
Learning Disability and Dementia
Pathway
Existing expertise, collaboration and
consistency
Project Report 2012
Thames Valley Health Knowledge Team
1
Table of Contents
Executive Summary ............................................................................................................ 2
Project Report ..................................................................................................................... 4
1. Making the case for change.................................................................................. 4 2. Project Brief……………………………………..…………………………………………5 3. LD Dementia Pathway commonality…………………………………………………..5 4. Picking up Signs and Symptoms……………...……………………………………....6 5. Screening – Preliminary Investigations …………………………………………….. 6 6. Assessment and Clinical Decision Making……………………..……………...……7 7. Formal Diagnosis – Action Planning…………………...……………………..…….10 8. Post Diagnosis………………………………………….……………………………….11 9. On-going Care/Review……………………………….………………………………...11 10. Combined Road Map………………………………….……….……………………….12 11. Closing comments…………………………………..................................................13
Annex 1 - Project Management Team …………..………………………………..……………14
Annex 2 – Project Brief…………………………………………………………………………...15
Annex 3 – Southern Health Pathway...…………………………………………………………19
Annex 4 – Southern Health Pathway Document……………………..………………………20

2
Executive Summary Learning Disability and Dementia Pathway
Existing expertise, collaboration and consistency
Background There have been significant improvements in the mean life-expectancy of people with
learning disabilities over the last 80 years. Given these improvements, it has been predicted
that the proportion of people with learning disabilities over 65 years of age will have doubled
by 2020 (Janicki & Dalton, 2000) and that over a third of all people with learning disabilities
will be over 50 years of age by that time (McConkey et al., 2006). It is therefore now critical
that proper consideration is given to illnesses that occur in later life.
It is also recognised that there is a higher prevalence of dementia in people with a learning
disability than in the general population, with a predicted increase in prevalence of 36%
anticipated by 2021 within learning disabilities services.
Ridgeway Partnership (Oxford Learning Disability NHS Trust) Quality Accounts and Quality
Strategy highlighted the need to develop a coordinated approach to supporting older people
with a learning disability; and now there is suitable evidence of best practice in other areas
which can be transferred to the Oxfordshire context to speed up local developments.
Aims of the project
Project funds, were therefore identified to develop an integrated, and consistent care
pathway for patients with learning disabilities with dementia across Oxfordshire. The care
pathway was to be collaborative in nature, incorporate NICE guidance, and draw on multi-
professional expertise across the system, including from pathways already developed in
Buckinghamshire and Wiltshire.
With the pathway agreed, the project would identify an appropriate training methodology and
then train the relevant staff in implementing the new pathway, with a particular emphasis on
care staff.
A project group, with an independent chair, was established to oversee this work.
Project outcomes
The project group met regularly and were successful in capturing existing positive
practice from multi professional sources. This has been identified in the report below
along with a combined ‘Road Map’ or Care Pathway.
This project’s progress was however interrupted by the processes and organisational
changes associated with Southern Health NHS Foundation Trust taking responsibility for
health care provision for those with a learning disability across Oxfordshire,

3
Buckinghamshire and Wiltshire from Ridgeway Partnership, Oxford Learning Disability NHS
Trust.
At the time of this project, Southern Health NHS FT was in the process of developing an
evidence based care pathway for Dementia themselves. This subsequently received
executive approval and Southern Health NHS FT have responsibility for the roll out of this
across Oxfordshire and beyond for those with learning disabilities. Early attempts were made
to join up the Dementia & LD project and the work developing through Southern Health NHS
FT. However, time did not permit joint working on this occasion. The project group, therefore
agreed that the LD Dementia project should be discontinued to avoid duplication.
It is hoped however that the information contained within the project report can act as an aid
memoire for future work in this area.
References
1. Janicki MP, Dalton AJ. Prevalence of dementia and impact on intellectual disability services. Mental Retardation. 2000;38:276–288. [PubMed]
2. McConkey, R., Mulvany, F. and Barron, S. (2006) Adult persons with an intellectual disability on the island of Ireland. Journal of Intellectual Disability Research (in press)

4
Project Report Learning Disability and Dementia Pathway
Existing expertise, collaboration and consistency
1. Making the case for change
There have been significant improvements in the mean life-expectancy of people with
learning disabilities over the last 80 years. Given these improvements, it has been predicted
that the proportion of people with learning disabilities over 65 years of age will have doubled
by 2020 (Janicki & Dalton, 2000)1 and that over a third of all people with learning disabilities
will be over 50 years of age by that time (McConkey et al., 2006)2. It is therefore now critical
that proper consideration is given to illnesses that occur in later life.
It is also recognised that there is a higher prevalence of dementia in people with a learning
disability than in the general population, with a predicted increase in prevalence of 36%
anticipated by 2021 within LD services.
In 2009, the Royal College of Psychiatrists and the British Psychological Society reported
that: “there is still a great deal of confusion and ignorance about the treatment and care of
those with learning disabilities who have dementia resulting in some quite inappropriate
practice and provision.” And, in 2011, the all-party Ombudsman’s report ‘Care and
Compassion’ suggests that there is inadequate support for the older adult and requests that
healthcare organisations think more carefully about the provision they offer.
