
LA RADIOTERAPIA DEL
CARCINOMA DEL PANCREAS
Paolo AntognoniPaolo AntognoniU.O. RADIOTERAPIA
Ospedale di Circolo e Fondazione MacchiVARESE
Nadia Di Muzio Nadia Di Muzio U.O. RADIOTERAPIA
IRCCS Ospedale San RaffaeleMILANO

ROLE OF RADIATION THERAPY IN THE MANAGEMENT OF PANCREATIC CANCER:
NEW CHALLENGES FOR AN OLD PARADIGM
• Literature Review and Clinical Controversial Issues(P. Antognoni)
• Advances in Radiation Therapy Techniques and The Contribution of Novel Technologies
(N. Di Muzio)
LA RADIOTERAPIA DEL
CARCINOMA DEL PANCREAS

RADIOTHERAPY IN THE MANAGEMENT RADIOTHERAPY IN THE MANAGEMENT
OF PANCREATIC CANCER OF PANCREATIC CANCER
BACKGROUND
5-year overall survival for all stages combined: 5%
Only mild improvement of trend in 5-yr relative survival rates (U.S. data): from 3% (1975-1986) to 6% (1999-2005)
At autopsy 30% of pts died with locally destructive pancreatic cancer: local failure is still a major cause of death and a main component of disease progression
The incorporation of systemic chemotherapy into the management of this disease is standard of care at all stages
The role of radiation therapy is less clear and represents a still controversial issue
J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137

• Adjuvant CHT-RT for resectable disease
• Neoadjuvant CHT-RT forresectable/borderline resectable disease
• “Radical” RT±CHT for locally advancedunresectable pancreatic cancer (LAPC)
• Palliative RT±CHT for LAPC
• RT for isolated local recurrence
J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137 RADIOTHERAPY IN THE MANAGEMENT RADIOTHERAPY IN THE MANAGEMENT
OF PANCREATIC CANCER OF PANCREATIC CANCER SEVERAL CLINICAL SETTINGS (MOSTLY IN
CONJUNCTION WITH CHEMOTHERAPY)

J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137
RADIOTHERAPY IN THE MANAGEMENT OF PANCREATIC CANCER
ADJUVANT CHT-RT: RANDOMIZED TRIALS(RCT)
The largest RCT
Established adjuvant CHT-RT as new
standard of resectable PC in the US:
the highest median survival
Survival detriment in
CHT-RT arm
Trend for surv. benefit
PARADOXICAL RESULTS IN TERMS OF SURVIVAL IMPROVEMENT WITH ADJUVANT CHEMO-RT!

• The GITSG, EORTC and ESPAC-1 studies utilized what isnow known to be an inferior radiation treatment schedule, asit is now believed that the treatment break in split-courseschedules allows for tumor repopulation and subsequentlypoorer outcomes
• These studies also failed to include quality assurance for the radiation treatments, a factor we now know to be associatedwith treatment deviations and poorer outcomes in numerousdisease sites including pancreatic cancer
• Finally, the radiation delivered in these trials utilizedsignificantly larger fields and target volumes than are currently used (more toxicity).
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER
ADJUVANT CHT-RT: CRITICISM OF RCT

J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137 RADIOTHERAPY IN THE MANAGEMENT OF PANCREATIC CANCER
ADJUVANT CHT-RT: NON-RANDOMIZED TRIALS
SOME ADDITIONAL BENEFIT TO THE POTENTIAL BENEFIT OF ADJUVANT CHEMO-RT (45-50.4 Gy continuous course)
1.092 PTS

• To avoid delays in adjuvant therapies by administering treatment before surgery
• Higher chances of delivering full-dose chemo and/or RT
• Avoid major surgery in pts who show local/systemic PD duringneoadjuvant treatment
• Potential downstaging of borderline resectable disease and increased rate of R0 resection
• Preoperatve treatment less toxic (less small bowel inside RT fields, higher tumor oxygenation and increased drug delivery than in postoperative setting)
RADIOTHERAPY IN THE MANAGEMENT OF PANCREATIC CANCER
RATIONALE OF NEOADJUVANT CHT-RT
J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137
NEOADJUVANTNEOADJUVANT APPROACH MAY BE APPROACH MAY BE BENEFICIALBENEFICIAL FOR A SUBSET OF THE FOR A SUBSET OF THE
PATIENT POPULATION, AND PARTICULARLY PATIENT POPULATION, AND PARTICULARLY FOR THOSE WITH BORDERLINE FOR THOSE WITH BORDERLINE
RESECTABLE DISEASE:RESECTABLE DISEASE: BUT THER ARE NO RANDOMIZED STUDIES!BUT THER ARE NO RANDOMIZED STUDIES!

