

HEMATOLOGY 101-HEMATOLOGY 101-PRACTICAL SOLUTIONSPRACTICAL SOLUTIONS
By: Jason A. Stern, D.OBy: Jason A. Stern, D.O
January 24,2014January 24,2014

FINANCIAL DISCLOSURESFINANCIAL DISCLOSURES
I WISH…I WISH…
OBJECTIVESOBJECTIVES
Review hemostasis and the hypercoaguable Review hemostasis and the hypercoaguable state.state.
Review pharmacologic interventions and Review pharmacologic interventions and some reversal agents.some reversal agents.
Survey selected common hematologic Survey selected common hematologic disorders and discuss their differential disorders and discuss their differential diagnosis and their management.diagnosis and their management.

COAGULATION CASCADECOAGULATION CASCADE

COAGULATION CASCADE
It’s all about Thrombin
Under normal circumstances, Antithrombin, Activated Protein C & Tissue Factor Pathway Inhibitor (TFPI) keep the endothelial cells an anticoagulant surface.
Antithrombin inhibits thrombin & FX.Activated Protein C inhibits Factors V & VIII.TFPI inhibits FVII.

COAGULATION CASCADE
Thrombin
FVIII amplifies FIXa production, & FV amplifies FXa production.
Thrombin activation accelerates the production of Factors V, VIII, XI, & XIII and promotes platelet aggregation. Thrombin splits fibrinogen to fibrin.

COAGULATION CASCADE
Severe deficiencies of Factors X, V, II, & VII are incompatible with life.
Deficiencies of high molecular weight kininogen, prekallkrein, & FXII increase PTT but are not associated with hemorrhage.
Severe FXIII deficiency does not increase PTT or INR but can be associated with spontaneous intracebral hemorrhage & hemorrhage secondary to trauma/surgery.

RISK FACTORS FOR VENOUS RISK FACTORS FOR VENOUS THROMBOSISTHROMBOSIS
INHERITEDINHERITED
Antithrombin deficiencyAntithrombin deficiencyProtein C deficiencyProtein C deficiencyProtein S deficiencyProtein S deficiencyFactor V Leiden (FVL)----A.P.C. resistanceFactor V Leiden (FVL)----A.P.C. resistanceProthrombin Gene Mutation---Increased Prothrombin Gene Mutation---Increased
prothrombin biosynthesisprothrombin biosynthesis

COAGULATION CASCADECOAGULATION CASCADE

PREVALENCE OF FVL & PREVALENCE OF FVL & PROTHROMBIN GENE MUTATIONPROTHROMBIN GENE MUTATION
PopulationPopulation FVL%FVL% PG%PG%EuropeanEuropean Northern 5-10Northern 5-10 1.7 1.7 Southern 2-3 Southern 2-3 3 3
Middle EastMiddle East IsraeliIsraeli 5 5 5 5 ArabArab 15 15 5 5
African/Asian African/Asian ≤ 1≤ 1 ≤ 1≤ 1

RISK FACTORS FOR VENOUS RISK FACTORS FOR VENOUS THROMBOSISTHROMBOSIS
ACQUIREDACQUIREDAdvancing ageAdvancing age APASAPAS NSNSPrior unprovoked DVTPrior unprovoked DVT MGUS MGUS IBDIBDObesityObesity MPDMPDTobaccoTobacco HITHITMalignancyMalignancy
TRIGGERSTRIGGERS
PregnancyPregnancyOral contraceptivesOral contraceptivesH.R.T.H.R.T.Tamoxifen, RaloxifeneTamoxifen, RaloxifeneTrauma, immobility, travel Trauma, immobility, travel Major surgery Major surgery

RISK FACTORS FOR VENOUS RISK FACTORS FOR VENOUS THROMBOSISTHROMBOSIS
Obesity→ Single most common risk factor for venous thrombosis. > 50% of patients with thrombosis are obese.
Malignancy→ Patients with unprovoked DVT/PE will have a 3-fold increased risk for presenting with an occult malignancy within 3 years of presentation.

D.V.T. MODELD.V.T. MODEL
GeneticsGenetics Acquired Risk Factors Acquired Risk Factors
\ \ / / Intrinsic Thrombosis RiskIntrinsic Thrombosis Risk
ProphylaxisProphylaxis || Triggering Factors Triggering Factors ||
Thrombosis ThresholdThrombosis Threshold ↓ ↓
D.V.T.D.V.T.
WHO NEEDS TESTING FOR WHO NEEDS TESTING FOR HEREDITARY THROMBOPHILIA?HEREDITARY THROMBOPHILIA?
DVT/PE age < 50 with positive family history DVT/PE age < 50 with positive family history first degree relativesfirst degree relatives
Pregnancy loss- 2Pregnancy loss- 2ndnd & 3 & 3rdrd trimester trimester
DVT/PE in association with OCP/HRT, or DVT/PE in association with OCP/HRT, or pregnancypregnancy
Cerebral venous thrombosisCerebral venous thrombosis
Hepatic/Portal/Mesenteric vein thrombosisHepatic/Portal/Mesenteric vein thrombosis
““HYPERCOAGULABLE WORKUP”HYPERCOAGULABLE WORKUP”
Always pursue symptoms or signs which Always pursue symptoms or signs which suggest an underlying malignancy and suggest an underlying malignancy and perform age-appropriate cancer screening perform age-appropriate cancer screening tests. ~20% of all patients will have a tests. ~20% of all patients will have a malignancy. malignancy.
Antithrombin, Protein C, Protein S functional Antithrombin, Protein C, Protein S functional assays—Omit in patients with 1assays—Omit in patients with 1stst thrombus, age >50, & negative family thrombus, age >50, & negative family history.history.

