

Lecture 3
MRSAMethicillin resistant S. aureus
Tues – 1/15/2008

S. aureus – the pathogen
• Microbiology – Gr+ cocci with many virulent factors (toxins and enzymes)
• Frequent nosocomial- and community-acquired pathogen
• Mode of transmission – contact
• Clinical manifestations:– Skin and soft tissue infections– Pneumonia– Osteomyelitis / Arthritis– Bacteremia / Sepsis – Endocarditis– Toxin-mediated disease: TSS, Food
poisining
S. aureus - Epidemiology
• Epidemiologic niche: – Nasal carriage (anterior nares)– GI tract (rectal)– Perineal– Throat
• Nasal carriage – 30% of adults– 20% Persistant carriers– 60% Transient carriers– 20% Never carriers
• Nosocomial transmission – transient hand carriage

Risk groups with high carriage rates
• Diabetes Mellitus• Dialysis patients• HIV• Chronic skin diseases• IV Drug abusers• Health care workers (?)

Antimicrobial resistance of S. aureus - history
200320001990198019701960
Introduction of Methicillin – ‘59
Epidemic spread of MRSA, Europe, India, Australia, USA
MRSA single clone theory Lacey & Grinsted, ‘73
Cloning of mecA
Matsuhashi ‘86
SCCmec sequenced Ito ‘99
1st MRSA isolate ‘61
2nd wave of epidemic MRSA (MDR), USA,
Australia, Ireland
Worldwide dissemination
Increasing reports - CA-MRSA
1st VISA, Japan ‘97 1st VRSA, USA ‘02
SA genome sequence, Kuroda ‘01
CA-MRSA sequence, Baba ‘02
CA-MRSA in Australia

MRSA – mechanism – I
• Horizontally transferred DNA element - SCCmec.
• Site specific recombination.
• mecA gene encodes PBP2a.
• PBP2a = 78 KDa PBP - capable of cell wall synthesis.
• PBP2a has low affinity for all -lactams.

