

Jallo 1
Intramedullary Low-Grade Astrocytomas: Long-Term Outcome Following Radical Surgery
George I Jallo MD, Shabbar Danish BA, Linda Velasquez MS and Fred Epstein
MD
Key Words: astrocytoma, intramedullary, radiotherapy, spinal cord tumor Summary: The management of low-grade intramedullary astrocytomas is controversial. Unlike ependymomas, which have a distinct cleavage plane, astrocytomas are diffuse infiltrative tumors. The intramedullary tumor database at NYU Medical Center was searched to identify all patients with intramedullary astrocytoma from 1988 to 1994. Seventeen patients presented with a low-grade diffuse astrocytoma. The medical, surgical and office records were reviewed retrospectively and statistically analyzed. All patients underwent a radical resection of the intramedullary tumor; 12 patients had gross total removal and 5 had subtotal removal. Nine patients received adjuvant radiotherapy. The median follow-up period was 7.4 years. Fourteen patients are alive and have stable disease. Eleven patients (79%) are functionally independent at last follow-up. The remaining patients are at functional Grade III. The 5-year overall survival was 82% for this group. These results indicate that aggressive surgery is associated with a prolonged survival for patients with intramedullary astrocytomas. Radiation therapy should only be reserved for patients who have radiographic progression or inoperable disease.
Correspondence/Reprint Author: George I Jallo MD, Division of Pediatric Neurosurgery, Johns Hopkins Hospital, 600 North Wolfe Street, Harvey 811, Baltimore, MD, 21287 410 955-7851, 410 955-7862 [email protected]

Jallo 2
INTRODUCTION
Intramedullary spinal cord tumors are rare central nervous system
neoplasms which affect individuals of all ages. Intramedullary low-grade
astrocytomas are the most frequent histologic type of intramedullary tumor in
children, however the majority of intramedullary neoplasms in adults are
ependymomas. Intramedullary spinal cord low-grade astrocytomas represent
only 5 to 15% of all adult spinal cord tumors [1], thus the literature is sparse
concerning the prognostic factors and long-term treatment results for adult
patients with low-grade intramedullary astrocytomas.
At most centers, a laminectomy and biopsy is typically performed for the
majority of intramedullary neoplasms. Following biopsy and histological
confirmation of an astrocytoma, the patient is then referred for adjuvant
radiotherapy. However, the efficacy of this treatment modality is controversial.
There are only few reports which substantiate the long-term benefits of
radiotherapy for intramedullary tumors [2-5]. This number is even smaller for
intramedullary astrocytomas [2,3,6-11]. In contrast, we have previously reported
our surgical approach and avoidance of radiation therapy for intramedullary
astrocytomas [12-15]. This review consists of a detailed analysis and long-term
follow-up of 17 adult patients, with histologically confirmed and characterized
low-grade intramedullary astrocytomas, who were treated with radical surgery.
Some of our patients have been previously included in other publications [13]
Jallo 3
CLINICAL MATERIAL and METHODS
Patient Population
The intramedullary tumor database at New York University Medical
Center was searched to identify all patients with histologically verified diffuse
low-grade astrocytoma. The search identified 17 adult patients with
intramedullary low-grade astrocytoma operated upon by the senior author from
April 1988 to April 1994. Intramedullary tumors other than low-grade
astrocytoma were excluded from this study. The medical, radiological, surgical,
pathological and office records from these 17 patients were reviewed
retrospectively. Data pertaining to clinical presentation, management and
outcomes were collected. The medical information analyzed for each patient
included age at presentation, symptoms at presentation, duration of symptoms,
previous treatment, adjuvant therapy and immediate and late functional status.
All patients were called and interviewed according to a carefully designed
questionnaire.
