
Ethical Considerations Regarding Competence in Military Psychologists Managing Dual Roles
as an Officer and Mental Health Care Provider
Seth D. Norrholm, Ph.D.
Emory University School of Medicine
Department of Psychiatry and Behavioral Sciences
Georgia Psychological AssociationAugusta, GA
April 16, 2016

https://www.youtube.com/watch?v=rNx3-R13FtAhttp://www.virtuallybetter.com/products-
training-technology/

Overview• Introduction
• Military Mental Health Providers
• Ethical Considerations–Dual roles–Competency and Potential Threats– Safeguards
• “Ellie” - Discussion
Military Mental Health Care Provider
• Tours of duty may include psychologically traumatic situations
• Potential for repeated exposure to DSM-5 Criterion A for posttraumatic stress disorder (PTSD)
(APA, 2013; W.B. Johnson et al., 2011)
Traumatic exposure can occur through direct contact in theater or via interactions with other service members (casual or clinical)

Ethical Considerations
• Dual loyalties – to client/patient and to military/government organization
• Conflicts of Interest
Threats to Competence- including impairment of one’s ability to
self-assess competence to practice
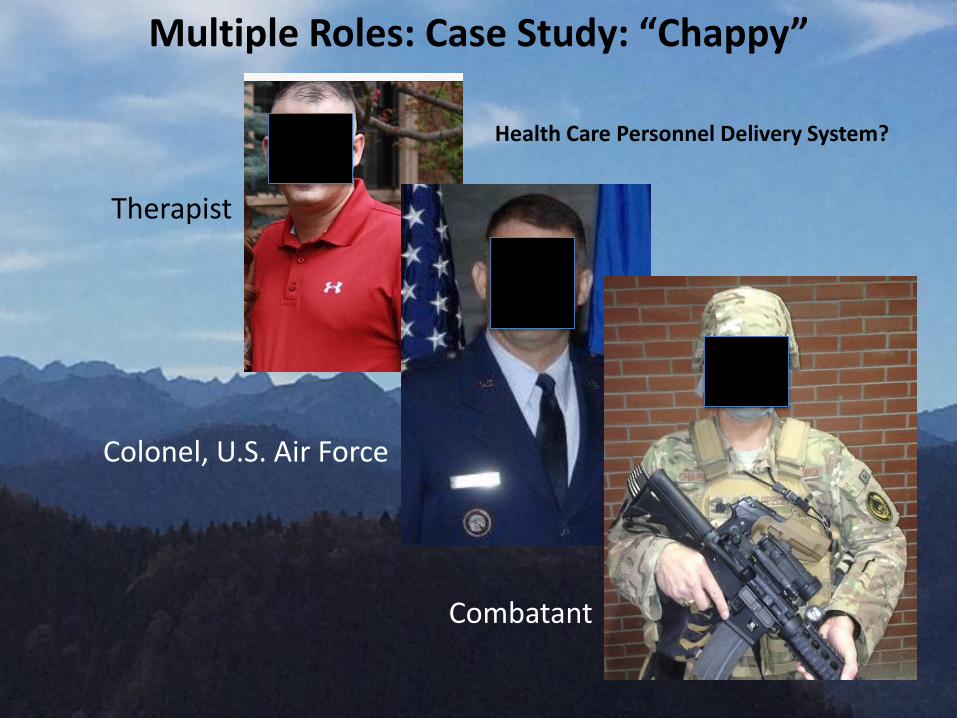
Multiple Roles: Case Study: “Chappy”
Therapist
Colonel, U.S. Air Force
Combatant
Health Care Personnel Delivery System?
Dual Roles• Military officer – duties and responsibilities as
determined by government supervisory agent (e.g., Department of Defense, U.S. Army, Commanding Officers)
• Mental Health Care Provider – uphold the principles and standards requisite with the position (e.g., APA, NASW)
Mixed Agency Dilemma

Mixed Agency Dilemma• Include, but not limited to:
– conflict between DoD regulations and APA Ethics
– ambiguity regarding who the “client” is when making decisions such as fitness for duty
– conflict between superior officers’ intentions and client’s well-being
(Kennedy & Johnson, 2009)

Ethical Principles of Psychology and Code of Conduct(Ethics Code, American Psychological Association, 2010)
• Individual psychologist accountable for maintaining competence to practice
• General Principle A: “be aware of the possible effect of their own physical and mental health on their ability to help those with whom they work (APA, 2010, p. 3)”
• Standard 2.06, “Personal Problems and Conflicts”(a) Psychologists refrain from initiating any activity when they
know or should know that there is a substantial likelihood that their personal problems will prevent them from performing their work-related activities in a competent manner.
Ethical Principles of Psychology and Code of Conduct(Ethics Code, American Psychological Association, 2010)
(b) When psychologists become aware of personal problems that may interfere with their performing work-related duties adequately, take appropriate measures, such as obtaining professional consultation or assistance, and determine whether they should limit, suspend, or terminate their work-related duties (APA, 2010, p. 5)