““HYPERCOAGULABLE WORKUP” HYPERCOAGULABLE WORKUP” CONTINUEDCONTINUED
Activated Protein C resistance off Coumadin Activated Protein C resistance off Coumadin or order FVLor order FVL
Prothrombin Gene Mutation (PGM)Prothrombin Gene Mutation (PGM)
DRVVT, ACA, Beta 2 Glycoprotein—Tests DRVVT, ACA, Beta 2 Glycoprotein—Tests for Antiphospholipid Antibodiesfor Antiphospholipid Antibodies
Add PNH Panel and MPD workup for Add PNH Panel and MPD workup for hepatic/portal/mesenteric vein hepatic/portal/mesenteric vein thromboses.thromboses.

CAVEATSCAVEATS
Acute thrombosis will falsely lower Antithrombin, Acute thrombosis will falsely lower Antithrombin, Protein C, & Protein S levels.Protein C, & Protein S levels.
Antithrombin and Lupus anticoagulant testing Antithrombin and Lupus anticoagulant testing affected by Heparin/LMWH.affected by Heparin/LMWH.
Protein C & Protein S levels decreased by Protein C & Protein S levels decreased by Coumadin. Pregnancy & estrogen Coumadin. Pregnancy & estrogen ↓ Protein S ↓ Protein S level.level.
APA—secondary etiologies: SLE, cancer, APA—secondary etiologies: SLE, cancer, infections, & phenothiazines. Must confirm infections, & phenothiazines. Must confirm positive results 3 months later.positive results 3 months later.

DURATION OF ANTICOAGULANT DURATION OF ANTICOAGULANT THERAPYTHERAPY
11STST event with reversible or time limited risk event with reversible or time limited risk factor-3 to 6 months. factor-3 to 6 months.
Unprovoked DVT/PE 1Unprovoked DVT/PE 1stst event. Risk of event. Risk of recurrence with a negative work up ~ 30%. recurrence with a negative work up ~ 30%. 6 months & then consider long-term 6 months & then consider long-term anticoagulation VS Aspirin 81mg/day. ASA anticoagulation VS Aspirin 81mg/day. ASA reduced long-term risk of recurrence by reduced long-term risk of recurrence by 40% in WARFASA study.40% in WARFASA study.

SPECIAL SITUATIONS-SPECIAL SITUATIONS-INDEFINITE ANTICOAGULATIONINDEFINITE ANTICOAGULATION
Antiphospholipid antibodies confirmedAntiphospholipid antibodies confirmedAntithrombin deficiency Antithrombin deficiency → 50% lifetime risk for → 50% lifetime risk for
thrombosisthrombosisProtein C & S Deficiency Protein C & S Deficiency → 75% lifetime risk for → 75% lifetime risk for
thrombosisthrombosisFVL-HomozygousFVL-HomozygousMultiple genetic defects-Risk increases Multiple genetic defects-Risk increases
multiplicativemultiplicativeMetastatic cancerMetastatic cancerSite & severity of thrombosis may modify durationSite & severity of thrombosis may modify duration

COUNSELING ASYMPTOMATIC COUNSELING ASYMPTOMATIC HETEROZYGOUS PATIENTS FOR FVL AND/OR HETEROZYGOUS PATIENTS FOR FVL AND/OR
PGMPGM
Avoid estrogen-containing oral Avoid estrogen-containing oral contraceptives and HRT.contraceptives and HRT.
Tobacco cessation/ weight loss.Tobacco cessation/ weight loss.Anticoagulation prophylaxis for immobility.Anticoagulation prophylaxis for immobility.Extended prophylaxis post-op for major Extended prophylaxis post-op for major
surgery.surgery.Review signs & symptoms of DVT/PE.Review signs & symptoms of DVT/PE.

PHARMACEUTICAL CONTRACEPTIONPHARMACEUTICAL CONTRACEPTION
OCP containing estrogens & progestins– OCP containing estrogens & progestins– increase risk 2-4 timesincrease risk 2-4 times
Injectable progestins - increase risk 2-4 Injectable progestins - increase risk 2-4 timestimes
Progestin only oral formulations- no risk Progestin only oral formulations- no risk increaseincrease

WHICH ANITCOAGULANT SHOULD I WHICH ANITCOAGULANT SHOULD I CHOOSE?CHOOSE?