The patient’s functional status was assessed in accordance to the
previously published McCormick scale [16]. Grade I, neurologically normal,
with mild focal deficit not significantly affecting the function of the involved
limb, mild spasticity or reflex abnormality and normal gait; Grade II, the
presence of a sensorimotor deficit affecting the function of the involved limb,
mild to moderate gait difficulty, and severe pain or dysesthetic syndrome
impairing the patient’s quality of life, but with independent function and

Jallo 4
ambulation; Grade III, more severe neurological deficit, the requirement of a cane
or brace for ambulation, or significant bilateral upper extremity impairment,
with or without independent function; and Grade IV, a severe neurological
deficit, the requirement of a wheelchair or cane or brace due to bilateral upper
extremity impairment, and usually without independence of function. The pre-
and postoperative functional grade as well as the grade at follow-up of all
patients alive was recorded.
Surgical Approach
The senior author attempted gross-total removal (GTR) in all patients.
Gross total removal is defined as removal of more than 95% of the tumor as
evidenced by both the surgical report and post-operative imaging studies. Sub-
total resection is defined as 80 to 95% removal of the tumor. The surgical
technique has been described in detail in previous publications [13-15]. Briefly,
ultrasonography was routinely employed before and after resection for
localization and to assure the extent of the resection [17]. The ultrasonic
aspirator was used to excavate the tumor from the inside outward until the glial-
white matter interface was reached. Sensory and motor evoked potentials were
used routinely for all the operations. Sensory evoked potential were monitored
for all patients, and motor potentials were monitored in patients operated upon
after 1991.
Statistical Analysis

Jallo 5
Progression-free survival (PFS) and overall survival rates were measured
from the first operation performed by the senior author. Progression-free and
overall survival rates were estimated using the technique of Kaplan and Meier
[18]. The parameters investigated include age, sex, duration of symptoms,
location, extent of resection and radiation therapy.
RESULTS
Presentation
The patient population consisted of 7 men and 10 women ranging in age
from 22 and 61 years (mean, 33.0 yrs). At the time of diagnosis the location of
tumors was cervical (10 cases), cervicothoracic (2 cases) and thoracic (4 cases).
The duration of symptoms before medical attention ranged from 1 to 48
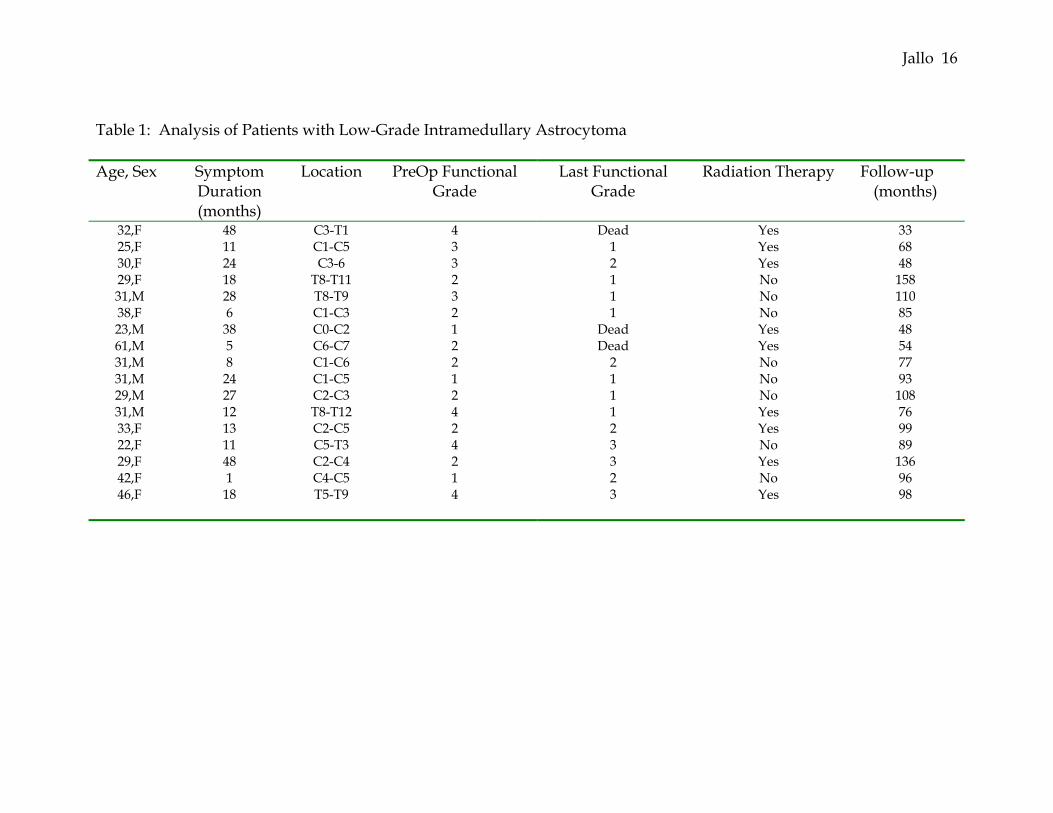
months, with mean of 20.0 months. Table 1 summarizes the characteristics for
this patient population. The most common indicators for radiographic imaging
were pain, sensory, motor difficulties or gait abnormalities. The most common
presenting symptoms were pain and sensory deficits with significant weakness
usually evolving much later. Pain was predominately along the spinal axis. The
mean preoperative functional status for the study group was 2.4. Prior to
surgery, 3 patients were classified as Grade I, 7 as Grade II, 3 as Grade III, and
4 as grade IV.