Ridgeway Partnership (Oxford Learning Disability NHS Trust) Quality Accounts and Quality
Strategy recognised the significance of the information above and committed to developing
an integrated pathway for dementia in the LD services and across the wider Oxfordshire
health economy. It intended to do this by: maximise local commissioning and clinical
expertise; supporting cross locality collaboration; and ensuring all available evidence of
positive national practice is taken into consideration.
It was fully acknowledged that this work had already begun. Teams had begun to design and
implement localised patient pathways which had already improved services to patients
through a vastly increased multi-professional approach to the care. It is also acknowledged,
however, that there was more to do to ensure universality of best possible practice.
1 Janicki MP, Dalton AJ. Prevalence of dementia and impact on intellectual disability services. Mental Retardation. 2000;38:276–288.
[PubMed] 2 McConkey, R., Mulvany, F. and Barron, S. (2006) Adult persons with an intellectual disability on the island of Ireland. Journal of
Intellectual Disability Research (in press)
5
2. Project Brief
The ‘Existing Expertise, Collaboration and Consistency’ Project (EECC Project)
intended to build on current multi-professional approaches and expertise. It was designed to
ensure that all patients with a learning disability, in need of dementia services, receive the
same high standard of care to either meet or exceed national guidelines, regardless of
whether they live in Buckinghamshire, Wiltshire or Oxfordshire.
This project, funded by the SHA, was undertaken by the Oxfordshire Learning Disability
Trust with leadership and support from Thames Valley HIEC. It was a key priority for the
Trust to honour its responsibilities to older people with a learning disability. Specifically, it
required a coordinated approach to dementia care across the Trust. This was to be done in
accordance with nationally published best practice standards and consistency with other key
priorities in the Corporate Business Plan 2011/12
The aims of the ‘Existing Expertise, Collaboration and Consistency Project’ (EECC
Project) were to:
Ensure a single, standardised, evidence informed care pathway was in place across
Buckinghamshire, Wiltshire and Oxfordshire that:
further improved the care of patients with co-existing Learning Disability and Dementia
was proactive - ensuring all young adults with Down’s Syndrome are offered baseline and prospective screening before the age of 30yrs
removed inequalities in access and provision across counties
drew on good work already in place
identified a process for agreeing any local pathway adaptations – to ensure these are determined by distinct patient and/or carer need alone.
The project ran from February 2012 until September 2012. A full project plan was produced
outlining deliverables, deadlines, risk mitigation and governance. A Steering Group, which
had locality representation including clinical leads, was established under the oversight of an
‘independent Chair’ from outside Oxfordshire. The Steering Group set the direction for the
project and monitored progress and outcome. The project also aimed to:
audit the experience of patients with dementia in LD services in the 3 counties
map all three locality pathways
develop the Assessment of Motor and Process Skills (AMPS) for this context
identified associated training needs for staff groups along the care pathway
disseminate the outcomes of the project widely
3. LD Dementia Pathway - commonality
The first step to identifying an appropriate care pathway was to collect and collate existing
pathway information and expertise. The following care pathway information was collated
from Ridgeway Partnership (Oxford Health NHS FT – Buckinghamshire and Oxfordshire)
and Southern Health NHS FT
6
Care pathway documents and discussions produced the combined Southern Health/
Ridgeway Partnership (Bucks /Oxon) pathway descriptors below. The following areas were
identified as common to all services.
Common areas covered by each service:
1. Signs and symptoms 2. Screening - preliminary investigations 3. Assessment and clinical decision making 4. Formal diagnosis and action planning 5. Post diagnosis
4. Signs and Symptoms 4.1Southern Health
Dementia suspected – Commence LD Dementia Map/Service(Professional with relevant competences)
4.2 Bucks
Referral to Dementia Group – (CLDT Nurse to coordinate) 4.3 Oxon
Referral to Team - (who within the team?) 5. Screening - Preliminary Investigations 5.1 Southern Health
Detailed History – PT & Carer
Plymouth Dementia Screening checklist
Exclude physical/GP physician exam 5.2 Bucks
DSQIID (Dementia Screening Questionnaire for individuals with Intellectual Disabilities) part 1 & 2
Nursing assessment 5.3 Oxon
Health Screen and GP/Family/Carer liaison
The project group reviewed all the information relating to ‘signs and symptoms’ and ‘screening’ and the additional areas listed below were identified for inclusion and further consideration:
Carers and family involvement
Health check - opportunities to screen
Timeframe for each ‘stage’ in the pathway to be identified (Maximum to be specified?)