COUMADINCOUMADIN
Vitamin K antagonistVitamin K antagonist
Has all indications except pregnancy & Has all indications except pregnancy &
malignancy (2malignancy (2ndnd choice) choice)
Least expensiveLeast expensive
Has reversal agentsHas reversal agents
May use with chronic kidney diseaseMay use with chronic kidney disease

LMWHLMWH
Potentiates Antithrombin’s inhibition of FXa Potentiates Antithrombin’s inhibition of FXa 11stst choice for malignancy choice for malignancy
Can use with pregnancy- EnoxaparinCan use with pregnancy- Enoxaparin
Can use with GI impairmentCan use with GI impairment
Fondaparinux used with HITFondaparinux used with HIT
Need CRCL of > 30 mls/min.Need CRCL of > 30 mls/min.
FXa level may be helpful for patients withFXa level may be helpful for patients with
CKD, pregnancy, & obesity.CKD, pregnancy, & obesity.

DIRECT THROMBIN INHIBITORS-IV
Directly binds to thrombin
Argatroban
Treatment of Heparin induced thrombocytopenia
Dose reduce for liver dysfunction

NEWER ORAL NEWER ORAL ANTICOAGULANTSANTICOAGULANTS
Patients having difficulty with consistent Patients having difficulty with consistent
INR’sINR’s
No monitoring desirableNo monitoring desirable
Rivaroxaban has most indicationsRivaroxaban has most indications
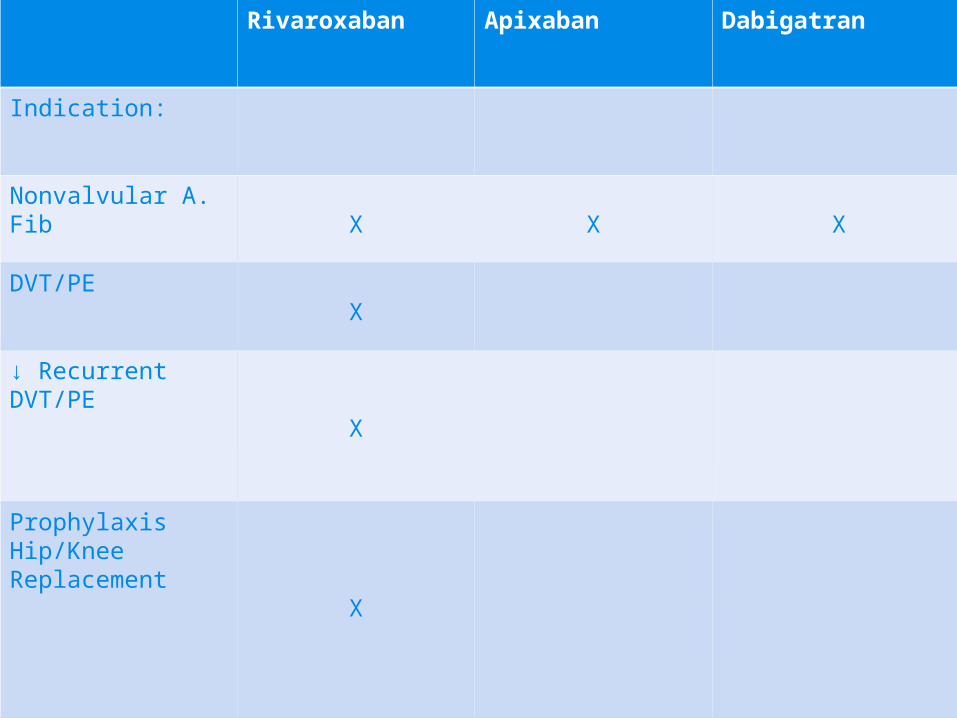
Rivaroxaban Apixaban Dabigatran
Indication:
Nonvalvular A. FibX X X
DVT/PEX
↓ Recurrent DVT/PE
X
Prophylaxis Hip/Knee Replacement
X

Apixaban Rivaroxaban Dabigatran
Mechanism Factor Xa Inhibitor Factor Xa Inhibitor Direct Thrombin Inhibitor
T1/2, hr. 12 5-9 12-17
Dosing If any 2 characteristics:Age ≥ 80BW ≤ 60kg.CR ≥ 1.5
2.5mg BID
DVT/PE/ Prophylaxis, CRCL < 30ml/min- Avoid
A. Fib, CRCL 15-50ml/min- 15mg/day
Not Dialyzable
80% Renal Excreted
CRCL > 30, 150 mg. BID
CRCL 15-30, 75 mg. BID
Dialyzable
Food With or Without With With or WithoutDyspepsia
Discontinuation for Surgery
Low Risk- 24 hrs.High Risk ≥ 48 hrs.
≥ 24 hrs. CRCL ≥ 50 1-2 days pre-op min.
CRCL < 50 3-5 days pre-op min.
Causes ↑ INR X X X

CONVERSIONSCONVERSIONS
Parenteral Anticoagulant→ Dabigatran→ Parenteral Anticoagulant→ Dabigatran→
Start when Heparin drip is discontinued.Start when Heparin drip is discontinued.
Start 0-2 hours before the next dose Start 0-2 hours before the next dose
LMWH is due.LMWH is due.
Dabigatran→ Parenteral Anticoagulant→ Dabigatran→ Parenteral Anticoagulant→
Start parenteral anticoagulant 12 hrs. Start parenteral anticoagulant 12 hrs.
(CRCL≥ mls/min) or 24 hrs. (CRCL <30(CRCL≥ mls/min) or 24 hrs. (CRCL <30
mls/min) after last dose of Dabigatran.mls/min) after last dose of Dabigatran.

