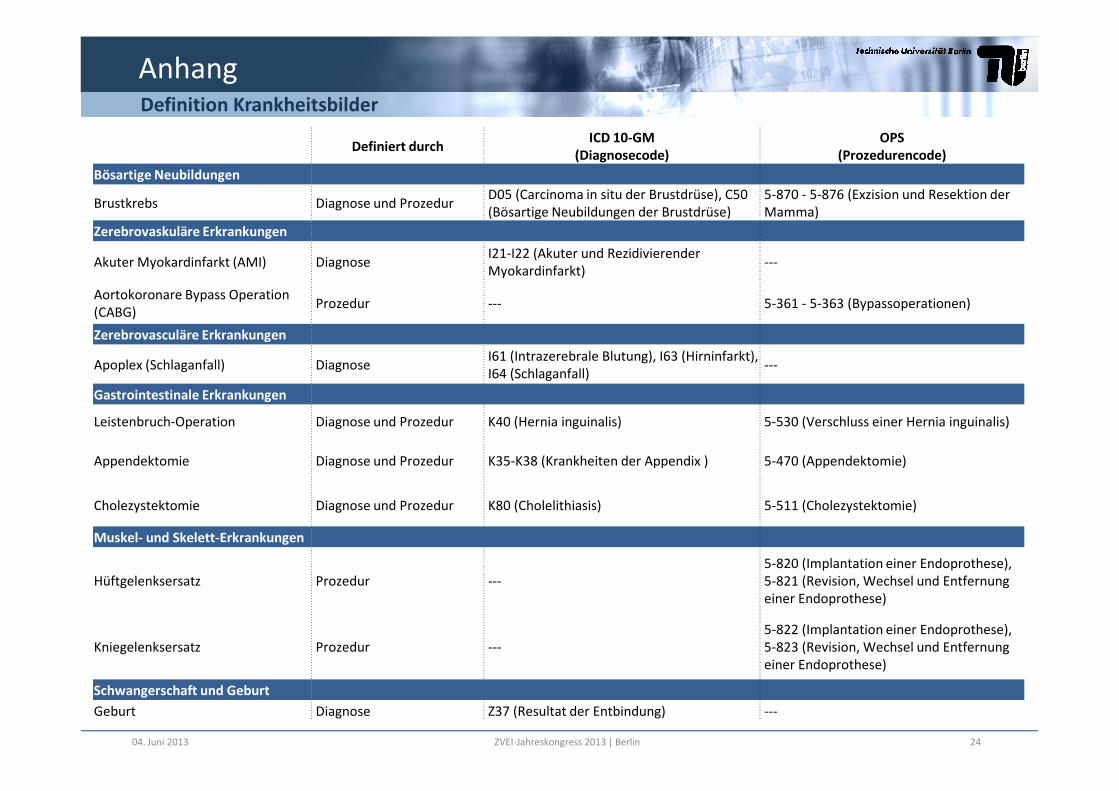
Definiert durchICD 10-GM
(Diagnosecode)
OPS
(Prozedurencode)
Bösartige Neubildungen
Brustkrebs Diagnose und ProzedurD05 (Carcinoma in situ der Brustdrüse), C50 (Bösartige Neubildungen der Brustdrüse)
5-870 - 5-876 (Exzision und Resektion der Mamma)
Zerebrovaskuläre Erkrankungen
Akuter Myokardinfarkt (AMI) DiagnoseI21-I22 (Akuter und Rezidivierender Myokardinfarkt)
---
Aortokoronare Bypass Operation(CABG)
Prozedur --- 5-361 - 5-363 (Bypassoperationen)
Zerebrovasculäre Erkrankungen
Apoplex (Schlaganfall) DiagnoseI61 (Intrazerebrale Blutung), I63 (Hirninfarkt), I64 (Schlaganfall)
---
Gastrointestinale Erkrankungen
AnhangDefinition Krankheitsbilder
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 24
Gastrointestinale Erkrankungen
Leistenbruch-Operation Diagnose und Prozedur K40 (Hernia inguinalis) 5-530 (Verschluss einer Hernia inguinalis)
Appendektomie Diagnose und Prozedur K35-K38 (Krankheiten der Appendix ) 5-470 (Appendektomie)
