
DOI 10.1378/chest.111.4.910 1997;111;910-915Chest
and Gila BenchetritPierre-Yves Carry, Pierre Baconnier, Andre Eberhard, Pierre Cotte of Respiratory WaveformsPlethysmography : Accuracy for Analysis Evaluation of Respiratory Inductive
http://chestjournal.chestpubs.org/content/111/4/910
services can be found online on the World Wide Web at: The online version of this article, along with updated information and
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
written permission of the copyright holder.article or PDF may be reproduced or distributed without the priorRoad, Northbrook, IL 60062. All rights reserved. No part of this 1997 by the American College of Chest Physicians, 3300 DundeePhysicians. It has been published monthly since 1935. Copyright
is the official journal of the American College of ChestCHEST
1997 by the American College of Chest Physicians at UJF-INP Grenoble SICD1 on June 3, 2010chestjournal.chestpubs.orgDownloaded from

Evaluation of Respiratory InductivePlethysmography*Accuracy for Analysis of Respiratory WaveformsPierre-Yves Carry, MD, PhD; Pierre Baconnier, PhD; Andre Eberhard, PhD;Pierre Cotte; and Gila Benchetrit, MD, PhD
Objective: To assess the accuracy of respiratory inductive plethysmography (RIP) waveforms tothose obtained with whole body plethysmograph (BP) as this device gives a plethysmographicsignal and a pneumotachograph (PNT).Design: Randomized controlled trial.Setting: Physiologic laboratory in a university hospital.Participants: Eleven subjects from the laboratory staff.Interventions: This study was achieved during four consecutive periods in subjects breathingspontaneously and through different added resistive loads. Using the least square methodcalibration, two RIP waveforms, VRiP.BP(t) and VRiP.PNT(t), were simultaneously calculated withcoefficients obtained from BP and from PNT volume waveforms, respectively VBP(t) and VPNT(t).For each recording, to compare volume waveforms, we calculated their differences in term ofdistances, Drip-bp and Drip-pnt, between the normalized RIP volume signal (respectively,VRiP.BP[t] and VRiP.PNT[t]) and its normalized reference (respectively, VBP[t] and VPNT[t]). We alsocalculated the distance Dpnt-bp between the two normalized references VBP(t) and VPNT(t).Results: No significant effect of load or time on the distance occurred. Including all therecordings, the mean distance Drip-bp (3.4± 1.1%) appears significantly lower than both the meandistance Drip-pnt (4,5±1.3%; p<0.04) and the mean distance Dpnt-bp (4.6±0.9%; p<0.008). Foreach period or load level, Drip-bp appears to be lower than Drip-pnt and Dpnt-bp.Conclusion: The RIP seems reasonably accurate for analysis of respiratory waveform whilesubjects subsequently breathe against resistive loads. (CHEST 1997; 111:910-15)
Key words: body plethysmography; respiratory inductive plethysmography; volume waveform
Abbreviations: ABD=abdomen; ANOVA=analysis of variance; BP=body plethysmograph; Dpnt-bp=distance be¬tween PNT waveform and body plethysmograph waveform; Drip-bp=distance between RIP waveform calibrated withbody plethysmograph and body plethysmograph waveform; Drip-pnt=distance between RIP waveform calibrated withpneumotachograph and pneumotachograph waveform; FetC02=fractional end-tidal C02; Pbody=pressure measuredby a pressure transducer; PNT=pneumotachograph; RC=rib cage; RIP=respiratoiy inductive plethysmograph;R4.7=resistive ventilatory load of 4.7 cm H20/L/s; R7.5=resistive ventilatory load of 7.5 cm H20/L/s; V=flow at mouth;VBP(t)=waveform from body plethysmographic signal; VBP(t)=normalized waveform from body plethysmographicsignal; VPNT(t) =waveform from pneumotachograph signal; VPNT(t)=normalized waveform from pneumotachographsignal; VRiP.BP(t)=waveform from RIP signal calibrated with body plethysmograph; VRip.BP(t)=normalized waveformfrom RIP signal calibrated with body plethysmograph; VRiP.PNT(t) ^waveform from RIP signal calibrated withpneumotachograph; VRiP.PNT(t)=normalized waveform from RIP signal calibrated with pneumotachograph; VT=tidalvolume
T^\ ifferent circumstances in anesthesia and inten--*-^ sive care can modify respiratory drive.1 Re¬cently, Renchetrit et al,2 using a quantitative analysisof respiratory waveforms, demonstrated that primaryvariables (frequency, mean inspiratory flow rate, andfractional inspiratory time) commonly used for mon¬itoring of breathing pattern are not sensitive enoughto detect respiratory personality differences. One
*From the Faculte de Medecine de Grenoble, PRETA-TIMC/IMAG, La Tranche, France.Supported by the University Hospital of Lyon (Dr. Carry).Manuscript received January 23, 1996; revision accepted October 2.
might expect that the monitoring of respiratorypattern via such a waveform analysis could help in
detecting respiratory drive changes in anesthesia andintensive care.
