

Heart Failure Disease Management Within the North Florida/South Georgia VHS
Richard S. Schofield MDLynnette Boyer ARNPCardiology Section
North Florida/South Georgia VHS

Epidemiology of Heart Failure in theUnited States
• 5 million patients1; estimated 10 million in 20372
• Incidence: about 660,000 new cases each year1
• Leading cause for inpatient hospitalization in the U.S.
• Costs $37 billion to the U.S. health care system annually3
• Sudden cardiac death is 6 to 9 times higher than in the non-heart failure population1
1991 2001 2037
3.5
5
10.0
Patients in US (millions)
Year
1. American Heart Association. 2008 Heart and Stroke Statistical Update. 2. Croft JB et al. J Am Geriatr Soc. 1997;45:270–275.3. National Heart, Lung, and Blood Institute. Congestive Heart Failure Data Fact Sheet. Available at:
http://www.nhlbi.nih.gov/health/public/heart/other/CHF.htm.

Heart Failure Hospitalizations
HF hospitalizations are increasing for both men and women
CDC/NCHS: hospital discharges include patients both living and dead.American Heart Association. 2002 Heart and Stroke Statistical Update. 2001.
An
nu
al
Dis
ch
arg
es
0
100,000
200,000
300,000
400,000
500,000
600,000
'79 '81 '83 '85 '87 '89 '91 '93 '95 '97
WomenMen
Year
'99

Rates of Hospital Readmission for CHF Patients in the Medicare Program
0
10
20
30
40
50
60
Within 2Days
Within 1Month
Within 6Months
Pa
tie
nts
Rea
dm
itte
d (
%)
2%
20%
50%
Aghababian RV. Rev Cardiovasc Med. 2002;3(suppl 4):S3–S9.

Preventable Causes of CHF Readmissions Are Present in >50% of Cases
0%
10%
20%
30%
40%
50%
1 2 3 4 5 6
29%
34%
29%
37%40%
37%
1= Medical Noncompliance2= Diet Noncompliance3= Inadequate Discharge Planning4= Inadequate F/U5= Failed Social Support6= Failure to Seek Medical AttentionVinson JM et al. J Am Ger Soc, 1990
Prev., 53%
Not Prev., 47%

Heart Failure Within the Veterans Administration
• Leading discharge diagnosis in the VA
• Up to 20% readmission rate within 14 days
• Avg. 1.42 hospital stays,14 inpatient days/year
• > 20 outpatient visits/year
• Approximately $2.5 billion in cost annually
• > 60% mortality at 5 years
1. VA QUERI CHF fact sheet, 2003
2. Med Care 1997;35:7683. Am J Med Qual 1999;14:45
4. Med Care 2000;38:I-26

VA Data - 14 day Outpatient Encounters Following VA Data - 14 day Outpatient Encounters Following HF Discharge (1999-2005)HF Discharge (1999-2005)
0
20
40
60
80
100
%
AnyEncounter
Office Med orCard
Card
CHF QUERI 2007

VA Heart Failure Practice Survey 2008: Physician ResourcesVA Heart Failure Practice Survey 2008: Physician Resources%
of
VA
s
VA Heart Failure QUERI Presentation, 6/29/09

NF/SG VA Heart Failure Team Concept
• The Heart Failure Team was created in response to a need for better utilization of inpatient beds (FIX Committee Initiative)
• The team was designed to target the most high risk cohort of HF patients, and to reduce admissions
• We attempt to screen all inpatient HF admissions
• HF disease management offered to all eligible patients
• Combines inpatient, outpatient, and home telehealth/case management strategies
• Outcomes are tracked for quality improvement

Unique Aspects of this HF Team
• Integrates multiple aspects of HF disease management
• Entry into the program is triggered by a HF admission, therefore targets the highest risk pts
• Early post-discharge clinic follow-up• Care coordination/home telehealth management is
available for appropriate patients• Patient outcomes are tracked in a HF database with
potential for automatic download of data from CPRS• HF-specific quality of life is measured• Directed by HF-specialty trained cardiologist

Identify potential inpatient HF admissions daily (M-F)from medical admissions pull list
Confirm likely HF admissions from brief CPRS chart reviewSubmit an electronic consult
•Complete inpatient consult•Optimize HF therapy•Discharge planning/HF education•Explain HF Team concept •Provide scale and BP cuff
Return to HF outpatient clinic within 7-14 days
6 months of HF clinic for stable ptsLong term HF clinic for complex pts
Enroll in the HF Team
HF Care Coordination and Home Telehealth management for
appropriate patients

Patient Characteristics
Age (years) 70.9 ± 13
Baseline LVEF (%) 33.5 ± 13.9%
NYHA Class III or IV (%) 72%
Ischemic cardiomyopathy (% ) 52%
Males (%) 100%
Body Mass Index 30.7 ± 7
Creatinine (mg/dl) 1.5 ± 0.6
NT-proBNP level (pg/ml) 7,597 ± 7,511
Clinical Characteristics of the First 137 Patients Screened

Patient Enrollment Information
75%
25%
Enrolled Not Enrolled
* Only 7% of all patients screened were enrolled in a telehealth program
Enrollment Breakdown of the First 137 Patients Screened

Sociodemographic Characteristics
Distance (miles)Residence Location
Education Level
Range Mean Rural Urban CollegeNo
College
0 – 279 44.1 73% 27% 39% 61%
Sociodemographic Characteristics of the First 137 PatientsScreened

