

Fakhr Zohair Al-Ayoubi, Msc
Clinical Pharmacist in: CCU & Cardiology Department
Poison Information CenterKKUH May 2010

Introduction• Poisoning is an important public health problem
• In 2009, 2 million human poison exposures were
reported to all poison centers in the US.
• Deaths from Poisoning:
– Total 19,269
– Unintentional14,078
– Suicide 5,191
• Medical costs is estimated at $3 billion in the USClinical Toxicology 1999, Vol. 37, No. 7Miller and Lestina, CDC, 1997
Definition of Poisoning• Toxicology
–The basic since of poisons (old)–The study of the adverse effects of
chemical agents on biological system (new)
• Poison –Any substance that causes injury or
illness or death of a living organism
Definition of Overdose
• Overdose “dose too heavily”
– Ingestion or application of a drug or other
substance in quantities ↑↑ than recommended
or generally practiced.
– Its considered harmful & dangerous, & it can
result in death.

Definition of Overdose
• Overdose “dose too heavily”
– This mean that there is a common safe
dosage & usage for the drug; therefore, the
term is only applied to drugs, not poison
though it should be noted that even certain
poisons are harmless at a low enough
dosage.
Types of Poisoning/Overdose• Accidental “Self-harm”
– Many are this type – Pediatric (most common)– Usually the result of either irresponsible
behavior or the misreading of product labels.
• Intentional “Suicide”– Throughout the ages– The act of deliberately killing oneself murder,
causing your own death suicide & execution.
Type of Poisons
Prescription drug
Over The Counter drugs (OTC)
Herbal medications or preparations
Household chemicals
Industrial chemicals
What do pharmacist provide in the center?
• immediate action real time answer ( for
health care & public)
• Expert & accessible ( coaching)
• Promoting education for all (awareness)
• Registry , statistic : (paracetamol child
resistance caps)
Clinical Pharmacist Role in Poising Management
• Identification of the poison
• Pharmacokinetic / Toxokinetic
• Antidotes dosing & update
• Patient treatment plans
• Monitoring outcomes
• Improving health care & Lay
public awareness
Am J Health-Syst Pharm,2006
Poison Resources
• Primary resources: – Journals
• Secondary resources– Poisondex– Iowa system
• Tertiary resources:– Text books:– Clinical Toxicology
Am J Health-Syst Pharm,2006
Poison Resources
•GUIDE TO POISONOUS AND TOXIC PLANTS From US Army Center for Health Promotion and Preventive Medicine
•Common Antidote Chart Common Antidote Chart From California Poison Control
•Management of Poisoning - A handbook for health care workers By World Health Organization
Poison Resources
• American Association of Poison Control Centers (AAPCC) The AAPCC provides a forum for poison centers and interested individuals to promote the reduction of morbidity and mortality from poisonings through public and professional education and scientific research. It also sets voluntary standards for poison center operations.
Poison Resources
• Basic Analytical Toxicology - WHO By World Health Organization
Guidelines for poison control - WHO By World Health Organization. Contains antidote information for drug poisoning.
Clinical Toxicology - Paddock Labs Clinical Toxicology published by Paddock Lab of Canada. Includes current and practical information on the management of various types of poisoning and overdose emergencies.
Poison Resources• Diseases and Disorders links pertaining to poisoning
A list of links compiled by Karolinska Institutet (a medical university in Sweden), covering topics from bites and stings, to poisoning related to foods, gas, lead, iron, plant, arsenic, mercury, cadmium, nickel, and permanganate, drug toxicity, and hazardous substances.
TOXNET From the National Library of Medicine in the U.S., this site is a collection of of databases on toxicology, hazardous chemicals, and related areas.
Arizona Poison and Drug Information Center Home Provides accessible poison and medication-related emergency treatment advice, referral assistance and comprehensive information on poisons and toxins, poison prevention, and the safe and proper use of medications.
Poison Resources
• Poisons Information Monographs International Programme on Chemical Safety Poison monographs of: Chemical, Pharmaceuticals, Animals, Plants, Bacteria and Fungi
Toxic Exposure Treatment Guides IPCS International Programme on Chemical Safety
AACT - American Academy of Clinical Toxicology An organization uniting scientists and clinicians in the advancement of research, education, prevention and treatment of diseases caused by chemicals, drugs and toxins.
Poison Resources
• EXTOXNET - The Extension Toxicology Network Provides info. on various types of pesticide toxicology and environmental chemistry. These include: discussions of toxicological issues of concern (TICs); toxicology newsletters; other resources for toxicology information; toxicology fact sheets; Pesticide Information Profiles (PIPs); and Toxicology Information Briefs (TIBs).
Consumer Products Safety - Health Canada
General Management
• Decontamination• Supportive care.• Prevent further exposure to the
poison.• Removal of the unabsorbed poison
from the stomach.• Inactivation of the poison remaining
in the stomach.• Enhancement of excretion.• Administration of an antidote.• Symptomatic treatment.
General Management
• General
– Absorption
– Elimination
– Specific antidotes
Absorption
• Gastric lavage
– Indications include coma or impending coma,
seizures, or a depressed gag reflex.
– Only if within 1 hour & life-threatening amount
– Oro-gastric tube should be used.
– Should be done only in older children.
– Never for corrosives & chronic cases
Absorption.... Cont.
• Activated charcoal
– Has no real contraindications and is the treatment of
choice to prevent absorption of the poisoning when
the patient is in the emergency room.
– It is ineffective against cyanides, heavy metals, Na, K,
Cl, ethanol, acids, and bases.
– 50 g single or repeated dose ( elimination)
Absorption.... Cont.
• Cathartic
– Decrease absorption by increasing the rate of
excretion
– Mg Sulphate should not be used if the patient has
renal failure
– Sorbitol
Elimination
• Multiple dose activated charcoal– Quinine, phenobarbitone, Carbamazepine
• Charcoal haemoperfusion– Barbiturates, theophylline
• Diuresis
– may be done using hemodialysis,
hemoperfusion, & peritoneal dialysis.
Elimination....Cont.
• Exchange transfusion
– Only if the patient is unresponsive to
appropriate care.
• Urinary alkalinization
• Whole Bowel Irrigation
Physiological Antidotes Classifications
• Antagonists:– Stimulate where the poisons depressed & vise
versa e.g:
• Diazepam in strychnine poisoning.• Atropine in organophosphorous (antagonize muscarinic
action).• Pilocarpine antagonize peripheral action of atropine.
Physiological Antidotes Classifications.... Cont..
• Chelators:– Antidotes forms chelates which are less toxic &easily excreted
through the kidneys e.g.:
– BAL (British anti-lewisite) in arsenic poisoning.
– EDTA (Ethylene Diamine Tetra-Acetate) in heavy metals poison.
– Desferrioxamine (Desferal) chelator in cases of iron poisoning.
– Penicillamine used as oral chelator in lead poisoning.
Physiological Antidotes Classifications.... Cont..
• Competitors:
– Compete with the poisons at the sites of their
action.
– Naloxone in morphine poisoning but recently used
as a narcotics antidote with no CNS depressant
action.
– Ethyl alcohol in cases of methanol poisoning.