J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER NEOADJUVANT CHT-RT: the MDACC Phase II Trials of
Preoperative Concurrent Chemo-RT for resectable PC
First phase II trials of neoadjuvant 5FU-based chemoRT ± IORT (1992-
2006)
Rapid-fractionation preoperative chemoRT: promising results in
resectable pts (3-yr OS: 23%)
No advantages to paclitaxel-based preoperative treatment

J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137 RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER NEOADJUVANT CHT-RT: NON-RCT FOR
BORDERLINE RESECTABLE PC
33%-64% of pts with borderline resectable cancers underwent surgical resection
Rate of R0 resections: 87%-100%
Small numbers of pts, but good potential for down staging of borderline resectabletumors to achieve R0 resection with CHT+RT tot. doses of 45-56 Gy or equivalent.
2001-2011 selected non-randomized trials

RADIOTHERAPY IN THE MANAGEMENT OF PANCREATIC CANCER
ONGOING AND RECENTLY COMPLETED
ADJUVANT/NEOADJUVANT TRIALS (CHT± RT)
Subset analyses of RTOG 0848 may provide additional
data that may help stratify patients who could benefit
from adjuvant radiation, leading to more personalized
treatment regimens;
NEED OF PERSONALIZED TREATMENT REGIMENS!

RADIOTHERAPY IN THE MANAGEMENT OF PANCREATIC CANCER
ADJUVANT RT: ONGOING Phase III RTOG 0848 TRIAL EVALUATING BOTH ERLOTINIB AND CHEMO-RT
RTOG 0848 will provide additional prospective randomized
data to help clarify whether adjuvant radiation adds benefit to
patients undergoing pancreaticoduodenectomy
• Adjuvant and Neoadjuvant chemoRT regimens usually
demand daily RT treatment for 5-6 wks, a significantburden on pts with life expectancies typically <1yr
• Neoadjuvant therapy can delay the only potentiallycurative procedure for pts with resectable lesions
J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137 RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER ADJUVANT & NEOADJUVANT CHEMO-RT:
Drawbacks
Potential for “short-course” chemoRT like those experimentedin the MDACC trials, but with more effective radiations: the case for Neoadjuvant Hypofractionated Proton Therapy!