The quantitative analysis of respiratory waveformsdeveloped by Renchetrit et al2 (harmonic or Fourieranalysis) relies on the precise measurement of air¬flow profile. In the intubated patient, this analysis ofbreathing pattern is easy to perform by attaching a
spirometer or a pneumotachograph (PNT) to thepatient's endotracheal tube. During recovery fromanesthesia or during weaning from mechanical ven-
910 Clinical Investigations
1997 by the American College of Chest Physicians at UJF-INP Grenoble SICD1 on June 3, 2010chestjournal.chestpubs.orgDownloaded from

tilation, problems arise because these devices, re¬
quiring a direct connection to the patient's airway,demonstrate a low tolerance.3 In addition, the use ofmouthpiece produces spurious alterations in thebreathing pattern, causing tidal volume (Vt) toincrease and respiratory frequency to decrease.47Other devices, such as body plethysmograph (RP),allowing the measurements of respired volumes, are
not convenient for clinical monitoring, particularlyduring a prolonged period or during sleep. Conse¬quently, devices have been developed to measure
ventilation directly.Respiratory inductive plethysmography (RIP) is
the most widely accepted method for quantitativeand qualitative noninvasive respiratory measure¬
ments.810 When correctly calibrated, the RIP allowsthe measurement of volume and time components ofthe breathing cycle as well as the relative participa¬tion of thorax and abdomen to this cycle.To our knowledge, the study of Stromberg et al11
is the only one that investigates the reliability of thetime course profile of RIP as compared to that of thePNT. While studying the influence of RIP accuracyon the respiratory phase chosen for the calibration,these authors observed that RIP underestimatedlung volume at the start of inspiration and overesti¬mated lung volume at the end of inspiration. Theyobserved a similar tendency during expiration.As RIP is supposed to give a plethysmographic
waveform,12 we undertook the present work to assess
the accuracy of RIP waveform by comparing it withthe volume waveform obtained from the whole RP.We also carried out the same comparison with thePNT as this device is commonly used for breathingpattern analysis.2 The waveforms of the RIP volumecalibrated, respectively, with a RP and a PNT were
compared with the waveforms of the volume ob¬tained, respectively, with RP and with PNT. Thisstudy was achieved in subjects breathing spontane¬ously and through added resistive loads to simulaterespiratory diseases.
Table 1.Subject Characteristics*
Materials and Methods
SubjectsEleven healthy subjects (eight male, three female) without
histoiy of respiratory disease, recruited from the laboratory staff,volunteered for RIP validation against BP and PNT. The protocolwas approved by the local ethics committee and all subjects gaveinformed consent. The characteristics of these subjects are
presented in Table 1.
ApparatusMeasurements were made with the subjects seated in a
690-L barometric whole BP. This device (Pulmostar SMB;
Subject/Sex/Age,vr
Weight, Ve,L/min
F,/min
FetC02%
l/M/272/M/463/M/234/M/385/M/286/F/247/F/258/F/339/M/3710/M/45ll/M/47
6890779265545557687572
11.712.212.512.78.7
12.09.17.97.19.0
12.1
101414181019111188
13
5.04.54.44.55.14.63.95.54.65.54.0
*Ve=minute ventilation; F=respiratory frequency.
Geneva, Switzerland), with high-frequency response, allowedthe measurements of rapid volume changes.13 A pressuretransducer measured the pressure (Pbody) of gas compressedin BP by pulmonary volume changes, giving after calibration(see below) a first volume waveform VBP(t). During protocol,absence of gas leaks in the BP was checked by measuring thestability of Pbody during a voluntary apnea. Stability of BP
temperature during each recording was checked by the aver¬
age stability of Pbody signal (no drift). A heated PNT (Fleisch;Lausanne, Switzerland) inserted in the front wall of the BPmeasured the flow at mouth (V). The zero flow of this channelwas carefully set at the beginning of each protocol but was not
readjusted afterward. The volume waveform from PNT,VPNT(t), was obtained by numerical integration of flow. Afterzero setting, BP and PNT were calibrated with a 1-L syringebefore each procedure.14 The coefficient of calibration foreach signal was determined from five syringe maneuvers.
