
BY
DR.YASSERA HAMEED
RADIOLOGYSIR GANGA RAM HOSPITAL LAHORE
DYSPLASIAS OF BONE

Bone dysplasias are genetic disorders of the skeleton.
More than 300 different bone dysplasias are currently known.

Bone dysplasias can cause dwarfism,brittle bones, leg and spine deformities and many other complications.
We study bone dysplasias to improve diagnosis and management of these rare
disorders.
In addition, bone dysplasias give the rare opportunity to study the impact of single genes on human bone and cartilage development.

The diagnosis of these lesions is mainly radiological and often entirely so.

Accurate diagnosis is of prime importance Genetic councelling is ,of course Well established speciality depending on
accurate diagnosis

PYKNODYSOSTOSIS
OSTEOPETROSIS
MELORRHEOSTOSIS
OSTEOPOIKILOSIS
DYSPLASIAS OF BONE

PYKNODYSOSTOSIS

also been named Toulouse-Lautrec syndrome, after the French artist
Henri de Toulouse-Lautrec, who suffered from the disease.

rare clinical entity, an autosomal recessive
osteochondrodysplasia, usually diagnosed at an early age
With INCIDENCE estimated to be 1.7 per 1 million births.
Life expectancy for a Pycnodysostosis patient is normal.

a lysosomal storage disease of the bone caused by a mutation in the gene that codes the enzyme cathepsin K.
cathepsin K. Is important for osteoclasts, to reabsorb the bone and build new bone

The normal functioning of osteoclasts in individuals with pycnodysostosis is disrupted by a lack of cathepsin K,
unable to adequately reabsorb the organic matrix. This process, also called remodelling, is
vital for normal bone maintenance.

The bones in individuals afflicted with pycnodysostosis are abnormally dense
and brittle as a result of this insufficient re-absorption process.

Pycnodysostosis is characterised by

short STATURE, fractures, large head with frontal and parietal bossing,Obtuse MANDIBULAR ANGLE, The typical 'open mouth outline ' facial
appearance is due to frontal bossing, micrognatia, loss of the mandibular angle

prominent eyes with bluish sclerae, underdeveloped facial bones,Deficient growth of the maxilla and
mandible makes normal tooth alignment impossible, with dental crowding, DENTAL ANOMALIES, persistence of deciduous teeth resulting
a double row of teeth.

short, broad HANDS and feet with dystrophic nails and
acro-osteolysis of the terminal PHALANGES
TRUNK DEFORMITIES such as kyphosis, scoliosis, increased lumbar lordosis.

Hands showing short, stubby, spoon shaped digits with dystrophic nails.

RADIOLOGICAL FINDINGS
pyknodysostosis

generalized sclerosis of the skeleton, including skull,

The “babygram”
demonstrates generalized sclerosis of the bones.

THE SKULL shows open anterior fontanelle and sutures small facial bones,hypoplastic maxilla. non-pneumatised paranasal sinusesflattened /obtuse mandibular angle . sclerosis being more pronounced in the
periorbital region (“harlequin appearance” or “raccoon mask” sign),also calvarium and the base .

obtuse angled mandible,
open anterior and posterior fontanelle and non pneumatised sinuses.

PA skull radiography
generalized sclerosis more pronounced in the periorbital region (“harlequin appearance” or “raccoon mask” sign),
open fontanelles and cranial sutures, absence of facial sinuses.

Pycnodysostosis: Lateral skull radiograph, age 3 years.
loss of the mandibular angle (arrow) and increased thickness of vault.