CONVERSIONS CONTINUEDCONVERSIONS CONTINUED
Warfarin→ Dabigatran→ Start Dabigatran Warfarin→ Dabigatran→ Start Dabigatran
when INR <2.0when INR <2.0
Dabigatran→ Warfarin → Dabigatran→ Warfarin →
CRCL≥ 50mls/min Start Warfarin 3 days CRCL≥ 50mls/min Start Warfarin 3 days
before stopping Dabigatranbefore stopping Dabigatran
CRCL 30-50mls/min Start Warfarin 2 daysCRCL 30-50mls/min Start Warfarin 2 days
before stopping Dabigatranbefore stopping Dabigatran
CRCL 15-30mls/min Start Warfarin 1 day CRCL 15-30mls/min Start Warfarin 1 day
before stopping Dabigatranbefore stopping Dabigatran
DABIGATRANDABIGATRAN
Drug-Drug InteractionsDrug-Drug Interactions
Avoid RifampinAvoid Rifampin
With CRCL 30-50mls/min & Dronedarone orWith CRCL 30-50mls/min & Dronedarone or
Ketoconazole are co-administered, ↓ Ketoconazole are co-administered, ↓
Dabigatran to 75mg. BID. Avoid with CRCLDabigatran to 75mg. BID. Avoid with CRCL
<30mls/min<30mls/min
RIVAROXABAN & APIXABANRIVAROXABAN & APIXABAN
Drug-Drug InteractionsDrug-Drug Interactions
Itraconazole, Ketoconazole, Ritonavir, & Indiravir Itraconazole, Ketoconazole, Ritonavir, & Indiravir coadministration should be avoided- Increased coadministration should be avoided- Increased risk for hemorrhage.risk for hemorrhage.
With Apixaban, can give at dose 2.5mg BID, if not With Apixaban, can give at dose 2.5mg BID, if not already at that dose. Carbamazepine, already at that dose. Carbamazepine, Phenytoin, & Rifampin coadministration should Phenytoin, & Rifampin coadministration should be avoided- decreased efficacy.be avoided- decreased efficacy.

RIVAROXABAN & APIXABAN RIVAROXABAN & APIXABAN CONTINUEDCONTINUED
Pregnancy category C- RivaroxabanPregnancy category C- Rivaroxaban→ no → no breastfeeding data & B- Apixabanbreastfeeding data & B- Apixaban
Avoid in patients with moderate/severe hepatic Avoid in patients with moderate/severe hepatic impairmentimpairment
No known reversal agentNo known reversal agentWith Apixaban, dose ↓ 2.5mg BID if ≥ 2 With Apixaban, dose ↓ 2.5mg BID if ≥ 2
characteristics present; age ≥ 80, weight ≤ 60 Kg characteristics present; age ≥ 80, weight ≤ 60 Kg or Creatinine ≥ 1.5. No data for CRCL < 15 or Creatinine ≥ 1.5. No data for CRCL < 15
mls/ minmls/ min

SWITCHING TO & FROM RIVAROXABAN SWITCHING TO & FROM RIVAROXABAN OR APIXABAN AND OTHER OR APIXABAN AND OTHER
ANTICOAGULANTSANTICOAGULANTSWarfarinWarfarin→ start when INR < 3.0 → start when INR < 3.0
(Rivaroxaban), < 2.0 (Apixaban)(Rivaroxaban), < 2.0 (Apixaban)Other anticoagulants→ stop Heparin drip & Other anticoagulants→ stop Heparin drip &
start at same timestart at same timeRivaroxaban→ substitute new drug at time Rivaroxaban→ substitute new drug at time
of next scheduled dose. If Warfarin, start of next scheduled dose. If Warfarin, start parenteral anticoagulant & Warfarin at parenteral anticoagulant & Warfarin at time of next scheduled dose.time of next scheduled dose.
Apixaban→ Same as RivaroxabanApixaban→ Same as Rivaroxaban

RIVAROXABAN USE FOR RIVAROXABAN USE FOR INITIAL DVT/PE TREATMENT:INITIAL DVT/PE TREATMENT:
Who should Who should NOTNOT get it? get it?
Active MalignancyActive Malignancy
Pregnancy/BreastfeedingPregnancy/Breastfeeding
Massive PE or DVT if thrombolysis is plannedMassive PE or DVT if thrombolysis is planned
Weight > 250lbs. Or < 110lbs.Weight > 250lbs. Or < 110lbs.
Severe renal or hepatic dysfunctionSevere renal or hepatic dysfunction
Contraindicated or caution advised with Contraindicated or caution advised with coadministration of certain drugscoadministration of certain drugs

DVT/PE IN CANCER PATIENTSDVT/PE IN CANCER PATIENTS
RISK FACTORS:RISK FACTORS:Advanced stageAdvanced stageMajor surgical resectionMajor surgical resectionCentral venous access devicesCentral venous access devicesChemotherapyChemotherapyAntiangiogenic agentsAntiangiogenic agentsHormonesHormonesESAESA