The rib cage (RC) and abdominal (ABD) displacements were
measured using a direct current-coupled RIP. This device con¬
sists of two belts, to which wavy coated wires are attached, thatencircle the RC and the ABD. A garment incorporating the twocoils was developed in our laboratory. It consists of a sleevelessjacket, made of a special fabric with texture allowing horizontalwiredrawing only.15
During each experiment, the subject had his or her backapplied to a wall inside the BP and was instructed to avoid anychanges in position to prevent interference of changes in spinalattitude with RIP calibration. This calibration is based on theassumption that the respiratory system behaves with two degreesof freedom motion16 such that the change in lung volume (Vrip)is the sum of the volume changes of the rib cage (Vrc) andabdominal (Vabd) compartments. Vrc and Vabd are expressedin terms of RC and ABD signals by the volume-motion coeffi¬cients a and b: VRiP=a-RC+b-ABD.The a and b coefficients are obtained by the least squares
calibration procedure.17 Two RIP waveforms (VRiP.BP[t] andVRiP.PNT[t]) are simultaneously calculated with coefficients ob¬tained respectively from BP volume waveform (VBPft]) and fromPNT volume waveform (VPNT[t]). The a and b coefficients were
calculated from the data recordings from each situation, thusallowing comparisons based on the same source data.
All signals (Pbody, V, ABD, and RC) were recorded on a
computer (Macintosh Ilci) equipped with a 12-bit analogue-to-digital converter (MacAdios; G.W. Instruments; Boston) andeach signal sampled at 32 Hz (softwares are written in ThinkPascal; Symantec SARL, Surenes, France).
CHEST / 111 / 4 / APRIL, 1997 911
1997 by the American College of Chest Physicians at UJF-INP Grenoble SICD1 on June 3, 2010chestjournal.chestpubs.orgDownloaded from
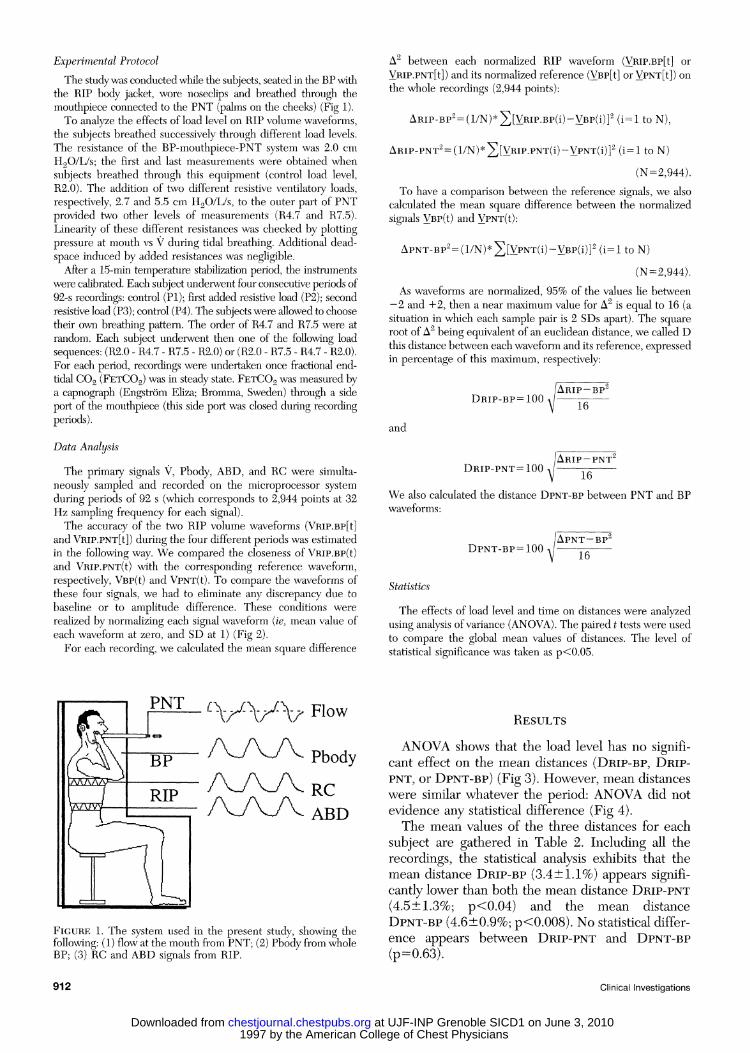
Experimental ProtocolThe study was conducted while the subjects, seated in the BP with
the RIP body jacket, wore noseclips and breathed through themouthpiece connected to the PNT (palms on the cheeks) (Fig 1).To analyze the effects of load level on RIP volume waveforms,
the subjects breathed successively through different load levels.The resistance of the BP-mouthpiece-PNT system was 2.0 cm
H20/L/s; the first and last measurements were obtained whensubjects breathed through this equipment (control load level,R2.0). The addition of two different resistive ventilatory loads,respectively, 2.7 and 5.5 cm H20/L/s, to the outer part of PNTprovided two other levels of measurements (R4.7 and R7.5).Linearity of these different resistances was checked by plottingpressure at mouth vs V during tidal breathing. Additional dead-space induced by added resistances was negligible.
