

1 | FRIDAY, JANUARY 24, 2014 INTERNATIONAL NEW YORK TIMES.
ADVERTISING SUPPLEMENT
Investing in health
KEYNOTE | Craig Williams, director, vaccines and disease of the developing world, GlaxoSmithKline
Why not go both fast and far?
T here is an old African saying that de-clares: ‘‘If you want to go fast, go alone.If you want to go far, go together.’’
It’s been over 10 years since I first heardthis saying, and I still find myself drawn to its in-herent message of collaboration — for its ap-plicability to the underlying challenge facingbusiness, government and nongovernmentalorganizations in addressing the stated devel-opment and health goals of nations. However,this saying seems to reinforce a false dicho-tomy implying that we can’t go fast together. Irefuse to believe that. Together, we can re-move barriers, align and move with command-ing speed toward a collective ambition.
I passionately believe that without moreinnovative and disruptive col-laboration — involving cross-sector partnerships — we willmiss opportunities to radicallyimprove health care infra-structure and save lives. Part-nerships can combine theskills and reach of charities,the efforts of governments,and the knowledge and capa-bilities of business to help im-prove infrastructure and cre-ate prosperity to lift peopleout of poverty for good. This isalso beneficial for business inthe long term, creating a virtu-ous and sustainable cycle ofgrowth and investment.
So new thinking and new partnershipsare key to ensure we do not miss the oppor-tunities to make step-changes to eradicatedisease, improve health care and raise livingstandards in the coming decade. There is arange of opportunities for wider and deepercollaboration and coordination, five of whichcould prove critical to our success.
First: Collaboration that anticipatesand acts. While we must remain vigilant inour fight against some of the developingworld’s most deadly diseases, such as mal-aria, HIV and tuberculosis, the shift in thedisease burden of developing countries to-ward noncommunicable diseases suchas diabetes, hypertension and obesityprovides an opportunity for us to anticipateand act. The key is to act before the dis-eases have had a debilitating effect on theindividuals, families and communities thatserve as the very foundation for economicprosperity. We must work together to sup-port the need for community awareness, onhow we can prevent disease through properplanning and nutrition, andhow to deliver effective andefficient treatment viaprimary care outlets, andresearch and developmentefforts.
Second: Measuringand reporting. Alongsidethe more strategic, longer-term view of the MillenniumDevelopment Goals(MDGs), we need to com-plement the 15-yeartimeline with shorter-term,tangible targets, or mile-stones — for which analigned procedure and me-chanism for reporting willbe critical. With alignmentcomes consistency, andwith consistency comesmomentum. We feel at GSKthat there is a strong casefor integrating financial, economic, socialand environmental data so as to significant-ly improve the ability to understand the typesof advances being made and provide asmarter baseline for measuring progress,making it attractive for nontraditional in-vestors and funders. In addition, more scru-tiny and consistency in how we evaluate sus-tainability, scalability and social value willhelp initiative owners design and implementmore efficient, sustainable and effectiveprograms.
Third: Data for development. Currently,the findings and results from developmentprojects are not routinely made available forexamination. As a result, there is an oppor-tunity to start to analyze what works — andwhat does not — so that it can be enhanced
and scaled appropriately. GSK is currentlysupporting the initiative, spearheaded bythe Center for Health Market Innovations(funded by the Gates Foundation, DFID andothers), to create an authoritative repositoryfor the results of development programs.This open-source-style concept has the po-tential to generate greater insights, as it willlead to better data analysis and better pa-tient coverage. It requires a strong sense ofopenness and cooperation among differentparties to become an effective and powerfultool for calibrating longer-term investmentsand shorter-term aid efforts. Having data isonly one part of the picture — and it likelywon’t be perfect initially. Moreover, the infor-
mation we do have must beused to inform our courage toact and invest, and not lead usinto a state of inaction via‘‘analysis paralysis.’’
Fourth: Political will andcooperation. If we are toachieve the current MDGs, es-pecially by 2015 — as well asset and meet future goals —the strength of political resolveis critical. In the most severelyaffected as well as the mostaffluent nations, both sets ofleaders have different roles toplay and different challengesto overcome. These clusteraround ensuring delivery, polit-
ical integrity and a positive consensus forpublic health and development goals. Theshortage of health workers is one of themost fundamental barriers to improvinghealth in developing countries. A fully trainedand well-supported community health work-er can deliver treatments and provide healtheducation to 5,000 children a year. In 34 ofthe poorest countries in the world, GSK ispartnering with three leading charities —Save the Children, AMREF and Care Interna-tional — to train 10,000 community healthworkers over the next three years. Commit-ment from leaders to invest in health-careinfrastructure remains the key to unlockingquality and long-term impact.