Seven patients had undergone prior surgery before being referred to the
senior author. All these patients had biopsies for histological diagnosis and 5
Jallo 6
patients then received adjuvant radiotherapy. These patients were referred for
further treatment because of clinical or radiographic progression.
Surgical Results
Complete removal was achieved in 12 patients and subtotal removal
performed in the remaining 5 patients. The histological diagnosis was low-grade
fibrillary astrocytoma in all cases. There were no cases of pilocytic astroctyoma
in this series. In several cases a peripheral rim of gliosis was present which
contained numerous Rosenthal fibers. Small biopsies of this gliotic tissue may
lead to the diagnosis of pilocytic astrocytoma, however with the large tumor
specimen a more definitive diagnosis of fibrillary astrocytoma was easily
confirmed.
Adjuvant therapy
A total of nine patients received additional therapy. Five patients received
adjuvant radiotherapy prior to referral. These patients received prior
radiotherapy after a laminectomy and biopsy of the intramedullary tumor was
performed. Four patients received postoperative radiotherapy after subtotal
removal at our institution. No patient received adjuvant chemotherapy. The
remaining patients were treated with surgery alone.
Outcome Analysis
All patients were available for follow-up review. There was no peri-
operative mortality, and the median long-term follow-up was 7.4 years (range

Jallo 7
33-158 months). There was only one complication, a cerebrospinal fluid leak
which required a wound revision.
Three patients died from tumor progression. The mean survival of these 3
patients was 33.3 months (range, 24-36 months). At the time of death, all 3
showed evidence of progressive local disease. The mean age of these three
patients was 38.7 years, compared with a mean of 34.7 years in patients who are
still alive. Fourteen patients are alive for analysis. In this group, 9 patients show
no evidence of tumor as evaluated by MRI. Five patients have evidence of
residual but stable disease. No patient currently alive has active disease.
