

Influenza and Influenza Vaccine
Epidemiology and Prevention of Vaccine-Preventable Diseases
National Center for Immunization and Respiratory Diseases
Centers for Disease Control and Prevention
Revised May 2009
Influenza Antigenic Changes
• Antigenic Shift
–major change, new subtype
–caused by exchange of gene segments
–may result in pandemic
• Example of antigenic shift
–H2N2 virus circulated in 1957-1967
–H3N2 virus appeared in 1968 and completely replaced H2N2 virus

Influenza Antigenic Changes
• Antigenic Drift–minor change, same subtype–caused by point mutations in gene–may result in epidemic
• Example of antigenic drift–in 2002-2003, A/Panama/2007/99
(H3N2) virus was dominant–A/Fujian/411/2002 (H3N2) appeared
in late 2003 and caused widespread illness in 2003-2004
Influenza Clinical Features
• Incubation period 2 days (range 1-4 days)
• Abrupt onset of fever, myalgia, sore throat, nonproductive cough, headache
• Severity of illness depends on prior experience with related variants
Influenza Complications
• Pneumonia
–secondary bacterial
–primary influenza viral
• Reye syndrome
• Myocarditis
• Death 0.5-1 per 1,000 cases

Impact of Influenza-United States, 1990-1999
• Approximately 36,000 influenza-associated deaths during each influenza season
• Persons 65 years of age and older account for more than 90% of deaths
• Higher mortality during seasons when influenza type A (H3N2) viruses predominate
• Highest rates of complications and hospitalization among young children and person 65 years and older• Average of more than 200,000
influenza-related excess hospitalizations • 57% of hospitalizations among
persons younger than 65 years of age• Greater number of hospitalizations
during type A (H3N2) epidemics
Impact of Influenza-United States, 1990-1999
Influenza Among School-Aged Children
• School-aged children
–typically have the highest attack rates during community outbreaks of influenza
–serve as a major source of transmission of influenza within communities
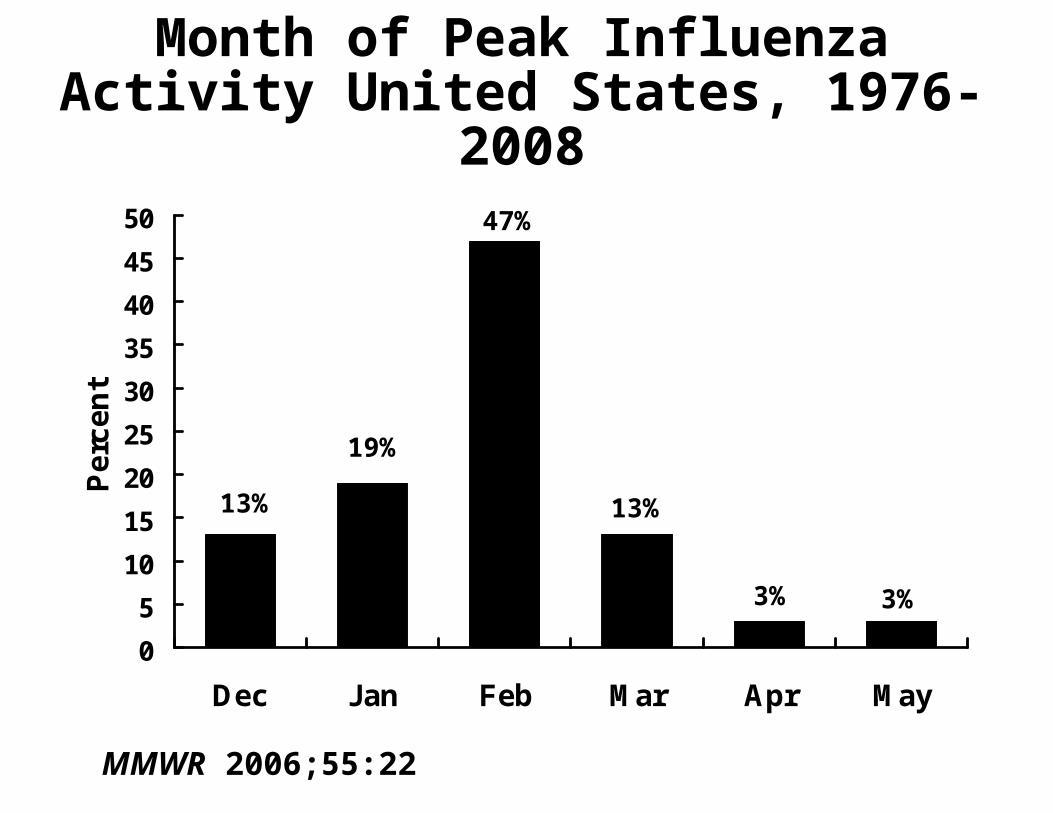
Month of Peak Influenza Activity United States, 1976-2008
0
5
10
15
20
25
30
35
40
45
50
Dec Jan Feb Mar Apr May
Pe
rce
nt
13%
19%
47%
13%
3% 3%
MMWR 2006;55:22

Influenza Vaccines
• Inactivated subunit (TIV)–intramuscular–trivalent–split virus and subunit types–duration of immunity 1 year or less
• Live attenuated vaccine (LAIV)–intranasal–trivalent–duration of immunity at least 1 year