Fifth: Financial will and innovation.More can be done to leverage the privatesector in general, and financial institutions inparticular, to raise investment funds — spe-cifically through using international capitalmarkets and creating new financialproducts. There remains a huge knowledgegap with respect to accessing capital that
helps to build scale at theright speed and size. Thereare some pioneering ex-amples, such as the Inter-national Financial Facilityfor Immunization, which hasraised funds backed bydonor funding for 20 years.Or via organizations thatharness the power and ca-pabilities of impact invest-ment funds (such as theGates Foundation’s GlobalHealth Investment Fund)and private equity firms(e.g., Abraaj) that blend cap-ital from a variety sourcesto achieve scale. We mustwork to connect the innov-ators with investors to helpproperly scale what isalready working.
The world looks very dif-ferent today than it did in 2000. There needsto be mutual learning and collaboration be-tween nations and their development part-ners. There are many examples of success-ful knowledge transfer from poorer to richercountries, and vice versa. Taken together,the combined impact of these initiativescould provide a paradigm shift in not onlyhow we identify, scale and combat dis-eases, but in the health prospects of someof the poorest communities on the planet. Itrequires governments, NGOs and busi-nesses, as well as health-care profession-als, to recognize the benefits of greatertransparency and form new partnerships.
This outcome is one thing that can resultfrom the high-level meetings in Davos thisyear.n
VIEWPOINT | John Beale and Wendy Prosser, VillageReach
Spotlight on a charity that’s teaching companies how to go the extra mile
V illageReach improves health care indeveloping countries by providing crit-ical ‘‘last mile’’ support for health in-
tervention programs. More than 5.2 millionpeople benefit from the organization’s ap-proach and activities in coun-tries like India, Malawi, Nige-ria and Zambia. Here, JohnBeale, strategic develop-ment director, and WendyProsser, program manager,talk about the organization’swork and goals, and involvingcompanies in the process.
What does VillageReachdo?
JB: Our mission is to im-prove health care in develop-ing countries — placeswhere communities are un-derserved in getting healthcare. VillageReach focuses exclusively onrural and more remote communities. Thereare an awful lot of funding partners and ini-tiatives that are vertically oriented. Welooked at that and said, Let’s focus on build-ing support for building health-care capacityin terms of what is actually needed and do-ing things horizontally.
What are VillageReach’s keystrategies?
JB: We have three main strategies. First,building up personnel capacity of the front-line health workers. Second, building under-lying infrastructure — better transport, bet-ter energy supply, better communications.
This is where we bring in the private sector.We’re working to improve health care, but intrying to solve that problem there are manyother challenges, such as these, that are ex-posed. Third, information technology. The
last mile of distribution is thefirst mile of data. With healthcare, there are challenges re-lated to what the populationrequires. Information technol-ogy can help with that. This in-cludes mobile applicationsand software platforms.
VillageReach operates adedicated logistics systemin Mozambique to help deliv-er vaccine to health-careclinics. How does the proj-ect work?
WP: We’re redesigning dis-tribution systems for vaccine.
In this case, the last mile of distribution isfrom the district level to the health-care cen-ters. We’re making it more cost-effective andmore efficient. Now, there is a dedicated logis-tic system for vaccine. And it’s now fully man-aged by the provincial government. The idea isto make the program self-sufficient. Improv-ing the distribution system and making surethe vaccine is available every month is a bigway to help build trust. If a mom walks fivemiles to the health center and there’s no vac-cine, that’s a big trustbuster.
How else does VillageReach build trustin local communities?
JB: In many cases, if there’s a lack of
pharmaceuticals, the health-center person-nel close the center, go and get what’sneeded and then come back. From a trustviewpoint, we need to keep the health-centerworkers in the health-care centers instead ofdoing ad hoc tasks they don’t have time for.
What opportunities does this offer theprivate sector?