Lateral skull film ;
• wide sutures,
•straightened angle of the mandible
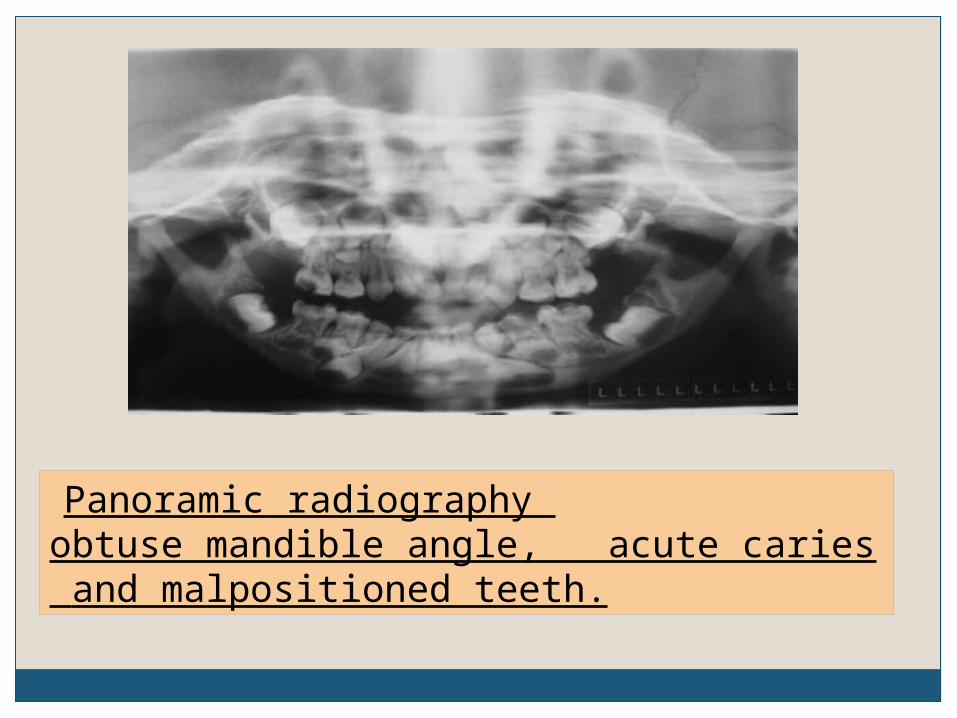
Panoramic radiography obtuse mandible angle, acute caries and malpositioned teeth.

IN THE HAND ; terminal phalanges are partially or totally
aplastic with loss of ungual tufts.
THORAX The acromial ends of the clavicles may be
aplastic.

Hand radiograph, age 3 years.
acro-osteolysis in the distal phalanx of thumb and index fingers (arrows)
and generalised increased bone density.

clubbing of the terminal phalanges.
PYKNODYSOSTOSIS

LIMBSCortices—dense,medullary canals are not completely
oblitreated. coxa valga and abnormal radioulnar
articulation.
SPINE failure of complete segmentation of the atlas,
axis, and the lower lumbar spine,

acroosteolysis hyperostosis
with sparing of medullary cavity and normal bone age.

54-year-old man with pycnodysostosis
subtrochanteric fracture of the right femur and a stress fracture in the left femur in the same region. Note that bones are sclerotic and medullary canal is visualized.
PYKNODYSOSTOSIS

typical facial features,, open fontenella,, high arched furrowed palate and radiological features including open cranial sutures, obtuse angle of mandible, generalized skeletal sclerosis.
PYKNODYSOSTOSIS