After a 15-min temperature stabilization period, the instrumentswere calibrated. Each subject underwent four consecutive periods of92-s recordings: control (PI); first added resistive load (P2); secondresistive load (P3); control (P4). The subjects were allowed to choosetheir own breathing pattern. The order of R4.7 and R7.5 were atrandom. Each subject underwent then one of the following loadsequences: (R2.0 R4.7 R7.5 R2.0) or (R2.0 R7.5 R4.7 R2.0).For each period, recordings were undertaken once fractional end-tidal C02 (FetC02) was in steady state. FetC02 was measured bya capnograph (Engstrom Eliza; Bromma, Sweden) through a sideport of the mouthpiece (this side port was closed during recordingperiods).Data AnalysisThe primary signals V, Pbody, ABD, and RC were simulta¬
neously sampled and recorded on the microprocessor systemduring periods of 92 s (which corresponds to 2,944 points at 32Hz sampling frequency for each signal).The accuracy of the two RIP volume waveforms (VRiP.BP[t]
and VRiP.PNTft]) during the four different periods was estimatedin the following way. We compared the closeness of VRiP.BP(t)and Vrip.pnt(0 with the corresponding reference waveform,respectively, VBP(t) and VpNT(t). To compare the waveforms ofthese four signals, we had to eliminate any discrepancy due tobaseline or to amplitude difference. These conditions were
realized by normalizing each signal waveform (ie, mean value ofeach waveform at zero, and SD at 1) (Fig 2).For each recording, we calculated the mean square difference
A2 between each normalized RIP waveform (VRiP.Bp[t] or
VRiP.PNT[t]) and its normalized reference (VBP[t] or VPNT[t]) on
the whole recordings (2,944 points):
ARiP-BP2=(l/N)*X[YRiP-BP(i)-VBP(i)]2 (i=l to N),
ARIP-PNT2=(l/N)*XKRIP-PNT(i)~VPNT(i)]2 (i=l to N)(N = 2,944).
To have a comparison between the reference signals, we alsocalculated the mean square difference between the normalizedsignals VBp(t) and VPNT(t):
APNT-BP2=(l/N)*^][VPNT(i)-VBP(i)]2 (i=l to N)(N=2,944).
As waveforms are normalized, 95% of the values lie between.2 and +2, then a near maximum value for A2 is equal to 16 (asituation in which each sample pair is 2 SDs apart). The squareroot of A^ being equivalent of an euclidean distance, we called Dthis distance between each waveform and its reference, expressedin percentage of this maximum, respectively:
and
Drip-bp=100
Drip-pnt=100
Arip-bp216
Arip-pnt16
We also calculated the distance Dpnt-bp between PNT and BPwaveforms:
Dpnt-bp = 100Apnt-bp2
16
Statistics
The effects of load level and time on distances were analyzedusing analysis of variance (ANOVA). The paired t tests were usedto compare the global mean values of distances. The level ofstatistical significance was taken as p<0.05.
PSL<vw Flow
t5p. /vy\yv Pbody^^/WVTVrc
Figure 1. The system used in the present study, showing thefollowing: (1) flow at the mouth from PNT; (2) Pbody from wholeBP; (3) RC and ABD signals from RIP.
Results
ANOVA shows that the load level has no signifi¬cant effect on the mean distances (Drip-bp, Drip-pnt, or Dpnt-bp) (Fig 3). However, mean distanceswere similar whatever the period: ANOVA did notevidence any statistical difference (Fig 4).The mean values of the three distances for each
subject are gathered in Table 2. Including all therecordings, the statistical analysis exhibits that themean distance Drip-bp (3.4±1.1%) appears signifi¬cantly lower than both the mean distance Drip-pnt(4.5±1.3%; p<0.04) and the mean distanceDpnt-bp (4.6±0.9%; p<0.008). No statistical differ¬ence appears between Drip-pnt and Dpnt-bp(p=0.63).