WP: This is another market for the privatesector, but there are lots of barriers betweenthe public and private sectors. So we have toshow them both what the benefits are. Forone thing, if corporations invest in healthcare and help improve the quality, they’re go-ing to have a better, healthier work force.
JB: And if they improve energy systemsor infrastructure, for instance, they get bet-ter production, better supply chains and bet-ter transportation systems.
How can you persuade companies toinvest?
JB: We can show companies what’sbeen done. We need to bringthe companies to this and letthem see how they can applytheir own resources. We try tohighlight the degree to whichthey can improve the state ofhealth care. We’re a nonprofit.You would think that a for-profit corporation with moreresources could do even morethan we can. There’s a lot of ef-fort to integrate the privatesector — we simply needmore of it.
WP: Companies are missing opportuni-ties and investments. We need to help theirinnovations get through.
What more needs to be done to makethis possible?
JB: We have to get beyond the regionallevel and pilot programs and scale up. We’dalso like to see large companies investing toimprove the energy system. We own a privateenergy company, VidaGas, which operates ata profit. Originally, it was intended to supplypropane to health-care centers. But onlyabout 15 percent of its delivery goes to theMinistry of Health. The rest goes to privateenterprise. It’s an example of a commerciallyviable company that is socially responsible.We also want to see a bigger wireless foot-print throughout Africa. Communication is vi-tal for health-care improvement.
How can the different organizations in-volved be more effective?
JB: We would like to see much greatertransparency from the organi-zations involved. We would liketo see a much stronger senseof organizations working to-gether. There needs to bemore collaboration. Whatwe’ve done is to try to makeavailable as much of whatwe’ve done and what we haveas possible, and put it online.
And, in the end, we’re all try-ing to work ourselves out ofour jobs.
ARIANE SAINS
Investing in health was produced by the Creative Solutions department and did not involve thenewspaper’s reporting or editorial departments. It was sponsored by GlaxoSmithKline.
Rapid progress in meeting global health challenges can beachieved only by innovation and collaboration
Craig Williams, GSK director,vaccines and disease of thedeveloping world.
John Beale, VillageReach’sstrategic development director.
Wendy Prosser, programmanager, VillageReach.
Clockwise from top left: Health workers in a rural health facility in Mozambique using a propane-powered refrigerator to store vaccines; VillageReach team and premises in Balaka, Malawi; Immunization program inMozambique’s Chiúre district; Mothers and babies from the Kalembo area of Balaka, Malawi.
GS
K
VIL
LAG
EREA
CH VIL
LAG
ER
EAC
H
VIL
LAG
EREA
CH
Taken together,the combined
impact of theseinitiatives could
provide aparadigm shift inhow we identify,
scale and combatdiseases in some
of the poorestcommunities
H istorically, data collection and anal-ysis in developing countries hasbeen difficult — the overall process
can be expensive, while the collected datacan be hard to standardize, quantify andcompare. Yet this is changing, thanks to theopen-source approach employed by devel-opment initiatives like the Washington, D.C.-based Center for Health Market Innovations.Managed by the Results for DevelopmentInstitute, CHMI makes health care more ac-cessible to the poorest communities byidentifying and analyzing health-careprograms on the ground and connectingthem with corporate investors, donors andlocal partners.
Open sourcing and open data allow phi-lanthropists, companies and decisionmakers looking to invest in health care, edu-cation and other sectors in developing coun-tries to make better-informed decisions.‘‘More information ultimately positions youfor success,’’ says Donika Dimovska,project manager at CHMI.
Both open sourcing and crowdsourcingenable broad collection of data that can help
companies invest and find lo-cal partners, and help createscalable models that deliverreal benefits to people in de-veloping countries.
‘‘Many companies usethe data as a pipeline or tofind models to invest in,’’says Dimovska. ‘‘CHMI is ago-to place.’’
Dimovska notes the im-portance of verifying the col-lected data. ‘‘Ensuring qualityis a challenge,’’ she says,adding that CHMI has a thor-ough review process to en-sure data quality and works to ensure thatdata is always updated.
CHMI collates the data, standardizes itand then posts it online. All the informationis publicly available — although Dimovskanotes that while CHMI focuses on healthcare in developing countries, it neither col-lects nor publicizes medical records or otherpersonal information.
