
Investigation and evaluation of arterial pulses,
blood pressure, and jugular venous pressure
Dr. András Tislér
October 2013.

Objectives
To understand the principles of…
• Assessing vital signs
• Examination of the peripheral arterial system
– Pulse
– Blood pressure
• Examination of jugular veins

Evaluation and management of the medical patient
• Reason for admission
• History of present illness/current complaints/ review of the systems
• Past medical / social / family history
• Mediactions/allergies
• Physical examination
• Laboratory tests
• Other investigations
• Differential diagnosis
• Confirmatory tests
• Therapy
• Follow up
DIAGNOSIS
Vital signs
• Heart rate / blood pressure
• Temperature
• Respiratory rate / 02 saturation
• Level of consciousness

Evaluating the peripheral pulse
• Palpable? (equal?)
• Heart rate?
• Regular? (rythm)
• Amplitude? contour? compressible?
• Variability?
– Beat-to-beat
– With respiration

Assessment of heart rate
• Rate
• Regularity / rhythm
• Amplitude / contour
• Variation
– Beat-to-beat
– With respiration

Heart rate regularity assessment

Irregular rhythms

Arterial system
Stiff system Elastic system
Pre
ssu
re
Systole Diastole
Mean
pressure
Pre
ssu
re
Systole Diastole
Mean
pressure

Pulse pressure wave reflects from the
periphery, augmenting central pressure

Propagation and reflecion of the pulse wave

Central pulse pressure:
incident (primary) + reflected wave amplitude

Brachial and aorta pressure cirve in a young heathy
(compliant arteries) and an elderly individual (with
stiff arteries)
elderlyyoung

Abnormalities of the arterial pulse wave contour

Examanation of the peripheral arterial system
• Palpable:
– Radial
– Dorsalis pedis/tibial posterior
– Popliteal
– Femoral
• Bruit
– Abdominal
– Femoral
– Carotid

Examanation of the peripheral arterial system
• Inspection
– Paleness
– Cyanosis
– Oedema
– Ulcers
– Emboli
• Palpation:
– Pulse
– Temperature
• Ausculatation
– Bruit

Acute arterial insufficiency in the limb:
Embolus, thrombosis
• „ 5 P-s”
– Pain
– Pallor (pale)
– Pulselessness
– Poikilothermia (coldness)
– Paresthesia

Chronic arterial insufficiency of the lower limb:
• Complain
– Intermittent claudication
• Physical examination
– Limb pale/cyanotic, colder
– Non palpable TP/DP arteries
– Muscle - skin atrophy
– Dependent rubor
– Ulcers
– Gangrene
Blood pressure measurement
• Factors influencing blood pressure
BP= volume x peripheral resistance
– Stroke volume
– Heart rate
– Distensibility of the large arteries
– Peripheral vascular resistance
– Viscosity of the blood

Arterial blood pressure
systolic
Pu
lse
pre
ssu
reMean blood pressure
diastolic

Systolic blood pressure increases towards the periphery:
amplification

Arterial blood pressure
• Systolic pressure
– Increases from the heart towards the periphery (amplification)
• Diastolic pressure
– Remains unchanged toward the periphery
• Pulse pressure
– Difference between the systolic and diastolic pressure
– Increases towards the periphery
• Mean arterial pressure
– Area under the pressure curve
– ~ diastolic + 1/3 pulse pressure
Stephen Hales, 1714