DDx Various bone diseases should be considered
in the differential diagnosis of pyknodysostosis, particularly
cleidocranial dysostosis, acroosteolysis, osteogenesis imperfecta, and osteopetrosis.
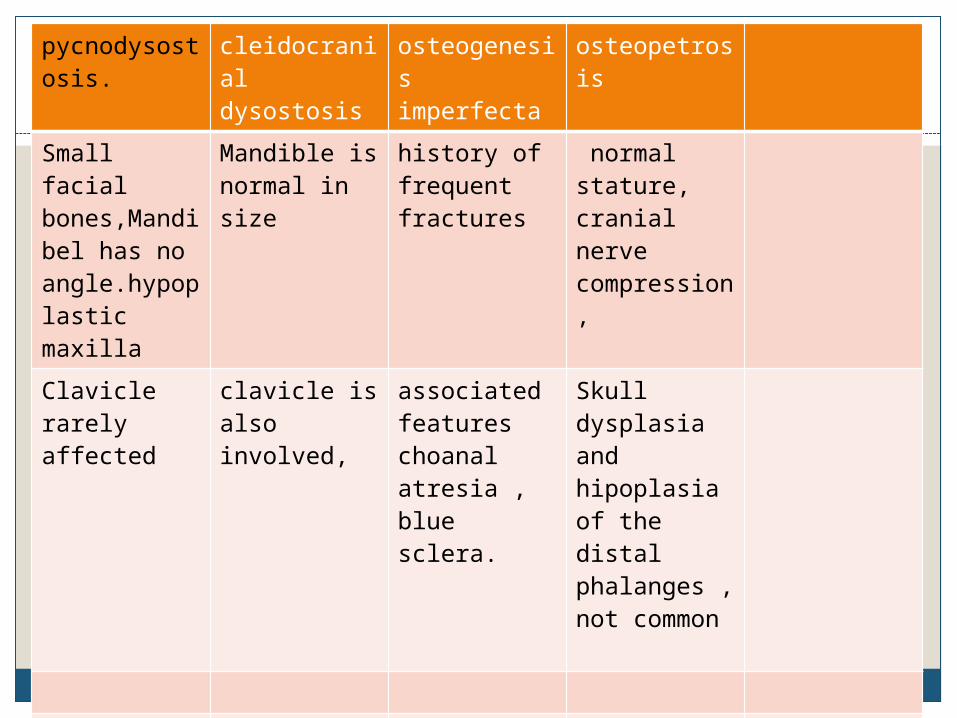
pycnodysostosis.
cleidocranial dysostosis
osteogenesis imperfecta
osteopetrosis
Small facial bones,Mandibel has no angle.hypoplastic maxilla
Mandible is normal in size
history of frequent fractures
normal stature, cranial nerve compression,
Clavicle rarely affected
clavicle is also involved,
associated featureschoanal atresia , blue sclera.
Skull dysplasia and hipoplasia of the distal phalanges ,not common
autosomally recessive
autosomal dominant inheritance
OSTEOPETROSIS

Osteopetrosis AKA: Albers-Schönberg Disease =
Marble Bone Disease

Rare hereditary disorderDefective osteoclast function with failure
of proper reabsorption produces sclerotic bone
Structurally weak

TYPES(osteopetrosois)
(1) AUTOSOMAL RECESSIVE TYPE i) Severe form (ARO): Also known as malignant osteopetrosis, usually results in stillbirth/early death. who survive present in early childhood with
fractures, diffuse marrow space obliteration leading to
pancytopaenia. ii) Intermediate severity form (IRO): (Infantile) with cerebral calcifications ("marble
brain syndrome").
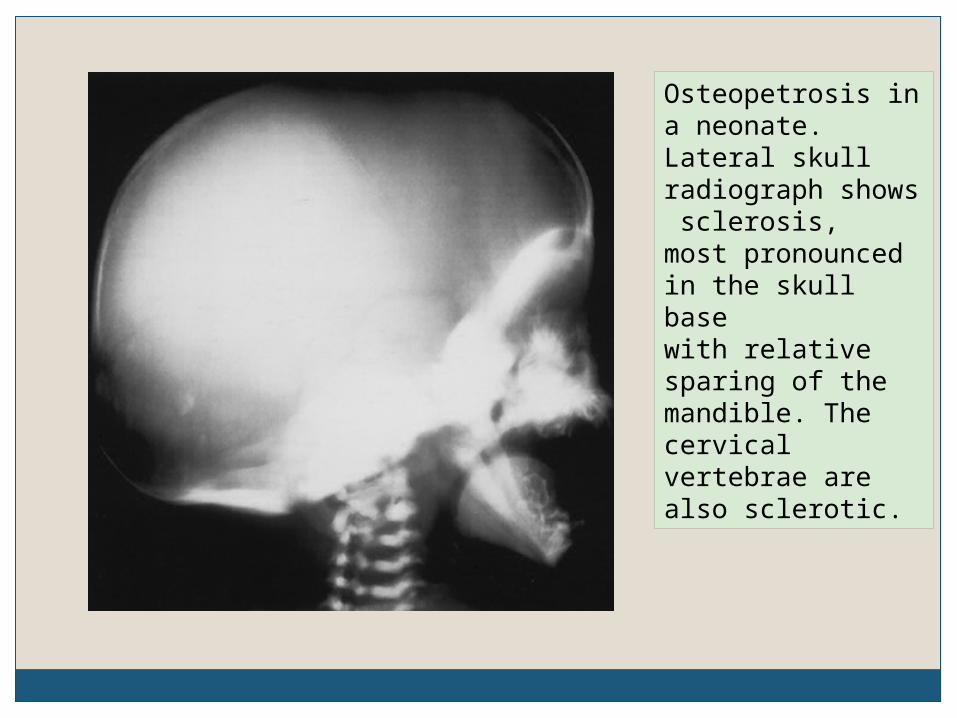
Osteopetrosis in a neonate. Lateral skull radiograph shows sclerosis,most pronounced in the skull base with relative sparing of the mandible. The cervical vertebrae are also sclerotic.