912 Clinical Investigations
1997 by the American College of Chest Physicians at UJF-INP Grenoble SICD1 on June 3, 2010chestjournal.chestpubs.orgDownloaded from

VRIP.PNT(t)VRIP.BP(t)VpNT(t)VBP(t)
B1.5 SD
VRIP.BP(t)YBP(t)
-1.5 SD
Figure 2. (A) The four waveforms Vbp(0, VPNT(t), VRiP.BP(t), and VRiP.PNT(t) for one breath duringa recording period in a representative subject; (B) normalized curves VBP(t) and VRiP.BP(t) waveformsfrom this breath showing that they almost overlap each other; (C) part of VBP(t) and VRlP.BP(t)waveforms has been enlarged and the distance for one sample (VRiP.BP[i] Vbp[i]) is illustrated (seetext for commentary).
Discussion
The purpose of the present study was to test thehypothesis that the RIP volume waveform is as
accurate as that obtained from RP and from PNT. Toconfirm this hypothesis, we analyzed the stability ofthe different signals during the recording period and
demonstrated that the measurements from the RIP,RP, and PNT were comparable.
Following the initial work of Konno and Mead,16several investigators proposed RIP as a method to
analyse RC-ARD motions. In clinical situations, theRIP generally is used for continuous noninvasivemonitoring.18 These different utilizations of RIP
? R2.0
R7.5
Dpnt-bp Drip-bp Drip-pnt
Figure 3. Mean distances Drip-bp, Drip-pnt, and Dpnt-bpfor all subjects while breathing against the three different loadlevels (R2.0, R4.7, and R7.5) (see "Experimental Protocol"section for more details). Results are expressed in percent;vertical bars indicate SD.
D PNT-BP D RIP-BP D RIP-PNT
Figure 4. Mean distances Drip-bp, Drip-pnt, and Dpnt-bpfor all subjects during the successive periods (PI= control,P2=resistive load R4.7 or R7.5 [random], P3= resistive load R7.5or R4.7 [random], P4=control) (see "Experimental Protocol"section for more details). Results are expressed in percent;vertical bars indicate SD.
CHEST/111 IM APRIL, 1997 913
1997 by the American College of Chest Physicians at UJF-INP Grenoble SICD1 on June 3, 2010chestjournal.chestpubs.orgDownloaded from
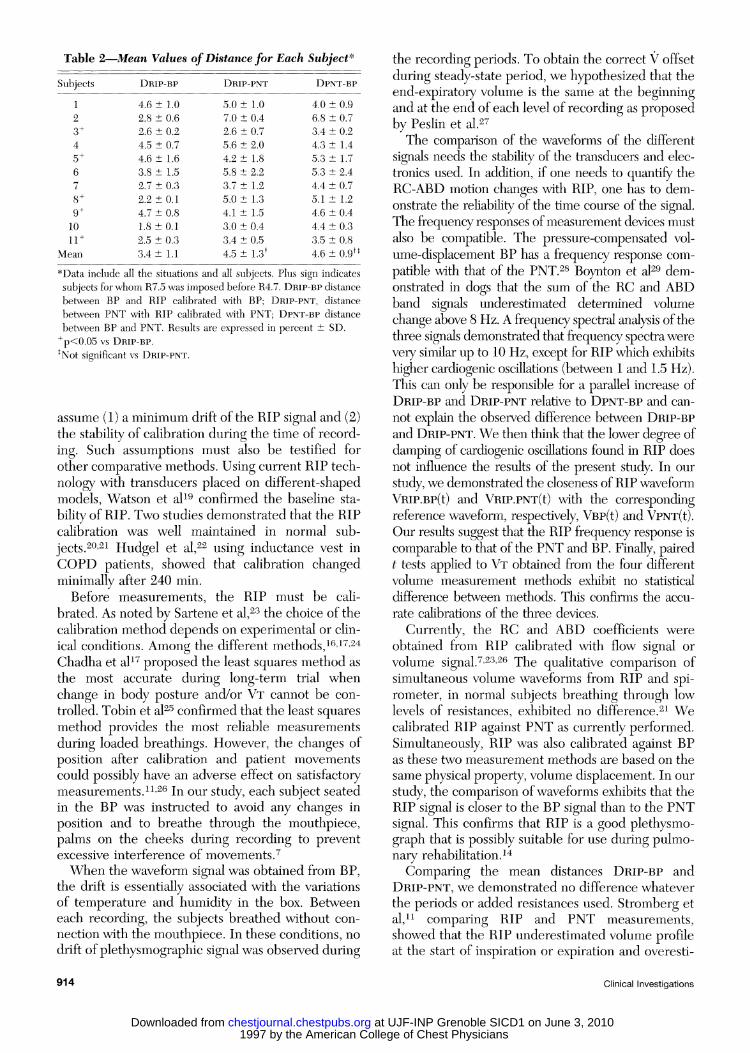
Table 2.Mean Values of Distance for Each Subject*Subjects Drip-bp Drip-pnt Dpnt-bp
9+1011 +
Mean
4.6 ± 1.02.8 ± 0.62.6 ± 0.24.5 ± 0.74.6 ± 1.63.8 ± 1.52.7 ± 0.32.2 ± 0.14.7 ± 0.81.8 ±0.12.5 ± 0.33.4 ± 1.1
5.0 ± 1.07.0 ± 0.42.6 ± 0.75.6 ± 2.04.2 ± 1.85.8 ± 2.23.7 ± 1.25.0 ± 1.34.1 ± 1.53.0 ± 0.43.4 ± 0,54.5 ± 1.3*
4.0 ± 0.96.8 ± 0.73.4 ± 0.24.3 ± 1.45.3 ± 1.75.3 ± 2.44.4 ± 0.75.1 ± 1.24.6 ± 0.44.4 ± 0.33.5 ± 0.84.6 ± 0.9n
*Data include all the situations and all subjects. Plus sign indicatessubjects for whom R7.5 was imposed before R4.7. Drip-bp distancebetween BP and RIP calibrated with BP; Drip-pnt, distancebetween PNT with RIP calibrated with PNT; Dpnt-bp distancebetween BP and PNT. Results are expressed in percent ± SD.
