

Drug Distribution
Dr.Sabitri BeshraPG 1st yr
Dept of PharmacologySCBMCH,Cuttack
OUTLINE
1. Definition
2. Pattern of drug distribution.
3. Factors affecting distribution
4. Redistribution of drug
5. Apparent volume of distribution
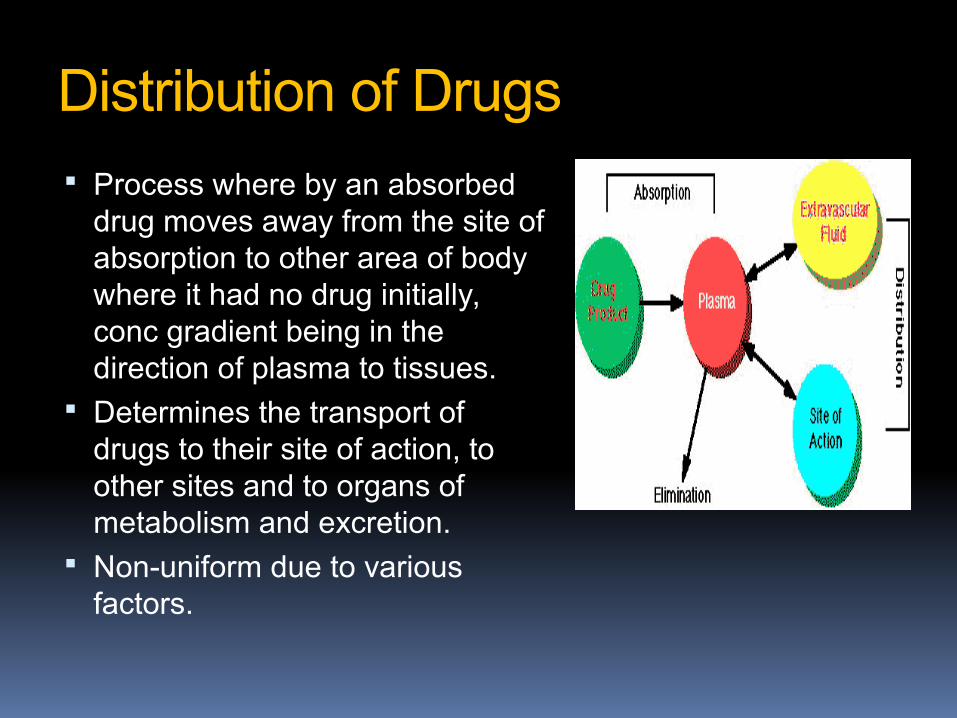
Distribution of Drugs Process where by an absorbed
drug moves away from the site of absorption to other area of body where it had no drug initially, conc gradient being in the direction of plasma to tissues.
Determines the transport of drugs to their site of action, to other sites and to organs of metabolism and excretion.
Non-uniform due to various factors.

PATTERNS of distribution
1.Largely confined to vascular system- E.g Plasma substitute like dextran. Drugs strongly bound to plasma protein
2.Troughout the body water- Alcohol, Sulphonamides(low molecular weight , water soluble
compounds)
3.Non uniform distribution- most drugs. 4.Concentrated specifically- in one or more tissues
which may or may not be their site of action. E.g Iodine – thyroid gland. Chloroquine- liver Chlorpromazine- uveal tract of eye. Griseofulvin- skin & nails.