Baseline assessment needed to track changes that may otherwise go undetected
Tools used to assess need to be specified and meet NICE guidance
Roles – the person responsible needs to be identified
7
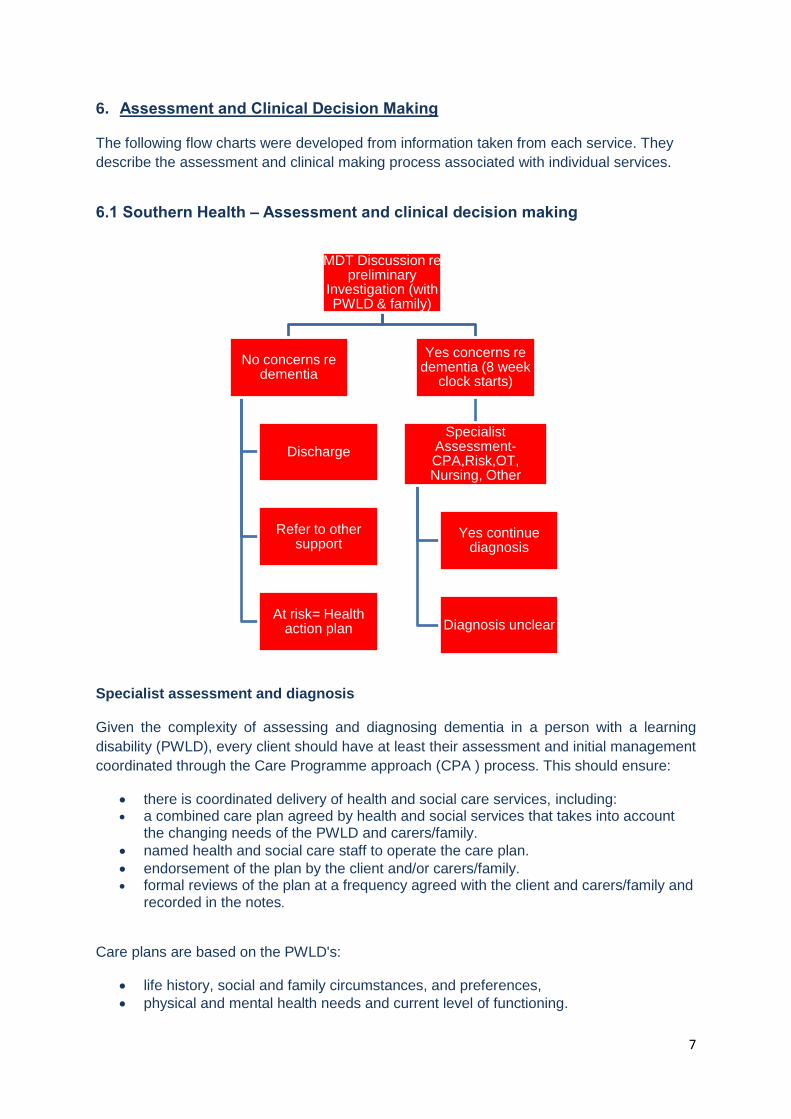
6. Assessment and Clinical Decision Making The following flow charts were developed from information taken from each service. They
describe the assessment and clinical making process associated with individual services.
6.1 Southern Health – Assessment and clinical decision making
Specialist assessment and diagnosis Given the complexity of assessing and diagnosing dementia in a person with a learning
disability (PWLD), every client should have at least their assessment and initial management
coordinated through the Care Programme approach (CPA ) process. This should ensure:
there is coordinated delivery of health and social care services, including: a combined care plan agreed by health and social services that takes into account
the changing needs of the PWLD and carers/family.
named health and social care staff to operate the care plan.
endorsement of the plan by the client and/or carers/family. formal reviews of the plan at a frequency agreed with the client and carers/family and
recorded in the notes.
Care plans are based on the PWLD's:
life history, social and family circumstances, and preferences,
physical and mental health needs and current level of functioning.
MDT Discussion re preliminary
Investigation (with PWLD & family)
No concerns re dementia
Discharge
Refer to other support
At risk= Health action plan
Yes concerns re dementia (8 week
clock starts)
Specialist Assessment- CPA,Risk,OT, Nursing, Other
Yes continue diagnosis
Diagnosis unclear
8
Good communication between health and social care professionals and PWLDs, and
families and carers, is essential. The PWLD, their carers and families should be provided
with information about the services available, assessment process and interventions at all
stages of the pathway. This should be supported by evidence-based written information
tailored to the client’s needs and ability. Evidence suggests that when people with dementia
and their carers are well–prepared and supported, initial feelings of shock, anger and grief
are balanced by a sense of reassurance and empowerment.
In addition, it is important that a person centred approach is taken to both assessment and
management. The latter should take into account the clients’ needs and preferences. PWLD
should have the opportunity to make informed decisions about their management, in
partnership with health and social care professionals. If people do not have the capacity to
make decisions, professionals should follow the Department of Health’s advice on consent
(available from www.dh.gov.uk/consent ) and the code of practice that accompanies the
Mental Capacity Act (summary available from www.publicguardian.gov.uk ).