A proton radiotherapy schedule consisting of 5 fraction of 5 CGE as part of neoadjuvant therapyfor adenocarcinoma of the pancreas seems
dosimetrically feasible, providing excellent
target volume coverage, dose homogeneity, and normal tissue sparing.
Hypofractionated Proton Radiotherapy in thissetting merits Phase I clinical trial investigation.
2007 dosimetric study
2011 Phase I study
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER NEOADJUVANT RT: Short-course Proton Therapy (PRT)
Neoadjuv. short-course PRT+Capecitabine is feasible:
a phase II study is underway
R0 resection rate: 82%
15 pts, with localized
resectable PC of the head
Preoperative chemoRT with1wk PRT+Capecitabinefollowed by early surgery (1-3 wks)
J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137
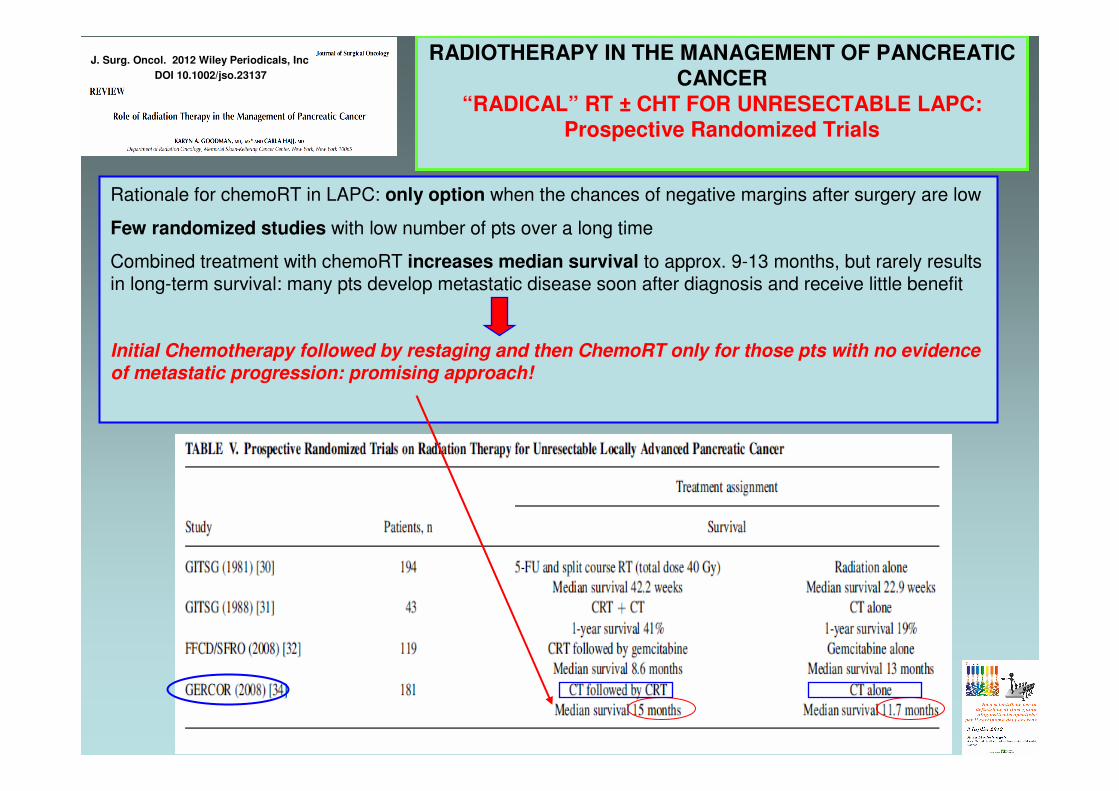
RADIOTHERAPY IN THE MANAGEMENT OF PANCREATIC
CANCER
“RADICAL” RT ± CHT FOR UNRESECTABLE LAPC:
Prospective Randomized Trials
Rationale for chemoRT in LAPC: only option when the chances of negative margins after surgery are low
Few randomized studies with low number of pts over a long time
Combined treatment with chemoRT increases median survival to approx. 9-13 months, but rarely resultsin long-term survival: many pts develop metastatic disease soon after diagnosis and receive little benefit
Initial Chemotherapy followed by restaging and then ChemoRT only for those pts with no evidenceof metastatic progression: promising approach!

J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137
RADIOTHERAPY IN THE MANAGEMENT OF PANCREATIC CANCER
BRACHYTHERAPY & IORT FOR LAPC
•• IntraoperativeIntraoperative BrachyBrachy (I(I--125, AU125, AU--198, Pd198, Pd--103):103): manysmall studies, low median survivals (7-15 wks), LC in the range of 65%, but…”complication rates felt to beunacceptably high”!
•• IORT: IORT: no clear survival benefit added by IORT in the setting of resectable PC. In the US it is still used in ptswith unresectable disease without demonstrated benefitsin survival or disease-free progression.
VERY LIMITED INDICATIONS IN THE ERA OF HIGHVERY LIMITED INDICATIONS IN THE ERA OF HIGH--DOSE DOSE
CONFORMAL STEREOTACTIC BODY RT AND IGCONFORMAL STEREOTACTIC BODY RT AND IG--IMRT! IMRT!

RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER
PALLIATIVE IRRADIATION OF LAPC
J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137
• In the palliative setting the median survival time is notsignificantly affected by a higher RT dose
• Compared with higher doses given over 5-6 wks, chemoRT (30 Gy/10 fract./2 wks + concurrent infusion5FU) results in similar median survival and local disease-progression rates
• Higher RT doses can lead to increased acute treatment-related morbidity
RECOMMENDED SCHEDULE:
30 Gy in 10 fractions + i.v. 5FU
• Chemoradiotherapy (3DCRT: 45 Gy in 25 fractions of 1.8 Gy/day + 5FU) is feasibleand may be an effective treatment optionalso in those patients who present withisolated local metastasis after primarysurgery for pancreatic cancer.
Wilkowski R, Thoma M, Bruns C, et al.: Combined chemoradiotherapy for isolated
local recurrence after primary resection of pancreatic cancer. JOP 2006;7:34–40.
RADIOTHERAPY IN THE MANAGEMENT OF PANCREATIC CANCER
RT FOR ISOLATED LOCAL RECURRENCE
J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137

J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137 RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER
“RADICAL” STEREOTACTIC BODY RT (SBRT) FOR LAPC
SEVERAL TRIALS BUT NO
ESTABLISHED STANDARD FOR SBRT
DOSE/FRACTIONATION FOR LAPC.
MORE COMMON RANGE: 25 Gy single