MOST COMMON PRIMARY SITESMOST COMMON PRIMARY SITES
PancreaticPancreatic
LungLung
BrainBrain
GynecologicGynecologic
StomachStomach

DVT/PE TREATMENT GUIDELINES FOR DVT/PE TREATMENT GUIDELINES FOR CANCER PATIENTSCANCER PATIENTS
LMWH-1LMWH-1stst choice choiceCoumadin-2Coumadin-2ndnd choice choiceOral Factor Oral Factor Xa Inhibitors-Limited data cancer Xa Inhibitors-Limited data cancer
patientspatientsCan stop treatment after 6 months if patient in Can stop treatment after 6 months if patient in
remission and off treatment.remission and off treatment.With metastatic disease, continue anticoagulation With metastatic disease, continue anticoagulation
indefinitely.indefinitely.Incidental DVT/PE noted on staging/restaging Incidental DVT/PE noted on staging/restaging
scans should be treated aggressively.scans should be treated aggressively.

MANAGEMENT OF RECURRENT MANAGEMENT OF RECURRENT DVT/PE IN CANCER PATIENTSDVT/PE IN CANCER PATIENTS
9% of patients treated with LMWH & ~ 20% 9% of patients treated with LMWH & ~ 20% treated with therapeutic Warfarin develop treated with therapeutic Warfarin develop recurrent DVT/PE.recurrent DVT/PE.
Treatment- Switch Warfarin to full dose Treatment- Switch Warfarin to full dose LMWH.LMWH.
-Already on LMWH, increase dose by 20--Already on LMWH, increase dose by 20-
25%. Check Anti-Xa level 4 hours post 25%. Check Anti-Xa level 4 hours post
injection.injection.

INDICATIONS FOR DVT/PE INDICATIONS FOR DVT/PE PROPHYLAXIS IN CANCER PATIENTSPROPHYLAXIS IN CANCER PATIENTS
Hospitalized with immobility/ acute illnessHospitalized with immobility/ acute illness -Heparin SQ/ LMWH.-Heparin SQ/ LMWH.Major surgery-abdominal or pelvic Major surgery-abdominal or pelvic -Ideally, pre-op Enoxaparin and -Ideally, pre-op Enoxaparin and sequential TEDs. Continue sequential TEDs. Continue pharmacologic treatment 7-10 days pharmacologic treatment 7-10 days minimum. Up to 4 weeks in high risk minimum. Up to 4 weeks in high risk patients.patients.

INDICATIONS FOR IVC FILTERINDICATIONS FOR IVC FILTER
Contraindication to anticoagulation.Contraindication to anticoagulation.
Recurrent DVT/PE or extension of existing Recurrent DVT/PE or extension of existing thrombus despite optimal treatment.thrombus despite optimal treatment.
Patient non-compliance.Patient non-compliance.

REVERSAL OF REVERSAL OF ANTITHROMBOTICSANTITHROMBOTICS
Heparin: Protamine 1mg/ 100 units Heparin- Heparin: Protamine 1mg/ 100 units Heparin-
Max dose 50mg/ 10 minutes.Max dose 50mg/ 10 minutes.
Enoxaparin: Protamine will partially reverseEnoxaparin: Protamine will partially reverse
Fondaparinux: ? Factor VIIa- 90mcg/kg, Fondaparinux: ? Factor VIIa- 90mcg/kg,
prothrombin concentrate 50 units/kg. prothrombin concentrate 50 units/kg.
Dabigatran: HemodialysisDabigatran: Hemodialysis
Rivaroxaban & Apixaban ?Rivaroxaban & Apixaban ?

VITAMIN K PROTEIN VITAMIN K PROTEIN CONCENTRATECONCENTRATE
Dosing: IU requested= Dosing: IU requested= weight (Kg) x target factor level (~70%) – current weight (Kg) x target factor level (~70%) – current
levellevel INR 2-3: 20% factor levelINR 2-3: 20% factor level INR 3-4: 10% factor levelINR 3-4: 10% factor level
Boulis et al. Neurosurgery 45: 1113, 1999Boulis et al. Neurosurgery 45: 1113, 1999