Inactivated Influenza Vaccine Efficacy
• 70%-90% effective among healthy persons younger than 65 years of age
• 30%-40% effective among frail elderly persons
• 50%-60% effective in preventing hospitalization
• 80% effective in preventing death

05
10152025303540
Illness
Perc
en
t
0
2
4
6
8
10
Hosp Pneu Death
Per
cen
t
Influenza and Complications Among Nursing Home Residents
Vaccinated* Unvaccinated
RR=1.9 RR=2.0 RR=2.5 RR=4.2
*Inactivated influenza vaccine. Genesee County, MI, 1982-1983
LAIV Efficacy in Healthy Children
• 87% effective against culture-confirmed influenza in children 5-7 years old
• 27% reduction in febrile otitis media (OM)
• 28% reduction in OM with accompanying antibiotic use
• Decreased fever and OM in vaccine recipients who developed influenza
LAIV Efficacy in Healthy Adults
• 20% fewer severe febrile illness episodes• 24% fewer febrile upper respiratory
illness episodes• 27% fewer lost work days due to
febrile upper respiratory illness• 18%-37% fewer days of healthcare
provider visits due to febrile illness• 41%-45% fewer days of antibiotic use
Timing of Influenza Vaccine Programs
• Influenza activity can occur as early as October
• In more than 80% of seasons since 1976, peak influenza activity has not occurred until January or later
• In more than 60% of seasons the peak was in February or later

Timing of Influenza Vaccine Programs
• Providers should begin offering vaccine soon after it becomes available, if possible by October
• To avoid missed opportunities for vaccination, providers should offer vaccine during routine healthcare visits or during hospitalizations whenever vaccine is available

Inactivated Influenza Vaccine Schedule
AgeGroup
6-35 mos
3-8 yrs
>9 yrs
Dose0.25 mL
0.50 mL
0.50 mL
No.Doses1* or 2
1* or 2
1
*Only one dose is needed if the child received 2 doses of influenza vaccine during the previous influenza season

Influenza Vaccination of Children
• Children 6 months through 8 years of age who did not receive the recommended second dose of influenza vaccine in the initial year that they received influenza vaccine should receive 2 doses during the next influenza season*
• Children 6 months through 8 years of age who are being vaccinated two or more seasons after receiving an influenza vaccine for the first time should receive a single annual dose, regardless of the number of doses administered previously
*applies only to the influenza season that follows the first season that a child younger than 9 years receives influenza vaccine
Influenza Vaccination Schedule
• All children younger than 9 years receiving seasonal influenza vaccine for the first time this season should receive 2 doses, separated by 4 weeks
• Children younger than 9 years who received a seasonal vaccine for the first time last season but who received only 1 dose should receive 2 doses this season
MMWR 2010;59 (early release) From the Immunization Update 2010 webcast (originally broadcast August 5, 2010

Influenza Vaccination Schedule
• Children younger than 9 years who did not receive at least 1 dose of a 2009 monovalent vaccine should receive 2 doses of seasonal vaccine this season
• Children younger than 9 years whose 2009 pandemic vaccine history is not known should receive 2 doses this season
MMWR 2010;59 (early release) From the Immunization Update 2010 webcast (originally broadcast August 5, 2010
Live Attenuated Influenza VaccineIndications
• Healthy*, nonpregnant persons 2 through 49 years of age, including
–healthy children
–healthcare personnel
–persons in close contact with high-risk groups
–persons who want to reduce their risk of influenza
*Persons who do not have medical conditions that increase their risk for complications of influenza
Fluzone High-Dose TIV
• Approved only for persons 65 years of age or older
• Each dose contains 4 times as much hemagglutinin as the regular formulation of Fluzone for adults
• ACIP has not expressed a preference for the high dose Fluzone formulation or any other inactivated vaccine for use in persons 65 years and older
MMWR 2010;59 (early release) From the Immunization Update 2010 webcast (originally broadcast August 5, 2010

Inactivated Influenza Vaccine Adverse Reactions
Local reactions 15%-20%
Fever, malaise not common
Allergic reactions rare
Neurological very rare reactions

Live Attenuated Influenza VaccineAdverse Reactions
• Children–no significant increase in URI symptoms,
fever, or other systemic symptoms–significantly increased risk of asthma or
reactive airways disease in children 12-59 months of age
• Adults–significantly increased rate of cough, runny
nose, nasal congestion, sore throat, and chills reported among vaccine recipients–no increase in the occurrence of fever
• No serious adverse reactions identified
Inactivated Influenza VaccineContraindications and Precautions
• Severe allergic reaction to a vaccine component (e.g., egg) or following a prior dose of vaccine
• Moderate or severe acute illness
• History of Guillian Barré syndrome within 6 weeks following a previous dose of TIV (precaution)

Live Attenuated Influenza VaccineContraindications and Precautions
• Children younger than 2 years of age*
• Persons 50 years of age or older*
• Persons with chronic medical conditions*
• Children and adolescents receiving long-term aspirin therapy*
*These persons should receive inactivated influenza vaccine

Live Attenuated Influenza VaccineContraindications and Precautions
• Immunosuppression from any cause*
• Pregnant women*
• Severe (anaphylactic) allergy to egg or other vaccine components
• History of Guillian-Barré syndrome
• Children younger than 5 years with recurrent wheezing*
• Moderate or severe acute illness
*These persons should receive inactivated influenza vaccine







