
Emerging trends in the therapy of Malaria
Better clarity, Better outcomes
Dr. B. K. Iyer
2
WhatWhat
WhoWho
WhyWhy
HowHow
Introduction
Malaria scenario is dynamic -1. Changes in parasite transmission2. Increasing drug & insecticide resistance
resistance3. Climatic changes4. New drugs
Over-reliance on quinoline & antifolate Base Drugs: (Cross) Resistance
Therapy must be up to date with current situation
3
WhatWhat
WhoWho
WhyWhy
HowHow
Cause
Next to mosquitoes the biggest cause of malaria is
“Ignorance”
This is because success is influenced by resistance patterns
4
WhatWhat
WhoWho
WhyWhy
HowHow
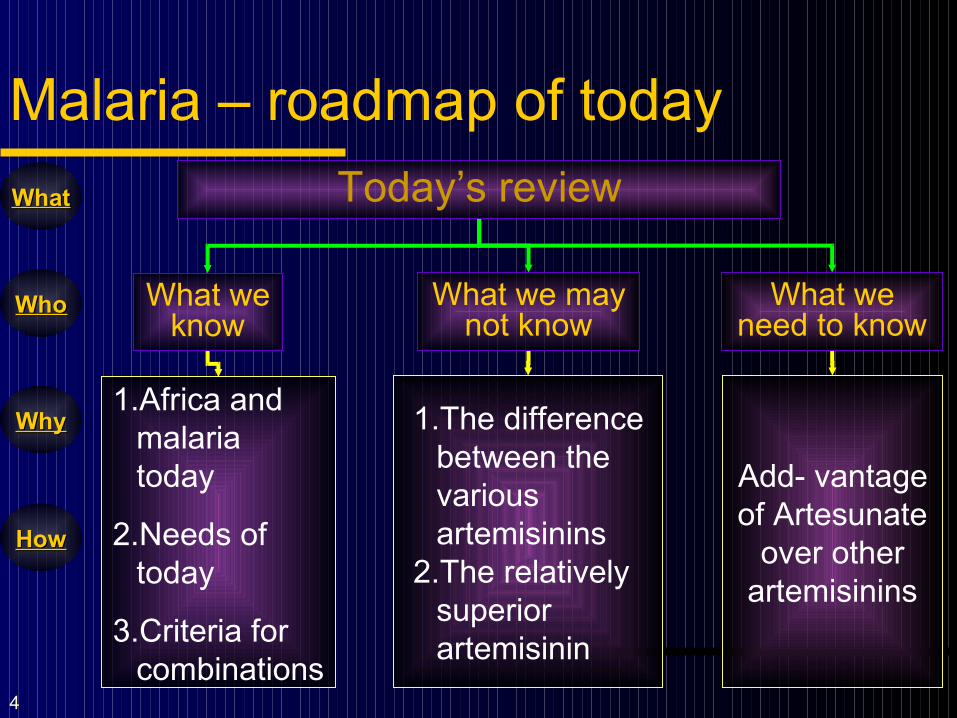
Malaria – roadmap of today
What we know
What we may not know
What we need to know
1.Africa and malaria today
2.Needs of today
3.Criteria for combinations
1.The difference between the various artemisinins
2.The relatively superior artemisinin
Add- vantage of Artesunate
over other artemisinins
Today’s review
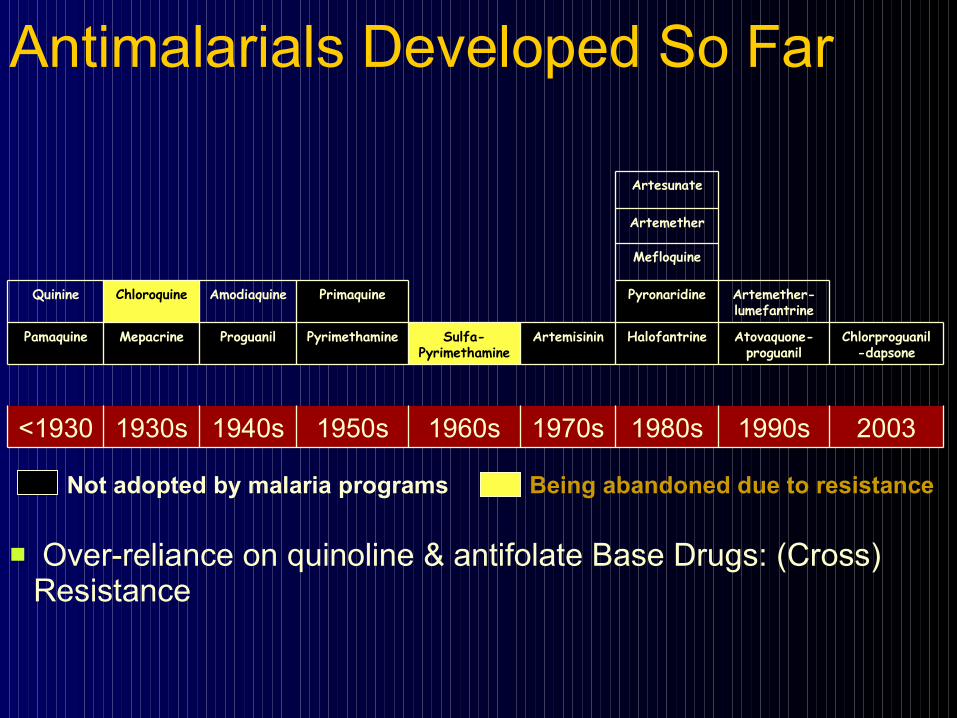
20031990s1980s1970s1960s1950s1940s1930s<1930
Chlorproguanil-dapsone
Atovaquone-proguanil
HalofantrineArtemisininSulfa-Pyrimethamine
PyrimethamineProguanilMepacrinePamaquine
Artemether-lumefantrine
PyronaridinePrimaquineAmodiaquineChloroquineQuinine
Mefloquine
Artemether
Artesunate
Not adopted by malaria programs Being abandoned due to resistance
Antimalarials Developed So Far
