

Carsten Tschöpe
Kardiologie, Campus Benjamin Franklin
Inflammation in heart failure:
Focus on fibroblasts
Berlin

nach Owan T et al. N Engl J Med 2006;
Prognosis and heart failure
HFREF
HFREF(Heart failure with reduced ejection fraction)
Deswal et al. Circulation 2001

Inflammation is a negative predictorin inflammatory cardiomyopathy
Kindermann et al. Circulation 2008
Basal
6 Monatsverlauf

nach Owan T et al. N Engl J Med 2006;
Prognosis and heart failure
HFREF HFPEF
HFPEF HFREF(Heart failure with reduced ejection fraction) (Heart failure with preserved ejection fraction)

Volume
Pres
sure
Mitral valveopen
Mitral Valveocclusion
Filling
Aortic Valveocclusion Ejection
Aortic valveopen
ContractionR
elax
atio
n
Cardiac Working Diagram(Pressure-Volume Relationship)

Volume
Pres
sure
Diastolic
Systolic
Cardiac Working Diagram(Pressure-Volume Relationship)
LVEDPTau
Dp/
dt m
in

Conductance Catheter
LV pressure and volume measurement

All signals

V. Cava Occlusion for transient preload reductionto evaluate end-diastolic pressure-volume
relationship(LV stiffness)
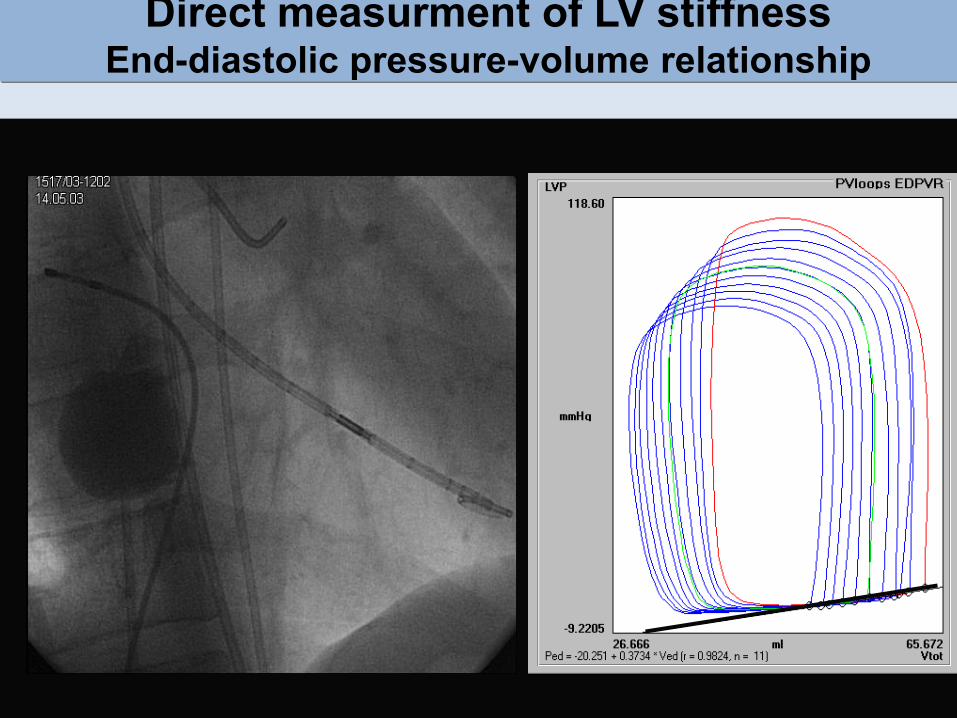
Direct measurment of LV stiffnessEnd-diastolic pressure-volume relationship

control HFNEF0.00
0.01
0.02
0.03
0.04st
iffne
ss c
onst
ant
*n =70/ Gruppe, *P<0.05Control HFPEF Control HFPEF
EF*
0
20
40
60
80
%
LV Stiffness
Conductance catheter(Pressure-Volume-Curves)
Hemodynamic characterisation of HFPEF
Kasner et al, Circulation 2007 Westermann et al, Circulation 2008
Aufzeichnungvon Druck-Volumen Schleifen
LVEDPSteifigkeit

LV Stiffness:Mechanismens
Matrix
C. Tschöpe

HFPEFKontrolle
LV Stiffness and collagen index in HFPEF
Kasner et al, JACC 2011 Westermann et al, Circulation 2008
.
p=0.001
Siriu
s re
d, C
VF (
%)
0
10
20
30
Col
lage
n C
ross
-Lin
king
p=0.007
0,0
1,0
2,0
3,0
4,0
HFPEFKontrolle HFPEFKontrolle
Kontrolle HFPEF0
5
10
15
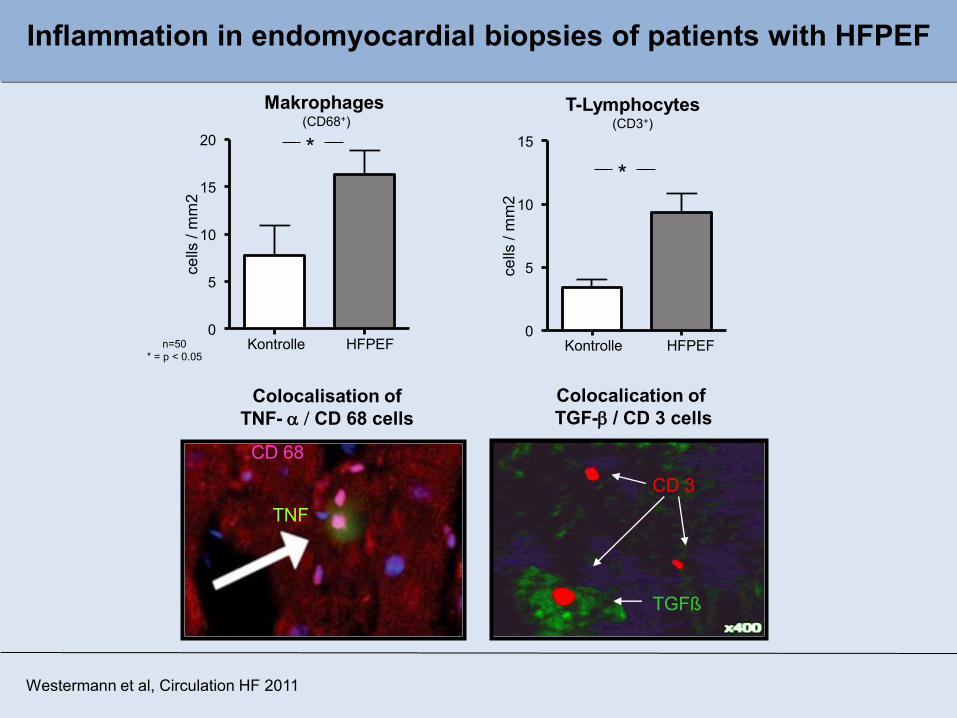
cells
/ m
m2
Makrophages(CD68+)
Kontrolle HFPEF0
5
10
15
20
cells
/ m
m2
*
T-Lymphocytes(CD3+)
*
CD 3
TGFß
Colocalisation ofTNF- a / CD 68 cells
Colocalication ofTGF-b / CD 3 cells
TNF
CD 68
Inflammation in endomyocardial biopsies of patients with HFPEF
Westermann et al, Circulation HF 2011
n=50* = p < 0.05

Correlation: Matrix - inflammation?
Primary human fibroblast cell culture
7 days 14 days
P4HB+Vimentin +Desmin –CD 31-a SMA-
Des
min
Vim
entin
P4H
BC
D31
α-SM
A
Linder et al, Biochem Res Int 2012

Role of growth Factor-b (TGF- b)
*
n=8* p < 0.05
HFPEF – TGF-ß
HFPEF + TGF-ß*
*
Myofibroblast Kollagen IConnective Tissue growth factor
Westermann et al, Circulation HF 2011
In vitro Fibroblastafter TGF-b Stimulation (alpha-SMA)
- TGF-ß + 5ng/ml TGF-ß, 24h + 5ng/ml TGF-ß, 72h
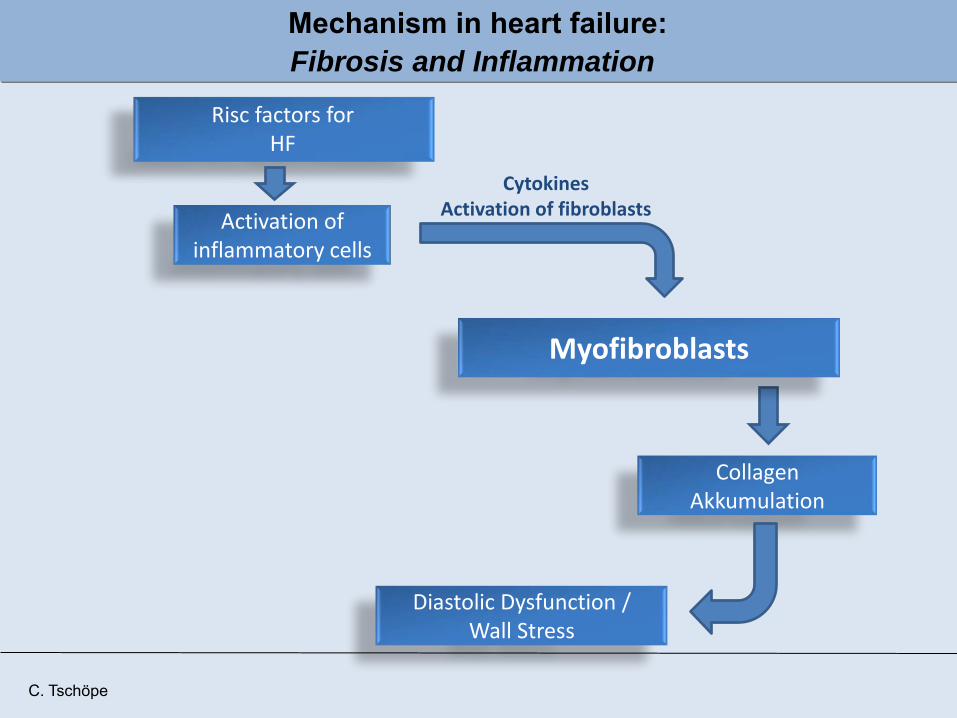
Risc factors forHF
Activation of inflammatory cells
CytokinesActivation of fibroblasts
Myofibroblasts
Collagen Akkumulation
Diastolic Dysfunction /Wall Stress
C. Tschöpe
Mechanism in heart failure:Fibrosis and Inflammation