Cholezystektomie Diagnose und Prozedur K80 (Cholelithiasis) 5-511 (Cholezystektomie)
Muskel- und Skelett-Erkrankungen
Hüftgelenksersatz Prozedur ---5-820 (Implantation einer Endoprothese), 5-821 (Revision, Wechsel und Entfernung einer Endoprothese)
Kniegelenksersatz Prozedur ---5-822 (Implantation einer Endoprothese), 5-823 (Revision, Wechsel und Entfernung einer Endoprothese)
Schwangerschaft und Geburt
Geburt Diagnose Z37 (Resultat der Entbindung) ---
Anhang
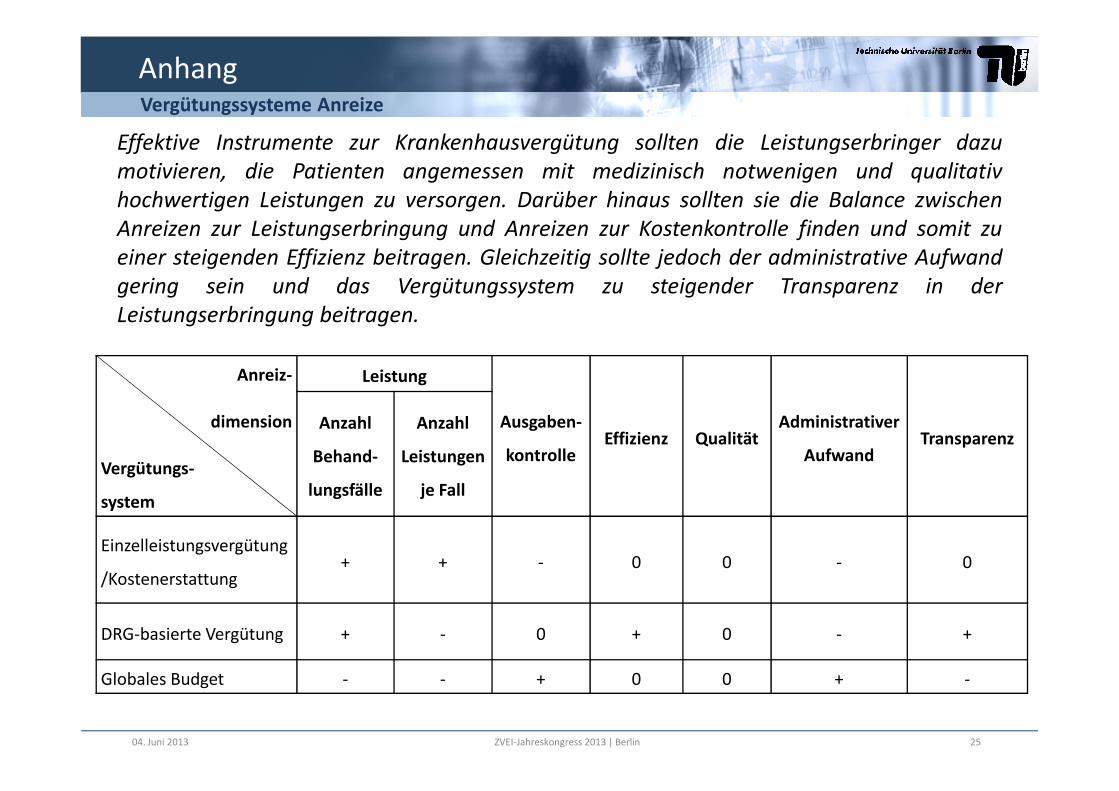
Anreiz- Leistung
Effektive Instrumente zur Krankenhausvergütung sollten die Leistungserbringer dazu
motivieren, die Patienten angemessen mit medizinisch notwenigen und qualitativ
hochwertigen Leistungen zu versorgen. Darüber hinaus sollten sie die Balance zwischen
Anreizen zur Leistungserbringung und Anreizen zur Kostenkontrolle finden und somit zu
einer steigenden Effizienz beitragen. Gleichzeitig sollte jedoch der administrative Aufwand
gering sein und das Vergütungssystem zu steigender Transparenz in der
Leistungserbringung beitragen.