The CHMI database is also a starting
point for companies thatwant to invest but don’t knowwhere or how to begin. ‘‘Wethink of ourselves as a con-nector,’’ Dimovska says,‘‘helping to establish a link-age.’’ She notes that the datamust be useful, regardless ofwhether it relates to healthcare, education or infrastruc-ture, and that useful meansdifferent things depending onwho is using the data. Sheadds that those providingdata also need to see theconcrete benefits of doing so.
Dimovska sees clear applications foropen sourcing far beyond health care. Build-ing on CHMI’s success, Results for Develop-ment launched the Center for Education In-novations to increase access to good,affordable education for all.
CEI has programs in, among otherplaces, South Africa, China and Kenya.These range from providing desksfor schoolchildren to helping establish
kindergartens and early childhood develop-ment centers. ‘‘We believe the CHMI modelis very applicable,’’ Dimovska says. CHMI isalso looking at replicating its model in agri-culture, water and sanitationas well as climate change andthe environment.
Started in 2010, CHMI isfunded by the Bill & MelindaGates Foundation, the Rocke-feller Foundation and UKaid,which is under the auspices ofthe U.K. government’s Department for Inter-national Development.
In 2013, CHMI saw a number of emerg-ing trends in financing health care in devel-oping countries and about 40 models thathave expanded and are scaling up to createreal impact. CHMI’s analysis indicates thatnetworks and franchising are among thebiggest trends. The latter includes providingprimary care through franchising, includingmobile primary care.
Governments are also coming on board,working in public-private partnerships asthey haven't before, she says. ‘‘Many
governments are working with privatecompanies and nonprofits to extend healthcare access through innovative businesspartnerships,’’ says Dimovska. ‘‘CHMI
works through local partnersin countries including India,Kenya, Nigeria, Pakistan andthe Philippines. These part-ners identify and connecthealth innovators to potentialpartners such as investors,academic evaluators and new
business collaborators.’’New technologies are key to making
open sourcing, data collection and theprojects that emerge from them work, sheadds. For instance, in parts of Asia andIndia, she says, ‘‘mobile phones are incred-ibly important,’’ because information canquickly and easily be sent to everyone frompregnant women to people with medicalconditions that need to be monitored.
Better supply chains to deliver medicine
to remote communities are another ex-ample of improving technology, she says,making it easier to put a project into action.Improved logistics mean that medicines canbe delivered more affordably.
CHMI is considering launching a mobileapplication to more easily collect data fromtablets and smartphones as people be-come more mobile and move away fromtheir computers.
In five years, CHMI would like its data-base to be more self-sustaining in terms ofcontribution and use. This would translate in-to lower funding costs and improvedsustainability.
Because open sourcing and the technol-ogies it uses are relatively new, Dimovskanotes that it’s important to follow up onwhat comes out of partnerships and howmodels are being developed and enlarged.‘‘It goes without saying that we want to seeimpact,’’ she says.
ARIANE SAINS
CHMI Project Manager DonikaDimovska.
OPEN SOURCING | Center for Health Market Innovations
How big data is transforming the fight against diseases in the developing world
‘We believethe CHMI
model is veryapplicable’
RES
ULT
SFO
RD
EVEL
OP
MEN
TIN
STI
TUTE
ADVERTISING SUPPLEMENT FRIDAY, JANUARY 24, 2014 | 2INTERNATIONAL NEW YORK TIMES.
INNOVATIVE INVESTING | Christopher Egerton-Warburton and Labeeb M. Abboud, Global Health Investment Fund managers, Lion’s Head Global Partners
Social impact fund backs late-stage global health innovations
U nder the sponsorship of the Bill &Melinda Gates Foundation, in partner-ship with Grand Challenges Canada, a
private fund has been launched to bring a newsource of capital for innovation in the area ofnew devices, diagnostic drugs and vaccinesfor global health diseases.