Mechanic stress activates myofibroblasts
0% 2.5% 7.5% 10%
Strech intensity
Production of collagen
Westermann et al, Circulation HF 2011

Mechanic stress induces chemokine production
2.5% 5% 7.5% 10%
0.0
0.5
1.0
1.5
2.0
2.5
3.0
ns
** ***
flexercell stretch, frequency 1 Hz
MC
P-1
m-R
NA
expr
essi
on le
vel
(x-fo
ld o
ver u
nstre
tche
d co
ntro
l)
2.5% 5% 7.5% 10% 12.5%
0.0
0.5
1.0
1.5
2.0
2.5
3.0
*
****
ns
flexercell stretch, frequency 1 HzM
CP-
3 m
-RN
A ex
pres
sion
leve
l(x
-fold
ove
r uns
tretc
hed
cont
rol)
Westermann et al 2012
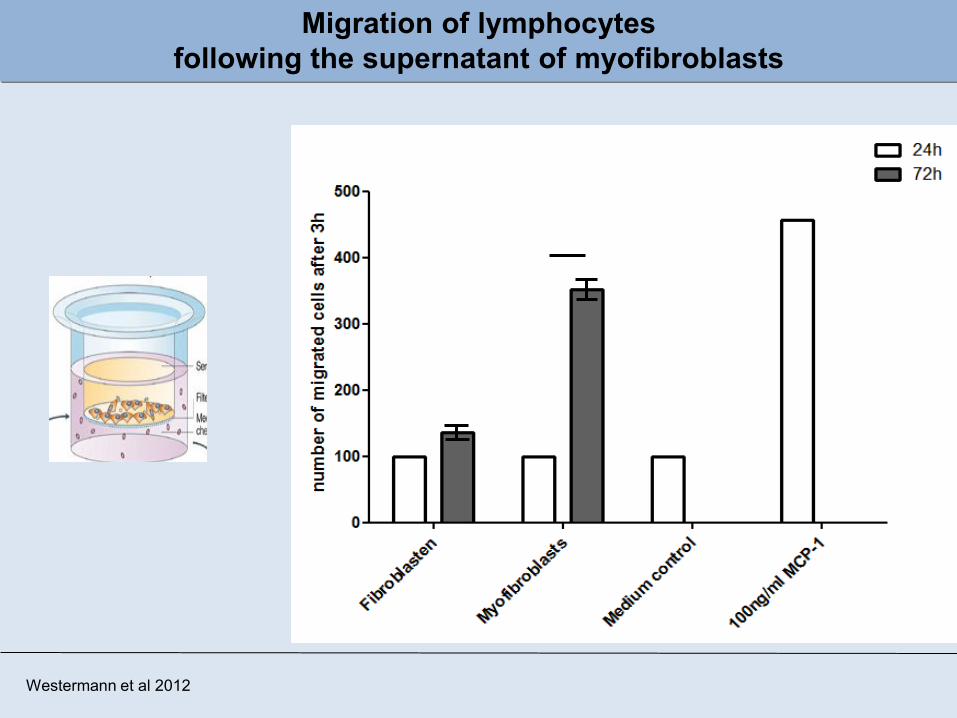
Migration of lymphocytes following the supernatant of myofibroblasts
Westermann et al 2012

Increased actin polymerization of PBMCs as a sign of increased cell mobility after incubation with the supernatant of myofibroblasts
Incubated with medium
Supernatant of fibroblasts
Supernatant of myofibroblasts
Ph
allo
ido
n-F
ITC
vo
n h
um
ane
n L
ymp
ho
zyte
n
unpublished
* *
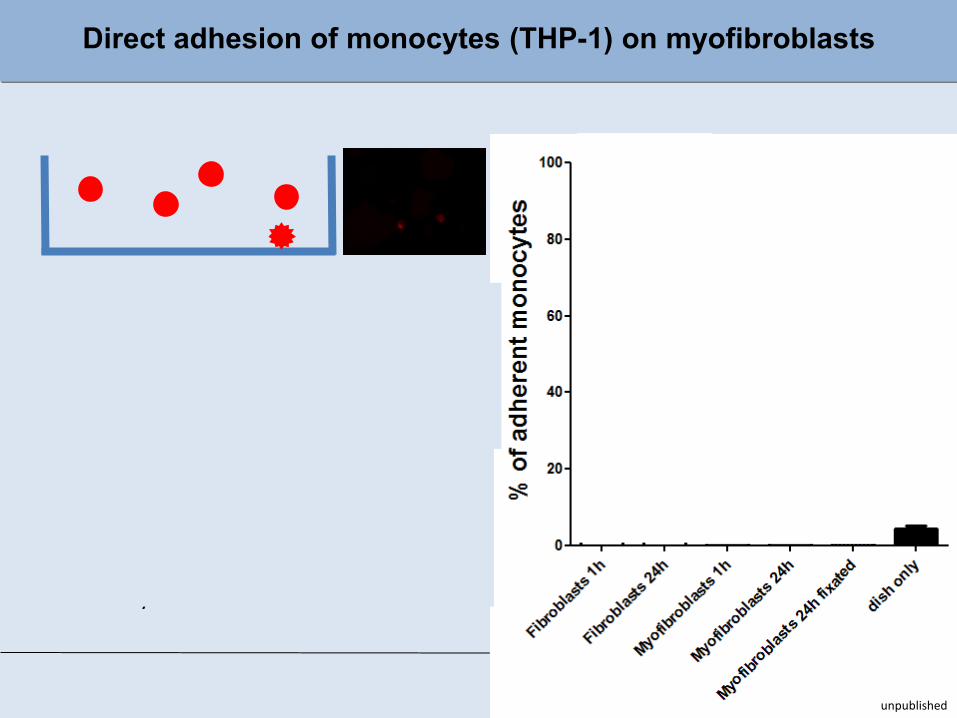
Direct adhesion of monocytes (THP-1) on myofibroblasts
Fibroblasts
Myofibroblasts
unpublished

Monocytes (Th1-Zellen) produce MMP-9 after treatement with the supernatant of myofibroblasts

α-SMA P4HB DAPI
MCP2-mRNA
*
control HFNEF0.000
0.005
0.010
0.015
0.020
gene
exp
ress
ion
MMP-2-mRNA
*
control HFNEF0.00
0.02
0.04
0.06
0.08
0.10
gene
exp
ress
ion
Identification of myofibroblasts in humanen cardiac biopsies
Control DHF
Controll DHF
Myofibroblasts
Migration and Chemotaxis
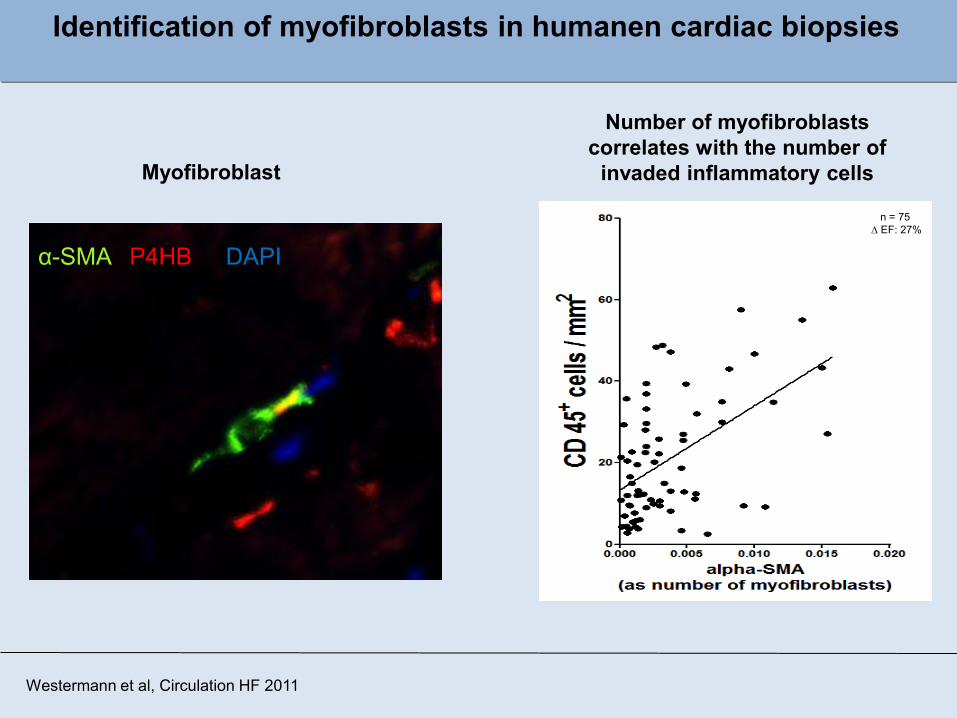
α-SMA P4HB DAPI
Myofibroblast
Number of myofibroblastscorrelates with the number of
invaded inflammatory cells
Westermann et al, Circulation HF 2011
n = 75D EF: 27%
Identification of myofibroblasts in humanen cardiac biopsies