Neonate with typical features of autosomal recessive type of osteopetrosis. widened costo-chondral junctions; typical metaphyseal lucent bands and lost bony cortico-medullary differentiation.

Dense sclerotic bones

(2) BENIGN ADULT AUTOSOMAL DOMINANT TYPE i) type I sclerosis of the skul vault ii) type 2 sclerosis of the skull base and pelvis a typical "bone-within-bone" appearance of the
vertebral bodies due to endplate sclerosis,,,RUGGER JERSEY SPINE.
("sandwich" spine"). (3) X-linked: Rare.
Benign adult autosomal dominant type50% asymptomaticRecurrent fracturesMild anemiaPrognosis: normal

Benign adult autosomal dominant typeX-ray findings
Diffuse osteosclerosis
Cortical thickening with medullary encroachment
Erlenmeyer flask deformity = clublike long bones due to lack
of tubulization + flaring of ends

Bone-within-bone appearance (differentiates from other sclerosing dysplasias) maybe
vertical-----in long bones,,shafts and digits
transverse-------at metaphysis Arcuate------beneath the iliac crest

"Sandwich“ vertebrae =alternating sclerotic + radiolucent transverse metaphyseal lines indicate fluctuating course of disease
Longitudinal metaphyseal striations
Mandible least involved

a young woman with autosomal dominant osteopetrosis.----sclerosis and widening of the diploic space . The spine images show the classic sandwich vertebrae sign (the rugger jersey spine). The femur demonstrates increased sclerosis and an Erlenmeyer flask deformity.

One of the classical appearances of autosomal dominant osteopetrosis is
the "bone within a bone" appearance .

Inner layer of cortical new bone within the existing bone.


Case 1 : Foot

Osteopetrosis_____not
e inset of an earlier vertebral body
Rugger jersey appearance

Osteopetrosis_____not
e inset of an earlier vertebral body
Rugger jersey appearance


classic sandwich vertebrae of osteopetrosis (red arrows) thickening and sclerosis of the vertebral endplates, and of the bone adjacent to the endplates.

The tubular bones may have an Erlenmeyer flask type deformity.

An Erlenmeyer flask deformity refers to a radiographic appearance typically
on a femoral radiograph where there is relative constriction of the diaphysis and flaring of the metaphysis.

Erlenmeyer flasks

Erlenmeyer flask deformity

Erlenmeyer flask deformity

Erlenmeyer flask deformity

Erlenmeyer flask deformity

Dense sclerotic bones with fracture

Dense sclerotic bones with fracture

OSTEOPETROSIS
Complications:Fractures (common because of brittle bones)
with abundant callus + normal healingCrowding of marrow ( anemia +
extramedullary hematopoiesis)Frequently terminates in acute leukemiaRx: bone marrow transplant

DDx: Heavy metal poisoning Melorheostosis (limited to one extremity)
Hypervitaminosis D Pyknodysostosis Fibrous dysplasia of skull / face

MELORHEOSTOSIS
LERI’S DISEASE, FLOWING PERIOSTEAL HYPEROSTOSIS

also known as Leri disease is a rare sclerosing bone dysplasia.