fraction / 45 Gy in 3 fract. DOSE-RESPONSE EFFECT AND INCREASED LOCAL CONTROL
RIGOROUS QUALITY CONTROL TO MINIMIZE TOXICITY to OARs: (duodenum and stomach)
J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137 RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER
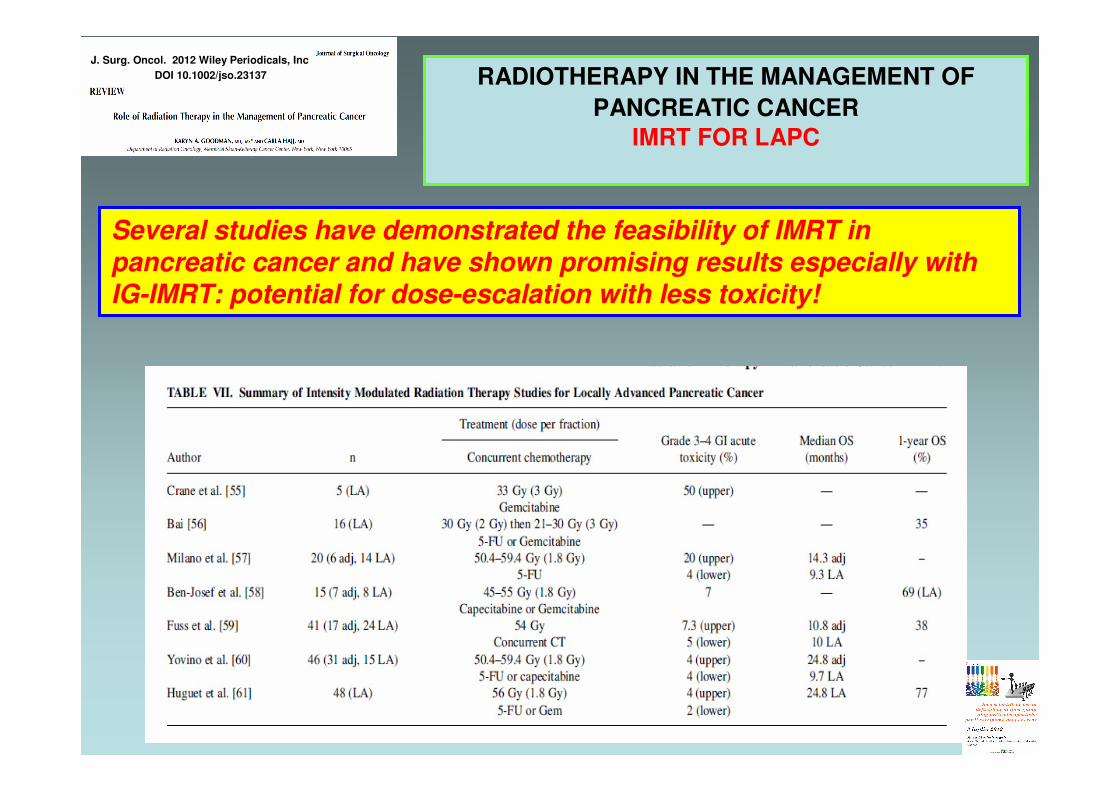
IMRT FOR LAPC
Several studies have demonstrated the feasibility of IMRT in pancreatic cancer and have shown promising results especially withIG-IMRT: potential for dose-escalation with less toxicity!
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCERNEW RESEARCH STRATEGIES AND REMAINING
CHALLENGES WITH RADIATION THERAPY
Pancreatic cancer is in general a tumour with a large stromal component and therefore less likelyto shrink radiologically, despite a possibleresponse from cancer cells. Functional imaging may be more appropriate tomeasure response for LAPC.
A major methodological flaw of preoperativechemoRT studies is that none of them israndomized and they all report the results ofthe subset of patients who actuallyunderwent a resection, rather then reportingby intention to treat
Despite the aforementioned methodological shortcomings,
literature appears to indicate that preoperative chemoRT in
borderline resectable and presumably also primarily resectablepancreatic cancer may improve resection rate, R0 resection rate