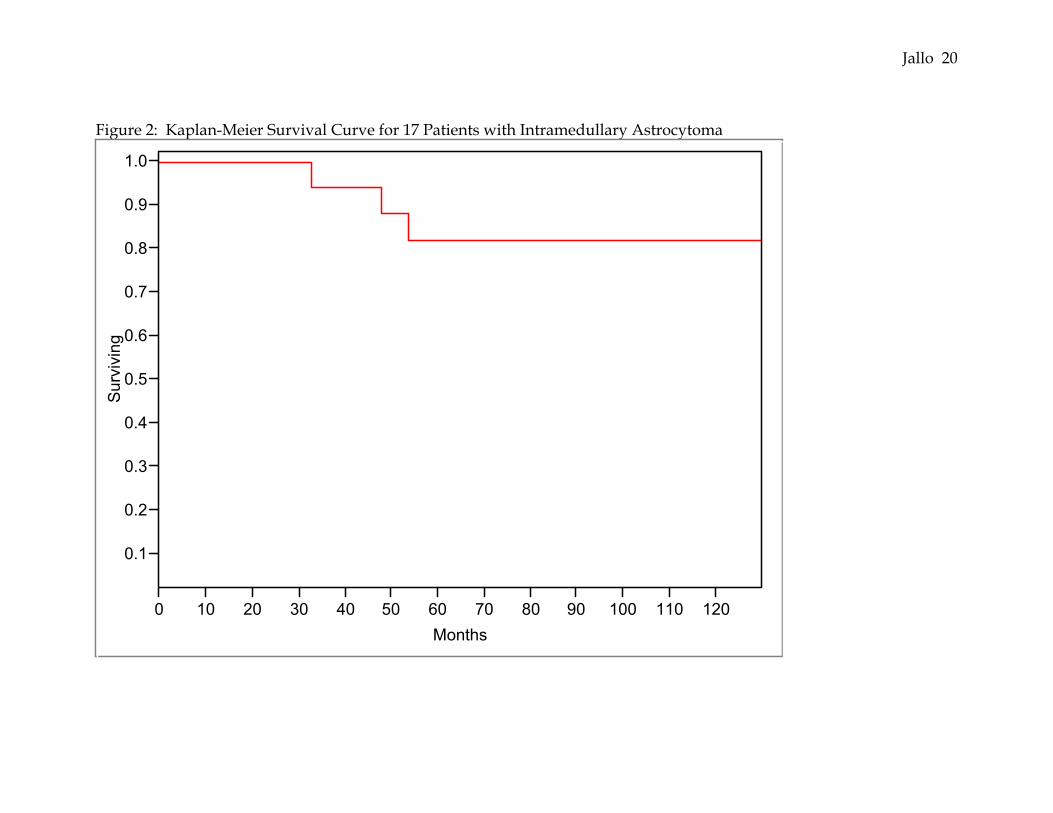
The survival rate for all patients with spinal cord low-grade astrocytoma
was 82% at 5-years and 82% at 10-years. Patient survival and progression-
free rate was not correlated with age, prior treatment, tumor span, or location.
Patients who did not receive radiation therapy did not have a poorer survival
rate than patients who did.
Functional Status of Patients
The mean functional status of the 14 surviving patients is 1.7. Twelve
(86%) patients have improved or remained the same as compared to the
preoperative status. Only two (14%) patients have worsened as compared to
their preoperative function. Eleven patients are functionally independent (Grade
I or II) and the remaining patients are functional Grade III.
DISCUSSION

Jallo 8
Intramedullary astrocytomas are much less frequent than ependymomas
in adults [1]. The potential for inflicting neurological injury by radical surgery
in patients with intramedullary neoplasms is significant and the optimum
treatment for these neoplasms remains controversial. In particular, the role of
surgery and radiation therapy in the treatment of these lesions is the center of
debate. The survival of adult low-grade astrocytomas of the spinal cord is
generally long in comparison with the high-grade astrocytomas. There have
been many studies investigating the role of radiotherapy for these tumors [2,3,6-
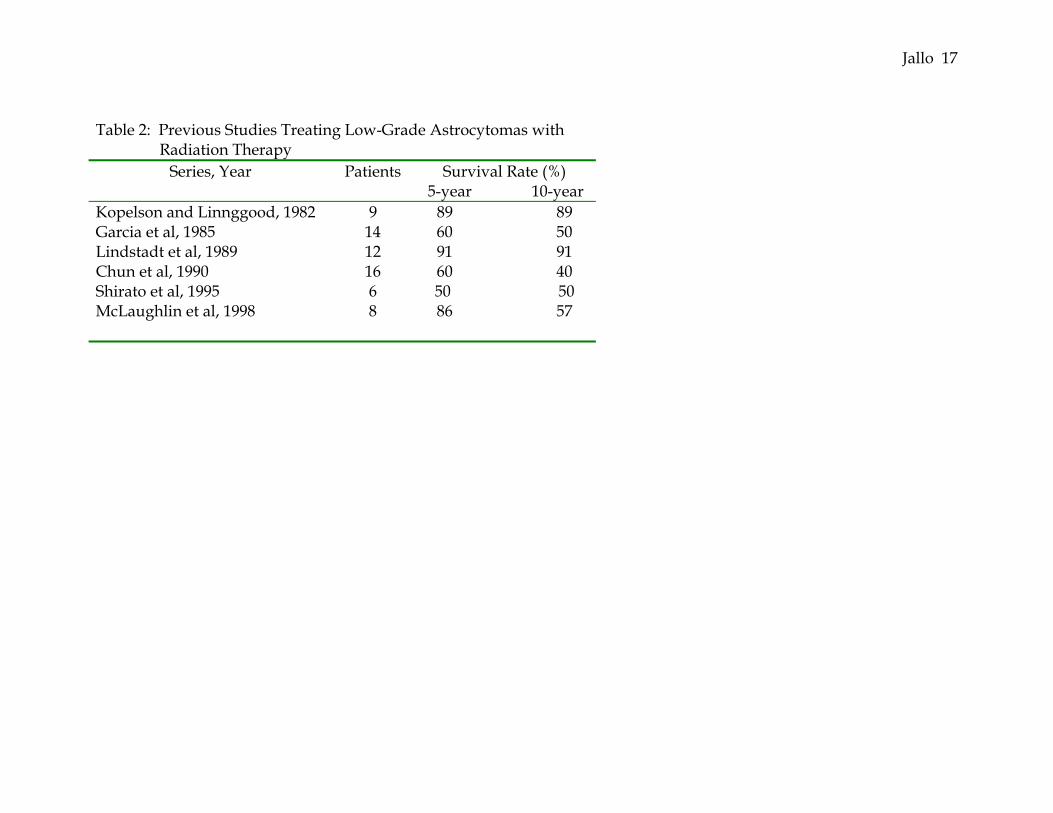
11], however the results have been inconclusive. Radiation therapy achieves a 5-
year survival rate in the range of 50-90% (see Table 2). There is a high incidence
of local failure, range 22-56%, usually occurring in the first 36 months, and there
does not appear to be a dose response relationship suggesting that better control
can be achieved with doses higher than 5040 cGy. The major concern with
radiation therapy is that the target organ and the structure most at risk for
normal tissue damage are the same [19].
We, like some authors[19-21], advocate aggressive surgery and avoidance
of radiation therapy for these low-grade tumors. Other surgeons believe that the