Over-reliance on quinoline & antifolate Base Drugs: (Cross) Resistance
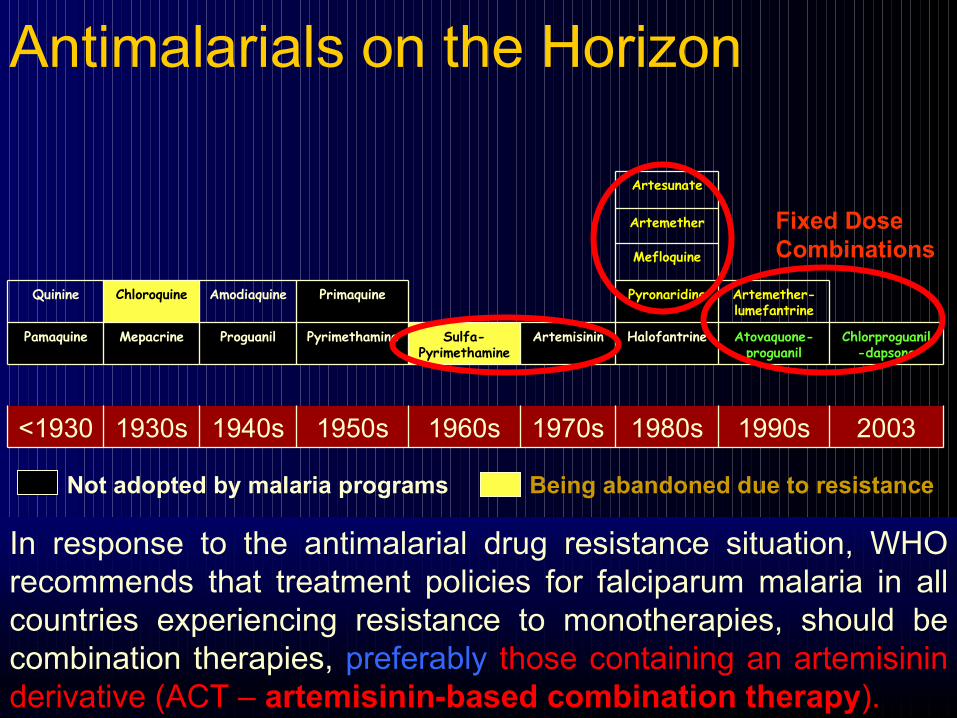
20031990s1980s1970s1960s1950s1940s1930s<1930
Chlorproguanil-dapsone
Atovaquone-proguanil
HalofantrineArtemisininSulfa-Pyrimethamine
PyrimethamineProguanilMepacrinePamaquine
Artemether-lumefantrine
PyronaridinePrimaquineAmodiaquineChloroquineQuinine
Mefloquine
Artemether
Artesunate
Not adopted by malaria programs Being abandoned due to resistance
Antimalarials on the Horizon
Fixed DoseCombinations
In response to the antimalarial drug resistance situation, WHO recommends that treatment policies for falciparum malaria in all countries experiencing resistance to monotherapies, should be combination therapies, preferablypreferably those containing an artemisinin derivative (ACT – artemisinin-based combination therapy).
7
WhatWhat
WhoWho
WhyWhy
HowHow
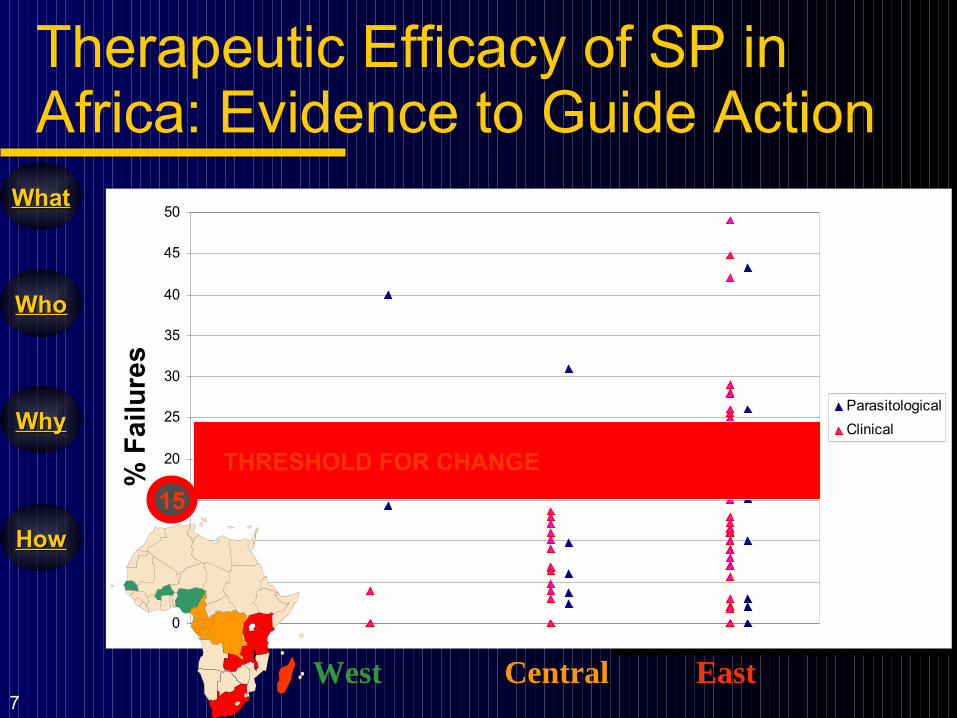
0
5
10
15
20
25
30
35
40
45
50
% F
ailu
res
Parasitological
Clinical
West Central East
THRESHOLD FOR CHANGE
15
Therapeutic Efficacy of SP in Africa: Evidence to Guide Action
8
WhatWhat
WhoWho
WhyWhy
HowHow
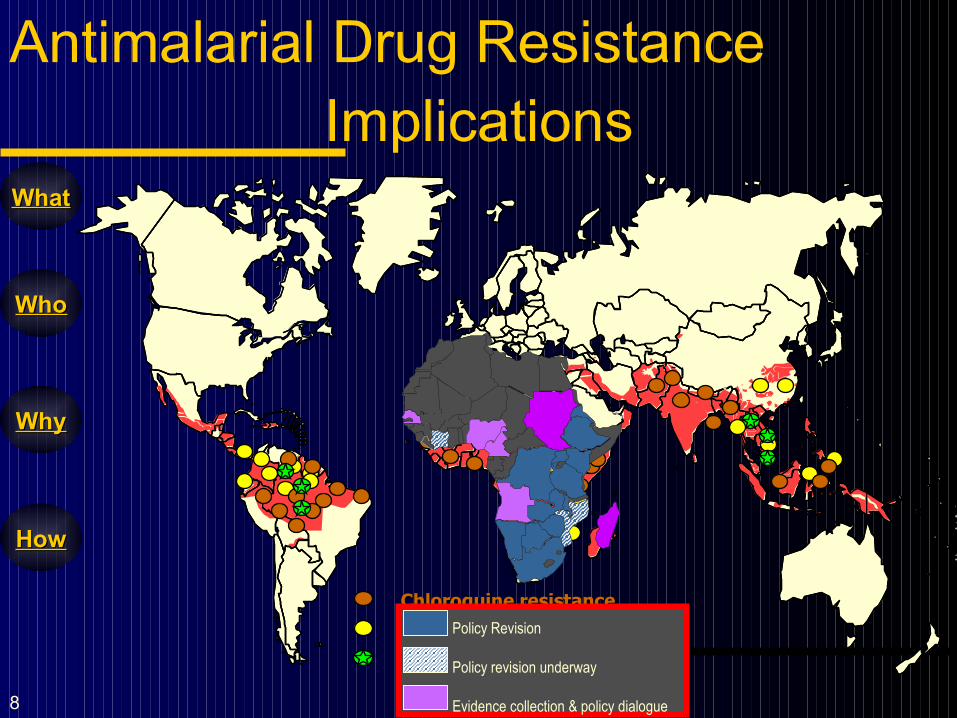
Chloroquine resistanceChloroquine resistance
S/P resistanceS/P resistance
Mefloquine resistanceMefloquine resistance
Antimalarial Drug ResistanceImplications
Policy Revision
Policy revision underway
Evidence collection & policy dialogue