+p<0.05 vs Drip-bp.'Not significant vs Drip-pnt.
assume (1) a minimum drift of the RIP signal and (2)the stability of calibration during the time of record¬ing. Such assumptions must also be testified forother comparative methods. Using current RIP tech¬nology with transducers placed on different-shapedmodels, Watson et al19 confirmed the baseline sta¬
bility of RIP. Two studies demonstrated that the RIPcalibration was well maintained in normal sub¬jects.20-21 Hudgel et al,22 using inductance vest inCOPD patients, showed that calibration changedminimally after 240 min.
Refore measurements, the RIP must be cali¬brated. As noted by Sartene et al,23 the choice of thecalibration method depends on experimental or clin¬ical conditions. Among the different methods,161724Chadha et al17 proposed the least squares method as
the most accurate during long-term trial whenchange in body posture and/or Vt cannot be con¬
trolled. Tobin et al25 confirmed that the least squaresmethod provides the most reliable measurements
during loaded breathings. However, the changes ofposition after calibration and patient movementscould possibly have an adverse effect on satisfactorymeasurements.11-26 In our study, each subject seatedin the RP was instructed to avoid any changes in
position and to breathe through the mouthpiece,palms on the cheeks during recording to preventexcessive interference of movements.7When the waveform signal was obtained from RP,
the drift is essentially associated with the variationsof temperature and humidity in the box. Retweeneach recording, the subjects breathed without con¬
nection with the mouthpiece. In these conditions, no
drift of plethysmographic signal was observed during
the recording periods. To obtain the correct V offsetduring steady-state period, we hypothesized that theend-expiratory volume is the same at the beginningand at the end of each level of recording as proposedby Peslin et al.27The comparison of the waveforms of the different
signals needs the stability of the transducers and elec¬tronics used. In addition, if one needs to quantify theRC-ARD motion changes with RIP, one has to dem¬onstrate the reliability of the time course of the signal.The frequency responses of measurement devices mustalso be compatible. The pressure-compensated vol¬ume-displacement RP has a frequency response com¬
patible with that of the PNT.28 Roynton et al29 dem¬onstrated in dogs that the sum of the RC and ARDband signals underestimated determined volumechange above 8 Hz. A frequency spectral analysis of thethree signals demonstrated that frequency spectra werevery similar up to 10 Hz, except for RIP which exhibitshigher cardiogenic oscillations (between 1 and 1.5 Hz).This can only be responsible for a parallel increase ofDrip-bp and Drip-pnt relative to Dpnt-bp and can¬
not explain the observed difference between Drip-bpand Drip-pnt. We then think that the lower degree ofdamping of cardiogenic oscillations found in RIP doesnot influence the results of the present study. In our
study, we demonstrated the closeness of RIP waveformVRiP.BP(t) and VRlP.PNT(t) with the correspondingreference waveform, respectively, VBP(t) and VPNT(t).Our results suggest that the RIP frequency response is
comparable to that of the PNT and RP. Finally, pairedt tests applied to Vt obtained from the four differentvolume measurement methods exhibit no statisticaldifference between methods. This confirms the accu¬
rate calibrations of the three devices.Currently, the RC and ARD coefficients were
obtained from RIP calibrated with flow signal or
volume signal.7'2326 The qualitative comparison ofsimultaneous volume waveforms from RIP and spi¬rometer, in normal subjects breathing through lowlevels of resistances, exhibited no difference.21 Wecalibrated RIP against PNT as currently performed.Simultaneously, RIP was also calibrated against RPas these two measurement methods are based on thesame physical property, volume displacement. In our
study, the comparison of waveforms exhibits that theRIP signal is closer to the RP signal than to the PNTsignal. This confirms that RIP is a good plethysmo¬graph that is possibly suitable for use during pulmo¬nary rehabilitation.14Comparing the mean distances Drip-bp and