Threats to Competency
• As a result of combat exposure:
– developing triage hierarchies
– rendering aid to foreign combatants
– directly observing, experiencing, or hearing about horrific and disturbing events (e.g., mutilations, death, destruction, despair)
(Gibbons et al., 2012; Johnson et al., 2014; Johnson & Kennedy, 2010; Larner & Blow, 2011; McLean, 2013)

Combat Involves Exposure to Multiple Types of Traumatic Events, Often Repeatedly

Re-experiencing symptoms as a result of fear conditioning and stimulus generalization
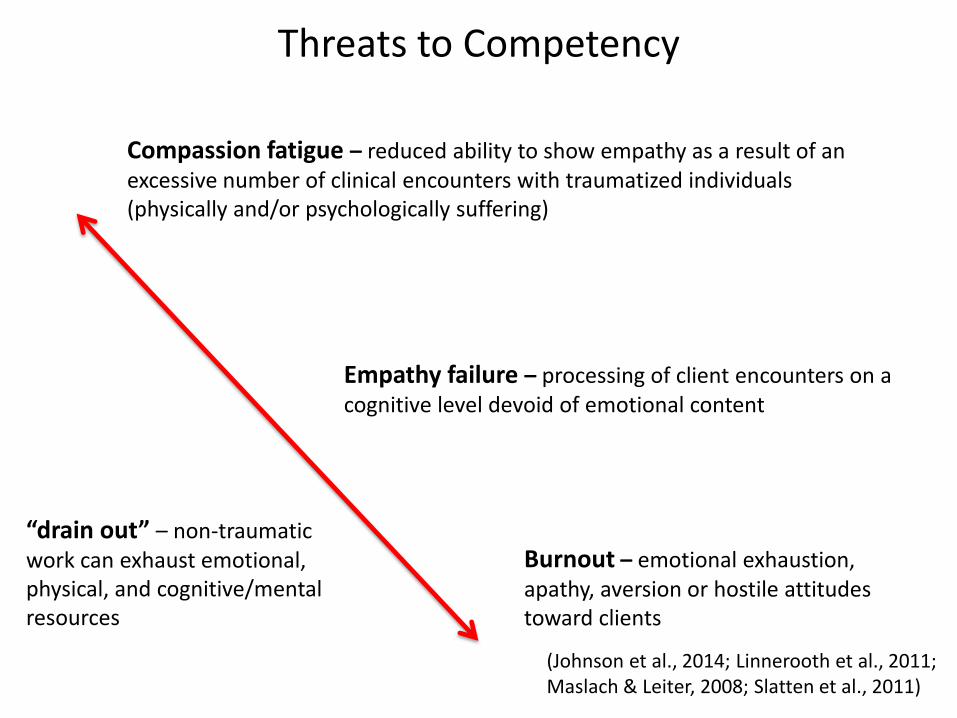
Threats to Competency
Compassion fatigue – reduced ability to show empathy as a result of an excessive number of clinical encounters with traumatized individuals(physically and/or psychologically suffering)
Empathy failure – processing of client encounters on a cognitive level devoid of emotional content
Burnout – emotional exhaustion, apathy, aversion or hostile attitudes toward clients
(Johnson et al., 2014; Linnerooth et al., 2011; Maslach & Leiter, 2008; Slatten et al., 2011)
“drain out” – non-traumatic work can exhaust emotional, physical, and cognitive/mental resources
• Secondary Traumatic Stress
– also termed indirect traumatization
– can occur through vicarious experience of traumatic events, descriptions, and imagery from interactions with fellow service members (clinical and non-clinical)
– can alter a clinician’s cognitions, expectations, interpersonal relationships, sense of self
– Danger of jeopardizing compliance with Ethics Standard 2.06• Herman (1992) suggested that repeated vicarious exposure could
make the clinician “suspect among their colleagues (Herman, 1992, p. 9).”
Threats to Competency
(Pearlman & Saakvitne, 1995; Voss Horrell et al., 2011)

Case Study: Dr. B
• Board Certified Clinical Psychologist
– Working with DoD for 12 years
• Residency at Ft. Gordon, GA (prescribing Ph.D.)
• Has been completing aeromedical evaluations for 10 years
10 years active duty in the U.S. Army (deployed to Iraq) Assignments include Ft. Bragg (home of the 82nd Airborne) and Ft. Carson