MRSA - mechanism of resistance
1. Modifying enzymes
2. Degrading enzymes
3. Target Change
4. Efflux pumps
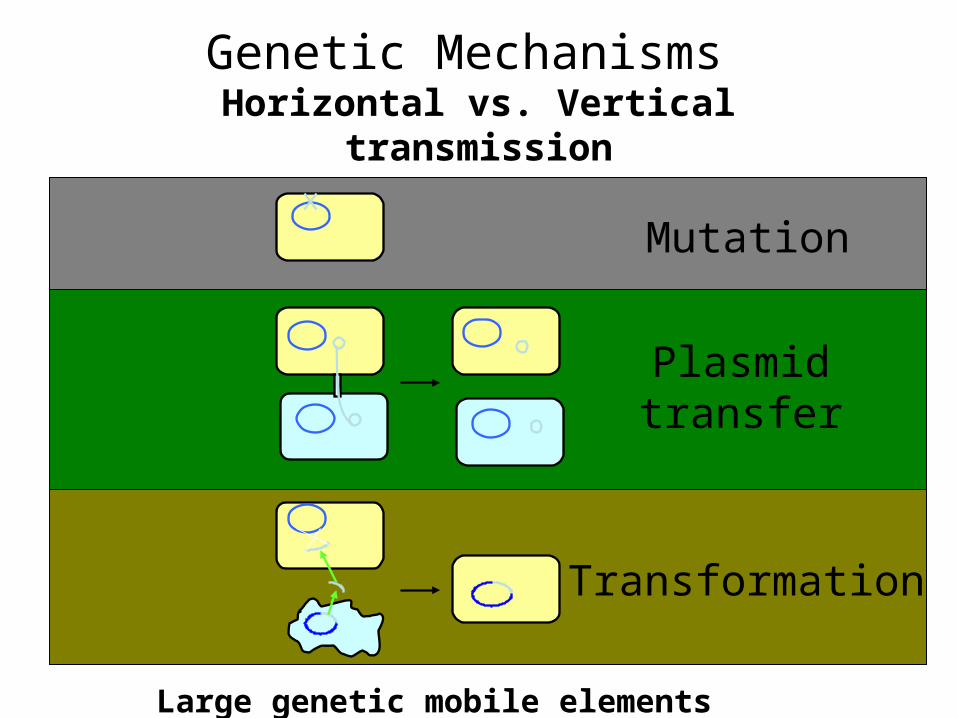
Transformation
Plasmidtransfer
Genetic Mechanisms Horizontal vs. Vertical transmission
Mutation
Large genetic mobile elements (cassettes)
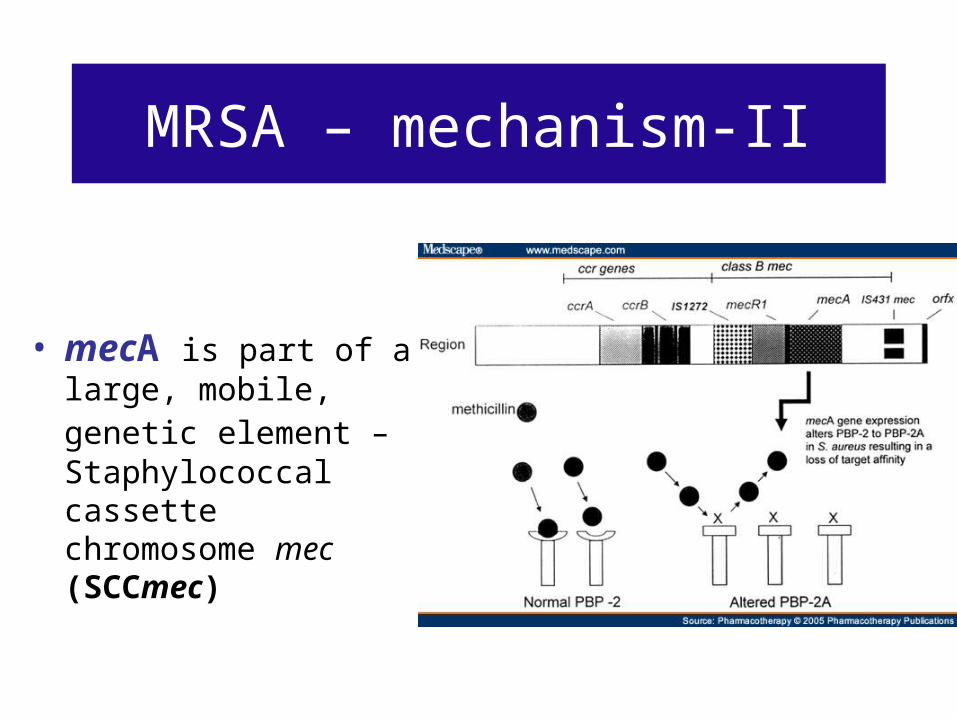
MRSA – mechanism-II
• mecA is part of a large, mobile, genetic element – Staphylococcal cassette chromosome mec (SCCmec)

SCCmec cassette
• A unique class of mobile genetic element (21-67kb) • Resembles a pathogenicity island, but with no virulence
genes.• Ccr complex: ccrA & ccrB encode recombinase A & B enable
SCCmec to integrate into the chromosome in correct orientation.
• Mec complex: encodes β-lactam resistance and its inducible regulation + transposons + integrated copies of plasmids that carry various resistance genes (non-b-lactam)
ccr complex (type2)Mec complex (class B)
orfX
IS 1272mecR1
mecA IS431mec

ccrA3ccrB3
Tn554 mecImecR1
mecAIS431mec
pT181
IS431 IS431
merTn554
orfXccr complexmec complex (class A)
ccr complex (type3)
Type III SCCmec (67kb)
ccrA1 ccrB1R-IIS1272
mecR1
mecAIS431mec
orfXTypeI SCCmec (34kb)
mec complex (class B)
ccr complex (type 1)
ccrA2 ccrB2 Tn554 mecImecR1
TypeII SCCmec (53kb)
mec complex (class A)orfX
IS431mec
pUB110
IS431mec
ccr complex (type 2)
ccr complex (type2)Mec complex (class B)
orfX
IS 1272mecR1
mecA IS431mec
Type IV SCCmec (24kb)
mecA