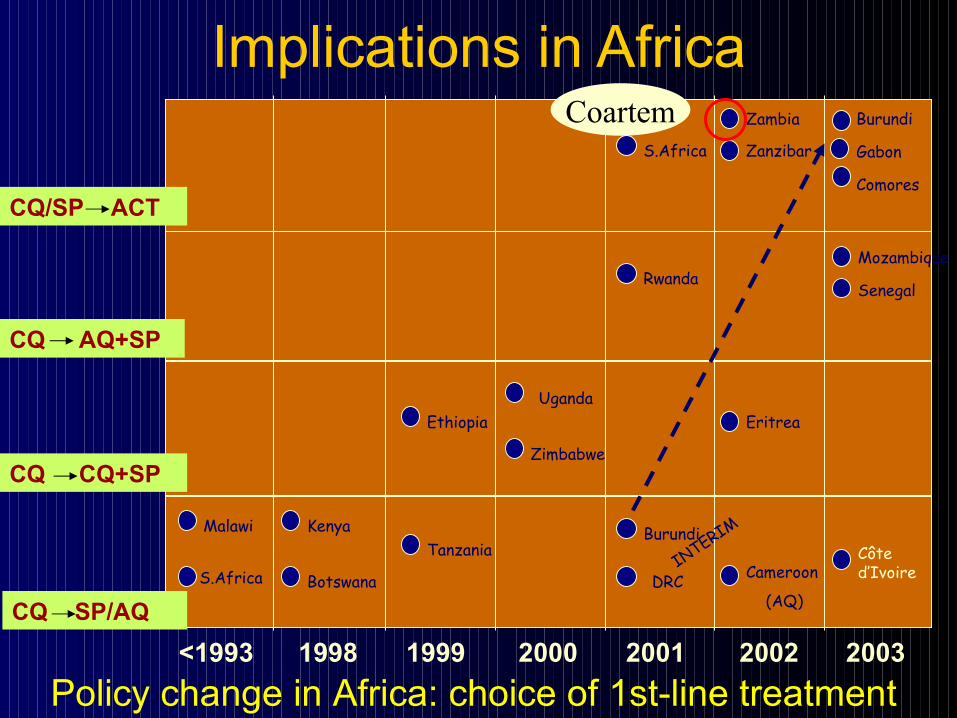
Implications in Africa
Policy change in Africa: choice of 1st-line treatment
CQ SP/AQ
CQ AQ+SP
CQ/SP ACT
Malawi
S.Africa
Kenya
Botswana
Tanzania
Ethiopia
Zimbabwe
Uganda
INTERIM
S.Africa
Rwanda
DRC
Burundi
Zambia
Eritrea
Zanzibar
Cameroon
(AQ)
<1993 1998 1999 2000 2001 2002 2003
Coartem Burundi
Gabon
Comores
Mozambique
Senegal
Côted’Ivoire
CQ CQ+SP
10
WhatWhat
WhoWho
WhyWhy
HowHow
Combination Therapies:Definition
WhatWhat
Parallel use of 2 or more antimalarials as free / fixed combinations to delay antimalarial drug
resistance in Falciparum malaria
HypertensionHypertension
CancerCancer
DiabetesDiabetesTuberculosisTuberculosis
AIDSAIDS
Combination Combination therapytherapy
11
WhatWhat
WhoWho
WhyWhy
HowHow
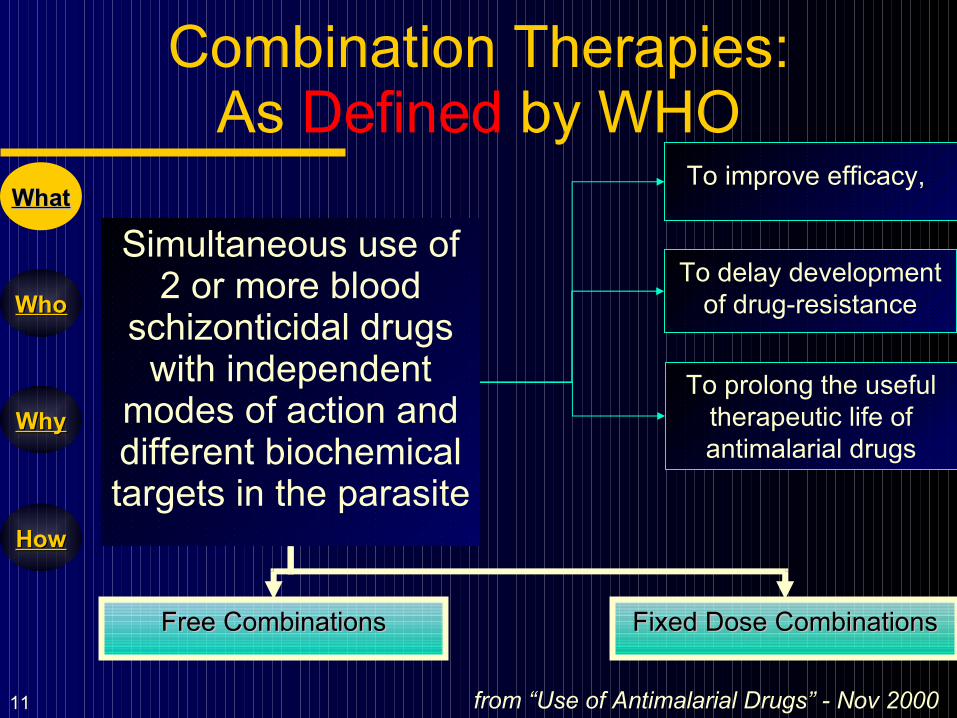
Combination Therapies:As Defined by WHO
Simultaneous use of 2 or more blood
schizonticidal drugs with independent
modes of action and different biochemical targets in the parasite
from “Use of Antimalarial Drugs” - Nov 2000
WhatWhat
Free CombinationsFree Combinations Fixed Dose CombinationsFixed Dose Combinations
To improve efficacy,
To delay development of drug-resistance
To prolong the useful therapeutic life of antimalarial drugs
12
WhatWhat
WhoWho
WhyWhy
HowHow
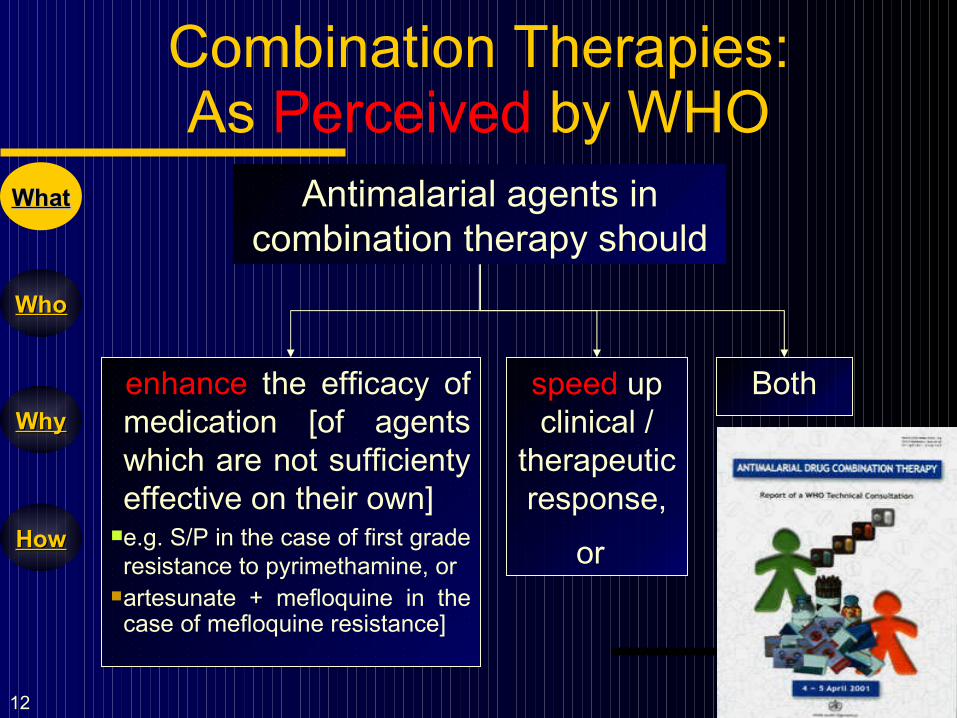
Combination Therapies:As Perceived by WHO