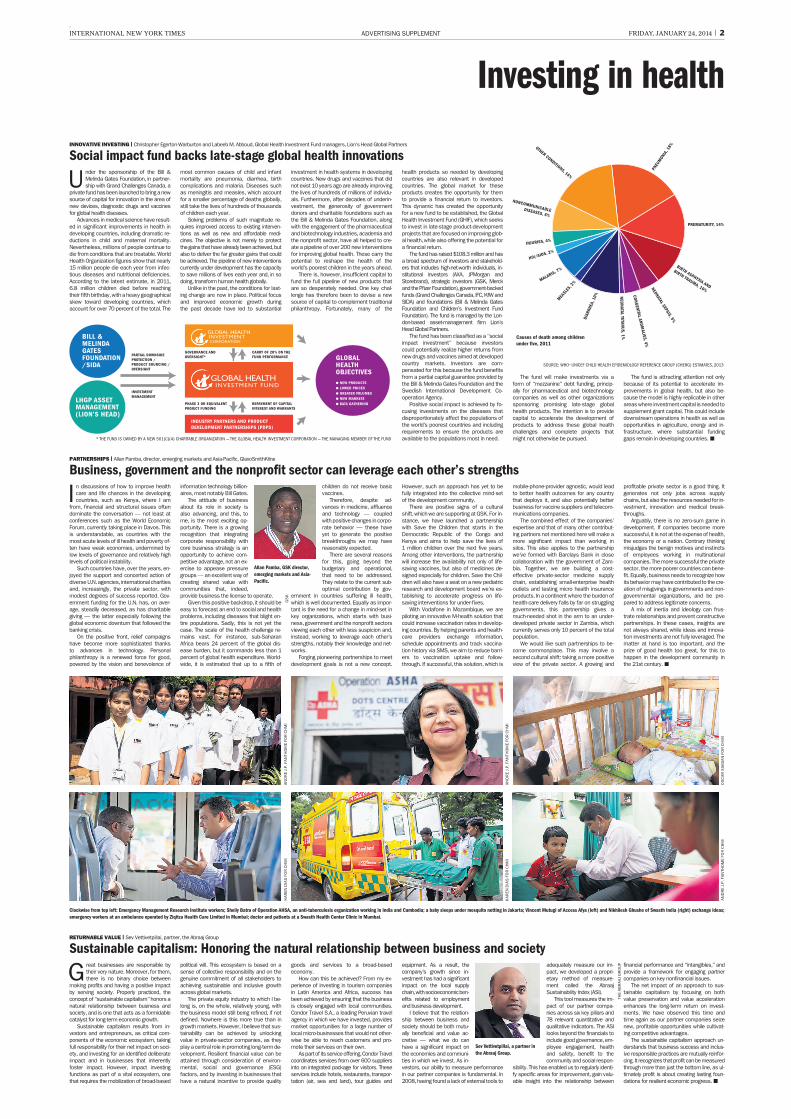
Advances in medical science have result-ed in significant improvements in health indeveloping countries, including dramatic re-ductions in child and maternal mortality.Nevertheless, millions of people continue todie from conditions that are treatable. WorldHealth Organization figures show that nearly15 million people die each year from infec-tious diseases and nutritional deficiencies.According to the latest estimate, in 2011,6.8 million children died before reachingtheir fifth birthday, with a heavy geographicalskew toward developing countries, whichaccount for over 70 percent of the total. The
most common causes of child and infantmortality are pneumonia, diarrhea, birthcomplications and malaria. Diseases suchas meningitis and measles, which accountfor a smaller percentage of deaths globally,still take the lives of hundreds of thousandsof children each year.
Solving problems of such magnitude re-quires improved access to existing interven-tions as well as new and affordable medi-cines. The objective is not merely to protectthe gains that have already been achieved, butalso to deliver the far greater gains that couldbe achieved. The pipeline of new interventionscurrently under development has the capacityto save millions of lives each year and, in sodoing, transform human health globally.
Unlike in the past, the conditions for last-ing change are now in place. Political focusand improved economic growth duringthe past decade have led to substantial
investment in health systems in developingcountries. New drugs and vaccines that didnot exist 10 years ago are already improvingthe lives of hundreds of millions of individu-als. Furthermore, after decades of underin-vestment, the generosity of governmentdonors and charitable foundations such asthe Bill & Melinda Gates Foundation, alongwith the engagement of the pharmaceuticaland biotechnology industries, academia andthe nonprofit sector, have all helped to cre-ate a pipeline of over 200 new interventionsfor improving global health. These carry thepotential to reshape the health of theworld’s poorest children in the years ahead.
There is, however, insufficient capital tofund the full pipeline of new products thatare so desperately needed. One key chal-lenge has therefore been to devise a newsource of capital to complement traditionalphilanthropy. Fortunately, many of the
health products so needed by developingcountries are also relevant in developedcountries. The global market for theseproducts creates the opportunity for themto provide a financial return to investors.This dynamic has created the opportunityfor a new fund to be established, the GlobalHealth Investment Fund (GHIF), which seeksto invest in late-stage product-developmentprojects that are focused on improving glob-al health, while also offering the potential fora financial return.