The name is derived from the Greek words formelos (limb),rhein (flow)and ostos (bone), due to its characteristic appearance of
flowing hyperostosis.

non-hereditary, benign, sclerosing mesodermal disease with an incidence of 0.9 cases per
million.
General Considerations

General ConsiderationsCause is unknownProduces thickening of the endosteum
and periosteumPeak age of presentation is 5-20 years

May be monostotic or polyostotic May involve one entire limb
Usually does not involve multiple limbs
Twice as common in lower extremities than elsewhere

Clinical FindingsAbout 50% affected develop symptoms by
age 20Adults present with
Pain Joint stiffness Deformity that may progress over time
Children may present with Leg length discrepancies Joint contractures


• predominantly affects the appendicular skeleton
• is most common in the long bones of the upper and lower extremities,
• can be seen in the hands and feet as well• It may affect a single bone (monostotic), a single limb (monomelic), or multiple bones (polyostotic).

Photographs showing the swelling in the ring finger.A 16 year old female--- a 4 year history of progressively increasing swelling and intermittent dull ache in the ring finger of the right hand. no similar swelling in any other part of her body. no history of paraesthesia or restriction of movement. There were no similar complaints in the family
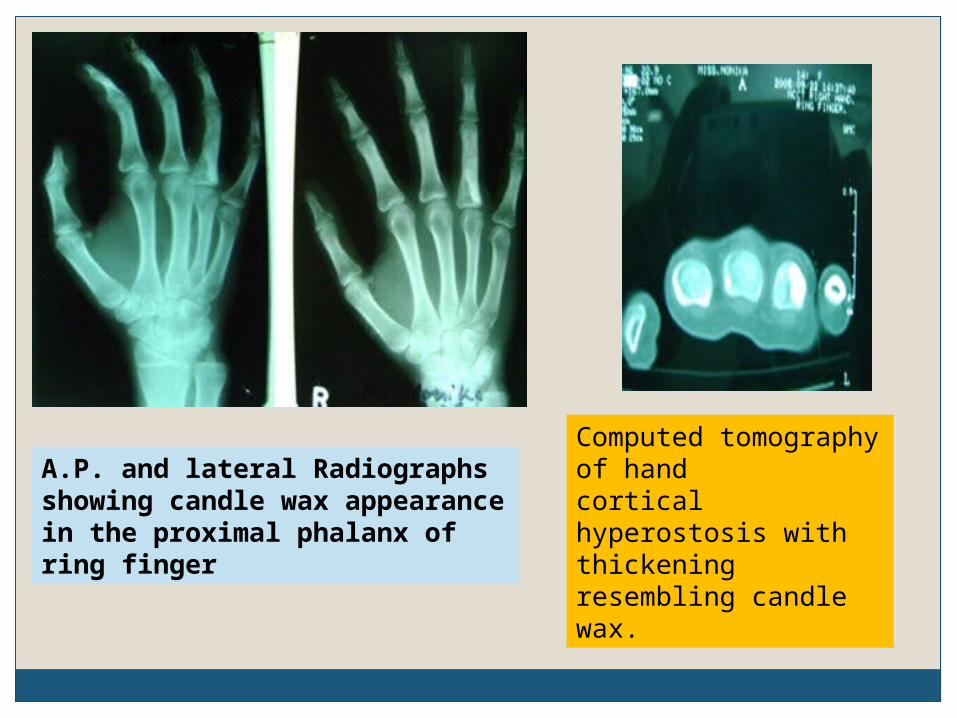
A.P. and lateral Radiographs showing candle wax appearance in the proximal phalanx of ring finger
Computed tomography of hand cortical hyperostosis with thickening resembling candle wax.