WhatWhat Antimalarial agents in combination therapy should
enhance the efficacy of medication [of agents which are not sufficienty effective on their own]
e.g. S/P in the case of first grade resistance to pyrimethamine, or
artesunate + mefloquine in the case of mefloquine resistance]
speed up clinical /
therapeutic response,
or
Both
13
WhatWhat
WhoWho
WhyWhy
HowHow
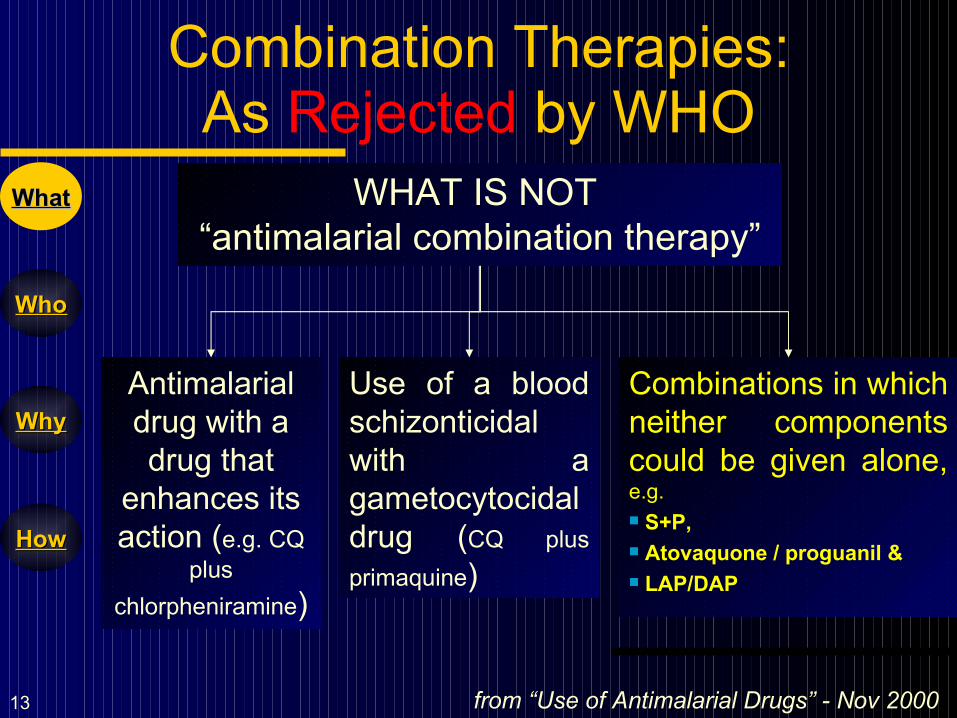
Combination Therapies:As Rejected by WHO
from “Use of Antimalarial Drugs” - Nov 2000
WhatWhat WHAT IS NOT “antimalarial combination therapy”
Antimalarial drug with a drug that
enhances its action (e.g. CQ
plus
chlorpheniramine)
Use of a blood schizonticidal with a gametocytocidal drug (CQ plus
primaquine)
Combinations in which neither components could be given alone, e.g. S+P, Atovaquone / proguanil & LAP/DAP
14
WhatWhat
WhoWho
WhyWhy
HowHow
Combination Therapies:Principles
WhatWhat
Principles
Dosages
Contra-
indications
Ease of
Use
15
WhatWhat
WhoWho
WhyWhy
HowHow
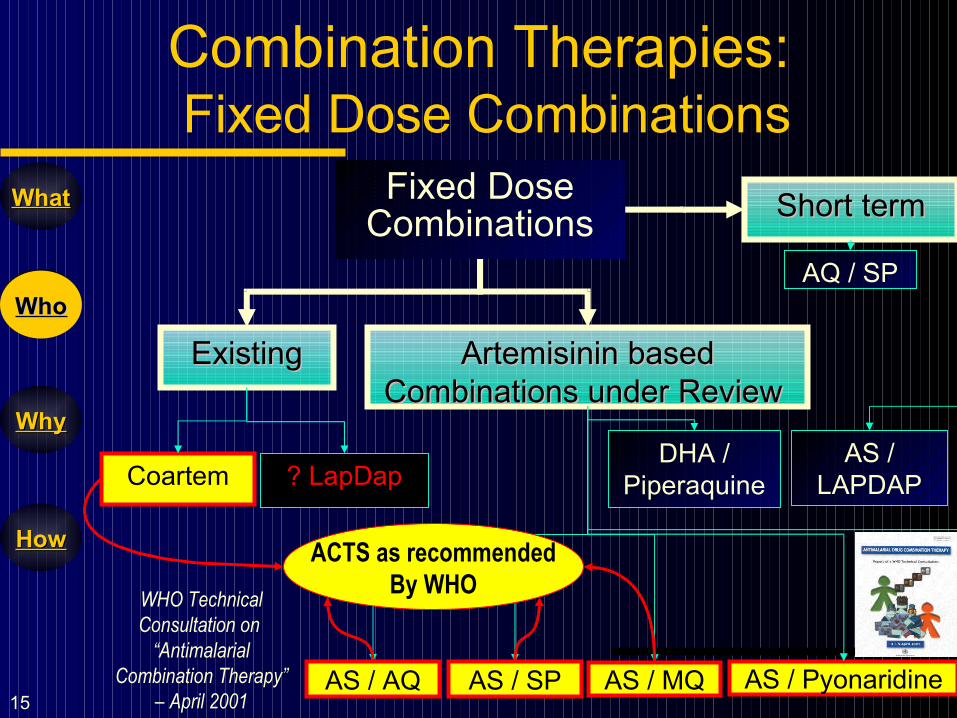
Combination Therapies: Fixed Dose Combinations
WhoWho
Fixed Dose Combinations
Artemisinin based Artemisinin based Combinations under Review Combinations under Review
ExistingExisting
Coartem ? LapDap
AS / AQ AS / MQ
AS / LAPDAP
AS / SP
Short termShort term
AQ / SP
DHA / Piperaquine
WHO Technical Consultation on
“Antimalarial Combination Therapy”
– April 2001