The fund has raised $108.3 million and hasa broad spectrum of investors and stakehold-ers that includes high-net-worth individuals, in-stitutional investors (AXA, JPMorgan andStorebrand), strategic investors (GSK, Merckand the Pfizer Foundation), government-backedfunds (Grand Challenges Canada, IFC, KfW andSIDA) and foundations (Bill & Melinda GatesFoundation and Children’s Investment FundFoundation). The fund is managed by the Lon-don-based asset-management firm Lion’sHead Global Partners.
The fund has been classified as a ‘‘socialimpact investment’’ because investorscould potentially realize higher returns fromnew drugs and vaccines aimed at developedcountry markets. Investors are com-pensated for this because the fund benefitsfrom a partial capital guarantee provided bythe Bill & Melinda Gates Foundation and theSwedish International Development Co-operation Agency.
Positive social impact is achieved by fo-cusing investments on the diseases thatdisproportionately affect the populations ofthe world’s poorest countries and includingrequirements to ensure the products areavailable to the populations most in need.
The fund will make investments via aform of ‘‘mezzanine’’ debt funding, princip-ally for pharmaceutical and biotechnologycompanies as well as other organizationssponsoring promising late-stage globalhealth products. The intention is to providecapital to accelerate the development ofproducts to address these global healthchallenges and complete projects thatmight not otherwise be pursued.
The fund is attracting attention not onlybecause of its potential to accelerate im-provements in global health, but also be-cause the model is highly replicable in otherareas where investment capital is needed tosupplement grant capital. This could includedownstream operations in health as well asopportunities in agriculture, energy and in-frastructure, where substantial fundinggaps remain in developing countries.n
G reat businesses are responsible bytheir very nature. Moreover, for them,there is no binary choice between
making profits and having a positive impactby serving society. Properly practiced, theconcept of ‘‘sustainable capitalism’’ honors anatural relationship between business andsociety, and is one that acts as a formidablecatalyst for long-term economic growth.
Sustainable capitalism results from in-vestors and entrepreneurs, as critical com-ponents of the economic ecosystem, takingfull responsibility for their net impact on soci-ety, and investing for an identified deliberateimpact and in businesses that inherentlyfoster impact. However, impact investingfunctions as part of a vital ecosystem, onethat requires the mobilization of broad-based
political will. This ecosystem is based on asense of collective responsibility and on thegenuine commitment of all stakeholders toachieving sustainable and inclusive growthacross global markets.
The private equity industry to which I be-long is, on the whole, relatively young, withthe business model still being refined, if notdefined. Nowhere is this more true than ingrowth markets. However, I believe that sus-tainability can be achieved by unlockingvalue in private-sector companies, as theyplay a central role in promoting long-term de-velopment. Resilient financial value can beattained through consideration of environ-mental, social and governance (ESG)factors, and by investing in businesses thathave a natural incentive to provide quality
goods and services to a broad-basedeconomy.
How can this be achieved? From my ex-perience of investing in tourism companiesin Latin America and Africa, success hasbeen achieved by ensuring that the businessis closely engaged with local communities.Condor Travel S.A., a leading Peruvian travelagency in which we have invested, providesmarket opportunities for a large number oflocal micro-businesses that would not other-wise be able to reach customers and pro-mote their services on their own.
As part of its service offering, Condor Travelcoordinates services from over 600 suppliersinto an integrated package for visitors. Theseservices include hotels, restaurants, transpor-tation (air, sea and land), tour guides and
equipment. As a result, thecompany’s growth since in-vestment has had a significantimpact on the local supplychain, with socioeconomic ben-efits related to employmentand business development.
I believe that the relation-ship between business andsociety should be both mutu-ally beneficial and value ac-cretive — what we do canhave a significant impact onthe economies and communi-ties in which we invest. As in-vestors, our ability to measure performancein our partner companies is fundamental. In2008, having found a lack of external tools to
adequately measure our im-pact, we developed a propri-etary method of measure-ment called the AbraajSustainability Index (ASI).