Radiographic features Plain film Five patterns have been described 1. Classic(Candle-wax appearance) osteoma - like myositis ossificans - like osteopathia striata - like mixed

The dripping (or flowing) candle wax sign
is seen on conventional radiographs depicting bone. The appearance is that of irregular cortical hyperostosis, typically occurring on one side of the involved bone, and has been likened to melted wax flowing down one side of a candle.

Radiographically, the lesions show undulating cortical hyperostosis
which has been likened to flowing candle wax.

The dripping candle wax signdevelopmental error ---in intramembranous
bone formation. leads to an irregular thickening of cortical
bone (cortical hyperostosis) that extends up to (but usually not past) the articular surface.
Pathologically— both overproduction of bone matrix and increased angiogenesis. The DISTRIBUTION OF AFFECTED BONE is
thought to be due to the predilection of melorheostosis to occur in sclerotomes (skeletal regions innervated by a single spinal sensory nerve).

Classical appearances of melorheostosis


Classical appearances of melorheostosis
involving the right fibula and lateral side of the foot. AP radiograph ;dense cortical and extra-cortical bone formation (white arrows) along the length of the distal fibula to the lateral malleolus
with associated hyperostosis in the lateral hind foot bones (black arrows).
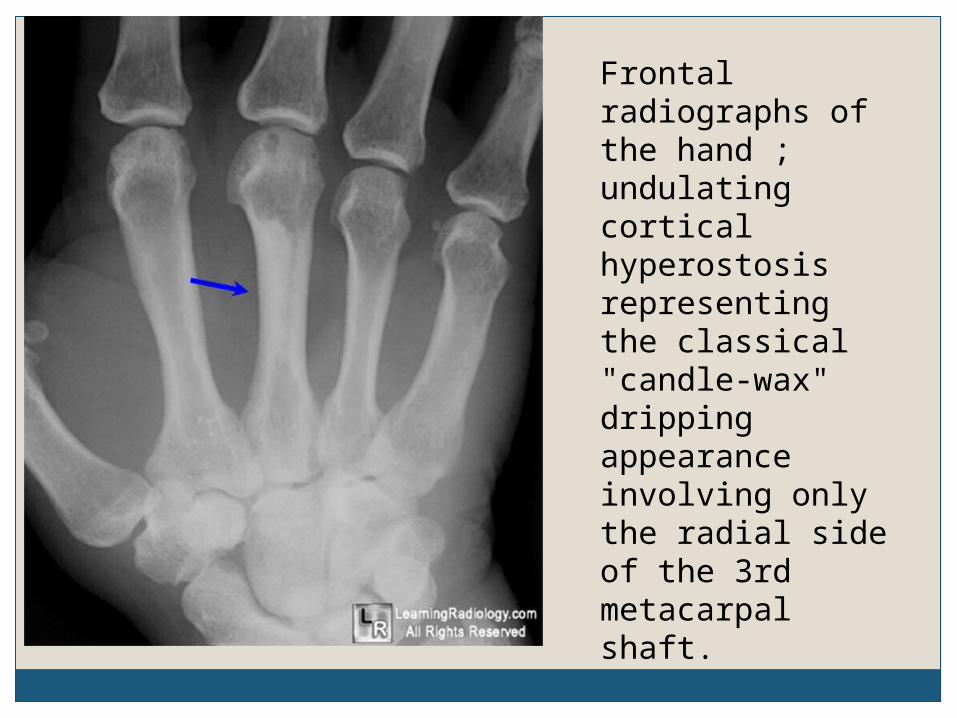
Frontal radiographs of the hand ;undulating cortical hyperostosis representing the classical "candle-wax" dripping appearance involving only the radial side of the 3rd metacarpal shaft.

oblique radiographs

Radiographically, the lesions show undulating cortical hyperostosis which has been likened to flowing candle wax.
Cortical lesions are progressive and may result in narrowing of the medullary canal and stenosis of an adjacent lumen, foramen, or of the spinal canal.




Melorheostosis in the ribs with typical candle wax appearance.