ACTS as recommendedBy WHO
AS / Pyonaridine
16
WhatWhat
WhoWho
WhyWhy
HowHow
Observations of International Studies
Data from Thailand suggest that for combination Therapy in malaria, Artemisinin derivatives are particularly effective combination partners as- They are very active antimalarials, producing up to
10,000-fold reductions in parasite biomass per asexual cycle;
They reduce malaria transmissibility; No resistance to these drugs has been reported yet. Halts the progression of resistance No adverse side effects from artesunate/artemether
and safe for use in 2nd/3rd trimesters
WhoWho
Antimalarial drug resistance and combination chemotherapy, Philos Trans R Soc
Lond B Biol Sci. 1999 Apr 29;354(1384):739-49, White N.
17
WhatWhat
WhoWho
WhyWhy
HowHow
Benefits of Adding artemisinins to Current monotherapy
Accelerates therapeutic response and so, deterioration of the patient's condition to severe malaria is extremely unusual
WhyWhy Superior cure rate / enhanced efficacy rate; Greater parasite killing and more rapid parasite
clearance; Reduced gametocyte carriage and hence low
recrudescence rates; Shortened duration of therapy No added overt toxicity
18
WhatWhat
WhoWho
WhyWhy
HowHow
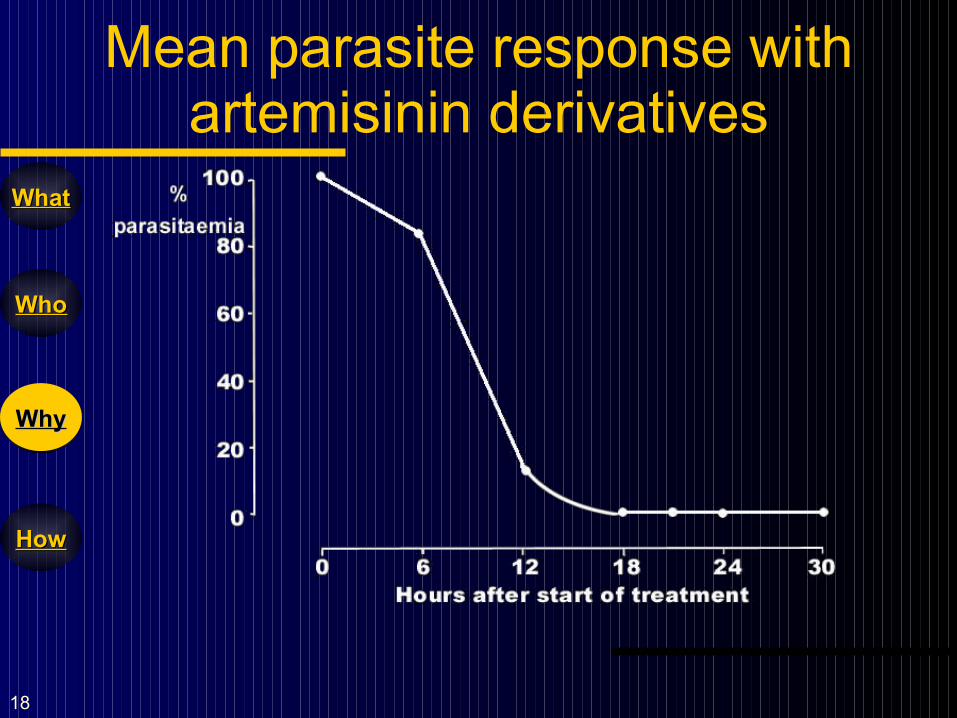
Mean parasite response with artemisinin derivatives
WhyWhy
19
WhatWhat
WhoWho
WhyWhy
HowHow
Why Not Artemisinin Derivatives As monotherapy?