Telephone Protocol For Handling Poison Calls
• I .Initial assessment – Substance– Symptoms – What has been done
• II. History– Basic information– Substance– Amount– Symptoms
• III. Assessment– Toxicity of the substance– Circumstances of exposure– Competency of the caller
Telephone Protocol For Handling Poison Calls
• IV. Treatment plan (one of the following)– No treatment– First aid and observe at home– Syrup of ipecac and observe at home– Refer t o MD, ER,etc
• V. Follow up Made at 0.5 hr,2-4hrs,12hrsor 24hrs
– Has the victim remained asymptomatic– Were instructions followed– Was treatment effective– Poison prevention teaching12– Referral
I .Initial assessment
a) Substance involved:
1) Toxic substance
b) Are symptoms present?
1) irritated, discolored or swollen lips, gums, tongue; coughing, convulsions, acting unusual, can't wake up,
c) What has been done?
1) is immediate first aid necessary e.g. dilution, washing area.
2) has incorrect first aid been done e.g. salt water as emetic.
3) is immediate ER referral indicated?
II. History
A. Basic Information:
1) Name of caller relationship of caller to victim - parent, friend, babysitter, MDRN.
2) Name and age of victim.
3) Weight of victim
4) Phone number.
5) Time of exposure how long has it been?
6) Route of exposure ingestion, inhalation, percu taneous, occular.