Vergütungssysteme Anreize
dimension
Vergütungs-
system
Ausgaben-
kontrolleEffizienz Qualität
Administrativer
AufwandTransparenz
Anzahl
Behand-
lungsfälle
Anzahl
Leistungen
je Fall
Einzelleistungsvergütung
/Kostenerstattung+ + - 0 0 - 0
DRG-basierte Vergütung + - 0 + 0 - +
Globales Budget - - + 0 0 + -
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 25
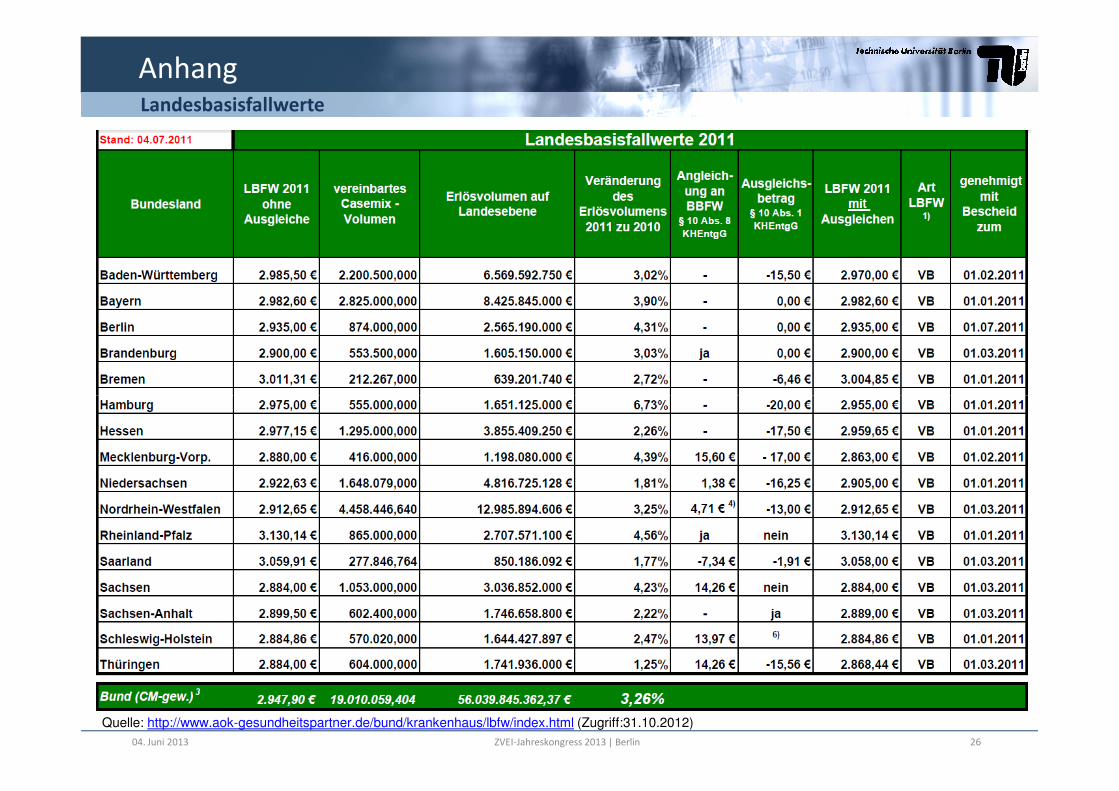
AnhangLandesbasisfallwerte
Quelle: http://www.aok-gesundheitspartner.de/bund/krankenhaus/lbfw/index.html (Zugriff:31.10.2012)
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 26

The G-DRG system
Tasks and stakeholders of the DRG system development
Health Ministry (federal, state)
Self-Administration (DKG, GKV, PKV)
AdministrationHealth Policy
Goals
and
monitoring
Forming
a legal
frameworkOther Institutions (HTA, quality)
Consultation Development
DIMDI (German Institute of Medical Information and Documentation)
InEK (German DRG Institute)
monitoring framework
Technical
managementContribution
of expertise
Other Institutions (HTA, quality)
Variety of Institutions(Professional medical associations, industry groups)
G-DRG
System
04. Juni 2013 ZVEI-Jahreskongress 2013 | Berlin 27