infiltrating nature of astrocytomas, in contrast to ependymomas, does not
portend to a radical resection [22,23]. These authors recommend a more
conservative approach for these tumors. We previously reported our favorable
experience with intramedullary astrocytomas in adults [13]. In this report, with a
longer follow-up period, we investigated the role of aggressive surgery and

Jallo 9
avoidance of radiation therapy for these low-grade tumors. This group of
patients was operated upon between the years 1988 to 1994 and the mean follow-
up period was 7.2 years.
In our series we were able to achieve a gross total resection in 71% of
patients. The remaining patients had a subtotal resection that was 80-95% tumor
removal. A biopsy was not performed in any patient. We believe, with
intraoperative neurophysiological monitoring of somatosensory and motor
potentials, that a radical resection of these infiltrative lesions is safely possible.
This surgical adjunct allows the surgeon to remove these infiltrative tumors and
selectively monitor the corticospinal tracts in a precise manner. Intraoperative
motor evoked potentials (MEPs) are an essential surgical adjunct to making
decisions about when to stop surgery for these infiltrative tumors. There is an
incremental decrease in the motor potentials, which guides the extent of tumor
resection [24]. If the MEPs remain present during tumor removal, the surgery
can be safely continued to allow for a total or near total resection, and radiation
therapy can be avoided.
At last follow-up the mean functional grade of all patients alive was 1.7 as
compared to the preoperative grade of 2.4. These results are similar to our
experience with children[12,25] and although there may be immediate worsening
of functional status following surgery, most patients improve or remain the same
as the preoperative status. No patient undergoing surgery deteriorated by more

Jallo 10
than one grade. These long-term results encourage us to continue with our
surgical strategy to these intramedullary tumors.