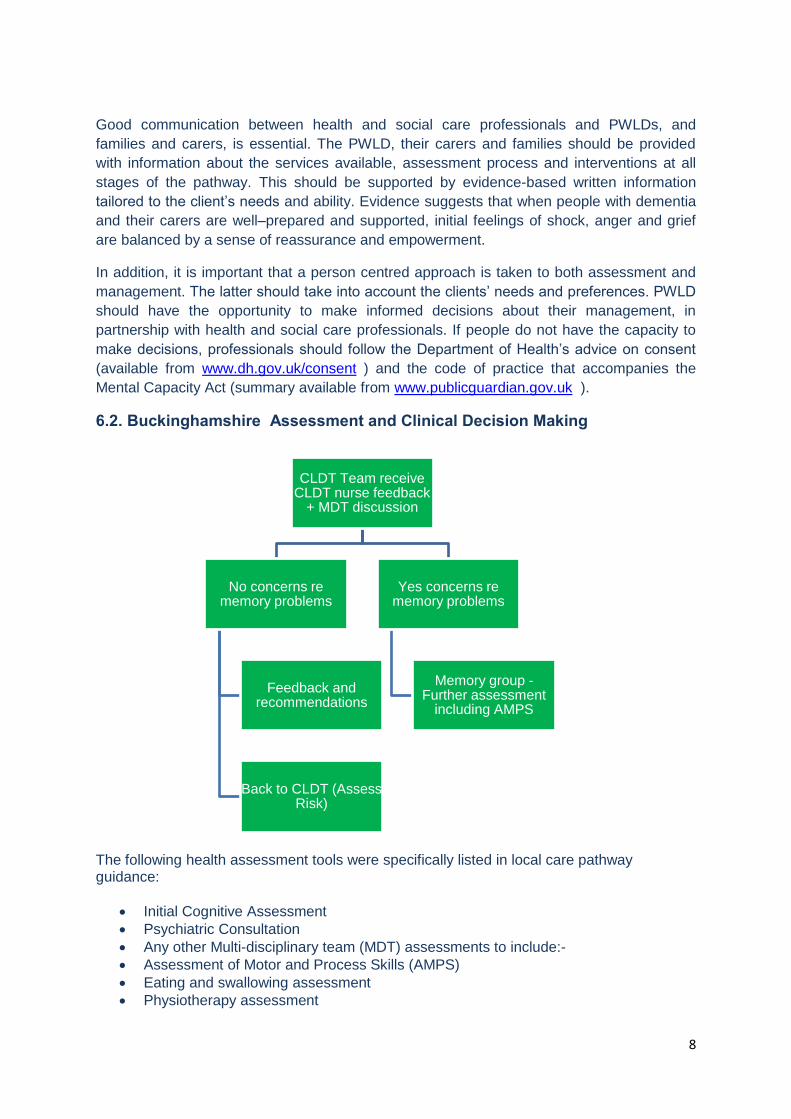
6.2. Buckinghamshire Assessment and Clinical Decision Making
The following health assessment tools were specifically listed in local care pathway guidance:
Initial Cognitive Assessment
Psychiatric Consultation
Any other Multi-disciplinary team (MDT) assessments to include:-
Assessment of Motor and Process Skills (AMPS)
Eating and swallowing assessment
Physiotherapy assessment
CLDT Team receive CLDT nurse feedback
+ MDT discussion
No concerns re memory problems
Feedback and recommendations
Back to CLDT (Assess Risk)
Yes concerns re memory problems
Memory group - Further assessment
including AMPS
9
Hearing therapy assessment
Environmental assessment
Community Care Act assessment
Communication assessment
Epilepsy assessment
Risk assessment
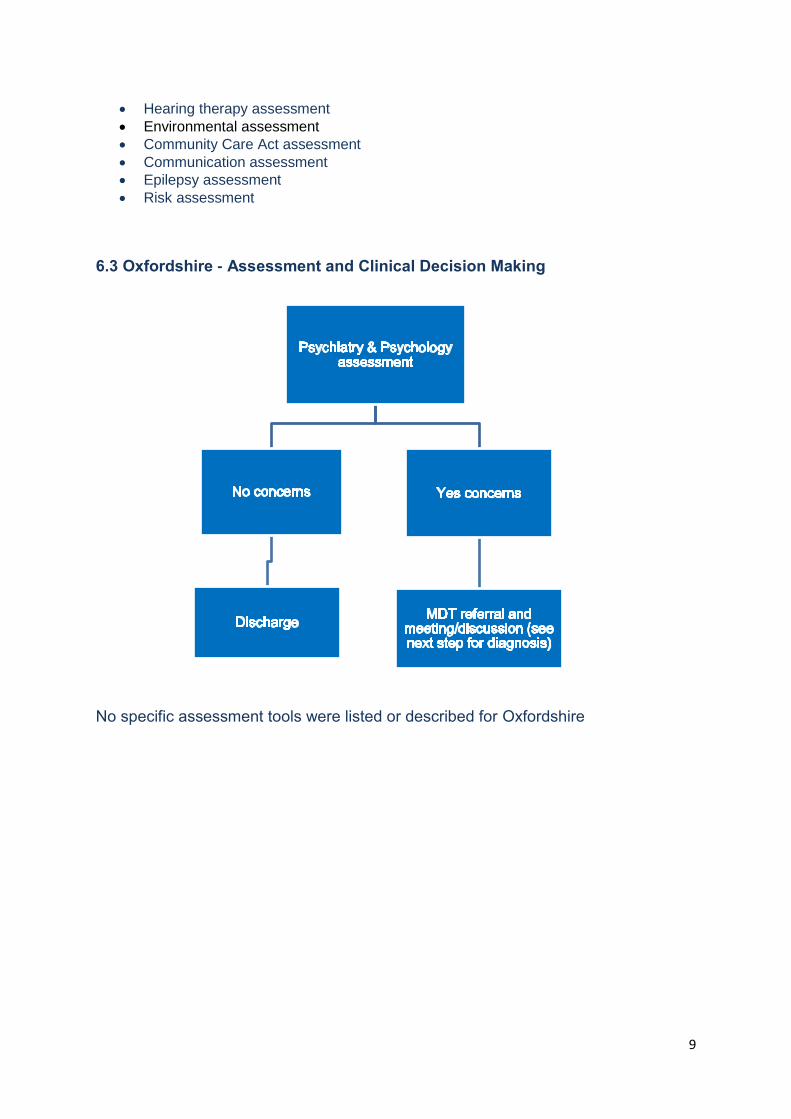
6.3 Oxfordshire - Assessment and Clinical Decision Making
No specific assessment tools were listed or described for Oxfordshire

10
7. Formal Diagnosis – Action Planning
7.1 Southern Health - Formal Diagnosis and Action Planning
7.2 Buckinghamshire - Formal Diagnosis and Action Planning
DMR – Dementia questionnaire for Mentally Retarded Adults was specifically identified
7.3 Oxfordshire - Formal Diagnosis and Action Planning
Formulation meeting – inc. clinical psychologist and MDT to give holistic/formal view of
needs
Is diagnosis clear? If not repeat earlier stages
Baseline DMR (Repeat DMR at 6/12months) – re. Down’s
Appointment with psychiatrist
Confirm Diagnosis or give ‘provisional diagnosis’