Factors affecting distribution
1. Difference in regional blood flow
2. Physico-chemical charecteristics of the drug. Lipid solubility Capillary permeability Ionization at physiological pH
3. Extent of binding to plasma & tissue proteins
4. Disease
5. Special compartments and barrier
6. Presence of tissue specific transporters
7. Tissue volume &
8. Age
1. Regional blood flow
Well perfused- Brain, Heart, kidneys, liver & lungs. drugs preferentially to these organs
Moderately perfused- muscle, skin
Poorly perfused- fat
Least blood supply- bone & teeth
2. Physico-chemical properties-
M.W- <500-600 Da- easily cross the capillary membrane to ECF(except in CNS)
Lipophilicity –lipid soluble drugs cross membrane
Water soluble molecules and ions- <50 Da-enter cell through aqueous channels
drug pKa &pH of membrane Less ionisation=better distribution E.g phenobarbitone>salicylic acid
Physical properties contd
Larger size- restricted unless a specialised transport system exist for them
E.g Heparin-confined to plasma Due to high molecular wt Ionization
Basic drugs- readily enter into tissues & fluids
Lipid soluble compounds like lignocaine, propranolol & tricyclic anti-depressants –widely distributed and concentrated in-
Tissues like brain, liver and lung.
PLASMA PROTEINS-
Many drugs circulate in blood stream bound to plasma proteins.
Albumin-acidic drugs Álpha-1 acid glycoprotein- basic drugs. Ceruloplasmin-copper Transferrin- Iron Transcortin- steroid hormones Specific hormone carrier protein-
E.g Estrogen & Testosteron- sex hormone binding globulin
Thyroid hormone-thyroxin binding globulin Non specific binding –other plasma proteins(much
smaller extent)
DRUGS HIGHLY BOUND
ALBUMIN- Barbiturates Benzodiazepines NSAIDS Valproic acid Phenytoin Penicillins Sulfonamides Tetracyclines Tolbutamide warfarin
ALPHA1-ACID glycoprotein Beta-blockers Bupivacaine Lidocaine Disopyramine Imipramine Methadone Prazosin Quinidine verapamil
Plasma Protein Binding
Free drug Bound drug
Always equilibrium
This equilibrium will always be maintained whatever might be the amount of the drug in circulation at any time.

Protein- bounddrug
Protein- bounddrug
Free drugFree drug
TissuePlasma
The free drug concentration gradient drives transport across the membrane.
mem
b rane

Significance of plasma protein binding High degree of protein binding(reservoir)-
makes the drug long lasting. Affects distribution Pharmacologically inactive Non-diffusible Bound fraction-not available for Metabolism
& Excretion-Unless actively extracted by liver or kidney tubules
Displacement reaction among drugs.
Plasma protein binding
Reversible process usually. covalent binding of reactive drugs
eg.Alkylating agents occurs occasionally.
Bound fraction-determined by Drug concentration Affinity of binding sites No. of binding sites.

Plasma pr binding Cont-
At low conc of drugs- fraction bound is a function of Conc of binding sites Dissociation constant
At high conc of drug- No. of binding sites Drug concentration
Non-linear saturable process. Increasing conc of the drug can progressively saturate the
binding site. i.e fractional binding may be lower when large amounts of
the drug are given. Binding percentage refers to the usual therapeutic plasma
conc of a drug.

Drug displacement reaction
Many drugs compete with one another for adsorption on the same site of plasma proteins
Drug with greater affinity displaces other compound
Mostly protein bound drugs that are given in large enough dosage act as displacing agents.E.g Sulphonamides
Theoretically, the inc free drug conc (of displaced drug) could have the potential to cause greater adverse effect.
But practically, the consequences are not so serious because clearance inc proportionately
Exceptions to this may be dangerous
Warfarin is highly bound to a
Warfarin is highly bound to albumin
This means that most of the drug is sequestered on albumin and is inert.
W
W
W
W

DRUG DISPLACEMENT
Warfarin+ sulfonamide if given together?
If a sulfonamide is administered at same time, it will displaces warfarin from albumin.Leading to a rapid increase in the concentration of free warfarin in plasma. Because almost 100 percent is now free, compared with the initial small percentageProlonged PTT & inc risk of haemorrhage
W
WWW
S
S
S
S

Displacement reaction cont
Displacement of bilirubin from albumin In jaundiced premature neonates –disastrous As bilirubin metabolism is underdeveloped in
the premature liver. Unbound bilirubin can cross immature BBB-
can cause kernicterus. Permanent movement disturbance-choreo
athetosis
Displacement reacn cont
Displacing drugs in an epileptic pt stabilised on phenytoin reduces the total plasma phenytoin conc.- inc. elimination of free drug but there is no loss of efficacy
because- Conc. Of unbound(active) phenytoin at the new steady state
is unaltered.
As phenytoin dose is adjusted acc to measurements of its conc in plasma
Do not routinely distinguish bound from free phenytoin an inc dose may be prescribed -Resulting in toxicity.