This tool measures the im-pact of our partner compa-nies across six key pillars and78 relevant quantitative andqualitative indicators. The ASIlooks beyond the financials toinclude good governance, em-ployee engagement, healthand safety, benefit to thecommunity and social respon-
sibility. This has enabled us to regularly identi-fy specific areas for improvement, gain valu-able insight into the relationship between
financial performance and ‘‘intangibles,’’ andprovide a framework for engaging partnercompanies on key nonfinancial issues.
The net impact of an approach to sus-tainable capitalism by focusing on bothvalue preservation and value accelerationenhances the long-term return on invest-ments. We have observed this time andtime again as our partner companies seizenew, profitable opportunities while cultivat-ing competitive advantages.
The sustainable capitalism approach un-derstands that business success and inclus-ive responsible practices are mutually reinfor-cing. It recognizes that profit can be measuredthrough more than just the bottom line, as ul-timately profit is about creating lasting foun-dations for resilient economic progress.n
Sev Vettivetpillai, a partner inthe Abraaj Group.
Investing in health
RETURNABLE VALUE | Sev Vettivetpillai, partner, the Abraaj Group
Sustainable capitalism: Honoring the natural relationship between business and society
Clockwise from top left: Emergency Management Research Institute workers; Shelly Batra of Operation AHSA, an anti-tuberculosis organization working in India and Cambodia; a baby sleeps under mosquito netting in Jakarta; Vincent Mutugi of Access Afya (left) and Nikhilesh Ghushe of Swasth India (right) exchange ideas;emergency workers at an ambulance operated by Ziqitza Health Care Limited in Mumbai; doctor and patients at a Swasth Health Center Clinic in Mumbai.
THE
AB
RA
AJ
GR
OU
P
AN
DR
EJ.
P.F
AN
THO
ME
FOR
CH
MI
* THE FUND IS OWNED BY A NEW 501(C)(4) CHARITABLE ORGANIZATION — THE GLOBAL HEALTH INVESTMENT CORPORATION — THE MANAGING MEMBER OF THE FUND
PARTIAL DOWNSIDEPROTECTION /PRODUCT SOURCING /OVERSIGHT
INVESTMENTMANAGEMENT
CARRY OF 20% ON THEFUND PERFORMANCE
REPAYMENT OF CAPITALINTEREST AND WARRANTS
GOVERNANCE ANDOVERSIGHT*
PHASE 3 OR EQUIVALENTPROJECT FUNDING
BILL &MELINDAGATESFOUNDATION/SIDA
LHGP ASSETMANAGEMENT(LION’S HEAD)
GLOBALHEALTHOBJECTIVES� NEW PRODUCTS� LOWER PRICES� GREATER VOLUMES� NEW MARKETS� DATA GATHERING
INDUSTRY PARTNERS AND PRODUCTDEVELOPMENT PARTNERSHIPS (PDPS)
GLOBAL HEALTHINVESTMENTCORPORATION
GLOBAL HEALTHINVESTMENT FUND
I n discussions of how to improve healthcare and life chances in the developingcountries, such as Kenya, where I am
from, financial and structural issues oftendominate the conversation — not least atconferences such as the World EconomicForum, currently taking place in Davos. Thisis understandable, as countries with themost acute levels of ill health and poverty of-ten have weak economies, undermined bylow levels of governance and relatively highlevels of political instability.
Such countries have, over the years, en-joyed the support and concerted action ofdiverse U.N. agencies, international charitiesand, increasingly, the private sector, withmodest degrees of success reported. Gov-ernment funding for the U.N. has, on aver-age, steadily decreased, as has charitablegiving — the latter especially following theglobal economic downturn that followed thebanking crisis.
On the positive front, relief campaignshave become more sophisticated thanksto advances in technology. Personalphilanthropy is a renewed force for good,powered by the vision and benevolence of
information technology billion-aires, most notably Bill Gates.
The attitude of businessabout its role in society isalso advancing, and this, tome, is the most exciting op-portunity. There is a growingrecognition that integratingcorporate responsibility withcore business strategy is anopportunity to achieve com-petitive advantage, not an ex-ercise to appease pressuregroups — an excellent way ofcreating shared value withcommunities that, indeed,provide business the license to operate.