11
8. Post Diagnosis
The following information regarding ‘post diagnosis’ was available in each area:
8.1 Southern Health – Post Diagnosis
CPA - Set up new CPA review to agree plan (including:- all Clinicians involved to
date, family & PWLD)
Info to client and carers
Managing behaviour and symptoms
Meds versus non-meds
Cognitive symptoms list
Management of co morbidity
Risk assessment and management
Palliative Care
Resuscitation Policy
8.2 Buckinghamshire – Post Diagnosis
Agree Management Plan/CPA
post diagnosis/intervention
Anti-dementia medication
Efficacy monitored using nursing DMR
CPA - Person centred
Family/carers invited to Dementia Training
No review mentioned
Need to add risk assessment
8.3 Oxfordshire – Post Diagnosis Person centred care plan Info for PT/Carers, Training to carer
9. On-going Care/Review 9.1 Southern Health – on-going care
Regular Reviews – person centered – MDT + CPA, if more than two professionals. Frequency determined by need.
9.2 Buckinghamshire – on-going care
Memory group follow-up at 3/6/9/12 months determined by need.
9.3 Oxfordshire– on-going care
Regular review identified (Review/ Specify, When & Why)
9.4 Areas discussed The project group reviewed all the information above and the additional areas listed below were identified for inclusion and further consideration: Who picks up what/when? (MDT/dementia group); context differentials? i.e. LD teams/ + inpatients; different tools listed – need to include AMPS ; all good processes – same order
12