Drip-pnt, we demonstrated no difference whateverthe periods or added resistances used. Stromberg etal,11 comparing RIP and PNT measurements,showed that the RIP underestimated volume profileat the start of inspiration or expiration and overesti-
914 Clinical Investigations
1997 by the American College of Chest Physicians at UJF-INP Grenoble SICD1 on June 3, 2010chestjournal.chestpubs.orgDownloaded from

mated it at the end of inspiration or expiration. Theyattributed these phase differences to the fact that themovements of the RC and the ARD are not linearlyrelated to the lung volume. This discrepancy may beinterpreted by the physical approach. The phasedifferences observed between volume displacement(measured by RIP) and air displacement (measuredby PNT) may be attributed to gas compression whichis similarly observed when volume displacement(measured by RP) and air displacement at mouth are
used to assess airway resistances.25'30The comparison between different signals was
carried out in subjects breathing against differentresistive loads. These resistive loads were lower thanthe values inducing respiratory muscle fatigue pro¬posed by Tobin et al.25 However, the resistive levelsobtained by added resistances were chosen to becomparable with the values of airway resistances
during steady state in some human diseases.9 Thevalues of resistances were calculated with RP using a
reference method to measure resistances.31In conclusion, the results of this study indicate that
the RIP seems reasonably accurate for analysis ofrespiratory waveform while subjects subsequentlybreathe against resistive loads. This confirms thatRIP can be considered as a good plethysmograph. Ifthis were to be also true in clinical situations, one
would then get a precise and noninvasive tool ofchest wall motion monitoring.ACKNOWLEDGMENTS: We gratefully acknowledge the coop¬eration of the staff of PRETA laboratory and V. Banssillon, MD,Professor of Anaesthesiology and Intensive Care.
REFERENCES1 Hornbein TF. Control of breathing. In: Stanley TH, Sperry
RJ, ed. Anesthesia and the lung. Norwell, Mass: KluwerAcademic, 1989;41-6
2 Benchetrit G, Shea SA, Pham Dinh T, et al. Individuality ofbreathing patterns in adults assessed over time. RespirPhysiol 1989; 75:199-210
3 Tobin MJ. Respiratory monitoring in intensive care unit. AmRev Respir Dis 1988; 138:1625-42
4 Gilbert R, Auchincloss JH, Brodsky J, et al. Changes in tidalvolume, frequency and ventilation induced by their measure¬
ment. J Appl Physiol 1972; 33:252-545 Perez W, Tobin MJ. Separation of factors responsible for
change in breathing pattern induced by instrumentation.J Appl Physiol 1985; 59:1515-20
6 Peslin R. Oscillation mechanics of respiratory system. In:Fishman AP, ed. Handbook of physiology, section 3: therespiratory system (vol 3). Bethesda, Md: American Physiol¬ogy Society, 1986; 145-77
7 Sackner JD, Nixon AJ, Davis B, et al. Effects of breathingthrough external dead space on ventilation at rest and duringexercise. Am Rev Respir Dis 1980; 122:933-40
8 Martinot-Lagarde P, Sartene R, Mathieu M, et al. What doesinductance plethysmograph really measure? J Appl Physiol1988; 64:1749-56
9 Tobin MJ, Chadha TS, Jenouri G, et al. Breathing patterns:II. Diseased subjects. Chest 1983; 84:286-94
10 McCool FD, Kelly KB, Loring SH, et al. Estimates of
ventilation from body surface measurements in unrestrainedsubjects. J Appl Physiol 1986; 61:1114-19
11 Stromberg NOT, Dahlback GO, Gustafsson PM. Evaluationof various models for respiratory inductance plethysmographycalibration. J Appl Physiol 1993; 74:1206-11
12 Sackner MA, Rao ASV, Birch S, et al. Assessment of time-volume and flow-volume components of forced vital capacity.Chest 1982; 82:272-78
13 Anthonisen NR. Test of mechanical ventilation. In: FishmanAP, ed. Handbook of physiology, section 3: the respiratorysystem (vol 3). Bethesda, Md: American Physiology Society,1986; 753-84
14 Yeh MP, Gardner RM, Adams TD, et al. Computerizeddetermination of pneumotachometer characteristics using a