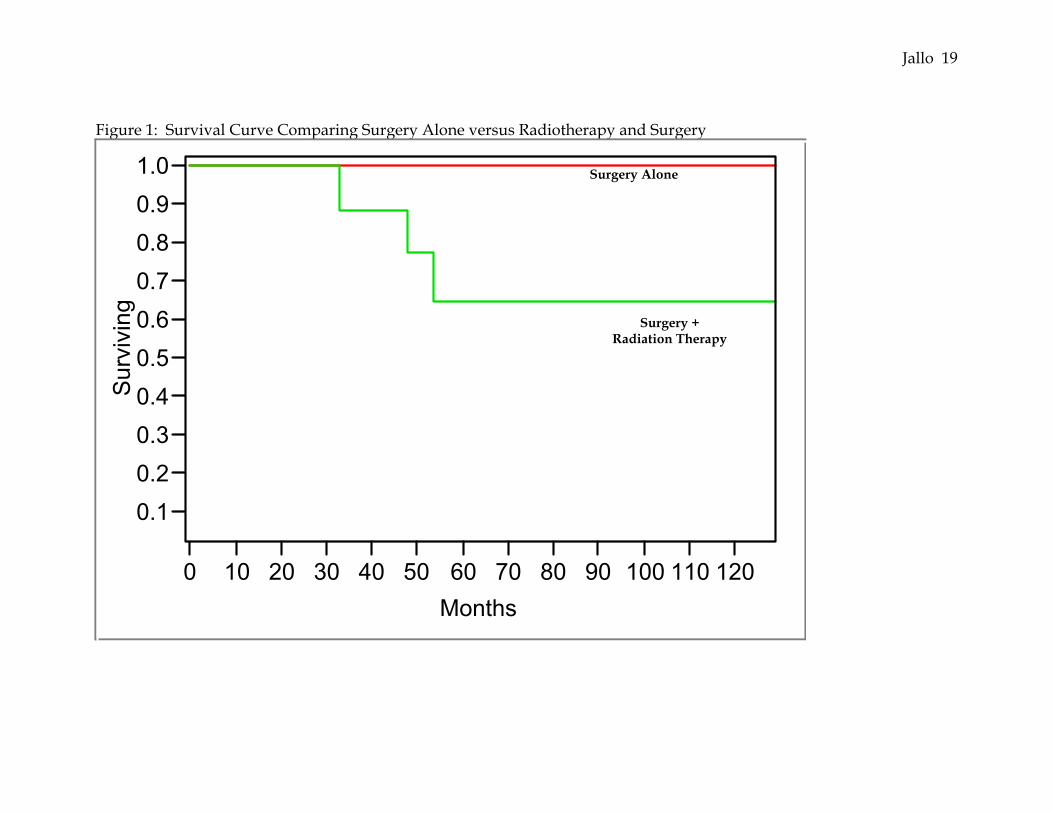
Our series shows that long-term progression-free and overall survival can
be achieved in patients with low-grade astrocytomas through aggressive surgery
alone (see Figure 1). Patients who did not receive radiation therapy faired as
well as those who did. The mean time to death for the three patients was 33.3
months. This progression rate is similar to the patients treated with radiation
therapy alone. Thus patients with low-grade astrocytomas should be followed
closely in the postoperative period for progression, and if no progression occurs
in this initial period the overall survival tends to be excellent. The extent of
resection, both gross total and subtotal resections, was equally efficacious for this
long-term survival. We cannot comment about the role of biopsy for these
tumors since only radical resections were performed. This supports our
aggressive approach for the management of these indolent tumors.
Our study shows a 5-year survival of 82% for patients with low-grade
astrocytoma (see Figure 2). These results are better than the majority of
published papers that advocate a conservative approach with biopsy and
adjuvant radiation therapy. These low-grade tumors possess very little potential
to transform spontaneously into high-grade malignant tumor. Irradiation may
induce a second malignant tumor or radiation myelopathy. Since a radical
resection yields a survival and functional outcome that is comparable to or better
than that achieved with biopsy and radiotherapy, this may be a treatment
Jallo 11
alternative to these tumors. We reserve radiotherapy for patients with
significant residual disease in the conus or when a second reoperation is unlikely
to be attempted.