Riskfactors for HF
Activation of inflammatory cells
Myofibroblasts
FibrosisChemokines
Diastolic Dysfunction /Wall Stress
ChemotaxisDegradationAdhesion
C. Tschöpe
CytokinseActivation of Fibroblasts
Fibrosis and Inflammation as a Circulus vitiosus
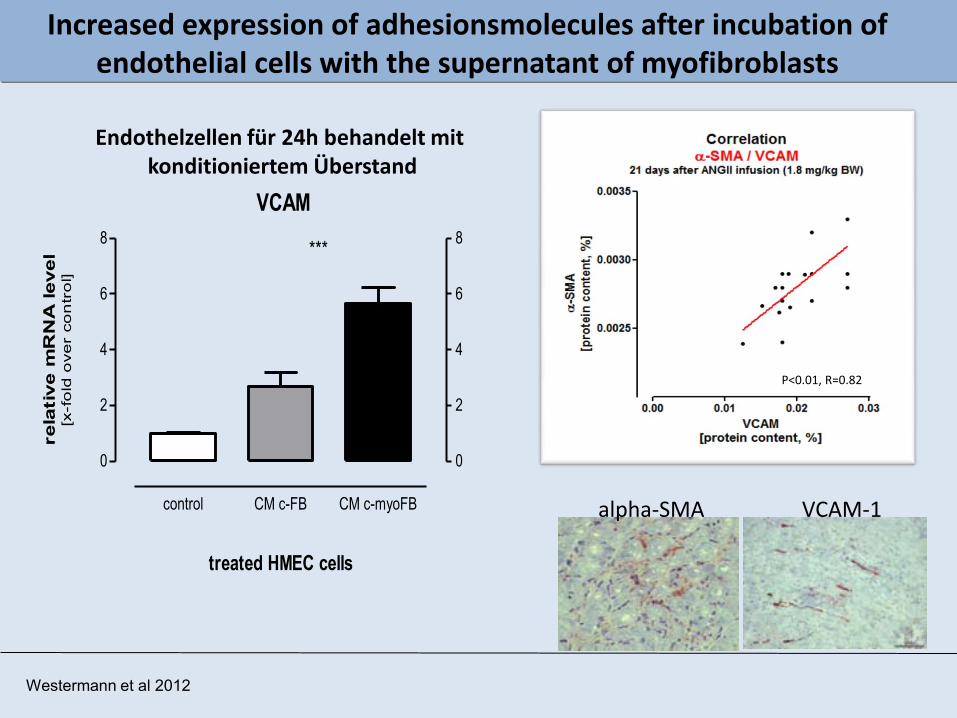
Increased expression of adhesionsmolecules after incubation of endothelial cells with the supernatant of myofibroblasts
VCAM
control CM c-FB CM c-myoFB
0
2
4
6
8
0
2
4
6
8***
treated HMEC cells
rela
tive m
RN
A level
[x-f
old
ove
r co
ntr
ol]
P<0.01, R=0.82
VCAM-1alpha-SMA
Endothelzellen für 24h behandelt mit konditioniertem Überstand
Westermann et al 2012

Endothelial dysfunction in vitro after stimulation with the supernatant of myofibroblasts
2.5%
2.5%
* vs. co
Westermann et al 2013

C. Tschöpe
Riscfactors for HF
Cardiac DysfunctionWall Stress
Activation ofinflammatory cells
Myofibroblasts
FibrosisChemokine
ChemotaxisDegradation
Adhesion
CytokinesActivated fibroblasts
Endothelial Activation
Myofibroblast and vascular in heart failure

LV Stiffness:Mechanisms
Matrix
Endothelium
Basal Ergonovine
C. Tschöpe
Myocyt

Titin function and inflammatory Stress
Paulus & Tschöpe JACC 2013
*
*
Myofibroblasts
TitinPhosphorylation
N =6 / group; *P<0,05
*
*
Becher et al, BRC in press
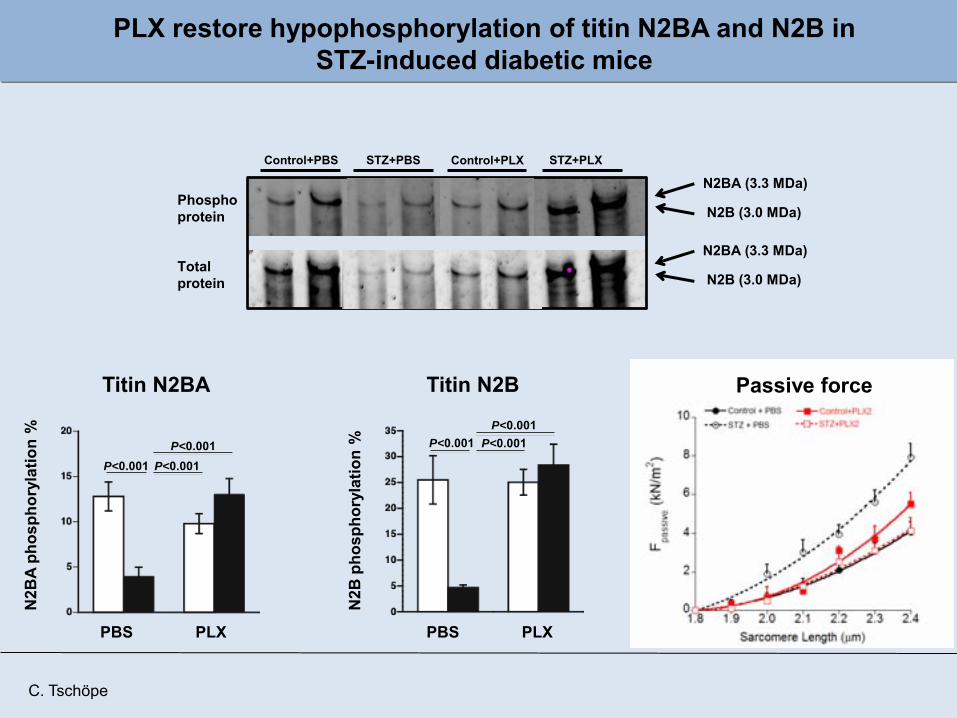
PLX restore hypophosphorylation of titin N2BA and N2B in STZ-induced diabetic mice
N2B
A ph
osph
oryl
atio
n%
PBS PLX
P<0.001P<0.001
P<0.001
Titin N2BAN
2B p
hosp
hory
latio
n%
PBS PLX
P<0.001P<0.001
P<0.001
Titin N2B
N2BA (3.3 MDa)
N2B (3.0 MDa)
N2BA (3.3 MDa)
N2B (3.0 MDa)
Control+PBS Control+PLXSTZ+PBS STZ+PLX
Phosphoprotein
Total protein
Passive force
C. Tschöpe
C. Tschöpe
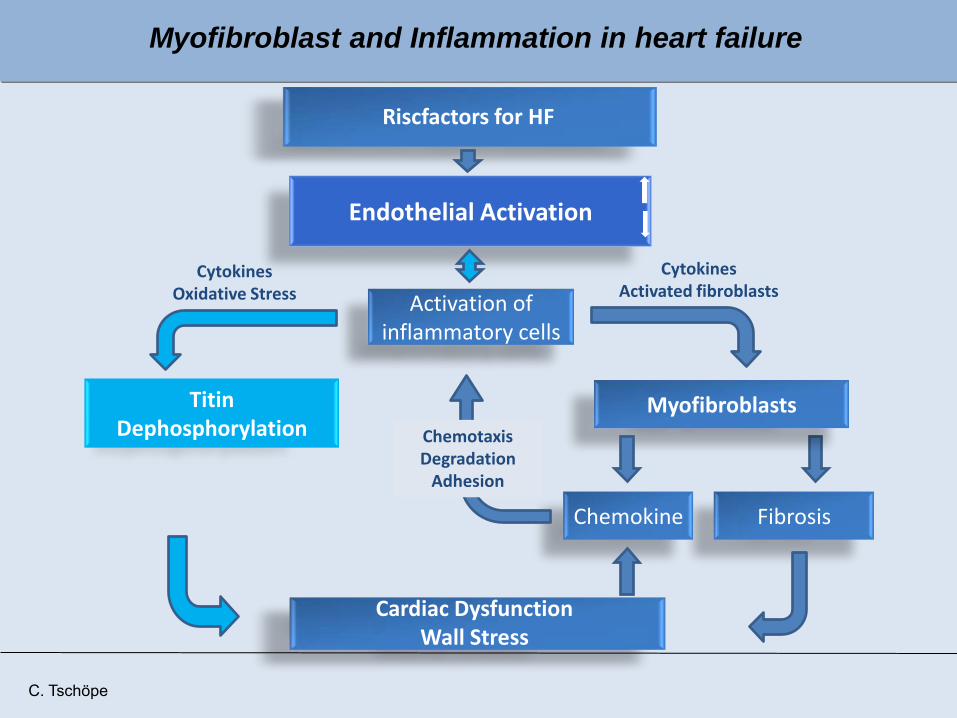
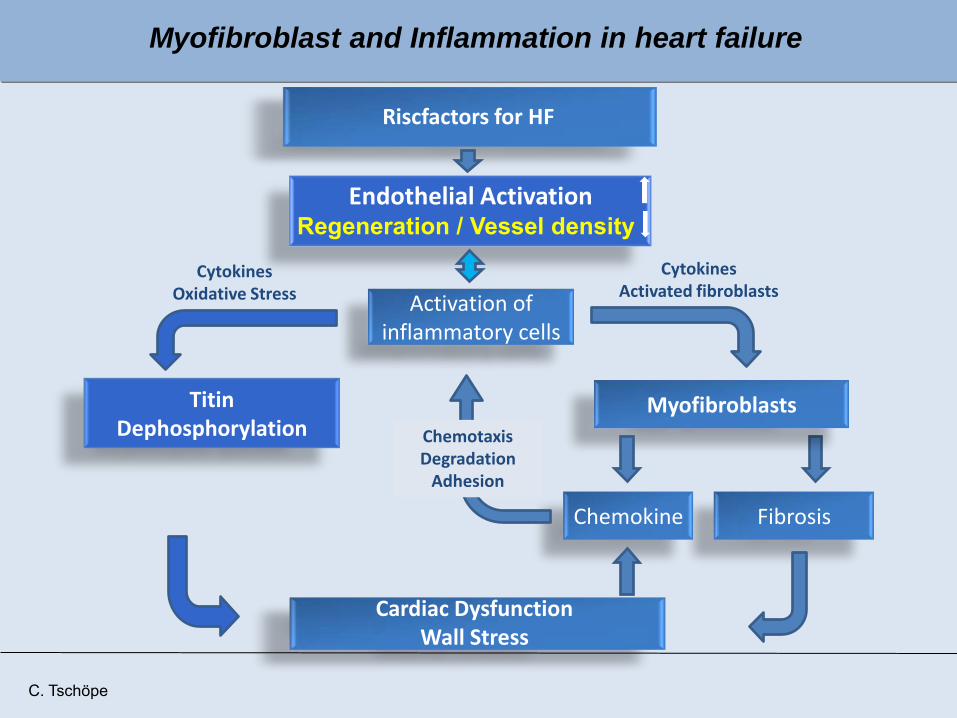
Riscfactors for HF
Cardiac DysfunctionWall Stress
Activation ofinflammatory cells
Myofibroblasts
FibrosisChemokine
ChemotaxisDegradation
Adhesion
CytokinesOxidative Stress
TitinDephosphorylation
CytokinesActivated fibroblasts
Endothelial Activation
Myofibroblast and Inflammation in heart failure