calibrated syringe. J Appl Physiol 1982; 53:280-8515 Esteve F, Blanc-Gras N, Baconnier P, et al. A new device for
pulmonary rehabilitation based on visual feedback: I. Princi¬ple and methods. Innov Tech Biol Med 1994; 15:10-9
16 Konno K, Mead J. Measurement of separate volume changesof rib cage and abdomen during breathing. J Appl Physiol1967; 22:407-22
17 Chadha TS, Watson H, Birch S, et al. Validation of respiratoryinductive plethysmography using different calibration proce¬dures. Am Rev Respir Dis 1982; 125:644-49
18 Tobin MJ, Jenouri G, Lind B, et al. Validation of respiratoryinductive plethysmography in patients with pulmonary dis¬ease. Chest 1983; 83:615-20
19 Watson H, Sackner MA, Poole DA. Accuracy of respiratoryinductive plethysmographic cross-sectional areas. J ApplPhysiol 1988; 65:306-08
20 Loveridge B, West P, Anthonisen NR, et al. Single-positioncalibration of the respiratory inductance plethysmograph.J Appl Physiol 1983; 55:1031-34
21 Valta P, Takala J, Foster R, et al. Evaluation of respiratoryinductive plethysmography in the measurement of breathingpattern and PEEP-induced changes in lung volume. Chest1992; 102:234-38
22 Hudgel DW, Capehart M, Johnson B, et al. Accuracy of tidalvolume, lung volume and flow measurements by inductancevest in COPD patients. J Appl Physiol 1984; 56:1656-65
23 Sartene R, Dartus J, Bernard JL, et al. Comparison ofthoracoabdominal calibration methods in normal human sub¬jects. J Appl Physiol 1993; 75:2142-50
24 Sackner MA, Watson H, Belsito AS, et al. Calibration ofrespiratory inductive plethysmograph during natural breath¬ing. J Appl Physiol 1989; 66:410-20
25 Tobin MJ, Guenther SM, Perez W, et al. Accuracy of therespiratory inductive plethysmograph during loaded breath¬ing. J Appl Physiol 1987; 62:497-505
26 Millman RP, Chung DC, Shore ET. Importance of breathsize in calibrating the respiratory inductive plethysmograph.Chest 1986; 89:840-45
27 Peslin R, Gallina C, Sannier C, et al. Fourier analysis versus
multiple linear regression to analyse pressure-flow data dur¬ing artificial ventilation. Eur Respir J 1994; 7:2241-45
28 Mengeot PM, Bates JHT, Martin JG. Effect of mechanicalloading on displacements of chest wall during breathing inhumans. J Appl Physiol 1985; 58:477-84
29 Boynton BR, Glass G, Frantz ID III, et al. Rib cage versus
abdominal displacement in dogs during forced oscillation to32 Hz. J Appl Physiol 1989; 67:1472-78
30 Ingram RH, Schilder DP. Effect of gas compression on
pulmonary pressure, flow, and volume relationship. J ApplPhysiol 1966; 21:1821-26
31 Dubois AB, Botelho SY, Comroe JH. A new method formeasuring airway resistance in man using a body plethysmo¬graph. J Clin Invest 1956; 35:327-35
CHEST/111 /4/APRIL, 1997 915
1997 by the American College of Chest Physicians at UJF-INP Grenoble SICD1 on June 3, 2010chestjournal.chestpubs.orgDownloaded from

DOI 10.1378/chest.111.4.910 1997;111; 910-915Chest
Gila BenchetritPierre-Yves Carry, Pierre Baconnier, Andre Eberhard, Pierre Cotte and
Analysis of Respiratory WaveformsEvaluation of Respiratory Inductive Plethysmography : Accuracy for
June 3, 2010This information is current as of
& ServicesUpdated Information
10http://chestjournal.chestpubs.org/content/111/4/9Updated Information and services can be found at:
Citations
10#related-urlshttp://chestjournal.chestpubs.org/content/111/4/9articles:This article has been cited by 6 HighWire-hosted
Permissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlat: (figures, tables) or in its entirety can be found online Information about reproducing this article in parts
Reprints
http://www.chestpubs.org/site/misc/reprints.xhtmlonline:Information about ordering reprints can be found
Citation Alerts
right of the online article.article. To sign up, select the "Services" link to the Receive free e-mail alerts when new articles cite this
formatImages in PowerPoint
slide format. See any online figure for directions. downloaded for teaching purposes in PowerPoint
articles can beCHESTFigures that appear in
1997 by the American College of Chest Physicians at UJF-INP Grenoble SICD1 on June 3, 2010chestjournal.chestpubs.orgDownloaded from