PERIOPERATIVE MANAGEMENT PERIOPERATIVE MANAGEMENT ON CHRONIC WARFARINON CHRONIC WARFARIN
Indication for Warfarin and the procedure willIndication for Warfarin and the procedure will
dictate plan.dictate plan.
Low risk procedures:Low risk procedures:
cataract, minor dental, & minor skincataract, minor dental, & minor skin
continue Warfarin or stop 2-3 days. Can continue Warfarin or stop 2-3 days. Can
add Epsilon aminocaproic Acidadd Epsilon aminocaproic Acid
Moderate to high risk procedures:Moderate to high risk procedures:
Low risk for thromboembolism: Stop Coumadin forLow risk for thromboembolism: Stop Coumadin for
5 days.5 days.
Moderate to high risk: Heparin or LMWH bridgeModerate to high risk: Heparin or LMWH bridge
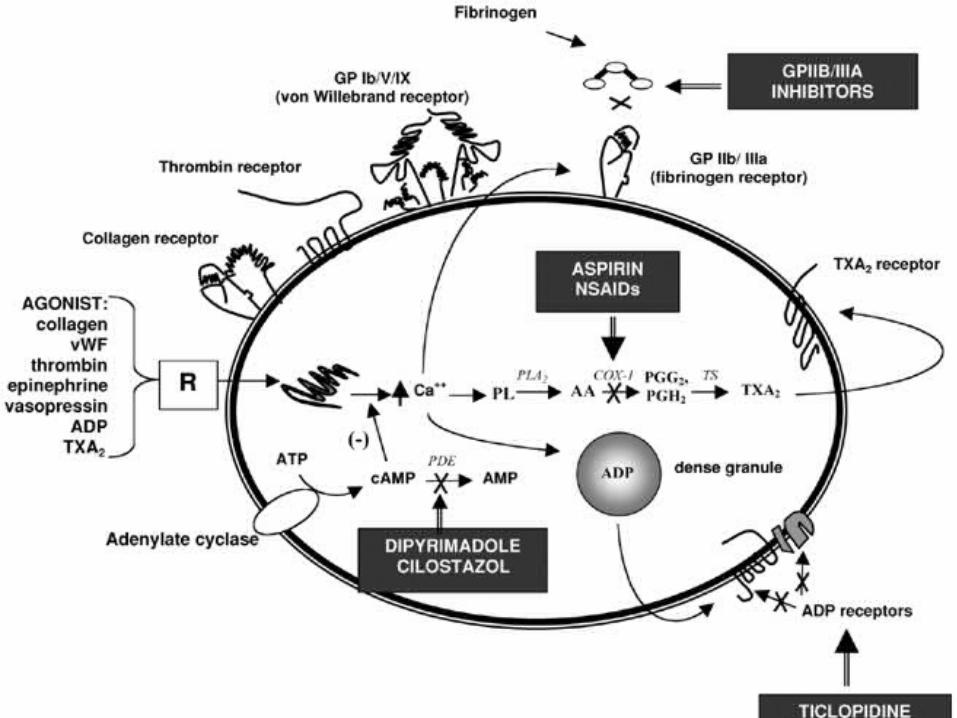

PLATELET FUNCTION
Adhesion- Platelet glycoprotein (GPlb) receptor interaction with vWf--platelet-vessel wall interaction
Aggregation- Platelet GPIIb-IIIa receptor interaction with Fibrinogen--platelet-platelet interaction
Secretion- Platelets release granule contents
PLATELET FUNCTION CONTINUED
Platelet receptor activation by ADP, thrombin, & collagen mediate aggregation and secretion
Provides membrane surface for activation of thrombin.

ECCHYMOSIS DdxECCHYMOSIS Ddx
Thrombocytopenia: ITP, bone marrowThrombocytopenia: ITP, bone marrow
disorders, drugs, CTDdisorders, drugs, CTD
Platelet dysfunction: NSAIDS, alcohol,Platelet dysfunction: NSAIDS, alcohol,
P2Y12 inhibitors, OTC’s, & HerbalsP2Y12 inhibitors, OTC’s, & Herbals
SSRI anti-depressants particularly when SSRI anti-depressants particularly when combined with other anti-platelet agentscombined with other anti-platelet agents
DTI, Factor Xa inhibitors, Warfarin DTI, Factor Xa inhibitors, Warfarin
Vitamin K Deficiency (no Coumadin): Poor Vitamin K Deficiency (no Coumadin): Poor
diet +/- antibioticsdiet +/- antibiotics

ECCHYMOSIS Ddx ECCHYMOSIS Ddx CONTINUEDCONTINUED
SteroidsSteroids
Senile PurpuraSenile Purpura
CKD, liver disease, paraproteinemiaCKD, liver disease, paraproteinemia
Congenital: von Willebrand disease (vWd), Congenital: von Willebrand disease (vWd),
Hemophilia, Rare platelet function Hemophilia, Rare platelet function
disordersdisorders

WARNING SIGNSWARNING SIGNS
Positive family history, prior hemorrhage Positive family history, prior hemorrhage
with trauma, surgery, or procedures.with trauma, surgery, or procedures.
Multiple sites of hemorrhage- hematomas,Multiple sites of hemorrhage- hematomas,
menses, epistaxismenses, epistaxis

WORK UPWORK UP
If minor hemorrhage, stop offending If minor hemorrhage, stop offending
medications for 10 days and reassess.medications for 10 days and reassess.
Persistent hemorrhage +/- positive familyPersistent hemorrhage +/- positive family
history- check CBC, INR, PTT, & Platelet history- check CBC, INR, PTT, & Platelet
closure time.closure time.

PRE-OPERATIVE PRE-OPERATIVE CLEARANCECLEARANCE
Isolated elevated PTT: Check F8, 9, 11, & DRVVTIsolated elevated PTT: Check F8, 9, 11, & DRVVT
Isolated elevated PT/INR: Check F7, fibrinogen, &Isolated elevated PT/INR: Check F7, fibrinogen, &
HFP. In the correct setting, can give Vitamin K HFP. In the correct setting, can give Vitamin K
trial first. trial first.
Isolated thrombocytopenia: Stop offending agents,Isolated thrombocytopenia: Stop offending agents,
Check B12, folate, ANA.Check B12, folate, ANA.
Abnormal platelet closure time: If on offending Abnormal platelet closure time: If on offending
agents, stop 10 days & repeat. No meds &/or agents, stop 10 days & repeat. No meds &/or
positive family history- check vWd panel.positive family history- check vWd panel.