nach Owan T et al. N Engl J Med 2006;
Prognosis and heart failure
HFPEF
HFPEF (Heart failure with preserved ejection fraction)
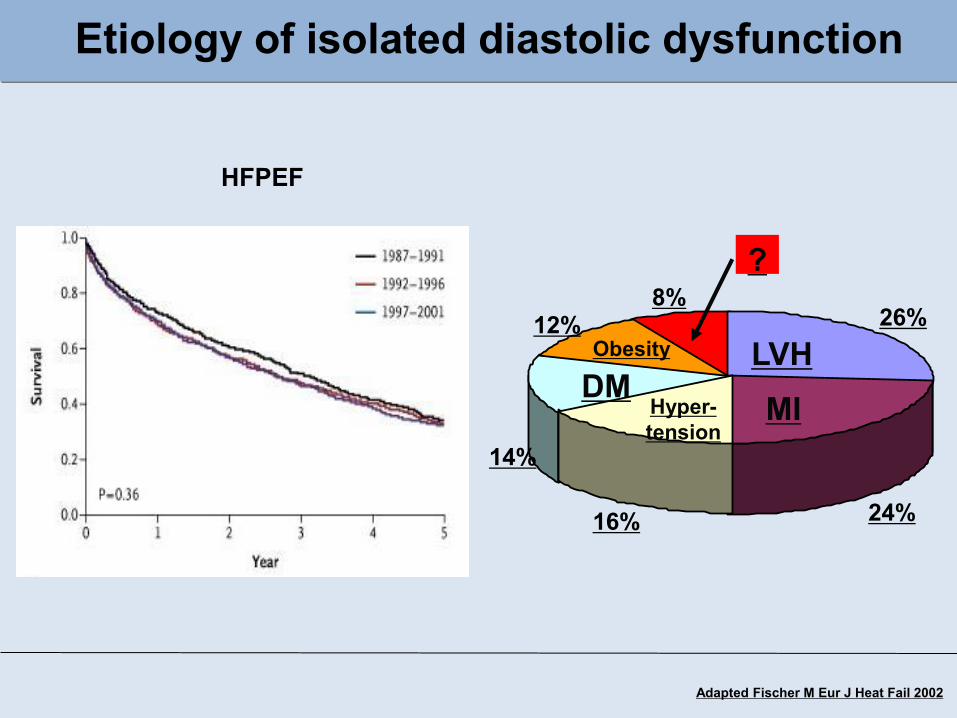
Adapted Fischer M Eur J Heat Fail 2002
Etiology of isolated diastolic dysfunction
26%
24%16%
14%
12%8%
LVHMIHyper-
tension
DMObesity
?
HFPEF

200 ml100500
160
80mm
Hg
C
200 ml100500
160
80mm
Hg
D
Tschöpe et al, Circulation 2005
Endothelial Dysfunction
LVEDPSteifigkeit

ABV:28 ABV:62
Basal Acethylcholine (7.2 µg/min)
Regular endothelial function
ABV:20 ABV:21
Endothelial Dysfunction
ABV: Average peak velocities

Reduced flow reserve and endothelial dysfunction in cardiacParvovirus B19 Infection
Vaskulotropism of PVB 19(In situ Hybridization)
Kandolf et al.
Apoptose zirkulierendermaturer Endothelzellen
p =0.004
Apop
totis
mat
ure
endo
thel
ial c
ells
(in
% o
f PM
NC
)
PV B19Kontrolle
0,07
0,06
0,05
0,04
0,03
0,02
0,01
0,00
Tschöpe et al, Circulation 2005
N = 60 /Gruppe; * p< 0.05
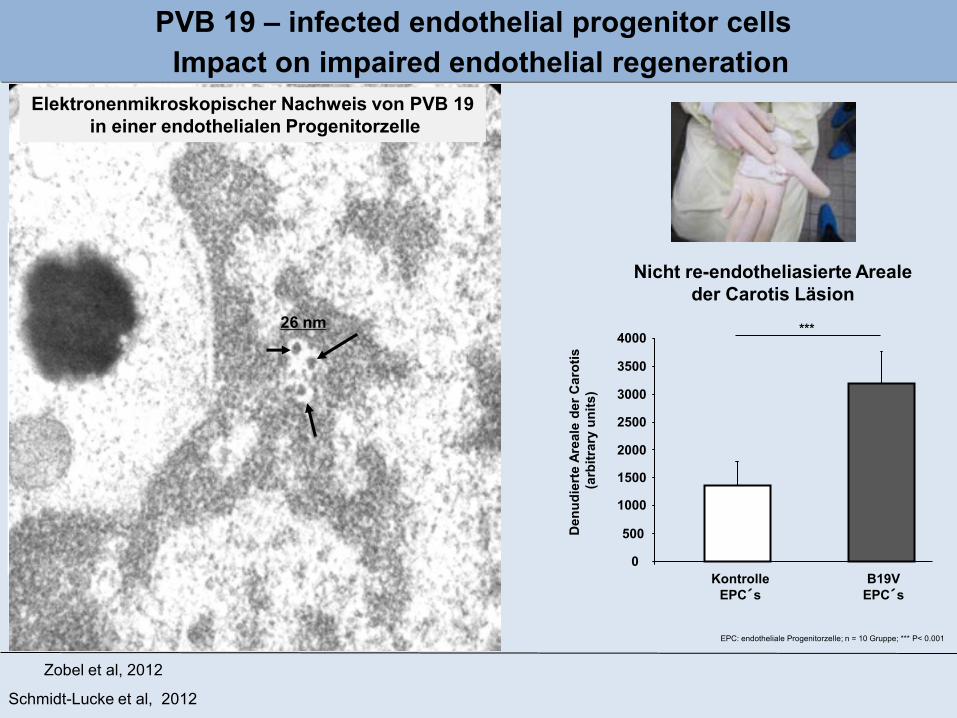
PVB 19 – infected endothelial progenitor cells
Schmidt-Lucke et al, 2012
Parv
oviru
sB
19 c
opie
s/ µ
g ge
nom
icD
NA
EBM Blut KM EBM Blut KM
CD 34+ CD34+KDR+
CD 34+ CD34+KDR+
CD 34+ CD34+KDR+
CD 34+ CD34+KDR+
5000
1000
015
000 KM
Endotheliale ProgenitorZellen
Nicht re-endotheliasierte Arealeder Carotis Läsion
0
500
1000
1500
2000
2500
3000
3500
4000
KontrolleEPC´s
B19VEPC´s
***
Den
udie
rte
Area
le d
er C
arot
is(a
rbitr
ary
units
)
Zobel et al, 2012
Endotheliale ProgenitorZellen
KM: Knochenmark; N = 15 Gruppe; kein Nachweis von PVB in CD 34 - Zellen EPC: endotheliale Progenitorzelle; n = 10 Gruppe; *** P< 0.001
Impact on impaired endothelial regeneration
26 nm
Elektronenmikroskopischer Nachweis von PVB 19in einer endothelialen Progenitorzelle

Vascular density and clinical symptoms in PV B 19 patients
Kontrolle
0,00
250,00
500,00
750,00
Gef
äßdi
chte
/cki
t+K
DR
+
n/m
m2
PV B19 mit
Angina
pectoris
PV B19 ohne
Angina
pectoris
P<0.05
Vascular density
P<0.05
Vascular densiry and anginapectors symptoms
Kontrolle
PVB19 pos
1:400
Schmidt-Lucke et al , 2012 in press
P<0.001
1:400
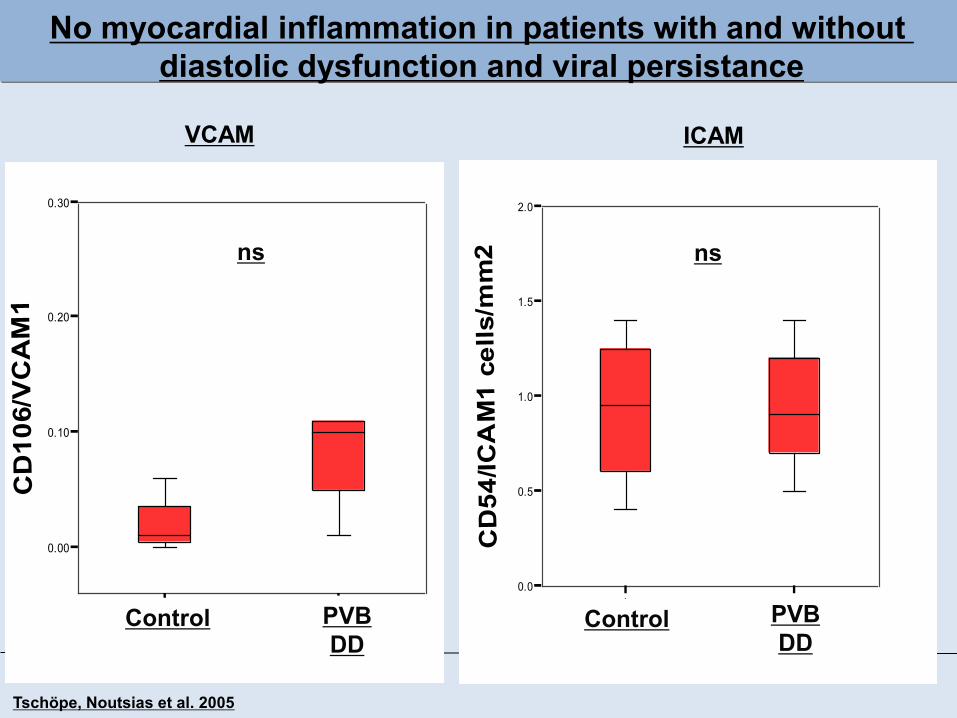
1 3
0.00
0.10
0.20
0.30
CD
106/
VC
AM
1
1 30.0
0.5
1.0
1.5
2.0
CD
54/IC
AM
1 ce
lls/m
m2
Control PVBDD
Control PVBDD
No myocardial inflammation in patients with and without diastolic dysfunction and viral persistance
Tschöpe, Noutsias et al. 2005
VCAM ICAM
ns ns

Mechansims ?
Fibrosis ?Inflammation ?
Endothelial Dysfunction ?