II. History
B. Substance:
1) Brand name and other identification form
2) Medication: read prescription label. is there a drug imprint code? what was it supposed to do?
3) Plant has it recently been sprayed?
4) Is it possible anything else involved look around for any other bottles, broken plants
C. Amount:
1) Describe situation tell me exactly what happened? did you see him/her swallow?
2) Extract quantitative details how many/much was there originally? count/measure how much is left when was it purchased? used often?
II. History
D. symptoms: Present Medical condition. does he/she take any medicineregularly? has he/she been sick lately?
II. History
III. Assessment:
A. Toxicity of substance. Poisindex
Reference texts and articles. Manufacturer emergency number Consultants and experts.
III. Assessment
B. Circumstances of Exposure Suicide
Accidental occupational Environmental Drug abuse.
III. Assessment
C. Competency of caller. will they be able to carry out instructions and make
observations?
How important does caller consider exposure to be?
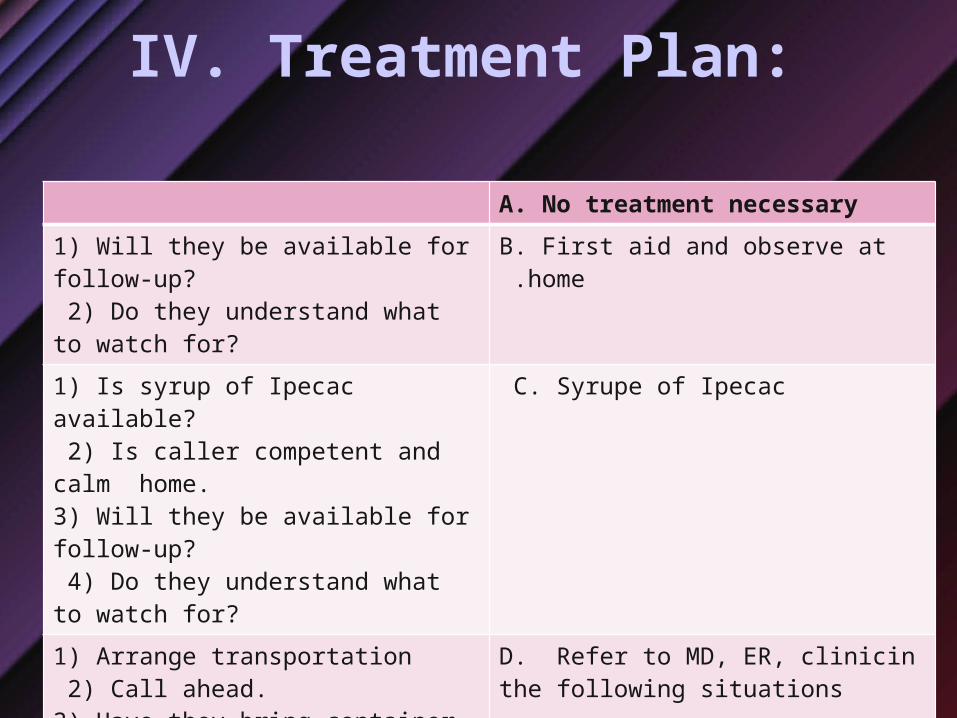
IV. Treatment Plan:
A. No treatment necessary
1) Will they be available for follow-up? 2) Do they understand what to watch for?
B. First aid and observe at home .
1) Is syrup of Ipecac available? 2) Is caller competent and calm home. 3) Will they be available for follow-up? 4) Do they understand what to watch for?
C. Syrupe of Ipecac
1) Arrange transportation 2) Call ahead. 3) Have they bring container, plant with them
D. Refer to MD, ER, clinicin the following situations
highly toxic substance; unknown substance; , unknown amount; signs plant, etc. symptoms not obvious, e.g. EKG changes; unstable situation.
V. Follow-up:
1) Anything at all unusual? 2) Sleeping, eating, etc. normally?
A. Has the victim remained asymptomatic?
1) How much Ipecac did you give2) Did you give water afterward? 3) How long did you wash the eye?
B. Were instructions followed?
1) Did victim vomit? 2) How many times? 3) Were pill fragments present? 4) Is he/she eating all right now?
C. Was treatment effective?
1) Education and first aid .. 2) Poison proof now-low the odds of a repeat.
D. Poison prevention teaching
1) Public health nurse 2) Workers clinic 3) Suicide prevention
E. Referral