CLOPIDOGREL (FDA 1997)CLOPIDOGREL (FDA 1997)
P2Y12 Platelet inhibitor (Thienopyridines)P2Y12 Platelet inhibitor (Thienopyridines)
Irreversible bindingIrreversible binding
ProdrugProdrug→CYP2C19→active metabolite→CYP2C19→active metabolite
Poor metabolizers have worse outcomesPoor metabolizers have worse outcomes
Can check CYP2C19 genotypeCan check CYP2C19 genotype
Avoid Omeprazole & Esomeprazole (CYP2C19 Avoid Omeprazole & Esomeprazole (CYP2C19 inhibitors). Can use Dexlansoprazole, inhibitors). Can use Dexlansoprazole, Lansoprazole, & Pantoprazole instead→ have Lansoprazole, & Pantoprazole instead→ have less effectless effect

CLOPIDOGREL (FDA 1997) CLOPIDOGREL (FDA 1997) CONTINUEDCONTINUED
TTP after < 2 weeks exposure. Agranulocytosis/Pancytopenia
Pregnancy B, No breastfeeding
No dose adjustment for elderly or hepatically impaired.
Reverse with platelets.

PRASUGREL (FDA 2009)PRASUGREL (FDA 2009)
P2Y12 ADP receptor irreversible inhibitor ofP2Y12 ADP receptor irreversible inhibitor of
platelet activation & aggregationplatelet activation & aggregation
ASA dose 81-325mg./ DayASA dose 81-325mg./ Day
Contraindications→ weight < 60, Prior TIA Contraindications→ weight < 60, Prior TIA oror
stroke- ↑ rate of stroke on Prasugrel stroke- ↑ rate of stroke on Prasugrel
unless patients ≥ 75 with history of unless patients ≥ 75 with history of
diabetes or prior MI diabetes or prior MI

PRASUGREL (FDA 2009) PRASUGREL (FDA 2009) CONTINUEDCONTINUED
TTP has been reported- can occur withTTP has been reported- can occur with
exposure < 2 weeks.exposure < 2 weeks.
Can give with mild to moderate hepatic Can give with mild to moderate hepatic
impairment.impairment.
Can give with H2blockers & proton pump Can give with H2blockers & proton pump
inhibitors.inhibitors.
No drug-drug interactions.No drug-drug interactions.

TICAGRELOR (FDA 2011)TICAGRELOR (FDA 2011)
P2Y12 reversible platelet inhibitor P2Y12 reversible platelet inhibitor
ASA dose 81 mg./ DayASA dose 81 mg./ Day
DyspneaDyspnea
No contraindication based on ageNo contraindication based on age
Contraindicated→ History intracranial Contraindicated→ History intracranial
hemorrhage, & severe hepatic impairment.hemorrhage, & severe hepatic impairment.
Renal impairment→ No dose adjustmentRenal impairment→ No dose adjustment
Discontinue 5 days pre-op.Discontinue 5 days pre-op.
TICAGRELOR (FDA 2011) TICAGRELOR (FDA 2011) CONTINUEDCONTINUED
Drug-Drug InteractionDrug-Drug Interaction
Avoid use with strong CYP3A inhibitors-Avoid use with strong CYP3A inhibitors-
Azole Antifungals, clarithromycin, &Azole Antifungals, clarithromycin, &
Anti-Retrovirals.Anti-Retrovirals.
Avoid use with Potent CYP3A Inducers-Avoid use with Potent CYP3A Inducers-
Rifampin, Dexamethasone, Phenytoin, Rifampin, Dexamethasone, Phenytoin,
Carbamazepine, & Phenobarbital.Carbamazepine, & Phenobarbital.
REVERSAL OF REVERSAL OF ANTIPLATELET AGENTSANTIPLATELET AGENTS
Aspirin & Clopidogrel: CAD patients-Aspirin & Clopidogrel: CAD patients-
transfuse platelets. Can try DDAVP for transfuse platelets. Can try DDAVP for
other patients.other patients.
Prasugrel: Transfuse plateletsPrasugrel: Transfuse platelets
Ticagrelor: T1/2= 8hrs., supportive care, noTicagrelor: T1/2= 8hrs., supportive care, no
data for platelet transfusionsdata for platelet transfusions
PERIOPERATIVE MANAGEMENT OF PERIOPERATIVE MANAGEMENT OF ANTIPLATELET AGENTSANTIPLATELET AGENTS
Low Risk Procedure: Continue medicationsLow Risk Procedure: Continue medications
Moderate to High Risk: Moderate to High Risk:
History of CABG- History of CABG-
continue ASA, stop Clopidogrelcontinue ASA, stop Clopidogrel
Drug eluting stent-Drug eluting stent-
need ASA & Clopidogrel 12 monthsneed ASA & Clopidogrel 12 months
If withholding agents, need at least 7-10 If withholding agents, need at least 7-10
days to clear.days to clear.