P < 0,033
1.0 2.0 3.0
0.0100
0.0200
0.0300
0.0400
0.0500
0.0600
Sti
ffne
ss
CO PVB+DD
PVB-DD
Cardiac passive stiffness Total collagen content
1.0 2.0 3.0
0.50
1.00
1.50
2.00
Sir
ius
Red
CO PVB+DD
PVB-DD
P < 0,006
LV stiffness and cardiac fibrosis in patients with and without diastolic dysfunction and viral persistance
Tschöpe, Westermann, Pauschinger et al. 2005
N=50 N=50 N=50N=18 N=50
% o
f tis
sue
N=18
P < 0,033
ns ns

VP1 Expression CD106/VCAM-1
Transgene Mausmodelle:Parvovirus B19 - induzierte Kardiomyopathie
Bock et al. 2012
*
IHC: Collagen I
VP1-Co
VP1-Dox
0.0000
0.0005
0.0010
0.0015
0.0020
AF in
%
Kollagen I
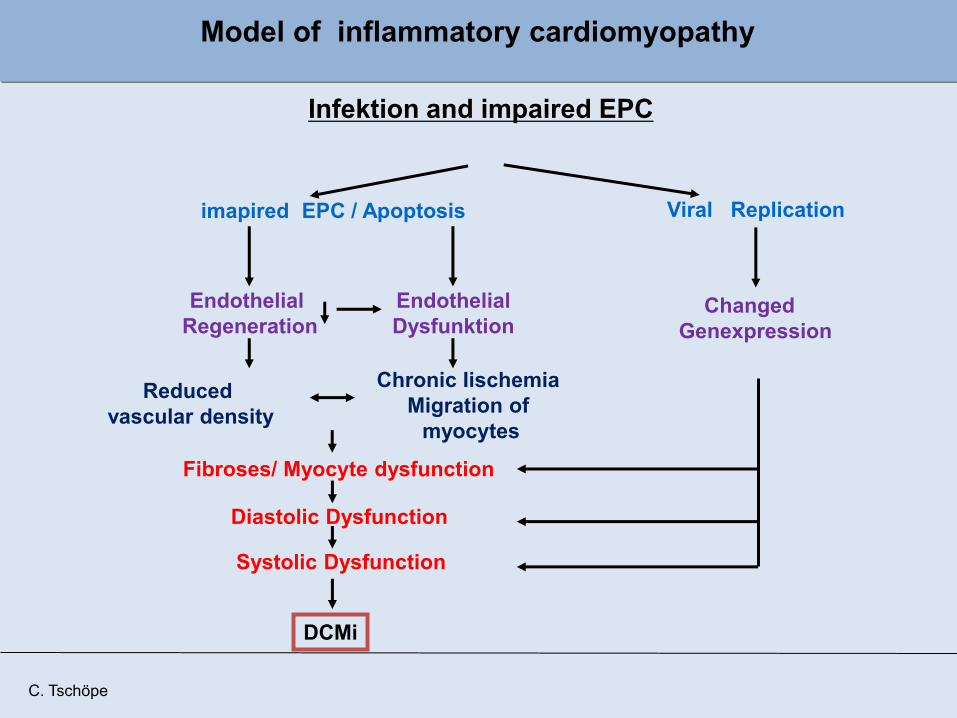
Model of inflammatory cardiomyopathy
Infektion and impaired EPC
imapired EPC / Apoptosis
EndothelialDysfunktion
EndothelialRegeneration
Reducedvascular density
Chronic IischemiaMigration of
myocytes
Fibroses/ Myocyte dysfunction
DCMi
Diastolic Dysfunction
Systolic Dysfunction
ChangedGenexpression
Viral Replication
C. Tschöpe
C. Tschöpe
Riscfactors for HF
Cardiac DysfunctionWall Stress
Activation ofinflammatory cells
Myofibroblasts
FibrosisChemokine
ChemotaxisDegradation
Adhesion
CytokinesOxidative Stress
TitinDephosphorylation
CytokinesActivated fibroblasts
Endothelial Activation
Myofibroblast and Inflammation in heart failure
Regeneration / Vessel density

Cardiac inflammation
Li et al. Eur J Pharmacol 2007Koch et al. Int Immunopharm 2010Riad et al. J Immunol 2011
Innate Immunsystem
TLR-4, -9TRIF, MYD-88
NOD2S100 A8/A9
Westermann et al. Circulation 2011Van Linthout et al. Eur Heart J 2011
Savvatis et al. PlosOne 2012
Regeneration
Development of new anti-inflammatory and antifibrotictherapy options for the future
MesenchymaleStromazelle
T reg´sCAP´s
IL: Interleukin, TNF; Tumor Nekrose faktor, TLR: Toll-like Rezeptor, NOD: Nucleotide-binding oligomerization domain-containing protein, MMP: Metalloproteinase,MSC: Mesenchymale Stromazelle, Treg´s: regulatve T-Zelle; CAP´s: cardiac derived adherent proliferating cell
Virustoxizity
Interferon ßTelvibudine
PV B19Coxsacki B
Cytokine-System
IL1β, IL2, IL4, IL6, IL10, IL23, TNFα
Matrix Proteine(MMP´s)
MMP-2, MMP-9Biglycan

Myofibroblast as a therapeutic target ?

CTGF (CCN2) upregulation in fibroblast after strech in vitro
Cooperation AG Poller, Charite, unpublished

New anti-CTGF intervention option in the futurevia cardiac RNA interefrence
Cooperation AG Poller, Charite, unpublished
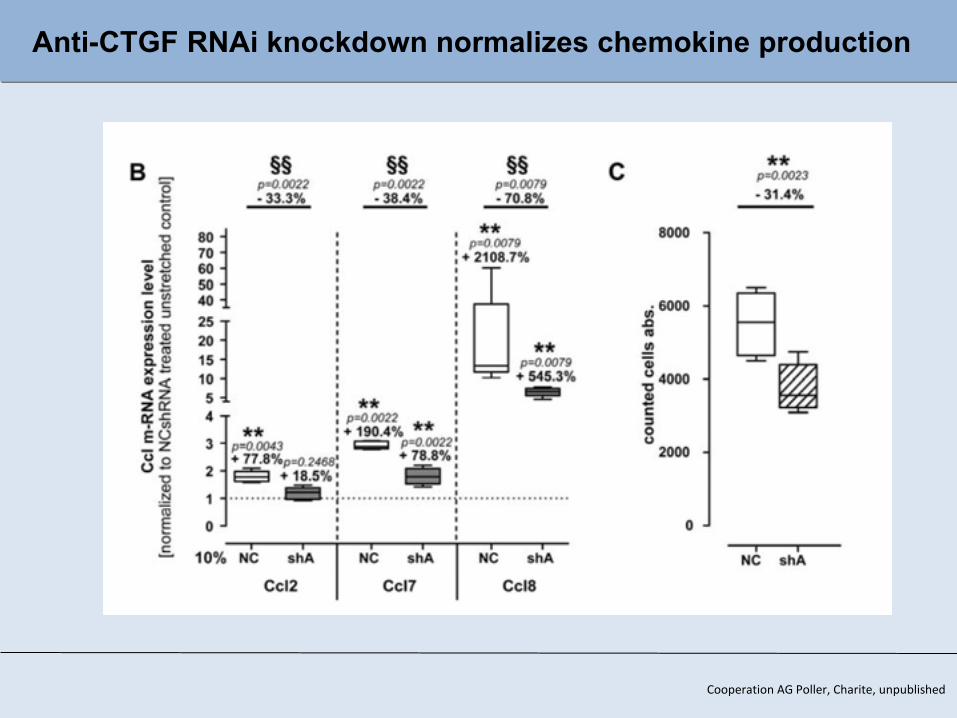
Anti-CTGF RNAi knockdown normalizes chemokine production
Cooperation AG Poller, Charite, unpublished

Cooperation AG Poller, Charite, unpublished
Anti-CTGF RNAi knockdown normalizes collagen and MMP expression

Conclusion
1. Myofibroblasts are chemo-active, activates lymphocytes and can incuse endothelial dysfunction.
2. The number of myofibroblasts correlate with the degree of collagen expression as well as with the number of invading inflammatory cells in the heart.
3. Therefore, myofibroblasts are inflammatory supporter cells
4. They are a therapeutic target to modulate cardiac fibrosis and inflammation.
Thank you for your attention
Charite, Campus Benjamin Franklin, Kardiologie
Thanks
DankeDirk WestermannDiana LindnerChristine ZietschNadine OrinKerstin Puhl
Funded by:SFB TR 19 „Inflammatory Cardiomyopathy“EU FP7-call „Diastolic Heart Failure“