Case Study: Dr. B
“SSG J made everyday at our clinic interesting. He loved his jazz music, and was proud to serve
double duty as a pharmacy tech and on the PSD (Personnel Support Detachment). Right
before he died, I would often joke with him about his new hairdo – he was starting to grow
it out and rebel a little after being in country for so long. The day before he died – we were
joking about if he was “crazy” to want to try out for Special Forces – I told him “just crazy
enough.” He would have done well. To SSG J’s family – know that he made a difference
every day taking care of other soldiers. I will miss his smile and sense of humor.”
- Dr. B
fallenheroesmemorial.com
SSG J died in Baghdad, Iraq when an improvised explosive device (IED) detonated near his humvee causing it to rollover
CaseStudy: Dr. P
• Chief of Behavioral Health Services
and Captain in the U.S. Army
“[I] was tasked with deciding who went to war, who returned home, who would deploy at a later date to the combat zone, who could redeploy, and who couldn’t.”
Psirakis, 2009
Emotional Competence
• one’s emotional, psychological, and interpersonal functioning
– assumed to be intact in competent mental health provider
– self-knowledge, self-awareness, self-monitoring
Pope & Vasquez, 2011; Doverspike, 2015, personal communication
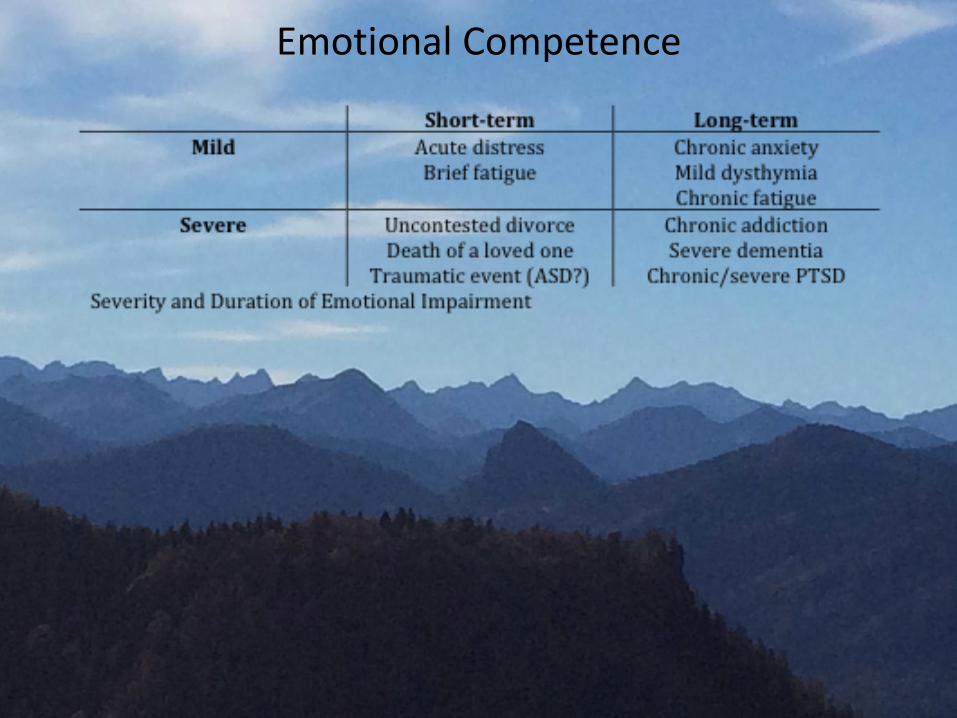
Emotional Competence

Self-assessment of Competence
• often biased, inconsistent, and repeatedly an overestimation of one’s present capabilities in the absence of repeated trauma exposure
• self-ratings can be worsened during deployment, following repeated exposure to traumatic material, and/or in the presence of clinically significant signs and symptoms
(Johnson et al., 2014; Johnson et al., 2012; Johnson & Koocher, 2011)

Safeguards

Safeguards
• From service member, combat Veteran, first responder, trauma physician, and palliative care literature:
(Daneault, 2008; Johnson et al., 2014;Trippany et al., 2004)
- increased clinical experience- strong sense of self-efficacy- manageable caseload - strong social support system- personal psychotherapy

Safeguards: In Practice
• Pursuit of self-care
– exercise
– good nutrition
– effective sleep hygiene
– recreation
– interacting with colleagues
(Trippany et al., 2004; Linnerooth et al., 2011;Johnson et al., 2012)

Safeguards: In Practice

Diversity/Multi-cultural Considerations
• Religious beliefs/faith system
– concurrent spirituality support
• Ethnocultural background
– trauma history
– sex, SES, education
– processing of guilt (e.g., Korean ferry disaster)