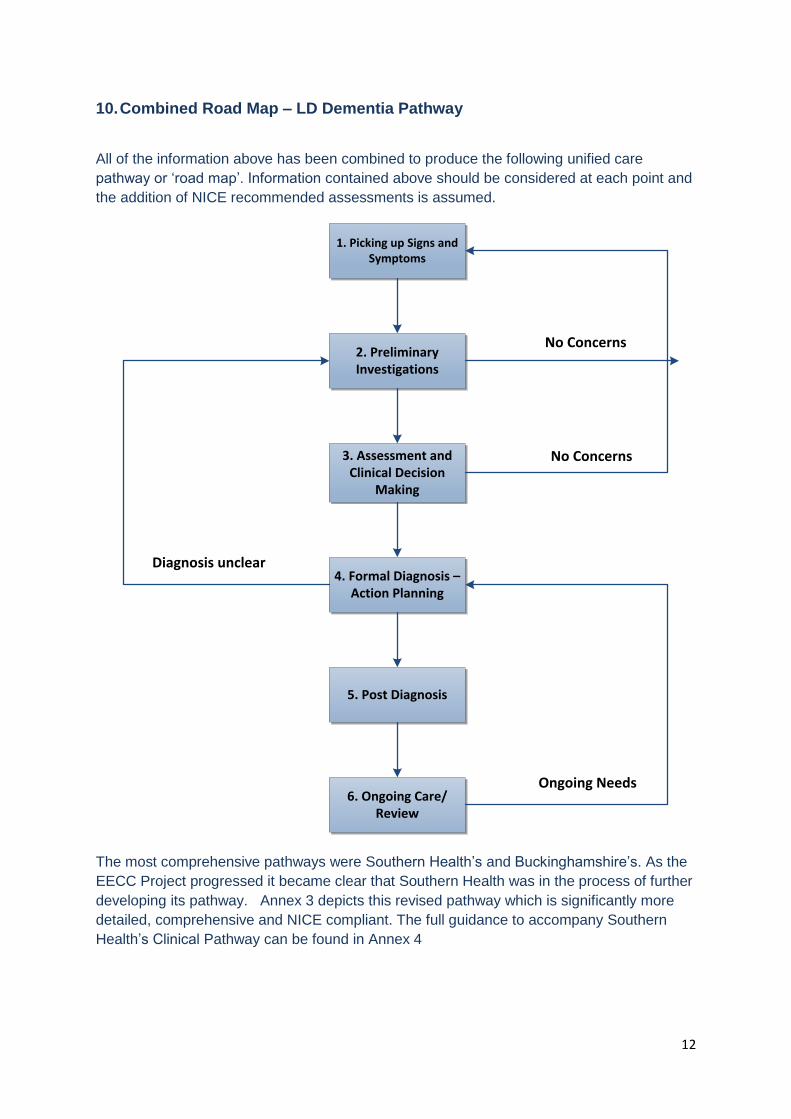
10. Combined Road Map – LD Dementia Pathway
All of the information above has been combined to produce the following unified care
pathway or ‘road map’. Information contained above should be considered at each point and
the addition of NICE recommended assessments is assumed.
1. Picking up Signs and Symptoms
2. Preliminary Investigations
3. Assessment and Clinical Decision
Making
4. Formal Diagnosis – Action Planning
5. Post Diagnosis
6. Ongoing Care/Review
No Concerns
No Concerns
Diagnosis unclear
Ongoing Needs
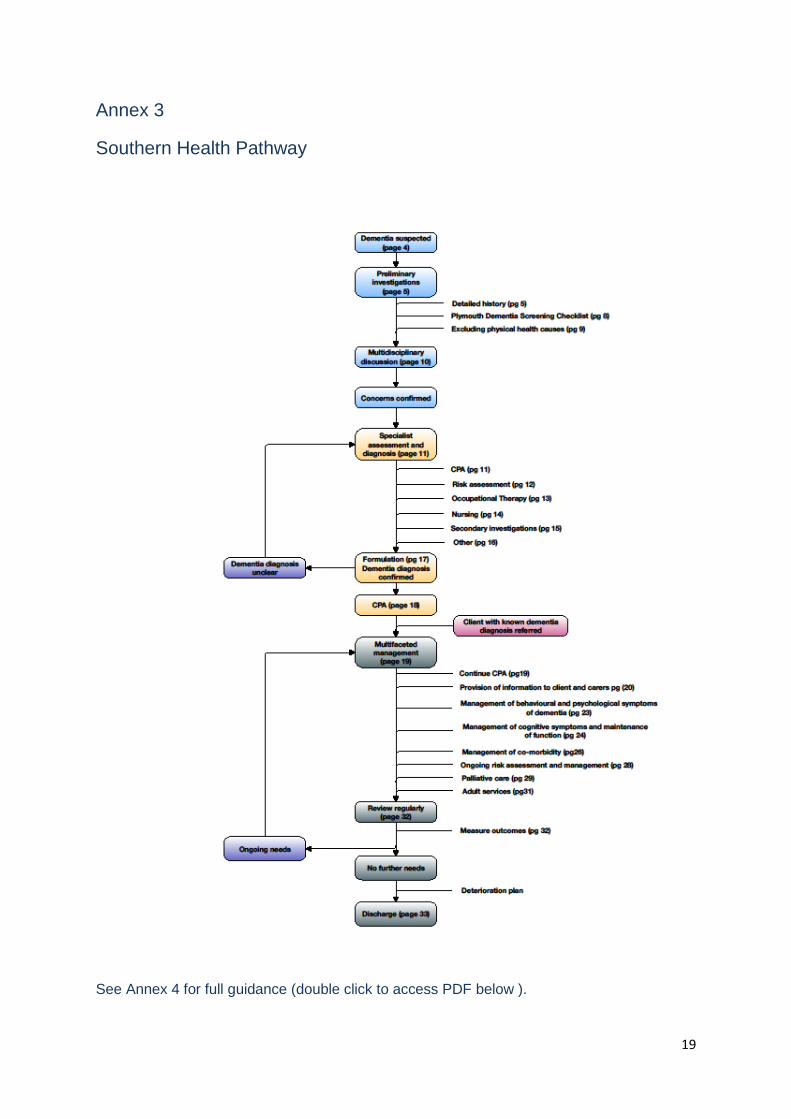
The most comprehensive pathways were Southern Health’s and Buckinghamshire’s. As the
EECC Project progressed it became clear that Southern Health was in the process of further
developing its pathway. Annex 3 depicts this revised pathway which is significantly more
detailed, comprehensive and NICE compliant. The full guidance to accompany Southern
Health’s Clinical Pathway can be found in Annex 4
13
11. Closing Comments
The pathway developed within Southern Health subsequently received executive approval
and Southern Health NHS FT have responsibility for the roll out of this across Oxfordshire
and Buckinghamshire for those with a learning disability. Early attempts were made to join
up the EECC Dementia & LD Project and the work developing through Southern Health NHS
FT. However, time did not permit joint working on this occasion. The project group therefore
agreed that the EECC project should be discontinued to avoid duplication.