Displacement reacn
salicylates displace methotrexate and reduce its secretion into nephron
Quinidine , verapamil & Amiodarone(anti-dysrhythmic drugs) displace Digoxin-
Reduced renal excretion Consequently cause severe dysrhythmias through Digoxin
toxicity.
Phenylbutazone, Salicylates displace Tolbutamide- Leading to hypoglycemia
Sulfonamides, probenecid, Indomethacin, phenytoin- warfarin

Drug displacement cont
Two highly bound drugs do not necessarily displace each other.
Their binding sites may not overlap. E.g Probenecid & Indomethacin highly bound to
albumin
Acidic drugs do not generally displace basic drugs and vice versa.
Plasma pr binding cont
Free drug is cleared from plasma and replaced by dissociation from plasma proteins and tissues.
In drugs eliminated by glomerular filtration-high protein binding delays elimination. E.g Tetracyclines
By active tubular secretion-no such effect- E.g Penicillins

Plasma pr binding Cont-
Mass-action relationship determine the unbound and bound concentration.
Most drugs- extent of binding & unbound fraction are relatively constant as therapeutic range of plasma conc is limited.
Extent of binding- depends on individual compound Small chemical change can alter protein binding. .e.g
Benzodiazepines Flurazepam-10% Alprazolam-70% Lorazepam-90% Diazepam-99%


TISSUE BINDING
Many drugs accumulate in tissues at higher conc than those in the extracellular fluids and blood.
E.g -long term adm of anti malarial agent Quinacrine conc in liver may be much higher than in blood
May be due to-Active transport or binding . Reservoir-prolongs drug action in same tissue or
at a distant site. Local toxicity-E.g - Aminoglycoside –Gentamycin
in kidney & vestibular system
Drugs concentrated in tissues
Skeletal muscle,heart- Digoxin, Emetine Liver- chloroquine, tetracycline, emetine, digoxin Kidney- digoxin, chloroquine, emetine Thyroid- Iodine Brain- chlorpromazine, acetazolamide, Isoniazid Retina- chloroquine Iris- ephedrine, atropine Bone & Teeth- tetracyclines, bisphosphonates Adipose tissue- thiopentone, ether, minocycline,
phenoxybenzamine, DDT
BONE
1. Tetracycline antibiotics
2. divalent metal-ion chelating agent
3. Heavy metals May accumulate in bone by adsorption onto
the bone crystal surface andEventual incorporation into the crystal lattice.
-Reservoir for slow release of toxic agents
E.g-lead or radium into the blood(effects thus can persist long after exposure ceases)

Bone cont
Adsorption onto the bone crystal surface and incorporation to crystal lattice-Have therapeutic advantages for the t/t of osteoporosis
Sodium etidronate bind tightly to hydroxy-apatite crystals in mineralised bone matrix.
Etidronate is resistant to degradation by pyrophosphatases and thus stabilises the bone matrix.
FAT as a reservoir
Lipid soluble drugs-stored by physical solution in the neutral fat.
E.g - Barbiturate Thiopental- 70% lipid soluble 3 hr after adm.(no anesthetic effect measurable)
Stable reservoir-due to low blood flow. But in highly lipophilic drugs distribution in
obese individual cant be predicted- E.g Remifentanil & some Beta Blockers
Active transport systems
Certain drugs are concentrated in certain tissues as a result of uptake by selective transport systems.
E.g Adrenergic neuron blockers actively transported into adrenergic nerve terminal

REFERENCES:
1. Goodman & Gilman’s – The Pharmacological Basis of Therapeutics
2. Rang & Dale’s - Pharmacology3. Barar – General Pharmacology4. KD Tripathi – Essentials of Medical
Pharmacology5. JCI – Journal of Clinical Investigation






![World war i_-_the_total_war_experience[1]](https://static.documents.pub/doc/80x56/5560cf49d8b42a0d088b4f24/world-war-i-thetotalwarexperience1.jpg)