“Ellie”- virtual human as part of SimSensei program- effort to avoid stigma associated with therapy- clinician aid for decision making- can detect object, physiological signs of distress
- tone of voice, gaze, head movement- Veterans who interacted with Ellie
- “good to be able to just talk”- “made me feel like I wasn’t being judged”
Ethical thoughts on Ellie as a supplementary clinical tool?
References
• American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, DSM-5. Arlington, VA: American Psychiatric Association.
• American Psychological Association. (2010). Ethical principles of psychologists and code of conduct. http://www.apa.org/ethics/code/index.aspx• Daneault, S. (2008). The wounded healer. Canadian Family Physician, 54, 1218-1219. • Figley, C. R. (2002). Compassion fatigue and the psychotherapist's chronic lack of self care. . Journal of Clinical Psychology, 58, 1433-1441. • Gibbons, S. W., Barnett, S. D., Hickling, E. J., Herbig-Wall, P. L., & Watts, D. D. (2012). Stress, coping, and mental-health seeking behaviors: gender
differences in OEF/OIF health care providers. Journal of Traumatic Stress, 25, 115-119. • Herman, J. (1992). Trauma and recovery. New York, NY: Basic.• Johnson, W. B., Barnett, J. E., Elman, N. S., Forrest, L., & Kaslow, N. J. (2012). The competent community: toward a vital reformulation of professional
ethics. American Psychologist, 67, 557-569. doi: 10.1037/a0024433• Johnson, W. B., Bertschinger, M., Snell, A. K., & Wilson, A. (2014). Secondary trauma and ethical obligations for military psychologists: preserving
compassion and competence in the crucible of combat. Psychological Services, 11(1), 68-74. doi: 10.1037/a0033913• Johnson, W. B., Grasso, I., & Maslowski, K. (2010). Conflicts between ethics and law for military mental health providers. Military Medicine, 175, 548-
553. • Johnson, W. B., Johnson, S. J., Sullivan, G. R., Bongar, B., Miller, L., & Sammons, M. T. (2011). Psychology in extremis: preventing problems of
professional competence in dangerous practice settings. Professional Psychology: Research and Practice, 42, 94-104. • Johnson, W. B., & Kennedy, C. H. (2010). Preparing psychologists for high-risk jobs: key ethical considerations for military clinical supervisors.
Professional Psychology: Research and Practice, 41, 298-304. doi: 10.1037a0019899• Johnson, W. B., & Koocher, G. P. (2011). Ethical conundrums, quandaries, and predicaments in mental health practice: a casebook from the files of
experts. New York, NY: Oxford University Press.• Kennedy, C. H., & Johnson, W. B. (2009). Mixed agency in military psychology: applying the American Psychological Association ethics code.
Psychological Services, 6, 22-31. doi: 10.1037/a0014602• Larner, B., & Blow, A. (2011). A model of meaning making coping and growth in combat veterans. Review of General Psychology, 15, 187-197. • Linnerooth, P. J., Mrdjenovich, A. J., & Moore, B. A. (2011). Professional burnout in clinical military psychologists: recommendations before, during,
and after deployment. Professional Psychology: Research and Practice, 42, 87-93. doi: 10.1037/a0022295• Maslach, C., & Leiter, M. P. (2008). Early predictors of job burnoutand engagement. Journal of Applied Psychology, 93, 498-512. doi: 10.1037/0021-
9010.93.3.498• McLean, C. P., Handa, S., Dickstein, B. D., Benson, T. A., Baker, M. T., Isler, W. C., . . . Litz, B. T. (2013). Posttraumatic growth and posttraumatic stress
among military medical personnel. Psychological Trauma: Theory, Research, Practice, and Policy, 5(1), 62-68. • Pearlman, L. A., & Saakvitne, K. W. (1995). Trauma and the therapist: countertransference and vicarious traumatization in psychotherapy of incest
survivors. New York, N.Y.: Norton.• Psirakis, A. (2009). Deciding who is sane enough to fight. In P. P. Driscoll & C. Straus (Eds.), Hidden Battles on Unseen Fronts. Havertown, PA:
Casemate.• Slatten, L. A., David, C. K., & Carson, P. P. (2011). Compassion fatigue and burnout: what managers should know. The Health Care Manager, 30, 325-
333. • Tabor, P. D. (2011). Vicarious traumatization: concept analysis. Journal of Forensic Nursing, 7, 203-208. doi: 10.1111/j.1939-3938.2011.01115.x• Trippany, R. L., Kress, V. E. W., & Wilcoxon, S. A. (2004). Preventing vicarious trauma: what counselors should know when working with trauma
survivors. Journal of Counseling and Development, 82, 31-37. doi: 10.1002/j.1556-6678.2004.tb00283.x• Voss Horrell, S. C., Holohan, D. R., Didion, L. M., & Vance, G. T. (2011). Treating traumatized OEF/OIF veterans: how does trauma treatment affect the
clinician? Professional Psychology: Research and Practice, 42, 79-86. doi: 10.1037/a0022297