It is hoped however that the information contained within this project report can act as an aid
memoire for future work in this area.
14
Annex 1
Project Management Team Structure
The core project team comprised of:
Jackie Prosser – Project Chair - Mental Health in Practice Ltd (appointed by the HIEC as an independent and external professional)
Yvonne Frewin - PM, Thames Valley Health Innovation and Education Cluster
Rachel Miller – Professional Head of OT, Ridgeway Partnership
Diane Statham – Head of Research and Development, Ridgeway Partnership
Multi professional stakeholders
Bucks Team Clinical Specialists
Helen Fletcher – Psychologist Bucks
Sheri Forchione – CQUIN Dementia Lead for Bucks, Oxford Health
Rajnish Attavar – Consultant Psychiatrist for Bucks Oxfordshire Team Clinical Specialists
Sarah Coles - Senior Clinical Psychologist for Oxfordshire
Amalsha Vithanaarachchi – Psychiatrist for Oxfordshire
Amanda Kitteringham - Community Nurse for Oxfordshire Wiltshire Team Clinical Specialists
Sarah Philips - Principal Counselling Psychologist for Wiltshire
15
Annex 2
Project Brief (prepared by Thames Valley HIEC for the SHA)
Innovation Adoption Challenge
Introduction
Care and Compassion, the Ombudsman’s report into the treatment of older people, identified
inadequate support for this group, requiring healthcare organisations to think more carefully
about the provision they offer to the older person. This is particularly an issue in the learning
disabilities service, where patients with dementia are expected to increase by 36% by 2021.
The purpose of this bid is to develop an integrated care pathway in Oxfordshire for patients
with learning disabilities with dementia. This care pathway will be based on those already
developed in Buckinghamshire and Wiltshire.
There have been significant improvements in the mean life-expectancy of people with
learning disabilities from as little as an estimated 18.5 years in the 1930s to 59 years in
1970s to 66 years in the 1990s (Braddock, 1999). Given these improvements, it has been
predicted that the proportion of people with learning disabilities over 65 years of age will
have doubled by 2020 (Janicki & Dalton, 2000) and that over a third of all people with
learning disabilities will be over 50 years of age by that time (McConkey et al., 2006). It is
because of these factors that consideration needs to be given to those age-related illnesses
that most commonly occur in later life, such as dementia. However, there is evidence from
several studies that people with learning disabilities have an increased risk of developing
dementia with increasing age compared to that observed in the general population.
Unfortunately, these particular patients may be too young to access general services for
patients with dementia which may not, in any case, be suitable for their particular needs.
There is thus a developing prevalence of adults with LD with early dementia and the need for
a coherent multi-agency response to this.
Aims of the project
The aim of the project is to source extra support and capacity to adopt the care pathways
that work well elsewhere for the context of Oxfordshire, and then to train the relevant staff in
implementing the new pathway, with a particular emphasis on care staff.
Background - why this and why now
There is a known higher prevalence of dementia in people with a learning disability. In 2009,
the Royal College of Psychiatrists/The British Psychological Society reported jointly that:
“there is still a great deal of confusion and ignorance about the treatment and care of those
with learning disabilities who have dementia resulting in some quite inappropriate practice
and provision.”
Since that time, attempts have been made to develop an integrated pathway for dementia in
the LD services and across the whole of the Oxfordshire health economy, but no great
progress has been made. In contrast, in both Buckinghamshire and in Wiltshire, care

16
pathways have been designed and implemented which improve services to patients through
a vastly increased multi-professional approach to the care of such patients.
Ridgeway Partnership (Oxford Learning Disability NHS Trust) Quality Accounts and Quality
Strategy highlight the need to develop a coordinated approach to supporting older people
with a learning disability; and now there is suitable evidence of best practice in other areas
which can be transferred to the Oxfordshire context to speed up local developments.
In part, the project funding is sought to employ an independent Chair for the Steering Group,
who will have credibility, and who is seen as having no vested interest in this area other than
a desire to make a positive contribution to patient care. It is anticipated that this will be an
important factor in unblocking some of the local resistances to change.
NICE guidelines specifically require that “when developing a care plan for a person with a
learning disability newly diagnosed with dementia, an assessment using the Assessment of
Motor and Process Skills (AMPS) should be considered.” This is one area that work already
completed in the Trust has identified as needing development as part of the implementation
of the revised pathway.
How does the proposal support key organisational priorities
For Ridgeway Partnership, a key priority in the Quality Accounts is that the Trust is compliant
with its responsibilities to older people with a learning disability. Specifically, it requires a
coordinated approach to dementia care across the Trust. This will be done in accordance
with nationally published best practice standards from the relevant bodies.