If artemisinin or one of its derivatives is given alone, completion of a 7-day treatment course is needed because:
Cure rate of Artemisinin derivatives as monotherapy depends on:
Dosage used
Duration of treatment
Severity of patients
WhyWhy
20
WhatWhat
WhoWho
WhyWhy
HowHow
Artemisinins Under Review in ACTs
Artemether Artesunate Dihydroartemisinin Arteether ArtefleneWhyWhy
Artemotil
21
WhatWhat
WhoWho
WhyWhy
HowHow
Artemisinin studies Under Review
1. Artemisinins vs. DHA2. Quinine vs. Artesunate3. Artemether vs. Artesunate4. Artemether+lumefantrine vs.
Artesunate+Mefloquine5. Amodiaquine + Artesunate 6. Amodiaquine + SP
WhyWhy
22
WhatWhat
WhoWho
WhyWhy
HowHow
Artemisinins with reference to DHA
Use of dihydroartemisinin could be beneficial in 2 ways: [1] Easy to make and [2] Low cost
All Artemisinin derivatives act after being converted into dihydroartemisinin [DHA] which has intrinsically greater antimalarial activity than artesunate.
In terms of the current-in-vitro 50% inhibitory concentrations for P. falciparum in western Thailand, artesunate has approx. 70% of the potency of DHA.
HowHow
Then, why is DHA still not popular over artemether or artesunate?
23
WhatWhat
WhoWho
WhyWhy
HowHow
Artemisinins With Reference to DHA
Antimicrobial Agents and Chemotherapy, April 2002, p. 1125-1127, Vol. 46, No. 4
HowHow
The time of dissolution of the relatively insoluble DHA tablet is higher providing: A higher lag time and Longer time to maximum antimalarial
activity (Tmax).
24
WhatWhat
WhoWho
WhyWhy
HowHow
Quinine / Artesunate
In one comparative study, 1461 patients with severe malaria were recruited from Bangladesh, Indonesia, India, and Myanmar into a randomised controlled trial comparing artesunate with quinine.
Half the patients were assigned IV artesunate and half IV quinine.
The investigators found that mortality from severe malaria was 15% in artesunate recipients compared with 22% in quinine recipients.= [A reduction of 35%]
HowHow
Lancet, 27 August 2005
25
WhatWhat
WhoWho
WhyWhy
HowHow
Quinine / Artesunate: Conclusion:
The World Health Organization this week announced that it will recommend artesunate as the first-line treatment for adults with severe malaria after a study found that the drug might be more effective than quinine at treating the disease,
HowHow
Aug 31, 2005
26
WhatWhat
WhoWho
WhyWhy
HowHow
Artemether + Lumefantrine
Initial response of Coartem in malaria is determined by Artemether but,
The principal determinant of overall cure rate is Lumefantrine AUC.
HowHow
Antimicrob Agents Chemother. 2000 March; 44 (3): 697–704 Artemether.
A fixed combination of artemether and lumefantrine in 3 different study regimens have all shown a rapid initial response with comparable parasite clearance time (PCT) and fever clearance time (FCT) although they vary in cure rates. Clin Drug Invest 19(5):343-348, 2000.
27
WhatWhat
WhoWho
WhyWhy
HowHow
Artemether + Lumefantrine Negative points
HowHow
1. Lumefantrine’s long half-life could also increase the risk of resistance to treatment developing more rapidly. Indeed, a study in Zanzibar, which recently began
using co-artemether, has already shown that the malarial parasite is mutating in response to the treatment.
Sisowath C et al,J Infect Dis. 191(6):1014-7, 2005.
Lumefantrine oral bioavailability is dependent on food and is consequently poor in acute malaria but improves markedly with recovery.
28
WhatWhat
WhoWho
WhyWhy
HowHow
Artemether + Lumefantrine Dosage observations
The Cochrane Review shows that the 6 dose regimen (480 mg of artemether + 2,880 mg of
lumefantrine) is more effective as compared to the 4 dose regimen of artemether-lumefantrine (320 mg of artemether + 1,920 mg of lumefantrine) but the failure rates with the 4 dose regimen was very high and the 6-dose regimen is largely untested.
HowHow
The Cochrane Database of Systematic
Reviews 2005 Issue 3
It is worth noting that artemether is liposoluble and not hydrophilic unlike artesunate.
29
WhatWhat
WhoWho
WhyWhy
HowHow
Artemether + Lumefantrine Comparative studies
In one comparative study, oral artesunate administration resulted in significantly larger mean area under the plasma antimalarial activity time curve and median maximum plasma antimalarial activity than after oral artemether.
The oral antimalarial bioavailability following artemether was significantly lower than that after artesunate. Artemether oral antimalarial bioavailability is reduced in acute malaria. British journal of clinical pharmacology, volume 52 issue 6 page
655 - December 2001.
HowHow
30
WhatWhat
WhoWho
WhyWhy
HowHow
Artemether + lumefantrinevs. Artesunate + mefloquine In one open-label, two-arm, randomized study
comparing oral artemether-lumefantrine and mefloquine-artesunate in 490 patients for the treatment of uncomplicated falciparum malaria with 42 days of follow up, the following was observed:
All patients had rapid initial clinical and parasitological responses.
In both groups, the PCR adjusted cure rates by day 42 were high.
Both regimens were very well tolerated with no serious adverse events observed attributable to either combination. Malaria Journal 2005, 4:46, A randomized trial of artemether-
lumefantrine versusmefloquine-artesunate for the treatment of uncomplicated multi-drug resistant Plasmodium falciparumon the western border of Thailand by Robert Hutagalung et al.
HowHow
31
WhatWhat
WhoWho
WhyWhy
HowHow
Combination Therapies: Alternatives: AQ + ART
Excellent efficacy reported on parameters of: Fever clearance rates Parasite clearance rates Gametocyte carriage rates Recrudescence rates Success rates Low failure rates
Why not SP combination? With SP as first line therapy, resistance / treatment failure are already prevalent and expected to increase rapidly.
HowHow
For AQ and ART, both are given according to the usual weight-specific dosage schedules for a minimum period of 3 days.
32
WhatWhat
WhoWho
WhyWhy
HowHow
Combination Therapies: Alternatives: AQ + S/P
Efficacy reported as superior to amodiaquine alone and S/P alone in an area of full chloroquine resistance and incipient S/P resistance (in this area amodiaquine alone was superior to S/P alone)..
Both are given according to the usual weight-specific dosage schedules and S/P (single dose) given with the first dose of amodiaquine.
HowHow
Efficacy of AQ alone and combined with SP and of SP combined with AS.Am J Trop Med Hyg. 2003 Jun;68(6):743-7, Rwagacondo CE, Niyitegeka F, et al.