Genetic organization of SCCmec type I-VI de Lencastre et al. 2007

Origin of SCCmec and the mec gene
• Single clonal origin theory• Hiramatsu et al. 1996: Clonal diversity:
different strains developed independently
• Origin of mecA gene - horizontal transfer from:– SCN – S. scuiri– Enterococcus hiriae


Prevalence of MRSA in USA (cumulative data 1998-2005) / Shorr CID 2007

MRSA among S. aureus isolates in Europe
MRSA – a nosocomial pathogenUntil ~1996

CA-MRSA – an emerging infection
JAMA 1998
EID 2003
CID 2004

CA-MRSA: 1996-2008Changing definitions
• No contact with health-care facilities in prior 6-12 m.– Maybe more than 1y.
• Resistant only to b-lactams, but not to other classes.– Resistant to quinolones, macrolides and
others
• SCCmec IV– and V … and VI…
X X

Community acquired MRSA (CA-MRSA)/ Weber. CID 2005

Risk factors for MRSA
CA-MRSA
• Skin, soft tissue infection
• ???
HA-MRSA
• Previous contact with health care system
• Longer hospitalization• ICU admission or
invasive procedures• Ab Rx.

Clonal spread of MRSA
• Spread is mainly clonal. Only few clones are the cause of most infections.
• Major cause for clonal spread: lapses in IC
• Yet - role of Ab pressure:…
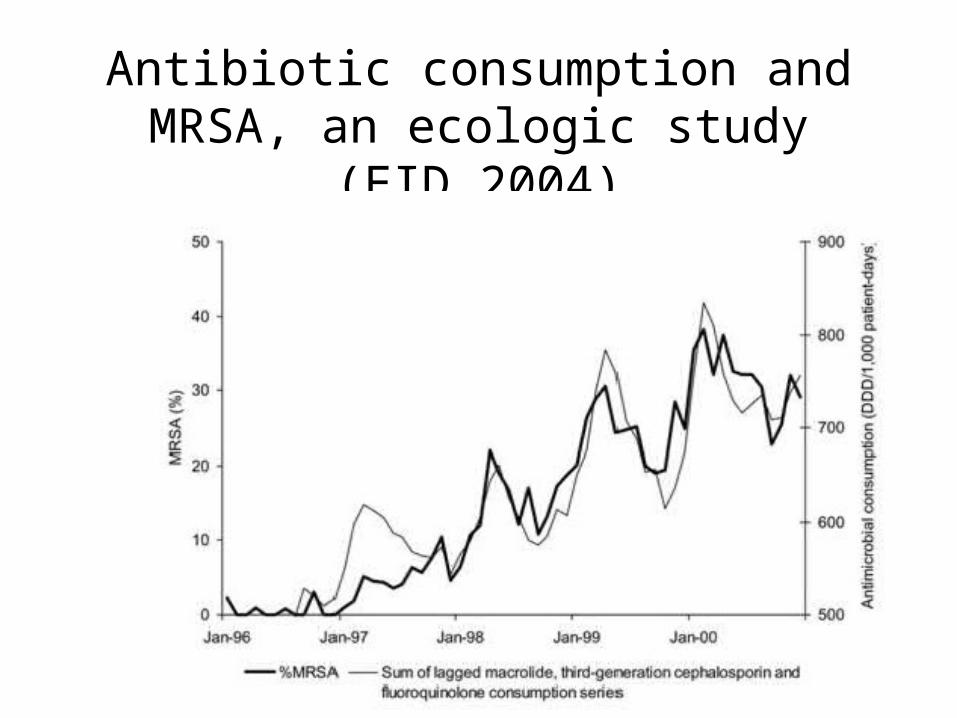
Antibiotic consumption and MRSA, an ecologic study (EID 2004)

Changing Epidemiology of MRSA / Crum et al. Am. J. Med 2006

CA-MRSA infections in Texas (2002-2004) / Kaplan et al. CID 2005

MRSA in the Netherlands

How did CA-MRSA evolve?
• Recent evolution of CA-MRSA from common MSSA?
• “Hospital escape” of unsuccessful HA-MRSA