and possibly overall survival.This hypothesis is valid and should be tested in randomizedprospective studies.
• Conflicting results from randomized studies• No general standard of care• Optimal treatment both curative and palliative is complex and needs a
multidisciplinary team• Adjuvant and Neoadjuvant treatments in pts with resectable PC need
more prospective trials• Newer RT techniques may increase the therapeutic benefit by higher RT
doses that may improve local control• Need of further studies focusing on the molecular pathways involved in
the carcinogenesis and progression of this disease• Molecular markers will begin to be used routinely as prognosticators and
may guide personalized therapeutic decisions
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER
CONCLUSION FROM THE LITERATURE ANALYSIS ON
THE ROLE OF RADIATION THERAPY
J. Surg. Oncol. 2012 Wiley Periodicals, Inc
DOI 10.1002/jso.23137
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER
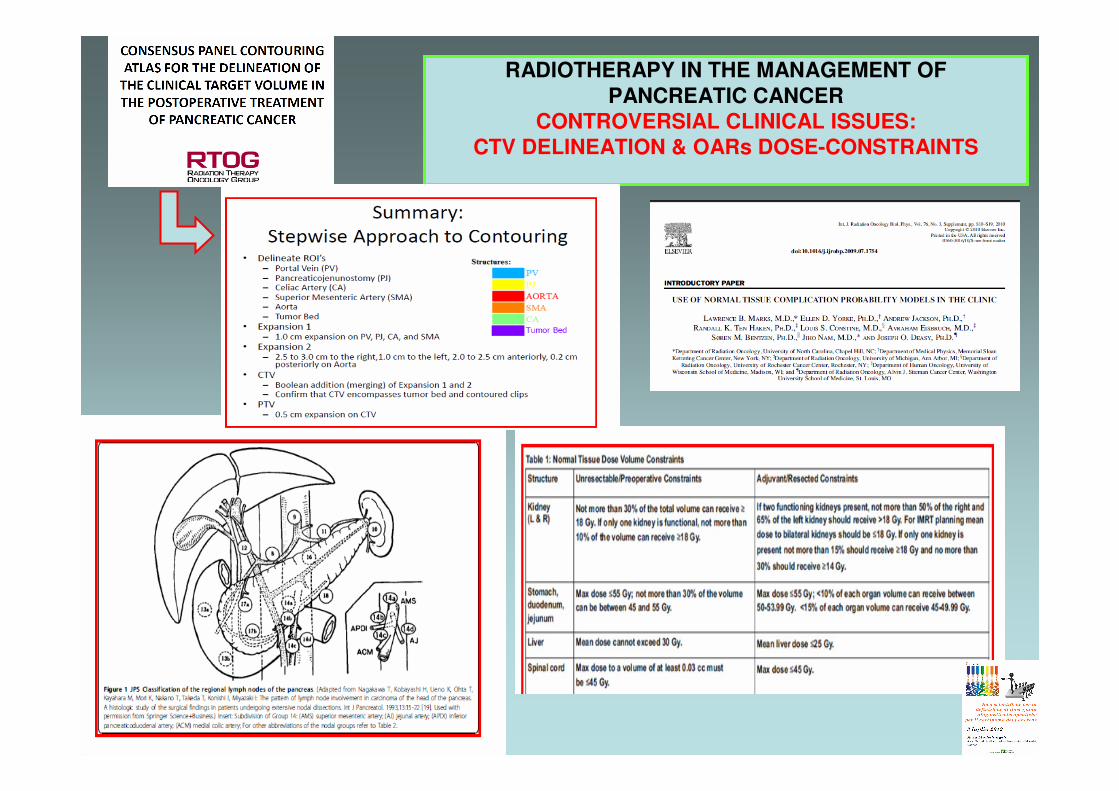
CONTROVERSIAL CLINICAL ISSUES:
CTV DELINEATION & OARs DOSE-CONSTRAINTS
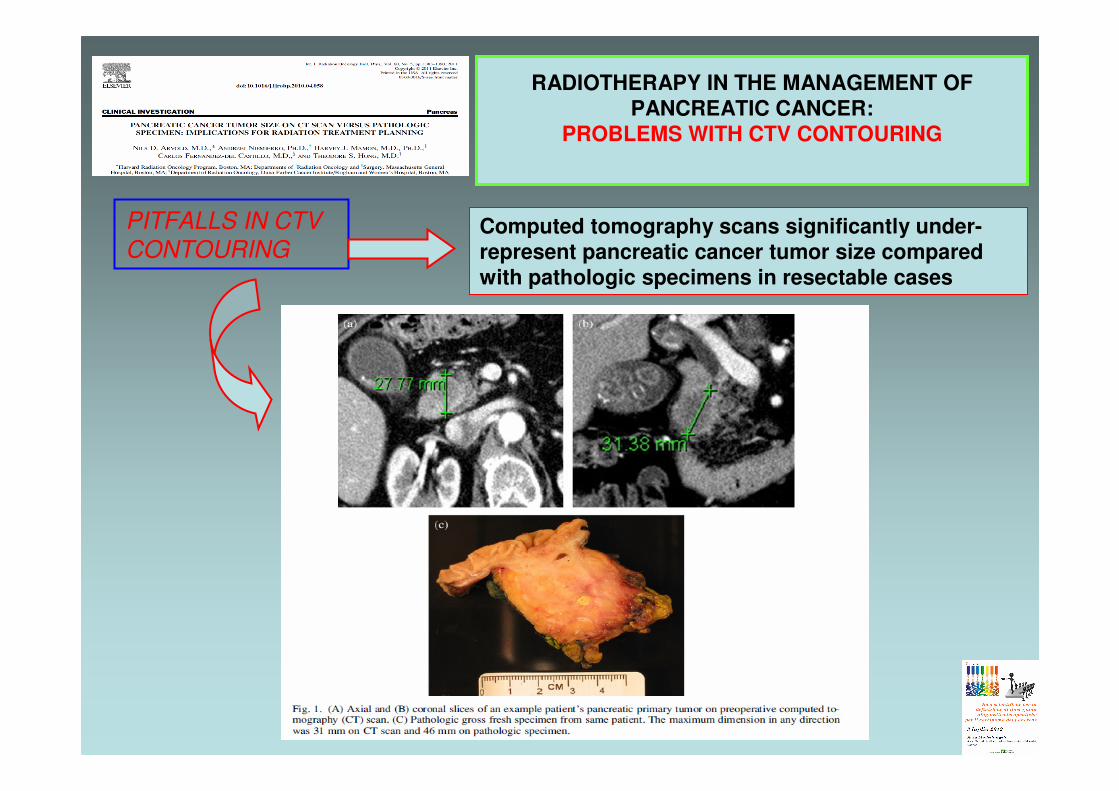
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER:
PROBLEMS WITH CTV CONTOURING
Computed tomography scans significantly under-
represent pancreatic cancer tumor size compared
with pathologic specimens in resectable cases
PITFALLS IN CTV
CONTOURING