Key elements of NICE guidelines in relation to dementia are: integrated working across all
agencies; provision of memory assessment services as a point of referral for diagnosis of
dementia; assessment, support and treatment (where needed) for carers; assessment and
treatment of non-cognitive symptoms and behaviour that challenges; dementia care training
for all staff working with older people; and improvement of care for people with dementia in
general hospitals.
Among the RCP/BPS key points in Dementia and People with Learning Disabilities, are:
It is important to utilise the skills of the multi-disciplinary team to support the
individual with learning disabilities and dementia.
Other agencies as well as those in the statutory sector can help to support the
person and their carers.
In order to achieve the organisational priorities for the Trust, it will be necessary to be
mindful of the national guidelines. Other key priorities in the Corporate Business Plan
2011/12 which will be addressed by this project are:
Working towards a philosophy of more people-centred services
Working more closely with commissioners/ commissioning for outcomes For the Thames Valley HIEC, the proposal supports their priority for Integrated Services.
17
Intended outcomes / benefits
By the end of the project we will have:
Researched the Bucks and Wiltshire approaches in more detail and learned from their experience of implementation
Audited the experience of patients with dementia in LD services in the 3 counties
Mapped those pathways against one another and redesigned the Oxfordshire pathway
Gained agreement from a cross-organisational multi-professional steering group
Developed the Assessment of Motor and Process Skills (AMPS) appropriately for this context
Designed or procured a training programme and planned its implementation to appropriate staff groups
Started the roll-out of the training programme
Disseminated the outcomes of the project across Oxfordshire
Details of where it has been proven and a description of the outcomes
achieved
Service users and staff report improved outcomes as a result of the changes made in
Buckinghamshire and Wiltshire. However, a part of this work is to audit the differences
between standards across Bucks, Wiltshire and Oxfordshire in order to provide a baseline
from which to measure service improvement to get Oxfordshire to the level of the best of the
three services.
More generally, there is ample research evidence of how care needs to be improved for LD
patients with dementia, and what are the best ways to achieve this. As long ago as 2001,
good practice guidance from the Foundation for People with Learning Disabilities (Turk et al.,
2001) recommended that every service for people with learning disabilities should set up a
register of adults with Down’s syndrome, conduct a baseline assessment of cognitive and
adaptive functioning before the age of 30 years, develop specialist skills in this area, offer
training to other professionals, front line staff and carers, and seek high quality co-ordination
between agencies. Despite this, the availability of screening and treatment across the UK is
inequitable. Although in most areas reactive assessment is provided for those with signs of
deterioration, very few services offer baselines and prospective screening such as that
described by McBrien et al. (2005) to all young adults with Down’s syndrome.
In addition, there are a range of specific factors associated with adults with learning
disabilities who develop dementia such as epilepsy, pain, sleep disorders etc. National
research has informed the development of approaches to combat these, and an element is
built into the budget to enable some time to visit others sites as they are identified where
there is a particularly effective approach which can be added to the adoption of the basic
pathway from Bucks/Wilts.
18
Who supports the plan - within your organisation and partner organisations?
Dr. John Turnbull, Director of Quality and Information, Ridgeway Partnership
Rachel Miller, Professional Head of OT, Ridgeway Partnership
Diane Statham, Head of Research and Development, Ridgeway Partnership
Sherry Forchione, CQUIN Dementia lead Bucks, Oxford Health
Dr. Catherine O’Sullivan, Chief Executive, Thames Valley HIEC
How it will be delivered and sustained?
The project will start in March 2012 and will run until the autumn. A full PID will be produced
outlining deliverables, deadlines, risk mitigation and governance. A Steering Group of
relevant clinical leads will be established under the leadership of an independent Chair from
outside Oxfordshire. The Steering Group will set the direction for the project and monitor
progress and outcomes.
At the end of this project, an effective steering group will have been established involving all
the key stakeholders who will be able to continue to ensure that the new service is delivered
according to plan. Consensus will have been developed in that group about the new
pathway and training will have been offered to targeted staff. After this time, the pathway will
be self-sustaining as it will be commonly accepted across the locality.
How you will share learning?
At least one event will be held for staff across Oxfordshire to introduce the new pathway, and
the associated training. However, it is likely that more than one event will be needed in
order to build local ownership, determined by the independent Chair and the steering group.
A willingness to produce a baseline report and a quarterly report
Thames Valley HIEC is experienced at producing the full range of appropriate monitoring
information in order to give assurance that the project is being managed effectively. All
partners to this proposal are happy to give the assurance that they will comply with whatever
monitoring arrangements that the SHA wants to put in place. The metrics used for the
project will include; patient outcome measures in line with service norms, staff and patient
satisfaction, project deliverables and deadlines.
19
Annex 3
Southern Health Pathway
See Annex 4 for full guidance (double click to access PDF below ).
20
Annex 4 Southern Health - LD Dementia Document 2012.pdf