CONCLUSION
Our experience reinforces our previous results for intramedullary low-
grade astrocytomas. These tumors tend to be indolent and have a favorable
long-term prognosis. Radical surgery alone results in long-term survival for
patients with intramedullary astrocytomas. Intraoperative electrophysiological
monitoring allows for the radical resection of these tumors, which obviates the
need for postoperative radiotherapy. Radiotherapy should be reserved for
progressive disease and tumors which are deemed inoperable.
ACKNOWLEDGEMENTS
This clinical study was supported by a research grant from Medtronic
Sofamar Danek.

Jallo 12
REFERENCES
1. Miller DC: Surgical pathology of intramedullary spinal cord neoplasms. J
Neuro-Oncol 47: 189-194, 2000
2. Minehan KJ, Shaw EG, Scheithauer BW, Davis DL, Onofrio BM: Spinal
cord astrocytoma: pathological and treatment considerations. J Neurosurg
83: 590-595, 1995
3. Linstadt DE, Wara WM, Leibel SA, Gutin PH, Wilson CB, Sheline GE:
Postoperative radiotherapy of primary spinal cord tumors. Int J Radiat
Oncol Biol Phys 16: 1397-1403, 1989
4. Whitaker SJ, Bessel EM, Ashley SE, Bloom HJG, Bell BA, Brada M:
Postoperative radiotherapy in the management of spinal cord
ependymoma. J Neurosurg 74: 720-728, 1991
5. Wood ES, Berne AS, Taveras JM: The value of radiation therapy in the
management of intrinsic tumors of the spinal cord. Radiology 63: 11-24,
1954
6. Chun HC, Schmidt-Ullrich RK, Wolfson A, Tercilla OF, Sagerman RH,
King GA: External beam radiotherapy for primary spinal cord tumors. J
Neuro-Oncol 9: 211-217, 1990
7. Garcia DM: Primary spinal cord tumors treated with surgery and
postoperative irradiation. Radiat Oncol Biol Phys 11: 1933-1939, 1985
Jallo 13
8. Kopelson G, Lingggood RM: Intramedullary spinal cord astrocytoma
versus glioblastoma: the prognostic importance of histologic grade.
Cancer 50: 732-735, 1982
9. Kopelson G, Linggood RM, Kleinman GM, Doucette J, Wang CC:
Management of intramedullary spinal cord tumors. Radiology 135: 473-
479, 1980
10. McLaughlin MP, Buatti JM, Marcus Jr RB, Maria BL, Mickle PJ, Kedar A:
Outcome after radiotherapy of primary spinal cord glial tumors. Rad
Oncol Invest 6: 276-280, 1998
11. Shirato H, Kamada T, Hida K, Koyanagi I, Iwasaki Y, Miyasaka K, Abe H:
The role of radiotherapy in the management of spinal cord glioma. Int J
Radiat Oncol Biol Phys 33: 323-328, 1995
12. Constantini S, Houten J, Miller DC, Freed D, Ozek MM, Rorke LB, Allen
JC, Epstein FJ: Intramedullary spinal cord tumors in children under the
age of 3 years. J Neurosurg 85: 1036-1043, 1996
13. Epstein FJ, Farmer J-P, Freed D: Adult intramedullary astrocytomas of the
spinal cord. J Neurosurg 77: 355-359, 1992
14. Epstein F: Spinal cord astrocytomas of childhood. Prog Exp Tumor Res 30:
135-153, 1987
15. Epstein F, Epstein N: Surgical treatment of spinal cord astrocytomas of
children. J Neurosurg 57: 685-689, 1982
Jallo 14
16. McCormick PC, Torres R, Post KD, Stein B: Intramedullary ependymoma
of the spinal cord. J Neurosurg 72: 523-532, 1990
17. Constantini S, Epstein FJ: Ultrasonic dissection in Neurosurgery. In
Wilkins RH, Rengachary SS (eds): "Neurosurgery." New York: McGraw-
Hill, 1996, 607-608
18. Kaplan EL, Meier P: Nonparametric estimation from incomplete
observations. J Am Stat Assoc 53: 457-481, 1958
19. Isaacson SR: Radiation therapy and the management of intramedullary
spinal cord tumors. J Neuro-Oncol 47: 231-238, 2000
20. Stein BM: Intramedullary spinal cord tumors. Clin Neurosurg 30: 717-741,
1983
21. Stein BM: Surgery of intramedullary spinal cord tumors. Clin Neurosurg
26: 529-542, 1979
22. Cooper PR: Outcome after operative treatment of intramedullary spinal
cord tumors in adults: intermediate and long-term results in 51 patients.