33
WhatWhat
WhoWho
WhyWhy
HowHow
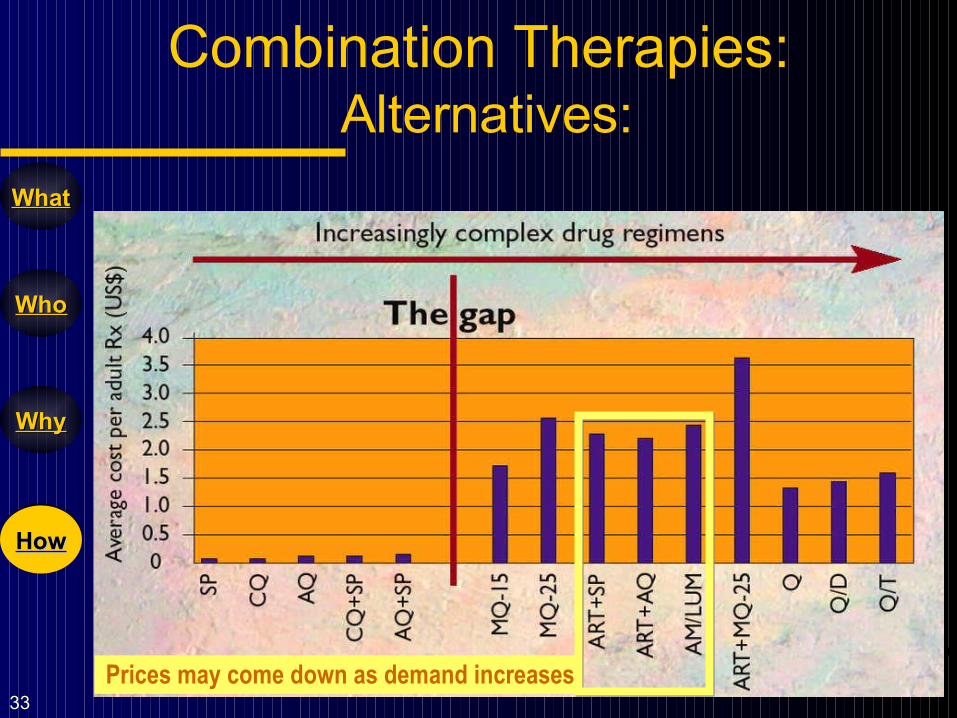
Prices may come down as demand increases
Combination Therapies: Alternatives:
HowHow
34
WhatWhat
WhoWho
WhyWhy
HowHow
Combination Therapies: Conclusion:
WHO recommends consideration of alternative artemisinin-based combination therapies to artemether-lumefantrine, based on susceptibility of the local malaria parasites. They include: Artesunate (3 days) + amodiaquine, Artesunate (3 days) + sulfadoxine / pyrimethamine
(SP) in areas where SP efficacy remains high; & Artesunate (3 days) + mefloquine in areas of low to
moderate transmission.
HowHow
WHO Information note draft 6 December 2004)
35
WhatWhat
WhoWho
WhyWhy
HowHow
Amqunate studies
In one study, 941 children patients who were 10 years or older and who had uncomplicated P falciparum malaria were observed and studied 400 in Kenya, 321 in Sénégal, and 220 in Gabon.
Patients were randomly assigned amodiaquine (10 mg/kg per day for 3 days) plus artesunate (4 mg/kg per day for 3 days) or amodiaquine (as above) and placebo (for 3 days).
HowHow
Lancet, volume 359, number 9315, page 1365-1372, 20 April 2002.
36
WhatWhat
WhoWho
WhyWhy
HowHow
Amqunate studies
HowHow
Lancet, volume 359, number 9315, page 1365-1372, 20 April 2002.
37
WhatWhat
WhoWho
WhyWhy
HowHow
Amqunate studies
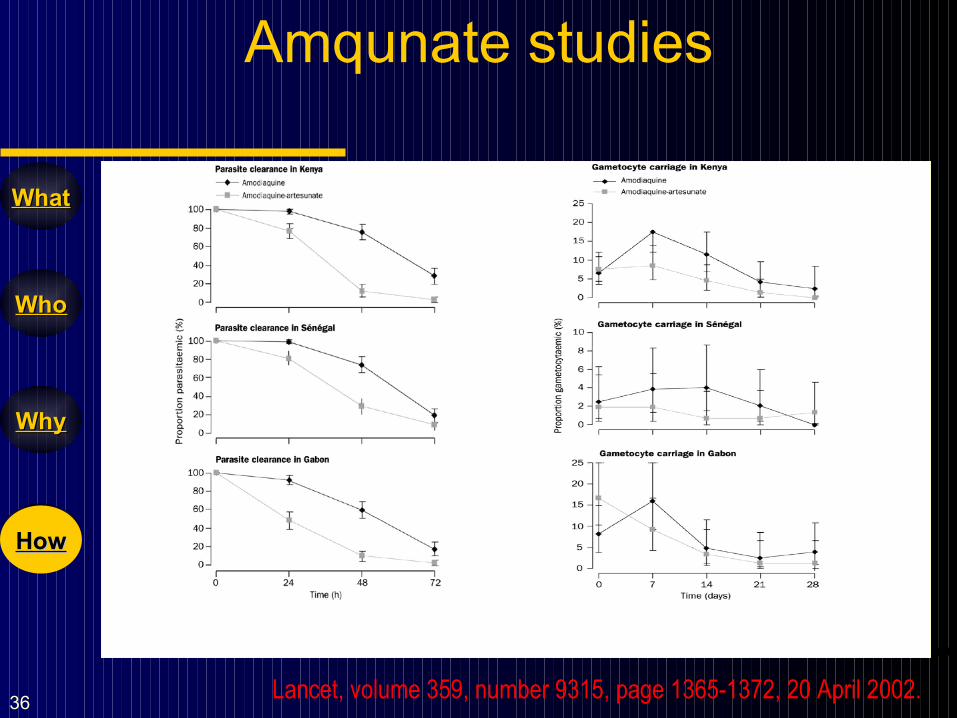
The primary endpoints were measured at days 14 and 28 also.
Artesunate + amodiaquine combination improved treatment efficacy across all the common end points.
HowHow
Lancet, volume 359, number 9315, page 1365-1372, 20 April 2002.
38
WhatWhat
WhoWho
WhyWhy
HowHow
Amqunate studies
In an individual patients’ data meta-analysis conducted as recently as 2004, 16 randomized trials with 5948 patients were reviewed.
It was seen that addition of 3 days of artesunate to standard therapies resulted in a 70% reduction in the absolute risk of treatment failure.
HowHow
International Artemisinin study group, artesunate combinations for treatment of malaria, meta-analysis, Lancet, 2004, volume 363, page 9-17.