AMERICAN SOCIETY OF HEMATOLOGY 2014
Anfibatide
Purified protein from snake venom.
Intravenous glycoprotein lb antagonist.
Phase l dose-finding study- 94 participants.
The inhibitory effect was undetectable 4 hours post treatment.

AMERICAN SOCIETY OF HEMATOLOGY 2014
Anfibatide
No significant change in bleeding time, PTT, INR, or platelet count noted.
No serious adverse events or deaths noted.
Phase II trial planned in NSTEMI patients receiving angioplasty.
Hou Y. Abstract # 577

PRIMARY VS SECONDARY PRIMARY VS SECONDARY POLYCYTHEMIAPOLYCYTHEMIA
Primary:Primary:
No obvious etiologyNo obvious etiology→ EPO level, JAK-2→ EPO level, JAK-2
→ → If EPO low & JAK-2 negative→ EXON-12If EPO low & JAK-2 negative→ EXON-12
deletiondeletion
PRIMARY VS SECONDARY PRIMARY VS SECONDARY POLYCYTHEMIAPOLYCYTHEMIA
Secondary Etiologies:Secondary Etiologies:TobaccoTobaccoOSAOSACardiopulmonary disorders Cardiopulmonary disorders Volume depletionVolume depletionRenal/liver malignancyRenal/liver malignancyCerebellar HemangioblastomaCerebellar HemangioblastomaPolycystic Kidney DiseasePolycystic Kidney DiseaseFamilialFamilial

MICROCYTIC ANEMIAMICROCYTIC ANEMIA
Iron deficiencyIron deficiencyCongenital Sideroblastic Anemia-B6Congenital Sideroblastic Anemia-B6Acquired Sideroblastic AnemiaAcquired Sideroblastic Anemia→ lead poisoning, Isoniazid, → lead poisoning, Isoniazid,
copper deficiency- bariatric surgery patientscopper deficiency- bariatric surgery patientsHemoglobinopathiesHemoglobinopathies --Alpha Thal Minor-Normal Hemoglobin ElectrophoresisAlpha Thal Minor-Normal Hemoglobin Electrophoresis -ß Thal Minor-Increase hemoglobin A2 & F-ß Thal Minor-Increase hemoglobin A2 & F -Hemoglobin C-Trait, Hemoglobin E-Hemoglobin C-Trait, Hemoglobin EAnemia of Chronic diseaseAnemia of Chronic diseaseRA often MCV-78 if not on Methotrexate and/or ImuranRA often MCV-78 if not on Methotrexate and/or Imuran

POST SPLENECTOMY/ FUNTIONAL POST SPLENECTOMY/ FUNTIONAL ASPLENIA SEPSIS PREVENTIONASPLENIA SEPSIS PREVENTION
Early antibiotics to cover encapsulated organisms-Early antibiotics to cover encapsulated organisms-Streptococcus pneumoniae, & Haemophilus Streptococcus pneumoniae, & Haemophilus Influenzae (H. flu)Influenzae (H. flu)
VaccinationVaccination -Pneumovax every 6 years-Pneumovax every 6 years -H. flu times one-H. flu times one -Meningococcal ? Every 5 years-Meningococcal ? Every 5 years -Influenza yearly-Influenza yearlyTobacco CessationTobacco Cessation

POLYCLONAL VS MONOCLONAL POLYCLONAL VS MONOCLONAL GAMMOPATHYGAMMOPATHY
Polyclonal-Ddx.Polyclonal-Ddx.
InfectionInfection
HIVHIV
Connective Tissue DiseaseConnective Tissue Disease
Liver DiseaseLiver Disease
SarcoidosisSarcoidosis

POLYCLONAL VS MONOCLONAL POLYCLONAL VS MONOCLONAL GAMMOPATHYGAMMOPATHY
Monoclonal Gammopathy-Ddx.Monoclonal Gammopathy-Ddx.
MGUSMGUSPlasmacytomaPlasmacytomaSmoldering Multiple MyelomaSmoldering Multiple MyelomaMultiple MyelomaMultiple MyelomaAmyloidosisAmyloidosisNon-Hodgkin's LymphomaNon-Hodgkin's Lymphoma
MGUSMGUS
3% of general population >503% of general population >50Associations-osteoporosis, peripheral neuropathy, Associations-osteoporosis, peripheral neuropathy,
& venous thrombosis& venous thrombosisHigh risk for MGUS-African Americans 2-3x High risk for MGUS-African Americans 2-3x
compared to whites, males, positive family compared to whites, males, positive family history, & immunosuppressionhistory, & immunosuppression
High risk for MGUS progression-positive serum High risk for MGUS progression-positive serum free light chain, IgA or IgM, & monoclonal protein free light chain, IgA or IgM, & monoclonal protein ≥≥
1.5g/dl1.5g/dl

CONCLUSIONS
Weight loss, tobacco cessation, exercise, appropriate DVT/PE prophylaxis, & age-appropriate cancer screening will prevent DVT/PE in most patients.
Proper management of prescription & OTC medications along with patient counseling can significantly reduce life-threatening hemorrhage.

CONCLUSIONS CONTINUED
The history & physical exam along with application of the coagulation cascade and normal platelet function will focus your differential diagnosis & work up of lab abnormalities & their treatments.