modifiziert nach: O`Neill et al., Nat Rev Immunol 2007,
Zellmembran/Endosommembran
Typ-I-Interferone(z.B. IFN-ß)
bakterielle und virale FragmenteOxidativer Stress
MyD88 TRIF TIR
IRAK
TRAF-6
NFkBIRFs
IRFs-P
pro-inflammatory cytokines(z.B. TNF-α, IL-1ß)
TLR1 TLR5 TLR6TLR2 TLR10TLR4TLR3
Innate Immunsystem:Toll-Like Receptors
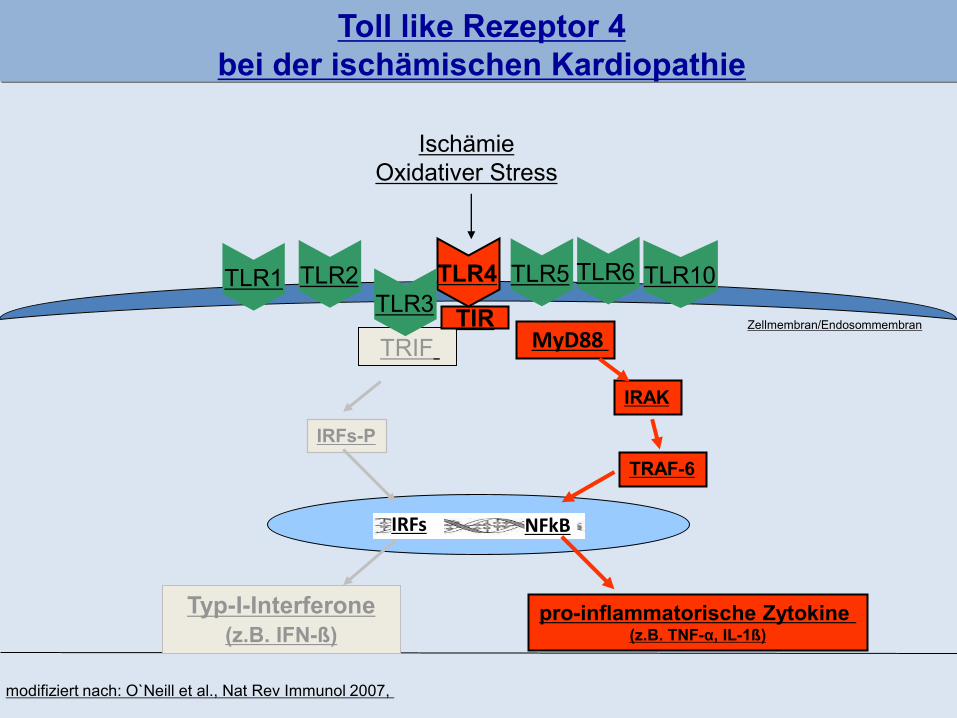
modifiziert nach: O`Neill et al., Nat Rev Immunol 2007,
Zellmembran/Endosommembran
Typ-I-Interferone(z.B. IFN-ß)
IschämieOxidativer Stress
MyD88 TRIFTIR
IRAK
TRAF-6
NFkBIRFs
IRFs-P
pro-inflammatorische Zytokine (z.B. TNF-α, IL-1ß)
TLR1 TLR5 TLR6TLR2 TLR10TLR4TLR3
Toll like Rezeptor 4 bei der ischämischen Kardiopathie

Das TLR System als kritischer Mortalitätsfaktorbeim Myokardinfarkt: Toll-like Rezeptor 4
C57BL/10ScN
Riad & Tschöpe et al. Journal of Immunology 2008
0 10 20 300
50
100
TLR4-/-
Wildtypen
p<0.0001
Tage post Herzinfarkt
Übe
rlebe
n in
Pro
zent
TLR4
TLR4 -/-
TLR4 -/-
n = 25 / Gruppe
Immunzellen
AKT
Apoptose(Tunnel)
JNK
Projektförderung: TR-SFB 19: B5/Z3

modifiziert nach: O`Neill et al., Nat Rev Immunol 2007,
Zellmembran/Endosommembran
Typ-I-Interferone(z.B. IFN-ß)
bakterielle und virale Fragmente
MyD88 TRIF TIR
IRAK
TRAF-6
NFkBIRFs
IRFs-P
pro-inflammatorische Zytokine (z.B. TNF-α, IL-1ß)
TLR1 TLR5 TLR6TLR2 TLR10TLR4TLR3
TIR domain-containing adaptor inducing IFN-ß (TRIF)bei der viralen Myokarditis

TIR domain-containing adaptor inducing IFN-ß (TRIF) bei der viralen Myokarditis
Riad & Tschöpe et al. Journal of Immunology 2011
0 20 40 60 800
25
50
75
100 WT-CVB3
KO-CVB3*
Days
Perc
ent s
urvi
val
TRIF-/-Coxsackievirus (5*105 PFU i.p.)
0 20 40 60 800
25
50
75
100 WT-CVB3
KO-CVB3
KO-CVB3-IFN
*
#
Days
Perc
ent s
urvi
val
Co-3d
TRIF-3d
Co-3d-C
VB3
TRIF-3d-C
VB30
3.5×10 -7
7.0×10 -7 *
IFN
-ß m
RN
A/1
8S
TRIF-/-CBV
TRIF+/+CVB
Kardiale Entzündungsreaktion
Projektförderung: TR-SFB 19: B5/Z3
TRIF+/+

Mögliche zukünftige therapeutische Ansätze
B1 AntagonistenTLR Rezeptor Antagonisten
Interferone
Stress
Endotheliale Aktivierung
Pro-inflammatorischeZytokine
Spezifische Immun-reaktion
Kardiale Dysfunktion
RemodelingHypertophie,
Fibrose,Apoptose
Zelltherapeutischen Ansatz ?
ZytokininhibitorenNO Enhancer
p38 Inhibitorenselekt. MMP-Inhibitoren

Immunmodulatorische Effekte von mesenchymalen Stammzellen
Diabetes mellitusPneumonie
ArthritisMultiple Sklerose
TransplantationNiereninsuffizienz
Infarkt
Review: Abdi et al. Diabetes 2008

Role of mechanic stress
0% 2.5% 7.5% 10%
Stretch
Stimulation ofcollagene production
Stretch
2.5% 5% 7.5% 10% 12.5%
0.0
1.0
2.0
3.0
4.0
ns
*****
*
flexercell-stretch, frequence 1Hz
MC
P-1
pro
tein
con
tent
(x-f
old
over
uns
tret
ched
con
trol
)
Stimulation ofchemokines production
Westermann et al, Circulation HF 2011

Myofibroblast and endothelial activation
VCAM
control CM c-FB CM c-myoFB
0
2
4
6
8
0
2
4
6
8***
treated HMEC cells
rela
tive m
RN
A level
[x-f
old
ove
r co
ntr
ol]
Westermann et al 2012
P<0.01, R=0.82
α-SMA P4HB DAPI

Endothelial Dysfunction in vitro
2.5%
2.5%
* vs. co
Westermann et al 2012

Riskfactors for HF
Activation of inflammatory cells
Myofibroblasts
FibrosisChemokines
Diastolic Dysfunction /Wall Stress
ChemotaxisDegradationAdhesion
C. Tschöpe
CytokinseActivation of Fibroblasts
Fibrosis and Inflammation as a Circulus vitiosus Identification of myofibroblasts in humanen cardiac biopsies

When is the Parvo B19 infection ofthe heart of clinical significance?

n=297/498 (59.6%) n=176/498 (35.3%)
709 +/-828
392 +/-317
84 +/-49
n= 7/91 (7.7%)
3,2x105 +/-8,2x105
P<0,0001
n= 25/498 (5.0%)
***
******
chronic
Myocarditis
dilated
Cardiomyopathycontrols
acute
Myocarditis
B19
V G
E /
µg N
A
P<0,0001
P<0,0001
Kardiale Parvovirus B19 – DNA Last von Patienten mitMyokarditis oder inflammatorischer dilatativer Kardiomyopathie
500
GE
/µg
Bock et al NEJM 2010
1.0×10 0
1.0×10 1
1.0×10 2
1.0×10 3
1.0×10 4
1.0×10 5
1.0×10 6
1.0×10 7

Virus Typen spezfische Reaktion auf eine Interferon-Therapie
n “Clearance” Virus Last Reduktion
Gesamt 88 40 (46%) 57 (65%)
Enterovirus 24 24 (100%)
Adenovirus 9 9 (100%)
Parvovirus 55 7 (14%) 17/55 (31%)
Kühl et al 2012
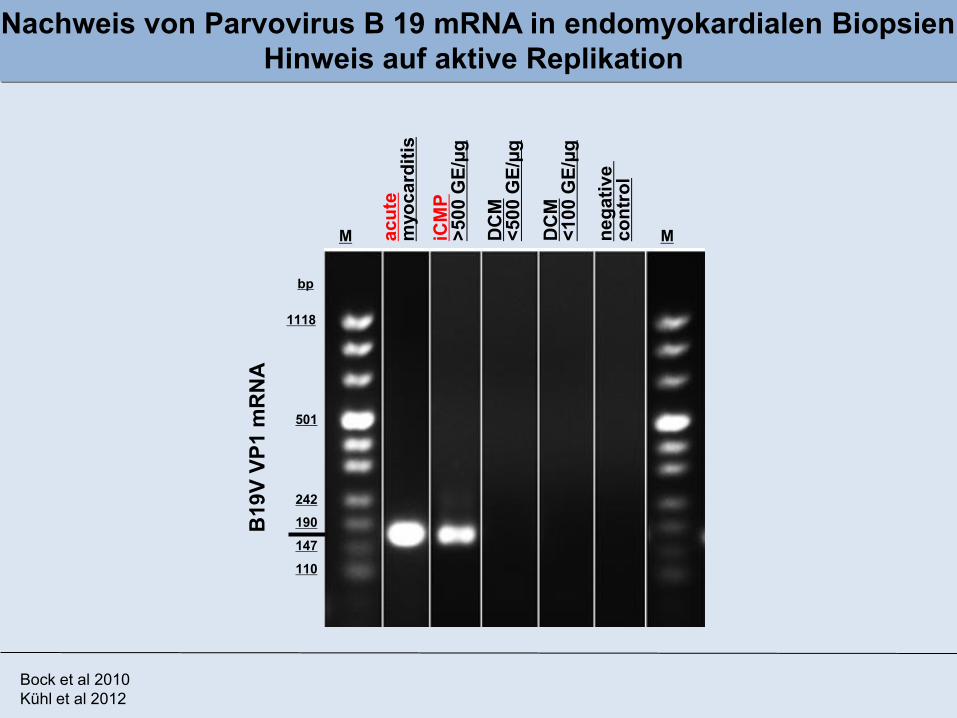
B19
V VP
1 m
RN
AM Mac
ute
myo
card
itis
iCM
P>5
00 G
E/µg
DC
M<5
00 G
E/µg
DC
M<1
00 G
E/µg
nega
tive
cont
rol
1118
501
242190
147
110
bp
Nachweis von Parvovirus B 19 mRNA in endomyokardialen BiopsienHinweis auf aktive Replikation
Bock et al 2010Kühl et al 2012