Given this positive backdrop, it should beeasy to forecast an end to social and healthproblems, including diseases that blight en-tire populations. Sadly, this is not yet thecase. The scale of the health challenge re-mains vast. For instance, sub-SaharanAfrica bears 24 percent of the global dis-ease burden, but it commands less than 1percent of global health expenditure. World-wide, it is estimated that up to a fifth of
children do not receive basicvaccines.
Therefore, despite ad-vances in medicine, affluenceand technology — coupledwith positive changes in corpo-rate behavior — these haveyet to generate the positivebreakthroughs we may havereasonably expected.
There are several reasonsfor this, going beyond thebudgetary and operational,that need to be addressed.They relate to the current sub-optimal contribution by gov-
ernment in countries suffering ill health,which is well documented. Equally as impor-tant is the need for a change in mind-set inkey organizations, which starts with busi-ness, government and the nonprofit sectorsviewing each other with less suspicion and,instead, working to leverage each other’sstrengths, notably their knowledge and net-works.
Forging pioneering partnerships to meetdevelopment goals is not a new concept.
However, such an approach has yet to befully integrated into the collective mind-setof the development community.
There are positive signs of a culturalshift, which we are supporting at GSK. For in-stance, we have launched a partnershipwith Save the Children that starts in theDemocratic Republic of the Congo andKenya and aims to help save the lives of1 million children over the next five years.Among other interventions, the partnershipwill increase the availability not only of life-saving vaccines, but also of medicines de-signed especially for children. Save the Chil-dren will also have a seat on a new pediatricresearch and development board we’re es-tablishing to accelerate progress on life-saving interventions for under-fives.
With Vodafone in Mozambique, we arepiloting an innovative M-health solution thatcould increase vaccination rates in develop-ing countries. By helping parents and health-care providers exchange information,schedule appointments and track vaccina-tion history via SMS, we aim to reduce barri-ers to vaccination uptake and follow-through. If successful, this solution, which is
mobile-phone-provider agnostic, would leadto better health outcomes for any countrythat deploys it, and also potentially betterbusiness for vaccine suppliers and telecom-munications companies.
The combined effect of the companies’expertise and that of many other contribut-ing partners not mentioned here will make amore significant impact than working insilos. This also applies to the partnershipwe’ve formed with Barclays Bank in closecollaboration with the government of Zam-bia. Together, we are building a cost-effective private-sector medicine supplychain, establishing small-enterprise healthoutlets and testing micro health insuranceproducts. In a continent where the burden ofhealth-care delivery falls by far on strugglinggovernments, this partnership gives amuch-needed shot in the arm to an under-developed private sector in Zambia, whichcurrently serves only 10 percent of the totalpopulation.
We would like such partnerships to be-come commonplace. This may involve asecond cultural shift: taking a more positiveview of the private sector. A growing and
profitable private sector is a good thing. Itgenerates not only jobs across supplychains, but also the resources needed for in-vestment, innovation and medical break-throughs.
Arguably, there is no zero-sum game indevelopment. If companies become moresuccessful, it is not at the expense of health,the economy or a nation. Contrary thinkingmisjudges the benign motives and instinctsof employees working in multinationalcompanies. The more successful the privatesector, the more poorer countries can bene-fit. Equally, business needs to recognize howits behavior may have contributed to the cre-ation of misgivings in governments and non-governmental organizations, and be pre-pared to address legitimate concerns.
A mix of inertia and ideology can frus-trate relationships and prevent constructivepartnerships. In these cases, insights arenot always shared, while ideas and innova-tion investments are not fully leveraged. Thematter at hand is too important, and theprize of good health too great, for this tohappen in the development community inthe 21st century.n
GS
K
Allan Pamba, GSK director,emerging markets and Asia-Pacific.
PARTNERSHIPS | Allan Pamba, director, emerging markets and Asia-Pacific, GlaxoSmithKline
Business, government and the nonprofit sector can leverage each other’s strengths
SOURCE: WHO�UNICEF CHILD HEALTH EPIDEMIOLOGY REFERENCE GROUP (CHERG) ESTIMATES, 2013
Causes of death among childrenunder five, 2011
AN
DR
EJ.
P.F
AN
THO
ME
FOR
CH
MI
OS
CA
RS
IAG
IAN
FOR
CH
MI
AN
DR
EJ.
P.F
AN
THO
ME
FOR
CH
MI
KA
REN
DIA
SFO
RC
HM
I
KA
REN
DIA
SFO
RC
HM
I