The Dripping Candle Wax Sign

CT scan will show clear demarcation between normal and abnormal bone . CT scan is helpful to confirm or exclude continuity of osseous and soft tissue abnormalities [7].

Noncontiguous transverse CT images through eighth (left) and ninth (right) right posterior ribs of patient in Figure 1 show sharp delineation between normal and
affected bone segments (arrows), highlighting sclerotomal distribution.

melorrheostosis
Osteoma-like appearance.

Osteoma-like appearance.
Anteroposterior radiograph of the right ilium showing an irregular area of medullary hyperostosis (arrows).

melorrheostosis
Myositis ossificans-like pattern.

Myositis ossificans-like pattern.
A P radiograph of the right elbow shows dense, lobular, soft-tissue mineralisation (arrows) adjacent to the radial head.

melorrheostosis
Osteopathia striata-like pattern.

Osteopathia striata-like pattern. AP radiograph right knee
demonstrates longitudinal, dense band-like areas of increased intramedullary density (arrows). Note also the soft-tissue mineralization.

MR imaging shows heterogeneous signal
intensity due to mixture of osseous, fibrous, adipose and cartilaginous tissue which these lesions contain

(a) MRI appearances. Sagittal, T2*-weighted, gradient echo image of the knee showing multiple areas of intramedullary signal void (arrows). Note the absence of patella as patellectomy was performed for severe pain. (b) Plain radiograph in the same patient showing the area of sclerosis seen as the signal void lesions on the MRI.

Patients with meloreostosis may have associated cutaneous and soft tissue lesions such as
vascular malformations, neurofibromatosis, hemangioma, arterial aneurysms, linear scleroderma, tuberous sclerosis, hemangiomas, and focal subcutaneous fibrosis.
Not infrequently
features of melorheostosis, osteopathia striata and osteopoikilosis may co-exist in so-called OVERLAP SYNDROMES.
These conditions may share an underlying aetiology 1.

Differential DiagnosisOsteopathia striata
Longitudinal dense striationsOsteopoikilosis
Punctate, rounded bone islands surrounding joints,symmetrical involvement, absence of soft tissue involvement, negative scintigraphy, no clinical complaints and autosomal dominancy
Osteosarcoma Bone destruction

Nuclear medicineIncrease in radiotracer uptake is usually
present on late phase bone scans 2.


reatmentAnalgesiaNerve blocksSurgery directed at relieving contracture

ComplicationsAssociated soft tissue lesions and cutaneous
lesions Vascular malformations Neurofibromatosis Tuberous sclerosis Hemangioma
Muscle contracturesScoliosis

PrognosisProgressive disorder

In conclusion, radiographs are diagnostic for melorheostotic
lesions. MR imaging is useful to detect the presence
and extent of associated mineralized and nonmineralised soft tissue masses and may obviate unwarranted biopsy and a radical procedure.

OSTEOPOIKILOSIS

Osteopoikilosis is a benign, asymptomatic sclerosing dysplasis.Affects both M and F.
May be seen at any age.Cutaneous lesions in 25%.Etiology unknown.Inherited and spontaneous cases occur.
RADIOGRAPHICALLY,Sclerotic circular or ovoid lesions
symmetrically distributed in a periarticular location.
Lesions can increase or decrease in size and number in serial radiographs or even disappear.
Lesions do not have increased bone radiotracer uptake.

multiple circular and ovoid sclerotic opacities
appear to be parallel each other and to the long axis of the bone.
A periarticular distribution

The main clinical significance is that these may be mistaken for sclerotic metastases. their classic distribution and appearance will distinguish them readily from evil entities like mets.
osteopoikilosis of the pelvis and proximal femurs

May be related to other sclerosing dysplasias including,Osteopathia striata.
melorheostosis.focal sclerosis.and when seen in combination with them, is
termed "MIXED SCLEROSING BONE DYSTROPHY."

DDx includes:Osteoblastic metastases.Mastocytosis.Tuberous Sclerosis.
THANK YOU