47
64.457.8
76.6
44.2
59.2
49.4
64.5
0
10
20
30
40
50
60
70
80
HF
Pa
tie
nts
(%
)
PhysicalLimitations
Symptoms SocialLimitation
QOL Domains
KCCQ Score Comparison in Veterans and non-Veterans with HF
KCCQ Scores in Veterans with HF
Literature KCCQ Scores in Stable non-Veterans with HF
Heart Failure-Specific Quality of Life Data on 52 Patients: Comparison with Non-Veterans with HF

55.9 54.3
86 83.3
0
10
20
30
40
50
60
70
80
90
HF
Pati
en
ts (
%)
Symptom Stability Self-Efficacy
KCCQ Symptom Stability and Self-Efficacy in Veterans and non-Veterans with HF
KCCQ scores in veterans with HF
Literature KCCQ scores in stable non-veterans with HF
Heart Failure-Specific Quality of Life Data on 52 Patients: Comparison with Non-Veterans with HF

Medication Usage in the First 137 Patients Screened
Figure 1. Medication Utilization
83.0%85.3%84.5%
15.5%14.7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Spironolactone Digoxin Beta-blocker ACEi/ARB Diuretic
Per
cen
t o
f P
atie
nts

Low Usage of Spironolactone and Digoxin Among the First 137 Patients Screened
Figure 2. Ideal Candidates for Spironolactone and Digoxin Use
36.7%
30.9%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Spironolactone Digoxin
Pe
rce
nt
(%)
of
Pa
tie
nts

HF 30 Day Readmission Rate
4.0%
11%
0%
2%
4%
6%
8%
10%
12%
Previous Fiscal Year HF Program Patients
Rea
dm
issi
on
Rat
e6-Month Outcomes of the Heart Failure Team:
30-day HF Readmission Rate for Primary Dx of HF
64% relative reduction compared to historical
control data
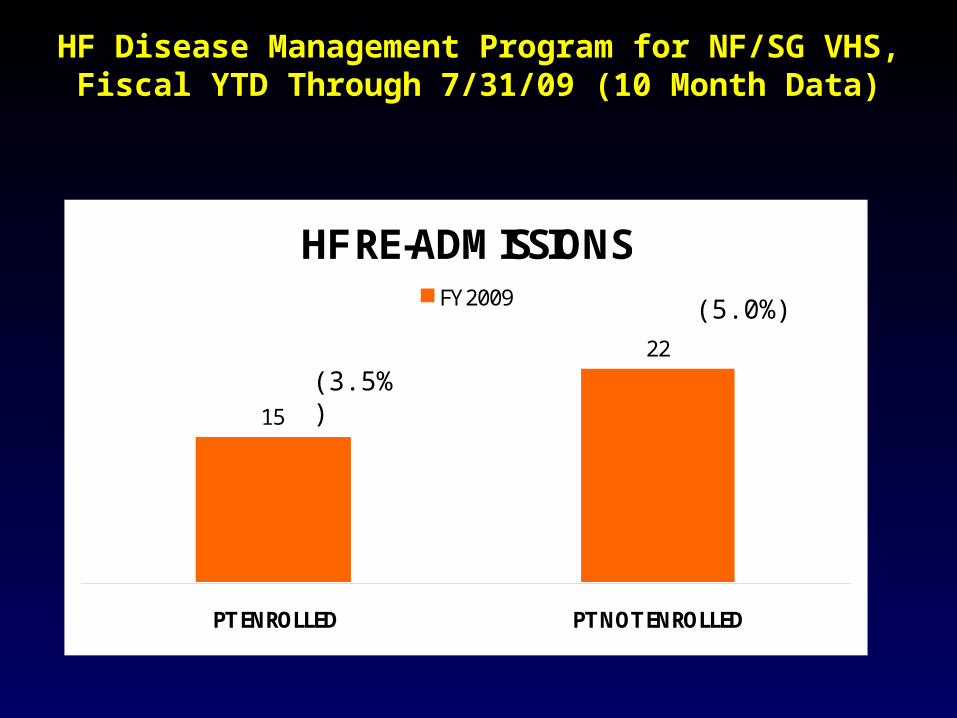
HF Disease Management Program for NF/SG VHS, Fiscal YTD Through 7/31/09 (10 Month Data)
HF RE-ADMISSIONS
15
22
PT ENROLLED PT NOT ENROLLED
FY 2009
(3.5%)
(5.0%)

Barriers to Implementation
• Travel cost reduces pt willingness to come for frequent clinic visits
• Clinic space is limited at our facility
• Broad inclusion of all-comers with HF has revealed a large proportion of patients with diastolic HF, right HF, morbid obesity, and renal failure; these patients will not likely respond well to standard HF therapy or to HF disease management
• Large proportion of very elderly (80+) pts
• Large proportion of pts with multiple co-morbidities
• Limited availability of ICU beds and lack of an IMC unit limits our access to more complex inpatient therapies such as diuretic infusions, inotropes, hemodynamic monitoring (Swan-Ganz catheterization), etc
• Our home telehealth program needs to be expanded

Limitations
• This is a retrospective, observational assessment of data accumulated from clinical chart review of patient data, and placed into a clinical HF database
• The number of patients reviewed thus far is small• Unclear whether short term reductions in hospitalizations
can be sustained over time• No data on mortality • No data on HF subsets (diastolic, right HF, CKD)• These clinical data do not necessarily correlate with other
datasets within the VHA which are derived from discharge codes, therefore results seen may not precisely match with 30 day readmission rates measured from coded data

Conclusions
• In this preliminary analysis, our new HF team led to a dramatic reduction in HF 30-day readmission rates compared to historical control data and to observational data within the program
• Several barriers to fuller implementation of the program have been identified, and will be addressed over time
• This program may offer important insights into the optimal management of high risk patients with HF in the Veterans Health System