0255075
100125150175200225250
%
Erythrovirus negativ Erythrovirus positiv ohne Replikation
Regulation der Genexpression bei transkribierter Parvovirus-RNA
C. Tschöpe
PVB19-Rezeptor
Zytokine AtmungskettengeneAdiponectinCarnitin
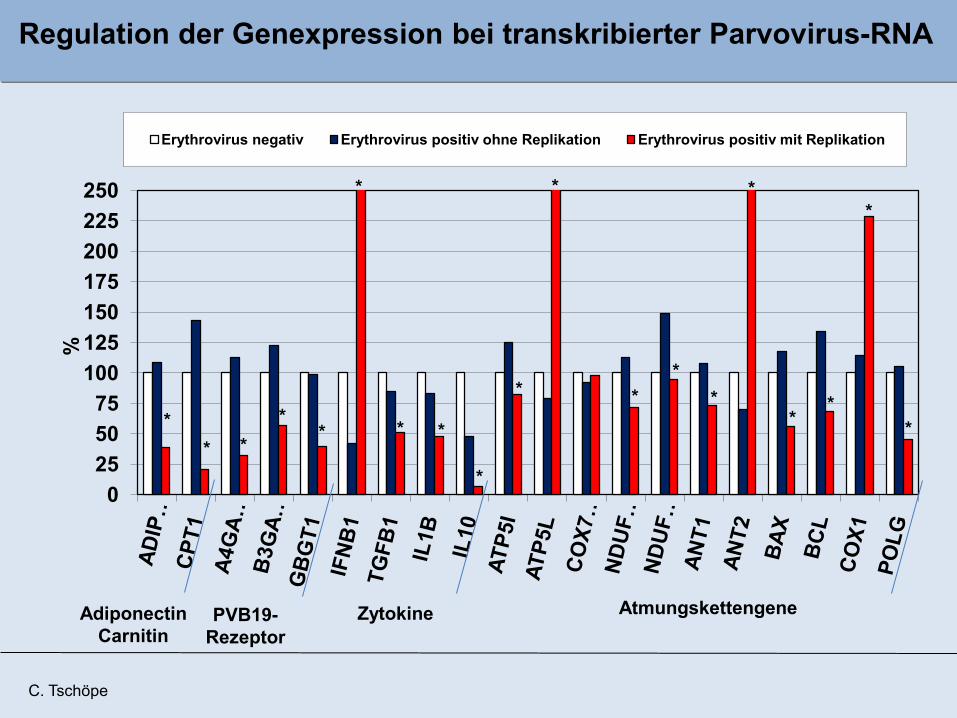
0255075
100125150175200225250
%
Erythrovirus negativ Erythrovirus positiv ohne Replikation Erythrovirus positiv mit Replikation
Regulation der Genexpression bei transkribierter Parvovirus-RNA
PVB19-Rezeptor
Zytokine AtmungskettengeneAdiponectinCarnitin
** *
**
*
* *
*
*
*
**
*
*
**
*
*
C. Tschöpe
Neue Therapie Option ?
Nucleosid Analogon:
Telbivudine
C. Tschöpe
Telbivudine Treatment of
Parvovirus B19-positive
Cardiomyopathy
Pilotstudie
C. Tschöpe

Baseline biopsy Follow up biopsy pB19V load (copies/µg DNA)
2543 1188 <0.05
B19V mRNA (copies/µg RNA)
249 0 <0.01
B19V load in patients with silencedtranscriptional activity (B19V-mRNA) during Telbivudine treatment

Effekt von Telvibudine in behandeltenPatienten mit chronischer kardialer Parvovirus B19 Infektion
n = 30
C. Tschöpe

Telbivudine Treatment of Parvovirus B19-positive Cardiomyopathy
Phase II Studie
Berlin
Göttingen
LübeckHamburg
Heidelberg
Greifswald
ToPIC - Study
C. Tschöpe
Kiel

DCM (EF < 45%; > 6 Monate)PVB mRNA positiv
N = 100
DCMPVB mRNA positiv
N = 50
DCMPVB mRNA positiv
N = 50 Plazebo Telbivudine
DCMPVB mRNA positiv
N = 50
DCMPVB mRNA positiv
N = 50 PlazeboTelbivudine
Nach 6 Monaten:Prim. Endpunkt : EF (Echo / Core Lab)
Sek. Endpunkt : QOL (KK-Score), PVB-Virus Replikation / Entzündung ( Re Biopsie)
Follow up nach 6 Monaten:Prim. Endpunkt : EF (Echo / Core Lab)
Sek. Endpunkt : QOL (KK-Score), PVB-Virus Replikation / Entzündung ( Re Biopsie)
Telbivudine Treatment of Parvovirus B19-positive Cardiomyopathy
C. Tschöpe
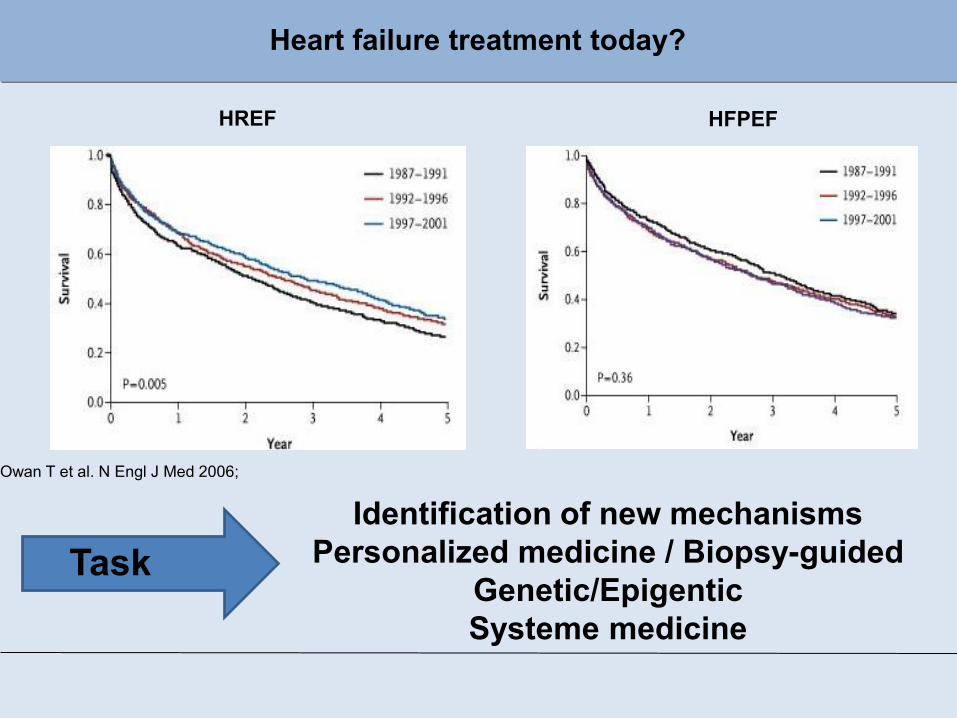
Owan T et al. N Engl J Med 2006;
Heart failure treatment today?
HREF HFPEF
Identification of new mechanismsPersonalized medicine / Biopsy-guided
Genetic/EpigenticSysteme medicine
Task

Merci
Kooperationspartner/Funding:
TR-SFB 19: inflammatorischeKardiomyopathieBCRT/BMBF: Immunsystem u. HerzEU FP7: Diabetes mellitus u. diastolische Herzinsuffizienz EU FP7: Stammzelle u. Diabetes mellitusDZHK: InflammatorischeKardiomyopathie


PVB19 genomes were predominant in patients with unexplainedisolated diastolic dysfunction in our study group.
A strong association with the incidence of endothelial dysfunctionwas obvious, consistent with the hypothesis that PVB19-inducedendothelial dysfunction may be a possible pathomechanismunderlying diastolic dysfunction.
Summary and Conclusion

AdiponectinCarnitin
PVB19Rezeptor
Zytokine Atmungsketten-Enzyme ApoptoseMitochondrium
Gegenregulation der Gene nach Abklingen der PVB19-mRNA (Follow-up Biopsien)
C. Tschöpe

AdiponectinCarnitin
PVB19Rezeptor
Zytokine Atmungsketten-Enzyme ApoptoseMitochondrium
Gegenregulation der Gene nach Abklingen der PVB19-mRNA (Follow-up Biopsien)
*
C. Tschöpe

Inflammatory Cardiomyopathy Conclusion I
-The detection of viral genome and or inflammation in the myocardium has been shown by multivariate regression analysis to be an independent predictorof clinical outcome.
- This cannot be detected by echo/MRI

- However, any rational immunomodulatory therapeutic regimen for inflammatory cardiomyopathy must consider the underlying pathogenesis based on
- histological, - immunohistological and - viral
evaluation of endomyocardial biopsies.
Inflammatory Cardiomyopathy Conclusion III

Cardiac Adherent Proliferating Cells (CAP´s):
Haag et al. J Cell Biochemistry 2010
Gen Expressionsmuster und FACS Analyse
Anti-fibrotische und anti-entzündliche Effekte
Milteva et al. PLOS One 2011
FibroblastenProliferation
MyofibroblastTransdifferentiation
Kollagensynthese
FIBROSE
α-S
MA
DiO
+ ce
lls(%
gat
ed
cells
)
monoculture+CAPs
P<0.001
CAP cells
monoculture+CAPs
Teilu
ngs
ind
ex
P<0.001

Personalised medicine inDilated Cardiomyopathy
DCM
Virus negativeInflammation negative
Virus positive
inflammation positive
Perforin +
Perforin -
immun-suppr.
therapy
sympt. therapy
Interferon-level ↑
Interferon-level ↓
TLR-mutations
mi-RNAProfile
mutation-screening
sympt.therapy
antiviraetherapy
risc-stratification
sympt. and/orrisic adjusted
therapy
CoxsackieVirus
ParvoVirus
Interferon ß Telbivudine
Schultheiss et al EHJ, 2011

Susceptibility and inhibitory concentration (IC) of Telbivudine on parvovirus B19 replication in endothelial cell culture experiments
IC50 < 0.001 µg (2 µM)comparable to HBV
Proposed mechanisms of telbivudineDetermination of IC50 of telbivudine in cell cell culture
Telbivudine can probably interact with DNA-synthesis during rolling hairpinreplication
Telbivudine can probably interact with host immune system to control B19V replication

0,000
0,200
0,400
0,600
0,800
1,000
1,200
control 100 ng/ml 1 µg/ml 5 µg/ml 10 µg/ml 20 µg/ml 50 µg/ml
´re
l. co
nz. B
19V
VP2
mR
NA
IC50 ~ 2.5 µg/ml
P>0.001
conz. Telbivudine
Inhibition of Parvovirus B19 Replication by Telbivudine Treatment in B19V-infected endothelial Cell Culture (hMEC-1)