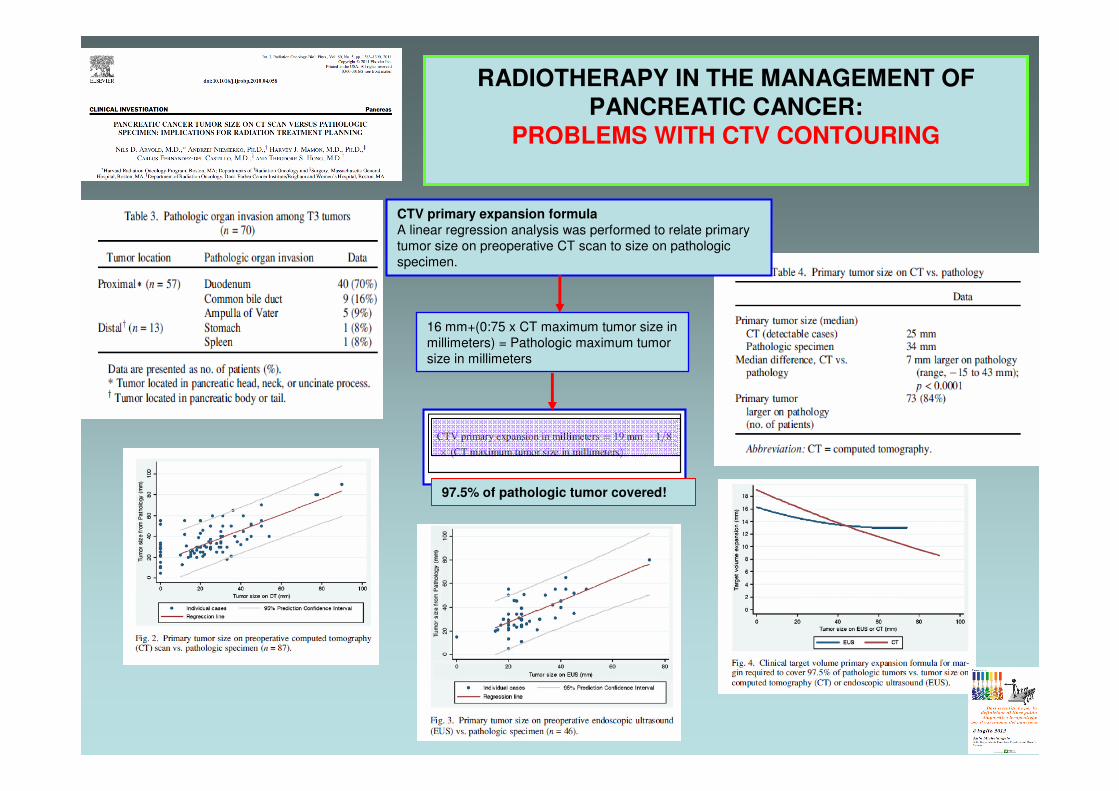
We found that nearly 60% of all tumors in the proximal pancreas (head, neck, or
uncinate process) had pathologic invasion into the duodenum, despite rare evidence
of duodenal invasion on preoperative CT and no cases seen on EUS
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER:
PROBLEMS WITH CTV CONTOURING
The high rate of pathologic duodenal invasion suggests a riskof duodenal undercoverage with highly conformal radiotherapy
CTV primary expansion formulaA linear regression analysis was performed to relate
primary tumor size on preoperative CT scan to size on
pathologic specimen.
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER:
PROBLEMS WITH CTV CONTOURING
CTV primary expansion formula
A linear regression analysis was performed to relate primary
tumor size on preoperative CT scan to size on pathologic
specimen.
16 mm+(0:75 x CT maximum tumor size in
millimeters) = Pathologic maximum tumor
size in millimeters
97.5% of pathologic tumor covered!

RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER
OARs DOSE-CONSTRAINTS FOR PANCREAS RT
Quantitative Analysis of Normal Tissue Effects in the Clinic (QUANTEC).
IJROBP, Volume: 76, Issue: 3, Supplement March 1, 2010
The current dose-constraints to OARs are defined according to the QUANTEC document and are related to specificclinical toxicity endpoints, depending also on the irradiation technique & dose fractionation (3D-CRT/IMRT/SBRT).
OO
AA
RR
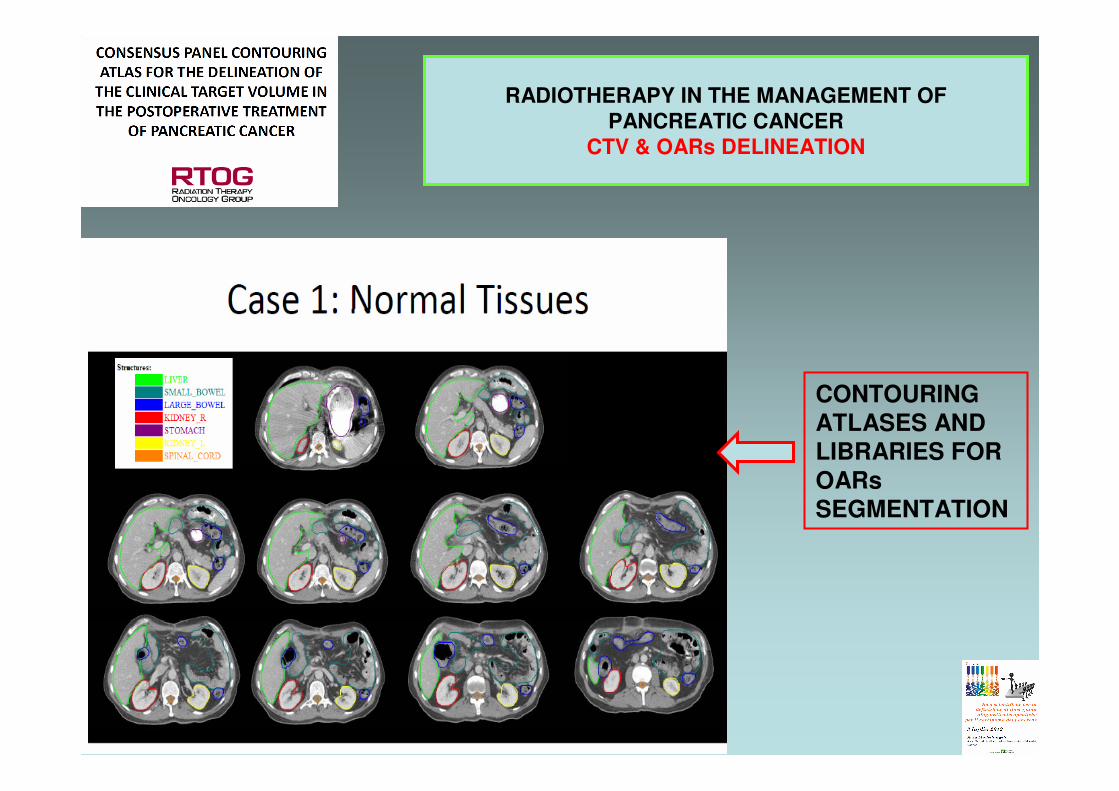
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER
CTV & OARs DELINEATION
CONTOURING
ATLASES AND LIBRARIES FOR
OARs
SEGMENTATION

A Whipple procedure was performed, the pathology showed a 1.3 cm moderately differentiated invasive adenocarcinoma in the pancreatic head with lymphovascular invasion. The marginswere negative; however, 1 of the 15 lymph nodes sampled waspositive. His CA19-9 was less than 3 preoperatively, indicatingthat he quite likely did not produce this marker.• He was staged as pT1N1M0 (AJCC Stage IIB)• The patient was referred for adjuvant chemoradiation
RADIOTHERAPY IN THE MANAGEMENT OF
PANCREATIC CANCER
CTV & OARs DELINEATION
SEVERAL CTVs
ACCORDING TO
SURGICAL
PROCEDURE AND
DISEASE STAGE
Nadia Di Muzio
ADVANCES IN RADIATION THERAPY
TECHNIQUES AND THE CONTRIBUTION OF
NOVEL TECHNOLOGIES:
EXPERIENCE OF THE IRCCS SAN RAFFAELE
LA RADIOTERAPIA DEL
CARCINOMA DEL PANCREAS