SCCmec Type IV = “Mobile mec”
• Novel SCCmec type
• Smaller – more efficient horizontal transfer
ccr complex (type2)Mec complex (class B)
orfX
IS 1272mecR1
mecA IS431mec
24kb
Small Size

Resistance and virulenceUS300
• Major CA-MRSA clones in US: US300 & US400
• US300 – the most common single clone of CA-MRSA
• SCCmec IV• Resistant to ciprofloxacin (mutation in gyrA)• Many strains acquired MDR by plasmides (tetK, erm )
• Several mobile genetic elements• Several Toxins

Resistance and virulencePanton Valentine leukocidine
• A pore forming cytotoxin• Strains containing pvl genes were associated
with severe SST – infections• Direct role of pvl – still controversial

ACME – arc gene cluster Complete genome sequence of US300
/ Diep et al. Lancet 2006
• Arginine Catabolic Mobile Element: virulence/strain survival factor
• Different from native arc gene carried by all S. aureus• Highly similar to ACME from S. epidermidis
• Arginine deiminase pathway – Inhibits the nitric oxide production– Allows survival in low ph, anaerobic conditions
• Enhances fitness: enhances potential to grow and survive within a host
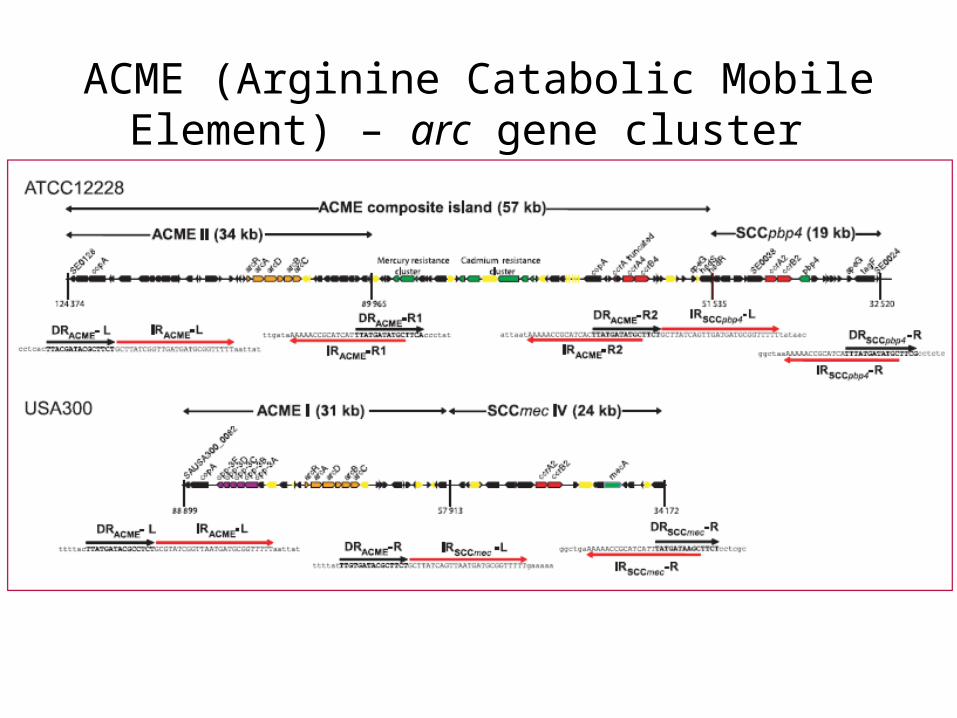
ACME (Arginine Catabolic Mobile Element) – arc gene cluster

ACME positive isolates in UK / Ellington et al. JAC 2008
ST97
ST8
ACME neg
ST8 (US300)

How do we control MRSA?
• Hospitals: – Infection control!!!– Antibiotic control??
• Community:– ?????

Treatment of MRSA
CA-MRSA
• Clindamycin ??– (high ery-R suggests
inducible clinda-R)
• TMP-SMX?• Rifampin?• Vancomycin
HA-MRSA
• Vancomycin
• Linezolid• Daptomycin