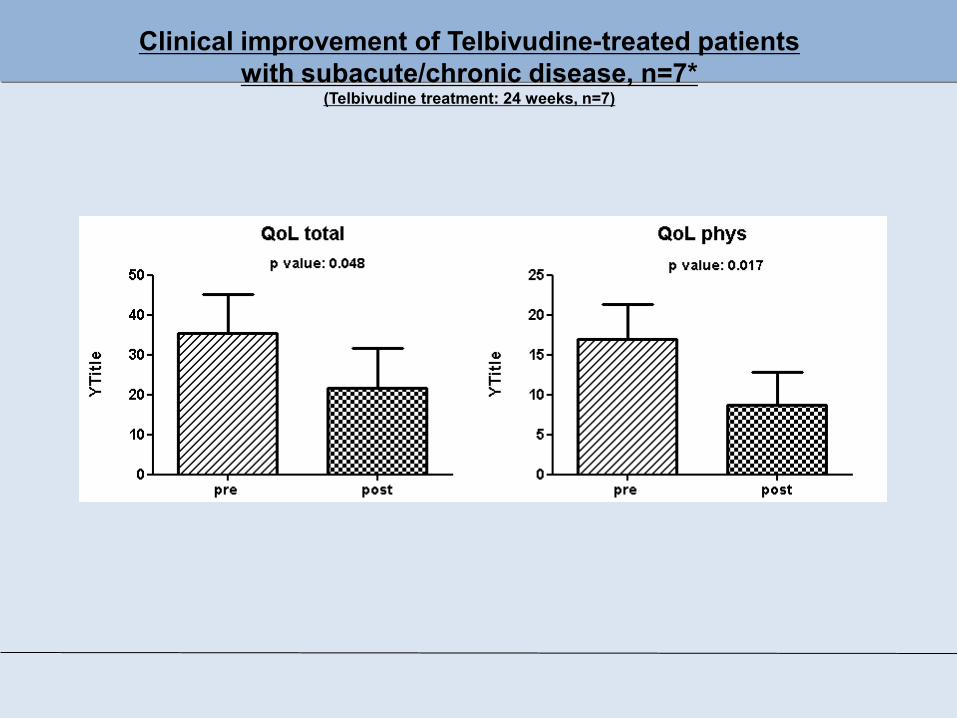
Clinical improvement of Telbivudine-treated patientswith subacute/chronic disease, n=7*
(Telbivudine treatment: 24 weeks, n=7)

Kardiale Inflammation
Zytokin-System
IL1β, IL2, IL4, IL6, IL10, IL23, TNFα
Li et al. Eur J Pharmacol 2007Koch et al. Int Immunopharm 2010Riad et al. J Immunol 2011
AngeboreneImmunsystem
TLR-4, -9TRIF, MYD-88
NOD2S100 A8/A9
Matrix Proteine(MMP´s)
MMP-2, MMP-9Biglycan
Westermann et al. Circulation 2011Van Linthout et al. Eur Heart J 2011
Savvatis et al. PlosOne 2012
Regeneration
Entwicklung neuer Interventionsziele zurTherapieoptimierung der Zukunft bei der Herzinsuffizienz
Virustoxizität
Interferon ßTelvibudine
MesenchymaleStromazelle
T reg´sCAP´s
PV B19Coxsacki B
IL: Interleukin, TNF; Tumor Nekrose faktor, TLR: Toll-like Rezeptor, NOD: Nucleotide-binding oligomerization domain-containing protein, MMP: Metalloproteinase,MSC: Mesenchymale Stromazelle, Treg´s: regulatve T-Zelle; CAP´s: cardiac derived adherent proliferating cell
Clinical improvement of Telbivudine-treated patientswith subacute/chronic disease, n=7*
(Telbivudine treatment: 24 weeks, n=7)

p = 0.080
LV-E
F (%
)
0
10
20
30
40
50
60
baseline week 4 week 12 week 24
LV-EF
Hemodynamic changes in Telbivudine-treated Patients with subacute/chronic disease
* Acute B19V infections excluded
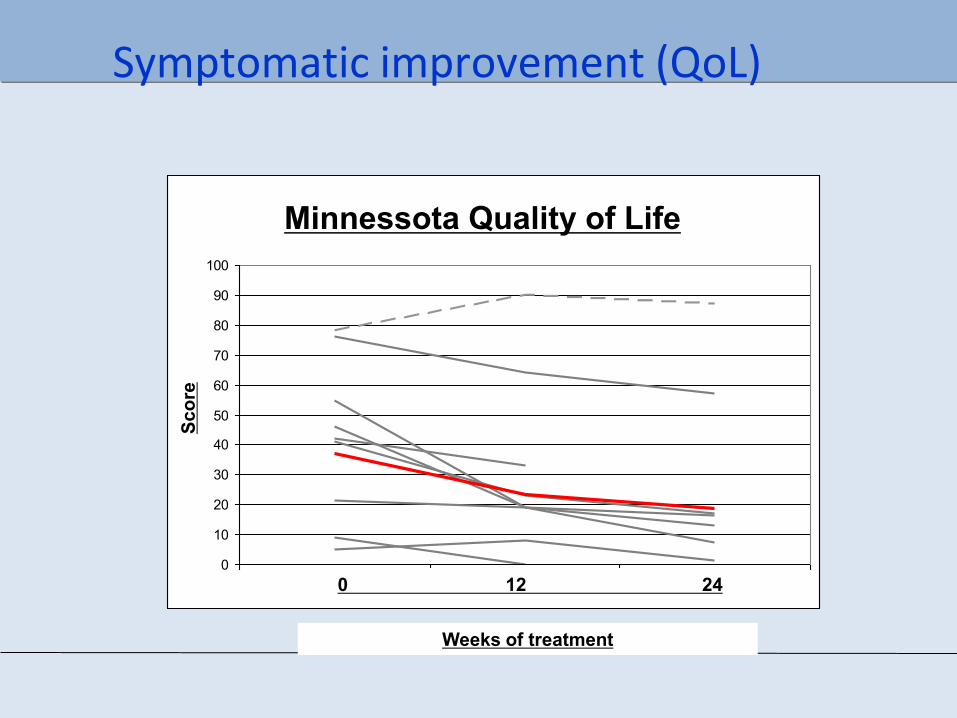
Symptomatic improvement (QoL)
Lebensqualität - gesamt- ohne den (grau dargestellten) Patienten mit psych. Begleiterkrankung -
0
10
20
30
40
50
60
70
80
90
100
0 12 24
nied
riger
Pun
ktw
ert =
bes
sere
Leb
ensq
ualit
ät
Minnessota Quality of Life
0 12 24
Scor
e
Weeks of treatment

Susceptibility and inhibitory concentration (IC) of Telbivudine on parvovirus B19 replication in endothelial cell culture experiments
IC50 < 0.001 µg (2 µM)comparable to HBV
Determination of IC50 of telbivudine in cell cell culture

Veränderung der kardialen Genexpression ist assoziiert mit transkribierter Parvovirus-RNA

B19
V VP
1 m
RN
A
M Macut
em
yoca
rditi
siC
MP
>500
GE/
µgD
CM
<500
GE/
µgD
CM
<100
GE/
µgne
gativ
e co
ntro
l
1118
501
242190147110
bp
Nachweis von Parvovirus B 19 mRNA in endomyokardialen Biopsien:Hinweis auf aktive Replikation
In situ Hybridisierung(PVB DNA)
Bock et al 2010Kühl et al 2012
α-SMA P4HB DAPI
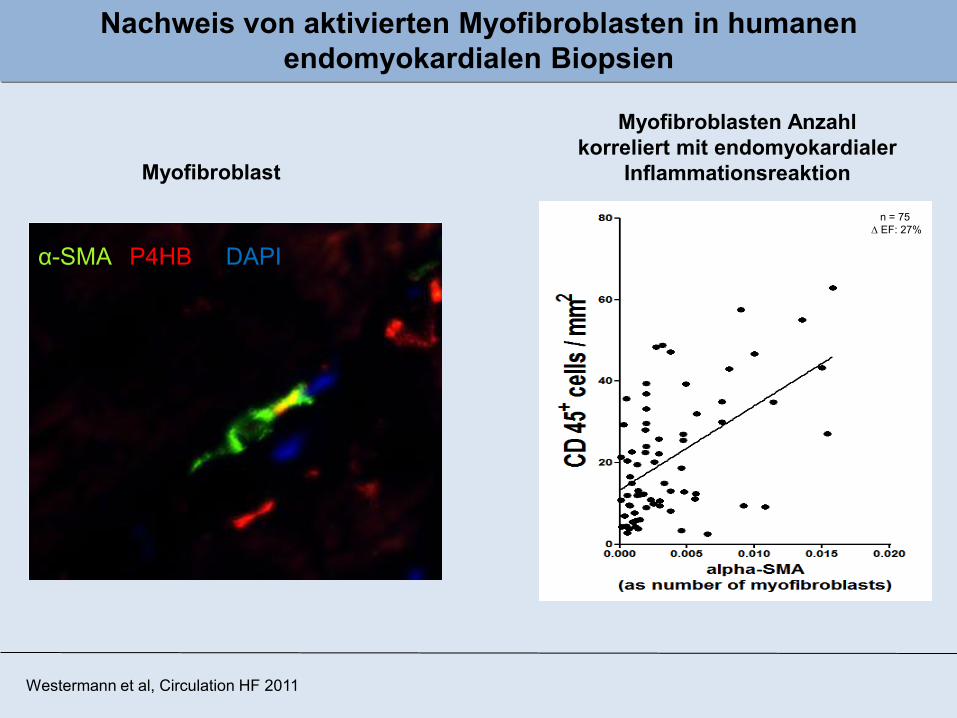
Nachweis von aktivierten Myofibroblasten in humanenendomyokardialen Biopsien
Myofibroblast
Myofibroblasten Anzahlkorreliert mit endomyokardialer
Inflammationsreaktion
Westermann et al, Circulation HF 2011
n = 75D EF: 27%
![Is the Local Potential Much Higher than the Exports?518]4. China W… · inflammation and tissue repair during which epithelial, endothelial, inflammatory cells, platelets and fibroblasts](https://static.documents.pub/doc/80x56/5fc06a0e694c856d8340d5fc/is-the-local-potential-much-higher-than-the-exports-5184-china-w-inflammation.jpg)