Neurosurgery 25: 855-859, 1989
23. Rossitch E, Jr., Zeidman SM, Burger PC, Curnes JT, Harsh C, Anscher M,
Oakes WJ: Clinical and pathological analysis of spinal cord astrocytomas
in children. Neurosurgery 27: 193-196, 1990
24. Kothbauer K, Deletis V, Epstein FJ: Intraoperative spinal cord monitoring
for intramedullary surgery: an essential adjunct. Pediatr Neurosurg 26:
247-254, 1997
Jallo 15
25. Constantini S, Miller DC, Allen JC, Rorke LB, Freed D, Epstein FJ: Radical
excision of intramedullary spinal cord tumors: surgical morbidity and
long-term follow-up evaluation in 164 children and young adults. J
Neurosurg (Spine) 93: 183-193, 2000
Jallo 16
Table 1: Analysis of Patients with Low-Grade Intramedullary Astrocytoma
Age, Sex Symptom Duration (months)
Location PreOp FunctionalGrade
Last Functional Grade
Radiation Therapy Follow-up (months)
32,F 48 C3-T1 4 Dead Yes 3325,F
11 C1-C5 3 1 Yes 6830,F 24 C3-6 3 2 Yes 4829,F 18 T8-T11 2 1 No 15831,M 28 T8-T9 3 1 No 11038,F 6 C1-C3 2 1 No 8523,M 38 C0-C2 1 Dead Yes 4861,M 5 C6-C7 2 Dead Yes 5431,M 8 C1-C6 2 2 No 7731,M 24 C1-C5 1 1 No 9329,M 27 C2-C3 2 1 No 10831,M 12 T8-T12 4 1 Yes 7633,F 13 C2-C5 2 2 Yes 9922,F 11 C5-T3 4 3 No 8929,F 48 C2-C4 2 3 Yes 13642,F 1 C4-C5 1 2 No 9646,F 18 T5-T9 4 3 Yes 98
Jallo 17
Table 2: Previous Studies Treating Low-Grade Astrocytomas with Radiation Therapy
Series, Year Patients Survival Rate (%) 5-year 10-year
Kopelson and Linnggood, 1982 9 89 89 Garcia et al, 1985 14 60 50 Lindstadt et al, 1989 12 91 91 Chun et al, 1990 16 60 40 Shirato et al, 1995 6 50 50 McLaughlin et al, 1998
8 86 57
Jallo 18
FIGURE LEGEND Figure 1: Survival curve analyzing the role of radiotherapy in patients with low-
grade intramedullary astrocytoma
Figure 2: Kaplan-Meier survival curve for 17 patients with intramedullary
astrocytoma
Jallo 19
Figure 1: Survival Curve Comparing Surgery Alone versus Radiotherapy and Surgery
0.10.20.30.40.50.60.70.80.91.0
Sur
vivi
ng
0 10 20 30 40 50 60 70 80 90 100 110 120Months
Surgery Alone
Surgery + Radiation Therapy
Jallo 20
Figure 2: Kaplan-Meier Survival Curve for 17 Patients with Intramedullary Astrocytoma
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Sur
vivi
ng
0 10 20 30 40 50 60 70 80 90 100 110 120Months

Jallo 21