39
WhatWhat
WhoWho
WhyWhy
HowHow
Amqunate studies
This analysis also showed that artesunate generally lowered gametocyte counts in peripheral blood potentially reducing the risk of transmission.
HowHow
International Artemisinin study group, artesunate combinations for treatment of malaria, meta-analysis, Lancet, 2004, volume 363, page 9-17.
40
WhatWhat
WhoWho
WhyWhy
HowHow
One Vital Question
Treatment of Uncomplicated Falciparum Malaria in Southern Vietnam: Can chloroquine or sulfadoxine-pyrimethamine be reintroduced in combination with
artesunate? Clinical Infectious Diseases 2003;37:1461-1466
HowHow
Can Conventional antimalarial Resistance Be Reversed in Combination With
artesunate?
The successful reintroduction of conventional therapies in combination with artesunate depends on epidemiological and / or parasitological factors and is not predictable since it varies from place to place.

41
WhatWhat
WhoWho
WhyWhy
HowHow
Combination Therapies: Brand: Amqunate
HowHow
42
WhatWhat
WhoWho
WhyWhy
HowHow
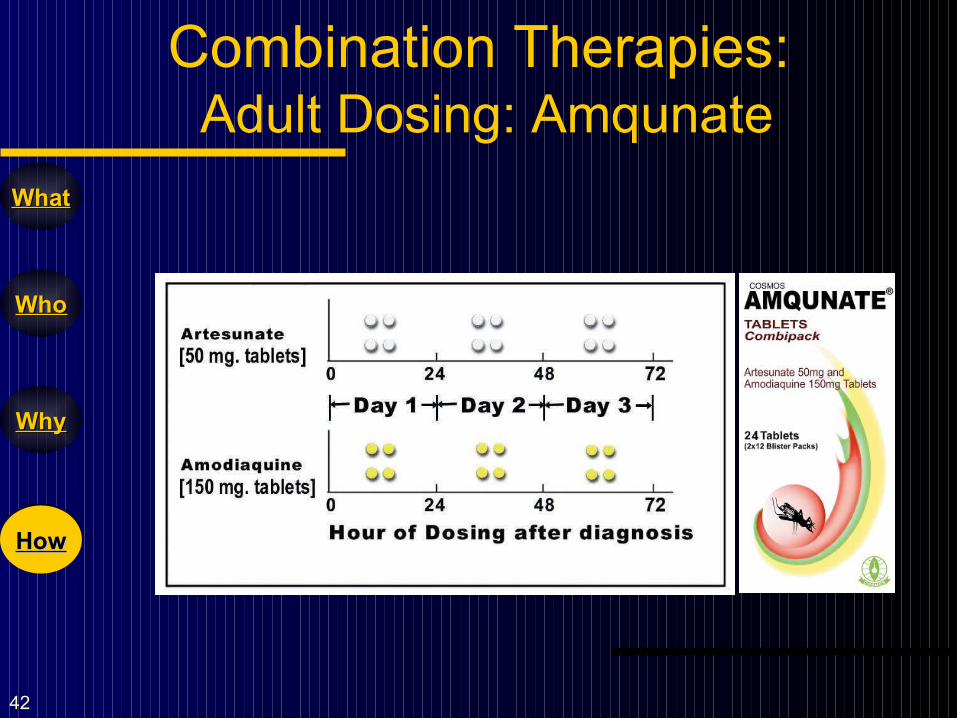
Combination Therapies: Adult Dosing: Amqunate
HowHow
43
WhatWhat
WhoWho
WhyWhy
HowHow
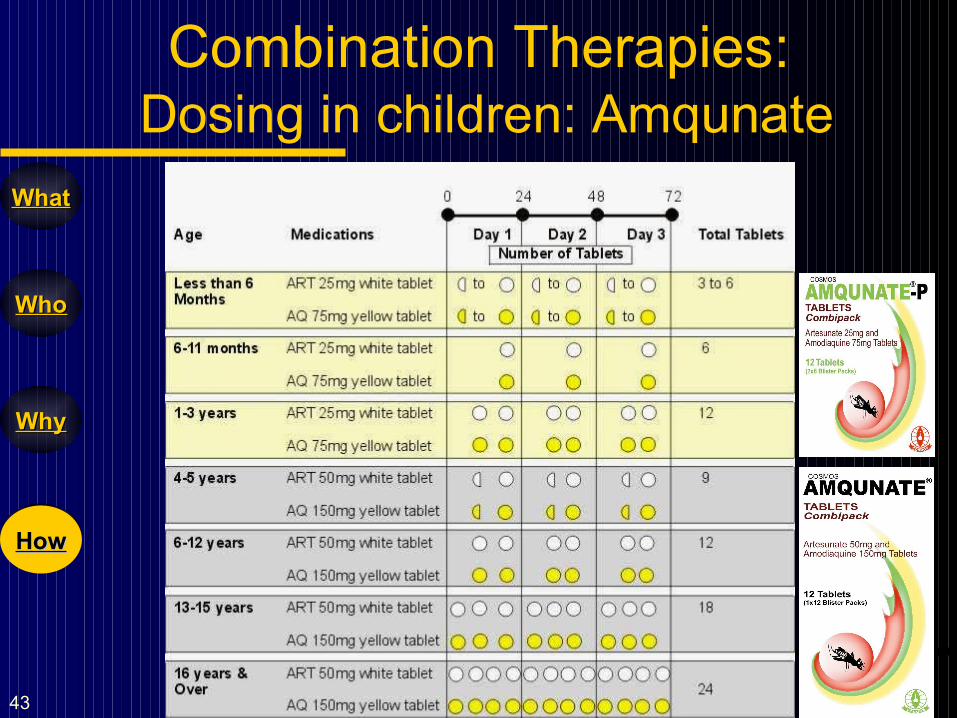
Combination Therapies: Dosing in children: Amqunate
HowHow
44
WhatWhat
WhoWho
WhyWhy
HowHow
Combination Therapies: Comparative Parameters
AS+MQAS+lap / dap
AS+Lumefantrine
Recrudescence rate
Gametocyte carriage
Parasite
clearance times [positivity after day 3]
Fever duration [Fever after 3 days]
DHA+Piperaquine
AS+AQAS+SPParameters
HowHow
45
WhatWhat
WhoWho
WhyWhy
HowHow
Conclusion
New combination in niche market.
Rationally sound dosage forms.
High safety profile / very low side effects.
Good success rates > 90%.
Faster efficacy - 90% of parasitaemia is cleared
within 24 hours.
Economical.
HowHow

Thank You!