Samuel von Bash (1837-1905)Der Shygmomanometer, Berlin 1887

Riva-Rocci sphagmomanometer
Blood pressure measurement: devices
• Mercury sphygmomanometer
• Aneroid sphygmomanometer
• Automated (oscillometric) devices
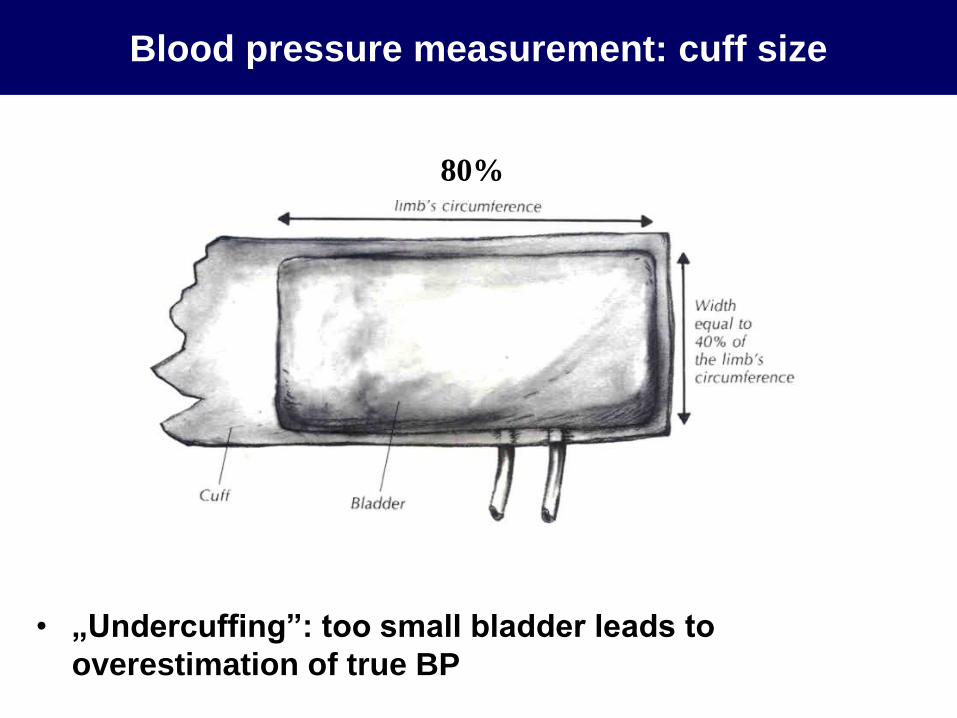
Blood pressure measurement: cuff size
• „Undercuffing”: too small bladder leads to
overestimation of true BP
80%

Blood pressure measurement: methods
• Quiet room
• After 5 minutes of rest
• More than 30 minutes after
meal/coffe/smoking
• Back supported, legs
uncrossed
• Arm supported at heart level
• Deflation rate: 2 mmHg/heart
beat
• Repeat measuremnts x2 or x3

Blood pressure measurement: normal values

Objectives
To understand the principles of…
• Assessing vital signs
• Examination of the peripheral arterial system
– Pulse
– Blood pressure
• Examination of jugular veins

Examination of the internal (external) jugular vein

Examination of the internal (external) jugular vein
• Used mostly to assess extracellular (intravascular) fluid
volume and heart failure
• Jugular vein distension is seen in
– Fluid overload
– tricuspid valve insufficiency
– heart failure (right venticule)
– SVC compression/thrombosis, e.g. mediastinal masses
• Hepato-jugular reflux to assess right ventricular function
– Pressure on the liver increases IJV (EJV) hight that
subsequently decreases
– If not may suggest fluid overload and/or right ventricular
failure

Examination of the internal (external) jugular vein

Examination of the internal (external) jugular vein

External jugular vein distention
Markedly distended right external jugular vein (EJV).
This is the result of elevated central venous pressure (CVP). In practice
the EJV is not as reliable in determining CVP as the internal jugular vein
due to the fact that it sometimes has valves and is not in a direct line with
the right atrium. Pressure on the liver, however, will have similar impact
on the appearance of the IJV as for the EJV. This is referred to as
hepatojugular reflux.

Objectives
To understand the principles of…
• Assessing vital signs
• Examination of the peripheral arterial system
– Pulse
– Blood pressure
• Examination of jugular veins





![Jugular Vein Obstruction Caused by Turning of the Head · The routine use of jugular venous catheterization during the past 10 years [1] has revolutionized treatment of seriously](https://static.documents.pub/doc/80x56/5fd24776808ec6345d62e523/jugular-vein-obstruction-caused-by-turning-of-the-the-routine-use-of-jugular-venous.jpg)

